Embed Size (px)
Citation preview

1 | P a g e
Responsibility/ Adaptations in Pregnancy Additional Information
Hormones ➢ Maintaining homeostasis ➢ Regulation of growth ➢ Development and Cellular communication
Perinatal Nursing – 2021 Simpson, Creehan, O’Brien-Abel, Roth & Rohan Chapter three – Physiological Changes of Pregnancy Blackburn, Susan Tucker Page 48
Placenta
➢ Responsible for transfer of nutrients to the fetus and waste products away from the fetus
➢ Functions as the fetal lungs, gi, liver, kidney and endocrine organ
➢ Major Hormones ❖ hCG - Human chorionic gonadotropin ❖ hPL – Human Placental Lactogen ❖ Estrogen ❖ Progesterone ❖ Serves as an endocrine gland ❖ Major Hormones ❖ hCG - Human chorionic gonadotropin ❖ hPL – Human Placental Lactogen ❖ Estrogen ❖ Progesterone
❖ Placental Hormones are critical for many of the metabolic and endocrine changes during pregnancy
❖ Fetal bone growth and placental calcium transport is mediated by Parathyroid hormone related protein or PTHrP
❖ Corticotrophin-releasing hormone or CRH and PGs have a major role in initiation of myometrial contractility and labor onset
Page 49
➢ HCG ➢ Primarily secreted by the placenta Page 49
2 | P a g e
➢ Major function is to maintain progesterone and estrogen production by the corpus luteum until the placental function is adequate (approximately 10 weeks post-conception)
➢ Thought to have a role in fetal testosterone and corticosteroid production and angiogenesis
➢ Found in maternal serum by within 7-8 days after implantation
➢ Positive pregnancy test – 3 weeks after conception and 5 weeks after LMP
➢ Elevated in multiple and molar pregnancies ➢ Lower in ectopic or abnormal placentation
➢ Human Placental Lactogen (hCS)
➢ Produced by syncytiotrophoblast tissues of the placenta
➢ Growth parallel to the placental growth and peaks near term
➢ Critical for fetal growth as it alters maternal protein, carbohydrate and fat metabolism and acts as an insulin antagonist
➢ free fatty acid availability for maternal metabolic
and maternal glucose uptake and use o Allows glucose to be reserved for fetal use o Mother will be at a higher risk for ketosis
with significant in maternal food intake
Page 49
➢ Estrogens (estrone,
➢ Steroid hormones secreted by the ovaries in early pregnancy and by the placenta in late pregnancy
Page 49

3 | P a g e
estradiol & estriol)
➢ Prevents further ovarian follicular development during pregnancy
➢ Prepares the breast for lactation
➢ blood flow to the uterus, growth of the uterine muscle and enhances myometrial activity – involved in the timing and onset of labor
➢ Rapid last 6 weeks in pregnancy o Factor in onset of labor
➢ Progesterone ➢ Initially produced by the corpus luteum & later by the placenta
➢ Assists with implantation and myometrial relaxation – smooth muscle relaxer
o GI system
o Venous wall to accommodate in blood volume
➢ Respiratory center - CO2 sensitivity ➢ Aids in the structural development of the breast to
prepare for breastfeeding ➢ Mediates the changes in the immune system
o Prevents rejection of the fetus
Page 49
➢ Relaxin ➢ Secreted by the corpus lutum and later by the myometrium and placenta
➢ Inhibits uterine activity during pregnancy ➢ Plays a role in decidual development and
implantation
Page 49

4 | P a g e
➢ Prostaglandins ➢ From the family of eicosanoids which includes PGs, prostacyclins (PGI2s), thromboxanes and leukotrienes
➢ PGI2 & Thromboxane thought to contribute to hypertensive disorders
➢ Effect smooth muscle contractility o Mediate the onset of labor, myometrial
contractility and cervical ripening
➢ PGI2s & Thromboxane thought to contribute to hypertensive disorders – PCI2 is release is mediated by nitric oxide which regulates vascular tone and SVR
Page 50
➢ Prolactin ➢ Released from the anterior pituitary gland ➢ Increase in and maturation of ducts in the breast
to aid in breastfeeding o After removal of placenta, high levels of
estrogen disappear, signaling the anterior pituitary gland to produce prolactin
o Levels rise rapidly and are elevated by the infants suckling
Page 50
➢ Cardiovascular ➢ Heart is displaced upward, forward to the left
➢ Heart rate 15-20 beats/minute
➢ Exaggerated split of the first sound and audible third ♥ sound
➢ Stroke volume25-30%
➢ Cardiac output 30-50%
➢ Blood volume 40-60% with in Hematocrit
o RBC’s 20-30%
➢ WBC to 15,000
➢ Blood pressure is the second trimester
➢ Perfusion depends on the heart rate
➢ Benign systolic murmurs are common
➢ ECG changes: inverted P waves, small Q wave, tachyarrhythmias
➢ Physiologic anemia
➢ risk for clot formation o Venous thromboembolism DIC – Disseminated Intravascular Coagulation

