Embed Size (px)
Citation preview
RESPIRATORY SYSTEM REVIEW
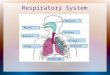
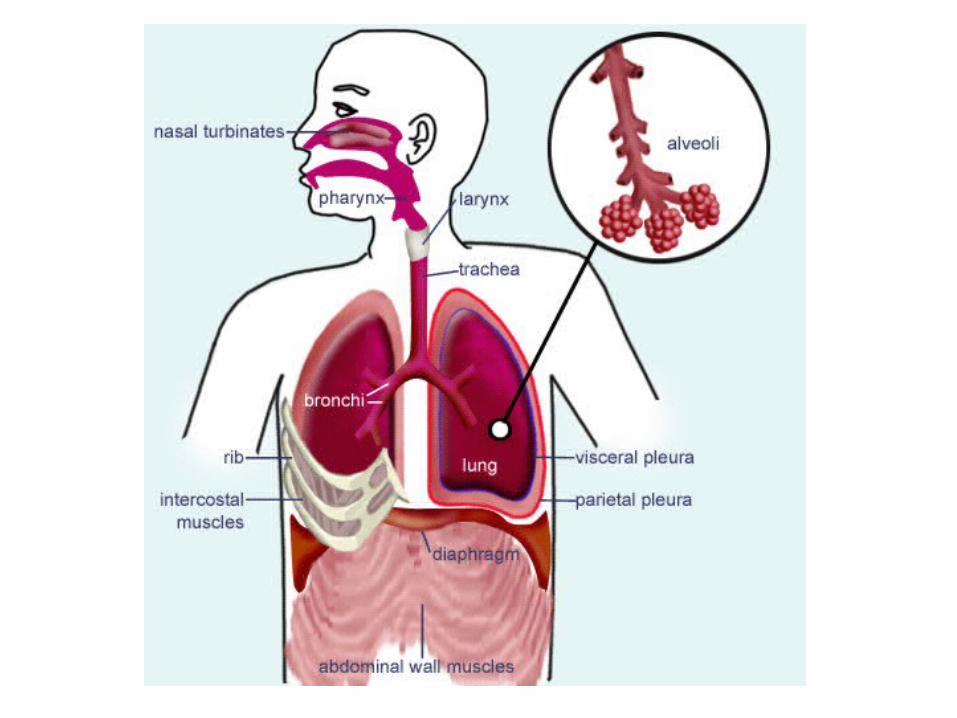
Respiratory System Anatomy • 2 lungs + airways + blood vessels + chest wall(Fig.25-1)
– Mediastinum – space between lungs
• Chest wall - protects lungs; muscular support for breathing
– Pleura with space between folds
• Membrane adheres to lungs, folds over itself, attaches to chest wall
• Space between the folds
– Usually filled w/ thin layer of fluid
– Important for lubrication; decr friction as membrane layers move against each other
– Gas P in pleural space < air P in lungs, airways
• Impt to gas pressure differential; helps lungs expand, stretch as chest wall moves out
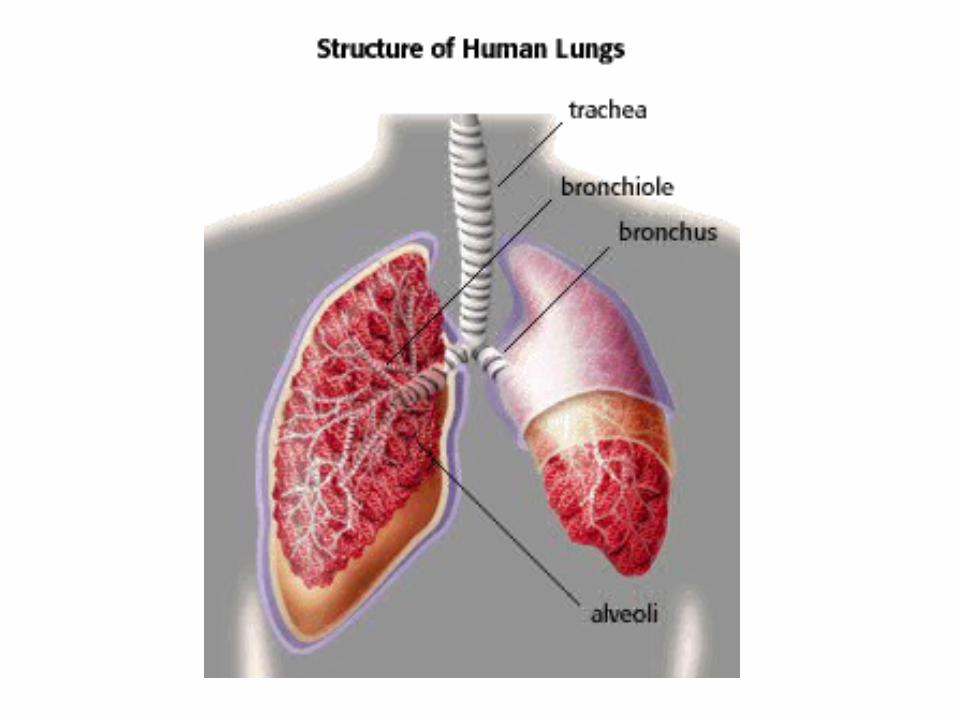
• Airways - tracheobronchial tree branches to alveoli (25-3)
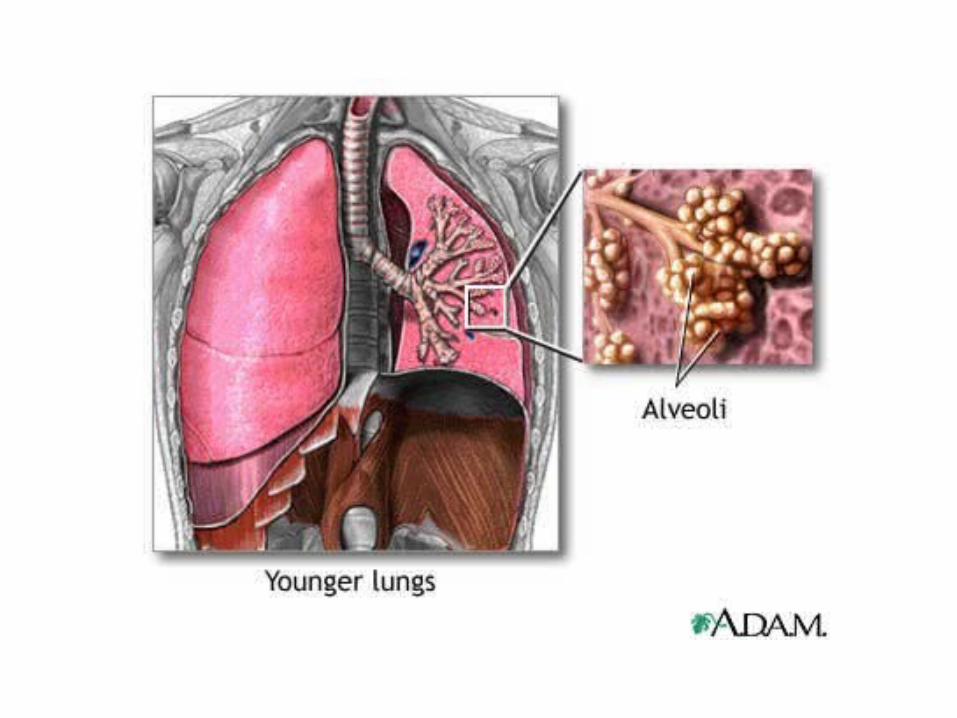
