Embed Size (px)
Citation preview

Responding tothe Challenge of
Diabetes in CanadaFirst Report of the National Diabetes
Surveillance System (NDSS) 2003

Our mission is to help the people of Canadamaintain and improve their health
Health Canada
For additional copies, please contact:
PublicationsHealth CanadaOttawa, OntarioK1A 0K9
Tel: (613) 954-5995Fax: (613) 941-5366
Available at www.NDSS.ca
This publication can be made available in/on computer diskette/large print/audio cassette/braille, upon request.
The opinions expressed in this publication are those of the authors anddo not necessarily reflect the views of Health Canada
Ce document est aussi publié en français sous le titre :Relever le défi posé par le diabète au CanadaPremier rapport du Système national de surveillance du diabète (SNSD), 2003
© Her Majesty the Queen in Right of Canada, represented by the Minister of Health (2003)Cat. N° H39-4/21-2003EISBN 0-662-35419-25602

Responding to the
Challenge of
Diabetes in Canada
First Report of the
National Diabetes Surveillance System (NDSS)
2003


Acknowledgements
Many organizations participate in the NationalDiabetes Surveillance System (NDSS) ascollaborators or partners: provincial/territorialgovernments, non-government organizations,aboriginal groups, academics/clinicians, thefederal government and the pioneering sponsor,
GlaxoSmithKline Inc. The full list of participantsas well as persons currently involved in NDSScommittees are listed in this report or itsappendices. We thank all current and pastmembers of NDSS for their contributions.
Acknowledgements
i

Executive Summary
Diabetes is a serious and growing public healthproblem in Canada, particularly in Aboriginalpopulations. The morbidity and mortalityassociated with diabetes are increasedconsiderably by complications such as heartdisease and stroke, blindness, kidney disease,nerve disease and amputations.
To date, there has been a lack of ongoing,systematic, validated Canadian analysis for basicprevalence and other diabetes information. TheNational Diabetes Surveillance System (NDSS) isthe mechanism developed to provide improveddata about diabetes. It is a network of regionallydistributed diabetes surveillance systems thatcompile administrative health care data relatingto diabetes, and send aggregate anonymous datato Health Canada for national analyses.
This is the first report comprehensively describingNDSS. It covers:
� the original concept of using health careadministrative databases to track diseaseburden in a population;
� studies that have demonstrated thefeasibility and validity of the concept;
� activities directed towards assessing andimproving provincial/territorial capacity toparticipate in NDSS;
� strengths and limitations of the NDSSapproach;
� structure and governance;
� a special focus on Aboriginal populations;
�methods of data capture;
� prevalence and mortality data; and
� future plans, including validation of adiagnostic algorithm for diabetes in peopleunder 20 years of age.
Highlights of NDSS data include the following:
� prevalence of diabetes among adult Canadiansin 1999/2000 was 5.1%;
� 1,196,370 adult Canadians were living withdiagnosed diabetes in 1999/2000;
� Canadian adults with diabetes are twice aslikely to die prematurely compared withadults without diabetes; and
� 41,483 adult Canadians with diabetes diedin 1999/2000.
NDSS represents the first time that acoordinated, national use of administrative datafor public health surveillance purposes has beenundertaken. NDSS can measure prevalence,incidence and outcomes over time for both thenation as a whole and for specific regions. Alsofor the first time, NDSS can compare healthservices use and other health outcomes of peoplewith and without diabetes. With these features,NDSS is also a prototype of enhanced capacityand infrastructure to support surveillance forother diseases that can be tracked through thehealth care system.
Executive Summary
ii

Canada was in a unique position to develop thistype of surveillance system, given its publiclyfunded health insurance generating person-specific administrative data. NDSS use of multipledatabases offers information on diabetes that is farsuperior to what would be possible using onesource alone. The resultant rich source of data can
be used not only for surveillance but also forexamining many policy and research questions.
Perhaps most importantly, NDSS was the catalystfor exciting partnerships with various jurisdictionsacross Canada cooperating to achieve the sharedgoal of reducing the burden of diabetes.
Executive Summary
iii

Table of Contents
Acknowledgements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . i
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ii
List of Figures and Tables . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Acronyms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . viii
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
The Challenge of Diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Diabetes as a Personal Challenge. . . . . . . . . . . . . . . . . . . . . . . . . . 3Diabetes as a National Challenge . . . . . . . . . . . . . . . . . . . . . . . . . . 3Diabetes as a Particular Challenge for Aboriginal People in Canada . . . . . . . . . . 4
National Diabetes Surveillance System (NDSS) – A Response to the Challenge . . . 5
The Original Concept . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Feasibility. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6The NDSS Model (goals, principles, attributes) . . . . . . . . . . . . . . . . . . . 7Capacity-Building . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Strengths and Limitations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Structure and Governance . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Steering Committee . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Working Groups . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Partnerships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Responsibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Table of Contents
iv

Focus on Aboriginal Populations . . . . . . . . . . . . . . . . . . . . . . . . 15
Identifying Aboriginal Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Basic Principles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Partnerships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Methods of Data Capture . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Physicians Claims File . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Hospital File . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Health Insurance Registry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Data Processing at the Provincial/Territorial Level . . . . . . . . . . . . . . . . . . 19Data Processing at the National Level. . . . . . . . . . . . . . . . . . . . . . . . 21Definitions and Calculations . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Data Validation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Facts and Figures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Accomplishments, Plans and Possibilities . . . . . . . . . . . . . . . . . . . . 32
What NDSS Tells Us . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32What NDSS Does Not Tell Us . . . . . . . . . . . . . . . . . . . . . . . . . . . 32What NDSS Will Tell Us in the Near Future . . . . . . . . . . . . . . . . . . . . . 34What NDSS May Tell Us in the Long Term . . . . . . . . . . . . . . . . . . . . . 35
Finding Answers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Table of Contents
v

Appendices
Appendix A: NDSS Capacity Assessment Form . . . . . . . . . . . . . . . . . . 43
Appendix B: Regional Activity . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Appendix C: NDSS Steering Committee Membership 2003 . . . . . . . . . . . . 56
Appendix D: NDSS Working Group Membership 2003. . . . . . . . . . . . . . . 57
Appendix E: Memorandum of Understanding (MOU) . . . . . . . . . . . . . . . 60
Appendix F: NDSS Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Appendix G: Comparison of NDSS and Statistics Canada Counts of Deathand Population . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
Appendix H: Annual Person-Level Summary File (APLSF) Data Elements . . . . . . 76
Appendix I: Canadian Standard Population Estimates - July 1, 1991 . . . . . . . 77
Appendix J: Validation Work . . . . . . . . . . . . . . . . . . . . . . . . . . 78
Appendix K: Age-Specific Prevalence by Fiscal Year, Sex and Province/Territory . . . 82
Appendix L: Age-Specific Mortality by Fiscal Year, Sex and Province/Territory . . . . 94
Table of Contents
vi

List of Figures and Tables
Figures
Figure 1: NDSS Governance Structure . . . . . . . . . . . . . . . . . . . . . . 10
Figure 2: Comparison of NDSS with Statistics Canada Deaths, April 1995 toMarch 1999, by Province/Territory . . . . . . . . . . . . . . . . . . . 18
Figure 3: Comparison of NDSS with Statistics Canada Population Counts,July 1997/98/99/2000, by Province/Territory. . . . . . . . . . . . . . 19
Figure 4: Data and Process Flow Diagram . . . . . . . . . . . . . . . . . . . . 20
Figure 5: Prevalence of Diabetes in Canadians by Fiscal Year and Sex . . . . . . . 25
Figure 6: Prevalence of Diabetes in Canada, 1999/2000, by Age and Sex . . . . . 26
Figure 7: Prevalence of Diabetes in Canada by Province/Territory, 1999/2000 . . . 28
Figure 8: Canadian Mortality Rates by Fiscal Year, Sex and Diabetes Status . . . . 29
Figure 9: Canadian mortality Rates by Age and Diabetes Status, 1999/2000. . . . 30
Figure 10: Comparison of Mortality for Canadians With and Without Diabetes,1999/2000, by Province/Territory . . . . . . . . . . . . . . . . . . . 30
Tables
Table 1: Steering Committee Membership . . . . . . . . . . . . . . . . . . . . 11
Table 2: Working Groups and Areas of Responsibility . . . . . . . . . . . . . . 12
Table 3: Percentage (%) of Physicians Paid Only on a Fee-For-Service Basis. . . . 17
Table 4: Contents of the Canadian Aggregate Datafile . . . . . . . . . . . . . . 22
Table 5: Prevalence of Diabetes in Canada by Fiscal Year, Province/Territory and Sex . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Table 6: Canadian Mortality Rates by Diabetes Status, Fiscal Year,Province/Territory, and Sex . . . . . . . . . . . . . . . . . . . . . . 31
Table 7: NDSS Accomplishments. . . . . . . . . . . . . . . . . . . . . . . . 33
Table 8: The Scope for Enhanced Diabetes Surveillance . . . . . . . . . . . . . 36
List of figures and Tables
vii

Acronyms
APLSF Annual Person Level Summary File
BMI Body Mass Index
CABG Coronary Artery Bypass Grafting
CCHS Canadian Community HealthSurvey (Statistics Canada)
CDA Canadian Diabetes Association
CDS Canadian Diabetes Strategy
CIHI Canadian Institute for HealthInformation
CIHR Canadian Institutes for HealthResearch
DCC Diabetes Council of Canada
DM Diabetes Mellitus
EHR Electronic Health Record
F/P/T Federal/provincial/territorial(governments)
FNIHB First Nations and Inuit HealthBranch
FTE Full-time Equivalents
FY Fiscal Year
HISP Health Infostructure SupportProgram
ICD-9 International Statistical Classificationof Diseases and Related HealthProblems (v. 9)
ICES Institute for Clinical EvaluativeSciences
IDDM Insulin Dependent Diabetes Mellitus
INMD Institute of Nutrition, Metabolismand Diabetes
MOU Memorandum of Understanding
NDSS National Diabetes SurveillanceSystem
NIDDM Non-Insulin Dependent DiabetesMellitus
NWT Northwest Territories
O&M Operating and MaintenanceFinancial Mechanism (HealthCanada)
P/T Provincial/territorial governments
PIRC Performance Indicator ReportCommittee
PPHB Population and Public HealthBranch
PTCA Percutaneous TransluminalCoronary Angioplasty
RCMP Royal Canadian Mounted Police
RFA Request for Applications
RIW Resource Intensity Weight
SAS® Statistical Analysis Software
Acronyms
viii

Introduction
Diabetes is a serious, chronic, systemic diseasecharacterized by the body’s inability tosufficiently produce and/or use insulin – ahormone produced by the pancreas that assistswith the conversion of glucose (sugar) intoenergy. Without insulin, blood sugar levels rise todangerous levels, interfering with the propernourishment of body cells.
The burden of illness associated with diabetes isincreased by the fact that people with diabetesare at greater risk of other diseases than peoplewithout diabetes. This risk is strongly related tohigh blood sugar and the duration of diabetes.Chronic high levels of blood glucose can lead toheart disease and stroke, retinopathy (the leadingcause of adult blindness in Canada), kidneydisease, amputations, nerve disease (includingerectile dysfunction) and other complications.
The Government of Canada recognizes thatdiabetes is a complex health problem and anational challenge. In 1999 it pledged $115million over five years to the development of aCanadian Diabetes Strategy (CDS) to enableCanadians to benefit more fully from theconsiderable resources and expertise availableacross the country.
The CDS allows the Government of Canada tomove forward in three areas of vital importance:
� The development of a health promotion-disease prevention strategy for the entirepopulation.
� The provision of care, treatment andprevention for First Nations people onreserve and for those in Inuit communities.
� The improvement of national and regionaldata about diabetes and its complications.
Introduction
1
Diabetes has been diagnosed in over onemillion Canadians. Projections based on ouraging population indicate that the burdenof diabetes and its complications willincrease considerably.

The present report describes progress madetowards meeting the need for information thatwill assist Canada to respond in an organized andintegrated way to the challenge of diabetes. Inparticular, this report describes the NationalDiabetes Surveillance System (NDSS) – anetwork of regionally distributed diabetessurveillance systems. The network wasdeveloped, implemented and coordinatedthrough collaboration among governments,industry and several non-government agenciesand Aboriginal groups committed to reducing theburden of diabetes in Canada.
This report is the first in a series designed todescribe NDSS. As such, it delves into thebackground and history of the project more thanwill future reports. It also presents data that serveto indicate the types of information that arecurrently available or will be forthcoming fromNDSS.
Introduction
2
In 1999, the first Diabetes in Canadareport highlighted the need for betterdata, in particular, data on the prevalenceand incidence of diabetes, itscomplications, the use of health services,and the effectiveness of prevention andcontrol initiatives. NDSS represents amajor milestone in achieving this.

The Challenge of Diabetes
Diabetes as a Personal Challenge
Diabetes affects people of all ages. Type 1diabetes (formerly referred to as insulin-dependent diabetes mellitus or IDDM) usuallybegins during the first two decades of life.
In type 1 diabetes, the immune system destroysthe insulin-producing cells of the pancreas.Although the process is poorly understood, acombination of genetic factors and environmentalstressors, such as viruses, is believed to be thetrigger.
Type 1 diabetes requires treatment with insulinthroughout the rest of life and is associated with ahigh incidence of complications. Type 1 diabetesusually results in a reduction in quality of life anda shortened lifespan.
Type 2 diabetes (formerly referred to asnon-insulin-dependent diabetes mellitus orNIDDM) occurs most often in obese individualsover the age of 40. In contrast to people with type1 diabetes, who do not produce enough insulin,some people with type 2 diabetes are “insulinresistant” and are not able to use the availableinsulin to control blood sugar.
Type 2 diabetes may be controlled by weightloss, exercise and medication taken orally.However, for some people with type 2 diabetes,daily insulin injections may be required. Lifeexpectancy is also reduced in people with type 2diabetes.
A third type of diabetes – gestational diabetes –occurs during pregnancy and usually resolvesafter delivery. Gestational diabetes can result inan increased incidence of very large babies andpre-eclampsia (toxemia of pregnancy).
Gestational diabetes is a strong risk factor for type2 diabetes later in life.
Better information about risk factors for diabetes,complication rates, quality and expectation oflife, and the efficacy of prevention and careapproaches could contribute greatly to theoutlook for Canadians with diabetes.
Diabetes as a National Challenge
In 2000 in Canada, diabetes was estimated toaffect about 5% of the population aged 20 yearsand over. The direct treatment costs forpeople with diabetes have been estimated at$400 million annually for hospital care andprescription drugs. In addition, there are costs fortreating complications and for physician care,costs borne by patients, and indirect costs suchas premature death, disability, and care-giving.
Canada has previously estimated the burden ofdiabetes by using mortality data, hospital data,self-report surveys or American data. Theseprovide underestimates for various reasons,including missed diabetes-related hospitalizationsand deaths, variable response rates to surveys,participation and self-report bias, the unreliability
The Challenge of Diabetes
3

of self-report, and relatively small samples insurveys. The appropriateness of extrapolatingestimates from American data is also limited bythe differing age structure and ethnicbackgrounds of the Canadian and Americanpopulations.
Diabetes as a Particular Challenge forAboriginal People in Canada
Aboriginal people, especially First Nations, beganspeaking of a diabetes epidemic in the 1980s.Since then, Canadian research has confirmed thehigh and increasing prevalence of diabetes inthese populations.
Other features of diabetes in First Nations groupsare earlier age at onset of type 2 diabetes, greaterseverity at diagnosis and higher complicationrates.
This burden of disease is associated with uniquechallenges in prevention and care. Information isurgently needed to help tailor prevention,diagnosis and treatment to the circumstances ofAboriginal populations in Canada.
The Challenge of Diabetes
4

The National Diabetes Surveillance System
(NDSS) – A Response to the Challenge
Although diabetes has attracted the attention andefforts of various organizations and levels ofgovernment, it is apparent that the magnitude ofthe problem demands a comprehensive andcollaborative strategy for control. In 1996 anumber of physicians, diabetes educators,non-government organizations, epidemiologistsand researchers concerned about the lack ofongoing systematic information surrounding thismajor public health problem proposed a nationalsurveillance system for diabetes.
Following the 1996 discussions, the DiabetesCouncil of Canada (DCC), a coalition ofdiabetes-related non-governmentalorganizations, Aboriginal groups and federalagencies, championed a national surveillanceeffort as one of its initiatives. The NationalDiabetes Surveillance System (NDSS) SteeringCommittee was formed in 1997 and begandeveloping the concept of a surveillance systemthat would maximize the potential value ofadministrative data to support diabetessurveillance.
The Original Concept
The concept for NDSS was based on initialcontributions from Young et al.1 and Blanchard etal.2,3 It was also a response to the National Forumon Health, which encouraged the use of existingprovincial/territorial administrative databases insupport of public health activities in Canada.4
Underlying the NDSS concept is the assumptionthat the clinical path of diabetes from detection tothe treatment and management of complicationstheoretically makes it possible to track thediabetes burden through various clientinteractions (physician visits, hospitalizations,etc.) within the provincial and territorial healthcare systems.
Tracking is possible because data are capturedroutinely in the provision of publicly funded,insured health services in the variousjurisdictions and are stored in three majorprovincial/territorial administrative databases –physician claims files, hospital files, and healthinsurance registries.
NDSS — A Response to the Challenge
5
Can information systems designedprimarily as tools for budgeting and billingbe used to provide disease-specificinformation that will benefit all Canadians?YES!

Feasibility
In 1999, a pilot project conducted in the threePrairie provinces (Alberta, Saskatchewan, andManitoba) demonstrated the feasibility of theNDSS approach to data collection and thedevelopment of inter-government agreements forsurveillance using provincial administrativedata.5 The project was funded by the Governmentof Alberta and Health Canada’s HealthInfostructure Support Program (HISP), withsignificant in-kind contributions from Manitobaand Saskatchewan.
The project extended an existing diabetessurveillance system operating in Manitoba toSaskatchewan and Alberta and identified amethod for reconciling variations in the threeprovincial health information systems so that thesame core body of software could be used in allthree provinces.
The initial project anticipated the transfer ofperson-level data to a central database heldwithin Health Canada. However, this model wasabandoned after review of provincial legislationregarding the privacy of personal health data. Inits stead, a model was developed for the creationof person-specific databases of healthinformation that would remain within eachparticipating province/territory and an aggregate,anonymous data set that each province andterritory would transmit to Health Canada.
The surveillance system developed through thisproject provided estimates of the incidence andprevalence of diabetes for each year of dataprovided by the provinces/territories. It alsodemonstrated that event rates for approximately40 complications of diabetes as well as healthservices use can be generated for both thepopulation with diabetes and the populationwithout.
The surveillance model can provide ongoing,systematic collection and analysis of publichealth data, suitable for dissemination to thepublic, for health planning and for use by healthprofessionals.
NDSS — A Response to the Challenge
6
Disease Surveillance for Public Health
Public health surveillance has been definedas “the ongoing, systematic collection,analysis, and interpretation of healthdata essential to the planning,implementation, and evaluation of publichealth practice, closely integrated withthe timely dissemination of these data tothose who need to know. . .”6
Disease surveillance collects information inorder to define the magnitude of theproblem, to portray its natural history, toidentify populations at particular risk, tomonitor changes in disease frequency andrisk factors, to evaluate the impact ofdisease control approaches, to generatehypotheses and stimulate research, and toaid planning.
Many of the techniques and methods ofdisease surveillance have been developed inrelation to both infectious and chronicdiseases. Cancer surveillance, inparticular, has spurred the development ofmethods for case ascertain- ment (cancerregistration), projections and recordlinkage.
One of the challenges of diseasesurveillance is to balance the need forinformation against the right to privacy.Methods developed to date havedemonstrated that responsible surveil-lance using personal information ispossible without sacrificing privacy.

The NDSS Model
NDSS represents the first time that coordinatednational use of administrative data for publichealth surveillance purposes has beenundertaken. Thus, NDSS has moved into largelyuncharted waters at both the provincial/ territorialand federal levels.
The balancing of practical considerations andepidemiological methods is at the heart of theNDSS design, which departs from other nationalhealth information systems in several importantways:
� The provinces and territories, Aboriginalgroups and Health Canada are equalpartners, with Health Canada's Centre forChronic Disease Prevention and Controlassuming a central coordinating role.
� Capacity in data capture and analysis isdeveloped within the provinces andterritories.
�NDSS is a network of regionally distributeddiabetes surveillance systems rather than acentral repository.
�Health data related to individuals are heldexclusively within the domain of theprovinces and territories, and no personalhealth data are transferred outside aprovince or territory.
� Aggregate anonymous data are transmittedto a central location.
� Long-term, ongoing data collection enableslongitudinal analyses.
� Provinces, territories and Aboriginal groupshave an important role in organizingadministrative data and in interpreting theresults of analyses.
Although these features compound the difficultyof start-up and implementation, they help buildregional capacity to enable provinces, territoriesand Aboriginal groups to use their own data toanswer questions unique to their needs. This is astrong incentive to buy-in, helping to ensure thelong-term survival of NDSS.
Capacity-Building
The capacity to participate in NDSS wasidentified as a challenge, requiring some of themost resource-intensive activities. A capacityassessment was conducted in each province andterritory to identify capacity inequities.Appendix A contains a description of the domainsassessed. Solutions to inequities includedplacement of officers in jurisdictions, placementof hardware and software, systems development,and upgrading and integration of databases.
NDSS — A Response to the Challenge
7
NDSS Goals
�A national standardized database fordiabetes surveillance, with long-termmonitoring for diabetes-related compli-cations through the integration of newand existing databases
�Ongoing surveillance of diabetes and itscomplications in each province andterritory, and in the Aboriginal community
�Dissemination of national comparativeinformation to assist in effectiveprevention and treatment strategies bypublic health departments, Aboriginalcommunities, non-governmental organi-zations and private industry
�A basis for evaluating economic/cost-related issues regarding the care,management and treatment of diabetesin Canada

These solutions have not yet resulted in uniformcapacity across the country; several jurisdictionsstill require significant amounts of work to moveforward. However, this has not slowed the overallprogress because stakeholders have agreed to thepractice of “providing data as ready rather thanwaiting for the picture to be complete.” By early2003, eight provinces and three territories hadsupplied data to NDSS: Yukon Territory,Northwest Territories and Nunavut, BritishColumbia, Alberta, Saskatchewan, Manitoba,Ontario, Quebec, Nova Scotia and Prince EdwardIsland. The other provinces, New Brunswick andNewfoundland and Labrador, are in the processof building their infrastructure and capacity inorder to participate. Capacity also needs to beaddressed for participation of Aboriginal groups.
At the provincial/territorial level, NDSS has builtcapacity for and interest in both diabetessurveillance in particular and chronic diseasesurveillance in general. Most provinces andterritories have enhanced the surveillancecapacity demonstrated by NDSS. A summary oftheir activities in these areas is contained inAppendix B.
Strengths and Limitations
Administrative databases have been proposed assources of population surveillance of diabetes,1-3
and are held to be accurate, timely and a cost-effective source of surveillance data. Theopportunity to use them for disease surveillanceis a strong advantage both economically andstrategically over having to collect new data.Nevertheless, because administrative databasesexist primarily for purposes other than diseasesurveillance, they may not be ideal in somerespects.
Administrative data cover the entire population,can be obtained without directly contactingindividuals, are not subject to recall bias, and are
largely computerized. Publicly funded healthinsurance in Canada is not dependent on incomeand covers almost the entire Canadianpopulation. Funding exceptions are people underfederal jurisdiction (e.g. in the military, in theRCMP, and in federal correctional facilities);however, they still have access to provincial/territorial health services and their records ofservice use are included in the regionaladministrative data. Medical services outside thepublicly funded system are not included; these
NDSS — A Response to the Challenge
8
NDSS Basic Principles
Consistency - A core set of variables iscollected in every province/territory on anongoing systematic basis.
Flexibility - Additional data can becollected within individual provinces orterritories in accordance with their uniqueneeds (e.g. data from prescribed druguse).
Quality - Data are validated and thecollection means are modified to ensureongoing data integrity across the country.
Cost-effectiveness - NDSS uses existingdata sources.
Accessibility - Data are available to thegeneral public under conditions agreed toby the Steering Committee, in accordancewith prevailing polices and regulationsregarding federal, provincial, territorial,and Aboriginal data.
Confidentiality - Personal identifiers areremoved, and only aggregate data areshared.
Responsiveness - Current information isdisseminated to public and privatestakeholders, thus enabling a promptresponse to changing trends in diabetes.

services are of limited availability in Canada, andmost are not regarded as medically necessary.
Disadvantages in using administrative databasesinclude the absence of detailed clinicalinformation and information on determinants ofhealth; duplication of information resulting fromhospital transfers and people accessing servicesin more than one jurisdiction; and currentinability to differentiate among the three types ofdiabetes. Also, administrative data includeinformation only on those who use healthservices; for people with diabetes, only thosewith a diagnosis from a health professional areincluded.
The requirement that Health Canada use onlyanonymous aggregate data for national analysesmay, at first, appear to be a serious constraint.However, because the aggregate data transferredto Health Canada can be customized to analysisneeds, the model is not limiting. Furthermore, asdiscussed later, data access guidelines allowresearchers to enter into agreements withprovinces, territories, and Aboriginal groups foruse of their data in bona fide research.
NDSS — A Response to the Challenge
9
Attributes of the NDSS System
�Distinct roles and responsibilities forprovinces and territories, the federalgovernment, Aboriginal groups, andother parties
�A shared data dictionary for coordinatingand comparing the administrativedatabases across provinces andterritories
�Three domains of measurement:descriptive epidemiology, complicationsand co-morbidities, and health servicesutilization
�A discrete set of outcomes related tohealth services and health status thatcan generally be implemented acrossmost provinces and territories
�Ability to produce annual person-specificsummarizations of health services andhealth status information forsurveillance purposes
�The option of using various casedefinitions
�A series of aggregate datasets thatreflect the major domains ofmeasurement and measured outcomes,and a strategy for sharing data withparties outside the provinces orterritories where the person-specificdata are held
�Software to run the system
�The ability to conduct longitudinalanalyses
NDSS represents the first time that acoordinated national use of administrativedata for public health surveillancepurposes has been undertaken.

