Embed Size (px)
Citation preview
Originai Paper
NEPHRON Nephron 2000;85:114-119 Accepted: November 2,1999
Responses of the Skin Microcirculation toAcetylcholine in Patients with EssentialHypertension and in Normotensive Patientswith Chronic Renal Failure
Adamasco Cupisti Marco Rossi Silvia Placidi Alessandra FabbriEster Morelli Guido Vagheggini Mario Meola Giuliano Barsotti
Dipartimentodi Medicina Interna, Università di Pisa, Italia
Key WordsAcetylcholine .Chronic renal failure .Cutaneous bloodflow. Endothelium . Essential hypertension .Laser
Doppler flowmetry
Abstract
Aims: To assess the endothelial function of the skin
microcirculation in chronic renal failure (CRF) indepen-dent of hypertension, we investigated the changes of thecutaneous blood flow induced by iontophoretic deliveryof acetylcholine (ACh) and of sodium nitroprusside(SNP) in CRF patients free from arterial hypertension andin patients with essential hypertension. Methods: Thestudy included 20 patients affected by CRF (mean creati-nine clearance 12 :t 2 mlfmin) without arterial hyperten-sion (mean blood pressure 96 :t 1 mm Hg), 15 patientsaffected by essential hypertension (mean blood pressure124 :t 1 mm Hg), and 20 normal controls. The changes ofskin blood flow following iontophoretic delivery of AChand of SNP were measured by laser Doppler flowmetry.Results: Following maximal ACh or SNP delivery, thechange of blood flow from the baseline was similar both
in normals (683 :t 92 vs. 684 :t 87%) and in CRF patients(778 :t 108 vs. 803 :t 124%), whereas in the hyperten-
KARGER @ 2000 S. Karger AG, Basel0028-2766/0010852-0114$17.5010
Fax+4l613061234
E-Mail [email protected]
Accessible online al:
www.karger.com/journals/nef
sives the response to ACh was lower than to SNP (434 :t48 vs. 702 :t 98%, p < 0.01). Since the third ACh deliverydose, the skin blood flow increments were significantlylower in the hypertensive than in the CRF or in the nor-mal control groups, whereas no difference was observedbetween uremics and controls. Conclusions: The endo-
thelium-dependent hyperemia following ACh iontophor-etic delivery is impaired in the skin microcirculation ofessential hypertensive patients, but this is not the case inCRF patients with no history of arterial hypertension.This suggests that CRF per se, independent of arterialhypertension, is not associated with endothelial dysfunc-tion of skin microcirculation.
Copyright@2000S. Karger AG, Basel
Introduction
Factors frequent1y found in rena1 disease patients, suchas arteria1 hypertension, hyperlipidemia, diabetes, andhyperhomocysteinemia, can negatively affect endothe1ia1cell functioning. Since endothe1ium dysfunction may bean early manifestation of the atherogenesis process, it
" cou1dbe imp1icated a1soin the high cardiovascu1ar riskreported in uremic patients [1-3]. Evidence exists that the
Prof. Giuliano Barsotti
Dipartimento di Medicina Interna, Università degli Studi di Pisavia Roma, 671-56100 Pisa (ltaly)
Te!. +39050993320, Fax +39050502617, E-Mail [email protected]
endothelium-dependent dilation of the brachial artery isimpaired in adult dialysis patients and in children withchronic renal failure (CRF) [4-6]. On the contrary, exper-imental data failed to demonstrate similar findings inmesenteric arteries of uremic rats [7]. Moreover, up todate, endothelium-dependent vasodilation of small arteri-al vessels has not been studied in CRF patients. Severalreports have c1ear1ydemonstrated that essential hyperten-sion is associated with endothelial dysfunction both in themusc1e vascular bed and in the skin microcirculation of
the forearm [8-11]. Since it is welI known that CRFpatients are usualIy hypertensive, the question arises asto whether uremia 'per se' or the frequent1y associatedarterial hypertension can negatively affect the endothelialcelI function in uremics. Hence, the arterial hypertensionand its pharmacological treatment could represent impor-tant confounding factors for the study of endothelial dys-function in these patients.
The recent use of iontophoresis coupled with laserDoppler flowmetry [12] alIows to assess the real-timechanges of the skin blood flow in a noninvasive manner[13-15]. In addition, since the drug is delivered locally inthe skin, systemic effects that could interfere with the skinmicrocirculatory responses are avoided.
