Resurgence of the interest in plants as sources of medicines and resistance-modifying agents
-
Upload
others
-
View
3
-
Download
0
Embed Size (px)
Citation preview
Microsoft Word - 67Resurgence of the interest in plants as sources
of medicines and resistance-modifying agents
A. C. Abreu1, A. Borges1 J. Malheiro1 and M. Simões1 1LEPAE,
Department of Chemical Engineering, Faculty of Engineering,
University of Porto, Rua Dr. Roberto Frias, s/n,
4200-465 Porto, Portugal
In the last decades, bacterial resistance to antimicrobials has
become a serious threat to clinical and public health. Traditional
methods of antibiotic discovery have failed to get new alternatives
and solutions to face the fast rhythmus of resistance evolution.
Therefore, new strategies to control bacterial infections are
highly desirable. The therapeutic value of plant extracts is
well-known for centuries. Indeed, medicinal plants always had an
important role on the treatment of several illnesses and
infections. Plants can produce complex mixtures of structural
different compounds. Some of them are being reported to have
significant antimicrobial activity against several important
clinical pathogens or for their action as synergists or
potentiators of other antibacterial agents, by interacting with
them or with the pathogens in several ways. This chapter aims to
present an overview about the current state of the use of
antibiotic coadjuvants and resistance-modifying agents in clinical
treatments. Also, the use of plants as promising sources of novel
compounds with clinical interest will be highlighted.
Keywords antimicrobial combinations; antibiotic coadjuvants;
multi-drug resistance; resistance-modifying agents
1. Introduction
The beginning of the era of antibiotics was one of the most
important events and a turning point in the history of medicine.
The introduction of antimicrobial drugs in clinical treatments
saved countless lives and gave hope for a future in which all
infectious diseases could be controlled [1]. Even now, decades
later, we are totally dependent on the use of antibiotics, not only
for the treatment of infectious diseases but also for guarantee the
success of advanced surgical procedures, including organ and
prosthetic transplants [2]. Since their introduction, millions of
tons of antibiotics have been produced and employed for a wide
variety of purposes. The excessive and, sometimes, inappropriate
use of these drugs has been accompanied by the rapid appearance of
resistant strains. Bacteria possess an impressive ability to adapt
to environmental challenges and develop resistance by altering the
expression or function of their own genes or by acquiring new
genes. The explosive spread of antibiotic resistance determinants
among pathogenic, commensal, and environmental bacteria has reached
a global dimension. Thus classical measures trying to contain or
slow the evolution of antibiotic resistance have clearly become
insufficient [3]. Consequently, newer pathogens with
multidrug-resistance profiles such as Acinetobacter baumannii have
emerged, as well as “old” pathogens such as Mycobacterium
tuberculosis and Neisseria gonorrhoeae which are now resistant to
frontline antibiotics [4]. Antibiotic resistance is an enormous
challenge that will require several strategies to address. The most
important obstacle is finding new effective antimicrobials, which
has proven to be difficult since few new classes of antibiotics
have been described over the past 40 years. This is not surprising
since identifying a new chemical matter that is effective and
nontoxic is hard, considering the actual even more complex
regulatory environment [4]. Also, there is little economic and
medical justification for the development of new antibiotics that
do not solve relevant resistance problems [5]. All of these facts
make the discovery of novel agents against new bacterial targets a
risky business. As so, major pharmaceutical companies have tended
to concentrate their efforts on improving antimicrobial agents in
established classes. However, it has been acknowledged that
researchers are getting close to the end of the possible
alternatives in terms of parent structure alterations [6].
Therefore, new strategies to control bacterial infections are
highly desirable. The use of two or more bioactive compounds
simultaneously has been a promising solution to the clinical
setting. Antimicrobial combinations can interfere with several
targets, which is thought to intensify their efficiency, increase
the pharmacological action and/or reduce adverse side effects.
Also, antimicrobial combinations could probably avoid the emergence
of resistant bacteria that might otherwise arise during treatment
[7]. Many studies report that the use of drug combinations against
multi-drug resistant bacterial pathogens have much better efficacy
compared to monotherapies [8]. It is a fact that this approach has
financial benefits since developing a new drug requires extensive
clinical trials [9]. However, the need for new antibacterial drugs
should not be address by an exclusive focus on combinations of
antimicrobial agents. Instead, a more comprehensive approach is the
development of antibiotic coadjuvants that include not only
antibiotics but also other bioactive molecules. New antimicrobial
combination drugs which include natural product combinations have
recently become a research priority. The plant kingdom is
recognized as a source of new chemical compounds, which may be
important due to their potential uses in medicine and,
specifically, for developing novel therapeutic agents. Some plant
compounds have been reported as antibacterials and, despite being
less potent compared with antibiotics, plants can fight off
infections
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1287
successfully [10]. Other compounds have direct activity against
many species of bacteria, by enhancing the activity of a specific
antibiotic, reversing the natural resistance of bacteria to
antibiotics, promoting the elimination of bacterial plasmids or by
inhibiting transport functions of the plasma membrane in regard to
given antibiotics [11]. Natural or synthetic bioactive compounds
that promote the enhancement of antibiotic activity or the reversal
of antibiotic resistance afford the classification of
resistance-modifying agents (RMAs). In this chapter, it is intended
to give an overview about the importance and the potential of
antimicrobial coadjuvants in clinical therapies. Several groups of
different antimicrobial coadjuvants will be addressed and discussed
in more detail. The prospects of using plants as source of this
type of compounds will also be discussed.
2. Antibiotic resistome
Selection for antibiotic resistance in bacteria provides one of the
most well-documented examples of an evolutionary response to
natural selection [12]. The development of antibiotic-resistant
microbes is the consequence of decades of constant selective
pressure from human applications of antibiotics, via underuse,
overuse, and misuse. Similar resistance development has also been
observed in viruses, fungi, plants and insects towards antiviral
drugs, antifungals, herbicides and insecticides, respectively,
creating increasing medical and economic problems [13]. Even before
the first clinical use of antibiotics more than 60 years ago,
resistant organisms had been isolated, which proves that this is
not a recent problem [14]. Indeed, antibiotic resistant genes have
been characterized in coliforms from glacial water and ice in the
Arctic estimated at 2000 years old [15]. And despite years of
intense investigations, there is no doubt that the situation with
respect to antibiotic resistance is pandemic and there are no
simple solutions to the problem. The term ‘antibiotic resistome’
was proposed for the collection of all antibiotic resistance genes
in microorganisms, including those from pathogenic and
non-pathogenic bacteria [16]. This resistome has suffered several
alterations over time, mainly in the last years with the
introduction of new resistance genes. Generally, the failure of
susceptibility of microorganisms to antimicrobial treatments arises
through: an inherent insusceptibility to the agents employed; the
acquisition of resistance, by previously susceptible strains,
either by mutation or by transfer of genetic material from another
species or genus; or the emergence of pre-existing, but
unexpressed, resistance phenotypes [17-19]. The exchange and
acquisition of new genetic material, by transduction,
transformation or conjugation, contributes to the rapid horizontal
dissemination of resistance determinants. The localization of
resistance determinants on mobile elements, such as genomic
islands, transposons, plasmids, or phages, greatly enhances their
dispersion [20]. The major mechanisms of bacterial resistance to
antimicrobials include drug inactivation, target modification,
alteration in the accessibility to the target through drug efflux
and decreased uptake, and over-expression of the drug target [21].