Structure and Governance
The NDSS governance structure (Figure 1)includes a multi-stakeholder Steering Committee,several working groups, Aboriginal communitygroups, national coordination and technicalsupport based at Health Canada, and technicalstaff within each province and territory.
Steering Committee
The Steering Committee (Table 1) is the maindecision-making body of NDSS. The SteeringCommittee reviews all NDSS activities, includingrecommendations by working groups, and
coordinates the publication and dissemination ofinformation products directly resulting fromNDSS activities. This body also acts asgatekeeper for NDSS national data, determiningunder what conditions NDSS-related data are tobe made available to partners and third parties,with appropriate input and direction from dataoriginators and custodians.
Any private-sector sponsors of NDSS may haveobserver status on the Steering Committee but donot have voting rights.
Structure and Governance
10
NDSS Steering Committee
(Federal/Provincial/Territorial Governments,Aboriginal Groups, Non-Government Sector, Academia)
CanadianDiabetes Strategy
ScientificWorkingGroup
ExternalManagement
Working Group
Data Access &Publications
Working Group
TechnicalWorkingGroup
ValidationWorkingGroup
AboriginalDiabetes
Working Group
NDSS Technical Consultants
(Each province andterritory is represented)
Figure 1.NDSS Governance Structure

Table 1.Steering Committee Membership(See Appendix C for names of members)
Provincial/Territorial Governments
YukonNorthwest TerritoriesNunavutBritish ColumbiaAlbertaSaskatchewanManitobaOntarioQuebecNew BrunswickPrince Edward IslandNova ScotiaNewfoundland and Labrador
Non-Government Organizations
Canadian Diabetes AssociationCanadian Institute for Health InformationCanadian Institutes of Health ResearchDiabetes Council of Canada
Aboriginal Groups
Assembly of First NationsCongress of Aboriginal PeoplesInuit Tapiriit KanatamiMétis National CouncilNational Aboriginal Diabetes Association
Federal Government
Health Canada – Centre for ChronicDisease Prevention and ControlHealth Canada – First Nations & Inuit HealthBranchStatistics Canada
Academics/Clinicians (2)
Note: GlaxoSmithKline Inc. is a pioneering sponsor ofNDSS and has observer status on the NDSS SteeringCommittee
Working Groups
Six working groups meet independently asneeded and report to the NDSS SteeringCommittee. Working group activities andresponsibilities are presented in Table 2 andcurrent members are listed in Appendix D.
Partnerships
Partnerships are central to the NDSS, which hasset a number of precedents in this area.Agreements are in place with some Aboriginalgroups, the Canadian Institutes of HealthResearch, Health Canada, and the provinces andterritories.
During 2000 to 2002, Health Canada and eachof the 10 provinces and 3 territories signedMemoranda of Understanding (MOUs), which setforth the terms for administering federal fundingfor NDSS under the direction of the SteeringCommittee and through Health Canada’sOperating and Maintenance (O&M) financialmechanism. The form of the MOUs is containedin Appendix E.
Three-way partnership activities amongAboriginal groups (First Nation, Métis, Inuit orother Aboriginal people in rural and/or urbanlocations), Health Canada and the respectiveprovincial or territorial health ministry began in2001. So far, MOUs have been signed in tworegions – all First Nations in British Columbia andthose in one area of Quebec.
Structure and Governance
11

Table 2.Working Groups and Areas of Responsibility
External Management Working Group� guides interactions with key external stakeholders� oversees efforts to obtain non-federal funding� manages all other aspects of public relations� developed agreements between governments for data activities� developed a duality of interest policy� developed guidelines for fundraising and sponsorship
Data Access and Publications Working Group� develops policies around conditions of NDSS data access, ownership, and publication� develops an annual publishing plan
Aboriginal Diabetes Working Group� promotes the development of the Aboriginal component of NDSS� provides technical leadership� provides guidance in relation to Aboriginal data ownership, access, and privacy� guides the development of a Memorandum of Understanding (MOU) between Aboriginal partners, respective
provinces/territories and Health Canada
Validation Working Group� advises the NDSS Steering Committee on standardization of the surveillance case definition� determines which variables are to be collected� decides on methods to be used for database validation
Scientific Working Group� provides support and advice to the Steering Committee on research initiatives/approaches to improving diabetes
surveillance and analysis of NDSS data� focuses on the state of knowledge of diabetes
Technical Working Group� focuses on the methods and algorithms for data development and programming� is responsible for the evolution of the NDSS software� translates into practice the scientific ideas proposed by the validation and scientific groups� fosters innovations for generating improved data products
Technical Consultants� responsible for the implementation of the NDSS software and hardware� documents the unique characteristics of the provincial/territorial databases
Structure and Governance
12

Responsibilities
Health Canada
Under the MOUs, Health Canada, through itsCentre for Chronic Disease Prevention andControl, agrees to provide the resources neededto coordinate NDSS activities nationally. Theseinclude, but are not limited to, monitoring ofnational NDSS-related staff, infrastructuresupport of national NDSS-related personnel,participation on committees and working groupsas appropriate, coordination of standardized dataextraction and linkage, and establishment andmaintenance of the central database of aggregatedata from the provincial/ territorial/Aboriginalpartners. Coordination also involves liaising withthe various working groups, providing secretariatsupport, and promoting a coordinated work plan.In addition, Health Canada liaises withnon-governmental partners with regard toprivate-sector funding for activities approved bythe Steering Committee.
Provinces and territories
As signatories to the Memorandum ofUnderstanding, all 13 provinces and territoriesare responsible for administering NDSS activitiesin their area, notably the maintenance of requiredsoftware and the transfer of aggregate data toHealth Canada. Provinces and territories alsomonitor regionally located NDSS-relatedpersonnel, provide infrastructure support forregional NDSS-related personnel, and participateon committees and working groups asappropriate. Provinces and territories areresponsible for submitting resource allocationinformation for each year to the SteeringCommittee.
Aboriginal groups
The Aboriginal partners in NDSS have severalroles. Initially, Aboriginal partners facilitateidentification of their members in NDSS datasetsprepared by the provinces and territories.Subsequently, Aboriginal partners contributeknowledge about and network within theirmembership to support data interpretation, useof appropriate communication styles, anddissemination. Aboriginal partners also anticipatea leadership role in applying NDSS findings toplan, implement, and evaluate diabetesstrategies and to develop policy.
Guidelines
Appendix F presents guidelines relating to threeareas – duality of interest; fundraising andsponsorship; and data access and publication.Highlights from each area are presented below.
Duality of interest
Within the context of membership on the SteeringCommittee, a situation involving duality ofinterest may arise in two ways: first, if a memberhas the opportunity to influence the businessdecisions of the Steering Committee in a way thatcould lead to personal financial gain for themember or his/her family; and second, if amember’s interests are opposed to the interests ofthe Steering Committee.
Structure and Governance
13

Disclosure of duality of interest is an agenda itemfor all meetings, and such disclosures arerecorded in the minutes. A member shall not voteon, approve or recommend approval of atransaction or contract with which he or she isassociated. Therefore, members with a conflict ofinterest are required to absent themselves fromthe meeting during discussion of any itemspertaining to the conflict.
Fund-raising and sponsorship
A unique aspect of NDSS is the opportunity forprivate-sector sponsorship. One of the roles of theCanadian Diabetes Association (CDA), anon-governmental founding partner, was themobilization of private sector sponsorship, mostnotably that of GlaxoSmithKline Inc. in 1999.
Principles for fund-raising have been establishedto ensure an open and transparent process.Private sponsors have no influence on thedecisions and activities of NDSS, and cannotdirectly benefit from public knowledge generatedby NDSS. Eligible sponsors are required toprovide long-term commitment and to have anappropriate fit between NDSS and corporatebusiness priorities.
Data access and publication
This policy outlines the procedures believednecessary to process research requests efficientlywhile ensuring both consideration of the publicinterest and full compliance with legislation. Thepolicy covers data collected, linked and/oranalyzed with the assistance of NDSS resources.Data and data products that can be accessed areunpublished aggregate data that reside at HealthCanada, person-level data that reside atprovincial and territorial sites, and NDSSprogramming codes.
The guidelines for data access cover:
� guiding principles (e.g. that the provinces,territories, and Aboriginal groups must be inagreement with any and all uses of theirrespective data);
� uses of data and products;
� ethical review for access;
� requirements to request access;
� disclosure (i.e. before release, reportscontaining any data requested throughNDSS, or reports generated using NDSSdata will be reviewed);
� protection of privacy and confidentiality; and
� destruction.
Structure and Governance
14

Focus on Aboriginal Populations
The prevalence of diabetes in some First Nationspopulations is three to five times the nationalrate. Rates are even higher in some First Nationslanguage groups, and there is a north-southgradient, with people in the south having higherdiabetes rates than those in isolated northerncommunities.7-9
Rates of diabetes in other Aboriginal groupsvary.9-11 In the 1991 Aboriginal Peoples’ Survey,self-reported diabetes prevalence was 5.5%among Métis and 1.9% among Inuit.10
Diabetes also develops at an earlier age amongFirst Nations people and, in recent years, type 2diabetes has been diagnosed in children.12
Almost one-third of First Nations women withdiabetes report first being given the diagnosisduring pregnancy.7
Factors that pose a risk to Aboriginal populationsare both heredity and lifestyle. The relativelyrecent shift from traditional diets high in animalprotein to “modern urban diets” high incarbohydrates, combined with decreasedphysical activity, result in high levels of obesitythat compound pre-existing risks for diabetes.
NDSS contains an “Aboriginal component”intended to address some of the uniqueinformation concerns of these populations. NDSShas endorsed the need to have Aboriginal peopleinvolved in its development.
Identifying Aboriginal Data
To identify records as belonging to an Aboriginalgroup, data routinely collected and managed bythe province or territory are linked to theAboriginal group’s membership information inthe province or territory. A temporary “identifier”is attached to selected records to allow extractionof Aboriginal-specific data. Routine NDSScalculations and data aggregation are thenapplied, and approved aggregate data files aresubmitted to Health Canada for nationalreporting.
A more complex and outstanding issue is how toidentify and then create diabetes surveillancedata for the urban Aboriginal population thatincludes non-status Indians.
Basic Principles
After review of the proposed NDSS model in1999, Aboriginal representatives’ questionsabout using personal health information led tothe development of principles specific to theirinterests. These principles define aspects of thepartnership arrangement and augment the basicNDSS principles. In particular, they address theneed to identify and then minimize possible risksassociated with the introduction of nominalmembership lists into NDSS processes.Specifically, the Aboriginal partners require thefollowing:
� Consent - An Aboriginal organization withlegitimate authority to represent a uniquegroup of Aboriginal people would provideconsent before any work begins in diabetessurveillance.
Focus on Aboriginal Populations
15
In some Aboriginal populations, the preva-lence rate of diabetes is three to five timesthe national rate.

� Confidentiality - The province or territorywould not release Aboriginal data withoutthe Aboriginal partner’s approval.
� Privacy - Aboriginal groups would haveenforceable assurances that the privacy oftheir membership lists and that of membersis protected when their information is usedto identify Aboriginal people withinpre-existing NDSS datasets.
�Data Storage - Aboriginal partners wouldspecify where, for how long, and under whatconditions data storage occurs, if at all.
�Ownership and Control - Aboriginal groupswould hold principal ownership of NDSSnon-nominal, person-level data and wouldspecify when and under what conditionsothers may have access to the data.Aggregate data would be released fornational reporting, and access by otherswould be controlled by the MOU and existingNDSS policy.
Partnerships
The proposed collaboration involves three-waypartnerships among Aboriginal groups,provinces/territories and Health Canada. Theprocess for forming these partnerships isinfluenced by the priorities of all three parties andby each Aboriginal group’s unique political andsocial history that defines inter-governmentalrelations. Rarely does either the history or currentrelations facilitate discussion.13
Staff shortages and constraints can interfere withmoving the recognized problem of diabetes intothe active phase of a decision-maker’s agenda.Also, Aboriginal leaders are often fully focused onmore urgent political or social threats and mustfollow the established protocol forcommunicating issues to membership andgaining their support in new initiatives. Yet,despite these difficulties, concerns are beingallayed and partnerships are forming.
Progress includes development of two MOUs.One MOU in Quebec involves the Cree Board ofHealth and Social Services of James Bay; theother MOU in British Columbia involves the FirstNations Chiefs’ Health Committee, First NationsSummit. In these regions, there was apre-existing infrastructure and a data-sharingprocess ready to accommodate the opportunity tocarry out diabetes surveillance. Other FirstNations, Métis and Inuit groups are consideringor are involved in developing MOUs to participatein diabetes surveillance. Though this work willtake time, the models for an MOU in BritishColumbia and Quebec will assist this process.
Focus on Aboriginal Populations
16

Methods of Data Capture
NDSS uses person-specific administrativedatabases organized originally to supportpayment of claims under publicly funded healthinsurance. In Canada, publicly funded healthinsurance is mainly the responsibility of theprovinces and territories and covers almost theentire population.
NDSS uses three types of databases, which existin all provinces and territories and can providedata by fiscal year: the physician claims file, thehospital file, and the health insurance registry.These databases are linked by a unique lifetimeidentifier that is usually an encryption of thepersonal health insurance number.
In each province and territory, the files arerestricted to residents to avoid duplicate countingof people, since tracking individuals who live inone jurisdiction but obtain much of their care inanother or who migrate back and forth betweenprovinces is problematic. NDSS does not yet useother data sources, such as prescription drug usedatabases, that are either not consistent or notavailable across the country.
The provincial/territorial physician claims file andthe hospital file supply numerator data; thehealth insurance registry supplies denominatorsand socio-demographic characteristics.
Physician Claims File
Physicians’ services performed in hospital, officeor clinic are captured in the physician claims file.With few exceptions, each physician claimcontains only one diagnosis, coded usingICD-9.14 Some provinces allow up to threediagnostic codes per claim. NDSS uses only the
first code for consistency. This may result insystematic under-reporting but generatescomparable data for describing trends.
The physician claims file is central to the diabetescase-ascertainment algorithm and to algorithmsbeing developed for estimating complications andhealth services use. Information in the claims fileabout payments for services may also be usefulas algorithms are developed to refine estimates ofthe economic burden of diabetes.
Table 3.Percentage (%) of Physicians Paid
only on a Fee-For-Service Basis
Fiscal Year
Province 1995/9615 1999/0016
British Columbia 92 79Alberta* 98 98Saskatchewan 84 82Manitoba* 47 40Ontario* 94 93Quebec 62 61New Brunswick 52 58Prince Edward Island* 92 63Nova Scotia* 74 62Newfoundland andLabrador
73 46
* shadow billing
A limitation of the claims file is that physiciansnot paid on a fee-for-service basis are not alwaysrequired to submit medical claims. Table 3shows the distribution by province of physicians
Methods of Data Capture
17

paid only on a fee-for-service basis. Otherpayment schemes include salary, contract,capitation, and partial fee-for-service. Alternativepayment of physicians is more frequent for somespecialties, in remote areas, and for someprimary health care centres. However, in somejurisdictions physicians under alternativepayment schemes are still expected to remitservice information, otherwise known as “shadowbilling”.
Hospital File
Information about each hospital visit or stay iscollected at discharge using an abstracting form.Diagnoses are coded using ICD-9 or ICD-9-CM.All jurisdictions except Quebec currently submitdischarge abstract data to the Canadian Institutefor Health Information, where data quality editsare conducted17 and the data are compiled intothe Discharge Abstract Database (DAD). Quebecuses a similar process for data quality checks.
The diagnostic information is used in the diabetescase ascertainment algorithm (although fewerthan 2% of cases have only a hospitaldiagnosis18,19). Although there maybe several diagnostic codes for asingle admission, only the first threeare used because of data limitationsin some provinces and territories.Also, records relating to day surgeryare excluded because some provincesdo not include these procedures intheir hospital discharge files.
Health Insurance Registry
The registry contains a record foreach person entitled to coverageunder the provincial/ territorial healthinsurance scheme. NDSS abstractssex, date of birth (to calculate age)
and geographic code from this file (even thoughthe information may also exist in the other files).
The registry is also used to determine whetherpeople using hospital or medical services areresidents. Hospital records or records ofphysicians’ services with health insurancenumbers not in the registry file for that year areexcluded from further processing.
The registry file supplies denominators for ratecalculations. Therefore, assessments of theregistry’s accuracy for this purpose are needed. Inparticular, how closely this file represents thepopulation depends upon its being regularlyupdated with deaths and migrations.
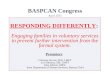
Generally, the date of death, or informationallowing its estimation, is recorded in the registry.Comparisons of provincial/territorial death countswith counts from Statistics Canada (Figure 2 andAppendix G) have demonstrated that, for mostjurisdictions, the registry is updated with deathinformation. Some problems have been identifiedwith updates in British Columbia.
Methods of Data Capture
18
YU NT BC AB SK MN ON PE NS
0
20
40
60
80
100
%a
gre
em
en
t:N
DS
Sto
Sta
tis
tic
sC
an
ad
a
Figure 2.Comparison of NDSS with Statistics Canada Deaths,
April 1995 to March 1999, by Province/Territory

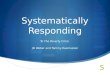
Comparisons of the mid-year population countsavailable from the registries with mid-yearestimates available from Statistics Canada(Figure 3 and Appendix G) have demonstratedthat, for most jurisdictions, registry updatingprovides population counts within 1% of theStatistics Canada estimates.
Problems identified in British Columbia areassociated with the premium system used there.Some duplicate counting of residents occurred inOntario, but the numbers were within 4% ofStatistics Canada estimates. Quebec’sregistration file was used only for people withdiabetes. Therefore, for this report, Quebec hasused estimates from l’Institut de la Statistique duQuébec rather than the registry population as thedenominator. In Nunavut, death data were notyet available for this report. All other provincesand territories were able to use the registry as adenominator, thereby more accurately reflectingthe population that generated the case countsobtained from the physicians’ services claims andhospital files.
Annual population counts are consistently higherthan the mid-year counts, by 4% for theprovinces and 8% for the territories (Appendix G),reflecting the difference between counting peopleand counting person-years; the sum ofperson-years will approximate the mid-yearpopulation count, but a count of people will
include those who reside in aprovince or territory for any portion ofa year. This effect is most evident inthe 40-55 age group (because ofmigration) and in the 80+ age group(because of deaths).
Data Processing at theProvincial/Territorial Level
Data processing at the provincial/territorial level, for which programsusing SAS® (Cary, NC) software havebeen developed, involves five discretephases, illustrated in Figure 4 andsummarized below:
� Select required data elements andtranslate provincial/territorial dataelement names/ types/codes intothe NDSS standard.
� Summarize each data source into one recordper person per year based on selectedcriteria.
�Merge the registry, hospital and physiciansclaims data, matching the unique identifier.
� Apply the diabetes case definition.
� Summarize the data by age group and sexand apply the appropriate calculations.
The first phase is customized to each jurisdiction,but all the remaining tasks are identical across allprovinces and territories.
Methods of Data Capture
19
YU NT BC AB SK MN ON PE NS
0
20
40
60
80
100
%a
gre
em
en
t:N
DS
Sto
Sta
tis
tic
sC
an
ad
a
Figure 3.Comparison of NDSS with Statistics Canada Population
Counts, July 1997/98/99, by Province/Territory

Figure 4.Data and Process Flow Diagram
Physician Claims Hospital RegistryPhase 1
Conversion/Translation
� unique identifier
� date of service
� diagnosis code
� fee item(service/procedure)
� amount paid
� unique identifier
� admission date
� separation date
� diagnosis codes (up to 16)
� procedures (up to 12)
� inpatient/day surgery
� Unique identifier
� sex
� Province/territory
� date of birth (age)
� geographic code
� fiscal year
� days of coverage in year
� date of death
� Select required data elements
� Rename and translatevariables into NDSS standarddefinitions
� Sort data by fiscal year
� Multiple records per person peryear permitted
Optional
� location where serviceprovied (hospital/office)
� physician specialty
Optional
� resource intensity (RIW)
� RIW exclusion factor
Optional
� insurance start date
� insurance end date
� insurance end reason
� insurance start reason
Data elements added:
� count of claims withdiagnosis of diabetesrecorded
� service date on first claimin fiscal year with diabetesas diagnosis
� service date of secondclaim in fiscal year withdiabetes as diagnosis
Data elements added:
� separation date for earliesthospital stay in year withdiabetes as one of thediagnoses
� total number of hospitaldays during stay
Data elements added:
� nonePhase 2
Summarization
� Sort data by ID and date
� Summarize data into one recordper person per year (linkagerequires unique identifier)
� Add/calculate data elements
� One file per fiscal year
Phases 3 and 4Create APLSF Dataset
� Merge (link) data sets by ID
� Exclude hospital and physiciandata with invalid ID
� Apply diabetes case definitionto all years of data forindividual
Phase 5Create Aggregate Data
� data summarized
� age groups can be specified
� optional cell suppression forcells with 1-5 observation
Methods of Data Capture
20
Annual Person Level Summary File (APLSF)
Data elements added:
� case date for diabetes case definition
� historic data elements from previous years
� days with diabetes in current year
� days without diabetes in current year
Incidence and Prevalence Output
� by P/T, age group, sex and year
� incident, prevalent and non-cases
� person-years at risk for incident,prevalent and non-cases
� incidence and prevalence rates
Mortality Output File
� by P/T, age group, sex and year
� deaths among diabetics and non-diabetics
� person-years
� mortality rates for diabetics andnon-diabetics
� rate ratio

The first phase, using a copy of theprovincial/territorial file, is to reduce the numberof variables retained in the file and to translatevariable names from provincial/territorial-specificcoding standards to a shared diabetes datadictionary. The remaining data processing steps(see Figure 4) summarize individual transactiondata into an annual summary, build the annualperson-level summary file (APLSF) and generateaggregate datasets.
A separate APLSF is constructed for each year.The APLSF is composed of a single recordsummary for each person in the registry fileregardless of diabetes status or whether insuredservices were used in the year. The recordsummary documents the year’s medical andhospital information for each person, includingevidence needed to determine whether the casedefinition was triggered. As NDSS develops,complications and health services use will beincluded in this file.
The APLSF retains personal health identifiers (orencrypted variants), allowing longitudinaltracking of individuals over time and, withappropriate consents, linkages to other datasets.
In a final step, additional variables are added tothe file, reflecting (where they exist) selected datafrom the individual’s record in the APLSF file forprevious years; this is of particular importance indetermining whether a specific diagnosis is newor pre-existing.
Because the APLSF holds data on individuals aswell as information such as dates of diagnosis,birth and death, the file is regarded as personalhealth data under the authority of existinglegislation and policy directives within eachprovince and territory. This makes the APLSF fileinappropriate to distribute outside the province orterritory.
The provinces and territories provide dataaggregated by age group and sex to the nationaloffice of NDSS (Health Canada). Data aresuppressed where the number of individualsrepresented in a cell is smaller than five. The dataare provided in a SAS® dataset, which isdescribed in Table 4. Definitions for the variablesin the APLSF dataset are provided in Appendix H.
The APLSF provides considerable flexibility inhow aggregate datasets might be created. Forexample, age groupings can be arbitrarily definedto suit analytic need, provided that the analyticneed is not inconsistent with the need to ensurethe confidentiality of personal health data.
Data Processing at the National Level
The aggregate datasets provided by the provincesand territories to Health Canada are the primarysurveillance products arising from NDSS. Asthese products are not personal health data underthe definitions of existing provincial policies orlegislation, they are suitable for distribution anddissemination.
The national calculations are the responsibility ofthe national office. To adjust for the effects ofdiffering age distribution on the rates, theprovincial/territorial data are standardized byspecific age group to the 1991 Canadian Censuspopulation (Appendix I).
Methods of Data Capture
21

Table 4.Contents of the Canadian Aggregate Datafile
Methods of Data Capture
22
Category Data Element Description Data Element Name
Demographic variables � Province or Territory . . . . . . . . . . . .� Fiscal year of Data. . . . . . . . . . . . .� Sex . . . . . . . . . . . . . . . . . . . .� Age Group . . . . . . . . . . . . . . . .
PTYEARSEXAGEGRP
People with a diagnosis of diabetes incurrent year
� Incident Cases: number of people withDM diagnosis in the current year . . . . . .� Person-years of observation after DM
diagnosis in current year . . . . . . . . . .� Person-years of observation before DM
diagnosis in current year . . . . . . . . . .� Incidence Rate . . . . . . . . . . . . . .
INCASE
INPYODM
INPYONDMIR
People with a diagnosis of diabetesprior to current year
� Prevalent Cases: number of people with DMdiagnosis prior to current year . . . . . . .� Prevalent Person-years. . . . . . . . . . .
PREVCASEPREVYRS
Prevalence (period) for current year � Period Prevalence Proportion . . . . . . . . PR
People not given a diagnosis of diabetes � Number of people not given a diagnosisof DM . . . . . . . . . . . . . . . . . .� Person-years Observed without diabetes . .
NONCASENONDMYRS
Mortality among people with diagnosisof diabetes
� Number of deaths among prevalentdiabetes cases . . . . . . . . . . . . . .� Person-years of observation for people
with a diagnosis of diabetes who died. . . .� Death rate for people with diabetes . . . . .
N1
D1Rill
Mortality among people without adiagnosis of diabetes
� Number of deaths among people notgiven a diagnosis of diabetes . . . . . . . .� Person-years of observation for people not
given a diagnosis of diabetes who died . . .� Death rate for people without diabetes . . .
N2
D2Rnil
Mortality comparison � Death rate with diabetes/death ratewithout diabetes (Rill/Rnil) . . . . . . . . . RR

Definitions and Calculations
Diabetes case
The case definition currently used in NDSSrequires that an individual have the following:
� one hospitalization with an ICD-9 code of250 (diabetes mellitus), selected from thefirst three diagnostic codes on the hospitalfiles, or
� two medical claims with an ICD-9 code of250 within 730 days, selected from the firstdiagnostic code.
The case date is currently defined as the earliestdate at which the case definition is met.
Age
Age is calculated as age as of the end of the fiscalyear. The age groups for national use are decadesbetween 20 and 49 (20-29, etc.) and 5-year agegroups thereafter (50-54, etc.) to age group85+.
Prevalence
Prevalence is the probability that an individualwithin a population will have diabetes during theyear.
In the NDSS, diabetes prevalence is calculated asfollows:
� (total number of people with a diabetes casedate prior to March 31 of the current fiscalyear) ÷
� (total population count for the current fiscalyear).
The denominator uses the count for the entireyear rather than the mid-year estimate, therebyincluding people who migrate or die during theyear, since they are included in the numerator.
In Quebec, however, the denominator is thecensus-based population estimate provided bythe ministère de la Santé et des Services sociauxdu Québec and calculated by the Institut de lastatistique du Québec.
Mortality
The mortality rate refers to the force of diabetesmortality for the total population. This measurecan refer either to deaths due to diabetes or todeaths of people with diabetes. Within NDSS, themortality rate is calculated separately for peoplewith diabetes and those without diabetes. Causeof death is not available, and therefore anymortality analyses are based on ALL causes ofdeath and not just deaths due to diabetes.
In NDSS the mortality rate among people withdiabetes is calculated as follows:
� (total number of deaths among people withdiabetes during the current fiscal year) ÷
� (total number of people with diabetes duringthe current fiscal year).
The mortality rate among people withoutdiabetes is calculated as follows:
� (total number of deaths among peoplewithout diabetes during the current fiscalyear) ÷
� (total number of people without diabetesduring the current fiscal year).
The mortality rate ratio is calculated as follows:
� (death rate among people with diabetes) ÷
� (death rate among people without diabetes).
In Quebec, the number of deaths among peoplewithout diabetes is derived from the Fichier desdécès (vital statistics, deaths), from which thenumber of deaths among people with diabetes issubtracted. The denominator for the rate among
Methods of Data Capture
23

people with diabetes is the difference betweencensus-based population estimates and thenumber of people with diabetes.
Data Validation
Since much of the administrative data used byNDSS was designed for billing purposes(particularly physicians’ services) rather than fordisease surveillance, the diagnoses capturedrequire validation. Such validation is ongoing andtakes several forms. Accuracy of thecase-definition algorithm is evaluated against agold standard that allows calculation of measuresof specificity and sensitivity, and then thesemeasures are examined in various ways:
� across jurisdictions
� against various gold standards
� over time
� for incident versus prevalent cases
� for special populations
� for designated complications
� for health services use
The case definition within NDSS is flexibleenough to incorporate improvements in thealgorithm suggested by the validation process.
Validation of the NDSS algorithm began withpublications in 1991 and 1996 and is stillongoing. Currently, nine of the 13 jurisdictionsare participating in validation studies. Recently,the NDSS and the CIHR Institute of Nutrition,Metabolism and Diabetes jointly funded
population health and validation research ondiabetes.
Various gold standards have been used, includingrecords from diabetes education3 and care19
programs, the National Population HealthSurvey,20-22 a provincial health survey,19 aprovincial diabetes registry18 and medicalcharts.23 Other studies, currently under way areusing prescription records for insulin and oralhypoglycemic medication, and clinical data.
So far, validation work has indicated that
� self-reported survey data should not be usedas a gold standard, since they underestimatethe true disease burden in thepopulation;21,22
� new cases and prevalent cases are difficultto differentiate in the early years,2 and atleast five years of data are needed beforestable estimates can be obtained;6,18
� the increase in prevalence among femalesseen during the child-bearing years may be theresult of miscoding of gestational diabetes;
� sensitivity measures have been 69%,19
85%18,23 and over 95%,3 depending uponthe gold standard used and the jurisdictionwhere the study was conducted;
� specificity has been over 95% and hasvaried less than sensitivity;18,19,23
� positive predictive value has been 78% and80% in two studies of adults,18,23 but hasbeen found to be low in children;24
� sensitivity, specificity and predictive valuemay be stable for five to seven years ofdata for adults, but they fall as more yearsof data are included and prevalent casesover-accumulate.18
The validation studies and definitions aredescribed in greater detail in Appendix J.
Methods of Data Capture
24
Validation work has substantiated the useof the NDSS algorithm for prevalence andmortality calculations using five to sevenyears of data for adults.