Hence, to assess the small-vessel endothelial functionin CRF independent ofhypertension, we investigated thechanges of cutaneous blood flow induced by the ionto-phoretic delivery of an endothelium-dependent (acetyl-choline; ACh) and of an endothelium-independent (sodi-um nitroprusside; SNP) vasodilator in patients with ad-vanced CRF, but free from arterial hypertension, and inpatients with essential hypertension.
Patients and Methods
SubjectsThe study population inc1uded20 CRF patients free from arterial
hypertension (CRF group), 15 patients affected by essential hyper-tension (EHT) with normal renal function (EHT group), and 20 nor-mal control subjects (NC group). The three groups did not differ asfar as the agewas concerned (table l).
Patients and subjects older than 65 years, heavy smokers (morethan 5 cigarettes daily), or those affected by diabetes mellitus (fastingglucose levels > 126mg/dl) or with abnormally elevated cholesterolplasma levels (>240 mg/dl) were exc1uded. Subjects smoking up to5 cigarettes daily were requested to refrain from smoking for 12h atleast before examination.
Blood urea nitrogen, creatinine, electrolyte, cholesterol, triglycer-ide, fasting glucose, total protein and albumin circulating levels, aswell as hematocrit and arterial blood pressure values of the threegroups are shown in table l.
Skin Microcirculation in Chronic RenalFailure and in Essential Hypertension
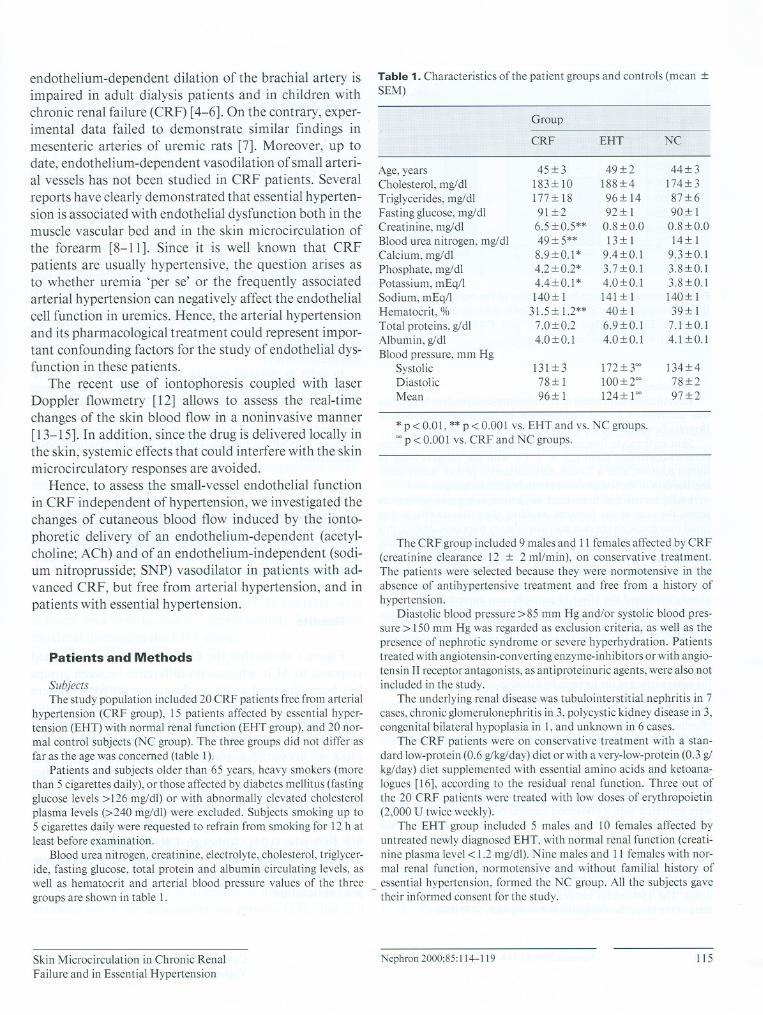
Table 1. Characteristics ofthe patient groups and controls (mean :tSEM)
The CRF group inc1uded9 males and II females affected by CRF(creatinine c1earance 12 :t 2 ml/min), on conservative treatment.The patients were selected because they were normotensive in theabsence of antihypertensive treatment and free from a history ofhypertension.
Diastolic blood pressure >85 mm Hg and/or systolic blood pres-sure > 150mm Hg was regarded as exc1usioncriteria, as well as thepresence of nephrotic syndrome or severe hyperhydration. Patientstreated with angiotensin-converting enzyme-inhibitors orwith angio-tensin II receptor antagonists, as antiproteinuric agents, were also notinc1uded in the study.