All of these mechanisms require new genetic programming by the cell
in response to the presence of antibiotics [22]. The most relevant
examples of bacterial resistance mechanisms are briefly described
in this section.
2.1. Inactivation of antibiotics
There are several strategies of antibiotic inactivation.
Hydrolysis, group transfer, and redox enzymes are involved in this
type of resistance. In Gram-negative pathogens, the production of
β-lactamases is a major resistance mechanism in β- lactam
antibiotics. Penicillins, cephalosporins and carbapenems
antibiotics with higher stability to hydrolysis were developed to
circumvent the inactivating activity of these enzymes [23].
However, extended-spectrum β-lactamases (ESBLs) have been reported
to confer resistance to newer generations of cephalosporins in
Escherichia coli, Enterobacter and Klebsiella species [24].
Regarding to carbapenemases, KPC, OXA-48, VIM and IMP-1 producers
are currently the most widespread types of carbapenemase in
Enterobacteriaceae. More recently, a new type of carbapenem
resistance gene was reported – NDM [25]. NDM producers are becoming
highly prevalent and several cases have been identified in many
countries all over the world [26].
2.2. Target modification
Other mechanism of bacterial resistance is related to the
alteration of the antibiotic target. The most common example
involves the clinically relevant resistance in staphylococci, which
is based on the acquisition of the modified penicillin-
binding-protein (PBP) 2a that mediates resistance to all known
β-lactam antibiotics, particularly the cephalosporins [5].
Alterations in PBPs are known to be responsible for specific
resistances, namely, methicillin-resistant Staphylococcus aureus
(MRSA) and penicillin-resistant Streptococcus pneumoniae (PRP)
[15]. This PBP 2a protein is encoded by mecA gene, which is carried
on the staphylococcal cassette chromosome mec (SCCmec) that is
integrated into MRSA. Five different types of SCCmec, designated
types I-V, are currently recognized, together with some variants
[27]. Other equally important examples are presented in Table
1.
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1288
Table 1 Examples of antibiotic resistance mediated by target
modification [15, 24, 27, 28].
Antibiotic class Target Resistance mechanism Examples of bacteria
Quinolones DNA gyrase or topoiso-
merase IV, (inhibition of DNA synthesis)
Chromosomal mutations in both target enzymes which promotes lower
affinity for quinolones
Gram-positive bacteria, particularly S. aureus and S.
pneumoniae
Glycopeptides (e.g.vancomycin, teicoplanin)
Biosynthesis of peptidoglycan with altered glycopeptide recognition
sites
Vancomycin-resistant S. aureus (VRSA), vancomycin- intermediate S.
aureus, glycopeptide-intermediate S. aureus
Acquisition of VanA and VanB, which encode for enzymes that produce
a modified peptidegly-can precursor terminating in d-Ala-d-
Lac
Vancomycin-resistant enterococci (VRE), such as E. faecium and E.
faecalis
Macrolides, lincosamides and streptogramin B
50S ribosomal subunit (block protein synthesis)
Post-transcriptional modification of the 23S rRNA component of the
50S ribosomal subunit involving methylation or dimethylation of key
adenine bases in the peptidyl transferase functional domain
Wide range of Gram-positive and Gram-negative bacteria
Oxazolidinones (e.g. linezolid)
50S subunit (inhibition of formation of the initiation complex and
interference with translocation of peptidyl- tRNA from A to P
site)
Mutations in the 23S rRNA resulting in decreased affinity for
binding; most mutations involve G to U substitutions in the
peptidyl transferase region of 23S rRNA
Several microorganisms including enterococci
Aminoglycosides 16S rRNA in the smaller subunit of the bacterial
ribosome, perturbing decoding of the mRNA
Mutations in the 16S rRNA gene
Mycobacterium smegmatis, Mycrobacterium tuberculosis and
Mycrobacterium abscessus
Polymyxin B and Polymyxin E (e.g. colistin)
Lipopolysaccharide (LPS) component of the outer membrane
Modification of the phosphate esters linked to the diglucosamine
components of the lipid A region by addition of 4-aminoarabinose
groups to the phosphate esters
Gram-negative bacteria
2.3. Alteration in the accessibility to the target
This can be performed by two ways: alteration in the accessibility
to the target through drug efflux or through decreased uptake.
Energy-driven drug efflux systems are increasingly recognized as
mechanisms of antibiotic resistance. These efflux systems are
either intrinsic to bacteria and activated in response to
environmental signals, or acquired by a mutation in a gene which
regulates their expression [14]. Reduced drug accumulation causing
increased minimum inhibitory concentrations (MICs) of antibiotics
is well described for macrolides, tetracyclines and quinolones
[15]. Bacterial drug efflux transporters are currently classified
into five families: (1) the major facilitator superfamily (MFS);
(2) the adenosine triphosphate (ATP)-binding cassette (ABC)
superfamily; (3) the small multidrug resistance (SMR) family; (4)
the resistance-nodulation-cell division (RND) superfamily; and (5)
the multidrug and toxic compound extrusion (MATE) family [29]. Four
different antibiotic efflux systems have been described in
Pseudomonas aeruginosa: mexAB-oprM, mexXY-oprM, mexCD-oprJ and
mexEF-oprN10. In S. aureus, several efflux pumps include QacA (MFS
family), Smr (SMR family) and NorA (MFS family) [29]. The TetA(B)
protein, among Gram-negative bacteria, and the Tet(K) from S.
aureus among Gram-positive bacteria confer resistance to
tetracyclines and is also one of the most extensively studied
members of the MF family [26, 30]. For E. coli, the best-studied
members of these pumps are the AcrAB–TolC system (RND superfamily)
and also AcrEF, AcrD, YhiUV and MdtABC. Multidrug transporter
systems, which may arise from deregulation of chromosomal genes
governing flux of drugs across the bacterial cell wall, also result
in resistance to multiple antimicrobials [24]. The outer membrane
of bacteria serves as a protective barrier from the environment,
and alterations in its permeability can confer antibiotic
resistance [24]. The import of an antibiotic can also be inhibited
by mutations that down-regulate, delete or modify outer-membrane
porins [25]. Porin mutations in Gram-negative bacteria may
confer
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
resistance to β-lactams, tetracyclines, chloramphenicol,
sulfonamides, and fluoroquinolones [24]. As such, changes in porin
copy number, size and selectivity will alter the rate of diffusion
of these antibiotics.
2.4. Increase of bacterial resistance by over-expression of the
drug target or stress-induced modifications
The over-expression of the drug target is also responsible for an
increasing bacterial resistance. Hyperproduction of TEM
β-lactamases leading to clavulanate resistance has been reported,
and could be considered over-expresssion of drug target [15].