Facts and Figures
The following represents the first comprehensivecompilation and public dissemination of data byNDSS. The data presented below are derivedfrom the data collection period starting in1995/1996. The first two years constituted therun-in period required by the case definition.Therefore, the earliest data presented here are forthe fiscal year 1997/1998, and the most recentyear of data available for this report is1999/2000.
The information represents eight provinces andthree territories, accounting for over 95% of theCanadian population. Data from New Brunswickand Newfoundland and Labrador are notincluded in this report.
The data include both type 1 andtype 2 diabetes, as ICD-9 (code 250)does not differentiate between thetwo. However, since the data arerestricted to people aged 20 yearsand over, they largely represent type2 diabetes. Although gestationaldiabetes has its own ICD-9 code(648.0), it is often miscoded as type1/type 2 and therefore some cases ofgestational diabetes are included inthese tabulations.
Prevalence
In 1999/2000, 5.1% of Canadians (1,196,370)aged 20 and over were living with diagnoseddiabetes (Figure 5). This rate is higher than theself-reported rate of diabetes among people aged20 and over found by the National PopulationHealth Survey in 1998/99 (3.9%),25 or even theself-reported rate found by the more recentCanadian Community Health Survey 2000/01(4.7%).25 This is consistent with validationstudies21,22 showing that self-report survey dataunderestimate the true disease burden in thepopulation.
NDSS prevalence estimates represent diagnoseddiabetes among health services users. Prevalencemay be underestimated by 30% as a result ofsubclinical, undiagnosed diabetes.26
Facts and Figures
25
In 1999/2000, 5.1% of Canadian adultswere living with diagnosed diabetes.
1997/1998 1998/1999 1999/20000%
1%
2%
3%
4%
5%
6%
Female Male Both
* crude rate per 100 persons aged 20+ (not age standardized)
%o
fp
op
ula
tio
nag
e20+
Figure 5.Prevalence* of Diabetes in Canada by Fiscal Year and Sex

Prevalence over time
Figure 5 suggests increasing prevalence. Thisincrease is expected for a chronic condition suchas diabetes that has a lengthy disease duration.However, at this early stage of diabetessurveillance, the observed increase in prevalenceis due, in part, to detection of cases diagnosedbefore the start of observation (1995/1996).Future NDSS reports will be based on more thanfive years’ of data, allowing a clearer distinctionbetween prevalent (existing) and incident (new)cases.
Prevalence by sex
Figure 5 also demonstrates that diabetes is morecommon among Canadian men aged 20 andolder (5.4%) than among women (4.9%). Anexception to the male pre-ponderance occurs in
the child-bearing years (20-39), where cases ofgestational diabetes may be miscoded astype 1/type 2 diabetes (Figure 6).
Prevalence by age group
For both sexes, prevalence increases with age,peaking in the 75-79 age group at 15.5%(17.4% among males and 14.2% amongfemales) (Figure 6). People aged 65 and overaccount for almost 50% of diabetes cases butrepresent only about 15% of the population aged20 and over. The slight decrease in prevalence inthe oldest age groups (80+) may be the result ofmortality associated with diabetes or an artefactof limiting the number of conditions coded pervisit; increased co-morbidity at older agesincreases the likelihood that conditions otherthan diabetes will be recorded.
Facts and Figures
26
20-29 30-39 40-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+0%
5%
10%
15%
20%
Male
Female
* age and sex specific rate per 100 persons aged 20+
%o
fp
op
ula
tio
nag
e20+
Figure 6.Prevalence* of Diabetes in Canada, 1999/2000, by Age and Sex

Prevalence by region
Table 5 presents age-standardized prevalencerates by fiscal year, province/territory and sex forpeople aged 20 years and older. Detailedprevalence data by age, sex, jurisdiction andfiscal year are found in Appendix K. Figure 7compares the provinces and territories using age-sex standardized rates and 95% confidenceintervals.
For the majority of jurisdictions, age-sex adjustedprevalence ranges from 4.0% to 5.5%. Apparentdifferences among the provinces should beinterpreted with caution because of the effects ofdifferent populations, different data collectionprocedures, and variations in the likelihood ofdiagnosis. For example, Manitoba’s higher ratemay reflect the fact that Aboriginal peoplerepresent a relatively high proportion of itspopulation (13%)27 and that diabetes prevalenceamong Aboriginals is 3 to 5 times higher than thenational rate.7 This emphasizes the need to
identify specific populations at high risk ofdiabetes, such as Aboriginal groups.
Differences between provinces and territoriesmay not result from differences in the level ofdiabetes in the population. For example, theterritories have the highest proportion ofAboriginal peoples (22% in the Yukon, 46% inthe Northwest Territories and 81% in Nunavut)27
but the lowest prevalence rates. This may bebecause of the inability of some administrativedata to capture diabetes diagnoses outside thefee-for-service payment system. To investigatethis, Nunavut is conducting a pilot project thatincludes addition of community health nurse datato NDSS, and other validation projects areunderway (Appendix J).
Finally, differences between provinces andterritories may reflect differences in the likelihoodof diagnosis. For example, the three provinceswith the highest prevalence (Manitoba, NovaScotia and Ontario) also have the mostestablished diabetes programs.28
Facts and Figures
27
1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
Yukon 3.1 3.2 3.6 3.4 3.9 3.8
Northwest Territories 3.4 3.1 3.7 3.5 3.9 4.0
British Columbia 3.4 4.1 3.8 4.5 4.0 4.8
Alberta 3.2 3.8 3.6 4.2 3.8 4.5
Saskatchewan 3.7 4.4 4.0 4.8 4.1 5.0
Manitoba 4.4 4.8 4.9 5.3 5.3 5.8
Ontario 3.9 4.7 4.3 5.1 4.7 5.5
Quebec 3.8 4.6 4.1 5.0 4.3 5.2
Prince Edward Island 3.4 4.4 4.0 5.1 4.1 5.2
Nova Scotia 4.4 5.2 4.8 5.6 4.9 5.8
CANADA 3.8 4.5 4.1 4.9 4.4 5.2
Table 5.Prevalence* of Diabetes in Canada, by Fiscal Year, Province/Territory and Sex
* Rate per 100 people aged 20+, age standardized to 1991 Canadian population

Since one of the goals of NDSS is comparableinformation on diabetes, the impact of theseissues is being more closely examined. In thefuture, we expect to have a better understandingof differences in systems that may affect the datacollection and, ultimately, regional comparisons.
Mortality
In 1999/2000, the death rate among Canadianadults with diabetes was 1,393 per 100,000(age-sex standardized to the 1991 Canadianpopulation). This includes deaths due to externalinjuries or other causes that may not be directlyrelated to diabetes. This all-cause mortality of41,483 Canadians aged 20 years and over withdiabetes is 6.5 times the 1999 mortality count of
6,131 Canadians aged 20 and older whoseleading cause of death was listed as diabetes.29
The all-cause mortality rate seems to supportpast calculations estimating that the number ofdiabetes-related deaths is over five times thenumber of deaths with diabetes coded as theunderlying cause.30 Studies have demonstratedthat only 28% of death certificates with anymention of diabetes were coded with diabetes asthe underlying cause of death31,32 and thatdiabetes was not mentioned at all for 41% ofpeople with diabetes who died.31
Facts and Figures
28
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
YT NT NU BC AB SK MB ON QC PE NS
Canada
*age-sex standardized to 1991 Canada population
Pro
po
rtio
no
fP
op
ula
tio
nA
ge
d2
0+
Figure 7.Prevalence* of Diabetes in Canada by Province/Territory, 1999/2000
Canadian adults with diabetes are twice aslikely to die prematurely, compared topersons without diabetes.

Mortality over time
Figure 8 shows the age-standardized death ratesby fiscal year. In all years, the death rate issignificantly higher among those with diabetesthan those without for both sexes. While thedeath counts are increasing, the mortality amongpeople with diabetes relative to those without isstable over time (see Appendix L for mortality rateratios).
Mortality by sex
Across all three fiscal years, male mortality isconsistently higher than female mortality amongboth people with diabetes and those without.However, mortality among people with diabetesrelative to those without is slightly higher forwomen (mortality rate ratio 2.11) than for men(mortality rate ratio 1.87).
Mortality by age group
Figure 9 shows that for all age groups the deathrate for people with diabetes is higher than thedeath rate for those without. Figure 9 also showsthe rate ratio, which compares mortality ratesamong people with and without diabetes. Therate ratio is higher in the younger age groups andgradually decreases for the older ones. Thismeans that a 35-year-old Canadian with diabetesis 4 times more likely to die than a person withoutdiabetes, whereas an 85-year-old Canadian withdiabetes is 1.4 times more likely to die than aperson without diabetes.
Mortality by region
Canadian adults with diabetes are twice as likelyto die prematurely as adults without diabetes.Figure 10 demonstrates that this age-sexstandardized ratio is between 1.8 and 2.1 for the
majority of jurisdictions. The threesmallest jurisdictions (Prince EdwardIsland, the Northwest Territories andthe Yukon territory) have a rate ratioless than 1.5. The smallestjurisdictions have zero death countsin many of the younger agecategories, artificially reducing theirage- standardized mortality rates.
Comparisons of mortality rates byregion are influenced by manyfactors. Since people with diabetesare older than the general population,age-standardization makes the ratesmore comparable. The mortality rateratio provides comparison of themortality of people with diabetesrelative to those without diabetes.Table 6 presents age-standardized
Facts and Figures
29
Female Male Female Male Female Male0
500
1000
1500
2000
1997-1998 1998-1999 1999-2000
Persons with diabetes
Persons without diabetes
* age standardized to the 1991 Canadian population
de
ath
sp
er
10
0,0
00
po
pu
lati
on
*a
ge
20
+
Figure 8.Canadian Mortality* Rates by Fiscal Year,
Sex and Diabetes Status

mortality rates by fiscal year,province/territory, sex and diabetesstatus. Detailed mortality data byage, sex, jurisdiction and fiscal yearare found in Appendix L.
National Impact
NDSS data begin to paint a picture ofthe burden of diabetes in Canada.Diabetes is a large and growinghealth problem in Canada.Prevalence is increasing and isparticularly high among older adults.The mortality associated withdiabetes is considerable. The nextNDSS report will contain incidencedata that can be used to study riskfactors for use in projection models.
Facts and Figures
30
0%
5%
10%
15%
20%
25%
30-39 40-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+
Age Group
0.0
1.0
2.0
3.0
4.0
5.0
Deaths with Diabetes Deaths without Diabetes Rate Ratio
Ag
eS
pe
cif
icD
ea
thR
ate
Ra
teR
ati
o
Figure 9.Canadian Mortality Rates by Age and
Diabetes Status, 1999/2000
YT NT BC AB SK MB ON QC PE NS
0.00
0.50
1.00
1.50
2.00
2.50
Canada
* age-sex standardized to 1991 Canadian population
Rati
oo
fm
ort
ality
rate
*w
ith
:wit
ho
ut
dia
bete
s
Figure 10.Comparison of Mortality* for Canadians With and
Without Diabetes, 1999/2000, by Province/Territory

Facts and Figures
31
1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
Yukon DiabetesNo diabetesRatio
1.690.642.60
1.450.861.70
0.990.781.30
0.710.990.70
0.910.661.40
1.371.151.20
Northwest Territories DiabetesNo diabetesRatio
1.801.011.80
0.591.640.40
1.781.391.30
0.861.660.50
1.360.761.80
0.361.080.30
British Columbia DiabetesNo diabetesRatio
1.110.562.00
1.590.871.80
0.970.521.90
1.470.801.80
0.960.492.00
1.390.761.80
Alberta DiabetesNo diabetesRatio
1.190.602.00
1.520.931.60
1.100.542.10
1.430.881.60
1.060.551.90
1.470.871.70
Saskatchewan DiabetesNo diabetesRatio
1.120.591.90
1.560.941.70
1.160.562.00
1.580.961.70
1.160.562.10
1.700.931.80
Manitoba DiabetesNo diabetesRatio
1.300.572.30
1.480.931.60
1.170.611.90
1.810.971.90
1.180.582.00
1.590.951.70
Ontario DiabetesNo diabetesRatio
1.230.572.20
1.740.872.00
1.150.532.20
1.580.821.90
1.100.532.10
1.560.801.90
Quebec DiabetesNo diabetesRatio
1.530.662.30
2.271.162.00
1.370.642.10
2.021.111.80
1.360.612.20
2.011.041.90
Prince Edward Island DiabetesNo diabetesRatio
0.710.601.20
0.881.040.80
0.730.601.20
1.301.031.30
0.840.581.50
1.271.011.30
Nova Scotia DiabetesNo diabetesRatio
1.170.651.80
1.701.071.60
1.020.581.70
1.410.971.40
1.230.582.10
1.600.941.70
Canada DiabetesNo diabetesRatio
1.280.592.20
1.790.951.90
1.170.562.10
1.660.901.80
1.150.552.10
1.640.871.90
Table 6.Canadian Mortality* Rates by Diabetes Status, Fiscal Year, Province/Territory, and Sex
*Rate per 100,000 people aged 20+, age standardized to the 1991 Canadian population

Accomplishments,
Plans and Possibilities
The NDSS has accomplished a great deal in thefour years since the Prairie Pilot Studydemonstrated the feasibility of the concept of acoordinated, national use of administrative datafor public health surveillance. In particular, NDSShas built a firm foundation and framework tosupport its ongoing development. Much of thisearly and necessary work has involved chartingnew territory in relation to federal-provincial-Aboriginal group agreements, capacity-building,data-sharing, governance and guidelines. Someof the fruits of these efforts have been realized inthe production of the first national diabetessurveillance data. NDSS accomplishments aredetailed in Table 7 and are summarized below interms of what NDSS tells us, what it cannot tellus, and what it will tell us in the future.
What NDSS Tells Us
In a relatively short period of time, NDSS hasdemonstrated, first and foremost, that datacollected for administrative purposes can also beused to inform policy relating to a major publichealth problem in Canada. In particular, NDSScan measure prevalence, incidence andoutcomes over time for both the nation as a wholeand for specific regions. It can also comparehealth services use and other health problems ofpeople with and without diabetes.
Second, NDSS has demonstrated that, despiteregional differences, the various jurisdictionsacross Canada are able to cooperate to achievethe shared goal of reducing the burden ofdiabetes. In so doing, they have arrived at a set ofcommon standards and definitions for diabetesthat can be applied across the country.
Third, NDSS has developed a prototype ofdisease surveillance that can be applied to otherdiseases and conditions.
Fourth, the ability to examine trends (age-, sex-and region-specific) and to compare the healthexperience of people with and without diabetesmeans that NDSS data can also be used toexamine many research questions.
Fifth, the suite of databases available to NDSSpermits numerous cross-validation studies andprovides a richer dataset than could be achievedwith a single database.
Finally, NDSS demonstrates that Canadacontinues to be a world leader in the developmentof record-linkage and database methods.
What NDSS Does Not Tell Us
The NDSS has some limitations, many of whichmay eventually be overcome. The one of mostconcern is the inability to distinguish among type1, type 2 and gestational diabetes. Current workto distinguish gestational diabetes is promising.
A second limitation results from populationmobility and the consequent difficulties of recordduplication and losses to follow-up, both ofwhich contribute to data inaccuracies. A partialsolution to this problem may be periodic linkagesof the provincial/territorial databases with theNational Mortality Database for death clearance.
Third, information on risk factors for diabetes iscurrently very limited.
Accomplishments, Plans and Possibilities
32

Table 7.NDSS Accomplishments
Accomplishments, Plans and Possibilities
33
Governance model� Established the necessary partnerships at federal, provincial and territorial levels� Established a governance model for a distributed system� Obtained buy-in from all provinces and territories, and some Aboriginal groups, with input also from academia and industry� Established Health Canada’s leadership role as a facilitator
Capacity-building� Implemented a capacity-assessment exercise� Devised and implemented solutions for capacity inequities among jurisdictions� Initiated capacity-building at various levels, according to jurisdictional readiness� Created technical consultant positions in all provinces and territories
Data-sharing agreements� Reviewed each jurisdiction’s legislative framework relating to participation in NDSS� Developed and implemented a series of data-sharing MOUs accommodating each jurisdiction’s privacy and confidentiality
requirements� Tested and verified a process for development of data-sharing agreements
Dedicated resources� Obtained multi-year funding for system development� Submitted detailed business plans and expenditures
Duality of interest� Developed guidelines to ensure disclosure of conflict of interest, abstinence from action where necessary, and respect for
confidentiality
Sponsorship� Developed guidelines to provide an open and transparent process, restrict influence on decisions, and allow for diversity of funding
Data validation� Adopted a standard case definition for diabetes� Determined the core set of variables to be collected� Began data validation (ongoing)� Collaborated with the CIHR to fund validation projects using NDSS
Data management� Identified data sources� Obtained agreement on the structure and organization of the databases� Developed provincial and territorial databases to permit necessary linkages� Provided technical solutions for data paring to include the necessary variables/records only and for transferring data from existing
hardware to the NDSS hardware/space� Provided standard software for transforming data to NDSS format� Produced a person-level summary file that is maintained by the provinces and territories
Data access and publications� Determined data ownership� Developed policies for data access and for NDSS database/information publication rights
Reporting and dissemination� Provided provinces with data for provincial performance indicator reporting (PIRC)� Provided aggregate data for the 2002 Diabetes in Canada report� Produced the first NDSS report on diabetes prevalence and mortality

What NDSS Will Tell Us in theNear Future
Current NDSS funding extends until the end ofMarch 2004. The original vision and goals forNDSS identified several items that requireadditional time for completion.33 Progresstowards achieving these goals is discussedbelow.
Population coverage
New Brunswick has recently provided data toNDSS, and Newfoundland and Labrador are alsoplanning to provide data for the 2004 NDSSreport. Ongoing work on the validation of adiagnostic algorithm for people under the age of20 should be completed in 2003. With thesedevelopments, the 2004 NDSS report shouldcontain data on all Canadians.
Incidence
Incidence calculations have been defined, butrequire at least five years of data to allow time forthe rates to stabilize. Incidence data will beincluded in the 2004 NDSS report.
Health services use
The databases already in use for NDSS willsupport analysis of health services use by bothpeople with and those without diabetes. Thisanalysis can include physician visits, specialistvisits and hospital use. The development ofmethods for applying costs to service use willpermit refined estimates of the economic burdenof diabetes. Days of hospital stay and number ofservices provided will be included in the 2004NDSS report.
Complications
One of the primary goals of NDSS is to developthe capacity for long-term monitoring ofdiabetes-related complications. The Prairie Pilotdeveloped a stroke module that is ready fortesting with NDSS software. The next priorityof the Validation Working Group is thedevelopment of standard definitions for diabetescomplications, and the identification andvalidation of data sources. The 2004 NDSSreport will include estimates of diabetes-relatedcardiovascular disease, cerebrovascular disease,peripheral vascular disease, retinopathy andrenal disease.
Aboriginal participation
Data for the Aboriginal population in Canada arecurrently captured by NDSS but not identified. Sofar, two Aboriginal groups (one in Quebec andone in British Columbia) are working onidentification of Aboriginal data. The 2004 NDSSreport will include data for at least one FirstNations group.
Dissemination
National-level dissemination of some NDSSsurveillance information has been achieved.Some jurisdictions (Ontario,34 Quebec35 andPrince Edward Island36) have taken initial stepstowards meeting the objective of regionaldissemination, and British Columbia, Alberta,and Nova Scotia plan to release data in 2003.Software updates are anticipated in 2003 toallow regional analyses.
Accomplishments, Plans and Possibilities
34

What NDSS May Tell Us in the Long Term
NDSS was designed with flexibility in mind toaccommodate several additional surveillance“modules”. The phase of diabetes surveillancebeyond March 2004 could include one or more ofthese modules.
Risk factors
Information on determinants of diabetes,including modifiable risk factors, is required tobuild a complete surveillance picture for diabetes(see Table 8). Risk factor information is crucial tothe development of effective prevention andcontrol strategies, a fact reflected in the recentdirective from the Conference of Deputy Ministersof Health for the establishment of a surveillancesystem for chronic disease risk factors.
Health Canada’s Canadian Diabetes Strategy(CDS) prevention group has identified activitylevel, body mass index (BMI) and dietary intakeas three important risk factors on which toconduct surveillance.
Because this type of information is not availablethrough the data sources currently available toNDSS, it will have to be obtained throughsurveys, with their attendant technical (datacomparability, record linkage) and governance(access, privacy) requirements and costs.
Care indicators
The CDS care group has recommended theincorporation of indicators for care into diabetessurveillance. Hence, a list of core clinical andself-care indicators is under development.Applied expertise will be required to formulatemethods for distinguishing type 1, type 2 andgestational diabetes.
Diabetes education
Diabetes education programs are an importantresource for surveillance because of theirpotential to collect information on self-care,complications and disease progression and todirect interventions to improve diabetesmanagement. However, directed research toprovide an evidence base for specificinterventions is a prerequisite to theirincorporation into surveillance.
Other data sources
The scope for expanded diabetes surveillance isoutlined in Table 8. Integration of varied datasources expands the possibilities for analysis ofsurveillance data. For example, pre-clinicalscreening could include blood glucose data,which may be accessed from a laboratory resultsdatabase.
Application to other chronic diseases
Diabetes shares risk factors with other diseasesand is both an outcome and a determinant ofother conditions. Smoking, for example, is a riskfactor for cancer, cardiovascular disease andrespiratory disease as well as diabetes. Theseinteractions, coupled with the realities of limitedresources, make a compelling case for collabora-tion in chronic disease surveillance. The NDSSmodel is suited to other types of chronic diseasesurveillance where similar opportunities exist fortracking via client interactions with the healthcare system.
Accomplishments, Plans and Possibilities
35

Table 8.The Scope for Enhanced Diabetes Surveillance†
† Roy D. Adapted from Chronic Disease Surveillance in Canada: A background paper, June 2003.(37)
*Some of the listed sources are potential and may not be available at this time.
Accomplishments, Plans and Possibilities
36
Determinants Pre-clinical Clinical Outcome
DATA EXAMPLES:
genetics:prevalence of implicated genes
risk behaviour:activity levelbody massdietary intakesmoking
environment:
socio-economic:income leveleducation
DATA EXAMPLES:
screening:blood pressureblood glucose
risk reduction:healthy dietphysical activity rates
DATA EXAMPLES:
diagnosis:modes of diagnosistime to diagnosislaboratory testing
treatment and procedures:surgery
service use:hospitalizationphysician visitshome careambulatory carepalliative care
pharmaceutical:drug usecomplications and interactions
DATA EXAMPLES:
mortality:cause-specific deathssurvival rates
morbidity:complicationsdegree of disabilityquality of life
DATA SOURCES*:
surveyscensusworkplace monitoring
DATA SOURCES*:
screening databasessurveyspublic health databasesprimary care physicianselectronic health record (EHR)
DATA SOURCES*:
hospital databasesDischarge Abstract Databaseregistry dataprovincial data repositories
DATA SOURCES*:
vital statisticscoroner’s databasemultiple causes of death

