Embed Size (px)
Citation preview

Respond Deliver & Enable
Blood Transfusion Update for General Practice
Hospital Transfusion Team
RD&E

Respond Deliver & Enable
Welcome to Transfusion Training!
• The aim of this training is to support you as General Practitioners in making appropriate, safe decisions when you request and prescribe blood
• There is a national mandatory requirement for all involved in the process of blood transfusion to have regular 3 yearly training, which this training will fulfil

Respond Deliver & Enable
Update from the Hospital Transfusion Team..
• The RD&E transfusion laboratory is now cross matching a maximum of 2 units for transfusion for one patient in 24 hrs
• This is in response to recent audit and National Guidance
• Some patients, particularly transfusion dependent haematology patients, may have a higher transfusion requirement, please discuss with the patient’s consultants if you feel you need more than 2 units
• All transfusion requests will be reviewed by a member of the Hospital Transfusion Team
Respond Deliver & Enable
SECTION 1
• When is transfusion appropriate? • How many units should I prescribe?

Respond Deliver & Enable
Indication for transfusion
• Haemoglobin trigger levels for transfusion are well established
• They are one of the reasons that there has been a national 20% reduction in the use of RBC transfusions in the last 15 yrs.
• There is increasing evidence in patients who are not acutely bleeding that a restrictive transfusion policy reduces patient mortality and morbidity

Respond Deliver & Enable
Is transfusion appropriate?
• A 78yr old patient with a chronic normochromic normocytic anaemia has a haemoglobin of 85g/l.
• What do the national guidelines say?• Should you transfuse?
Respond Deliver & Enable
Transfusion in Patients who are not acutely bleeding
National Guidance ( NBTC 2013)
• In chronic anaemia aim to maintain haemoglobin levels so as to prevent symptoms of anaemia
• Transfusing when haemoglobin levels fall below 80g/l is appropriate for many patients

Respond Deliver & Enable
Some patients will do better with higher oxygen delivery…..
• Haematology or Renal patients often have a higher transfusion requirement, be guided by symptoms and consultants
• Patients who have cardiovascular disease have higher oxygen requirements to remain symptom free, aim to keep haemoglobin levels above 80g/l
• For chemotherapy patients maintain Hb above 80-90g/l• For radiotherapy patients maintain Hb above 100g/l
As ever be guided by your patient’s symptoms rather than their numbers

Respond Deliver & Enable
So in this patient…..
• The haemoglobin is not at the trigger level for transfusion but clearly the decision must be made on individual symptoms
• If his symptoms do warrant transfusion, one unit is all he is likely to need.
Respond Deliver & Enable
Is transfusion appropriate?
• 78 yr old man with a microcytic anaemia of 72 g/l, who is slightly breathless on exertion
• The anaemia is being fully investigated• He is intolerant of oral iron• Should you arrange a transfusion?
Respond Deliver & Enable
Iron Deficiency Anaemia (IDA)• In IDA, patients need iron rather
than blood unless there are symptoms of end organ failure
• IV iron now much safer to give and readily available within the RD & E (AMU will arrange)
• 1 gram of iron can be infused over 60 minutes, this is the amount of iron contained in 4 units of blood

Respond Deliver & Enable
So in this patient…..
• Arrange for patient to have an intravenous iron infusion
• If you feel patient’s symptoms mean that you need to increase his haemoglobin more quickly than the 7-14 days it will take with intravenous iron, then a 1 unit transfusion followed by iv iron may be appropriate

Respond Deliver & Enable
How many units to prescribe?
• An 84 yr old lady with a longstanding anaemia of chronic disease has a haemoglobin of 70g/l and is feeling breathless and a bit dizzy on standing.
• She weighs 50 kg• How many units should you prescribe?