5 | P a g e
➢ Widening of pulse pressure
➢ Hypercoaguable: procoagulant activity and fibrinolytic activity
➢ Plasma volume returns to normal after 6 weeks PP
➢ Post-partum – Left atrium appears enlarged due to the ↑in blood volume immediately following removal of placenta
Pages 50-52 ➢ Respiratory ➢ Pressure from the uterus shifts the diaphragm
upward approx. 4cm which the length of the lungs
o To compensate for this the chest enlarges 2cm
➢ Increased pressure from the uterus widens the substernal angle 50% and causes the ribs to slightly flare out
➢ Circumference of the thoracic cage may by 5-7 cm
➢ Ph 7.40-7.45
➢ PaCO2 27-32mmHg
➢ HCO3 18-21 mmHg
➢ Tidal volume 30-40% ➢ Expiratory Reserve Vol
▪ 15-20%
➢ Compensated respiratory alkalosis
➢ in Oxygen consumption ➢ Shortness of breath is a common
complaint Page 55
➢ Renal ➢ Glomerular filtration 40-60% ➢ Dilatation of the renal calyces, pelvis and ureters
are due to the effects of progesterone
➢ Proteinuria, Glycosuria and renal
clearance and in serum levels of some electrolytes more common

6 | P a g e
➢ Hypertrophy of the kidneys due to in blood volume
➢ Dilatation of the ureters on the right side is more pronounced than on the left side
o Cushioning that occurs due to the displacement of the uterus by the sigmoid colon.
o Filtered load of substance exceeds the tubular reabsorptive capacity
➢ Hydronephrosis and Hydroureter – may take 3-4 months to resolve post-partum
➢ Increased risk of urinary tract infections
o Due to increase in muscular relaxation, increase in urine volume and urinary stasis
➢ Gastrointestinal ➢ Nutritional requirements increase ➢ Common discomforts of pregnancy are due to
physiological and structural changes ❖ Heartburn, gingivitis, constipation, nausea
and vomiting
Page 57
➢ Mouth ➢ Gingival edema and hyperemia ❖ Begins in the 2nd month and peaks in the 3rd
trimester ➢ Gingival changes are related to increase in
vascularity and blood flow, changes in connective tissue and the release of inflammatory mediators
➢ in plaque and dental calculus
➢ in previous periodontal disease ➢ 3-5% have an epulis (tumor like enlargement (i.e.
lump) situated on the gingival or alveolar mucosa.) between their upper, anterior maxillary teeth
Page 57