Overexpression of the transcriptional activator MarA from mar
operon in E. coli, which confers drug resistance by altering the
expression of multiple genes located on the bacterial chromosome,
affected the expression of more than 60 genes [14]. Some of these
genes have well-known functions: activation of AcrAB/TolC efflux,
repression of the synthesis of OmpF, the point of entry for some
antibiotics, and alteration of the expression of other membrane
proteins [31]. Others presumably have something to do with stress
because they are affected by the stress locus [14]. Stress derived
from nutrient starvation, hypoxia, low pH, increased osmotic
pressure, extreme temperature shifts or antimicrobial exposure, can
also affect the gene expression patterns and cell physiology of
bacteria in ways that can influence their susceptibility to
antimicrobials. This occurs indirectly, as a result of
stress-induced growth cessation, since antimicrobials typically act
on growing cells, or directly as a result of the stress-dependent
recruitment of resistance determinants (e.g. antimicrobial efflux),
changes to antimicrobial targets, generation of resistance
mutations, promotion of resistant growth modes (biofilms), etc.
[32].
3. Antibiotic coadjuvants: how to increase the activity of a
selected antibiotic?
New classes of antibiotics and more effective antimicrobial agents
are needed. High-throughput methodologies combined with traditional
molecular biology techniques have enabled the discovery of
potential drug targets for new antibiotics and antibiotic
potentiators. However, translating these targets from
identification to actual drug compounds requires a significant
amount of additional work and financial investment [33]. Also, a
successful antibiotic must satisfy a perplexing number of demands:
it should be able to cross bacterial cell membranes at high rates,
avoid bacterial efflux pumps, not be a target for bacterial
modifying or hydrolyzing enzymes, reach its target at a
sufficiently high concentration, have a broad spectrum of
antibacterial activity, have little or no toxicity and minimal side
effects in humans [25]. There is no perfect antibiotic, and even if
such antibiotic was discovered, it would be essential that
prescription of this antibiotic would be restricted to very
specific uses. Recently, multidrug therapy has gained a wider
acceptance in the fight against multidrug resistant microbial
strains. The therapeutic value of synergistic interactions has been
known since antiquity, and many different cultural healing systems
(such as Ayurveda and traditional Chinese herbal medicine) have
relied on this principle in the belief that combination therapy may
enhance efficacy [9]. The use of drug combinations rather than
single drugs provide better clinical outcomes, as the use of single
agent is highly associated with occurrence of resistance [8].
Antimicrobial combinations are employed in order to prevent the
emergence of resistant strains or to increase activity, in cases of
mixed infections or to reduce the toxicity of a substance without
compromising the antimicrobial action. The World Health
Organization, for example, has urged pharmaceutical companies to
stop promoting the use of artemisinin derivatives in monotherapy
[9]. Also, with respect to tuberculosis, streptomycin was highly
effective, until the pathogen acquired a mutation in the 30S
ribosomal protein RpsL. So, new anti-TB drugs were introduced, but
the microorganisms acquired mutations in the targets for each of
these drugs which led to its resistance. It has become clear that a
multidrug approach must be used to treat tuberculosis (e.g.
isoniazid, rifampicin, pyrazinamide, and ethambutol), in order to
have a realistic chance of success [34]. Several additional
approaches to antibiotic discovery have been pursued, including
targeting virulence factors, antimicrobial peptides and phage
therapy [34]. Also, the use of vaccines, monoclonal antibodies,
immuno-regulatory cytokines and hematopoiesis-stimulating factors
may have utility in the control of antibiotic resistant infectious
diseases [35]. Due to the reduction in the number of new
antimicrobial agents, there has been a resurgence of interest in
the search for compounds that will restore the activity of licensed
antimicrobial agents. Antibiotic adjuvants offer an orthogonal
approach to addressing the emergency of multi-drug-resistant
pathogens [36]. Potentiation of antibiotic activity can occur
through several mechanisms, including complex multi-target effects,
serial or orthogonal inhibition of vital physiological pathways,
inhibition of resistance enzymes that degrade or covalently modify
an antibiotic to a nonactive form or of compounds that block
antibiotic efflux, enhancement of the permeability of the cell for
antibiotics causing improved solubility, resorption rate and
enhanced bioavailability, and dispersal of a biofilm to
planktonically growing cells, resulting in increased susceptibility
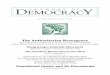
to antibiotics [4, 37, 38]. Fig. 1 presents several schematic
explanations of potentiation between antibiotics and other
bioactive compounds.
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1290
Fig. 1 Several possible mechanisms explaining a potentiating
activity between two compounds (two antibiotics or an antibiotic
and a bioactive coadjuvant): A – Multi-target effect; B - serial or
orthogonal inhibition of vital physiological pathways; C -
inhibition of resistance enzymes, of compounds that block
antibiotic efflux or that decrease the uptake into the cell; D -
compounds that enhance the permeability of the cell for
antibiotics; E - dispersal of a biofilm to planktonically growing
cells, resulting in increased susceptibility to antibiotics.
4. Plants as source of antibiotic coadjuvants
Natural products have served as an important source of drugs for
combating diseases since ancient times. In modern pharmaceutical
industries, they continue to be a major resource for the generation
of lead compounds, and half the drugs on the market are direct
descendants of natural products [39]. Plants are a rich source of
useful secondary metabolites of different chemical structures, such
as tannins, terpenoids, alkaloids, flavonoids and polyphenols, that
are used as plant defense mechanisms against pathogenic invaders
[8, 40]. The number of characterized phytochemical compounds has
been estimated to be at least 200,000 and still represents only a
fraction of the compounds produced by the around 250,000 plant
species growing on Earth [41]. Interest in medicinal plants has
increased in recent years. It is encouraging to observe that there
has been a recent increase in the number of publications reporting
on plant-based pharmacological interactions and synergistic
principles [9]. This interest has led to the discovery of new
biologically- active molecules by the pharmaceutical industry and
the adoption of crude extracts of plants for self-medication by the
general public. Examples include the use of bear-berry
(Arctostaphylos uvaursi) and cranberry juice (Vaccinium
macrocarpon) to treat urinary tract infections, essential oils of
Tea Tree (Melaleuca alternifolia) as active ingredients in many
topical formulations to treat cutaneous infections and Hydrastis
canadensis and Echinacea species for tuberculosis infections
[42-44]. Also, many plant extracts were reported to enhance the
activity of several antibiotics [45-49]. Based on their biological
activities, secondary plant metabolites were reported to be highly
active with a great selectivity for cellular targets and others are
weakly active compounds, which attack various cellular targets
[41]. Some of them have been found to have effective antibacterial
properties in vitro against both Gram-positive and Gram- negative
bacteria. However, phytochemicals have higher MICs (100-5000 μg/ml)
than antibiotics and cannot be used in monotherapy as sole agents
[8]. Active ingredients derived from these natural products can
serve as a model in semi- synthesis and total syntheses and their
activities can be enhanced [50]. Many plant-derived compounds have
been evaluated not only for their inherent antimicrobial activity,
but also for their action as potentiators of antibiotics. RMAs can
enhance the antibiotic activity by reversing antibiotic resistance.