The underlying renal disease was tubulointerstitial nephritis in 7cases, chronic glomerulonephritis in 3,polycystic kidney disease in 3,congenital bilateral hypoplasia in I, and unknown in 6 cases.
The CRF patients were on conservative treatment with a stan-dard low-protein (0.6 g/kg/day) diet or with a very-Iow-protein (0.3 glkg/day) diet supplemented with essential amino acids and ketoana-logues [16], according to the residual renal function. Three out ofthe 20 CRF patients were treated with low doses of erythropoietin(2,000 U twice weekly).
The EHT group inc1uded 5 males and IO females affected byuntreated newly diagnosed EHT, with normal renal function (creati-nine plasma level < 1.2 mg/dl). Nine males and Il females with nor-mal renal function, normotensive and without familial history of
" essential hypertension, formed the NC group. All the subjects gavetheir informed consent for the study.
Nephron 2000;85:114-119 115
Group
CRF EHT NC
Age,years 45:t 3 49 :t 2 44 :t 3Cholesterol, mg/di 183:t lO 188:t 4 174:t3
Triglycerides, mg/dl 177:t18 96:t 14 87:t 6Fasting glucose,mg/dl 91:t2 92:t l 90:t ICreatinine, mg/dl 6.5:t 0.5** 0.8:t 0.0 0.8:t 0.0Blood urea nitrogen, mg/dl 49:t 5** 13:t1 14:t1Calcium, mg/dl 8.9:t0.1* 9.4:t0.1 9.3:t0.1Phosphate, mg/dl 4.2:t 0.2* 3.7:t0.1 3.8:t0.1Potassium, mEq/1 4.4:t0.1* 4.0:t0.1 3.8:t0.1Sodium, mEq/1 140:t l 141:t1 140:t lHematocrit, % 31.5 :t 1.2** 40:t l 39:t lTotal proteins, g/dl 7.0:t0.2 6.9:t0.1 7.1 :t0.1Albumin, gldi 4.0:t0.1 4.0:t 0.1 4.1 :t0.1Blood pressure, mm Hg
Systolic 131:t3 172:t 300 134:t 4Diastolic 78:t1 100 :t 200 78:t2Mean 96:t l 124:t1o0 97 :t 2
* p < 0.01, **p < 0.001 vs. EHT and vs. NC groups.00 p < 0.00 I vs. CRF and NC groups.
1,000
900
.~ 800
~ 700'".D 600E
.g 500
@, 400c:~ 300u
<f2. 200
100
O
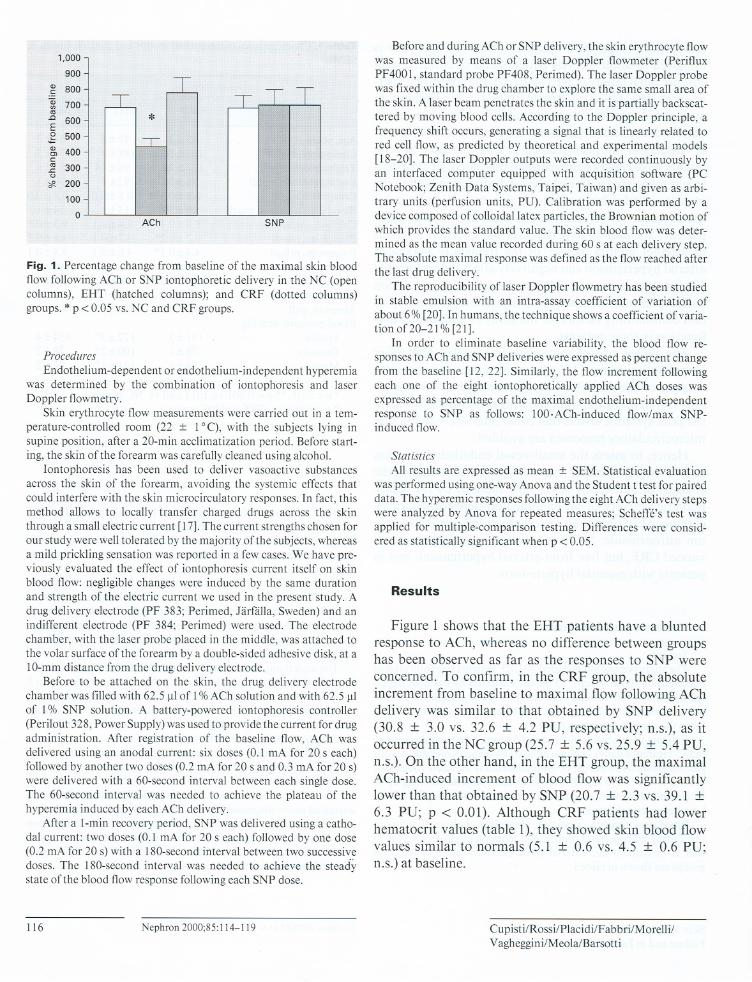
Fig. 1. Percentage change from baseline of the maximal skin bloodflow following ACh or SNP iontophoretic delivery in the NC (opencolumns), EHT (hatched columns); and CRF (dotted columns)groups. * p < 0.05 vs. NC and CRF groups.