7 | P a g e
❖ Regresses during post-partum but may reoccur with subsequent pregnancies
➢ Esophagus ➢ Decrease in lower esophageal sphincter (LES)muscle tone and pressure due to effects of progesterone
➢ LES function further altered after the uterus is large enough to change the positioning of the stomach & intestines and move the LES into the thorax
❖ Changes heartburn and reflux
Page 57
➢ Nausea and Vomiting
➢ Affects 70-80% of pregnant women ➢ Exact mechanism unclear ➢ Theories:
❖ Mechanical, endocrinologic, allergic, metabolic, genetic and psychosomatic
➢ Most frequent hormone linked is estrogen- particularly HCg
➢ Usually begins at 4-6 weeks and peaks at 8-12 weeks but may begin sooner and last longer
➢ TX- supportive ❖ Frequent small meals
➢ Hyperemesis Gravidarum –associated with weight loss, electrolyte imbalance, ketosis and dehydration more serious and requires fluid replacement
Page 57
❖ Stomach ❖ Progesterone
8 | P a g e
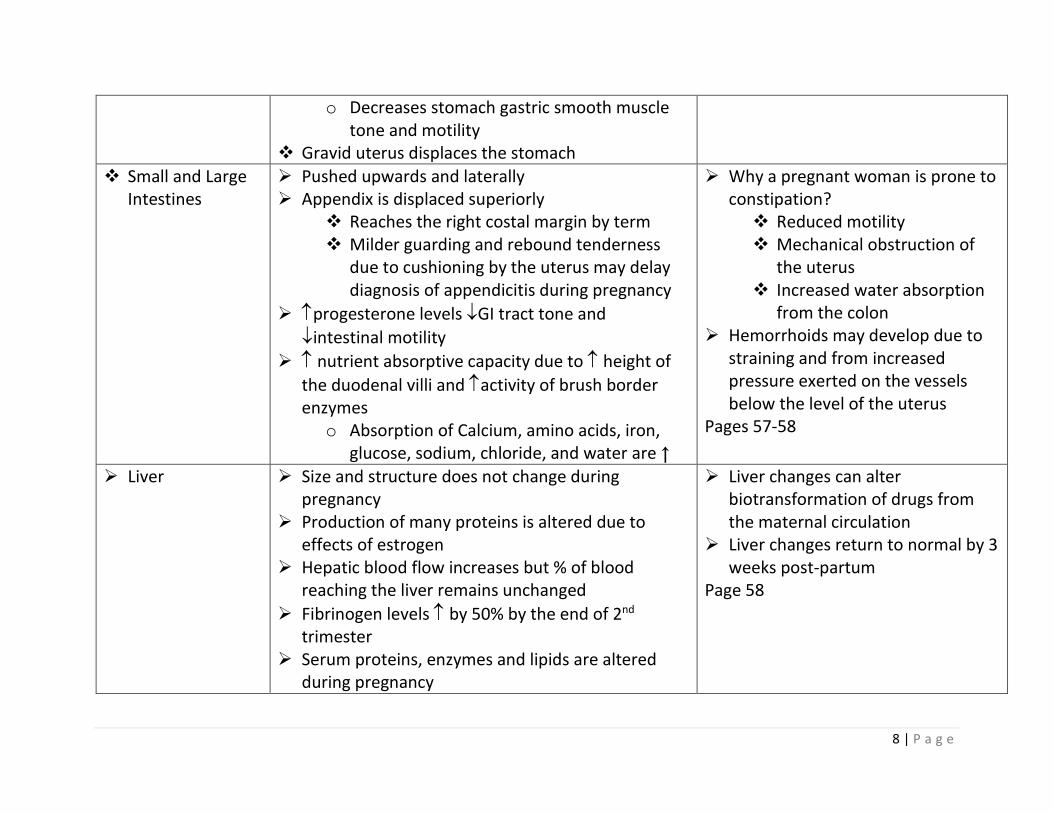
o Decreases stomach gastric smooth muscle tone and motility
❖ Gravid uterus displaces the stomach
❖ Small and Large Intestines
➢ Pushed upwards and laterally ➢ Appendix is displaced superiorly
❖ Reaches the right costal margin by term ❖ Milder guarding and rebound tenderness
due to cushioning by the uterus may delay diagnosis of appendicitis during pregnancy
➢ progesterone levels GI tract tone and
intestinal motility
➢ nutrient absorptive capacity due to height of
the duodenal villi and activity of brush border enzymes
o Absorption of Calcium, amino acids, iron, glucose, sodium, chloride, and water are ↑
➢ Why a pregnant woman is prone to constipation? ❖ Reduced motility ❖ Mechanical obstruction of
the uterus ❖ Increased water absorption
from the colon ➢ Hemorrhoids may develop due to
straining and from increased pressure exerted on the vessels below the level of the uterus
Pages 57-58
➢ Liver ➢ Size and structure does not change during pregnancy
➢ Production of many proteins is altered due to effects of estrogen
➢ Hepatic blood flow increases but % of blood reaching the liver remains unchanged
➢ Fibrinogen levels by 50% by the end of 2nd trimester
➢ Serum proteins, enzymes and lipids are altered during pregnancy
➢ Liver changes can alter biotransformation of drugs from the maternal circulation
➢ Liver changes return to normal by 3 weeks post-partum
Page 58
9 | P a g e
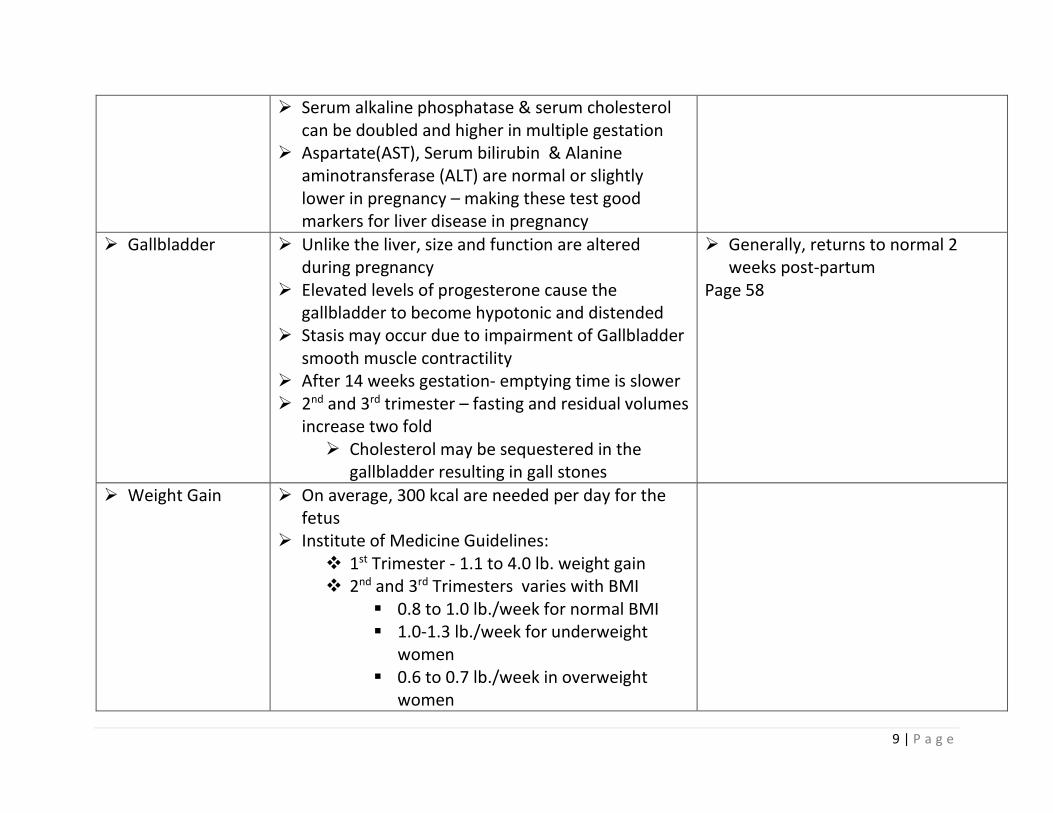
➢ Serum alkaline phosphatase & serum cholesterol can be doubled and higher in multiple gestation
➢ Aspartate(AST), Serum bilirubin & Alanine aminotransferase (ALT) are normal or slightly lower in pregnancy – making these test good markers for liver disease in pregnancy
➢ Gallbladder ➢ Unlike the liver, size and function are altered during pregnancy
➢ Elevated levels of progesterone cause the gallbladder to become hypotonic and distended
➢ Stasis may occur due to impairment of Gallbladder smooth muscle contractility
➢ After 14 weeks gestation- emptying time is slower ➢ 2nd and 3rd trimester – fasting and residual volumes
increase two fold ➢ Cholesterol may be sequestered in the
gallbladder resulting in gall stones
➢ Generally, returns to normal 2 weeks post-partum
Page 58
➢ Weight Gain ➢ On average, 300 kcal are needed per day for the fetus
➢ Institute of Medicine Guidelines: ❖ 1st Trimester - 1.1 to 4.0 lb. weight gain ❖ 2nd and 3rd Trimesters varies with BMI
▪ 0.8 to 1.0 lb./week for normal BMI ▪ 1.0-1.3 lb./week for underweight
women ▪ 0.6 to 0.7 lb./week in overweight
women