RMAs and other type of antibiotic coadjuvants or
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1291
bioactive compounds will be discussed in this section, according to
their specific function. Also, it is intended to succinctly collate
some the available literature that has focused on interactive
plant-derived compounds that have a positive interaction with
antibiotics against resistant pathogens.
4.1. Potentiation of antibiotics due to a multi-target effect
A group of drugs or multicomponent mixtures are expected to have
multiples targets. This multiplicity of targets and the subsequent
unpredictable mode of action has been over many years the main
argument against the use of phytopreparations [51]. Multi-target
combinations provide evolutionary advantages, since plants can
protect themselves against a wide variety of predators.
Interestingly, 90% of all thoroughly described medicinal plants
contain broad spectrum compounds with rather weak or moderate
bioactivity [41]. It is also interesting to note that
phytochemicals that have different antibacterial modes of action
can potentiate the activity of the same antibiotic classes [52].
Multi- target effects caused by mixtures of phytochemicals can
modulate the three-dimensional structure of proteins (and thus
their function), by interfering with DNA or RNA (especially gene
expression), can target and disrupt the cell membrane, inhibit
cytochrome P450 or enhance absorption and thus bioavailability of
active metabolites [41, 53]. For example, myricetin, found in many
fruits, vegetables and herbs was found to inhibit DNA B helicase
[54, 55]. Allicin from Allium sativum was reported to inhibit RNA
synthesis and to interact with important thiol-containing enzymes
[54, 56-58]. The interactions may be synergistic, neutral or
antagonistic [59]. Positive interactions that intensify the potency
of a bioactive product by an inactive adjuvant are generally called
potentiating. According to European Committee for Antimicrobial
Susceptibility Testing (EUCAST) of the European Society of Clinical
Microbiology and Infectious Diseases (ESCMID) there are four
possible outcomes:
• synergism is present when the combination of antibacterials
exceeds the additive effects of the individual products;
• an additive effect is observed when a combination of
antibacterial products is equal to that of the sum of the effects
of the individual products;
• indifference is present when a combination of antibacterial
products promotes equal effects to those obtained with the most
active product;
• antagonism interactions occur when certain components of the
mixture inhibit full biological activity of
pharmacologically-active compounds by reducing their stability or
bioavailability or by enhancing their metabolism and, for that
reason, promotes a reduced effect comparatively to that of the most
effective individual product [52, 60].
However, the fact that a combination of two antibiotics is more
effective than either agent alone does not necessarily mean that
the combination has synergistic activity in vivo, but it could
reflect an additive effect. In practice, most investigators use
statistical methods to evaluate the in vivo effectiveness of
combinations, and they call in vivo synergism a statistically
significant difference between the activity of a combination and
that of the most effective agent alone [61]. Also, the FIC index
(FICI) is usually calculated in order to characterize a combination
as synergistic (FIC (drug A) + FIC (drug B), where FIC (drug A/B) =
MIC (drug A/B in combination) / MIC (drug A/B)) [18]. Synergy has
generally been defined as a FICI ≤ 0.5 and antagonism as a FICI
> 4 [62, 63].
4.2. Potentiation of antibiotics by resistance-modifying
agents
The concept of using a compound that inhibits resistance in a
bacterium which may be employed with a conventional antibiotic is
well proven [64]. Important examples of these inhibitors are
clavulanic acid, which binds with high affinity to many bacterial
β-lactamases and is available commercially in combination with
amoxicillin (as Augmentin®) and ticarcillin (Timentin®) [35, 65,
66]; sulbactam, marketed in combination with ampicillin (as
Unasyn®), and tazobactam, marketed in combination with piperacillin
(as Tazocin®) [35, 65, 67]. There have been considerable efforts to
discover other inhibitors of β-lactamases and, in particular,
molecules that target the emerging metallo-β-lactamases [22].
Expanding this strategy to other antibiotics is a possibility that
should be explored in order to maintain the effectiveness of our
current arsenal of antibiotics [22]. Many plants have been
evaluated not only for direct antimicrobial activity, but also as
RMAs [18, 68-71]. Their potential use in combinations can help to
recycle older antibiotics for which resistance mechanisms are
greatly disseminated. There is a significant interest in plant
compounds that inhibit bacterial efflux pumps. Ideally, a good
bacterial efflux inhibitor (EPI) must not inhibit the human
P-glycoprotein involved in the xenobiotic efflux of normal tissues
[72]. Numerous phytochemicals have been shown to have activity
against S. aureus or other Gram-positive bacteria, or to act as
potential EPIs with antimicrobials for Gram-positive bacteria [73].
Some of them are: carnosol and carnosic acid from Rosmarinus
officinalis, reserpine from Rauwolfia serpentina, piperine from
Piper nigrum, sylibin from Silybum marianum, chalcone from Dalea
versicolor, chrysosplenol-D and chrysoplenetin from Artemisia annua
[6, 7, 18, 47, 74-76]. The toxicity of reserpine and its adverse
effect to humans, even at low concentrations, limit its usage
thereby warranting the quest for alternative EPIs [72]. Other
phytochemicals were reported for their action as
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1292
inhibitors of PBP 2a; such as baicalein from Scutellaria species,
tellimagrandin I and rugosin B from Rosa canina L., corilagin from
Arctostaphylos uva-ursi [18, 77, 78].
4.3. Synergism between active compounds due to enhanced cell
permeability effects
Another strategy to overcome resistance is to improve the delivery
or enhance the accessibility of antibiotics to their sites of
action. Many compounds have been reported to affect membrane
permeability of a diverse range of microorganisms [79], mainly due
to the perturbation of the lipid fraction of the cell membrane.
Also, owing to their lipophilic character, they can increase
membrane permeability [80]. Such permeabilizers, as they have been
termed, can non-specifically enhance the permeability of bacterial
cells to exogenous products, including antimicrobial agents, and
may therefore potentiate the antibacterial activity of antibiotics
that interact with intracellular targets [52]. Carvacrol and thymol
are two main products of the essential oil of Thymus vulgaris, and
were reported to disintegrate the outer membrane and thus to
increase membrane permeability and fluidity in Gram-negative
bacteria, facilitating the penetration of antibiotics [37, 42, 52,
79, 81]. Gallic acid from berry extracts has proven to be an
efficient permeabilizer for several Salmonella strains due to a
disintegrating activity of the outer membrane based on the
chelation of divalent cations and to the partial hydrophobicity of
this product, which promote the membrane destabilization [82].
Also, this compound was reported to cause irreversible changes in
membrane properties through hydrophobicity changes, decrease of
negative surface charge, and occurrence of local rupture or pore
formation in the cell membranes [83]. Xanthohumol and lupulon, from
Humulus lupulus, also promote changes in the properties and
permeability of the membrane [84]. For this reason, potentiation of
several antibiotics by these compounds was reported.
