Embed Size (px)
Citation preview

Results of a Job Analysis of PsychologistsWorking in State Hospitals
Ä
Patrick W. Corrigan, Larry Hess,and Andrew N. GarmanUniversity of Chicago Center for Psychiatric Rehabilitation
The graduate training of psychologists should prepare them for centralroles in state hospitals, especially roles involving direct patient care andsupervision of colleagues. To what extent do actual job practices matchgraduate preparation? To find out, 55 psychologists from 12 state hospi-tals in the Midwest were surveyed regarding their educational back-grounds and time currently spent in various job activities. Results indicatedthat paperwork consumes more time than any other activity, followed bytherapeutic services, psychological assessment, supervision, and case man-agement. Almost 50% of the sample was trained under a cognitive-behavioral orientation; however, more than 60% of survey participantsnow practice according to eclectic models. These results imply that psy-chologists in these settings may not be utilized to their full potential becauseof a variety of organizational constraints. © 1998 John Wiley & Sons, Inc.J Clin Psychol 54: 11–18, 1998.
The quality of treatment conducted in state mental health hospitals has been criticized as beinglargely unreflective of state-of-the-art practices and, for the most part, ineffectual (Torrey et al.,1990). Much is known about what this state-of-the-art should look like, both in terms of overalltherapeutic philosophy as well as specific intervention strategies. In this paper, psychologistsfrom several Midwestern hospitals were surveyed to determine how their job practices corre-spond with the state-of-the-art.
State-of-the-art treatment of the hospitalized patient typically includes careful symptomassessment and administration of corresponding psychotropic medication. Psychologists arefrequently called on to use their assessment acumen in monitoring patients’ symptoms. Ideally
We wish to thank Joseph Mehr, Ph.D., for assistance in obtaining permission to complete this study, for distribution ofthis survey to state operated facilities, and for a cogent review of an early version of this manuscript. Our appreciationis extended to Brett Buican for data collection and management. Please address all correspondence to Patrick Corrigan,University of Chicago Center for Psychiatric Rehabilitation, 7230 Arbor Drive, Tinley Park, IL 60477.
JOURNAL OF CLINICAL PSYCHOLOGY, Vol. 54(1), 11–18 (1998)© 1998 John Wiley & Sons, Inc. CCC 0021-9762/98/010011-08

these assessments will be behaviorally defined by severity scales anchored to clear, operation-alized definitions (Lukoff, Ventura, Nuechterlein, & Liberman, 1992). However, medicationtherapies are by no means sufficient to treat all problems that severely mentally ill adults suffer(Liberman, Corrigan, & Schade, 1989). Psychiatric rehabilitation is also a necessary compo-nent of comprehensive patient care and tends to more fully reflect the influence of clinicalpsychology.
Successful and responsible psychiatric rehabilitation is a multifaceted intervention that,depending on the patient, includes functional assessment (Vaccaro, Pitts, & Wallace, 1992),incentive therapies (Ayllon & Azrin, 1968; Paul & Lentz, 1977), social and coping skills train-ing (Liberman, DeRisi, & Mueser, 1989), generalization training (Stokes & Baer, 1977), andbehavioral family management (Anderson, Reiss, & Hogarty, 1986; Falloon, Boyd, & McGill,1984). Although many of these interventions can be provided to patients individually, they aremore efficiently, and perhaps most effectively, provided in groups. Severely disabled patientsalso require ongoing case managers who help to coordinate the various care providers thatdeliver these interventions (Test & Stein, 1978).
How has psychiatric rehabilitation been influenced by the various schools of psychother-apy? Principles of behavior therapy tend to dominate rehabilitation models (Bellack & Mueser,1993; Liberman, 1992). Most targets of intervention are defined in terms of discrete and mea-surable behaviors. Most intervention strategies are based on learning principles and incentives.In addition, rehabilitation principles have been significantly affected by the human potentialmovement (Anthony & Nemec, 1984; Bachrach, 1992). Human potential concepts such as“change” in functioning and “growth” toward improved quality of life are fundamental assump-tions of rehabilitation programs. The recipient of services is seen as having a central role inguiding rehabilitation leading to growth and change. Psychodynamic models, on the otherhand, have been unsupported in terms of the rehabilitation of severe psychiatric disorders(Klerman, 1984; Mosher & Keith, 1980). In the absence of further empirical support, Mueserand Berenbaum (1990) have urged mental health professionals to abandon insight-orientedapproaches altogether.