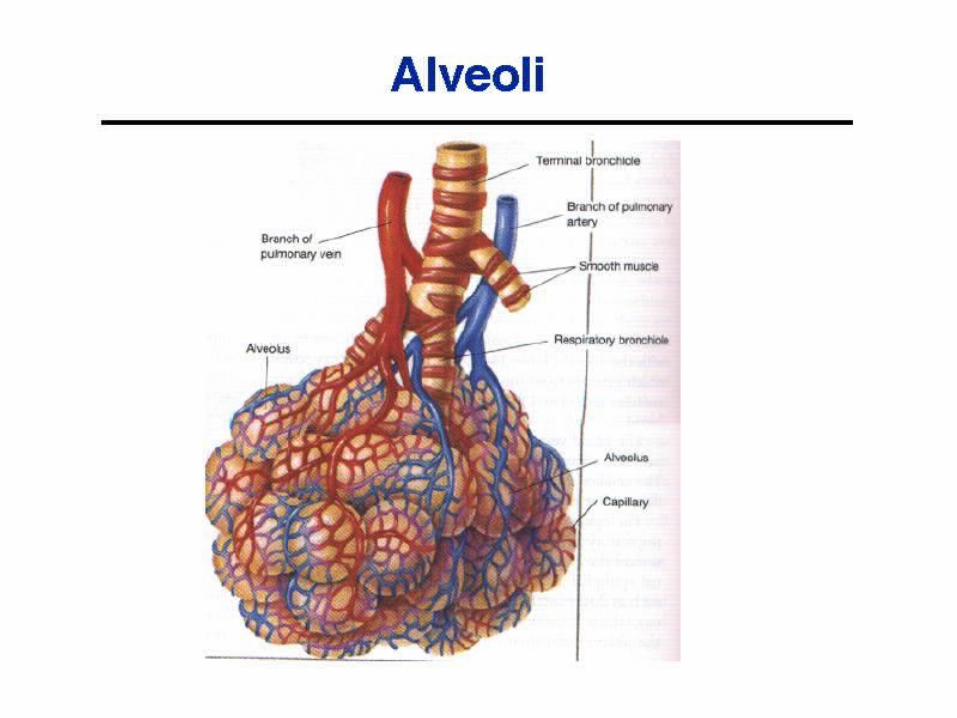
• Alveoli
– Tiny, thin-walled sacs at ends of terminal bronchi
– About 300 million alveoli in two lungs
• Mechanical barriers protect
– Mucus – holds inhaled particles within tracheobronchi
• Secretes biochemicals toxic to microorganisms
– Cilia – move mucus (w/ trapped particles)
– Resident macrophages – phagocytize invaders
– If vent’n decr’d decr’d ability to clear tract
– Two means of support
• Connective tissue fibers (collagen & elastin)
– Allows stretch of tracheobronchi to fill, then return
• Surfactant - lipoprotein
– Detergent-like substance prod’d and held in alveoli
– Nec to decr surface tension of alveolar walls
less gas pressure needed to open alveoli during inspiration
Pulmonary Circulation• Nec to gas exchange
• Blood vessels in lung have thinner walls (Fig.25-5,6)
– Also, alveoli thin-walled