4.4. Potentiation of antibiotics by promoting the dispersal of a
biofilm to planktonically growing cells
It is well known that bacteria in biofilms are much more resistant
compared with planktonic cells. The microorganisms generate
physiological changes when cells attach to a surface by expressing
a biofilm phenotype that can confer resistance face to stress
environmental conditions such as nutrient limitation, heat and cold
shocks, changes in pH and to chemical agents. Chronic infections in
which biofilms have been demonstrated to be involved are many and
include periodontitis, cystic fibrosis pneumonia, and numerous
infections associated with indwelling devices such as catheters,
heart valves, and prostheses [85]. Also, biofilms constitute a
major threat in the clinical environment by acting as reservoirs of
multidrug resistant pathogenic bacteria. Biofilm resistance
involves multiple mechanisms [86]. One obvious difference between
planktonic cells and biofilms is the presence of a polymeric matrix
enveloping the community that retards diffusion of antimicrobials
into the biofilm [87-89]. Many studies have investigated the
formation of biofilms as an explanation for microbial resistance
[90-93]. Antibiotics have been shown to penetrate biofilms readily
in some cases and poorly in others, depending on the particular
agent and biofilm [87]. However, given that, in many cases,
biofilms consist of stacks of cells with aqueous channels flowing
in between, only impenetrability seems unlikely [93]. Because of
the special structure of biofilms, there are gradients of nutrients
and oxygen and, for this reason, cells can be in distinct growth
states. Consequently, cells in different layers of the biofilm will
be affected differently by different types of antimicrobials
depending on their mechanism of action [1]. For example, penicillin
antibiotics, which target cell-wall synthesis, kill only growing
bacteria [94]. Other theories include a reduced susceptibility of
biofilm microorganisms compared to their freely suspended
counterparts [90]; and the existence of persister cells, a small
population of cells with a highly protected phenotype [85, 88, 95].
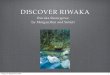
Fig. 2 represents some hypotheses explaining the higher resistance
to antibiotics in biofilms.
Fig. 2 Four hypothesized biofilm resistance mechanisms: A – The
antibiotic (black points) penetrates slowly or incompletely the
biofilm; B – an adaptive stress response is expressed by some cells
(marked cells); C – a concentration gradient of a metabolic
substrate or product leads to zones of slow non-growing bacteria
(shaded cells); D – a small fraction of the cells differentiate
into a highly protected persister state (dark cells).
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1293
Plant-based antimicrobial studies on planktonic microorganisms have
been given extensive priority. The inhibition of biofilms, however,
has been largely neglected [9]. The rapid reversal of resistance
upon dispersion from a biofilm suggests that this is an adaptive
resistance mechanism rather than a genetic alteration [85]. Cells
in the biofilm can return to a planktonic lifestyle by two possible
ways. In order to colonize new areas or in response to
environmental cues, such as starvation, a programmed set of events
leads to hydrolysis of the extracellular polysaccharide matrix and
conversion of a subpopulation of cells into motile planktonic
cells, which can rapidly multiply and leave the sessile communities
[87]. Also, biofilm dispersal can occur as a consequence of
physical detachment or mechanical breakage due to flow or shear
stresses [96]. Potential therapies include enzymes that dissolve
the matrix polymers of the biofilm, chemical reactions that block
biofilm matrix synthesis, and analogues of microbial signaling
molecules that interfere with cell-to-cell communication, required
for normal biofilm formation [94]. Many bacteria are known to
regulate diverse physiological processes through a mechanism called
quorum sensing (QS) which is accomplished through the production,
secretion and subsequent detection of extracellular signal
molecules called autoinducers (AIs). When these molecules reach a
particular threshold concentration, they are taken up by other
microbes and trigger adaptive changes appropriate to the community
of organisms [1, 97, 98]. QS has been found to regulate a number of
physiological activities, including motility, conjugation,
competence, sporulation, virulence and biofilm formation. Some of
these quorum sensing molecules, such as the Pseudomonas quinolone
signal (PQS) and the homoserine lactones (AHL) from P. aeruginosa,
possess antimicrobial activity at very high concentrations [1].
Consequently, QS pathways of competing bacteria are potential
targets for such nontoxic chemical defenses. Screening for natural
products able to promote biofilm dispersal has led to the
identification of inhibitors of AHL-based QS, such as
bromoageliferin and oroidin [96]. The aqueous extract of Moringa
oleifera was found to inhibit violacein production, a QS-regulated
behavior in Chromobacterium violaceum [99]. In other study, the
hexane, chloroform and methanol extracts of an Ayurveda spice,
namely clove (Syzygium aromaticum), shown anti-QS activity by
inhibiting the response of C. violaceum CV026 to exogenously
supplied N-hexanoyl-homoserine lactone, in turn preventing
violacein production [100]. Aqueous extracts of six plants,
Conocarpus erectus, Chamaesyce hypericifolia, Callistemon
viminalis, Bucida buceras, Tetrazygia bicolor and Quercus
virginiana, caused the inhibition of QS genes and QS-controlled
factors, with marginal effects on bacterial growth of P. aeruginosa
[101]. Also, common dietary fruit, herb and spice extracts also
significantly inhibited QS [102].
5. Conclusions
Our planet is saturated with antibiotics, which had a major
contribution to the selection of resistant strains. Resistance
mechanisms are pandemic and create an enormous clinical and
financial burden on health care systems worldwide. Resistance
remains as a primary driver for antibacterial R&D. Plant-based
medicines are important therapeutic weapons to cure human diseases,
and are of extremely relevance to pharmacology. Indeed, it has been
shown that resistance to crude extracts occurs less than resistance
to single actives. The concept of antimicrobial synergy is based on
the principle that, in combination, the formulation may enhance
efficacy, reduce toxicity, decrease adverse side effects, increase
bioavailability, lower the dose and reduce the advance of
antimicrobial resistance [9]. Research into antimicrobial
combinations may yield new developments that may address the
increasing concern towards antimicrobial resistance. Recent
advances in combinatorial chemistry have allowed the synthesis of
large number of compounds by automated high-throughput synthesis.
Also, new techniques, such as metabolomics and other “omics”, are
providing new tools to explore the mechanism of action of complex
herbal preparations. Understanding the molecular diversity that
underlies resistance using up-to-date technology will guide new
efforts to develop effective antibiotics [14]. Exploration of
structure-activity relationships can lead to the rational
preparation and evaluation of new analogs that offer some
protection against one or more of the known resistance mechanisms.
More studies of inhibitory- target and inhibitory-resistance
interactions will also provide new leads. However, any new chemical
that is initially identified as having an interesting antimicrobial
activity in a screening process will have a long way before being
approved as an antibiotic.
Acknowledgements This work was supported by Operational Programme
for Competitiveness Factors – COMPETE and by FCT – Portuguese
Foundation for Science and Technology through Projects Bioresist -
PTDC/EBB-EBI/105085/2008; Phytodisinfectants –
PTDC/DTP-SAP/1078/2012; and the PhD grants awarded to Ana Abreu
(SFRH/BD/84393/2012) and Anabela Borges (SFRH/BD/63398/2009).
References
[1] Fernández L, Breidenstein EBM, Hancock REW. Creeping baselines
and adaptive resistance to antibiotics. Drug Resistance Updates.