Finding Answers
� Almost half of Canadian adults areoverweight. Since obesity is a risk factor fordiabetes, how will this trend affect theincidence and prevalence of diabetes inCanada in years to come?
� Cardiovascular disease is the leading causeof death in Canada. What proportion of heartdisease in Canada is associated withdiabetes?
� Canada’s population is aging. How willpopulation trends affect the number ofpeople in Canada with diabetes? What will itcost to care for them?
� To what degree have lifestyle changescontributed to the increased risk of diabetesin Aboriginal peoples relative to non-Aboriginals? After adjusting for differences inrisk factors between Aboriginals and otherCanadians, are Aboriginals more susceptibleto diabetes?
These are just a few of the many questions thatmust be answered in order to stem the rising tideof diabetes in Canada. Fortunately, with NDSS,Canada is well positioned to answer them.
A recognized world leader in record linkage anddatabase methods, Canada is applying itsconsiderable expertise to diabetes through NDSS.Since securing funding in 1999, NDSS is well onits way to meeting its four stated goals:
� a national standardized database fordiabetes with long-term monitoring fordiabetes-related complications through theintegration of new and existing databases;
� ongoing surveillance of diabetes and itscomplications in each province and territory,and in the Aboriginal population;
� dissemination of national comparativeinformation, and
� a basis for the evaluation of economic/cost-related issues regarding the care,management and treatment of diabetes inCanada.
In accomplishing its mission, NDSS is also aprototype for other types of chronic diseasesurveillance. In an expanded NDSS model, datacollected on diabetes include risk factors andcomplications. Those same data can also beanalyzed and disseminated for the preventionand control of other conditions, such ascardiovascular, cerebrovascular and renaldiseases.
Thus, the question posed at the beginning of thisreport – Can information systems designedprimarily as tools for budgeting and billing, beused to provide disease-specific information thatwill benefit all Canadians? – has been answered.And this means that answers will be found formany more questions important to Canadians.
Finding Answers
37

References
1. Young TK, Roos N, Hammerstrand MA.Estimated burden of diabetes mellitus inManitoba according to health insuranceclaims: a pilot study. Can Med Assoc J1991;144(3):318-324.
2. Blanchard JF, Ludwig S, Wajda A, Dean H,Anderson K, Kendall O, et al. Incidence andprevalence of diabetes in Manitoba,1986-1991. Diabetes Care 1996; 19:807-11.
3. Blanchard JF, Dean H, Anderson K, WajdaA, Ludwig S, Depew N. Incidence andprevalence of diabetes in children aged 0-14years in Manitoba, Canada. Diabetes Care1997;20:512-5.
4. Canada health action: building on thelegacy. National Forum on Health. Ottawa:Health Canada,1997.
5. Noseworthy T, Blanchard J, Campbell D,Chapman S, Clottey C, James R, Osei W,Svenson L. Final report: demonstration ofthe proposed National DiabetesSurveillance System in the three prairieprovinces. Report to Health InfostructureSupport Program. Ottawa: Health Canada,March 2001.
6. Thacker SB, Berkelman RL. Public healthsurveillance in the United States. EpidemiolRev 1988;10:164-190.
7. First Nations and Inuit Regional HealthSurvey National Steering Committee. FirstNations and Inuit Regional Health Survey:national report 1999. Ottawa: HealthCanada, January 1999.
8. Johnson J, Martin D, Sarin C. Diabetesmellitus prevalence in the First Nationspopulation of British Columbia Canada,1987 to 1997. Int J Circumpolar Health2002;61:260-264.
9. Young TK, Szathmary E, Evers S, WheatleyB. Geographical distribution of diabetesamong the native population of Canada: anational survey. Soc Sci Med 1990;31:129-139.
10. Statistics Canada. Aboriginal PeoplesSurvey: language, tradition, health, lifestyleand social issues. Ottawa: StatisticsCanada, 1993.
11. Harris S, Gittelsohn J, Hanley A, Barnie A,Wolever T, Gao J, et al. The prevalence ofNIDDM and associated risk factors in NativeCanadian. Diabetes Care 1997;20:185-7.
12. Dean H. NIDDM among youth in FirstNation children in Canada. Clin Pediatr1998;37:89-96.
13. Joseph R. Issues relating to diabetessurveillance in the Aboriginal community.Ottawa: Health Canada, Aboriginal DiabetesWorking Group, December 2000.
14. International classification of diseases, 9threv. Geneva: World Health Organization,1997.
15. Canadian Institute for Health Information.Health Care in Canada, a first annualreport, 2000. Ottawa: CIHI, 2000.
References
38

16. Canadian Institute for Health Information.Alternative payments and the NationalPhysician Database (NPDB), the status ofalternative payment programs forphysicians in Canada, 1999/2000. (Table4). Ottawa: CIHR, October 2001.
17. Canadian Institute for Health Information.Discharge abstract database. Availablefrom: URL: http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=services_dad_e
18. Van Til L. PEI diabetes validation project.Report to the NDSS Validation WorkingGroup. Charlottetown: Document PublishingCentre, March 2001.
19. LeBlanc J, Kephart G. Assessment of thesensitivity and specificity of Nova Scotiaadministrative databases for detectingdiabetes mellitus. Report to the NDSSValidation Working Group. Halifax: PopulationHealth Research Unit, January 1998.
20. Tamblay JL, Catlin G. Sample design of theNational Population Health Survey. HealthRep 1995;7:29-38.
21. Svenson L. Assessment of the sensitivityand specificity of Alberta Health admini-strative data for diabetes surveillance.Report to the NDSS Validation WorkingGroup. Edmonton, March 1999.
22. Hux JE. Using administrative data to definethe prevalence of diabetes mellitus inOntario. Report to the NDSS ValidationWorking Group. Toronto: ICES, March1999.
23. Hux JE, Ivis F, Flintoft V, Bica A. Diabetes inOntario: determination of prevalence andincidence using a validated administrativedata algorithm. Diabetes Care 2002;25(3):512-6.
24. Clayton D, Smith M, Dunbar P, Salisbury S,Kephart G, LeBlanc J. Validity of theDiabetes Care Program of Nova Scotiadatabase of new cases (DNC) of diabetesaged < 19 years in determining theincidence of type 1 diabetes mellitus in thispopulation. Report to the NDSS ValidationWorking Group. Halifax, May 2000.
25. Statistics Canada. Health indicators.Available from URL: www.statcan.ca/english/freepub/82-221-XIE/01002/hlthstatus/conditions2.htm#diabetes
26. Harris MI, Robbins DC. Prevalence ofadult-onset IDDM in the US population.Diabetes Care 1994;17:1337-1340.
27. Statistics Canada. Population reportingAboriginal identity by province/territory,2001 census. Available from : URL:www.statcan.ca/english/Pgdb/demo38_96b.htm
28. Canadian Diabetes Association. Diabetesreport card 2001. Available from: URL:www.diabetes.ca/files/cda_report_card.pdf
29. Health Canada. Data from the StatisticsCanada Mortality File, compiled forDiabetes in Canada. Ottawa: HealthCanada, 2002.
30. Health Canada. Diabetes in Canada:national statistics and opportunities forimproved surveillance, prevention, andcontrol. Ottawa: Health Canada, 1999.
31. Tan HM, Wornell CM. Diabetes mellitus inCanada. Diabetes Res Clin Prac1991;14:S3-S8.
32. Wilkins K, Wysocki M, Morin C, Wood P.Multiple causes of death. Health Rep1997;9(2):19-30.
References
39

33. Diabetes Surveillance Working Group,NDSS. Diabetes surveillance blueprint2000 to 2010. Report to the CoordinatingCommittee of the National DiabetesStrategy. Ottawa: Health Canada, January2003.
34. Hux JE, Booth GL, (Slaughter PM, LaupacisA (eds). Diabetes in Ontario: an ICESPractise Atlas. Institute for Clinical andEvaluative Sciences; 2003. Available atwww.ICES.on.ca
35. Institut national de santé publique.Prévalence du diabète au Québec et dansses régions : premières estimations d’aprèsles fichiers administratifs. Octobre 2002.Available from: URL: www.inspq.qc.ca
36. Van Til L. Prince Edward Island healthindicators, provincial and regional.Charlottetown: Document PublishingCentre, January 2003. Available at: URL:www.gov.pe.ca
37. Health Surveillance Coordination Division,Centre for Surveillance Coordination,Population and Public Health Branch.Chronic Disease Surveillance in Canada: ABackground Paper. Ottawa: Health Canada,July 2003.
References
40

Appendices
Appendix A
NDSS Capacity Assessment Form . . . . . . . . . . . . . . . . . . . . . . . . . 43
Appendix B
Regional Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Appendix C
NDSS Steering Committee Membership 2003 . . . . . . . . . . . . . . . . . . . . 56
Appendix D
NDSS Working Group Membership 2003 . . . . . . . . . . . . . . . . . . . . . . 57
Appendix E
Memorandum of Understanding (MOU) . . . . . . . . . . . . . . . . . . . . . . . 60
Appendix F
NDSS Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Appendix G
Comparison of NDSS and Statistics Canada Counts of Death and Population . . . . . 74
Appendix H
Annual Person-level Summary File (APLSF) Data Elements . . . . . . . . . . . . . . 76
Appendix I
Canadian Standard Population Estimates – July 1, 1991. . . . . . . . . . . . . . . 77
Appendix J
Validation Work . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
Appendix K
Age-specific Prevalence by Fiscal Year, Sex and Province/Territory . . . . . . . . . . 82
Appendix L
Age-specific Mortality by Fiscal Year, Sex and Province/Territory . . . . . . . . . . . 94
Appendices
41


Appendix A
NDSS Capacity Assessment Form
This is a summary of the capacity assessmentcompleted by the provinces and territories forNDSS funding allocations in 2000/01. Mostjurisdictions provided answers to the series ofquestions.
The capacity assessment had five components:
� description of existing infrastructure
� description of availability of data variablesincluded in NDSS data dictionary
� assessment of capacity to achieve NDSScore model activities
� outline of funding proposal 2000/01
� addendum describing funding criteria andguidance on computer hardwarerequirements
Existing Infrastructure
Data: Where are the registry, hospital andphysicians’ claims data (or comparable datasources) currently stored? Is there documentationto describe the input data? Provide a subjectiveassessment of the quality of extantdocumentation. For what time periods do reliabledata exist for the registry, physicians’ andhospital files? Who is/are the key contactperson(s) needed to facilitate technical access tothe data? Name(s), title(s), phone number(s).
Computing infrastructure: Is SAS used within theMinistry? What mechanisms exist to transfer data“out” of this environment to a common platformfor NDSS development? Tape? CD? Other?
Computer/data security: What, if any, legislationgoverns the collection and use of personal healthdata (please provide copies of statutes)?
Epidemiology and diabetes infrastructure inprovince/territory environment: Is there aprovincial “office” for diabetes? Is there aprovincial “office” for epidemiology?
Provincial/territorial health system: Is there alifelong personal identifier in use within thejurisdiction? What year was it established? Doesit cover all eligible individuals (e.g. other thanRCMP, military, federal prisoners)? Are theresubpopulations that are differentially less or morelikely to be observed by core data sources?
The databases: Are there files that operationalizethe three “core” databases described in the NDSSdata model (Jan 2, 2000)?
NDSS data environment: Is there an existing,physically secure location in which the NDSSdata might be housed?
Appendix A
43

Availability of Variables Included in NDSS Data Dictionary1
Registry File
ID Personal identifierSex M or FDate of Birth Are invalid dates allowed?Year For which data are applicable?Postal Code (in year) or other subprovincial geographic variable, such as regional health areaInsurance Start Date (in year)Insurance Start Code 1 In force on Jan 1 of year
2 Newly insured from Jan 1of year3 Other
Insurance End Date (in year)Insurance End Code 1 In force on Dec 31 of year
2 Death3 Migration4 Other
Medical Claims File
IDService DateProcedure Code (please specify codes if available)
Amputations, new hemodialysis, cataract surgery, new peritoneal dialysis, ongoing peritonealdialysis, ongoing hemodialysis, lower-limb amputations, cardiovascular surgery (CABG, angio),laser photocoagulation, vascular reconstruction procedures (PTCA)
Diagnosis ICD-9 3-digitFee PaidPhysician ID*Physician Speciality* (List specialties supported)Location of Service* 1 Inpatient
2 Outpatient
Appendix A
44
1 Variables with asterisks will be used in the initial release of the NDSS software, but if this variable is not available in a province orterritory, the associated loss of functionality does affect the core goals and measures of NDSS.

Hospital Discharge File
IDDate of AdmissionDate of DischargeAdmission Type* . . . . . e.g. urgent, elective, etc.Discharge Type* . . . . . Death, transfer, to communityDiagnosis 1 . . . . . . . ICD-9 5-digitDiagnosis 2Diagnosis 3Procedure 1Procedure 2Procedure 3Transfer in?*Transfer out?*Resource Intensity Weight*Case Mix Group*
Capacity to Achieve NDSS Core Model in 2000-01
Feasibility of core activities (1 = no anticipated problems - planned implementation, 2 = some problems anticipated,but implementation still likely, 3 = major problems anticipated, implementation uncertain, 4 = not proposed)
Activity Description Suggested Skill Set
A. Core Model Activities
InputsIdentify data source for physician claims, hospital and coverage files. Ideally,select a “run” of 5-7 years for which there are continuously available data,and a single data dictionary.
SAS/systems analysis
Process(A1.1) Transfer data from existing hardware to NDSS hardware/disk space.
(A1.2) Reduce data from (A1.1) to include only necessary variables andnecessary records.
(A1.3) Concurrent with (A1.2) or subsequent to (A1.2) transform data from(A1.2) to NDSS common input data dictionary.
(A1.4) Read data from (A1.3) into SAS files.
(A1.5) Transform data from (A1.4) to calendar years.
(A1.6) Input data from (A1.5) into NDSS core software.
(A1.7) Produce “working” person-level summary.
SAS/systems analysis
Appendix A
45

Activity Description Suggested Skill Set
A. Core Model Activities (continued)
Outputs(A1.8) Prepare aggregate data files to estimate incidence, prevalence andmortality from (7).
(A1.9) Prepare aggregate data files to estimate rates for specifiedcomplications and health services utilization patterns in subpopulation withdiabetes.
(A1.10) Prepare aggregate data files to estimate rates for specifiedcomplications and health services utilization patterns in subpopulationwithout diabetes.
Statistical analysis
(A1.11) Transfer aggregate datasets to Health Canada, as defined by FPTagreements.
(A1.12) Retain (A1.7) for diabetic populations.2
(A1.13) Retain (A1.7) for non-diabetic populations.3
SAS/systems analysis
(A1.14) Disseminate data products coordinated with NDSS SteeringCommittee on an annual basis.
Policy/ communication-related
Policy-relatedDocument and apply for data access.
Define reporting relationships and related matters for NDSS personnel.PolicyEpidemiological/ Policy/Administrative
Define target audiences for surveillance data. Epidemiology/ Policy/ Administrative
Appendix A
46
2 if possible; retention allows for analysis of diabetic populations for longitudinal analysis.
3 if possible; retention allows for analysis of non-diabetic populations for longitudinal analysis.

Activity Description Suggested Skill Set
B. Expanded Model Activities
InputsIntegrate records for years not incorporated into Activity A. SAS/systems analysis
Process(B2.1) Transfer data from existing hardware to NDSS hardware/disk space.
(B2.2) Reduce data from (B2.1) to include only necessary variables andnecessary records.
(B2.3) Concurrent with (B2.2) or subsequent to (B2.2) transform datafrom (B2.2) to NDSS common input data dictionary.
(B2.4) Read data from (B2.3) into SAS files.
(B2.5) Transform data from (B2.4) to calendar years.
(B2.6) Input data from (B2.5) into NDSS core software.
(B2.7) Produce “working” person-level summary.
SAS/systems analysis
Outputs(B2.8) Prepare aggregate data files to estimate incidence, prevalenceand mortality from (B2.7)
(B2.9) Prepare aggregate data files to estimate rates for specifiedcomplications and health services utilization patterns in subpopulationwith diabetes.
(B2.10) Prepare aggregate data files to estimate rates for specifiedcomplications and health services utilization patterns in subpopulationwithout diabetes.
Statistical analysis
(B2.11) Transfer aggregate datasets to Health Canada, as defined by FPTagreements.
(B2.12) Retain (B2.7) for diabetic populations.4
(B2.13) Retain (B2.7) for non-diabetic populations.5
SAS/systems analysis
(B2.14) Disseminate data products coordinated with NDSS SteeringCommittee on an annual basis.
Policy/communication-related
C. Alternative Model Activities
Description of alternative activities (where the NDSS Core Model is notfeasible) (2-3 pages)
Appendix A
47
4 if possible; retention allows for analysis of diabetic populations for longitudinal analysis.
5 if possible; retention allows for analysis of non-diabetic populations longitudinal analysis.

Funding Proposal 2000/01 Based onCapacity Assessment
Rationale
�Describe obstacles to carrying out NDSScore activities in your province/territory in2000-01.
� Attach previous three sections of capacityassessment.
Main goals for 2000-2001
� Summary of main activities and milestones.
Data/information products
� Items achievable before the end of the initialfunding period 2000-2001: incidence,prevalence, mortality (with and withoutdiabetes), complications (with and withoutdiabetes; specify conditions), health servicesutilization (with and without diabetes;specify measures).
Work plan
� For each activity listed within ActivityModules A, B, and/or C, indicate schedulewith approximate time frame.
Human resource requirements
� For each activity listed within ActivityModules A, B, and/or C, list staff members,anticipated full-time equivalent (FTE)allocation, skill set and annual FTE salary,assuming 20% benefits. Summarize thenumber of people (the number of total FTEsis expected to range between 0.5 and 2 butmay be distributed across the hiring of morethan 2 people at less than full-time hours),skill set, pay rate ($ per year plus %benefits), employment period (e.g. numberof months), number of FTEs, cost (salaryplus benefits).
Computer hardware
�Number of items and cost (attach quote) foreach of the following: servers, hard diskspace for existing devices, workstations,other
(see Addendum for guidelines)
Appendix A
48

Addendum
Funding Criteria
Objective: To build capacity in each province andterritory for the standardized surveillance ofdiabetes and its complications and for theproduction of nationally comparative data,primarily through the use of administrativedatabases where possible.
Initial funding period
April 1, 2000, to March 30, 2001
Criteria for funding allocations
NDSS funding will be allocated only to activitiesthat are directly related to the development ofsurveillance of diabetes and its complications,including policy-related activities.
A. Core Model Activities: Achievement of corefunctionality on an ongoing basis in allprovinces and territories is the priority forfederal funding in fiscal year (FY)2000/2001. It is recognized that achievingthis functionality involves bothdata-oriented tasks (such as assemblingand manipulating data) and policy-relatedtasks (such as the development ofsurveillance policies, reporting structures).6It is the responsibility of the province orterritory to prioritize data-oriented versuspolicy-related activities.
B. Expanded Model Activities: Where federaldollars are available and where ongoingfunctionality is established in a province orterritory, the integration of records for yearsnot incorporated into Activity A should beundertaken, if feasible.
C. Alternative Model Activities: Alternatives tothe core model, where core functionality isnot feasible in a province or territory, will beassessed and funded by the SteeringCommittee to the extent to which suchalternatives allow the production ofnationally comparative data.
If a province/territory has not yet fully completedActivity A but wishes to proceed to Activity B, itshould provide a rationale to the SteeringCommittee as part of the proposal, explainingwhy the completion of a particular model is notfeasible, needs to be postponed, or should becompleted concurrently with some other stage.
Enhancements to the core model will not formpart of this proposal, but proposals forenhancements can be submitted at this time andwill be forwarded to the appropriate NDSSworking group(s) for consideration.
Appendix A
49
6 It is expected that the core model may evolve and be redefined by the NDSS Steering Committee over time (in subsequentfunding periods) as provincial/territorial capacities improve.

Suggested parameters for funding allocations
Each province and territory should receive a baselevel of funding to maintain the ongoing capacitynecessary to generate nationally comparativedata. The suggested base level of funding is for aminimum of 0.5 FTEs per province or territory,and for hardware requirements commensuratewith the information processing task in eachprovince or territory.7
The total number of FTEs per province/territory isexpected to be capped at 2 FTE’s. Anyrecommendation over and above that amountwill require substantial justification and will bedependent on allocations from the SteeringCommittee and funding availability.
The estimated pay rate per year for personnelwith the relevant skill sets is approximately$50,000 per year plus 20% benefits, as per theNDSS Business Plan.
Submission guidelines
Each province and territory may submit aproposal for NDSS funding for the initial NDSSfunding period. Proposals should employ thetemplate provided at the Winnipeg workshop.
Deadlines
Proposals are due on January 28th, 2000.Applications should be forwarded electronicallyto Rob James (NDSS Technical Director) andSheila Chapman, Health Canada.
Funding decisions
Applications will be reviewed by the Secretariat inearly February 2000, with final allocationdecisions determined by the Steering Committeein early March 2000.
Special Projects (optional): ProposedEnhancements to the Core Model
Outline the proposed enhancement(s), indicatinghow it (they) will complement core NDSSactivities in the province/territory and whetherthere is an opportunity for a multi-jurisdictionalcollaboration now or in the future.
Note: These special projects will be circulated tothe appropriate subcommittee/technical workinggroup and considered separately from the fundingstream for implementation of core NDSSfunctionality. An appropriate subcommittee/working group will request further details. DoNOT expect funding for special projects to beavailable on April 1, 2000/01.
Provide brief description of the project (includeactivities, methodology, outputs).
Provide resource request (specify how theseresources will be used).
Appendix A
50
7 Thus, provinces with larger populations are likely to legitimately require more computing hardware to store and manipulate theirdata files.

Guidance on Computer HardwareRequirements
Principles
� establish a “floor”, which is provided to all
� need clear growth pathway for all hardware
�will fund hardware differentially based onpopulation size
� address questions about moving from testsite in 2000/01 to operational site in sub-sequent years
�must fit within existing computer procure-ment rules (if any) in P/T
Operating systems
� should run SAS version 8 eventually
� strongly prefer (not ranked): NT (SP 6;Windows 2000; UNIX)
� should support multi-processor hardware
� need ability to have multiple disk drives actas if one directory/drive
Base model (not required, but stronglyrecommended)
� INTEL BX chipset motherboard, i.e. 100Mhz FSB
� Pentium III CPU (supports 100 MHFSB)
� 100 Mhz RAM (PC-100) in 128 MB DIMMs
�RAM upgradable to 1 GIG (except for basesystems)
�Wide-SCSI hard drives
Security and communication
� Can data reside on work-station?
�Does data have to reside in secure room?
�What speed network do you maintain?
Upgrading and performance
Tentative benchmark for performance:
� should be able to re-assemble AnnualPerson-level Summary Files (APLSF) for 10years over one weekend, without attention
� should be able to obtain simple estimatesfrom 1 APLSF within 1 hour, e.g.prevalence, mortality
If proposed capacity does not performreasonably, P/T can apply back to NDSS SteeringCommittee to move up.
Maintenance, backups, etc.
� get 3-year maintenance contract
� define a strategy for backing up data
Appendix A
51

Appendix B
Regional Activity
Most provinces/territories have built upon thesurveillance capacity demonstrated by NDSS.The relation between diabetes and other chronicdiseases has stimulated interest in chronicdisease surveillance in general.
Yukon
� provided 1995/96 to 1999/00 data toHealth Canada;
� investigating possible expansions of the coreNDSS model to include other databases,such as the Diabetes Education Centre andthe Seniors’ Pharmacare Program;
� has partnership with the Chronic DiseaseProgram, expansion of the NDSS model toinclude other co-morbidities, and increasedcapacity in epidemiology.
Northwest Territories
� provided 1995/96 to 1999/00 data toHealth Canada;
� discussions with NWT Dene Nationconcerning Aboriginal data;
� developing a Northwest Territories diabetesregistry in consultation with the threeDiabetes Education Programs inYellowknife, Inuvik and Hay River and withother stakeholders;
� developing a Northwest Territories diabetesstrategy.
Nunavut
� became a territory in 1999;
� completed data cleaning of health numbersintroduced in 1999 confounded with the oldNorthwest Territories health number;
� completed a retrospective Nunavutpopulation starting in 1995/96, using bothNunavut and Northwest Territories healthnumbers;
� implemented NDSS software on 1995/96 to1999/00 data;
� preliminary review necessitated expansion ofthe NDSS model to incorporate communityhealth nurse data, since these nursesprovide primary care for approximately 60%of the population;
� completed data entry and formatting to thepre-1999 community health nurse data, andthe paper records for 2000 and 2001;
� implementing expanded NDSS software.
British Columbia
� provided 1995/96 to 1999/00 data toHealth Canada;
�working with First Nations’ Chiefs HealthCommittee to identify Status Indianpopulation;
� provincial diabetes surveillance reportexpected later in 2003 that includes regionalmeasures (incidence, prevalence, mortality)for 16 health service delivery areas,
Appendix B
52

Pharmacare utilization, cost analysis, andprevalence projections;
� investigating possible expansions of the coreNDSS model to include other databases,such as Vital Statistics (deaths), Pharmanet(insulin and oral hypoglycemic use forpopulation), and the provincial renal agency;
� partnership with Chronic DiseaseManagement to provide chronic disease caremeasures for surveillance, and expansion ofthe NDSS model to include other chronicdiseases such as hypertension, ischemicheart disease, congestive heart failure, renaldisease, retinopathy, depression andasthma.
Alberta
� one of the original partners in the PrairiePilot;
� provided 1995/96 to 1999/00 data toHealth Canada;
� provincial diabetes surveillance reportexpected later in 2003 that includes regionalmeasures (prevalence, mortality) for ninehealth regions;
� possible expansion of the core NDSS modelto include other databases, such as VitalStatistics (deaths) and CCHS;
� partnership with patient health managementactivities and expansion of the NDSS modelto include other chronic diseases, such asheart disease, renal disease and retinopathy.
Saskatchewan
� one of the original partners in the PrairiePilot;
� provided 1995/96 to 1999/00 data toHealth Canada;
�NDSS has also been used for ongoingdiabetes program planning and evaluation atprovincial and regional levels. NDSS will beincorporated into program planning andevaluation in primary care services;
�work under way to produce costs and burdenof illness estimates for major causes ofmorbidity and mortality, expected later in2003.
Manitoba
� one of the original partners in the PrairiePilot;
� provided 1995/96 to 1999/00 data toHealth Canada;
� the NDSS model as initially developed inManitoba was used to produce 11 regionaldiabetes profiles, including incidence,prevalence and major complications, as wellas data to support the provincial diabetesstrategy,8 diabetes projections,9 and a Métishealth report;10
� provincial First Nations diabetes profileexpected later in 2003 will be available at:www.gov.mb.ca/health/publichealth/diabetes/index.html
Appendix B
53
8 Diabetes: a Manitoba strategy. 1998. Available at: www.gov.mb.ca/health/documents
9 Epidemiologic projections of diabetes and its complications: “Forecasting the coming storm”. 1999. Available at:www.gov.mb.ca/health/documents
10 The health of Manitoba’s Métis population and their utilization of medical services: a pilot study. May 2002. Available at:www.gov.mb.ca/health/documents