10 | P a g e
▪ 0.4 to 0.6 lb./week in obese women
➢ Metabolic Changes
➢ Adequate maternal weight gain, and changes in maternal glucose, protein and fat metabolism play an important role in fetal growth and development
➢ Pregnancy can be divided into 2 metabolic phases ❖ Initial anabolism dominant phase ❖ Later catabolism predominant phase
➢ Initial Anabolism Dominant Phase o Nutrient uptake, energy is
stored as fat and maternal weight gain
o Estrogen causes in insulin production due to stimulation of pancreatic beta cell hypertrophy and hyperplasia
o insulin promotes storage of
glucose as glycogen, fat synthesis, storage of triglycerides and fat, fat cell hypertrophy and inhibition of lipolysis
o Lipoproteins (low density and high density) increase
o Maternal protein storage increases, with a net retention of 1.3g/day of nitrogen for use by mother and fetus
➢ Later Catabolism Predominant Phase ❖ Maternal weight gain is due
to fetal growth

11 | P a g e
❖ Adipose tissue lipolytic activity is enhance
❖ in Plasma, free fatty acids, glycerol and ketones
• These provide for alternative energy sources for the mother since the fetus is an obligatory user of glucose who cannot readily break down fat for energy
❖ Maternal urinary nitrogen excretion decreases conserving protein for fetal transfer
❖ Maternal insulin levels increase as insulin resistance in the peripheral tissues becomes prominent
Page 59 ➢ Insulin in
Pregnancy ➢ Insulin antagonism is caused by hCS (Human
Placental Lactogen) and other placental hormones (progesterone, estrogen, cortisol and prolactin)
o Promote lipolysis and oppose the action of insulin
Page 59