2011;14:1-21.
[2] Davies J, Davies D. Origins and evolution of antibiotic
resistance. Microbiology and Molecular Biology Reviews.
2010;74:417- 433.
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1294
[3] Baquero F, Coque TM, de la Cruz F. Ecology and evolution as
targets: the need for novel eco-evo drugs and strategies to fight
antibiotic resistance. Antimicrobial Agents and Chemotherapy.
2011;55:3649-3660.
[4] Kalan L, Wright GD. Antibiotic adjuvants: multicomponent
anti-infective strategies. Expert Reviews in Molecular Medicine.
2011;13:null-null.
[5] Theuretzbacher U. Resistance drives antibacterial drug
development. Current Opinion in Pharmacology. 2011;11:433-438. [6]
Cushnie TPT, Lamb AJ. Antimicrobial activity of flavonoids.
International Journal of Antimicrobial Agents. 2005;26:343-356. [7]
Gibbons S, Oluwatuyi M, Kaatz GW. A novel inhibitor of multidrug
efflux pumps in Staphylococcus aureus. Journal of
Antimicrobial Chemotherapy. 2003;51:13-17. [8] Kyaw BM, Arora S,
Lim CS. Bactericidal antibiotic-phytochemical combinations against
methicillin resistant Staphylococcus
aureus. Brazilian Journal of Microbiology. 2012;43:938-945. [9] van
Vuuren S, Viljoen A. Plant-based antimicrobial studies - methods
and approaches to study the interaction between natural
products. Planta Med. 2011;77:1168-1182. [10] Klannik A, Moina SS,
Zhang Q. Anti-Campylobacter activities and resistance mechanisms of
natural phenolic compounds in
Campylobacter. PLoS ONE. 2012;7:e51800. [11] Coutinho H, Costa J,
Lima E, Falcao-Silva V, Siqueira J. Herbal therapy associated with
antibiotic therapy: potentiation of the
antibiotic activity against methicillin - resistant Staphylococcus
aureus by Turnera ulmifolia L. BMC Complementary and Alternative
Medicine. 2009;9:13.
[12] Walker ES, Levy F. Genetic trends in a population evolving
antibiotic resistance. Evolution. 2001;55:1110-1122. [13]
Maisnier-Patin S, Andersson DI. Adaptation to the deleterious
effects of antimicrobial drug resistance mutations by
compensatory evolution. Research in Microbiology. 2004;155:360-369.
[14] Levy SB. Active efflux, a common mechanism for biocide and
antibiotic resistance. Journal of Applied Microbiology.
2002;92:65S-71S. [15] Barker KF. Antibiotic resistance: a current
perspective. Brasilian Journal of Clinical Pharmacology.
1999;48:109-124. [16] Edgar R, Friedman N, Molshanski-Mor S, Qimron
U. Reversing bacterial resistance to antibiotics by phage-mediated
delivery
of dominant sensitive genes. Applied and Environmental
Microbiology. 2011; [17] Gilbert P, Maira-Litran T, McBain AJ,
Rickard AH, Whyte FW. The physiology and collective recalcitrance
of microbial
biofilm communities. Advances in Microbial Physiology.
2002;46:203-256. [18] Abreu AC, McBain AJ, Simoes M. Plants as
sources of new antimicrobials and resistance-modifying agents.
Natural Product
Reports. 2012;29:1007-1021. [19] Simões M, Rocha R, Coimbra MA,
Vieira M. Enhancement of Escherichia coli and Staphylococcus aureus
antibiotic
susceptibility using sesquiterpenoids. Medicinal Chemistry.
2008;4:616-623. [20] McCallum N, Berger-Bächi B, Senn MM.
Regulation of antibiotic resistance in Staphylococcus aureus.
International Journal
of Medical Microbiology. 2010;300:118-129. [21] Brehm-Stecher BF,
Johnson EA. Sensitization of Staphylococcus aureus and Escherichia
coli to antibiotics by the
sesquiterpenoids nerolidol, farnesol, bisabolol, and apritone.
Antimicrobial Agents and Chemotherapy. 2003;47:3357-3360. [22]
Wright GD. Bacterial resistance to antibiotics: Enzymatic
degradation and modification. Advanced Drug Delivery Reviews.
2005;57:1451-1470. [23] Ulrich-Merzenich G, D. P, Zeitler H, Vetter
H, Wagner H. Drug development from natural products: Exploiting
synergistic
effects. Indian Journal of Experimental Biology. 2010;48:208-219.
[24] Hoffman SB. Mechanisms of antibiotic resistance. Compendium.
2001;23:464-473. [25] Hughes D. Expoliting genomics, genetics and
chemistry to combat antibiotic resistance. Nature Reviews.
2003;4:432-441. [26] Guay GG, Tuckman M, Rothstein DM. Mutations in
the tetA(B) gene that cause a change in substrate specificity of
the
tetracycline efflux pump. Antimicrobial Agents and Chemotherapy.
1994;38:857-860. [27] Lambert PA. Bacterial resistance to
antibiotics: Modified target sites. Advanced Drug Delivery Reviews.
2005;57:1471-1485. [28] Wright GD. Mechanisms of resistance to
antibiotics. Current Opinion in Chemical Biology. 2003;7:563-569.
[29] Kumar A, Schweizer HP. Bacterial resistance to antibiotics:
Active efflux and reduced uptake. Advanced Drug Delivery
Reviews. 2005;57:1486-1513. [30] Borges-Walmsley MI, McKeegan KS,
Walmsley AR. Structure and function of efflux pumps that confer
resistance to drugs.
Biochemical Journal. 2003;376:313-338. [31] Alekshun MN, Levy SB.
The mar regulon: multiple resistance to antibiotics and other toxic
chemicals. Trends in Microbiology.
1999;7:410-413. [32] Poole K. Bacterial stress responses as
determinants of antimicrobial resistance. Journal of Antimicrobial
Chemotherapy.
2012;20:227-234. [33] Lu TK, Collins JJ. Engineered bacteriophage
targeting gene networks as adjuvants for antibiotic therapy.
Proceedings of the
National Academy of Sciences. 2009;106:4629-4634. [34] Lewis K.
Platforms for antibiotic discovery. Nature Reviews.
2013;12:371-387. [35] Chopra I, Hodgson J, Metcalf B, Poste G. The
search for antimicrobial agents effective against bacteria
resistant to multiple
antibiotics. Antimicrobial Agents and Chemotherapy.
1997;41:497-503. [36] Taylor PL, Rossi L, De Pascale G, Wright GD.
A forward chemical screen identifies antibiotic adjuvants in
Escherichia coli.
ACS Chemical Biology. 2012;7:1547-1555. [37] Wagner H,
Ulrich-Merzenich G. Synergy research: Approaching a new generation
of phytopharmaceuticals. Phytomedicine.
2009;16:97-110. [38] Zimmermann GR, Lehár J, Keith CT. Multi-target
therapeutics: when the whole is greater than the sum of the parts.
Drug
Discovery Today. 2007;12:34-42. [39] Cremin PA, Zeng L.