� collaboration with medical experts in theareas of dialysis, peripheral arterial diseaseand eye disease resulted in case definitionsfor these complications.
Ontario
� provided 1995/96 to 1999/00 data toHealth Canada;
� a modified NDSS model was used by theInstitute for Clinical Evaluative Sciences (ICES)to publish regional diabetes profiles;11
�NDSS has contributed toward increasing theprofile of diabetes in Ontario, includingdiabetes research at ICES.
Quebec
� provided 1995/96 to 1999/00 data toHealth Canada;
�working with the Cree Board of Health andSocial Services of James Bay on a diabetessurveillance project;
� the NDSS model was used in October 2002to produce diabetes prevalence data byhealth region;12
�NDSS has served as a catalyst for otherdiabetes research;
� expanding model to include vital statisticsand drug data from the Régie de l’assurancemaladie du Québec.
New Brunswick
� provided 1995/96 to 1999/00 data toHealth Canada in May 2003;
� physician data did not include diagnosticcodes used by other provinces. This requiredpre- liminary work to develop algorithms tosearch a text field for key words in Englishand French.
Prince Edward Island
� provided 1995/96 to 1999/00 data toHealth Canada;
�NDSS methodology was used to describediabetes prevalence by health region withinPrince Edward Island13;
� investigating possible expansion of the coreNDSS model to include other databases,such as laboratory testing, diabetes programand CCHS;
� use of the NDSS model to evaluate PrinceEdward Island’s Strategy for Healthy Living,a collaborative effort to address common riskfactors for chronic disease.
Appendix B
54
11 Diabetes in Ontario: an ICES practice atlas. 2003. Available at URL: www.ICES.on.ca
12 Institut national de santé publique. Prévalence du diabète au Québec et dans ses régions : premières estimations d’après lesfichiers administratifs. Octobre 2002. Brochure available on the INSPQ website: www.inspq.qc.ca
13 Van Til L. Prince Edward Island Health indicators, provincial and regional. Charlottetown: Document Publishing Centre, January2003. Available at: www.gov.pe.ca

Nova Scotia
� provided 1995/96 to 1999/00 data toHealth Canada;
� provincial diabetes surveillance reportexpected later in 2003 that includes regionalmeasures (prevalence, mortality) for ninedistrict health authorities as well as healthcare utilization (hospitalization rate, lengthof stay, and burden of disease). Thesereports will be posted on the web withsecure access;
� investigating possible expansion of the coreNDSS model to include other databases,such as the Diabetes Care Program andReproductive Care Program;
�NDSS has served as a catalyst for otherresearch activities such as the newly formedMaternal/Infant/ Diabetes Research Group,and validation of diabetes in people underthe age of 20.
Newfoundland and Labrador
� data not yet provided to Health Canada;
� partnership with the Department of Healthand Community Services and theNewfoundland and Labrador Centre forHealth Information;
�NDSS software currently being implementedusing data from 1995/96 to 1999/00;
� quality of registry information and thepotential use of census data are beingevaluated.
Appendix B
55

Appendix C
NDSS Steering Committee Membership 2003
Chair: Linda Van Til, Prince Edward Island Department of Health and Social ServicesAboriginal Groups
Aboriginal Diabetes Working GroupCongress of Aboriginal PeoplesHealth Secretariat - Assembly of First NationsInuit Tapiriit KanatamiMétis National CouncilNational Aboriginal Diabetes Association
Rhea JosephJudy Chapman-PriceAnita StevensOnalee RandellDon FiddlerCatherine Cook
Academics/Clinicians
McMaster University Hertzel Gerstein
Federal Government
Health Canada - First Nations and Inuit Health BranchHealth Canada - Population and Public Health BranchStatistics Canada
Adam ProbertClarence Clottey, Yang MaoGary Catlin
Non-Government Organizations
Canadian Diabetes AssociationCanadian Institute for Health InformationCanadian Institutes of Health Research - Institute of Nutrition, Metabolism & Diabetes
Donna LillieIndra PulcinsDiane T. Finegood
Provinces/Territories
YukonNorthwest TerritoriesNunavutBritish ColumbiaAlbertaSaskatchewanManitobaOntarioQuebecNew BrunswickPrince Edward IslandNova ScotiaNewfoundland and Labrador
Joy KajiwaraJohn MorseSylvia HealeyKim ReimerLarry SvensonWilliam OseiKelly McQuillenJoan CanavanDanielle St-LaurentChristofer BalramLinda Van TilPeggy DunbarFaith Stratton
Sponsor (observer status)
GlaxoSmithKline Raymond Fox
Past Chairs include Wilson Rodger and Bernard Zinman.
Note: The report editor for the 2003 NDSS Report was Shirley Huchcroft.
Appendix C
56

Appendix D
57

Validation Working Group
Chair: Valérie Émond, Institut national de santé publique du QuébecMunaza Chaudhry, British Columbia Ministry of Health PlanningJane Griffith, Manitoba HealthJan Hux, Ontario - Institute for Clinical Evaluative SciencesWilliam Osei, Saskatchewan HealthKim Reimer, British Columbia Ministry of Health PlanningMark Smith, Nova Scotia - Population Health Research Unit, Dalhousie UniversityLarry Svenson, Alberta Health and WellnessLinda Van Til, Prince Edward Island Department of Health and Social ServicesGlenn Robbins, Health CanadaRebecca Stuart, Health Canada
Past Chairs: Jamie Blanchard, Larry Svenson
Scientific Working Group
Co-chairs: Diane T. Finegood, Canadian Institutes of Health Research, INMDLarry Svenson, Alberta Health and Wellness
Gary Catlin, Statistics CanadaHertzel Gerstein, McMaster UniversityJan Hux, Ontario - Institute for Clinical Evaluative SciencesJeffrey A. Johnson, University of AlbertaWilliam Osei, Saskatchewan HealthIndra Pulcins, Canadian Institute for Health InformationDaniel Tessier, Université de SherbrookeEllen L. Toth, University of AlbertaLinda Van Til, Prince Edward Island Department of Health and Social ServicesJean-François Yale, Université de McGillChris Robinson, Health Canada
Technical Working Group
Chair: Glenn Robbins, Health CanadaMunaza Chaudhry, British Columbia Ministry of Health PlanningValérie Émond, Institut national de santé publique du QuébecJane Griffith, Manitoba HealthJan Hux, Ontario - Institute for Clinical Evaluative SciencesRob Ranger, Nova Scotia - Population Health Research UnitDeanna Rothwell, Ontario - Institute for Clinical Evaluative SciencesMark Smith, Nova Scotia - Population Health Research Unit
Appendix D
58

Larry Svenson, Alberta Health and WellnessLinda Van Til, Prince Edward Island Department of Health and Social ServicesAsako Gomi, Health CanadaChris Waters, Health Canada
Past Chair: Rob James
Technical Consultants
Chair: Glenn Robbins, Health CanadaSherri Wright, Yukon Department Health and Social ServicesJoyce Bourne, Northwest Territories Department Health and Social ServicesManon Asselin/Sylvia Healey, Nunavut Department Health and Social ServicesMunaza Chaudhry, British Columbia Ministry of Health PlanningKen Morrison, Alberta Health and WellnessJanice Hawkey, Saskatchewan HealthAndré Wajda, Manitoba HealthAlexander Kopp, Ontario -Institute for Clinical Evaluative SciencesValérie Émond, Institut national de santé publique du QuébecHeather MacLennan-Cormier/Jason Liu, New Brunswick Department of Health and WellnessConnie Cheverie, Prince Edward Island Department of Health and Social ServicesRob Ranger/Jill Casey, Nova Scotia - Population Health Research UnitKayla Gates/Don MacDonald, Newfoundland & Labrador Centre for Health InformationRhea Joseph, Aboriginal Diabetes Working Group
Appendix D
59

Appendix E
Memorandum of Understanding (MOU)
Between:
HER MAJESTY THE QUEEN in right of Canada, as represented by the Minister of Health (hereinafter referredto as “Health Canada”)
And:
HER MAJESTY THE QUEEN in right of the Province/Territory of _____________________________, asrepresented by the Minister of Health (hereinafter referred to as “X”)
1. General
1.1 Purpose of the Memorandum of Understanding
The purpose of this Memorandum of Understanding (MOU) is to confirm the participation andresponsibilities of parties in the National Diabetes Surveillance System (hereinafter referred to as the“NDSS”), regarding the development of provincial, territorial and federal capacity for standardizeddiabetes surveillance using primarily administrative data.
1.2 Objectives of the Memorandum of Understanding
The main objectives of the MOU are to:
1.2.1 provide for the establishment of personnel support for the NDSS in “X” to carry out approvedNDSS activities and to assist “X” in analyzing its own data.
1.2.2 obtain agreement in principle for the transfer of aggregate NDSS-related data from “X” to HealthCanada, subject to a written amendment to this MOU.
1.2.3 set out the terms and conditions for NDSS-related activities and financial administration of thisMOU.
1.3 Term of the Memorandum of Understanding
Subject to termination of this MOU, the term of this MOU shall be for a four-year period to commenceon April 1, 2000, (the “Effective Date”) and end on March 31, 2004, or such other date agreed uponin writing by the parties.
Appendix E
60

2. Context
Multi-Stakeholder Response to Lack of Diabetes Data
Diabetes has been recognized in recent years as a serious public health problem in this country.Diabetes prevention programs require a well-planned, organized and viable surveillance system.However, there is limited surveillance capacity for diabetes at all levels of public health in Canada,and to address this problem government and non-government sectors have collaborated on thedevelopment of the NDSS and participate on the NDSS Steering Committee to set policy and to directactivities.
The NDSS Steering Committee has representation from every province and territory, thenon-governmental sector, Aboriginal groups, academia, Health Canada, Canadian Institute for HealthInformation, and Statistics Canada. This Steering Committee is the main decision-making body of theNDSS and acts as the data gate-keeper. The Steering Committee meets twice yearly. To assist theSteering Committee, a multi-sectoral Secretariat provides ongoing management of the NDSS. Inaddition, two subcommittees and three expert technical working groups are responsible foraddressing key issues that have been identified by the NDSS Steering Committee.
Any private sector sponsors of the NDSS may have observer status on the Steering Committee but donot have voting rights.
Funding for the NDSS
Health Canada funding for the NDSS is through the Canadian Diabetes Strategy (CDS) over a five-yearperiod commencing in fiscal year 1999/2000, as approved by Federal Cabinet in November 1999and Treasury Board in February 2000.
NDSS: Development of Core Functionality in 2000/01
The main goals of the NDSS include the development and support in every province and territory andat the federal level of a core level of functionality with regard to standardized surveillance of diabetes.Another key goal of the NDSS, although outside the scope of this MOU, is the development andsupport for diabetes surveillance in the Aboriginal community.
The NDSS core data model relies on the utilization and record linkage of provincial and territorialhealth administrative data, beginning in the start-up year with linkage of health insurance coverage,physician claims, and hospitalization data sources to allow monitoring of diabetes incidence andprevalence, rates of diabetes complications, and levels of health care utilization in the population withdiabetes compared with the population without diabetes. In the core NDSS model, person level dataremain within provinces and territories, and only aggregate data on population groups will be sent toHealth Canada for a national picture of the diabetes burden.
Provincial and Territorial Capacity and Needs Assessments
In order to determine appropriate NDSS funding levels for fiscal year 2000/01, each province andterritory completed an assessment of its capacity to accomplish core NDSS functionality within thattime period. In some cases, a province or territory indicated that the core model was not possible in itsjurisdiction in fiscal year 2000/01 and proposed “alternative” activities that would move them towardcore functionality in subsequent years.
Appendix E
61

Provinces and territories also indicated in their submissions their personnel and technical resourceneeds in fiscal year 2000/01 to accomplish NDSS-related activities. These resource requests wereassessed and in some cases revised by the NDSS Secretariat, and allocations were approved by theNDSS Steering Committee in March 2000.
This MOU pertains to approved funding allocations for NDSS personnel resources in “X”. Approvedallocations for technical resources to each province and territory will be handled through a non-federalfinancing mechanism and source.
The understanding is that NDSS core surveillance activities conducted in fiscal year 2000/01 in aprovince or territory will be carried out on an annual basis and will form the main component of theongoing functioning of the NDSS. In the case of provinces or territories that will be engaging inalternative activities in fiscal year 2000/01 because of particular challenges in those jurisdictions, theunderstanding is that they will be moving toward implementation of core NDSS functionality insubsequent years.
4. Responsibilities of Parties
4.1 Health Canada agrees to pay to “X” on an annual basis an amount not to exceed the amount asindicated in Appendix A, subject to annual review and adjustment by the NDSS Steering Committee.
4.2 The payment is to be used to reimburse the cost of hiring or otherwise engaging personnel toaccomplish NDSS-approved activities. Nothing in this agreement should be construed as establishingan employer/ employee relationship between Health Canada and any personnel hired pursuant to thisagreement.
4.3 “X” is responsible for submitting resource allocation information for each subsequent year to theNDSS Steering Committee on or before December 31 of the current fiscal year. The NDSS SteeringCommittee will review and approve or adjust the resource allocation on or before January 31 of eachyear.
4.4 “X” agrees to provide in kind resources to the NDSS as needed. These resources are expected toinclude, but may not be limited to, the provision of data for NDSS activities, monitoring ofNDSS-related personnel in “X”, infrastructure support of NDSS-related personnel, and participation onNDSS committees and working groups as appropriate.
4.5 Health Canada agrees to provide in kind resources as needed to nationally coordinate NDSSactivities, to include (but may not be limited to) monitoring of national NDSS-related staff,infrastructure support of national NDSS-related personnel, and participation on NDSS committeesand working groups as appropriate.
5. Activities of Parties
5.1 “X” will engage in NDSS-approved activities as set out in Appendix B, subject to writtenamendments agreed to by both parties and the NDSS Steering Committee.
5.2 Health Canada will provide a national coordination function for the NDSS, including administeringNDSS funding from federal sources on behalf of the NDSS Steering Committee.
5.3 Subject to a Provincial Privacy Impact Assessment being conducted where required and to thesuccessful completion of activities set out in item 5.1 where these involve “core” NDSS activities,
Appendix E
62

5.3.1 “X” agrees in principle to transfer aggregate (non-person-level, de-identified) data to HealthCanada, pending a written agreement between the parties specifying terms and conditions if requiredor under the auspices of related “X” policy and regulations, and
5.3.2 both parties agree that the proposed information to be transferred will not constitute personalhealth information under legislation that governs the collection, use and disclosure of personal healthinformation.
5.4 Subject to the successful completion of activities set out in item 5.1, both parties agree inprinciple to coordinate the publication and dissemination of information products directly resultingfrom NDSS activities, pending oral or written agreement by both parties and the NDSS SteeringCommittee regarding the content and schedule of information publication and dissemination.
6. Administration of Agreement
6.1 Both parties will formally participate on the NDSS Steering Committee, and will meet andcommunicate on an as-needed basis to collaboratively direct and monitor the activities set out in thisagreement.
7. Principles of Data Privacy, Access and Ownership
7.1 Data privacy standards as set out in all applicable provincial/territorial legislation and the federalPrivacy Act will be respected.
7.2 It is the intention of the parties to uphold the principle of public access to health information to thefullest extent expedient consistent with applicable provincial and federal legislation regarding dataprivacy and ownership.
8. Intellectual Property
8.1 Any intellectual products such as NDSS standardized statistical programs and analysis tools givento “X” to fulfill the activities set out in Appendix B are to be considered in the public domain. TheNDSS must be acknowledged in any publications arising from the use of these products.
8.2 Any innovations to the standardized NDSS intellectual products that are developed by “X” as wellas any information products developed from data for which “X” is the custodian remain the property of“X”.
9. Financial Administration
9.1 The parties accept accountability for demonstrating good management practices in financialplanning, expenditure control and reporting, according to generally accepted accounting practices.
9.2 Health Canada, on behalf of the NDSS Steering Committee, may commission audits of any or allNDSS-related financial records of “X” relating to the hiring of NDSS personnel to ensure that all NDSSfunds are expended in accordance with the terms of this MOU.
Appendix E
63

9.3 Health Canada will make payments on a quarterly basis to “X” pursuant to activities described inAppendix B. The payment will be made upon receipt of an invoice and presentation of evidence ofactivities completed and of any personnel hired or otherwise engaged for NDSS activities.
9.4 Invoices should include a forecast showing any budget adjustments required for the remainder ofthe fiscal year.
9.5 In the case of an approved adjustment to Health Canada’s annual payment to “X”, HealthCanada’s representative on the NDSS Steering Committee is responsible for informing the budget andplanning units of financial and corporate services within Health Canada in a timely fashion of theapproved adjustment in payment level.
10. Termination by Consent
The MOU may be terminated by the consent of either of the parties giving ninety (90) days’ notice inwriting to the other party.
11. Termination for Cause
11.1 If “X” fails to perform the activities set out in Appendix B to the satisfaction of the NDSS SteeringCommittee, Health Canada may terminate in whole or in part this MOU, including Health Canada’sobligation to make additional payments of NDSS funds to the other party for the remainder of theMOU.
11.2 If Health Canada fails to pay the amount at the level set out in Appendix A or at the approvedadjusted level pursuant to annual review by the NDSS Steering Committee, “X” may terminate inwhole or in part this MOU, including “X”’s obligation to perform the activities set out in Appendix B.
12. Amendments
This MOU will only be amended, in writing, by mutual consent of both parties.
13. Conflict of Interest
13.1 No member of the House of Commons shall be admitted to any share or part of this Agreementor to any benefit to arise therefrom.
13.2 It is a term of this Agreement that no former public office holder who is not in compliance withthe post-employment provisions of the Conflict of Interest and Post-Employment Code for PublicOffice Holders shall derive a direct benefit from this Agreement.
13.3 If the status of any party changes in any way that prejudices the project, such party shallpromptly inform the other parties.
Appendix E
64

14. Funding Changes
If Health Canada will be reducing or terminating the funding under the MOU because of changes orreduction in Health Canada funding for the NDSS, Health Canada shall give notice in writing to “X” asearly as possible. Health Canada will give “X” sixty (60) days’ notice in writing before reducing orterminating the funding, whether the funding change is to occur during or at the beginning of a fiscalyear. In case of such termination, Health Canada will pay “X” all outstanding amounts for activitiesperformed under this agreement.
15. Notice
Any notice or other communication required to be given or made under this MOU shall be in writingand shall be deemed to be sufficiently given if sent by registered mail, or by telegram, or by facsimile,or by delivery in person, to the other party at the following address(es).
If to Health Canada:NAME/TITLE/ORGANIZATION/ TEL/ FAX
If to “X”:NAME/TITLE/ORGANIZATION/ TEL/ FAX
AGREED to this ________ day of __________________, 2000For Health Canada:
Date _______________ _________________________________Signed on Behalf of Health Canada
Witness ________________________________
For “X”:
Date ______________ _________________________________Signed on Behalf of “X”
Witness __________________________________
Appendix E
65

Appendix F
NDSS Guidelines
Duality of Interest(Approved by NDSS Steering Committee
October 2, 2000)
The purpose of this policy is to assist the NDSSby providing duality of interest guidelines formembers of the Steering Committee.
A duality of interest may arise in two situations:(1) when a member has the opportunity toinfluence the business decisions of the SteeringCommittee in a way that could lead to personal,financial gain for the member or his/her family;and (2) when a member’s interests are contraryto the interests of the Steering Committee.
In order to avoid both the fact and theappearance of improper influence, a membershould not vote on, approve or recommendapproval of a transaction or contract with whichthe member is associated and should discloseany potential conflict prior to a vote or otheraction.
General principles regarding duties of members
�Members shall deliberate impartially on allissues placed before the SteeringCommittee.
�Members shall respect matters of aconfidential nature and shall not provideunauthorized information on these mattersto the media, the public or others.
Disclosure of duality of interest
�Disclosure of duality of interest shall be anagenda item for all meetings.
� A member shall, as soon as possible afterthe start of the meeting, disclose the natureof his/her duality of interest, and this shall berecorded in the minutes of the meeting.
Abstinence from action
�Members who are deemed to have afinancial conflict of interest position withreference to any item under discussionshould absent themselves from the meetingduring the period when such discussion istaking place.
�On the Steering Committee, only a singlerepresentative of each province, territory andorganization present shall vote on matterspertaining to contracts or transactions withthat province, territory or organization.
�On NDSS subcommittees or working groups,on which not all jurisdictions may berepresented equitably, members shallabstain from voting on contractual/transactional matters pertaining to their ownprovince, territory or organization.
Compliance
� After a member has disclosed the nature of apotential financial conflict of interest at thestart of the meeting, the existence of aconflict of interest will be determined by amajority vote of the Steering Committeemembers present, on a case-by-case basis.
� The Chairperson is responsible for ensuringthat all members comply with this policy.
Appendix F
66

� These principles shall be binding on allmembers of the Steering Committee, itssubcommittees and working groups.
Definitions
� “Steering Committee” is to be interpreted asthe National Diabetes Surveillance SystemSteering Committee.
� “Member” is to be interpreted as thedesignated representatives on the NationalDiabetes Surveillance System SteeringCommittee. A member may contributefunding to the National DiabetesSurveillance system and has votingprivileges.
Fund-Raising and Sponsorship(approved by NDSS Steering Committee
October 2, 2000)
The purpose of this policy is to assist the NDSSby providing principles for fund-raising andeligibility criteria for NDSS sponsors, and bydefining potential benefits to sponsors, includinga protocol for sponsors as observers at generalsessions of the Steering Committee.
Principles for fund-raising
� There must be an open and transparentprocess for the solicitation of funds wherebyall likely funders of the NDSS are informed ofthe opportunity to become a funder, and anybenefits accruing to the sponsors are publicknowledge and agreed to by the SteeringCommittee.
� There should be a diversity of fundingsources so that one funder does not haveundue control over the stability of NDSSfunds.
� Private funders should not interfere or bepromised influence regarding decisions andactivities of the Steering Committee.
� The Steering Committee should be informedof the willingness of a private company tobecome a sponsor of the NDSS.
�Draft funding agreements with potentialsponsors should be circulated to the SteeringCommittee for approval prior to signing.
� The Steering Committee must approve theacceptance of funding from any specifiedprivate source.
Eligibility criteria for sponsors
All prospective sponsors will be rated on thefollowing:
Interest: NDSS fits with corporate businessand/or funding priorities
Capacity: Declares the ability to contributesignificant dollars to this initiative eitherphilanthropically or otherwise
All the following criteria must be met by apotential sponsor:
� There must be a long-term financial commit-ment ( > 1 year) to the NDSS.
� It must be a substantial financialcontribution ( > $100,000 per year) to theNDSS.
� There must be no outstanding commercialmatters before an organization or theSteering Committee, which, in the opinion ofthe Steering Committee, gives theappearance of, if not the fact of, conflict ofinterest.
� The potential sponsor must accept the “noinfluence” stipulation in the affairs of theSteering Committee.
Appendix F
67

� There should be no inconsistency/incompatibility between the goals andobjectives of the NDSS and thegoals/products of the potential sponsor.
Potential benefits to sponsors
�Observer status at Steering Committeemeetings, in-camera sessions excluded
�Name acknowledgement on NDSS products
� Advance release of publicly distributedreports
Protocol for sponsors as observers at SteeringCommittee meetings
� Sponsors may attend Steering Committeemeetings as observers and may only speakby invitation of the Chair.
� Sponsors do not have voting authority atSteering Committee meetings.
� Sponsors may not attend in-camera sessionsof the Steering Committee.
� The Steering Committee should sendsponsors reports on an agreed-uponschedule regarding NDSS projectaccomplishments.
� Sponsors may be identified as such on NDSSproducts.
� As corporations wish to provide financialsupport to the NDSS, their relation with theSteering Committee as observers at SteeringCommittee meetings will be reviewed on acase-by-case basis.
Definitions
� “Steering Committee” is to be interpreted asthe NDSS Steering Committee.
� “Member” is to be interpreted as thedesignated representatives on the NDSS
Steering Committee. A member maycontribute funding to the NDSS and hasvoting privileges.
� “Sponsor” is to be interpreted as a privatefinancial contributor to the NDSS. A sponsoris not a designated member of the SteeringCommittee, does not have voting privileges,and may not attend in-camera sessions ofthe Steering Committee.
� “Confidential” is to be interpreted asmaterial that is so designated at a meeting,such as funding proposals, data results,business strategies, pricing information,financial data, research protocols andintellectual property.
� “No influence” is to be interpreted as notinterfering with or having influence overdecisions and activities of the SteeringCommittee.
Data Access and Publications(approved by NDSS Steering Committee
November 27, 2002)
The purpose of this policy is to promote thecredibility, usefulness and accountability of theNDSS by defining principles around which dataand products may be accessed from NDSS, howdata or products may be obtained, and thepublication thereof. This policy outlines theprocedures believed necessary to processresearch requests efficiently while ensuring bothconsideration of the public interest and fullcompliance with legislation.
This policy covers data that have been collected,linked and/or analyzed with the assistance ofNDSS resources. The audiences anticipated asusers of NDSS data are (although this does notpreclude others from requesting access, ifwarranted) as follows:
Appendix F
68