Applying effective rehabilitation techniques in state hospitals requires sufficient time dur-ing the workday to carry them out as well as efficient and economical structuring of staff duties.State regulations and administrative directives, however, require the completion of numerousforms and narratives that document the provision of care and the consideration of patients’rights and privileges. Hospital staff have identified paperwork as one of the greatest barriers tothe provision of quality patient care (Browner et al., 1987; Corrigan, 1993; Drolen & Atherton,1993; Reppucci & Saunders, 1974). Bachelor’s level mental health technicians tend to have agreat deal of influence over patients but often do not receive enough supervision (Carlyn &Stoffelmayr, 1981), a role that psychologists could fill. In fact, Corrigan (1995) recently arguedthat the most cost effective use of psychologists on inpatients units may be in program devel-opment and the supervision of colleagues, rather than in the provision of care which might beprovided by lesser trained, and less expensive, professionals.
Few studies have been conducted regarding the manner in which psychologists actuallywork with severely mentally ill inpatients. Do unit psychologists spend most of their timeproviding direct care to patients or do they assume supervisory roles managing peers inprogramatic efforts? Given the lack of research on state hospital psychologists, findings fromsurveys on other groups of clinical psychologists may shed some light on these issues. Interms of direct care, psychologists working in private practice tend to classify their training orcurrent practice as analytical/psychodynamic more often than cognitive behavioral (Sammons& Gravitz, 1990; Tyler & Clark, 1987). When conducting assessments, psychologists in privatepractice tend to rank projective and intelligence tests—irrelevant measures for symptom
12 Journal of Clinical Psychology, January 1998

management—among the most important instruments for psychological assessment (Lubinet al., 1985; Piotrowski & Keller, 1989).
Findings from studies like these lead to the rather disconcerting conclusion that manypsychologists espouse interventions and philosophies that are contrary to clinical research find-ings describing appropriate care of the severely mentally ill inpatient. However, participants inthese studies were mostly private practitioners. The goal of this study is to survey psychologistsworking in state hospitals regarding their theoretical orientation, clinical preferences, and waysin which they carry out their treatment day.
METHOD
Subjects
Professionals classified as psychologists who worked at one of the 12 Midwestern state hospi-tals involved in this study were asked to complete a survey regarding their theoretical orienta-tion and daily work-related practices; 55 psychologists out of a possible 221 who worked at theselected hospitals completed the survey. The sample had a mean age of 46.9 years (SD5 6.8)and was 26.4% female; 17.6% of the group were single, 66.7% were married, and 15.7% wereseparated or divorced. The group was 82.7% White and 17.3% Nonwhite. In terms of educa-tion, 39.6% had earned their doctorate, 54.7% had a master’s degree, and 5.7% had a bach-elor’s degree.1 The sample had worked 15.3 years (SD 5 7.1) on average with the severelymentally ill.
Subjects were asked to complete a pencil-and-paper measure in which they reported thepercent of work time spent on various clinical activities including testing and assessment,therapy (i.e., individual therapy, rehabilitation groups), behavior modification, consultationand supervision, paperwork, responding to emergencies, and case management. Testing andassessment were further subdivided into time spent on various types of psychological measure-ment (i.e., behavioral assessment, intelligence testing, projectives). Subjects also rated individ-ual duties during the work day in terms of whether they were done by choice or because theywere required by supervisors and/or governmental regulations. Finally, subjects were asked toreport the main theoretical orientation under which they were trained and under which theycurrently practiced.
RESULTS
The mean percent of time spent on various work-related tasks is summarized in Figure 1.Results of a Friedman’s Test2 suggested that time spent on activities was ranked in similarorder by staff (x2(54) 5 123.5,p ,.001). Subsequent Wilcoxon signed-rank tests showed thatpaperwork was ranked as the single most time consuming task, requiring more than one quarterof psychologists’ work time. Paperwork included progress notes, periodic treatment plans, anddocumentation regarding unit activity, but not write-ups of test batteries. Eighty-three percentof the sample reported that paperwork consumed too much work time.
Therapeutic services accounted for about 18% of the sample’s work day. Therapeutic servicesbreak down into individual therapy (comprising 46.5% of the therapeutic services category),
1 Statutes allow professionals in these state systems to be called psychologist, and to assume duties similar to those ofother psychologists, without earning a doctorate.2 Friedman’s Test is a nonparametric statistic that examines differences in two or more within group, nonparametricmeasures by comparing rank sums of these measures.