12 | P a g e
➢ Normally insulin aids in glucose from the blood and promote glycogen and fat storage
➢ Insulin resistance (insulin sensitivity by 50-70%) causes maternal glucose levels to be higher after a meal to allow for glucose to be transferred to the fetus ❖ Diabetogenic State
• Relative hyperinsulinemia and hyperglycemia of pregnancy caused by a
sensitivity to insulin in the liver and peripheral tissues which leads to a persistent relative hyperglycemia after meals
❖ Maternal metabolic responses alter responses on glucose tolerance tests
• Lower initial fasting glucose
o Due to glucose utilization
and fat utilization enhancing glucose availability for the fetus
&
o blood glucose for a longer period of time after ingestion carbohydrates( due to insulin antagonism
and insulin sensitivity)

13 | P a g e
➢ Endocrine ➢ Thyroid Gland ❖ Production, circulation and disposal of the
thyroid hormone are altered during pregnancy
❖ Increased vascularity and hyperplasia of thyroid gland ▪ Increase in hormone production ▪ Increase in thyroid size but not goiter
like-in populations with adequate iodine supplies
❖ Most changes occur in the 1st half of pregnancy –T4 are elevated “euthyroid hyperthyroxinemia” ▪ Due to estrogen, TBG (Thyroxine
Binding Protein) and hCG which
stimulates T3 and T4 and urinary iodide excretion
➢ T4 and T3 by 10 -15 weeks and remain higher to term
❖ Free T4 & T3 during 1st trimester but 2nd and 3rd trimester as Thyroxine-binding
globulin (TBG) ▪ Serum T4 &T3 levels reduced due to
extra binding of thyroid hormones from TBG
➢ Maternal iodine needs increase during pregnancy
➢ More t4 and T3 are produced but
because they are bound to TBG the serum levels are reduced

14 | P a g e
➢ Maternal thyroid hormone is critical for fetal CNS development ❖ Especially during early pregnancy prior to
the fetus ability to produce thyroid hormone(T4)
❖ Poor control can lead to fetal loss and altered fetal brain development, and both altered neurocognitive and development impairments.
➢ Subclinical Hyperthyroidism ❖ Occurs in approximately 3.5-18% of healthy
populations ❖ Hard to distinguish due to normal s/s of
pregnancy- Hyperthyroidism - heat intolerance, tachycardia, wide pulse pressure and vomiting and Hypothyroidism – constipation, fatigue, weight gain and muscle cramps
❖ If left untreated could result in pregnancy loss, thyroid crisis, and preterm labor
➢ Transient Post-Partum Thyroid Disorder (PPTD) ❖ Autoimmune base occurring 4-9% of
postpartum women and thought to be autoimmune based
❖ 2-4 months of mild hyperthyroidism, followed by a period of hypothyroidism with a return to normal at 12 months pp.
Page 60