� parties engaged in predetermined NDSSprojects, outcomes or activities;
� parties engaged in independent research;
� other audiences such as media, othergovernment organizations, anddiabetes-related stakeholders, includingnon-governmental organizations and healthcare professionals, and the general public.
Nature of data and products that can beaccessed:
� unpublished NDSS aggregate data kept byHealth Canada;
� person-level data kept at provincial andterritorial sites (data from one specific sitemay be requested directly from thejurisdiction responsible for the data; thispolicy aims at coordinating multi-siterequests); and
�NDSS programming codes.
Guiding principles
� Provinces and territories must be inagreement with any and all uses (includingcollection, linkage, analysis, access, andpublication) of their respective provincialand territorial data within NDSS.
� This policy must comply with provincial,territorial and federal legislation and policiesregarding data access and protection ofprivacy, and comply with existingMemoranda of Understanding. Access toand dissemination of data fromprovincial/territorial NDSS data files mustcomply with provincial/territorial legislationand policy, and access to and dissemina-tion of Health Canada NDSS data files mustcomply with federal legislation and policy.
� Terms defining access to the NDSS datarelating to Aboriginal peoples on a nationallevel will be determined by the AboriginalDiabetes Working Group.
� In accordance with the Memorandum ofUnderstanding, any use of data that identifyspecific Aboriginal groups must have priorapproval of the signatories to theMemorandum of Understanding. Specialinstances outside the MOU will beconsidered on a case-by-case basis.
� Person-level data will remain within thecustody of the provincial/territorial NDSSdatafile.
� All parties recognize that nothing hereininterferes with provincial and territoriallegislated obligations to manage publichealth reporting in each jurisdiction orHealth Canada obligations as they relate toFirst Nations.
�NDSS statistics must be based oncomparable data derived from differentprovincial/ territorial data sets, must reflectconsistent approaches to data collection andmust lead to valid and reliableinterpretations. Should data not becompletely comparable, provinces andterritories will be requested to providetechnical notes, which will be forwardedwith any data requests and noted inpublications. The Technical Working Groupwill determine whether or not the data arecomparable.
Uses of NDSS data and products accessed
Data are provided for the exclusive purpose asstated in a proposal and may not be used for anyother purpose without the explicit writtenapproval, in advance, of the NDSS Data Accessand Publications Subcommittee. Authorized
Appendix F
69

users are prohibited from using NDSS data orproducts in the pursuit of any commercial orincome-generating venture. Any breach of theagreed upon terms may affect subsequent accessto data maintained by the NDSS. Also, other legalremedies are not precluded by any such action.The NDSS data and products thereof (e.g.computer software, analytical tools) remain in thepublic domain. Sharing of data with third partiesis prohibited without specific permission.
Ethical review for access
NDSS data should be used for scientificallysound, high-quality analyses, to supportacademic, policy, health economic or businessresearch. Proposals for research using NDSSdata must demonstrate acceptable rationale,analytical methods, and security/confidentialitysafeguards. All NDSS investigator-initiatedprojects requesting unpublished data mustreceive ethical approval from an ethics board thatcomplies with the “Tri-Council Policy Statement:Ethical Conduct for Research Involving Humans”before data are released.
Requirements to request access
� Proposals to access NDSS data held at aprovincial or territorial site will be submittedfor review to the relevant provincial orterritorial body with custody of the data.Where applicable, proposals to accessAboriginal data for a specific province orterritory will be submitted for review to theAboriginal partner as identified in the MOU.Provincial and/or territorial approval isrequired before data will be released, andsign off will occur within the jurisdiction.Aboriginal partner approval is requiredaccording to the conditions agreed by allparties.
� Proposals to access NDSS aggregate dataheld by Health Canada will be submitted for
review to Health Canada. Third party accesswill be reviewed on a case-by-case basis.The NDSS will be permitted to carry outon-site visits and other inspections to ensurecompliance with the conditions of access.All requests will be logged at Health Canada.
�Requests to access NDSS programmingcode will be logged at Health Canada toensure that sharing parties have the mostcurrent version of the code. The NDSSprogramming code is in the public domainand may be shared with requesting partieswith appropriate access to the technologyused.
All requests for data must be submitted in writingto the secretary of the Data Access andPublication Subcommittee and include thefollowing:
� the party requesting the data;
� the purpose of the project;
� the benefits of the project;
� the list of data being requested;
� the analysis to be performed;
� the nature and intent of any data linkages;
� any publications expected to result fromdata analysis and where and when they willbe distributed;
� the means by which the client will ensurethe security of the data;
� a description of how and when the data willbe disposed of or returned;
� the names and titles of all individuals whowill have access to the data;
� the complete document package submittedfor ethical review;
� the results of any ethical committee reviewof the project; and
Appendix F
70

� the source(s) of funding for the request andproposed analysis.
When a prospective user approaches the NDSS torequest access to data, the NDSS should forwardto the researchers a package containing aresearch application. Requests are to beaccompanied by a signed Non-DisclosureAgreement stating that the researcher agrees tocomply with NDSS policies respecting use anddisclosure of the data:
� to use the data only for the stated purpose;
� to make no attempt to link or otherwiseidentify a data subject other than asdivulged;
� to maintain the data’s electronic and/orphysical security and dispose of the data asspecified;
� to not disclose the data to others;
� to provide two advance copies of anypublication or report to the NDSS SteeringCommittee for review and comments. Thecopies will be kept confidential. This isintended to ensure that data are beinginterpreted accurately;
� to acknowledge NDSS as the data source inany publication or report and to state thatthe interpretation and conclusions containedin the publications or report do notnecessarily represent those of the NDSS,Health Canada, or any province or territory;
� to provide a copy of the final publication orreport to the NDSS.
All requests will be received and reviewed by thearea responsible for the data (i.e. Health Canada,province/territory) in accordance with the NDSSprinciples, policies and procedures for datadisclosure. The secretary of the Data Access andPublication Subcommittee (also an employee of
Health Canada) will be co-ordinating the processand collecting the necessary authorizations fromeach jurisdiction.
Decisions regarding NDSS unpublishedaggregate data will be made by the Data Accessand Publications Subcommittee and are subjectto the endorsement and approval of the NDSSSteering Committee.
Disclosure
Before release, reports containing any datarequested through the NDSS, or reportsgenerated using NDSS data, will be reviewed.The Data Access and PublicationSubcommittee’s review will ensure that privacystandards are complied with and that the correctdata are used and are not misrepresented. TheData Access and Publication Subcommittee willreceive a copy of every report before publication,at the same time as the NDSS partners or theNDSS Steering Committee, according to the ruleslisted below.
Parties engaged in independent research:
� The NDSS provides parties engaged inindependent research a right to publish,assuring the parties that once the use of thedata has been approved, no censure rightscan be applied by NDSS partners and nopublication can be suppressed because ofdifferences of interpretation or political con-sequences. However, NDSS partners,specifically those whose data contributed tothe research, may request a delay or specificprocess whereby they can review themanuscript to detect any error of fact. Theinterpretation and conclusions contained inthe publications or report may notnecessarily represent those of the NDSS,Health Canada, or any province or territory.
Appendix F
71

�Before being sent to publishers, manuscriptsfrom parties engaged in independentresearch, peer-reviewed or not, should besent to the Data Access and PublicationSubcommittee, and the Subcommittee willsend the manuscripts to provinces orterritories whose data contributed to theresearch for review. NDSS partners and DataAccess and Publication Subcommitteereviewers have two weeks upon receipt tomake recommendations for changes.
� Peer-reviewed or non-peer-reviewedmanuscripts must be sent to the DataAccess and Publications Subcommitteeonce they are accepted for publication (forinformation purposes and to facilitate acoordinated approach to publication ofNDSS data only, not to prevent publication).
When NDSS data are used for presentations andconference abstracts, the Data Access andPublication Subcommittee should be notified.
Protection of privacy and confidentiality
Privacy and confidentiality must be protected.Successful applicants must comply with theNDSS Privacy and Confidentiality Policy, whichdescribes detailed measures for ensuring theprotection of privacy and confidentiality of NDSSdata. Measures to be used include, but are notlimited to, checks for residual disclosure ofindividual identity prior to release of any reportsor aggregate data, and ensuring thatapproval/release of any person-level data (forexample, for research) is in accordance with thelegislation, polices and processes of theindividual organizations at the provincial andterritorial level where the data reside. It is aprovincial and territorial role to ensure adequatesecurity arrangements for all person-level data.
Destruction
Data files may be provided for a five-year timeperiod, following which the original data set andany copies thereof must be destroyed at thecompletion of the project or according to thesigned agreement destruction date or negotiateddata expiry date.
Penalties
Those who violate conditions for disclosure orwho misrepresent the nature of the data suppliedto them will be subject to sanctions, which mayinclude
� a written complaint to the sponsoringorganization;
� rebuttal in the journal;
� refusal of future access to data for theresearcher and/or the institution he/sherepresents;
� seizure of any data released by NDSS;and/or
� legal action.
Publication
� The NDSS Steering Committee willendeavour to publish on an annual basis areport with core epidemiological measuresfrom aggregate NDSS data at the HealthCanada site.
� The NDSS Steering Committee retainsauthority to approve publication of NDSSinformation by Health Canada.
� The NDSS Steering Committee permitsHealth Canada to release a public-use NDSSaggregate data file on its website afterapproval of the content of the data file by theSteering Committee and Aboriginal DiabetesWorking Group.
Appendix F
72

� The National Diabetes Surveillance Systemmust be credited as a contributor in anypublications arising from NDSS data atprovincial, territorial or Health Canada sitesor any other organization using NDSS data,and a disclaimer added that theinterpretation and conclusions contained inthe publications or report do not necessarilyrepresent those of the NDSS, HealthCanada, or any province or territory.
�Diabetes-related stakeholders not alreadyrepresented on the NDSS SteeringCommittee will be first in line for obtainingcopies of public-release annual NDSSreports, starting with the memberorganizations of the Diabetes Council ofCanada.
� The Data Access and PublicationsSubcommittee is responsible for submittingits publication plans (schedule and proposedcontent) to the Steering Committee forapproval each year. In addition, theSubcommittee will work to coordinatesimilar publications from provinces andterritories, as feasible and desired.
� Provinces and territories will continue topublish their own diabetes data at timesdictated by provincial/territorialrequirements.
Cost-recovery
� Cost-recovery fees for NDSS publicationsand for the provision of unpublished NDSSinformation or data files can be set at levelsto be determined by the governments wherethe NDSS data are kept. Health Canada willhave copies of aggregate data already held atrespective provincial/ territorial sites and willtherefore never charge a province or territoryfor a copy of its own data.
� The prospective user of data held by HealthCanada may be required to sign an“Agreement to Proceed with DataPreparation” form, which briefly outlines thesearch activity and the estimated costs, forwhich the user agrees to reimburse HealthCanada. For data at the provincial/territoriallevel, an individual province/territory mayhave its own agreement that the prospectiveuser may be required to sign.
Evaluation
� The NDSS Steering Committee will evaluatethe activities covered by this Data Accessand Publications Subcommittee as onecomponent of the overall evaluation of theNDSS. The Steering Committee will alsodetermine whether and to what extent thegeneral guiding principles of the NDSS havebeen followed; namely the principles ofconsistency, flexibility, quality, cost-effectiveness, accessibility, privacy andconfidentiality, and responsiveness.Measures to be used for this evaluation areto be determined and may includeconsistency in reporting on the samepopulation/area from different NDSS sites,flexibility in the range of themes addressedin special reports, quality of research fromNDSS aggregate data, the impact ofcost-recovery fees, rates of successfulrequests for NDSS aggregate data andinformation, absence of confidentialityleaks, and assessment of whether the NDSSis having an impact on research activity andis responding (e.g. in its special reports andenhanced analyses) to questions raised byresearch.
� The Access and Data Publication WorkingGroup should review this policy every twoyears.
Appendix F
73

Appendix G
Comparison of NDSS and Statistics Canada
Counts of Death and Population
Death Counts
Province/Territory Death Counts* and Ratio (%) 1995/1996 1996/1997 1997/1998 1998/1999
Yukon NDSSStatistics CanadaNDSS: Statistics Canada (%)
14915496.75
145139104.32
119111107.21
13013596.30
Northwest Territories NDSSStatistics CanadaNDSS: Statistics Canada (%)
238234101.71
27829095.86
260255101.96
27928797.21
British Columbia NDSSStatistics CanadaNDSS: Statistics Canada (%)
24,97126,618
93.81
26,32927,734
94.93
26,42327,750
95.22
25,17127,665
90.98
Alberta NDSSStatistics CanadaNDSS: Statistics Canada (%)
15,78915,906
99.26
16,37116,532
99.03
16,63716,819
98.92
15,92116,817
94.67
Saskatchewan NDSSStatistics CanadaNDSS: Statistics Canada (%)
8,5818,475
101.25
8,8968,845
100.58
8,7978,789
100.09
8,8928,893
99.99
Manitoba NDSSStatistics CanadaNDSS: Statistics Canada (%)
9,5879,555
100.33
9,6869,672
100.14
9,1909,569
96.04
9,8059,834
99.71
Ontario NDSSStatistics CanadaNDSS: Statistics Canada (%)
77,44677,977
99.32
79,29779,868
99.29
78,21680,292
97.41
76,11480,027
95.11
Prince Edward Island NDSSStatistics CanadaNDSS: Statistics Canada (%)
1,1711,172
99.91
1,2951,248
103.77
1,1151,076
103.62
1,1271,125
100.18
Nova Scotia NDSSStatistics CanadaNDSS: Statistics Canada (%)
8,0407,743
103.84
7,6557,850
97.52
7,9438,124
97.77
7,4107,739
95.75
*counts of deaths due to any cause, people aged 20+
Appendix G
74

Population Counts
Province/TerritoryPopulation Counts
(Ages 20+) and Estimates 1997/1998 1998/1999 1999/2000
Yukon NDSS annual countNDSS July countStatistics Canada July estimate
24,32022,43222,549
23,84621,86722,141
23,51421,60221,896
Northwest Territories NDSS annual countNDSS July countStatistics Canada July estimate
29,59327,44926,918
29,38127,20926,579
28,83726,77826,600
British Columbia NDSS annual countNDSS July countStatistics Canada July estimate
2,947,3632,518,8932,941,849
2,970,2432,568,3202,980,366
2,996,6662,588,3343,016,521
Alberta NDSS annual countNDSS July countStatistics Canada July estimate
2,074,9522,025,4702,004,598
2,130,0582,076,7412,062,669
2,172,8362,124,2412,110,691
Saskatchewan NDSS annual countNDSS July countStatistics Canada July estimate
738,042711,309712,441
745,309718,880717,473
752,753726,971721,810
Manitoba NDSS annual countNDSS July countStatistics Canada July estimate
847,294818,002812,180
848,247818,203815,330
852,112822,341820,391
Ontario NDSS annual countNDSS July countStatistics Canada July estimate
8,778,9478,509,4638,250,541
8,937,5078,683,0608,369,816
9,130,3088,872,1658,491,836
Prince Edward Island NDSS annual countNDSS July countStatistics Canada July estimate
105,04499,66997,837
104,340100,32398,436
105,019101,09499,602
Nova Scotia NDSS annual countNDSS July countStatistics Canada July estimate
716,220692,053691,021
722,403698,270695,177
731,016707,022700,854
Appendix G
75

Appendix H
Annual Person-level Summary File
(APLSF) Data Elements
Category Description Name
Demographic
Age as of March 31 of fiscal yearCalculated using the date of birth and year ending date
Personal lifetime identifierIdentifier that is unique to that person for perpetuity
Municipality or other geographic descriptor as defined by the province or territory (optional)Province or territorySexFiscal year to which data apply
AGE
ID
MUNPTSEXYEAR
Exposure
Person-days of observation with diabetes in current yearPerson-days of observation without diabetes in current yearPerson-days of observation
Total number of days person was eligible for health insurance in the province/territory within the current year
DM_PDODM_PDONPDO
Diabetes Case Ascertainment Information
Hospital discharge date where diabetes was recorded among the first three diagnosis codesDate of first diabetes diagnosis from physician data in current fiscal yearDate of second diabetes diagnosis from physician data in current fiscal yearDate of first diabetes diagnosis from physician data in previous fiscal year
D_DH3DD_DMD1D_DMD2DM_DMD1
Case Date
Perpetual diabetes case date DM_CASE
Complication/Co-morbidity Data
(NOTE: Other co-morbid conditions will be added as the case definitions are defined.)
Date of death DOD
Health Services Use
(NOTE: Other health services measures will be added as definitions are defined)
Treatment days – number of days admitted to hospital (not included in current data) TDAYS
History
Count of medical diagnoses in current yearMulti-year count of physician diagnosis of diabetesYear first observing ID/earliest NDSS year person was observed within NDSS, withinprovince/territoryThe fiscal year in which the person was given a diagnosis of diabetes within the NDSS
D_CMDDM_CMDFIRSTYR
DM_YRCCS
Note: Health Canada can provide access to a dummy file for researchers interested in testing SAS code.
Appendix H
76

Appendix I
Canadian Standard Population
Estimates — July 1, 1991
Sex Age Group Population Population Over Age 20 Proportion Over Age 20
Both 00-0910-1920-2930-3940-4950-5455-5960-6465-6970-7475-7980-8485+Total
3,906,3913,839,2054,638,6914,943,1613,813,0441,339,9021,238,4411,190,2171,084,588
834,024622,221382,303287,877
28,120,065
4,638,6914,943,1613,813,0441,339,9021,238,4411,190,2171,084,588
834,024622,221382,303287,877
20,374,469
0.227670.242620.187150.065760.060780.058420.053230.040930.030540.018760.01413
Female 00-0910-1920-2930-3940-4950-5455-5960-6465-6970-7475-7980-8485+Total
1,910,1641,873,1252,276,2392,467,2951,897,274
670,271620,986613,550588,370469,865365,286237,631198,419
14,188,475
2,276,2392,467,2951,897,274
670,271620,986613,550588,370469,865365,286237,631198,419
10,405,186
0.111720.12110.093120.03290.030480.030110.028880.023060.017930.011660.00974
Male 00-0910-1920-2930-3940-4950-5455-5960-6465-6970-7475-7980-8485+Total
2,006,7731,976,7342,343,7752,480,5461,917,714
676,641617,879580,323497,485362,500252,779139,40885,869
13,938,426
2,343,7752,480,5461,917,714
676,641617,879580,323497,485362,500252,779139,40885,869
9,954,919
0.115030.121750.094120.033210.030330.028480.024420.017790.012410.006840.00421
Appendix I
77

Appendix J
Validation Work
Diagnostic information provided byadministrative data is limited on the basis of asingle interaction with the health care system.NDSS uses a more elaborate algorithm that isbased on multiple interactions between theperson with diabetes and physicians andhospitals. Consequently, NDSS requires anarticulated case definition and ongoing validationof that definition. NDSS validation uses asystematic approach, with different aspects ofvalidation conducted in at least twoprovinces/territories to demonstrate potentialdifferences by jurisdiction.
Gold Standards and Jurisdictions
The case definition currently used by NDSS isbased on developmental work in Manitoba thatproduced sensitivity of over 95% (specificitycould not be assessed) using the gold standard ofthe Diabetes Education Resource1. Initialvalidation work in Alberta2 and Ontario3 used theNational Population Health Survey4 as the goldstandard. Both studies concluded thatself-reported survey data could not be used as agold standard, since they underestimate the truedisease burden in the population.
Other completed validation projects havesubstantiated the use of the NDSS algorithm.Studies in Nova Scotia,5 Ontario6 and PrinceEdward Island7 produced sensitivity measuresranging from 69% in Nova Scotia to 83% and86% in Prince Edward Island and Ontariorespectively. The gold standards were acombination of the provincial health survey andthe Diabetes Care Program Registry in NovaScotia, the diabetes registry in Prince EdwardIsland, and medical charts in Ontario.
In the same three studies, specificity measuresvaried much less, at 99% in Nova Scotia andPrince Edward Island and 97% in Ontario.Positive predictive value was 80% in Ontario and78% in Prince Edward Island.
Validation work is ongoing in other jurisdictions.In British Columbia, the gold standard is thenumber of prescriptions for insulin and oralhypoglycemic medication; in the Yukon it is useof the Diabetes Education Centres, and in Quebecthe use of clinical data.
Appendix J
78
�NDSS algorithm: a person is identifiedas having diabetes with one hospital ortwo physician visits within two yearscoded with a diagnosis of diabetesmellitus.
�Sensitivity: the proportion of people whotruly have diabetes who are identified bythe NDSS algorithm.
�Specificity: the proportion of people whotruly do not have diabetes who areclassified as such by the NDSSalgorithm.
�Positive Predictive Value: theprobability that a person identified by theNDSS algorithm as having diabetes trulydoes have diabetes. This is influenced bysensitivity, specificity, and prevalence.

Validity Over Time
The Prince Edward Island study found sensitivity,specificity and predictive value to be stable forfive to seven years of data for people aged 25 andover, and for a series of sequential five-year datawindows.7 With the use of 10 or more years ofadministrative data, specificity and positivepredictive value decreased as prevalent casesover-accumulated. Alternative algorithms areunder investigation in Nova Scotia to incorporatethe concept of cumulative probability of diabetes.
Incidence Versus Prevalence
New cases and prevalent cases are difficult todifferentiate in the early years.8 Several studiesfound at least five years of data are requiredbefore stable estimates of incidence can beobtained.7,9 Therefore incidence rates are notincluded in the first NDSS report.
Special Populations
Validation has not yet been completed for peopleunder the age of 20 years. Initial investigation ofseveral algorithms for type 1 diabetes hasproduced positive predictive values of less than40%.10 Prince Edward Island and Ontario arealso investigating several algorithms for detectingdiabetes among people under age 20, using thePrince Edward Island Diabetes Registry andhospital chart abstracts respectively.
Initial work in British Columbia and Ontariosuggests that the increase in female prevalenceseen during the child-bearing years may be theresult of miscoding of gestational diabetes. Oneproject funded by the Canadian Institutes ofHealth Research (CIHR) is validation of analgorithm for removal of gestational diabetesusing chart abstracts from maternity hospitals.
This project will also provide validation forindividuals under non fee-for-servicearrangements, using electronic patient recordsand drug claims data. Validation work inAboriginal communities will include use of theSandy Lake diabetes community screeningdatabase and Northern Diabetes Health Networkdatabase.
Complications
The complications of diabetes are also underinvestigation, with an initial focus onco-morbidities of cardiovascular disease,cerebrovascular disease, peripheral vasculardisease, including lower limb amputations,retinopathy and dialysis. Projects are under wayin Ontario,11 Quebec, Manitoba, and the Yukon.One of the CIHR-funded projects will describe thedistribution of co-morbid conditions andCharlson’s co-morbidity index12 among inpatientsusing the national Hospital Morbidity Datamaintained at the Canadian Institute for HealthInformation (CIHI) and the Person-OrientedInformation Database maintained at StatisticsCanada. The effect of co-morbid conditions onhospital stay, hospital readmission, and hospitalmortality will be assessed. The distribution ofco-morbid conditions in the general Canadianpopulation will be described using the 1996/97National Population Health Survey.
Health Service Use
Work is also planned for health service use. Theneed for accurate identification of people withand without diabetes will become increasinglyimportant as NDSS looks toward themanagement of diabetes.
Appendix J
79

New Initiatives with CIHR
Recently, the NDSS and the CIHR Institute ofNutrition, Metabolism and Diabetes collaboratedin funding health services and population healthresearch on diabetes. Each partner contributed$250,000 for a total of $500,000 in fundingavailable. A Request for Applications (RFA) wascalled in April 2002. Eligible research areas weredata validation (diabetes case definition, casedefinitions for complications related to diabetes,and community-based screening) and healthservices and population health research (qualityof life, access to diabetes-related health careservices, economic analysis of the burden ofdiabetes).
Seven applications were peer-reviewed by asix-person committee of Canadians andAmericans chaired by Dr. Sam Sheps from theUniversity of British Columbia. Two projects werefunded, and reports are expected by January2005:
� Validation of administrative data algorithmsfor diabetes surveillance in specialpopulations ($92,024) by J. Hux, G. Booth,A. Hanley, T. To, D. Daneman, H. Lee, D.Feig
� Evaluation of co-morbidities andcomplications in relation to hospitaloutcomes for diabetes among Canadianinpatients and general Canadianpopulations ($192,940) by Y. Chen, R.Sigal
References
1. Blanchard JF, Ludwig S, Wajda A, Dean H,Anderson K, Kendall O, Depew N. Incidenceand prevalence of diabetes in Manitoba,1986-1991. Diabetes Care1996;19:807-11.
2. Svenson L. Assessment of the sensitivityand specificity of Alberta Healthadministrative data for diabetessurveillance. Report to NDSS ValidationWorking Group. Edmonton: March 1999.
3. Hux JE. Using administrative data to definethe prevalence of diabetes mellitus inOntario. Report to NDSS ValidationWorking Group. Toronto: ICES, March1999.
4. Tamblay JL, Catlin G. Sample design of theNational Population Health Survey. HealthReports 1995;7:29-38
5. LeBlanc J, Kephart G. Assessment of thesensitivity and specificity of Nova Scotiaadministrative databases for detectingdiabetes mellitus. Report to NDSSValidation Working Group. Halifax:Population Health Research Unit, January1998.
6. Hux JE, Ivis F, Flintoft V, Bica A. Diabetes inOntario: determination of prevalence andincidence using a validated administrativedata algorithm. Diabetes Care 2002;25(3):512-6.
Appendix J
80

7. Van Til L. PEI Diabetes Validation Project,Report to NDSS Validation Working Group.Charlottetown: Document PublishingCentre, March 2001.
8. Young TK, Roos N, Hammerstrand MA.Estimated burden of diabetes mellitus inManitoba according to health insuranceclaims: a pilot study. Can Med Assoc J1991;144(3):318-324.
9. Noseworthy T, Blanchard J, Campbell D,Chapman S, Clottey C, James R, Osei W,Svenson L. Final report: demonstration ofthe proposed national diabetes surveillancesystem in the three Prairie provinces.Report to HISP. March 2001.
10. Clayton D, Smith M, Dunbar P, Salisbury S,Kephart G, LeBlanc J. Validity of theDiabetes Care Program of Nova Scotiadatabase of new cases (DNC) of diabetesaged < 19 years in determining theincidence of type 1 Diabetes Mellitus inthis population. Report to NDSS. Halifax:Validation Working Group, May 2000.
11. Diabetes in Ontario: an ICES practice atlas,2003. Available at URL: www.ICES.on.ca
12. Charlson M, Szatrowski TP, Peterson J, GoldJ. Validation of a combined comorbidityindex. J Clin Epidemiol 1994;47:1245-51.
Appendix J
81

Appendix K
Prevalence
Age-specific Prevalence by Fiscal Year, Sex and Province/Territory
Canada
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.7
14,8201,997,477
0.4
9,0412,024,463
0.8
16,4541,994,491
0.5
9,8062,023,346
0.9
17,4941,997,640
0.5
10,5622,029,248
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.4
35,1492,528,645
1.0
24,2722,544,838
1.6
40,6262,499,595
1.1
26,8762,515,198
1.8
45,4062,471,874
1.2
28,6832,490,412
40-49 Prevalence (%)
� People with diabetes
� Annual population count
2.2
49,6072,289,110
2.6
60,1602,289,206
2.4
56,7872,348,501
2.9
67,3382,349,403
2.6
62,6952,410,680
3.0
72,7852,412,997
50-54 Prevalence (%)
� People with diabetes
� Annual population count
4.1
36,708894,409
5.7
50,825898,957
4.5
42,145939,131
6.2
58,092939,131
4.7
46,566985,939
6.4
63,598987,280
55-59 Prevalence (%)
� People with diabetes
� Annual population count
6.0
41,374690,681
8.3
56,480684,001
6.5
46,626720,363
9.0
64,048714,799
6.8
50,981750,683
9.5
70,751746,490
60-64 Prevalence (%)
� People with diabetes
� Annual population count
8.1
48,840600,281
10.7
62,265579,751
8.9
54,002608,538
11.9
69,613586,737
9.3
57,623619,702
12.5
74,906597,864
65-69 Prevalence (%)
� People with diabetes
� Annual population count
10.2
58,906579,798
12.9
69,132535,662
11.0
63,593579,565
14.1
75,923539,503
11.5
66,893579,176
14.9
80,829540,838
70-74 Prevalence (%)
� People with diabetes
� Annual population count
11.7
61,870530,424
14.5
62,869433,241
12.7
67,535532,012
15.9
69,956441,247
13.5
71,814533,607
16.9
75,972449,917
75-79 Prevalence (%)
� People with diabetes
� Annual population count
12.1
52,132432,184
14.8
45,497306,934
13.2
59,504449,659
16.3
52,428321,181
14.2
65,349461,785
17.4
57,856331,731
80-84 Prevalence (%)
� People with diabetes
� Annual population count
11.6
34,280295,571
14.0
25,275180,014
12.8
38,247299,326
15.4
28,064182,152
13.7
42,119307,457
16.7
31,260187,627
85+ Prevalence (%)
� People with diabetes
� Annual population count
9.5
26,337276,946
11.5
14,213123,232
10.6
30,647290,099
12.8
16,685130,019
11.5
35,044305,043
13.8
18,956137,462
Total* Prevalence (%)
� People with diabetes
� Annual population count
4.1
460,02311,115,526
4.5
480,02910,600,299
4.6
516,16611,261,280
5.0
538,82910,745,676
4.9
561,98411,423,586
5.4
586,15810,911,866
CanadianTotal
� People with diabetes** 479,346 500,193 537,848 561,463 585,590 610,780
* for participating jurisdictions** estimated using NDSS prevalence and adjusting for 4.2% of Canadian population in New Brunswick and Newfoundland andLabrador (2001 census)
Appendix K
82