• M any thin-walled capillaries immediately adjacent to alveoli
– Alveoli + blood vessels sep’d by <0.5 microns
– Alveoli highly perfused -- large network of cap’s
– Alveoli/capillary membranes may fuse little, no separation between blood in cap’s and air in alveoli
much surface for gas exchange between blood and air in lungs
– Very thin layer of blood lies on large space of alveolus
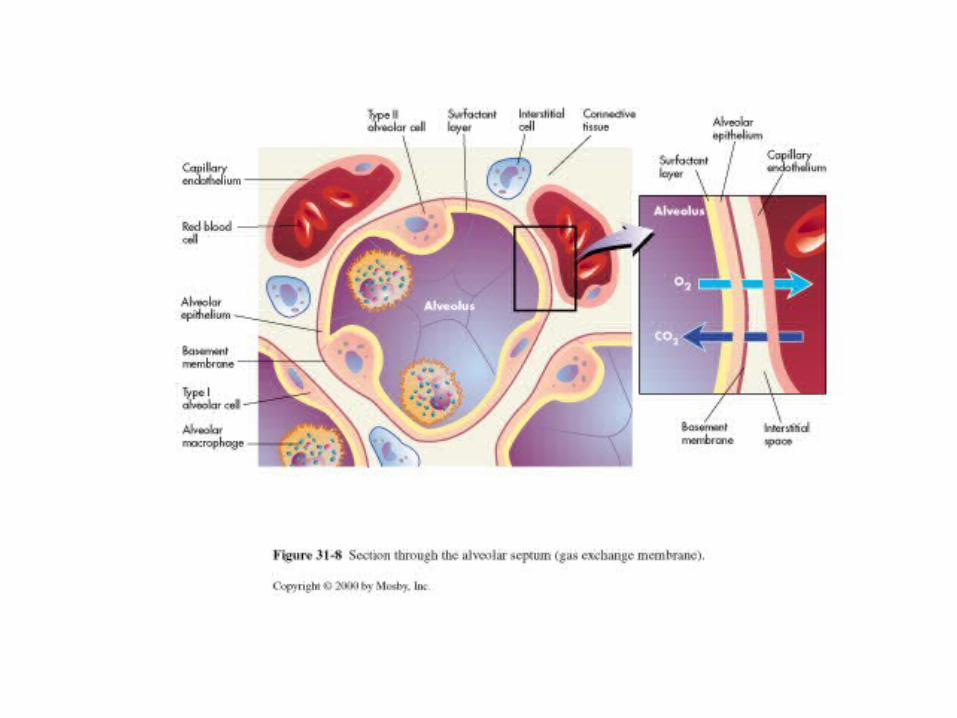
• Gas exchange by simple diffusion
– Through cells of alveoli and capillaries or through junctions between cells
– NOTE: oxygen available at lung must closely match oxygen supply nec to tissues. THIS IS IMPORTANT
Breathing = ventilation
• Mechanical movement gas/air into/out of lung
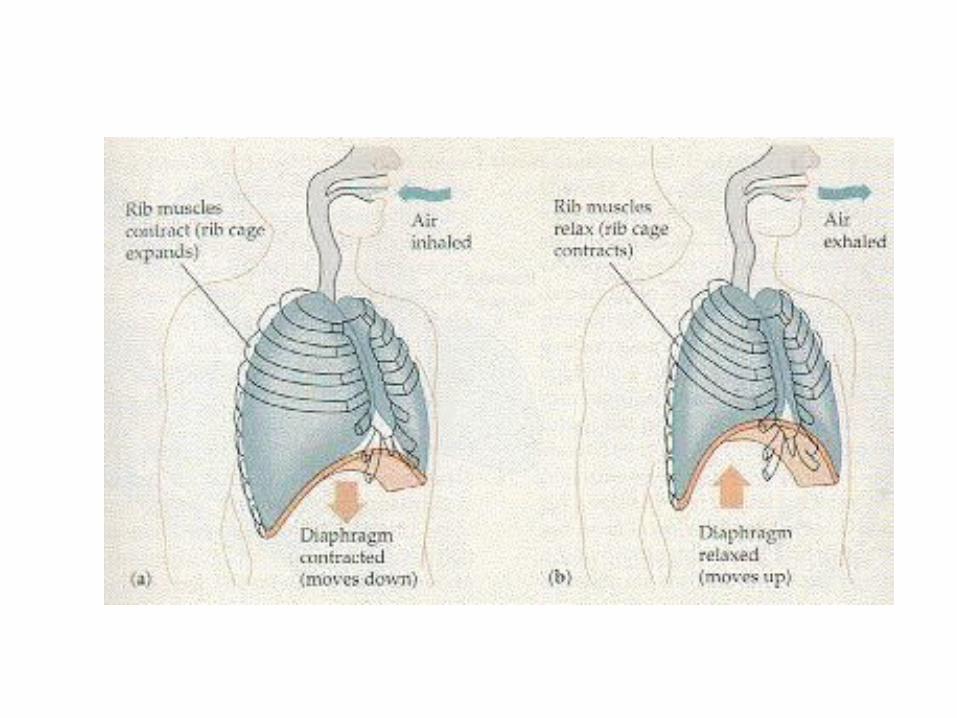
– Use: chest muscles (Fig.25-7,25-12)
– diaphragm
– Also, elastic properties of chest wall and lungs impt
• Major accessory muscles used for involuntary mechanisms
