Embed Size (px)
Citation preview

Retained Catheter Fragment from a FracturedTunneled Catheter—A Rare and Potentially LethalComplication
Anand Reddy,* Anondo Stangl,† and Brian Radbill‡
*Department of Nephrology, Mount Sinai School of Medicine, New York, †Department of Radiology, MountSinai School of Medicine, New York City, New York, and ‡Department of Nephrology, Mount Sinai School ofMedicine, New York City, New York
ABSTRACT
Despite efforts to curtail central vein catheter use for dialysiscatheters are frequently used in the treatment of end-stage renaldisease (ESRD). In 2006, 82% of patients in the USA initiateddialysis via a catheter. The overall of tunnelled cuffed catheter(TCC)usewas 35%greater in 2005 comparedwith 1996.Dialy-
sis catheter tip fracture is a rare and potentially serious compli-cation. Herein, we present the case of an incidental finding of aretained catheter fragment from a fractured TCC in the rightatrium. Fragment retrieval (via snare technique) and subse-quent placement of anewcentral venous catheter are outlined.
Well-functioning, long-term vascular access remainsthe Achilles’ heel of hemodialysis (HD) and is essentialto providing efficient dialysis therapy. Vascular access isa major cause of morbidity and mortality (1) in end-stage renal disease (ESRD), accounting for the majorityof hospitalizations (2) and 14% of all ESRD expenses(an estimated $1 billion annually) (1). There are threemain types of longterm vascular access: native arteriove-nous fistula (AVF), arteriovenous graft (AVG) and cen-tral vein catheter (CVC), typically a tunnelled cuffedcatheter (TCC). Originally hailed as a viable alternativeto the arteriovenous graft (AVG), TCCs have been asso-ciated with as much as a threefold increased mortalityrate as compared to AVFs (3,4). Sepsis-related death is100 times greater in dialysis patients than in the generalpopulation, with infection-related death and all-causemortality highest in those with TCCs (5). Approximately20% of patients dialyzed through a TCC develop osteo-myelitis, septic arthritis, and endocarditis and often die,regardless of whether or not the infected catheter isremoved (6,7). In addition to infection-related complica-tions, a several-fold increase in cardiovascular risk hasalso been associated with catheter use (5). The cost ofplacing a TCC is approximately $13,000, and that of
treating one TCC-related episode of bacteremia is ashigh as $45,000 (5).
Case Report
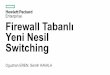
A 35-year-old caucasian woman presented with ahistory of ESRD on HD via a right internal jugularvein CVC. Other past medical history included a 22-yearhistory of insulin-dependent diabetes mellitus (IDDM)complicated by gastroparesis, peripheral vascular dis-ease, ischemic cardiomyopathy status-post AICD and avocal cord lesion requiring a prior tracheostomy. Patientpresented to the emergency department because ofshortness of breath attributed to difficulty managing hertracheostomy. Her initial physical examination andbloodworkwere unremarkable except for elevated bloodurea nitrogen and creatinine and a potassium of5.6 mEq ⁄ l. Routine chest X-ray revealed mild pulmo-nary congestion, right internal jugular CVC, and whatappeared to be a catheter fragment in the cardiac silhou-ette (Fig. 1A and B). CT scan confirmed the presence ofa foreign body (Fig. 1C), most likely a fractured cathetertip, in the right atrium. After discussion with the patientand the interventional radiology team regarding poten-tial risks and benefits of catheter tip retrieval, the cathe-ter fragment was successfully removed by percutaneoussnare technique under fluoroscopy guidance through afemoral approach (Fig. 2A–E). The catheter tip frag-ment and the indwelling CVC, which was exchanged atthe time of the procedure, were sent for pathology. Itwas later revealed that the fragment was part of a
Address correspondence to: Anand Reddy, One GustaveL.Levy Place, Mount Sinai School of Medicine, New York, NY10029, Tel.: +1-212-241-8002, Fax: +1-212-987-0389, or e-mail:[email protected].
Seminars in Dialysis—Vol 23, No 5 (September–October)2010 pp. 536–539DOI: 10.1111/j.1525-139X.2010.00756.xª 2010 Wiley Periodicals, Inc.
536