Age-specific Prevalence by Fiscal Year and Sex
Yukon Territory
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.9
232,495
0.4
92,468
1.2
282,384
0.5
122,263
1.1
252,292
0.6
122,117
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.0
343,347
0.6
213,292
1.3
413,198
0.7
203,056
1.4
443,060
0.7
212,830
40-49 Prevalence (%)
� People with diabetes
� Annual population count
1.7
523,062
1.5
513,386
1.9
593,110
1.7
583,318
1.9
603,134
1.7
543,267
50-54 Prevalence (%)
� People with diabetes
� Annual population count
3.9
38985
4.9
621,273
4.5
471,036
5.0
651,295
4.6
511,111
5.2
671,299
55-59 Prevalence (%)
� People with diabetes
� Annual population count
4.8
28582
6.4
52817
4.5
28618
6.2
53851
5.7
37647
6.0
55922
60-64 Prevalence (%)
� People with diabetes
� Annual population count
7.5
31413
5.7
30527
10.4
43414
7.2
39542
10.0
42421
8.5
48567
65-69 Prevalence (%)
� People with diabetes
� Annual population count
9.3
28300
11.2
47421
7.0
21300
10.9
46422
8.1
26322
10.1
43424
70-74 Prevalence (%)
� People with diabetes
� Annual population count
7.3
14192
10.6
25236
14.1
27191
12.2
33270
17.2
35203
14.7
43293
75-79 Prevalence (%)
� People with diabetes
� Annual population count
12.1
17140
9.8
13133
9.7
15155
7.9
11140
9.3
14151
10.7
16150
80+ Prevalence (%)
� People with diabetes
� Annual population count
6.1
9148
9.7
10103
7.6
13170
10.6
12113
9.4
17181
14.6
18123
Total Prevalence (%)
� People with diabetes
� Annual population count
2.3
27411,664
2.5
32012,656
2.8
32211,576
2.8
34912,270
3.0
35111,522
3.1
37711,992
Appendix K
83

Age-specific Prevalence by Fiscal Year and Sex
Northwest Territories
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.3
123,843
0.3
113,764
0.2
93,659
0.4
143,639
0.3
103,525
0.4
143,460
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.0
424,384
0.8
384,524
1.1
464,263
0.9
394,339
1.0
424,107
0.9
384,149
40-49 Prevalence (%)
� People with diabetes
� Annual population count
2.4
753,175
2.3
803,550
2.5
803,251
2.8
1043,664
2.4
773,236
3.0
1083,644
50-54 Prevalence (%)
� People with diabetes
� Annual population count
4.1
39961
5.3
681,272
5.5
551,002
5.3
701,320
6.1
661,074
5.6
781,381
55-59 Prevalence (%)
� People with diabetes
� Annual population count
6.2
40646
6.9
54786
6.5
43658
8.6
71822
7.0
46660
9.2
76829
60-64 Prevalence (%)
� People with diabetes
� Annual population count
6.2
25405
9.1
47515
7.5
32424
8.9
47526
7.9
34432
11.1
57512
65-69 Prevalence (%)
� People with diabetes
� Annual population count
9.2
27292
7.3
28382
8.0
25311
10.2
39384
8.7
28321
13.7
54395
70-74 Prevalence (%)
� People with diabetes
� Annual population count
12.0
26216
9.7
23237
14.6
31212
9.3
24257
13.6
29214
8.8
23261
75-79 Prevalence (%)
� People with diabetes
� Annual population count
9.6
13136
4.1
6147
9.2
14153
6.5
9139
12.6
20159
8.0
11137
80+ Prevalence (%)
� People with diabetes
� Annual population count
11.7
23197
4.3
7161
11.4
22193
4.8
8165
11.7
21179
6.2
10162
Total Prevalence (%)
� People with diabetes
� Annual population count
2.3
32214,255
2.4
36215,338
2.5
35714,126
2.8
42515,255
2.7
37313,907
3.1
46914,930
Appendix K
84

Age-specific Prevalence by Fiscal Year and Sex
Nunavut
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.2
53,068
0.1
42,994
0.3
82,978
0.2
52,953
0.2
72,965
0.2
72,899
30-39 Prevalence (%)
� People with diabetes
� Annual population count
0.4
122,726
0.2
62,913
0.5
132,887
0.3
93,011
0.6
172,967
0.4
123,113
40-49 Prevalence (%)
� People with diabetes
� Annual population count
0.9
141,523
0.8
161,894
1.1
171,588
1.0
201,926
0.8
131,678
1.2
252,008
50-54 Prevalence (%)
� People with diabetes
� Annual population count
0.9
5555
1.6
11689
1.4
8582
2.1
16761
2.2
14624
2.3
18797
55-59 Prevalence (%)
� People with diabetes
� Annual population count
1.8
7396
2.6
12454
1.4
6435
3.0
15495
2.0
9441
4.0
21525
60-64 Prevalence (%)
� People with diabetes
� Annual population count
1.8
5282
2.5
8325
2.3
7309
3.2
11342
3.3
11338
4.7
18384
65-69 Prevalence (%)
� People with diabetes
� Annual population count
1.7
3174
4.4
8182
1.7
3181
3.3
7209
2.9
6208
3.3
8239
70+ Prevalence (%)
� People with diabetes
� Annual population count
–
–207
–
–261
–
–236
–
–293
–
–266
–
–318
Total Prevalence (%)
� People with diabetes
� Annual population count
0.6
548,931
0.7
699,712
0.8
699,196
0.9
899,990
0.9
859,487
1.1
11610,283
Appendix K
85

Age-specific Prevalence by Fiscal Year and Sex
British Columbia
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.7
1,933270,437
0.4
1,133259,333
0.8
2,132265,240
0.5
1,173253,392
0.8
2,182259,727
0.5
1,187249,203
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.4
4,699336,203
0.9
2,922326,758
1.6
5,412330,789
1.0
3,200320,456
1.8
6,000325,439
1.0
3,302315,659
40-49 Prevalence (%)
� People with diabetes
� Annual population count
1.9
6,187320,842
2.4
7,653318,016
2.2
7,126327,697
2.6
8,502322,650
2.3
7,779333,202
2.7
8,974326,834
50-54 Prevalence (%)
� People with diabetes
� Annual population count
3.7
4,572122,324
4.9
6,195125,209
4.1
5,307129,066
5.5
7,183131,339
4.3
5,827136,696
5.7
7,857138,518
55-59 Prevalence (%)
� People with diabetes
� Annual population count
5.6
5,21393,051
7.6
7,19494,513
6.0
5,83797,474
8.2
8,09698,937
6.3
6,368101,746
8.6
8,877103,361
60-64 Prevalence (%)
� People with diabetes
� Annual population count
7.5
5,96579,218
10.1
8,03779,842
8.2
6,67180,861
11.1
8,99881,131
8.6
7,10282,776
11.6
9,60182,649
65-69 Prevalence (%)
� People with diabetes
� Annual population count
9.3
7,07375,947
12.0
9,02675,272
10.1
7,70175,881
13.3
10,06575,544
10.7
8,10875,645
14.1
10,67575,715
70-74 Prevalence (%)
� People with diabetes
� Annual population count
10.4
7,42171,069
13.0
8,04161,627
11.5
8,16470,726
14.4
9,03362,561
12.3
8,69370,888
15.3
9,79463,989
75-79 Prevalence (%)
� People with diabetes
� Annual population count
10.4
6,40261,812
13.3
6,19646,485
11.4
7,31064,063
14.7
7,18048,745
12.4
8,05064,924
15.8
7,83149,604
80-84 Prevalence (%)
� People with diabetes
� Annual population count
9.7
4,13342,815
12.8
3,63128,376
10.9
4,69543,233
14.1
4,01328,460
11.6
5,12944,404
15.2
4,48729,452
85+ Prevalence (%)
� People with diabetes
� Annual population count
7.8
3,02238,534
10.5
2,05919,680
8.6
3,52140,953
11.6
2,43921,045
9.4
4,11843,743
12.7
2,85122,492
Total Prevalence (%)
� People with diabetes
� Annual population count
3.7
56,6201,512,252
4.3
62,0871,435,111
4.2
63,8761,525,983
4.8
69,8821,444,260
4.5
69,3561,539,190
5.2
75,4361,457,476
Appendix K
86

Age-specific Prevalence by Fiscal Year and Sex
Alberta
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.7
1,435211,313
0.4
899214,861
0.7
1,506217,036
0.4
997221,584
0.7
1,531219,957
0.5
1,067224,898
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.3
3,345255,273
0.8
1,990254,359
1.5
3,796253,954
0.9
2,278253,221
1.6
4,072251,360
1.0
2,464250,403
40-49 Prevalence (%)
� People with diabetes
� Annual population count
1.9
4,212224,025
2.2
5,060232,598
2.1
4,895233,818
2.4
5,759242,682
2.3
5,464242,758
2.5
6,275251,586
50-54 Prevalence (%)
� People with diabetes
� Annual population count
3.5
2,81579,535
4.8
3,90181,890
3.8
3,24184,473
5.3
4,63386,827
4.1
3,66889,716
5.5
5,07592,439
55-59 Prevalence (%)
� People with diabetes
� Annual population count
5.2
3,07259,178
7.1
4,30860,619
5.7
3,51862,129
7.7
4,91963,743
5.9
3,85265,020
8.3
5,53766,879
60-64 Prevalence (%)
� People with diabetes
� Annual population count
6.9
3,44150,135
9.1
4,59250,528
7.4
3,78251,347
10.2
5,23551,384
7.9
4,11252,368
10.8
5,67252,511
65-69 Prevalence (%)
� People with diabetes
� Annual population count
8.7
4,06946,741
10.9
5,00645,919
9.5
4,47847,037
12.0
5,60746,586
9.8
4,62247,349
12.7
5,95546,915
70-74 Prevalence (%)
� People with diabetes
� Annual population count
9.8
3,99940,647
12.6
4,46535,539
10.8
4,44441,314
13.7
5,04236,798
11.4
4,78841,923
14.5
5,51438,057
75-79 Prevalence (%)
� People with diabetes
� Annual population count
10.0
3,39134,051
12.8
3,25925,392
11.1
3,90435,198
14.2
3,74826,371
11.8
4,20835,524
15.4
4,14526,890
80-84 Prevalence (%)
� People with diabetes
� Annual population count
9.7
2,29923,631
12.4
1,88715,181
10.5
2,52524,030
13.8
2,13715,534
11.3
2,78224,651
14.7
2,33215,816
85+ Prevalence (%)
� People with diabetes
� Annual population count
8.4
1,87822,468
10.7
1,18211,069
9.3
2,19423,599
11.7
1,33411,393
10.1
2,45424,250
13.1
1,51711,566
Total Prevalence (%)
� People with diabetes
� Annual population count
3.2
33,9561,046,997
3.6
36,5491,027,955
3.6
38,2831,073,935
3.9
41,6891,056,123
3.8
41,5531,094,876
4.2
45,5531,077,960
Appendix K
87

Age-specific Prevalence by Fiscal Year and Sex
Saskatchewan
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.7
51470,067
0.5
36073,352
0.8
55770,732
0.5
37874,573
0.8
57471,723
0.5
41075,634
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.3
1,03978,278
1.0
81878,569
1.5
1,14076,710
1.2
92877,495
1.6
1,22074,991
1.3
96875,994
40-49 Prevalence (%)
� People with diabetes
� Annual population count
2.5
1,80471,597
2.7
1,99874,458
2.7
2,01873,739
3.0
2,26676,556
2.8
2,13175,911
3.0
2,37078,590
50-54 Prevalence (%)
� People with diabetes
� Annual population count
4.5
1,18026,197
5.7
1,55627,120
4.8
1,32727,554
6.2
1,77128,410
4.8
1,40028,969
6.3
1,90229,979
55-59 Prevalence (%)
� People with diabetes
� Annual population count
6.2
1,34921,720
8.0
1,72621,592
6.6
1,47622,220
8.8
1,95022,283
6.9
1,56122,670
9.0
2,06522,912
60-64 Prevalence (%)
� People with diabetes
� Annual population count
7.6
1,53520,287
10.3
2,04919,904
8.4
1,68620,105
11.2
2,20619,733
8.7
1,75520,200
11.4
2,26719,802
65-69 Prevalence (%)
� People with diabetes
� Annual population count
8.8
1,79120,321
12.0
2,35319,558
9.4
1,88120,074
13.1
2,52019,267
9.9
1,96319,781
13.5
2,56218,971
70-74 Prevalence (%)
� People with diabetes
� Annual population count
10.8
2,13919,855
13.6
2,37217,394
11.5
2,26119,720
14.8
2,55817,310
11.8
2,29219,403
15.5
2,67217,234
75-79 Prevalence (%)
� People with diabetes
� Annual population count
10.9
1,98118,168
14.6
2,03513,926
12.0
2,17518,089
16.1
2,27414,108
12.5
2,26218,070
16.6
2,34514,148
80-84 Prevalence (%)
� People with diabetes
� Annual population count
10.9
1,56014,298
14.2
1,3599,579
11.7
1,68114,353
15.2
1,4579,606
12.0
1,75214,599
16.3
1,5669,596
85+ Prevalence (%)
� People with diabetes
� Annual population count
9.0
1,27814,277
12.0
9067,525
9.9
1,47514,911
13.4
1,0397,761
10.5
1,62715,519
14.3
1,1528,057
Total Prevalence (%)
� People with diabetes
� Annual population count
4.3
16,170375,065
4.8
17,532362,977
4.7
17,677378,207
5.3
19,347367,102
4.9
18,537381,836
5.5
20,279370,917
Appendix K
88

Age-specific Prevalence by Fiscal Year and Sex
Manitoba
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.9
70080,186
0.6
46082,008
1.0
78679,363
0.6
51480,620
1.1
83478,756
0.7
56680,164
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.8
1,67192,502
1.4
1,26793,839
2.1
1,86090,320
1.5
1,38891,553
2.3
2,03588,651
1.7
1,51089,507
40-49 Prevalence (%)
� People with diabetes
� Annual population count
3.2
2,73885,419
3.3
2,86285,772
3.6
3,10086,488
3.7
3,19086,854
3.9
3,40787,865
3.8
3,39988,498
50-54 Prevalence (%)
� People with diabetes
� Annual population count
5.9
1,94833,130
6.7
2,25633,561
6.5
2,25334,737
7.4
2,59134,971
6.8
2,46336,482
8.0
2,91036,334
55-59 Prevalence (%)
� People with diabetes
� Annual population count
7.7
2,01126,057
8.8
2,24525,639
8.3
2,22826,831
9.7
2,57626,585
8.9
2,46427,616
10.5
2,90827,757
60-64 Prevalence (%)
� People with diabetes
� Annual population count
9.7
2,18522,564
11.6
2,56022,087
10.5
2,41022,847
12.7
2,81922,217
11.3
2,60223,011
13.5
3,00622,319
65-69 Prevalence (%)
� People with diabetes
� Annual population count
11.0
2,49222,634
13.0
2,70720,801
12.2
2,69722,137
14.5
3,00820,690
13.0
2,84221,818
15.9
3,25220,474
70-74 Prevalence (%)
� People with diabetes
� Annual population count
11.9
2,64822,316
14.4
2,61518,151
13.0
2,83821,835
15.6
2,83018,103
13.8
2,97421,477
16.9
3,04518,068
75-79 Prevalence (%)
� People with diabetes
� Annual population count
11.6
2,32220,065
13.6
1,95114,305
12.7
2,62320,590
15.5
2,25414,524
14.1
2,91220,647
16.7
2,46714,742
80-84 Prevalence (%)
� People with diabetes
� Annual population count
10.9
1,63514,956
12.6
1,1889,401
11.9
1,77114,907
14.0
1,3089,326
13.2
1,97114,931
15.2
1,4069,252
85+ Prevalence (%)
� People with diabetes
� Annual population count
8.3
1,23514,871
11.3
7937,030
9.3
1,43015,408
12.2
8967,341
10.2
1,64916,131
13.0
9927,612
Total Prevalence (%)
� People with diabetes
� Annual population count
5.0
21,585434,700
5.1
20,904412,594
5.5
23,996435,463
5.7
23,374412,784
6.0
26,153437,385
6.1
25,461414,727
Appendix K
89

Age-specific Prevalence by Fiscal Year and Sex
Ontario
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.8
6,431803,717
0.5
3,919811,280
0.9
7,271802,624
0.5
4,333811,191
1.0
7,976806,980
0.6
4,789816,213
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.5
15,8771,041,079
1.1
11,2681,049,639
1.8
18,7401,041,354
1.2
12,6351,049,776
2.1
21,5871,044,054
1.3
13,8131,053,776
40-49 Prevalence (%)
� People with diabetes
� Annual population count
2.4
21,542910,722
2.9
26,387903,353
2.7
25,003938,173
3.2
29,703932,730
2.9
28,382970,112
3.4
33,165967,532
50-54 Prevalence (%)
� People with diabetes
� Annual population count
4.3
15,547358,099
6.1
21,778359,875
4.8
17,999377,273
6.6
25,064378,637
5.2
20,567397,842
7.1
28,135397,832
55-59 Prevalence (%)
� People with diabetes
� Annual population count
6.2
17,370278,154
8.6
23,717274,985
6.9
19,863289,115
9.4
27,038286,576
7.4
22,142300,782
10.2
30,381299,148
60-64 Prevalence (%)
� People with diabetes
� Annual population count
8.5
20,783244,012
11.2
26,464235,378
9.3
23,115248,977
12.4
29,635239,437
9.9
25,167253,989
13.3
32,416244,360
65-69 Prevalence (%)
� People with diabetes
� Annual population count
10.4
24,455235,200
13.3
29,009218,307
11.3
26,639235,546
14.5
31,799220,042
12.2
28,741236,375
15.7
34,616220,972
70-74 Prevalence (%)
� People with diabetes
� Annual population count
11.6
25,494219,417
14.5
26,243180,479
12.7
27,828219,469
15.9
29,282183,787
13.7
30,182220,157
17.2
32,353187,789
75-79 Prevalence (%)
� People with diabetes
� Annual population count
11.8
20,650175,561
14.8
18,710126,807
13.0
24,053185,093
16.3
21,837134,200
14.1
26,969191,826
17.6
24,581139,554
80-84 Prevalence (%)
� People with diabetes
� Annual population count
11.2
12,990115,960
13.9
10,04272,173
12.3
14,468117,382
15.3
11,15373,096
13.4
16,338121,752
16.4
12,56776,412
85+ Prevalence (%)
� People with diabetes
� Annual population count
9.1
10,373114,589
11.1
5,57850,161
10.1
12,089119,715
12.4
6,58553,314
11.1
13,956125,895
13.2
7,51456,956
Total Prevalence (%)
� People with diabetes
� Annual population count
4.3
191,5124,496,510
4.7
203,1154,282,437
4.7
217,0684,574,721
5.3
229,0644,362,786
5.2
242,0074,669,764
5.7
254,3304,460,544
Appendix K
90

Age-specific Prevalence by Fiscal Year and Sex
Quebec
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.7
3,189475,195
0.4
1,800497,742
0.7
3,514474,044
0.4
1,915497,579
0.8
3,691475,725
0.4
2,035499,548
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.2
7,237622,102
0.8
4,967643,339
1.4
8,260605,247
0.8
5,288625,992
1.5
9,051587,489
0.9
5,445609,707
40-49 Prevalence (%)
� People with diabetes
� Annual population count
1.9
10,853582,749
2.3
13,508582,294
2.0
12,087593,300
2.5
14,959594,166
2.1
12,864603,472
2.6
15,554604,835
50-54 Prevalence (%)
� People with diabetes
� Annual population count
3.7
8,745237,477
5.4
12,703233,163
4.0
9,829246,411
5.8
14,124241,913
4.1
10,323254,727
5.9
14,831250,252
55-59 Prevalence (%)
� People with diabetes
� Annual population count
5.6
10,363184,089
8.2
14,669178,038
5.9
11,461192,971
8.8
16,537186,877
6.0
12,214201,947
9.1
17,800195,242
60-64 Prevalence (%)
� People with diabetes
� Annual population count
7.9
12,597160,168
10.7
15,791148,175
8.6
13,776159,959
11.8
17,568148,314
8.8
14,223162,379
12.3
18,609151,241
65-69 Prevalence (%)
� People with diabetes
� Annual population count
10.5
16,390156,747
13.4
18,080135,102
11.1
17,393156,639
14.4
19,696136,432
11.4
17,720155,663
14.9
20,368136,432
70-74 Prevalence (%)
� People with diabetes
� Annual population count
12.8
17,485136,795
15.9
16,407103,446
13.7
18,998138,577
17.2
18,178105,847
14.2
19,809139,496
18.0
19,397107,751
75-79 Prevalence (%)
� People with diabetes
� Annual population count
14.3
14,823103,934
16.7
11,17666,912
15.4
16,673107,952
18.3
12,79570,050
16.1
18,087112,331
19.1
14,02673,472
80-84 Prevalence (%)
� People with diabetes
� Annual population count
14.1
9,88670,256
15.9
5,89036,929
15.5
11,13171,659
17.4
6,56337,733
16.4
11,98572,900
19.0
7,31038,509
85+ Prevalence (%)
� People with diabetes
� Annual population count
12.3
7,24658,827
13.7
3,00521,928
13.6
8,41461,660
15.4
3,56923,114
14.7
9,55864,998
16.3
4,00024,505
Total Prevalence (%)
� People with diabetes
� Annual population count
4.3
118,8142,788,339
4.5
117,9962,647,068
4.7
131,5362,808,419
4.9
131,1922,668,017
4.9
139,5252,831,127
5.2
139,3752,691,494
Appendix K
91
* for participating jurisdictions
** estimated using NDSS deaths and adjusting for 4.2% of Canadian population in New Brunswick and Newfoundland and Labrador (2001 census)

Age-specific Prevalence by Fiscal Year and Sex
Prince Edward Island
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.8
7710,151
0.7
7410,574
0.9
869,891
0.7
7710,305
0.9
879,723
0.8
7710,134
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.0
11911,520
1.1
12511,264
1.3
14511,100
1.3
14410,917
1.4
15510,834
1.2
13310,757
40-49 Prevalence (%)
� People with diabetes
� Annual population count
1.9
20410,805
2.7
28710,671
2.3
25010,701
3.1
33010,560
2.3
25210,894
3.3
35610,673
50-54 Prevalence (%)
� People with diabetes
� Annual population count
3.9
1724,355
5.6
2474,415
4.2
1934,583
6.4
2934,603
4.5
2184,864
6.1
2964,872
55-59 Prevalence (%)
� People with diabetes
� Annual population count
5.7
1853,252
8.0
2613,279
6.6
2253,398
8.5
2913,415
6.4
2283,564
9.3
3253,493
60-64 Prevalence (%)
� People with diabetes
� Annual population count
6.9
2002,900
8.8
2502,840
8.0
2342,915
10.8
3112,880
8.9
2642,953
11.4
3422,987
65-69 Prevalence (%)
� People with diabetes
� Annual population count
9.2
2432,639
13.3
3382,537
10.7
2842,643
14.3
3642,548
10.7
2882,697
14.2
3672,581
70-74 Prevalence (%)
� People with diabetes
� Annual population count
10.6
2562,424
14.5
2962,039
11.6
2812,418
16.5
3442,079
12.0
2912,426
17.3
3612,081
75-79 Prevalence (%)
� People with diabetes
� Annual population count
12.1
2812,313
14.8
2361,592
13.6
3102,276
16.7
2641,585
13.6
2992,198
17.7
2881,627
80-84 Prevalence (%)
� People with diabetes
� Annual population count
11.5
2031,759
13.9
1471,061
13.5
2381,760
16.0
1681,050
15.1
2711,800
16.2
1651,016
85+ Prevalence (%)
� People with diabetes
� Annual population count
9.2
1671,817
9.2
77837
9.5
1771,854
11.5
99859
10.2
1981,948
13.6
122897
Total Prevalence (%)
� People with diabetes
� Annual population count
3.9
2,10753,935
4.6
2,33851,109
4.5
2,42353,539
5.3
2,68550,801
4.7
2,55153,901
5.5
2,83251,118
Appendix K
92