15 | P a g e
▪ 25% of these women develop permanent hypothyroidism within 5-15 years
➢ Pituitary Gland ➢ Anterior Pituitary gland > in weight by 30% and 2-fold in volume
➢ Becomes more convex and dome shaped
o Changes are due to in prolactin o ACTH- Adrenocorticotropin secretion and
serum levels ▪ Peaking during intrapartum
➢ Pituitary Growth Hormone
➢ By the placental growth hormone which 15-20 weeks gestation to term
➢ FSH (stimulates follicle growth) & LH (needed for ovulation) are inhibited during pregnancy
➢ Posterior Pituitary Gland ❖ Oxytocin and AVP ❖ Oxytocin
▪ Influences contractility of uterus after birth
▪ Stimulates milk ejection ❖ AVP
▪ Also called the antidiuretic hormone ▪ Causes vasoconstriction when
released in large amounts and BP ▪ Major action is the antidiuretic action
to regulate H2O balance
16 | P a g e
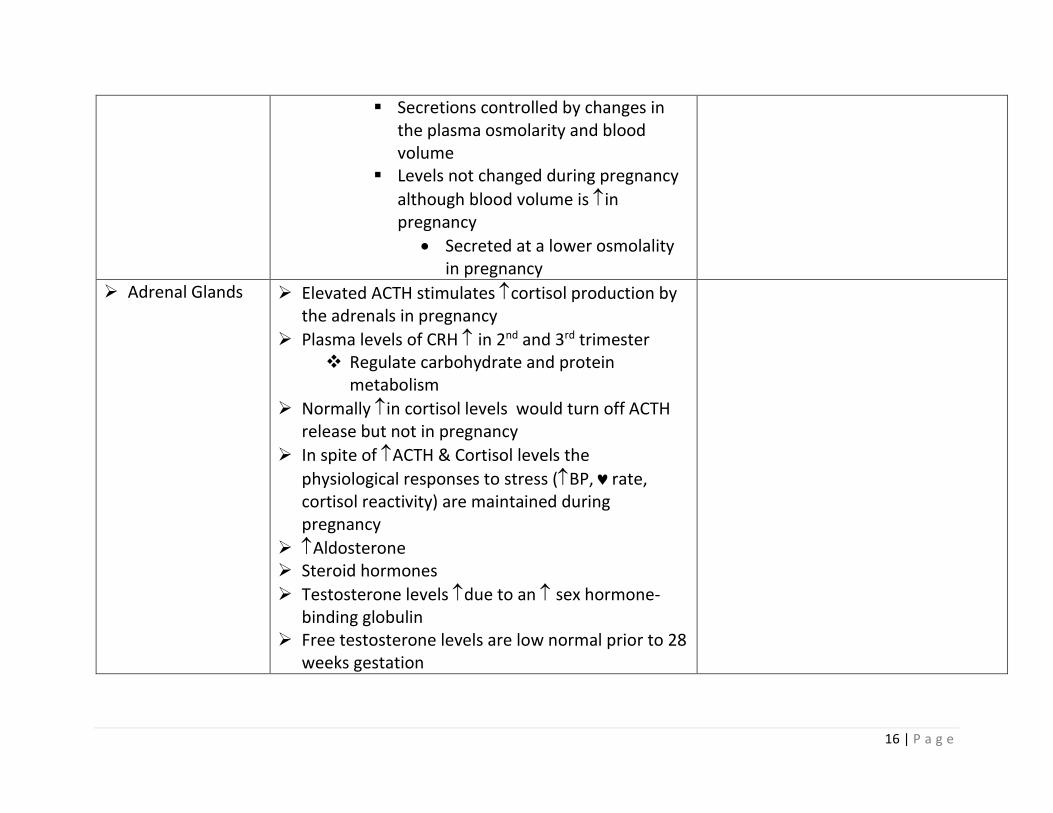
▪ Secretions controlled by changes in the plasma osmolarity and blood volume
▪ Levels not changed during pregnancy
although blood volume is in pregnancy
• Secreted at a lower osmolality in pregnancy
➢ Adrenal Glands ➢ Elevated ACTH stimulates cortisol production by the adrenals in pregnancy
➢ Plasma levels of CRH in 2nd and 3rd trimester ❖ Regulate carbohydrate and protein
metabolism
➢ Normally in cortisol levels would turn off ACTH release but not in pregnancy
➢ In spite of ACTH & Cortisol levels the
physiological responses to stress (BP, rate, cortisol reactivity) are maintained during pregnancy
➢ Aldosterone ➢ Steroid hormones
➢ Testosterone levels due to an sex hormone-binding globulin
➢ Free testosterone levels are low normal prior to 28 weeks gestation

17 | P a g e
➢ Parathyroid Glands
➢ Parathyroid hormone (PTH) 1st trimester then at term ❖ Early decrease is due to PTHrP production by
the fetus and placenta ➢ Regulation of calcium is closely r/t magnesium,
phosphate, PTH, vitamin D and calcitonin levels ❖ Any alteration in one is likely to affect the
other
▪ in magnesium or calcium PTH levels
▪ in magnesium or calcium PTH levels
➢ Total serum calcium falls in pregnancy primarily related to the fall in albumin, lowest reaching 28-
32 weeks then plateaus and slightly at term ➢ Overall calcium not changed, however daily
maternal calcium intestinal absorption and doubles by the 3rd trimester to assist with fetal bone development in late pregnancy. Maternal overall bone mass is not loss during pregnancy
Pages 60-61
➢ Immune System ➢ Cytokines ➢ PGE2 ➢ Steroid Hormones ➢ Estrogen ➢ hCG ➢ Various pregnancy-specific proteins exert
immunosuppressive effects during pregnancy
Page 61

18 | P a g e
➢ Immune Innate Responses in Pregnancy
❖ in WBCs (especially neutrophils and monocytes)
➢ Immune Adaptive Responses in Pregnancy ❖ B and T lymphocyte responses ❖ Switch in balance of Th1 to Th2 cytokines
(subsets of T-lymphocytes)
▪ Th2 cytokines are which enhance antibody-mediated immunity
▪ T lymphocytes and Th1 cytokines are
which associated with tissue rejection
❖ Slight in IgG may risk of bacterial colonization
❖ Selective localized immunosuppression may
occur and the risk of viral and mycotic infections
➢ Neuromuscular and Sensory Systems
➢ In general no major CNS changes in pregnancy ➢ Mild frontal headaches 1st and 2nd trimester may
be due to tension or hormones Severe headache after 20 weeks gestation may be an indicator of preeclampsia ➢ Dizziness may be due to
❖ Vasomotor instability ❖ Postural hypotension
• After long periods of sitting/standing ❖ Hypoglycemia