• Contraction of diaphragm diaphragm moves down (Fig.25-13) Incr’d vol thoracic cavity
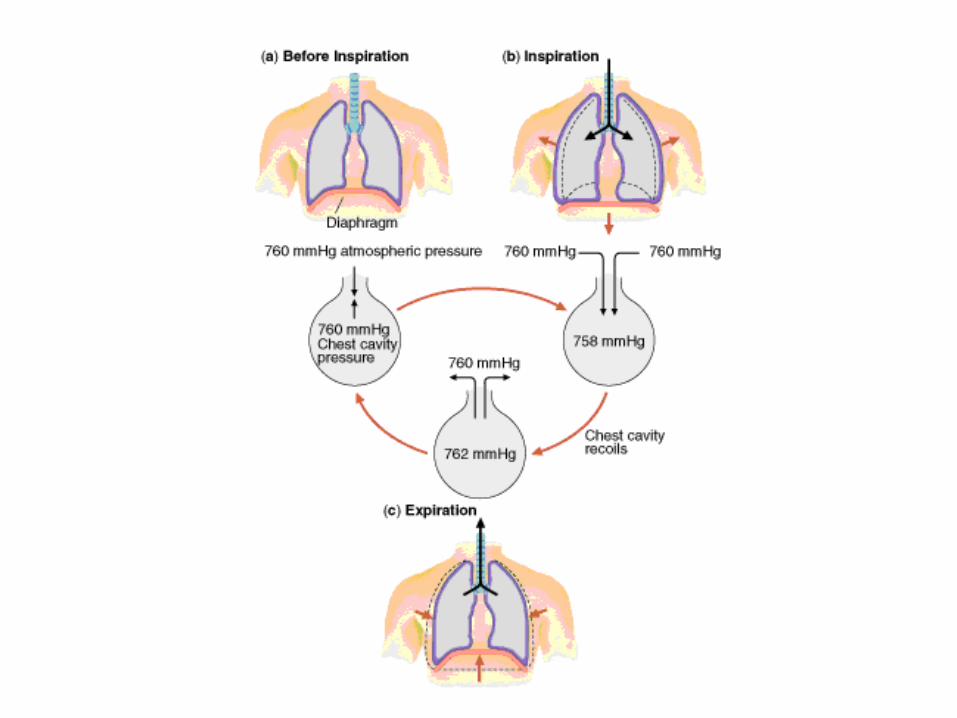
Decr’d pressure gas in lung
• Note: If fixed amount of gas in a space, gas exerts pressure on container walls. If container vol incr’s, that same amount of gas will exert less pressure on walls. As thoracic cavity incr’s, lungs expand and see decr’d gas pressure inside lung
– Air moves from area of higher pressure (atmosphere) to area of lower pressure (lung) (Fig.25-16)
• Contraction intercostal muscles ribs move outward
Further increase in thoracic cavity volume
Further decrease in gas pressure in lung
Movement of air from area of higher pressure (atmosphere) to area of lower pressure (lung) (Fig.25-16)
• Elastic properties of lung/chest wall
– Permit expansion followed by return (Fig.25-13)
– Recoil
• Chest wall recoils outward, lungs recoil inward (opposing)
change in thoracic pressures air taken into lung with inspiration
– Compliance = measure of lung, chest wall distensibility
• If incr'd – lungs abnormally easy to inflate
– Lose elastic recoil
– Ex: emphysema
• If decr'd – lungs abnormally stiff, difficult to inflate
– Ex: fibrosis, pneumonia, pulmonary edema
• Control of breathing both voluntary and involuntary
– CNS (Fig.25-11)
• Through respiratory center at base of brain
– Peripheral nervous system (PNS)
• Receptors in lung sensitive to stretch, irritation
– Signals respiratory center, which responds by altering breathing
• Chemoreceptors in bloodstream sensitive to pH, PaCO2 and PaO2
– PaCO2 = arterial pressure of CO2
– What do you think happens to breathing when the chemoreceptors signal a decrease in O2? What if there is an increase in acid in the blood?