High-throughput analysis of natural product compound libraries by
parallel LC−MS evaporative light
scattering detection. Analytical Chemistry. 2002;74:5492-5500. [40]
Dixon RA. Natural products and plant disease resistance. Nature.
2001;411:843-847.
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
[41] Efferth T, Koch E. Complex interactions between
phytochemicals. The multi-target therapeutic concept of
phytotherapy. Current Drug Targets. 2011;12:122-132.
[42] Schelz Z, Hohmann J, Molnar J. Recent advances in research of
antimicrobial effects of essential oils and plant derived compounds
on bacteria. In: Chattopadhyay D, eds. Ethnomedicine: A Source of
Complementary Therapeutics. Kerala: Research Signpost;
2010:179-201.
[43] Nikaido H. Antibiotic resistance caused by Gram-negative
multidrug efflux pumps. Clinical Infectious Diseases. 1998;27:S32-
S41.
[44] Gibbons S. Phytochemicals for bacterial resistance –
strengths, weaknesses and opportunities. Planta Medica.
2008;74:594– 602.
[45] Braga LC, Leite AAM, Xavier KGS, Takahashi JA, Bemquerer MP,
Chartone-Souza E, Nascimento AMA. Synergic interaction between
pomegranate extract and antibiotics against Staphylococcus aureus.
Canadian Journal of Microbiology. 2005;51:541-547.
[46] Darwish RM, Aburjai T, Al-Khalil S, Mahafzah A. Screening of
antibiotic resistant inhibitors from local plant materials against
two different strains of Staphylococcus aureus. Journal of
Ethnopharmacology. 2002;79:359-364.
[47] Stavri M, Piddock LJV, Gibbons S. Bacterial efflux pump
inhibitors from natural sources. Journal of Antimicrobial
Chemotherapy. 2007;59:1247-1260.
[48] Dickson RA, Houghton PJ, Hylands PJ, Gibbons S. Antimicrobial,
resistance-modifying effects, antioxidant and free radical
scavenging activities of Mezoneuron benthamianum Baill., Securinega
virosa Roxb. & Wlld. and Microglossa pyrifolia Lam.
Phytotherapy Research. 2006;20:41-45.
[49] Adwan G, Mhanna M. Synergistic effects of plant extracts and
antibiotics on Staphylococcus aureus strains isolated from clinical
specimens. Middle-East Journal of Scientific Research.
2008;3:134-139.
[50] Puhl MCMN, Cortez DAG, Ueda-Nakamura T, Nakamura CV, Filho
BPD. Antimicrobial activity of Piper gaudichaudianum Kuntze and its
synergism with different antibiotics. Molecules.
2011;16:9925-9938.
[51] Ulrich-Merzenich G, Panek D, Zeitler H, Wagner H, Vetter H.
New perspectives for synergy research with the “omic”-
technologies. Phytomedicine. 2009;16:495-508.
[52] Simoes M, Bennett RN, Rosa EAS. Understanding antimicrobial
activities of phytochemicals against multidrug resistant bacteria
and biofilms. Natural Product Reports. 2009;26:746-757.
[53] Wink M. Evolutionary advantage and molecular modes of action
of multi-component mixtures used in phytomedicine Current Drug
Metabolism. 2008;9:996-1009.
[54] Hemaiswarya S, Kruthiventi A, Doble M. Synergism between
natural products and antibiotics against diseases. Phytomedicine.
2008;15:639-652.
[55] Lin R-D, Chin Y-P, Lee M-H. Antimicrobial activity of
antibiotics in combination with natural flavonoids against clinical
extended-spectrum β-lactamase (ESβL)-producing Klebsiella
pneumoniae. Phytotherapy Research. 2005;19:612-617.
[56] Cai Y, Wang R, Pei F, Liang B-B. Antibacterial activity of
allicin alone and in combination with β-lactams against
Staphylococcus spp. and Pseudomonas aeruginosa. Journal of
Antibiotics. 2007;60:335-338.
[57] Abascal K, Yarnell E. Herbs and drug resistance: Part 1 -
herbs and microbial resistance to antibiotics. Alternative and
Complementary Therapies. 2002;8:237-241.
[58] Ankri S, Mirelman D. Antimicrobial properties of allicin from
garlic. Microbes and Infection. 1999;1:125-129. [59] Zahin M, Aqil
F, Khan MSA, Ahmad I. Ethnomedicinal plants derived antibacterials
and their prospects. In: Chattopadhyay D,
eds. Ethnomedicine: a source of complementary therapeutics. Kerala:
Research Signpost; 2010:149-178. [60] Lila MA, Raskin I.
Health-related interactions of phytochemicals. Journal of Food
Science. 2005;70:20-27. [61] Fantin B, Carbon C. In vivo antibiotic
synergism: contribution of animal models. Antimicrobial Agents and
Chemotherapy.
1992;36:907-912. [62] Mackay ML, Milne K, Gould IM. Comparison of
methods for assessing synergic antibiotic interactions.
International Journal
of Antimicrobial Agents. 2000;15:125-129. [63] Rand KH, Houck HJ,
Brown P, Bennet D. Reproducibility of the microdilution
checkerboard method for antibiotic synergy.
Antimicrobial Agents and Chemotherapy. 1996;37:613-615. [64]
Gibbons S. Plants as a source of bacterial resistance modulators
and anti-infective agents. Phytochemistry Reviews. 2005;4:63-
78. [65] Sullivan Å, Edlund C, Nord CE. Effect of antimicrobial
agents on the ecological balance of human microflora. The
Lancet
Infectious Diseases. 2001;1:101-114. [66] Miller LA, Ratnam K,
Payne DJ. β-Lactamase-inhibitor combinations in the 21st century:
current agents and new
developments. Current Opinion in Pharmacology. 2001;1:451-458. [67]
Drawz SM, Bonomo RA. Three decades of β-lactamase inhibitors.
Clinical Microbiology Reviews. 2010;23:160-201. [68] Santos NKA,
Coutinho HDM, Viana GSB, Rodrigues FG, Costa JM. Chemical
characterization and synergistic antibiotic
activity of volatile compounds from the essential oil of
Vanillosmopsis arborea. Medicinal Chemistry Research. 2011;20:637-
641.
[69] Gibbons S, Oluwatuyi M, Veitch NC, Gray AI. Bacterial
resistance modifying agents from Lycopus europaeus. Phytochemistry.
2003;62:83-87.
[70] Coutinho HDM, Costa JGM, Falcão-Silva VS, Siqueira-Júnior JP,
Lima EO. Effect of Momordica charantia L. in the resistance to
aminoglycosides in methicilin-resistant Staphylococcus aureus.
Comparative Immunology, Microbiology and Infectious Diseases.
2010;33:467-471.
[71] Coutinho HDM, Costa JGM, Lima EO, Falcao-Silva VS, Siqueira
JP. Herbal therapy associated with antibiotic therapy: potentiation
of the antibiotic activity against methicillin – resistant
Staphylococcus aureus by Turnera ulmifolia L. BMC Complementary and
Alternative Medicine. 2009;9:9-13.