Respond Deliver & Enable
Why give 2 when 1 will do?
• The rule that 1 unit of blood increases Hb by 10 g/l only holds for someone of 70 kg
• In a ‘little elderly lady’ weighing 50kgs, the Hb may rise by 15 to 20 g/l after 1 unit
• It is very rare to need to transfuse anyone to over 100 g/l
Respond Deliver & Enable
So in this case…..
• She has a haemoglobin of 70g/l and given her size every unit will increase her haemoglobin by at least 15g/l
• You could bring her in for 1 unit and check her haemoglobin and then bring her in again for another unit if needed, but in the community this may be difficult and you may want to give her 2 units to bring her Hb up to 100g/l
• If you prescribed 3 units, you would over transfuse her and unnecessarily put her at risk of cardiac overload and other transfusion reactions

Respond Deliver & Enable
SECTION 2
The practicalities of arranging a blood transfusion
Respond Deliver & Enable
Patient Consent to Blood Transfusion
• Where possible patients should have the risks, benefits and alternatives to transfusion explained to them
• Record reason for transfusion consent in notes
• Provide written information, leaflets available within all community hospitals
Respond Deliver & Enable
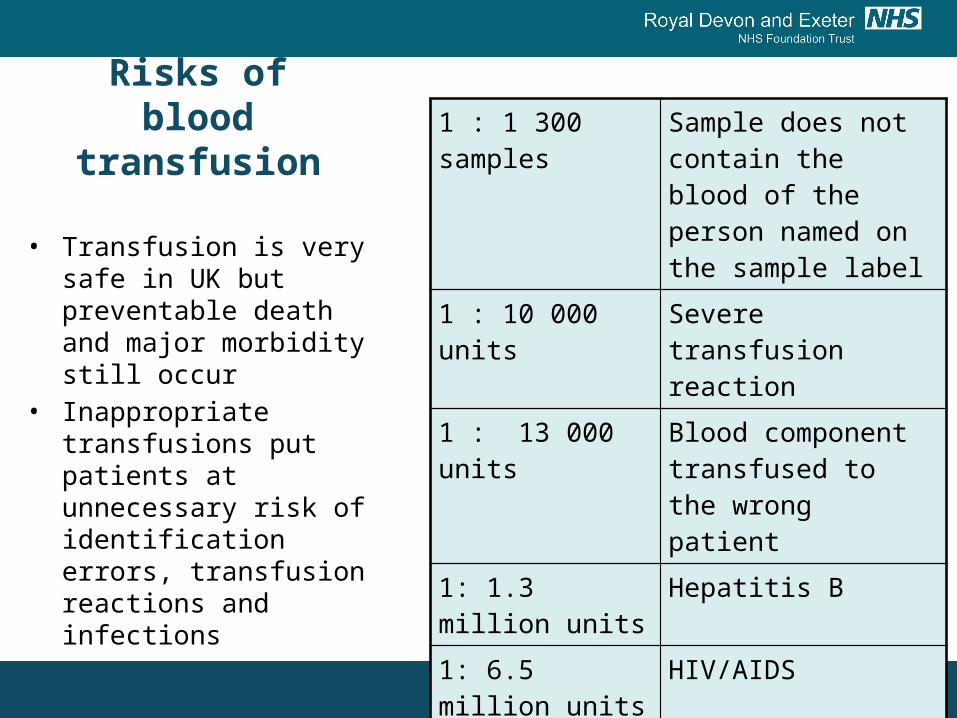
Risks of blood transfusion
1 : 1 300 samples Sample does not contain the blood of the person named on the sample label
1 : 10 000 units Severe transfusion reaction
1 : 13 000 units Blood component transfused to the wrong patient
1: 1.3 million units Hepatitis B
1: 6.5 million units HIV/AIDS
1: 28 million Hepatitis C
unknown CJD
• Transfusion is very safe in UK but preventable death and major morbidity still occur
• Inappropriate transfusions put patients at unnecessary risk of identification errors, transfusion reactions and infections

Respond Deliver & Enable
Taking the blood……• Ask the patient for their
name and date of birth, let them tell you.
• If they are inpatients always check the ID band
• Always write details on the tube straight away and AT the bedside
• Only take blood and label samples for one patient at a time

Respond Deliver & Enable
Patient Identification Errors• We detect an average of 6 Wrong Blood in
Tube (WBIT) incidents per year• WBIT means that the blood in the sample
bottle is not the blood of the patient whose details are written on the label
• There are 2 main causes for this:– Failure to identify the patient correctly– Failure to label the sample at the bedside