19 | P a g e
➢ Musculoskeletal ➢ Posture ➢ Gait ➢ Ligament laxity ❖ “loose” ligaments ❖ Early in pregnancy due to effects of
progesterone and relaxin
• To facilitate birth ➢ Center of gravity changes ➢ Posture changes ➢ Separation of the rectus abdominis due to the
pressure of the growing uterus ❖ Producing Diastasis Recti
➢ Risk of ligament injury, muscle cramps, back & joint pain & falls
➢ May develop Restless Leg Syndrome (Willis Ekbom Disease) in the 3rd trimester which usually disappears after 1 month post-partum
➢ Sleep ➢ Sleep pattern changes ❖ Mediated by mechanical forces and
hormonal changes
❖ in sleep time ❖ Insomnia ❖ Night awakenings, often related to:
• Nocturia • Fetal activity • Backache
20 | P a g e
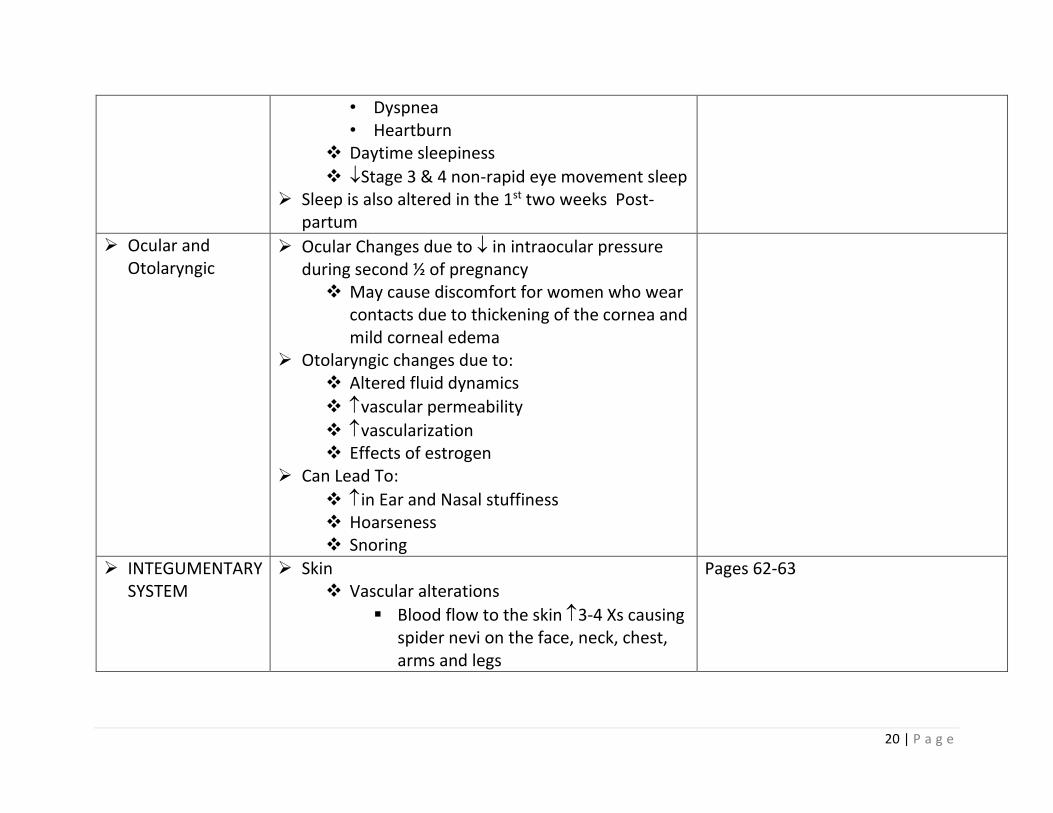
• Dyspnea • Heartburn
❖ Daytime sleepiness
❖ Stage 3 & 4 non-rapid eye movement sleep ➢ Sleep is also altered in the 1st two weeks Post-
partum
➢ Ocular and Otolaryngic
➢ Ocular Changes due to in intraocular pressure during second ½ of pregnancy ❖ May cause discomfort for women who wear
contacts due to thickening of the cornea and mild corneal edema
➢ Otolaryngic changes due to: ❖ Altered fluid dynamics
❖ vascular permeability
❖ vascularization ❖ Effects of estrogen
➢ Can Lead To:
❖ in Ear and Nasal stuffiness ❖ Hoarseness ❖ Snoring
➢ INTEGUMENTARY SYSTEM
➢ Skin ❖ Vascular alterations
▪ Blood flow to the skin 3-4 Xs causing spider nevi on the face, neck, chest, arms and legs
Pages 62-63