Age-specific Prevalence by Fiscal Year and Sex
Nova Scotia
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Prevalence (%)
� People with diabetes
� Annual population count
0.7
50167,005
0.6
37266,087
0.8
55766,540
0.6
38865,247
0.9
57766,267
0.6
39864,978
30-39 Prevalence (%)
� People with diabetes
� Annual population count
1.3
1,07481,231
1.1
85076,342
1.5
1,17379,773
1.3
94775,382
1.5
1,18378,922
1.3
97774,517
40-49 Prevalence (%)
� People with diabetes
� Annual population count
2.6
1,92675,191
3.1
2,25873,214
2.8
2,15276,636
3.3
2,44774,297
2.9
2,26678,418
3.3
2,50575,530
50-54 Prevalence (%)
� People with diabetes
� Annual population count
5.3
1,64730,791
6.7
2,04830,490
5.8
1,88632,414
7.1
2,28232,015
5.8
1,96933,834
7.2
2,42933,577
55-59 Prevalence (%)
� People with diabetes
� Annual population count
7.4
1,73623,556
9.6
2,24223,279
7.9
1,94124,514
10.3
2,50224,215
8.1
2,06025,590
10.6
2,70625,422
60-64 Prevalence (%)
� People with diabetes
� Annual population count
10.4
2,07319,897
12.4
2,43719,630
11.0
2,24620,380
13.6
2,74420,231
11.1
2,31120,835
14.0
2,87020,532
65-69 Prevalence (%)
� People with diabetes
� Annual population count
12.4
2,33518,803
14.7
2,53017,181
13.1
2,47118,816
16.0
2,77217,379
13.4
2,54918,997
16.5
2,92917,720
70-74 Prevalence (%)
� People with diabetes
� Annual population count
13.7
2,38617,406
17.0
2,38013,969
15.2
2,65817,449
18.6
2,63014,102
15.7
2,71517,298
19.4
2,76714,250
75-79 Prevalence (%)
� People with diabetes
� Annual population count
14.1
2,25215,949
17.1
1,91311,157
15.1
2,42716,029
18.3
2,05311,229
15.9
2,52815,897
18.9
2,14311,314
80-84 Prevalence (%)
� People with diabetes
� Annual population count
13.3
1,55311,672
15.7
1,1197,125
14.6
1,71311,772
17.5
1,2527,145
15.3
1,86212,194
19.1
1,4077,363
85+ Prevalence (%)
� People with diabetes
� Annual population count
9.9
1,12611,377
12.5
6084,868
11.3
1,33511,792
14.2
7165,046
11.9
1,47312,339
15.3
7995,222
Total Prevalence (%)
� People with diabetes
� Annual population count
5.0
18,609372,878
5.5
18,757343,342
5.5
20,559376,115
6.0
20,733346,288
5.6
21,493380,591
6.3
21,930350,425
Appendix K
93

Appendix L
Mortality
Age-specific Mortality by Fiscal Year, Sex and Province/Territory
Canada
Age group 1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
2614,815
6181,979,594
5.62
259,037
1,7272,012,432
3.22
2016,446
5411,975,067
4.44
189,801
1,6272,010,592
2.27
2017,487
5601,977,188
4.04
2510,555
1,5952,015,794
2.99
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
7735,137
1,3092,490,782
4.17
11024,266
2,7852,517,659
4.10
7240,613
1,2222,456,095
3.56
8926,867
2,4792,485,320
3.32
10245,389
1,1862,423,518
4.59
11728,671
2,4142,458,628
4.16
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
23849,593
2,8562,237,994
3.76
41360,144
4,5632,227,168
3.35
24756,770
2,8142,290,143
3.54
46467,318
4,1962,280,159
3.75
28362,682
2,9022,346,320
3.65
51572,760
4,5052,338,229
3.67
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
30836,703
2,117857,151
3.40
57350,814
3,307847,454
2.89
33842,137
2,161896,412
3.33
56058,076
3,181883,254
2.68
35746,552
2,209938,763
3.26
59763,580
3,261922,903
2.66
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
48641,367
2,584648,918
2.95
94956,468
4,110627,079
2.56
52846,620
2,600673,308
2.93
89964,033
3,920650,271
2.33
54850,972
2,661699,270
2.83
1,03170,730
3,987675,235
2.47
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
81748,835
3,495551,164
2.64
1,55862,257
5,525517,169
2.34
84553,995
3,238554,234
2.68
1,52369,602
5,249516,793
2.15
87757,612
3,284561,752
2.60
1,63774,888
5,218522,592
2.19
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1,46158,903
5,264520,721
2.45
2,47469,124
8,605466,356
1.94
1,42363,590
4,885515,794
2.36
2,64575,916
7,994463,378
2.02
1,51566,887
4,798512,081
2.42
2,60880,821
7,632459,778
1.94
Appendix L
94

Canada (continued)
Age group 1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
2,37961,868
7,481468,469
2.41
3,38262,867
11,049370,250
1.80
2,30367,530
7,227464,381
2.19
3,62469,954
10,470371,160
1.84
2,34071,808
7,166461,677
2.10
3,68875,969
10,326373,804
1.76
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
2,97652,132
10,653379,997
2.04
3,68545,495
12,790261,361
1.66
3,13859,504
10,244390,094
2.01
4,06152,425
12,577268,666
1.65
3,38365,349
10,303396,378
1.99
4,36757,853
12,348273,785
1.67
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
3,04534,279
13,095261,256
1.77
3,11725,275
12,724154,702
1.50
3,28638,245
12,482261,043
1.80
3,31028,063
12,218154,046
1.49
3,42042,117
12,332265,298
1.75
3,55631,259
11,450156,320
1.55
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
4,45926,337
30,729250,580
1.38
2,82614,213
16,691108,997
1.30
4,89230,647
30,287259,416
1.37
3,24516,685
16,604113,307
1.33
5,36435,044
30,270269,955
1.37
3,46118,956
16,618118,473
1.30
Total* Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
16,272459,969
80,20110,646,626
4.70
19,112479,960
83,87610,110,627
4.80
17,092516,097
77,70110,735,987
4.58
20,438538,740
80,51510,196,946
4.80
18,209561,899
77,67110,852,200
4.53
21,602586,042
79,35410,315,541
4.79
CanadianTotal
Diabetes� deaths** 16,955 19,915 17,810 21,296 18,974 22,509
Appendix L
95

Age-specific Mortality by Fiscal Year and Sex
Yukon Territory
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
*206
2110,678
*
*225
3411,538
*
*246
1610,514
*
*247
4011,078
*
*259
1910,406
*
*257
4810,745
*
65+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
11474
6517,931
6.4
*520
5417,640
*
12548
7317,456
5.24
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
7274
3911,390
7.46
6320
6212,336
3.73
6322
4611,254
4.56
4349
6911,921
1.98
5351
4211,171
3.79
11377
8811,615
3.85
* cell suppressed
Appendix L
96

Age-specific Mortality by Fiscal Year and Sex
Northwest Territories
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
*233
3513,181
*
*298
7214,113
*
*265
4412,992
*
*345
7713,965
*
*275
2512,759
*
*371
3713,604
*
65+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
9563
11320,329
2.88
11651
11720,313
2.93
*704
6720,036
*
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
10322
7013,933
6.18
4362
13014,976
1.27
9357
9313,769
3.73
5425
13714,830
1.27
7373
5213,534
4.88
2469
7914,461
0.78
* cell suppressed
Appendix L
97

Age-specific Mortality by Fiscal Year and Sex
British Columbia
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
01,933
91268,504
0
01,133
310258,200
0
02,132
66263,108
0
51,173
188252,219
5.72
02,182
61257,545
0
01,187
166248,016
0
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
84,699
217331,504
2.6
162,922
457323,836
3.88
85,412
152325,377
3.16
73,200
286317,256
2.43
106,000
132319,439
4.03
93,302
280312,357
3.04
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
246,187
410314,655
2.98
457,653
638310,363
2.86
207,126
372320,571
2.42
358,502
536314,148
2.41
277,779
320325,423
3.53
578,974
521317,860
3.88
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
364,572
281117,752
3.3
646,195
456119,014
2.7
325,307
279123,759
2.67
567,183
373124,156
2.6
355,827
256130,869
3.07
537,857
378130,661
2.33
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
545,213
34387,838
2.65
1127,194
53887,319
2.53
525,837
32291,637
2.54
948,096
46490,841
2.27
496,368
33595,378
2.19
1078,877
44894,484
2.54
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
895,965
40573,253
2.7
1678,037
65471,805
2.28
866,671
39574,190
2.42
1538,998
59772,133
2.05
817,102
39375,674
2.2
1789,601
59173,048
2.29
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1407,073
66368,874
2.06
2799,026
1,09466,246
1.87
1457,701
61368,180
2.09
30110,065
96865,479
2.02
1438,108
56967,537
2.09
28610,675
88365,040
1.97
Appendix L
98

British Columbia (continued)
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
2457,421
93163,648
2.26
4028,041
1,43653,586
1.87
2398,164
92162,562
1.99
3909,033
1,30653,528
1.77
2508,693
85462,195
2.09
4489,794
1,24954,195
1.98
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
3566,402
1,45055,410
2.12
4436,196
1,67940,289
1.72
3307,310
1,36156,753
1.88
5177,180
1,70041,565
1.76
3878,050
1,35356,874
2.02
5667831
1,59841,773
1.89
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
3364,133
1,84938,682
1.70
4123,631
1,76124,745
1.59
3784,695
1,61738,538
1.92
4304,013
1,72224,447
1.52
3905,129
1,65539,275
1.80
4654,487
1,67124,965
1.55
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
4893,022
3,91335,512
1.47
3882,059
2,43617,621
1.36
5053,521
3,99837,432
1.34
4492,439
2,49618,606
1.37
5954,118
3,95039,625
1.45
4822,851
2,58319,641
1.29
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1,77756,620
10,5531,455,632
4.33
2,32862,087
11,4591,373,024
4.49
1,79563,876
10,0961,462,107
4.07
2,43769,882
10,6361,374,378
4.51
1,96769,356
9,8781,469,834
4.22
2,65175,436
10,3681,382,040
4.68
Appendix L
99

Age-specific Mortality by Fiscal Year and Sex
Alberta
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
01,435
80209,878
0
0899
201213,962
0
01,506
76215,530
0
0997
197220,587
0
01,531
68218,426
0
01,067
193223,831
0
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
123,345
149251,928
6.07
61,990
312252,369
2.44
103796
131250,158
5.03
72,278
295250,943
2.61
84,072
118247,288
4.12
122,464
258247,939
4.68
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
214,212
262219,813
4.18
325,060
468227,538
3.07
264,895
268228,923
4.54
485,759
424236,923
4.66
255,464
288237,294
3.77
426,275
452245,311
3.63
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
152,815
17476,720
2.35
293,901
27477,989
2.12
213,241
21581,232
2.45
414,633
28082,194
2.6
343,668
19786,048
4.05
345,075
27587,364
2.13
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
343,072
22656,106
2.75
624,308
35556,311
2.28
343,518
22358,611
2.54
444,919
34158,824
1.54
383,852
22761,168
2.66
595,537
36361,342
1.80
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
603,441
30046,694
2.71
1134,592
49045,936
2.31
573,782
26547,565
2.71
895,235
46046,149
1.71
614,112
27048,256
2.65
1195,672
45046,839
2.18
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
924,069
45642,672
2.12
1575,006
70840,913
1.81
824,478
37842,559
2.06
1785,607
67340,979
1.93
994,622
41242,727
2.22
1685,955
67340,960
1.72
Appendix L
100

Alberta (continued)
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1403,999
61736,648
2.08
1824,465
84431,074
1.50
1484,444
51736,870
2.38
2335,042
88231,756
1.66
1334,788
59637,135
1.73
2165,514
87232,543
1.46
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1873,391
83830,660
2.02
2383,259
1,03622,133
1.56
2013,904
75731,294
2.13
2483,748
97722,623
1.53
1924,208
81931,316
1.74
3144,145
97022,745
1.78
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1822,299
1,05021,332
1.61
2101,887
1,02613,294
1.44
1842,525
96421,505
1.63
2092,137
1,01313,397
1.29
2052,782
98821,869
1.63
2562,332
97213,484
1.52
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
2931,878
2,50120,590
1.28
2391,182
1,5889,887
1.26
3472,194
2,40021,405
1.41
2341,334
1,47210,059
1.2
3662,454
2,46421,796
1.32
2681,517
1,49910,049
1.18
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1,03633,956
6,6531,013,041
4.65
1,26836,549
7,302991,406
4.71
1,11038,283
6,1941,035,652
4.85
1,33141,689
7,0141,014,434
4.62
1,16141,553
6,4471,053,323
4.56
1,48845,553
6,9771,032,407
4.83
Appendix L
101

Age-specific Mortality by Fiscal Year and Sex
Saskatchewan
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
0514
3569,553
0
0360
6872,992
0
0557
2570,175
0
0378
9074,195
0
0574
3371,149
0
0410
7775,224
0
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
01,039
5277,239
0
0818
11577,751
0
01,140
5275,570
0
0928
8876,567
0
01,220
5273,771
0
0968
10075,026
0
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
61,804
10869,793
2.15
161,998
15672,460
3.72
102,018
10771,721
3.32
152,266
14574,290
3.39
142,131
9873,780
4.95
162,370
16676,220
3.1
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
131,180
6725,017
4.11
161,556
10925,564
2.41
91,327
6226,227
2.87
221,771
11126,639
2.98
141,400
7627,569
3.63
321,902
13128,077
3.61
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
141,349
7320,371
2.9
301,726
12019,866
2.88
281,476
8420,744
4.68
311,950
15620,333
2.07
231,561
9421,109
3.31
342,065
13320,847
2.58
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
301,535
13418,752
2.73
522,049
21617,855
2.1
311,686
11118,419
3.05
502,206
17917,527
2.22
281,755
11218,445
2.63
592,267
21417,535
2.13
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
481,791
19118,530
2.60
922,353
30117,205
2.23
491,881
18818,193
2.52
902,520
28816,747
2.08
531,963
16817,818
2.86
982,562
27916,409
2.25
Appendix L
102

Saskatchewan (continued)
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
832,139
26217,716
2.62
1322,372
43215,022
1.94
832,261
28217459
2.27
1572,558
43514,752
2.08
822,292
25617,111
2.39
1612,672
41014,562
2.14
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1041,981
46416,187
1.83
1392,035
58311,891
1.39
1062,175
37815,914
2.05
1842,274
60911,834
1.57
1162,262
40615,808
2
2082,345
54111,803
1.94
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1211,560
57512,738
1.72
1381,359
6298,220
1.33
1191,681
53112,672
1.69
1511,457
6388,149
1.32
1301,752
55712,847
1.71
1921,566
5768,030
1.71
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1851,278
1,52312,999
1.24
163906
9666,619
1.23
2361,475
1,56413,436
1.37
1941,039
1,0166,722
1.24
2381,627
1,55813,892
1.3
2101,152
1,0196,905
1.24
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
60416,170
3,484358,895
3.85
77817,532
3,695345,445
4.15
67117677
3,384360,530
4.04
89419,347
3,755347,755
4.28
69818,537
3,410363,299
4.01
1,01020,279
3,646350,638
4.79
Appendix L
103

Age-specific Mortality by Fiscal Year and Sex
Manitoba
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
0700
3179,486
0
0460
7981,548
0
0786
3278,577
0
0514
8280,106
0
0834
3877,922
0
0566
8079,598
0
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
71,671
5290,831
7.32
01,267
10292,572
0
01,860
6188,460
0
51,388
10490,165
3.12
92,035
6486,616
5.99
01,510
9387,997
0
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
132,738
10682,681
3.7
172,862
16182,910
3.06
163,100
9283,388
4.68
383,190
14783,664
6.78
203,407
11984,458
4.17
283,399
19885,099
3.54
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
131,948
7631,182
2.74
222,256
11731,305
2.61
212,253
8532,484
3.56
312,591
10932,380
3.55
222,463
10134,019
3.01
332,910
13333,424
2.85
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
222,011
9624,046
2.74
392,245
15823,394
2.57
342,228
12024,603
3.13
372,576
16024,009
2.16
262,464
11125,152
2.39
612,908
15624,849
3.34
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
432,185
12320,379
3.26
542,560
19619,527
2.1
482,410
15420,437
2.64
742,819
25619,398
1.99
372,602
14220,409
2.04
843,006
19219,313
2.81
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
712,492
20020,142
2.87
982,707
33218,094
1.97
622,697
20519,440
2.18
1123,008
32517,682
2.03
692,842
18918,976
2.44
1013,252
36117,222
1.48
Appendix L
104

Manitoba (continued)
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1062,648
28019,668
2.81
1172,615
43315,536
1.61
1142,838
31318,997
2.44
1482,830
44615,273
1.79
842,974
28718,503
1.82
1643,045
44415,023
1.82
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1232,322
47417,743
1.98
1391,951
62812,354
1.4
1522,623
53517,967
1.95
1832,254
59812,270
1.67
1622,912
46017,735
2.14
1772,467
62112,275
1.42
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1401,635
64013,321
1.78
1411,188
6568,213
1.49
1421,771
62713,136
1.68
1671,308
6838,018
1.5
1521,971
60312,960
1.66
1461,406
5967,846
1.37
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
2141,235
1,59113,636
1.49
148793
9166,237
1.27
1951,430
1,70613,978
1.12
180896
9956,445
1.3
2351,649
1,62314,482
1.27
191992
9686,620
1.32
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
75221,585
3,669413,115
3.92
77520,904
3,778391,690
3.84
78423,996
3,930411,467
3.42
97523,374
3,905389,410
4.16
81626,153
3,737411,232
3.43
98525,461
3,842389,266
3.92
Appendix L
105

Age-specific Mortality by Fiscal Year and Sex
Ontario
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
116,431
188797,286
7.25
133,919
485807,361
5.52
127,271
169795,353
7.77
84,333
481806,858
3.1
117,976
170799,004
6.48
154,789
473811,424
5.37
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
2715,877
4431,025,202
3.94
4211,268
9341,038,371
4.14
2718,740
4401,022,614
3.35
4212,635
8411,037,141
4.1
4421,587
4271,022,467
4.88
5513,813
8191,039,963
5.06
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
9121,542
1,014889,180
3.7
17026,387
1,579876,966
3.58
10125,003
1,001913,170
3.69
16829,703
1,386903,027
3.69
10828,382
1,012941,730
3.54
20433,165
1,536934,367
3.74
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
12415,547
806342,552
3.39
23921,778
1,177338,097
3.15
13417,999
773359,274
3.46
22425,064
1,118353,573
2.83
13520,567
896377,275
2.76
26428,135
1,212369,697
2.86
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
16817,370
972260,784
2.59
36423,717
1,475251,268
2.61
22519,863
946269,252
3.22
33427,038
1,376259,538
2.33
22322,142
1,004278,640
2.8
40830,381
1,463268,767
2.47
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
32420,783
1,369223,229
2.54
62326,464
2,046208,914
2.4
32723,115
1,242225,862
2.57
62029,635
1,946209,802
2.26
35825,167
1,282228,822
2.54
63332,416
1,940211,944
2.13
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
56024,455
2,018210,745
2.39
98229,009
3,175189,298
2.02
58026,639
1,879208,907
2.42
1,01031,799
2,950188,243
2.03
62228,741
1,890207,634
2.38
1,00734,616
2,809186,356
1.93
Appendix L
106

Ontario (continued)
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
96625,494
3,027193,923
2.43
1,37226,243
4,316154,236
1.87
90427,828
2,779191,641
2.24
1,42929,282
4,039154,505
1.87
93130,182
2,878189,975
2.04
1,47632,353
4,017155,436
1.77
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1,15620,650
4,147154,911
2.09
1,49918,710
4,943108,097
1.75
1,25224,053
4,137161,040
2.03
1,61921,837
4,848112,363
1.72
1,32726,969
4,231164,857
1.92
1,73424,581
4,891114,973
1.66
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1,21712,990
4,965102,970
1.94
1,22610,042
4,79662,131
1.58
1,24314,468
4,842102,914
1.83
1,30911,153
4,52161,943
1.61
1,31716,338
4,777105,414
1.78
1,36312,567
4,39363,845
1.58
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1,79310,373
12,367104,216
1.46
1,0975,578
6,31644,583
1.39
1,95212,089
11,843107,626
1.47
1,3086,585
6,25346,729
1.48
2,10313,956
12,166111,939
1.39
1,3517,514
6,38649,442
1.39
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
6,437191,512
31,3164,304,998
4.62
7,627203,115
31,2424,079,322
4.9
6,757217,068
30,0514,357,653
4.51
8,071229,064
29,7594,133,722
4.89
7,179242,007
30,7334,427,757
4.27
8,510254,330
29,9394,206,214
4.7
Appendix L
107

Age-specific Mortality by Fiscal Year and Sex
Quebec
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
153,189
161472,006
13.79
121,800
501495,942
6.6
83,514
135470,530
7.93
51,915
494495,664
2.62
93,691
150472,034
7.67
102,035
542497,513
4.51
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
187,237
350614,865
4.37
394,967
743638,372
6.75
268,260
342596,987
5.49
285,288
772620,704
4.26
239,051
345578,438
4.26
365,445
754604,262
5.3
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
7410,853
840571,896
4.64
12113,508
1,357568,786
3.75
6612,087
859581,213
3.69
13814,959
1,375579,207
3.89
8212,864
947590,608
3.98
15215,554
1,416589,281
4.07
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1008,745
613228,732
4.27
17812,703
1,005220,460
3.07
1089,829
651236,582
3.99
17014,124
1,022227,789
2.68
10410,323
596244,404
4.13
15414,831
980235,421
2.49
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
17610,363
737173,726
4
29414,669
1,260163,369
2.6
14111,461
784181,510
2.85
31716,537
1,244170,340
2.62
16712,214
778189,733
3.33
32217,800
1,247177,442
2.57
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
23212,597
994147,571
2.73
50415,791
1,688132,384
2.50
26513,776
930146,183
3.02
47417,568
1,565130,746
2.25
25714,223
950148,156
2.82
48818,609
1,611132,632
2.16
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
48316,390
1,486140,357
2.78
77618,080
2,595117,022
1.94
43617,393
1,428139,246
2.44
84019,696
2,445116,736
2.04
46917,720
1,367137,943
2.67
83620,368
2,304116,064
2.07
Appendix L
108

Quebec (continued)
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
75417,485
2,052119,310
2.51
1,03216,407
3,11887,039
1.76
71518,998
2,084119,579
2.16
1,12218,178
2,94987,669
1.83
74119,809
1,990119,687
2.25
1,06419,397
2,90388,354
1.67
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
91914,823
2,80589,111
1.97
1,06411,176
3,31255,736
1.6
96116,673
2,63591,279
2
1,15612,795
3,28257,255
1.58
1,04718,087
2,59794,244
2.1
1,18914,026
3,14359,446
1.6
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
9029,886
3,40460,370
1.62
8505,890
3,22931,039
1.39
1,06111,131
3,31060,528
1.74
8916,563
3,06831,170
1.38
1,05311,985
3,18860,915
1.68
9437,310
2,68131,199
1.5
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1,2887,246
7,29951,581
1.26
6663,005
3,61918,923
1.16
1,4308,414
7,38353,246
1.23
7543,569
3,53219,545
1.17
1,5889,558
7,03255,440
1.31
8004,000
3,41320,505
1.2
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
4,961118,814
20,7412,669,525
5.37
5,536117,996
22,4272,529,072
5.29
5,217131,536
20,5412,676,883
5.17
5,895131,192
21,7482,536,825
5.24
5,540139,525
19,9402,691,602
5.36
5,994139,375
20,9942,552,119
5.23
Data source for the number of deaths among non-diabetic people : Registre des événements démographiques du Québec (1997, 1998,1999 and 2000). Data from the Fichier des décès of 2000 are preliminary.
Appendix L
109

Age-specific Mortality by Fiscal Year and Sex
Prince Edward Island
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
*957
6242,026
*
*1,244
12341,799
*
*1,133
6341,455
*
*1,446
11241,234
*
*1,204
7341,628
*
*1,529
11441,387
*
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
8243
282,396
2.82
11338
472,199
1.52
7284
252,359
2.33
11364
412,184
1.61
6288
172,409
2.95
12367
392,214
1.86
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
0256
362,168
0
15296
561,743
1.58
12281
382,137
2.4
19344
611,735
1.57
10291
332,135
2.22
16361
511,720
1.49
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
16281
442,032
2.63
21236
751,356
1.61
12310
561,966
1.36
19264
731,321
1.3
12299
521,899
1.47
17288
741,339
1.07
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
12203
751,556
1.23
8147
78914
0.64
15238
821,522
1.17
24168
92882
1.37
25271
671,529
2.11
20165
78851
1.32
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
30167
2201,650
1.35
777
120760
0.58
23177
1871,677
1.17
1399
109760
0.92
26198
2121,750
1.08
24122
128775
1.19
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
662,107
46551,828
3.49
622,338
49948,771
2.59
692,423
45151,116
3.23
982,685
48848,116
3.6
842,551
45451,350
3.72
1022,832
48448,286
3.59
* cell suppressed
Appendix L
110

Age-specific Mortality by Fiscal Year and Sex
Nova Scotia
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
20-29 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
0501
2666,504
0
0372
5265,715
0
0557
2465,983
0
0388
5264,859
0
0577
2665,690
0
0398
4864,580
0
30-39 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
51,074
4180,157
9.10
7850
8675,492
7.23
01,173
3678,600
0
0947
6674,435
0
81,183
3977,739
13.48
5977
7873,540
4.83
40-49 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
71,926
9573,265
2.80
112,258
16170,956
2.15
82,152
9174,484
3.04
212,447
13371,850
4.64
62,266
9376,152
2.17
162,505
16273,025
2.88
50-54 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
71,647
7729,144
1.61
242,048
13928,442
2.40
121,886
7830,528
2.49
152,282
13729,733
1.43
131,969
6631,865
3.19
262,429
11831,148
2.83
55-59 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
171,736
11221,820
1.91
482,242
15921,037
2.83
141,941
9122,573
1.79
352,502
14321,713
2.12
222,060
8823,530
2.86
342,706
14722,716
1.94
60-64 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
382,073
13217,824
2.48
442,437
19117,193
1.63
302,246
11218,134
2.16
562,744
20417,487
1.75
482,311
11118,524
3.47
672,870
18717,662
2.20
65-69 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
562,335
20916,468
1.89
782,530
32814,651
1.38
612,471
15716,345
2.57
1012,772
28114,607
1.89
512,549
17816,448
1.85
972,929
26514,791
1.85
Appendix L
111

Nova Scotia (continued)
Age group1997/1998 1998/1999 1999/2000
Female Male Female Male Female Male
70-74 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
852,386
26315,020
2.03
1262,380
39711,589
1.55
852,658
28514,791
1.66
1242,630
33311,472
1.62
1072,715
26114,583
2.20
1382,767
35611,483
1.61
75-79 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1132,252
42313,697
1.62
1411,913
5199,244
1.31
1242,427
36913,602
1.88
1342,053
4729,176
1.27
1372,528
37213,369
1.95
1602,143
4939,171
1.39
80-84 Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1291,553
53110,119
1.58
1321,119
5356,006
1.32
1401,713
48810,059
1.68
1291,252
4705,893
1.29
1481,862
49310,332
1.67
1711,407
4755,956
1.52
85+ Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
1651,126
1,30210,251
1.15
117608
7154,260
1.15
2001,335
1,18410,457
1.32
113716
7134,330
0.96
2121,473
1,25110,866
1.25
135799
6084,423
1.23
Total Diabetes� deaths� population count
No diabetes� deaths� population count
Mortality rate ratio
62218,609
3,211354,269
3.69
72818,757
3,282324,585
3.84
67420,559
2,915355,556
4.00
72820,733
3,004325,555
3.81
75221,493
2,978359,098
4.22
84921,930
2,937328,495
4.33
Appendix L
112