Embed Size (px)
Citation preview
RESTRAINING MEASURES IN THE PSYCHIATRIC HOSPITAL AND CORRELATIONS WITH DIAGNOSIS AND TREATMENT
RESTRAINING MEASURES IN THE PSYCHIATRIC HOSPITAL AND CORRELATIONS
WITH DIAGNOSIS AND TREATMENT
UNIVERSITY OF MEDICINE AND PHARMACY OF TÎRGU MUREȘ
Author: Alexandra Paula SărmășanCoauthor: Melania Renata Simon
Coordinator: Lect. Adriana Mihai As. Prof. Istvan Zsolt Szasz

Violence is a negative deviation of the healthy behavior; having a multifactorial etiology, numerous risk factors and psycopathological manifestations, the required treatment
measures are both necesary and controversial: the restraining measures.
Restraining measures are representing the restriction of a persons freedom and movement to prevent the free
movement of one arm, both arms, a leg or both legs or to completely immobilize the patient by specific means of
protection to not cause injury.
INTRODUCTION

The purpose of this study was to evaluate the risk of restraint and correlations with diagnosis and treatment of hospitalized
patients in the Acute Psychosis department of Psychiatric Hospital, Tîrgu-Mureș.
OBJECTIVE
We realised a retrospective study based on:
• one year data collection (2014-2015) • sample of 50 patients• demographic data(age, gender, residency) • clinical data(diagnosis, treatment, restraining reasons) • data collection: patient`s medical paper and restaining register • department of acute psychosis of Psychiatry Clinic II of Tîrgu-Mureș
Method of analysis:
• program of data analysis MedCalc• Microsoft Excel
MATERIAL AND METHOD
Gender ratio
RESULTS
60%• 30 Male out of 50 patients
40%• 20 Female out of 50 patients

40%
Rural
Urban
RESULTS
60%
schizophre-nia
22%
al-co-hol
abuse
dis-or-der and
Preponderant diagnosis
brief psychoticdisorder 10%
major depressive disorder 16%
RESULTS

0%
10%
20%
30%
40%
50%
60%
70%
80%Elected drugs
771,4%1
50%
35,7%
RESULTS

Schi
zoph
reni
a
Major
Dep
ress
ive
Disor
der
Alcoh
ol A
buse
Brief p
sych
otic D
isor
der
Diagnosis and medication
Clonazepanum Valproic acid Zopiclonum
RESULTS

Correlation between residency and diagnosis
Schizophrenia Alcohol Abuse Major Depressive Disorder
Brief Psychotic Disorder
Urban N=9 69,23% N=4 44,44% N=2 40% N=3 60%
Rural N=4 30,76% N=5 55,55% N=3 60% N=2 40%
RESULTS
RESULTS
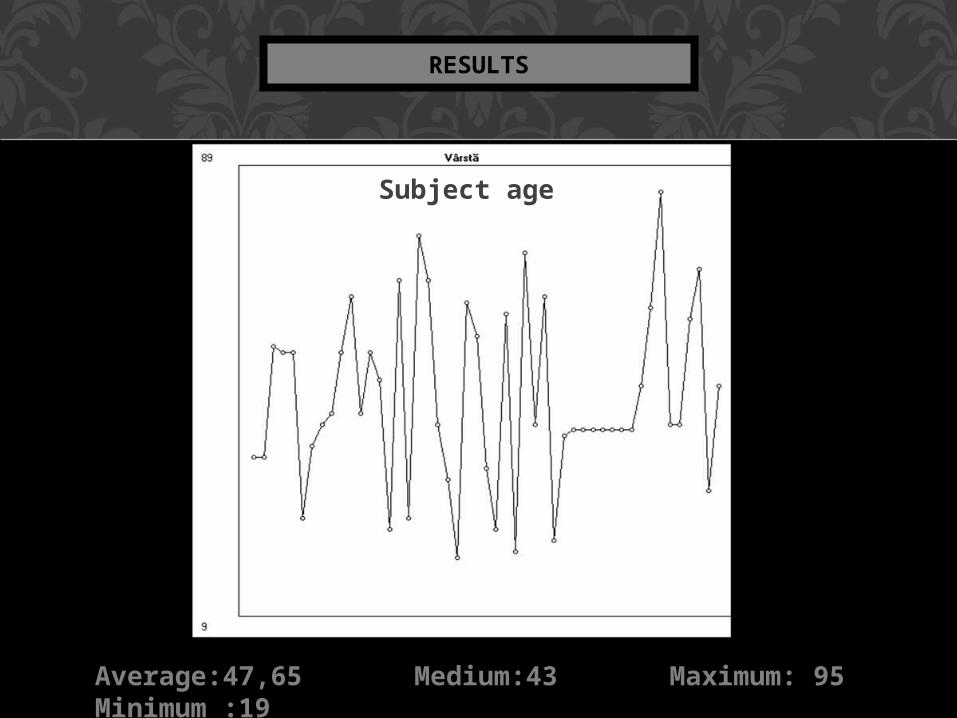
Average:47,65 Medium:43 Maximum: 95 Minimum :19
Subject age