Psychologist’s Job Survey 13
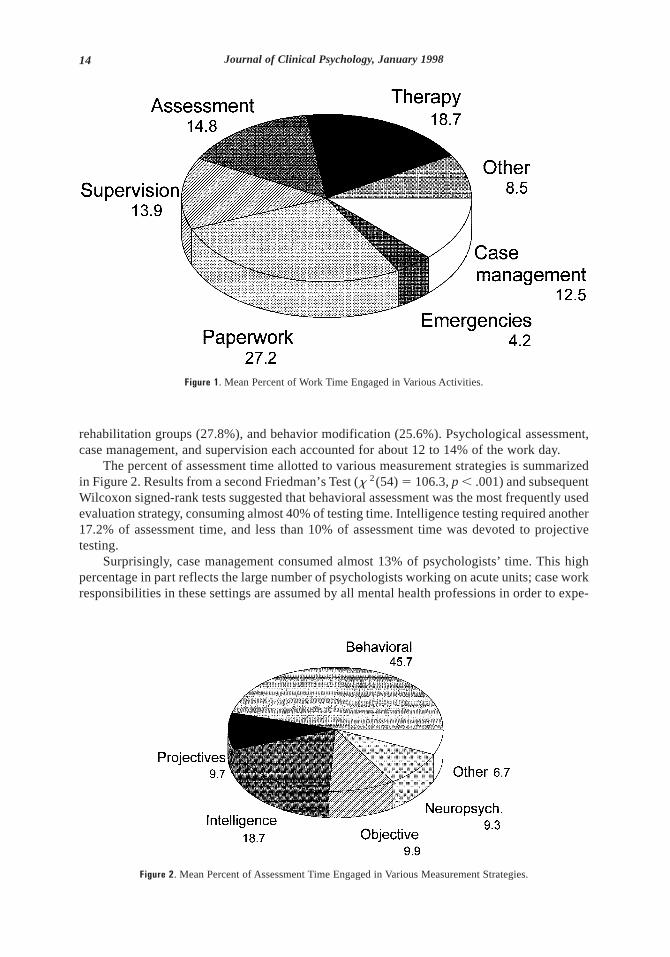
rehabilitation groups (27.8%), and behavior modification (25.6%). Psychological assessment,case management, and supervision each accounted for about 12 to 14% of the work day.
The percent of assessment time allotted to various measurement strategies is summarizedin Figure 2. Results from a second Friedman’s Test (x 2(54)5 106.3,p , .001) and subsequentWilcoxon signed-rank tests suggested that behavioral assessment was the most frequently usedevaluation strategy, consuming almost 40% of testing time. Intelligence testing required another17.2% of assessment time, and less than 10% of assessment time was devoted to projectivetesting.
Surprisingly, case management consumed almost 13% of psychologists’ time. This highpercentage in part reflects the large number of psychologists working on acute units; case workresponsibilities in these settings are assumed by all mental health professions in order to expe-
Figure 1. Mean Percent of Work Time Engaged in Various Activities.
Figure 2. Mean Percent of Assessment Time Engaged in Various Measurement Strategies.
14 Journal of Clinical Psychology, January 1998

dite patients’ returns to the community. Psychologists spent only about 14% of their time insupervision of and consultation with colleagues.
Additional analyses were conducted to determine if time spent on work tasks varied withdemographic characteristics of the sample such as age, race, gender, education level, or yearsworking with the severely mentally ill. Results yielded few significant differences. Femalepsychologists spent less time using projective assessment than their male counterparts (t(54)51.94,p ,.05). Master’s level psychologists were more likely to use behavioral assessmentsthan doctoral-level psychologists (t(52) 5 2.11,p ,.05). However, neither of theset-test val-ues was significant if Bonferroni criteria were adopted to correct for Type I error due to mul-tiple analyses.
Theoretical Orientations
Theoretical orientations of the sample, which described their training and which currentlyguided their practice, are summarized in Table 1. Almost 50% of the sample were trained undera cognitive-behavioral model. Another third of the sample characterized their training programas eclectic, combining behavioral, psychodynamic, and humanistic principles. Contrast thisfinding to orientations currently adopted to guide practice; almost 60% are now eclectic, and31.3% stated they are cognitive behavioral, a significant change from training days (x2 5 5.25,p ,.05). Neither training nor current orientation varied significantly with demographic char-acteristics of the sample or with time spent on work-related tasks.