Gas Exchange• Oxygen from gas to blood (Fig.25-16)
– PO2 in alveolar gas >>> PO2 in blood
• Large pressure gradient between O2 in lung and in blood
• Promotes movement of O2
• Gas moves by diffusion through alveolar and capillary membr’s (Fig.25-6)
– Oxygen transport
• O2 dissolves in plasma, binds Hb increased PaO2
– Hb has 4 binding sites, binds 4 oxygen (O2) molecules
• Total blood O2 = O2 dissolved in the plasma + O2 bound to Hb
– About 5% of O2 is gas dissolved in blood; most travels through blood bound
to Hb
– Diffusion of O2 from air to blood stops when pressure of O2 in alveoli = pressure of O2 in arterial blood
– Hb-O2 associated at lung dissociates at tissues to Hb + O2
• At tissues, pressure concentration: O2 pressure in blood >>> O2 pressure in tissues (Fig.25-16)
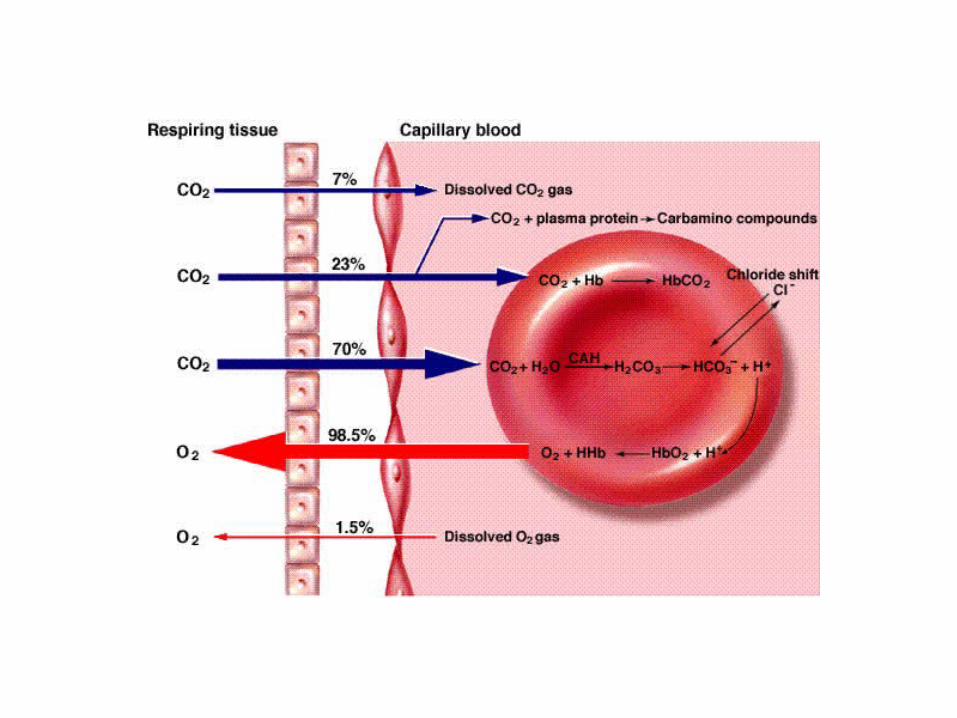
• CO2 transport (Fig.25-16)
– CO2 -- byproduct of metabolism
• Tissue CO2 pressure >>> venous blood CO2 pressure
• Must be eliminated or respiratory acidosis
– CO2 from tissues dissolves in plasma
• Diffuses into rbc’s
• Carbonic anhydrase catalyzes reaction:
CO2 + H2O H2CO3 H+ + HCO3-
• Bicarbonate carried in rbc and dissolved in blood
– CO2 soluble in alveolo-capillary membrane
• Diffuses quickly from blood to alveolus (concentration gradient), then expired into atmospheric air
• Approx. even distribution nec between gas in lungs/blood perfusing the lung
– Rate of gas moving into lung = ventilation (V)
– Rate of blood perfusing lung = perfusion (Q)
• Best if V matches Q
– V/Q = relationship between ventilation, perfusion
• Normal V/Q = 0.8
– In healthy lung, ventilation slightly < perfusion
• If different (with disease, impairment in breathing)
V/Q mismatch
Signs and Symptoms• Cough – protective reflex
– “Explosive expiration”
– Clears lower airways
– From stimulation of irritant receptors
– If persistent, indicates disease
• Nonproductive (no mucus, etc.) indicates:
– Bronchitis
– Viral pneumonia
– Tumor
• Productive - produces sputum
– If purulent: infection
• Dyspnea - uncomfortable breathing
– Due to incr'd work of breathing with:
• Diseases of lung tissue
• Disturbances of:
– Ventilation
– Gas exchange
– Mismatch of V/Q
• Chemoreceptor stimulation or other reasons
• Decreased pH or PaO2, or increased PaCO2
• Cyanosis – blue discoloration of skin due to Hb not associated w/ oxygen
– So blood not red color (need O2 bound for Hb to be red)
• Can result from decreased PaO2 or decreased cardiac output
• Does not necessarily indicate respiratory disease
• Pain
– Originating in pleura usually due to infection
– Originating in central chest (pronounced after coughing)
• May be due to inflammation of bronchi, trachea
– Originating in chest wall
• May be due to rib or muscle injury
• Possible with excessive coughing