Procedures
Endothelium-dependent or endothelium-independent hyperemiawas determined by the combination of iontophoresis and laserDoppler flowmetry.
Skin erythrocyte flow measurements were carried out in a tem-perature-controlledroom (22 :t 1oC), with the subjects lying insupine position, after a 20-min acc1imatization periodo Before start-ing, the skin ofthe forearm was carefully c1eanedusing a1cohol.
Iontophoresis has been used to deliver vasoactive substancesacross the skin of the forearm, avoiding the systemic effects thatcould interfere with the skin microcirculatory responses.In fact, thismethod allows to locally transfer charged drugs across the skinthrough a small electric current [17]. The current strengths chosen forour study were well tolerated by the majority ofthe subjects, whereasa mild prickling sensation was reported in a few cases.We have pre-viously evaluated the effect of iontophoresis current itself on skinblood flow: negligible changes were induced by the same durationand strength of the electric current we used in the present study. Adrug delivery electrode (PF 383; Perimed, Jarfàlla, Sweden) and anindifferent electrode (PF 384; Perimed) were used. The electrodechamber, with the laser probe placed in the middle, was attached tothe volar surface ofthe forearm by a double-sided adhesive disk, at alO-mm distance from the drug delivery electrode.
Before to be attached on the skin, the drug delivery electrodechamber was filled with 62.5 Jll of 1% ACh solution and with 62.5 Jllof 1% SNP solution. A battery-powered iontophoresis controller(Perilout 328, Power Supply) was used to provide the current for drugadministration. After registration of the baseline flow, ACh wasdelivered using an anodal current: six doses (0.1 mA for 20 s each)followed by another two doses(0.2 mA for 20 s and 0.3 mA for 20 s)were delivered with a 60-second interval between each single dose.The 60-second interval was needed to achieve the plateau of thehyperemia induced by each ACh delivery.
After a 1-min recovery period, SNP was delivered using a catho-dal current: two doses (0.1 mA for 20 s each) followed by one dose(0.2 mA for 20 s)with a 180-secondinterval between two successivedoses. The 180-second interval was needed to achieve the steactystate ofthe blood flow response followingeach SNP dose.
116 Nephron 2000;85:114-119
Before and during ACh or SNP delivery, the skin erythrocyte flowwas measured by means of a laser Doppler flowmeter (PerifluxPF4001, standard probe PF408, Perimed). The laser Doppler probewas fixed within the drug chamber to explore the same small area ofthe skin. A laser beam penetrates the skin and it is partially backscat-tered by moving blood cells. According to the Doppler principle, afrequencyshiftoccurs,generatinga signalthat is linearlyrelatedtored cellflow,as predictedby theoreticaland experimentalmodels[18-20]. The laserDoppleroutputswere recordedcontinuouslybyan interfaced computer equipped with acquisition software (PCNotebook; Zenith Data Systems, Taipei, Taiwan) and given as arbi-trary units (perfusion units, PU). Calibration was performed by adevice composed of colloidallatex partic1es,the Brownian motion ofwhich provides the standard value. The skin blood flow was deter-mined as the mean value recorded during 60 s at each delivery step.The absolute maximal response was defined as the flow reached afterthe last drug delivery.
The reproducibility of laser Doppler flowmetry has been studiedin stable emulsion with an intra-assay coefficient of variation ofabout6%[20].In humans,thetechniqueshowsacoefficientofvaria-tionof20-21 % [21].
In order to eliminate baseline variability, the blood flow re-sponses to ACh and SNP deliveries were expressed as percent changefrom the baseline [12, 22]. Similarly, the flow increment followingeach one of the eight iontophoretically applied ACh doses wasexpressed as percentage of the maximal endothelium-independentresponse to SNP as follows: 100.ACh-induced flow/max SNP-induced flow.
StatisticsAll results are expressed as mean :t SEM. Statistical evaluation
was performed using one-way Anova and the Student t test for paireddata. The hyperemic responses followingthe eight ACh delivery stepswereanalyzedby Anova for repeatedmeasures;Scheffé'stest wasapplied for multiple-comparison testing. Differences were consid-ered as statistically significant when p < 0.05.