Respond Deliver & Enable
The Request Form…..
This is your way of communicating with our lab staff
PLEASE: • Tell us the name of the GP making the request so if
there are any difficulties we can contact you• Tell us why you are transfusing the patient ( not just
low hb..) and their pre transfusion haemoglobin level • Tell us where the blood needs to be sent to and what
day/time it is needed, we will be able to alert you earlier if there are any difficulties
Respond Deliver & Enable
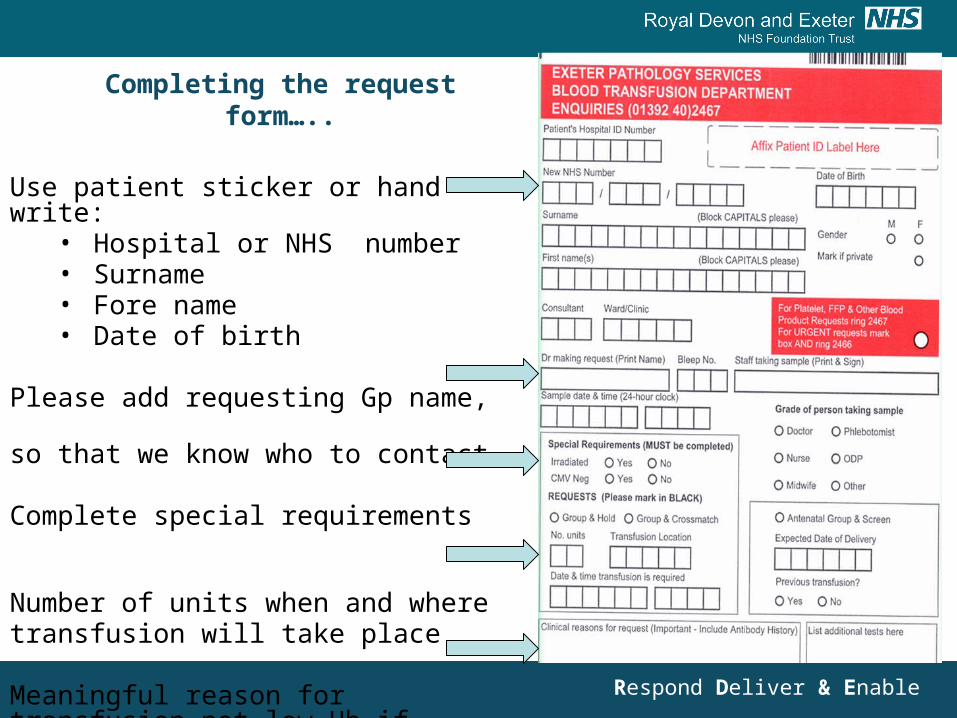
Completing the request form…..
Use patient sticker or hand write: • Hospital or NHS number• Surname• Fore name• Date of birth
Please add requesting Gp name, so that we know who to contact
Complete special requirements
Number of units when and wheretransfusion will take place
Meaningful reason for transfusion not low Hb if possible…
Respond Deliver & Enable
Special Requirements: Irradiated Blood
• Irradiating donated blood removes any remaining leucocytes, this eliminates the risk of Transfusion Associated Graft vs Host disease
• This is a rare but frequently fatal complication of blood transfusion
• Some patients because of present or prior treatment or illness are at increased risk of TaGvH disease and require irradiated blood
Respond Deliver & Enable
• In the community, consider if patient has history of :
– Chemotherapy with purine analogues eg fludarabine– Hodgkin's disease either in the past or present– Bone marrow transplant– Has been treated with anti-CD52 antibodies or anti-thymocyte
globulin
• This list is now available on the back of transfusion forms
• There is a system for identifying these patients at diagnosis and a warning system on the laboratory computer, ask the lab if you are not sure
Who needs Irradiated blood?