21 | P a g e
o Related to increased subcutaneous blood flow and estrogen
❖ Palmar erythema ▪ Normal vascular change in pregnancy
but has been associated with liver and collagen disease
❖ Striae Gravidarum (Stretch Marks) ▪ May occur on the hips, breast, upper
thighs but are usually more pronounced on the abdomen
▪ Occur in approximately 50% of pregnancies
▪ Due to normal stretching of the skin and softening and relaxing of the dermal collagenous and elastic tissues during the last months of pregnancy
❖ in estrogen and progesterone
▪ May cause an in melanocyte-
stimulating hormone → hyperpigmentation in the integumentary system
▪ Darkening of the nipples, areolae and perianal and genital areas occur
▪ Linea alba becomes the Linea nigra o Divides the abdomen from the
sternum to the symphysis

22 | P a g e
▪ “Mask of pregnancy” – Melasma (previously referred to as chloasma)
o Brown splotches - Mask like distribution on the cheeks, forehead and eyes
o Disappears after pregnancy but could reoccur with excessive sun exposure
➢ Hair ❖ In early stage of pregnancy the number of
hairs in the growth phase remain stable
❖ In later stages, hormonal levels the
number of hairs in the growth phase and the number of hairs in the resting phase
❖ After delivery the proportion of hairs that enter the resting phase doubles ▪ Women may see a hair loss 2-4
months postpartum ➢ Nails
❖ Occasional changes ▪ Transvers grooving
▪ softening/ brittleness
➢ Uterus ➢ Prior to pregnancy is a small, semisolid pear shaped organ weighing approx. 40-50 g.
➢ At the end of pregnancy weighs approx. 1,100 to 1,200 g.
➢ Regulated by the BP and SVR (Systemic Vascular Resistance)
➢ Supine position compresses inferior
vena cava and aorta, blood flow

23 | P a g e
❖ At the beginning of the pregnancy the uterine wall thickens due to hypertrophy of
the myometrial cells from estrogen and progesterone levels
❖ At the end of the pregnancy the uterine wall becomes thinner to allow for palpation of contractions and fetal position
➢ Receives 10-20% of cardiac output
➢ 700 to 800 ml/minute perfusion→ 80% is directed to the placental bed
➢ Maternal position, maternal arterial pressure and uterine contractility influence uterine blood flow
Page 63
➢ Cervix ➢ Changes are characterized by :
❖ Vascularity o Causes a softening and bluish
discoloration – Chadwick's Sign
❖ Water Content ❖ Softening ❖ Dilation
➢ Estrogen stimulates glandular tissue of the cervix ➢ Endocervical glands secrete a thick, tenacious
mucus which forms the mucous plug and prevents bacteria from entering the uterus
➢ Hyperactive glandular tissue causes an in normal mucous production
➢ Ovaries ➢ Ovulation ceases in pregnancy

24 | P a g e
➢ Corpus luteum persists and secretes progesterone until the 10th to 12th week ❖ This maintains the endometrium until
adequate progesterone can be secreted by the placenta
➢ Vagina ➢ Vaginal epithelium and muscle layers in response to estrogen undergo: ❖ Hypertrophy
❖ in vascularization ❖ Hyperplasia
➢ Loosening of the connective tissue and thickening
of the mucosa vaginal secretions
❖ Thick, white and acidic → play a role in infections
➢ At the end of pregnancy the vaginal wall and perineal body are relaxed enough to allow stretching of the tissues and delivery of the infant
Page 63
➢ Breast ➢ size and nodularity to prepare for lactation ➢ Nipples become more easily erectile and veins are
more prominent
➢ Areola pigmentations ➢ Montgomery follicles, sebaceous glands located in
the areola hypertrophy ➢ Striae may develop ➢ Colostrum – yellow secretion rich in antibodies
may leak during the last trimester of pregnancy
Page 63 and 64
25 | P a g e
➢ Feelings of fullness, tingling, and sensitivity begin in the 1st few weeks of gestation
REFERENCES
❖ Association of Women’s Health, Obstetric, and Neonatal Nurses (2015). Fetal Heart Rate Monitoring: Principles and Practices. 5th Edition. Kendall/Hunt Professional. Washington, DC: AWHONN.
❖ Simpson, K.R, Creehan, P.A., O’Brien-Abel, N., Roth, C.K. & Rohan, A. J. (2021). AWHONN Perinatal Nursing ( 5th ed). Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins
❖ Blackburn, S.T. (2018). Maternal, Fetal, & Neonatal Physiology. (5th ed). Maryland Heights, MO: Elsevier Saunders.
❖ Davidson, M.R., London, M.L. & Ladewig, P.A. (2020). OLDS’ Maternal-Newborn Nursing & Women’s Health Across the Lifespan. (11th ed). Boston, MA: Pearson
❖ https://www.youtube.com/watch?v=nIog3oizP8A retrieved February 24th, 2016.