[72] Mohtar M, Johari S, Li A, Isa M, Mustafa S, Ali A, Basri D.
Inhibitory and resistance-modifying potential of plant-based
alkaloids against methicillin-resistant Staphylococcus aureus
(MRSA). Current Microbiology. 2009;59:181-186.
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
1296
[73] Garvey MI, Rahman MM, Gibbons S, Piddock LJV. Medicinal plant
extracts with efflux inhibitory activity against Gram- negative
bacteria. International journal of antimicrobial agents.
2011;37:145-151.
[74] Kang H-K, Kim H-Y, Cha J-D. Synergistic effects between
silibinin and antibiotics on methicillin-resistant Staphylococcus
aureus isolated from clinical specimens. Biotechnology Journal.
2011;6:1397-1408.
[75] Jin J, Zhang J, Guo N, Feng H, Li L, Liang J, Sun K, Wu X,
Wang X, Liu M, Deng X, Yu L. The plant alkaloid piperine as a
potential inhibitor of ethidium bromide efflux in Mycobacterium
smegmatis. Journal of Medical Microbiology. 2011;60:223- 229.
[76] Marquez B. Bacterial efflux systems and efflux pumps
inhibitors. Biochimie. 2005;87:1137-1147. [77] Shimizu M, Shiota S,
Mizushima T, Ito H, Hatano T, Yoshida T, Tsuchiya T. Marked
potentiation of activity of β-lactams
against methicillin-resistant Staphylococcus aureus by corilagin.
Antimicrobial Agents and Chemotherapy. 2001;45:3198-3201. [78]
Shiota S, Shimizu M, Sugiyama J, Morita Y, Mizushima T, Tsuchiya T.
Mechanisms of action of corilagin and tellimagrandin I
that remarkably potentiate the activity of β-lactams against
methicillin-resistant Staphylococcus aureus. Microbiology and
Immunology. 2004;48:67-73.
[79] Helander IM, Alakomi H-L, Latva-Kala K, Mattila-Sandholm T,
Pol I, Smid EJ, Gorris LGM, von Wright A. Characterization of the
action of selected essential oil components on Gram-negative
bacteria. Journal of Agricultural and Food Chemistry.
1998;46:3590-3595.
[80] Trombetta D, Castelli F, Sarpietro MG, Venuti V, Cristani M,
Daniele C, Saija A, Mazzanti G, Bisignano G. Mechanisms of
antibacterial action of three monoterpenes. Antimicrobial Agents
and Chemotherapy. 2005;49:2474-2478.
[81] Lambert RJW, Skandamis PN, Coote PJ, Nychas GJE. A study of
the minimum inhibitory concentration and mode of action of oregano
essential oil, thymol and carvacrol. Journal of Applied
Microbiology. 2001;91:453-462.
[82] Nohynek LJ, Alakomi H-L, Kähkönen MP, Heinonen M, Helander IM,
Oksman-Caldentey K-M, Puupponen-Pimiä RH. Berry phenolics:
antimicrobial properties and mechanisms of action against severe
human pathogens. Nutrition and Cancer. 2006;54:18-32.
[83] Borges A, Saavedra MJ, Simões M. The activity of ferulic and
gallic acids in biofilm prevention and control of pathogenic
bacteria. Biofouling. 2012;28:755-767.
[84] Natarajan P, Katta S, Andrei I, Babu Rao Ambati V, Leonida M,
Haas GJ. Positive antibacterial co-action between hop (Humulus
lupulus) constituents and selected antibiotics. Phytomedicine.
2008;15:194-201.
[85] Stewart PS. Mechanisms of antibiotic resistance in bacterial
biofilms. International Journal of Medical Microbiology.
2002;292:107-113.
[86] Inoue T, Shingaki R, Fukui K. Inhibition of swarming motility
of Pseudomonas aeruginosa by branched-chain fatty acids. FEMS
Microbiology Letters. 2008;281:81-86.
[87] Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a
common cause of persistent infections. Science.
1999;284:1318-1322.
[88] Brooun A, Liu S, Lewis K. A dose-response study of antibiotic
resistance in Pseudomonas aeruginosa biofilms. Antimicrobial Agents
and Chemotherapy. 2000;44:640-646.
[89] Fux CA, Costerton JW, Stewart PS, Stoodley P. Survival
strategies of infectious biofilms. Trends in Microbiology.
2005;13:34- 40.
[90] Stewart P. Theoretical aspects of antibiotic diffusion into
microbial biofilms. Antimicrobial Agents and Chemotherapy.
1996;40:2517-2522.
[91] Xu KD, McFeters GA, Stewart PS. Biofilm resistance to
antimicrobial agents. Microbiology. 2000;146:547-549. [92] Mah
T-FC, O'Toole GA. Mechanisms of biofilm resistance to antimicrobial
agents. Trends in Microbiology. 2001;9:34-39. [93] Smith AW.
Biofilms and antibiotic therapy: Is there a role for combating
bacterial resistance by the use of novel drug delivery
systems?. Advanced Drug Delivery Reviews. 2005;57:1539-1550. [94]
Stewart PS, William Costerton J. Antibiotic resistance of bacteria
in biofilms. The Lancet. 2001;358:135-138. [95] Lai S, Tremblay J,
Déziel E. Swarming motility: a multicellular behaviour conferring
antimicrobial resistance. Environmental
Microbiology. 2009;11:126-136. [96] Landini P, Antoniani D, Burgess
JG, Nijland R. Molecular mechanisms of compounds affecting
bacterial biofilm formation
and dispersal. Applied Microbiology and Biotechnology.
2010;86:813-823. [97] Cvitkovitch DG, Li Y-H, Ellen RP. Quorum
sensing and biofilm formation in Streptococcal infections. Journal
of Clinical
Investment. 2003;112:1626-1632. [98] Hammer BK, Bassler BL. Quorum
sensing controls biofilm formation in Vibrio cholerae. Molecular
Microbiology.
2003;50:101-104. [99] Singh BN, Singh BR, Singh RL, Prakash D,
Dhakarey R, Upadhyay G, Singh HB. Oxidative DNA damage protective
activity,
antioxidant and anti-quorum sensing potentials of Moringa oleifera.
Food and Chemical Toxicology. 2009;47:1109-1116. [100] Krishnan T,
Yin W-F, Chan K-G. Inhibition of quorum sensing-controlled
virulence factor production in Pseudomonas
aeruginosa PAO1 by Ayurveda spice clove (Syzygium aromaticum) bud
extract. Sensors. 2012;12:4016-4030. [101] Adonizio A, Kong K-F,
Mathee K. Inhibition of quorum sensing-controlled virulence factor
production in Pseudomonas
aeruginosa by south Florida plant extracts. Antimicrobial Agents
and Chemotherapy. 2008;52:198-203. [102] Vattem DA, Mihalik K,
Crixell SH, McLean RJC. Dietary phytochemicals as quorum sensing
inhibitors. Fitoterapia.
2007;78:302-310.
Microbial pathogens and strategies for combating them: science,
technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013