Results
Figure 1 shows that the EHT patients have a bluntedresponse to ACh, whereas no difference between groupshas been observed as far as the responses to SNP wereconcerned. To confirm, in the CRF group, the absoluteincrement from baseline to maximal flow following AChdelivery was similar to that obtained by SNP delivery(30.8 :t 3.0 vs. 32.6 :t 4.2 PU, respectively; n.s.), as itoccurred in the NC group (25.7 :t 5.6 vs. 25.9 :t 5.4 PU,n.s.). On the other hand, in the EHT group, the maximalACh-induced increment of blood flow was significantlylower than that obtained by SNP (20.7 :t 2.3 vs. 39.1 :t6.3 PU; p < 0.01). Although CRF patients had lowerhematocrit values (table 1), they showed skin blood flowvalues similar to normals (5.1 :t 0.6 vs. 4.5 :t 0.6 PU;n.s.) at baseline.
Cupisti/Rossi/Placidi/F abbri/Morelli/Vagheggini/Meola/Barsotti
120
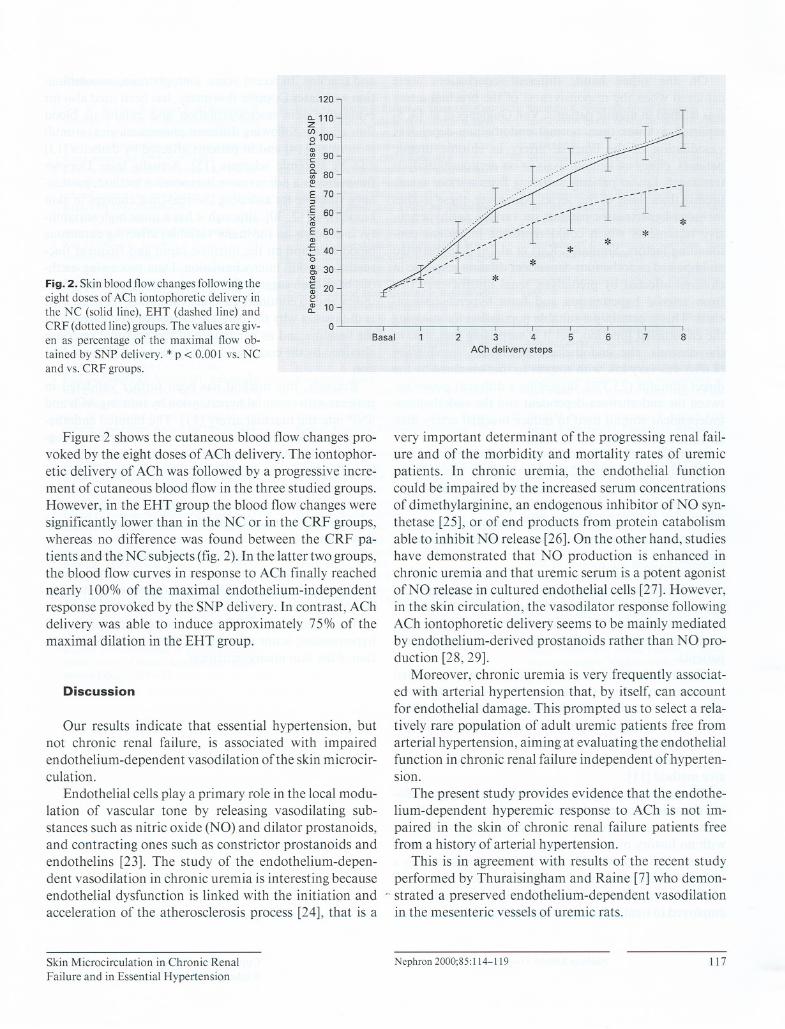
Fig. 2. Skin blood flowchanges followingtheeight doses of ACh iontophoretic delivery inthe NC (solid line), EHT (dashed line) andCRF (dotted line) groups. The values are giv-en as percentage of the maximal flow ob-tained by SNP delivery. * p < 0.001 vs. NCand vs. CRF groups.