Respond Deliver & Enable
What about theCytomegalovirus box??
• CMV screened red cells & platelets are only needed for – neonates and intra uterine blood transfusions– Planned transfusions during pregnancy– Some granulocyte transfusions
• In the community you are pretty safe to tick the no box!
Respond Deliver & Enable
Taking the sample.. How many do you need to take?
• The RD&E needs confirmation of a patient’s ABO group from 2 separate samples to reduce the risk from mislabelled samples
• Over 90% of patients already have a group recorded on our computer system and just need 1 new sample for cross match
• If you are unsure of how many samples to take please ring the Transfusion Laboratory
• If taking 2 samples they should be taken from 2 venepunctures with 2 SEPARATE attempts at patient identity, please use 2 forms with time difference on samples

Respond Deliver & Enable
Taking the sample.. How far in advance of the transfusion can it
be taken? • The standard sample validity time is
72 hours between sampling and transfusion
• If no pregnancy or transfusion within previous 3 months then the sample validity time extends to 7 days
• In transfusion dependent haematology patients it may be possible to waive the 72 hr rule after discussion with their consultant
Respond Deliver & Enable
Time to blood transfusion from taking blood sample…….
• Day 1: Blood sample taken in Community arrives in lab on transport at 3pm when the blood sample will be cross matched but not in time for the routine transport out which leaves at 4 pm each day
• Day 2:Blood transported to Community Hospital, leaving RD&E at 4 pm
• Day 3:Blood Transfusion

Respond Deliver & Enable
Section 3
Safe Administration of blood:
Blood Transfusion Reactions
Respond Deliver & Enable
A patient is 10 minutes into the start of a blood transfusion
• She complains of feeling itchy, develops an urticarial rash and feels light headed
• The nurses contact you for advice• What is this likely to be and what should your
first action be?
Respond Deliver & Enable
This is likely to be an acute transfusion reaction
• Key action is to STOP the transfusion
• Follow the Transfusion Reaction Chart which is available on the ward
• The on call haematologist may need to be involved

Respond Deliver & Enable
Acute Transfusion Reactions
Within 24 hrs of transfusion1. Febrile reactions, often mild
2. Allergic reactions ranging from urticaria to anaphylaxis
3. Acute Haemolytic Reactions eg ABO incompatibility
4. Bacterial contamination range from mild pyrexia to septic shock
5. Transfusion - associated circulatory overload (TACO)
6. Transfusion – related lung injury (TRALI)

Respond Deliver & Enable
A frail 85 year old man is having his 3rd unit of blood and starts to
feel breathless
• What should you do?• What is the likely diagnosis?• How can you try and prevent this happening
again?
Respond Deliver & Enable
This is likely to be Transfusion Associated Circulatory Overload
(TACO)
• This is defined as acute or worsening pulmonary oedema within 6 hours of a blood transfusion
• It is now the leading cause of mortality related to blood transfusion in the UK ; 9 deaths and 32 patients admitted to HDU last year

Respond Deliver & Enable
What should you do?
• Stop the transfusion• Assess patient as per Blood Transfusion
Reaction protocol• If you think this is TACO, treat as Left
Ventricular failure, the patient will need a CXR and admission to RD&E or NDDH
• Contact the Consultant Haematologist on call
Respond Deliver & Enable
Who is at risk of TACO? • Patients over 70 yrs old of low weight with cardiac or
renal failure or a low albumin are higher risk of TACO• In these patients:
– Clearly record reason for transfusion, is this transfusion really necessary?
– Assess patient before transfusion and if at risk transfuse slowly, consider diuretic cover
– Ask nursing staff to observe for signs of fluid overload
– Single unit transfusions are advised
Respond Deliver & Enable
Delayed Transfusion Reaction
• A patient who had a transfusion 8 days ago presents to you feeling generally unwell, with dark urine and loin pains
• Apart from a UTI, what else would you consider?
Respond Deliver & Enable
This could be a delayed transfusion reaction..
• These occur up to 14 days post transfusion • They present with features of haemolysis, with a less
than expected rise in haemoglobin levels post transfusion, jaundice, fever, haemoglobinuria, acute renal failure
• Initial blood tests should include a repeat Group and Save, also requesting a DAT (Direct Antiglobulin Test) on the same form, FBC and LFTs.
• Easy to miss, treatment is supportive, refer for investigation to clarify nature of antibody for future transfusions

Respond Deliver & Enable
5 Key Points…..
1. Transfuse appropriately using haemoglobin trigger levels
2. Try not to over transfuse, remember size does matter
3. Use oral or iv iron in patients with iron deficiency rather than blood transfusion
4. Identify patients correctly; ‘Right Blood Right Patient every time’
5. Transfusion related Circulatory Overload (TACO) is highest cause of mortality from transfusion

Respond Deliver & Enable
Thank You!!
Hospital Transfusion Team
RD&E