RESULTS
Correlation between restraint and:
Schizophrenia Alcohol Abuse Major Depressive Disorder
Brief Psychotic Disorder
Aggressivebehaviour disorders
P=0,016(significant association)RR = 11,3 (pozitive association)
P=0,68 (insignificant association)RR=0,52(negative association)
P=0,89(insignificant association)RR=1,22(no association)
P=0,89(insignificant association)RR=1,22(no association)
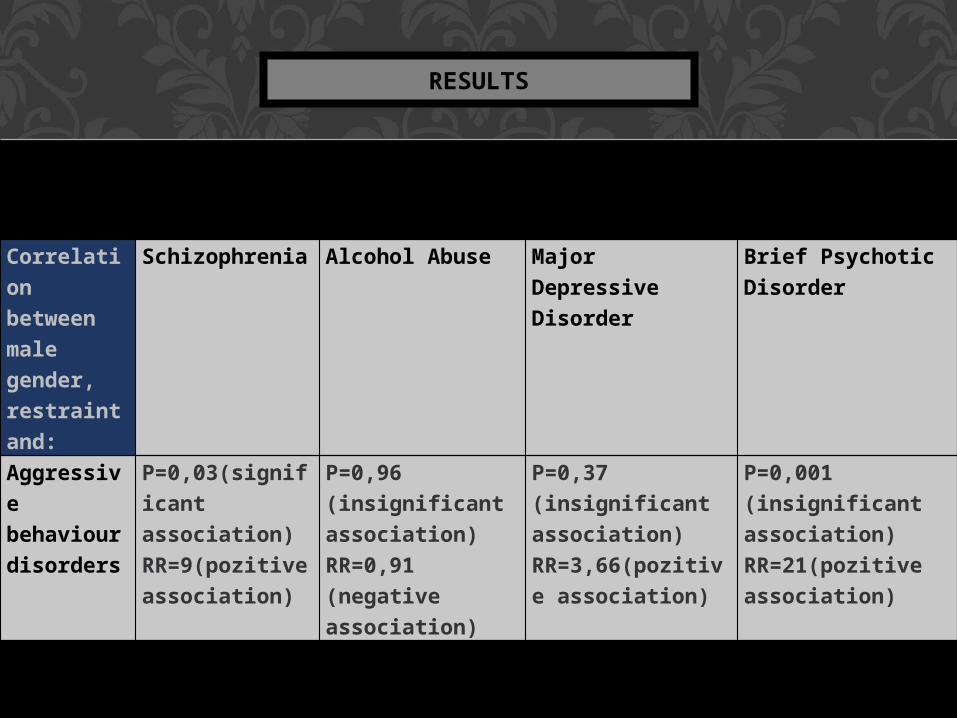
Correlation between male gender, restraint and:
Schizophrenia Alcohol Abuse Major Depressive Disorder
Brief Psychotic Disorder
Aggressive behaviour disorders
P=0,03(significant association)RR=9(pozitive association)
P=0,96 (insignificant association)RR=0,91 (negative association)
P=0,37 (insignificant association)RR=3,66(pozitive association)
P=0,001 (insignificant association)RR=21(pozitive association)
RESULTS
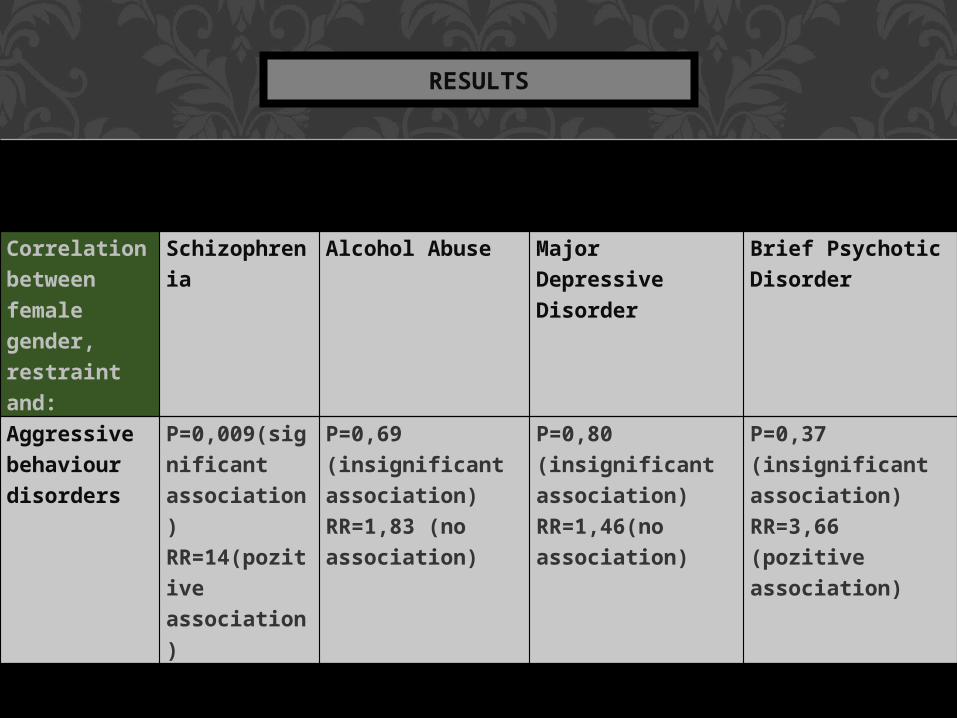
Correlation between female gender, restraint and:
Schizophrenia
Alcohol Abuse Major Depressive Disorder
Brief Psychotic Disorder
Aggressivebehaviour disorders
P=0,009(significant association)RR=14(pozitive association)
P=0,69 (insignificant association)RR=1,83 (no association)
P=0,80 (insignificant association)RR=1,46(no association)
P=0,37 (insignificant association)RR=3,66 (pozitive association)
RESULTS