~ 110(/)
8100eD
~ 90og- 80eE 70'".§ 60x'"E 50eD.!::~ 40o~ 30'"~ 20"~ 10
o
Figure 2 shows the cutaneous blood flow changes pro-voked by the eight doses of ACh delivery. The iontophor-etic delivery of ACh was followed by a progressive incre-ment of cutaneous blood flow in the three studied groups.However, in the EHT group the blood flow changes weresignificant1y lower than in the NC or in the CRF groups,whereas no difference was found between the CRF pa-tients and the NC subjects (fig. 2). In the latter two groups,the blood flow curves in response to ACh finally reachednearly 100% of the maximal endothelium-independentresponse provoked by the SNP delivery. In contrast, AChdelivery was able to induce approximately 75% of themaximal dilation in the EHT group.
Discussion
Our results indicate that essential hypertension, butnot chronic renal failure, is associated with impairedendothelium-dependent vasodilation ofthe skin microcir-culation.
Endothelial cells play a primary role in the local modu-lation of vascular tone by releasing vasodilating sub-stances such as nitric oxide (NO) and dilator prostanoids,and contracting ones such as constrictor prostanoids andendothelins [23]. The study of the endothelium-depen-dent vasodilation in chronic uremia is interesting becauseendothelial dysfunction is linked with the initiation andacceleration of the atherosclerosis process [24], that is a
Skin Microcirculation in Chronic RenalFailure and in Essential Hypertension
---1
-1
- --- _1- li r-- .--l
. *
1--- * *
-- ***
Basai 5 86 72 3 4
ACI'l deliverv steps
very important determinant of the progressing renal fail-ure and of the morbidity and mortality rates of uremicpatients. In chronic uremia, the endothelial functioncould be impaired by the increased serum concentrationsof dimethylarginine, an endogenous inhibitor of NO syn-thetase [25], or of end products from protein catabolismable to inhibit NO release [26].On the other hand, studieshave demonstrated that NO production is enhanced inchronic uremia and that uremic serum is a potent agonistofNO release in cultured endothelial cells [27]. However,in the skin circulation, the vasodilator response followingACh iontophoretic delivery seems to be mainly mediatedby endothelium-derived prostanoids rather than NO pro-duction [28, 29].
Moreover, chronic uremia is very frequent1yassociat-ed with arterial hypertension that, by itself, can accountfor endothelial damage. This prompted us to select a rela-tively rare population of adult uremic patients free fromarterial hypertension, aiming at evaluating the endothelialfunction in chronic renal failure independent ofhyperten-slon.
The present study provides evidence that the endothe-lium-dependent hyperemic response to ACh is not im-paired in the skin of chronic renal failure patients freefrom a history of arterial hypertension.
This is in agreement with results of the recent studyperformed by Thuraisingham and Raine [7] who demon-
" strated a preserved endothelium-dependent vasodilationin the mesenteric vesselsof uremic rats.
Nephron 2000;85:114-119 117

On the other hand, different conclusions wereachieved when the responsiveness of the brachial arterywas studied in uremic patients. Van Guldener et al. [4, 5]reported a lower than normal endothelium-dependentvasodilation of the brachial artery in chronic uremicpatients, either on hemodialysis or on peritoneal dialysistreatment, i.e., in patients suffering from a more severeuremia than those of our series. Moreover, these studiesincluded hypertensive patients on various antihyperten-sive treatments which could represent important con-founding factors. Similarly, Kari et al. [6] demonstratedan impaired endothelium-dependent dilation response inchildren affected by predialysis renal insufficiency freefrom arterial hypertension and from hypercholesterol-ernia. This is certainly a suitable population for studyingthe endothelial function, but it is surprising that, also inthe controls, the endothelium-dependent vasodilation(8.6%) was very low with respect to that obtained by thedirect stimulus (23.3%), suggestinga different power be-tween the endothelium-dependent and the endothelium-independent stimuli used to induce brachial artery dila-tion.
In addition, the differencebetweenbrachial artery andcutaneous vessels can reflect also different mechanismsof endothelium-dependent vasodilation [28, 29]. A pre-served endothelium-derived dilator prostanoid produc-tion in the skin vasculature of CRF patients, independentofNO generation changes,could contribute to explain ourfindings.
Althoughthe CRF group showedlowerhematocrit lev-elsthan normal, similar blood flowvaluesat baseline weredetected. This seems to exclude significant vasoconstric-tion or vasodilation that could overestimate or underesti-mate the responses to ACh or to SNP delivery in CRFpatients.
Our results also show that patients with essentialhypertension have a skin hyperemic response to ionto-phoretically applied ACh doses lower than that to SNPones. This is in keeping with the impairment of endothe-lium-dependent dilation in the skin microcirculation, al-ready described in hypertensive patients using an inva-sive method [11].