DISCUSSION
The job practices of surveyed psychologists include a variety of administrative, supervisory,and treatment-related tasks. Results suggested that paperwork requires the single greatest blockof psychologists’ time. The average psychologist reported that more than one quarter of his orher work-day is spent completing clinical documentation. This work activity does not neces-sarily reflect the psychologist’s expertise. For example, paperwork as reported here did notinclude filling out test forms and writing up test batteries; these were subsumed under the“Assessment” rubric of the survey. Perhaps not surprisingly, more than three quarters of psy-chologists participating in this study expressed concern about the amount of time required forpaperwork. In contrast, approximately 47% of psychologists’ time is spent in direct patientcare, including assessment, case management, individual therapy, rehabilitation groups, andbehavior modification. Psychological assessment was one of the most time demanding directcare activities, which makes sense given the psychologists’ acumen in terms of formal assess-ment procedures. Survey results showed that state hospital psychologists in this study reliedmainly on behavioral assessments; less than 10% of testing time was spent on projectives.These findings were more encouraging than earlier surveys of clinical psychologists as a whole
Table 1. Frequency of Theoretical Orientation under which Samplewas Trained and Currently Practice
Orientation Trained Current Practice
Cognitive-Behavioral 47.9% 31.3%
Analytic-Dynamic 10.4 2.1Humanistic 10.4 6.2Eclectic 31.3 60.4
Psychologist’s Job Survey 15

(Lubin et al., 1985; Piotrowski & Keller, 1989) which showed assessment to be dominated byintelligence tests and projectives. Behavioral assessment is especially germane to the symptommonitoring and functional assessment that undergirds psychiatric rehabilitation.
Information about theoretical orientation is a little murkier. Almost half of the sample ratedtheir graduate training as cognitive-behavioral, which would be consistent with a rehabilitationapproach. However, this group became more eclectic as they entered practice, deciding to addpsychodynamic formulations of patients’ problems to their armamentarium. This type of eclec-ticism is less consistent with a rehabilitation model.
Psychologists also spent a relatively sizable amount of their time providing case manage-ment services. In some ways this finding is encouraging. Case work is an essential aspect ofacute inpatient care in which patients must be linked to community services that will provideaftercare. However, graduate psychology training does not typically focus on developing ex-pertise in these kinds of tasks. Conversely, only about 14% of work time was spent on man-agement and consultation activities, a more suitable role for highly trained psychologists. Thisfinding suggests that psychologists are not assuming supervisory roles in state hospitals in largenumbers.
Interestingly, the pattern of job practices and theoretical orientation did not seem to varywith subgroups of the sample. For example, master’s and doctoral level psychologists reportedrelatively similar day-to-day job responsibilities. Negative findings like these may representflaws in the methods of the study or in the power of the statistical analyses. Still, it is surprisingthat almost no significant differences were found across groups, even when usingas uncor-rected for multiple tests. These findings suggest that the persons’ job classification, and nottheir gender, race, or age, decides their work duties. It is somewhat surprising that more expe-rienced or better educated (master’s versus doctorate) psychologists do not assume greaterwork responsibilities.
The generalizability of these results may be limited to the mental health agenda of thesystems involved. For example, the extent to which case management has been made a centralgoal of inpatient care in the systems surveyed may explain the relatively high percent of timeallocated to this activity. An interesting subsequent study might examine differences in psy-chologists’ jobs as a function of state and region. Given this caveat, however, there appear to beobvious commonalities in care across state mental health systems such that these findingsprovide useful information for psychologists.
Administrators need to evaluate information in surveys like these to determine whetherspending relatively large amounts of time on paperwork and case management, and relativelylittle time as unit managers or in direct service, is a cost effective use of the unit psychologist.There are lesser trained members of the clinical team (e.g., mental health specialists withbachelor’s degrees) receiving smaller salaries who might assume some paperwork and casemanagement responsibilities. Psychologists would then have more time to perform duties moregermane to their training and level of pay, such as assessment and program development. Suchleadership positions would also take more complete advantage of psychologists’ skill in humanrelations and the application of such skills to administrative duties (Grusky, Thompson, &Tillipman, 1991).
REFERENCES
Anderson, C.M., Reiss, D.J., & Hogarty, G.E. (1986). Schizophrenia and the family. New York:Guilford.
Anthony, W.A., & Nemec, P.B. (1984). Psychiatric rehabilitation. In A.S. Bellack (Ed.),Schizophrenia:Treatment, management and rehabilitation(pp. 375–414). New York: Grune & Stratton.
16 Journal of Clinical Psychology, January 1998

Ayllon, T., & Azrin, N. (1968).The token economy: A motivational system for therapy and rehabili-tation. New York: Appleton–Century–Crofts.
Bachrach, L.L. (1992). Psychosocial rehabilitation and psychiatry in the care of long-term patients.American Journal of Psychiatry, 149, 1455–1463.