From a number of 14 diagnosis found in data retrieval, Schizophrenia, Major Depressive Disorders, Alcohol Abuse and Brief Psychotic Disorder are the predominant diagnosis with a prevalence of 22%, 16% and 10%.
We observed that:
• masculine gender prevails with a percentage of 60% (n=30) aged between 22-85 years.
• female gender followed it with a percentage of 40%( n=20 ), aged between 19-75 years.
• a significant number of patients with urban recidency are diagnosed with Schizophrenia, and those with rural recidency are diagnosed with Alcohol Abuse
DISCUSIONS
• an increased restraining risk ratio exists at patients diagnosed with Schizophrenia and aggressive behaviour
disorders
• male patients with Brief Psycotic Disorder and aggressive behaviour disorders had a raising risk ratio of restraining comparative to other diagnosis or manifestation disorders
• female patients with Schizophrenia and Aggressive Behaviour disorders had an significant risk ration
comparative to other diagnosis or associated disorders
DISCUSIONS

The elected drugs were: • Clonazepamum 71.4%• Alprazolamum, Valproic acid and Midazolamum 50%• Diazepamum, and Haloperidolum 35.7%
Also, reviews of specialized literature on restrained patients showed that researches on the subject included demographic and precipitant characteristics, and it had been discovered that younger patients diagnosed with schzophrenia are at a considerable major risk of restraining than patients with other ages and diagnosis.
DISCUSSIONS

We noticed an increased risk of restraint :
1. young male patients
2. urban residency
3. diagnosis of Schizophrenia
4. male patients with Brief Psycotic Disorder
5. female patients with Schizophrenia
6. control treatment is composed of antipsychotic medication like anxiolytics(Clonazepamum, Alprazolamum, Diazepamum) and conventional antipsychotics(Haloperidolum, Zopiclonum)
CONCLUSIONS
1. Legea sănătăţii mintale şi a protecţiei persoanelor cu tulburări psihice nr. 487, 11 iulie 2002/republicata în 9 septembrie 2012)
2. Codul penal, Decretul 313/1980
3. Mihai A., Agresivitatea, o abordare bio-psiho-sociala. Editura Risoprint, 2013, 350-352.
4. Flannery RB Jr1, Walker AP., Characteristics of patients in restraint: fifteen-year analysis of the Assaulted Staff Action Program (ASAP) with EMS implications. Int J Emerg Ment Health. 2008 Summer;10(3):191-6.
5. Wanda K. M., Restraints and the code of ethics: An uneasy fit, Psychiatric Mental Health Nursing, UMDNJ School of Nursing, Stratford, NJ, Published Online: August 07, 2009
6. Hecser L., Ardelean M, Jung H., Psihiatria si medicina legală: elemente correlative, University Press Tg. Mureș, 2008, 56.
7. Birț M.A. , Phihiatrie, prolegomena clinice. Ed. Dacia, Cluj Napoca 2001, 599-600.
8.Boncu Ş., Psihologie socială, Comportamentul agresiv, Cursul 30 http://www.psih.uaic.ro/~sboncu/romana/Curs_psihologie_sociala/Curs30.pdf
9. http://e-psihiatrie.ro/medicatia-psihiatrica/
BIBLIOGRAPHY

10. Marian G., Baloescu A., Comportamentul agresiv. Editura Tritonic, 2009, 81
11. Nestor PG., Mental Disorder and Violence: Personality Dimensions and Clinical Features, American Journal of Psychiatry, 159, 1978
12.NICE guidelines [CG115]: Alcohol-use disorders: diagnosis, assessment and management of harmful drinking and alcohol dependence. Published date: February 2011
13. NICE guidelines [CG178]: Psychosis and schizophrenia in adults: treatment and management, Published date: February 2014.
14. Binder R.L. and McNeil D.E.: The Effects of Diagnosis and Context on Dangerousness, American Journal of Psychiatry,1998, 145: 728–32.
15. American Psychiatric Associacion. Diagnostic and Statistical Manual of Mental Disorders DSM IV-TR fourth edition, text revision, Washington DC: American Psychiatric, 2000
BIBLIOGRAPHY





