The present study represents the first attempt to evalu-ate the skin microcirculation responsiveness in patientswith essentialhypertension and in patients with CRF, butwith no history of arterial hypertension, using the ionto-phoretic delivery of ACh and SNP. Iontophoresis is atechnique commonly used to allow the local absorptionof drugs across the skin tissue. In clinical practice it isemployed to treat inflammatory diseasesof skin, muscles,
118 Nephron 2000;85:114-119
and tendons. In recent years, iontophoresis, in combina-tion with laser Doppler flowmetry, has been used also forevaluating skin microcirculation and cutaneous bloodflow changes followingdifferent pharmacological stimuliin normals [14] and in patients affected by diabetes [13]and by systemic sclerosis [15]. Actually laser Dopplerflowmetry is a noninvasive inexpensive method, particu-larly valuable for assessing the real-time changes in skinblood flow [12,30], although it has a quite high variabili-ty. It depends on the many variables affecting cutaneousblood flow and on the intrinsic rapid and frequent fluc-tuations of skin microcirculation. Data processing meth-ods have been suggestedto increase day-to-day reproduc-ibility and to eliminate baseline variability [12, 22]. Thisis the reason why the data are expressed as change fromthe baseline and as percentage of the maximal responseobtained by the endothelium-independent SNP vasodila-tion.
Recently, this method has been further validated inpatients with essential hypertension by infusing ACh andSNP into the brachial artery [11]. The blunted endothe-lium-dependent vasodilation observed using plethysmog-raphy in the muscle vascular bed was detected also bylaser Doppler in the cutaneous microcirculation. This sug-geststhat the skin vascular bed is a good 'window' to eval-uate endothelial function and validates the laser Doppleras a useful noninvasive tool for measurement of bloodflowchanges [12].
In summary, our results demonstrate a preserved hy-peremic response to iontophoretic delivery of ACh in theskin microcirculation of CRF patients, whereas it is im-paired in patients affected by EHT.
The suggeststhat CRF per se, independent of arterialhypertension, is not associated with endothelial dysfunc-tion of the skin microcirculation.
Cupisti/Rossi/Placidi/F abbri/Morelli/Vagheggini/Meola1Barsotti

References
I Gris JC, Branger B, Vecina F, AI Sabadani B,Fourcade J, Schved JF: Increased cardiovascu-lar risk factors and features of endothelial acti-
vation and dysfunction in dialyzed uremic pa-tients. Kidney Int 1994;46:807-813.
2 London GM, Guérin AP, Marchais SJ, PannierB, Safar ME, Day M, Métivier F: Cardiac andarterial interactions in end-stage renal disease.Kidney Int 1996;50:600-608.
3 Luke RG: Chronic renal failure - a vasculo-
pathic state. N Engl J Med 1998;339:841-843.4 Van Guldener C, Lambert J, Janssen MJFM,
Donker AJM, Stehouwer CDA: Endothelium-dependent vasodilatation and distensibility oflarge arteries in chronic haemodialysis pa-tients. Nephrol Dial Transplant 1997;12(suppl2):14-18.
5 Van Guldener C, Janssen MJFM, Lambert J,Steyn M, Donker AJM, Stehouwer CDA: En-dothelium-dependent vasodilatation is im-paired in peritoneal dialysis patients. NephrolDial Transplant 1998; 13:1782-1786.
6 Kari JA, Donald AE, Vallace DT, BruckdorferKR, Leone A, Mullen MJ, Bunce T, Dorado B,Deanfield JE, Rees L: Physiology and biochem-istry of endothelial function in children withchronic renal failure. Kidney Int 1997;52:468-472.
7 Thuraisingham RC, Raine AEG: Maintenanceof normal agonist-induced endothelium-de-pendent relaxation in uraemic and hyperten-sive resistance vessels. Nephrol Dial Trans-plant 1999;14:70-75.
8 Linder L, Kiowski W, Biihler FR, Liischer TF:Indirect evidence for the release of endothe-
lium-derived relaxing factor in the human fore-arm circulation in vivo: Blunted response inessential hypertension. Circulation 1990;81:1762-1767.
9 Panza JA, Quyyumi AA, Brush JE Jr, EpsteinSE: Abnormal endothelium dependent vascu-lar relaxation in patients with essenti al hyper-tension. N Engl J Med 1990;323:22-27.
IO Taddei S, Virdis A, Mattei P, Salvetti A: Vaso-dilation to acetylcholine in primary and sec-ondary forms of human hypertension. Hyper-tension 1993;21:929-933.