Bellack, A.S., & Mueser, K.T. (1993). Psychosocial treatment for schizophrenia.Schizophrenia Bul-letin, 19, 317–336.
Browner, C.H., Ellis, K.A., Ford, T., Silsby, J., Tampoya, J., & Yee, C. (1987). Stress, socialsupport, and health of psychiatric technicians in a state facility.Mental Retardation, 25, 31–37.
Carlyn, M., & Stoffelmayr, B. (1981). Diversity of goals in a state psychiatric hospital.Administra-tion in Mental Health, 9, 57–66.
Corrigan, P.W. (1993). Staff stressors at a developmental center and state hospital.Mental Retardation,31, 234–238.
Corrigan, P.W. (1995). Wanted: Champions of rehabilitation for psychiatric hospitals.American Psy-chologist, 50, 514–521.
Drolen, C.S., & Atherton, C.R. (1993). Turnover in state hospital social workers.Administration andPolicy in Mental Health, 20, 379–382.
Falloon, I.R.H., Boyd, J.L., & McGill, C.W. (1984). Family care of schizophrenia. New York:Guilford.
Grusky, O., Thompson, W.A., & Tillipman, H. (1991). Clinical versus administrative backgrounds formental health administrators.Administration and Policy in Mental Health, 18, 271–278.
Klerman, G.L. (1984). Ideology and science in the individual psychotherapy of schizophrenia.Schizo-phrenia Bulletin, 10, 608–612.
Liberman, R.P. (1992).Handbook of psychiatric rehabilitation. New York: Macmillan.
Liberman, R.P., Corrigan, P.W., & Schade, M.L. (1989). Drug and psychosocial treatment inter-actions in schizophrenia.International Review of Psychiatry, 1, 283–294.
Liberman, R.P., DeRisi, W.J., & Mueser, K.T. (1989).Social skills training for psychiatric patients.New York: Pergamon.
Lubin, B., Larsen, R.M., Matarazzo, J.D., & Seever, M.F. (1985). Psychological test usage patternsin five professional settings.American Psychologist, 40, 857–861.
Lukoff, D., Ventura, J., Nuechterlein, K., & Liberman, R.P. (1992). Integrating symptom assess-ment into psychiatric rehabilitation. In R.P. Liberman (Ed.),Handbook of psychiatric rehabilitation(pp. 56–77). New York: Macmillan.
Mosher, L.R., & Keith, S.J. (1980). Psychosocial treatment: Individual, group, family and communitysupport approaches.Schizophrenia Bulletin, 6, 127–158.
Mueser, K.T., & Berenbaum, H. (1990). Psychodynamic treatment of schizophrenia: Is there a future?Psychological Medicine, 20, 253–262.
Paul, G.L., & Lentz, R.J. (1977).Psychosocial treatment of chronic mental patients: Milieu versussocial learning programs. Cambridge, MA: Harvard University Press.
Piotrowski, C., & Keller, J.W. (1989). Psychological testing in outpatient mental health facilities: Anational study.Professional Psychology: Research and Practice, 20, 423–425.
Repucci, N., & Saunders, J. (1974). Social psychology of behavioral modification: Problems of imple-mentation in natural settings.American Psychologist, 29, 649–660.
Sammons, M.T., & Gravitz, M.A. (1990). Theoretical orientations of professional psychologists andtheir former professors.Professional Psychology: Research and Practice, 21, 131–134.
Stokes, T.F., & Baer, D.M. (1977). An implicit technology of generalization.Journal of Applied Behav-ioral Analysis, 10, 349–369.
Test, M.A., & Stein, L.I. (1978). Community treatment of the chronic patient: Research review.Schizo-phrenia Bulletin, 4, 350–364.
Psychologist’s Job Survey 17

Torrey, E.F., Erdman, K., Wolfe, S.M., & Flynn, L.M. (1990).Care of the seriously mentally ill: Arating of state programs. Washington, DC: Public Citizen Health Research Group and the NationalAlliance for the Mentally Ill.
Tyler, J.D., & Clark, J.A. (1987). Clinical psychologists reflect on the usefulness of various compo-nents of graduate training.Professional Psychology: Research and Practice, 18, 381–384.
Vaccaro, J.V., Pitts, D.B., & Wallace, C.J. (1992). Functional assessment. In R.P. Liberman (Ed.),Handbook of psychiatric rehabilitation(pp. 78–94). New York: Macmillan.
18 Journal of Clinical Psychology, January 1998