Skin Microcirculation in Chronic RenalFailure and in Essential Hypertension
II Rossi M, Taddei S, Fabbri A, Tintori G, Cre-didio L, Virdis A, Ghiadoni L, Salvetti A, Giu-sti C: Cutaneous vasodilation to acetylcholinein patients with essential hypertension. J Car-diovasc PharmacoI1997;29:406-411.
12 Schabauer AMA, Rooke TW: Cutaneous laserDoppler flowmetry: Applications and findings.Mayo Clin Proc 1994;69:564-574.
13 Morris SJ, Shore AC, Tooke JE: Responsesof the skin microcirculation to acetylcholineand sodium nitroprusside in patients withNIDDM. Diabetologia 1995;38:1337-1344.
14 Sernè EH, Stehouwer CDA, ter Maaten JC, terWee PM, Rauwerda JA, Donker AJM, GansROB: Microvascular function relates to insulin
sensitivity and blood pressure in normal sub-
jects. Circulation 1999;99:896-902.15 La Civita D, Rossi M, Vagheggini G, Credi dio
L, Fabbri A, Giusti C, Pasero R, Ferri C:Microcirculatory effects of acetylcholine andsodium nitroprusside in patients with systemicsclerosis: A preliminary investigation. ArchRheum Dis 1998;6:231-239.
16 Giovannetti S: Low-protein diets for chronicrenal failure; in Giovannetti S (ed): NutritionalTreatment of Chronic Renal Failure. Boston,Kluwer Academic Publishers, 1989, pp 179-190.
17 Harris R: Iontophoresis; in Licht E (ed): Physi-cal Medicine Library. Connecticut, ElizabethLicht, 1967, voI 4, pp 156-178.
18 Bonner R, Nossal R: Model of laser Dopplermeasurement ofblood flow in tissue. Appl Op-tics 1981 ;20:2097 -2107.
19 Nilsson GE, Tenland T, Oeberg PA: Evalua-tion of laser Doppler flowmeter far measure-ments oftissue blood flow. IEEE Trans Biomed
Eng 1980;27:597-604.20 Tenland T, Salerud KG, Nilsson KG, Oberg
PA: Spatial and temporal variations in humanskin blood flow.Int J Microcirc Clin Exp 1983;2:81-90.
21 Sundberg S: Acute effects and long-term varia-tion in skin blood flow measured with laser
Doppler flowmetry. Scand J Clin Lab Invest1984;44:341-345.
22 Silverman DG, Jotkowitz AB, Freemer M,Gutter V, O'Connor TZ, Braverman OIM: Pe-ripheral assessment of phenylephrine-inducedvasoconstriction by laser Doppler flowmetryand its potential relevance to homeostaticmechanisms. Circulation 1994;90:23-26.
23 Liischer TF, Vanhoutte PM: The Endothelium:Modulator of Cardiovascular Function. Boca
Raton, CRC Press, 1990, pp 1-215.24 Cooke JP, Tsao PS: Is NO an anti-atherogenic
molecule? Arterioscler Thromb 1994;14:653-655.
25 Vallace P, Leone A, Calver A, Collier L, Mon-cada S: Accumulation of an endogenous inhibi-tor of nitric oxide synthesis in chronic renalfailure. Lancet 1992;339:572-575.
26 Sorrentino R, Sorrentino L, Pinto A: Effect ofsome products of protein catabolism on theendothelium-dependent and -independent re-laxation of rabbit tharacic aorta rings. J Phar-macol Exp Ther 1993;266:626-633.
27 Noris M, Benigni S, Boccardo P, Aiello S, Gas-pari F, Todeschini M, Figliuzzi M, Remuzzi G:Enhanced nitric oxide synthesis in uremia: Im-plications for platelet dysfunction and dialysishypotension. Kidney Int 1993;44:445-450.
28 Noon JP, Walker BR, Hand MF, Webb DJ:Studies with iontophoretic administration of
drugs to human dermal vessels in vivo: Cholin-ergic vasodilation is mediated by dilatar pros-tanoids rather than nitric oxide. Br J Clin Phar-
macoI1998;45:545-550.29 K.han F, Davidson NC, Littleford RC, Litch-
field SJ, Struthers AD, Belch JJF: Cutaneousvascular responses to acetylcholine are me-diated by a prostanoid-dependent mechanismin mano Vasc Med 1997;2:82-86.
30 Rossi M, Cupisti A, Morelli E, Tintori G, Fab-bri A, Battini S, Vagheggini G, Barsotti G:Laser Doppler flowmeter assessment of skinmicrocirculation in uremic patients on hemo-dialysis treatment. Nephron 1996;73:544-548.
Nephron 2000;85:114-1 19 119