different catheter than the indwelling CVC (Fig. 3),which was found to be intact.
Discussion
Here we described a case of a retained catheter frag-ment incidentally discovered in the right atrium of anESRDpatient with a history ofmultiple prior CVCs suc-cessfully removed percutaneously via a snare technique.In addition to pulmonary embolization (8–10), otherpotential serious complications of dialysis catheter tipfracture may include: myocardial rupture, valvular per-foration, pulmonary artery rupture, infective endocardi-tis, and pulmonary abscess.
The fractured catheter component may lodge any-where distal to its original location including the venacava, right atrium, right ventricle, and pulmonary artery,depending on the size and weight of the broken segment(11). Removal of the foreign body by a nonsurgical per-cutaneous approach is possible in most cases. This canbe done using snares, hooked guide wires, Fogarty bal-loon catheters, orDormia baskets (12).
Central venous catheter fracture has primarily beenreported in patients with central venous access devicesused primarily for the administration of chemotherapy.These catheters are commonly inserted in the subclavian
vein and fracture is attributed to chronic mechanicalfriction and shear forces on the catheter as it passesbetween the clavicle and the first rib (4,13). The ‘‘pinch-off’’ sign, characterized by a kink or narrowing of thecatheter at this position, is an early warning sign forimpending catheter fracture at that site (4). This type ofmechanical friction and catheter stenosis may beavoided by choosing an internal jugular vein approach,which is better, suited for cuffed tunneled hemodialysiscatheters but not for long term implanted chemotherapydevices (10).
Early indications of catheter fracture are not welldescribed. In a few case reports, associated symptoms ⁄findings included intermittent catheter malfunction,resistance to fluid administration, pain during dialysistreatment, chest pain and palpitations, all of which arerelatively nonspecific (10,14,15). The majority of casereports are asymptomatic. Our patient did present withshortness of breath but this was directly attributable todifficulties with her tracheostomy. During a recent hos-pital admission, the patient developed an episode of ven-tricular tachycardia; however, given the patient’s historyof reduced LV function and prior dysrhythmia requiringAICD placement, we do not feel this was related to thepresence of the retained catheter fragment.
In our patient it was not clear why the catheter frac-tured but most likely as various reports have shown that
A
C
B
Fig. 1. Imaging studies (A) CXR lateral view; (B) CXR PA; (C) CT scan.
RETAINED FRACTURED CATHETER FRAGMENT 537

vascular catheter could be affixed to the wall of the supe-rior vena cava or the atrium (16–21). Tradional methodsof catheter removal not only cause vascular or atrialavulsion but may also result in catheter breakage withresultant retention of the broken fragments (16,17).Recently a novel new Laser sheath technique wasapplied to remove the retained catheters which showncatheter withdrawal without any risk of catheter fracture(22).Unfortunately, as we have learned all too well, the
dialysis access catheter is a double-edged sword. Withthe frequent use of cuffed catheters it is important to be
aware of all potential problems (however rare) and rec-ognize the need for amultidisciplinary approach inman-aging vascular access complications and failure.
References
1. Feldman HI, Kobrin S, Wasserstein A: Hemodialysis vascular accessmorbidity. J Am Soc Nephrol 7:523–535, 1996
2. NKF-DOQI clinical practice guidelines for vascular access. NationalKidney Foundation-Dialysis Outcomes Quality Initiative. Am J KidneyDis 30:S150–S191, 1997
3. Carr ME: Catheter embolization from implanted venousaccess devices:case reports. Angiology 40:319–323, 1989
4. Van der Hem KG, Meijer S, Werter CJ, van Groeningen CJ: ‘‘Sponta-neous’’ catheter fracture and embolization of a totally implanted venousaccess port. Neth J Med 38:262–264, 1991
5. Peynircioglu B, Ozkan F, Canyigit M, Cil BE, Balkanci F: Tunneledinternal jugular catheters in adult patients: comparison of outcomes inhemodialysis versus infusion catheters. Acta Radiol 48:613–619, 2007
6. Noyen J, Hoorntje J, de Langen Z, Leemslag JW, Sleijfer D: Spontane-ous fracture of the catheter of a totallyimplantable venous access port:Case report of a rare complication. J Clin Oncol 5:1295–1299, 1987
7. Krause U, Doetsch N, Meusers P, Kock HJ: Catheter break in animplantable central venous infusion system with embolization in thepulmonary artery. Dtsch Med Wochenschr 114:1882–1884, 1989
8. Vishal Sagar MD, Eleanor Lederer MD: Pulmonary embolism due tocatheter fracture from a tunneled dialysis catheter. Am J Kidney Dis43:e13–e14, 2004
9. Weijmer MC, Kars SM, ter Wee PM: A scanning electron microscopyanalysis of a spontaneous hemodialysis catheter fracture. Am J KidneyDis 38:858–861, 2001
10. Chawla LS, Chegini S, Thomas JW, Guzman NJ: Hemodialysis centralvenous catheter tip fracture with embolization into the pulmonaryartery. Am J Kidney Dis 38:1311–1315, 2001
11. Kadir S, Athanasoulis CA: Percutaneous retrieval of intravascular for-eign bodies. In: Athanasoulis CA, Pfister RC (eds). Interventional Radi-ology. Philadelphia, PA: W.B. Sauders, 1982:379–397
12. Fisher RG, Ferreyro R: Evaluation of current techniques for nonsurgi-cal removal of intravascular iatrogenic foreign bodies. Am J Roentgenol130:541–548, 1978
A B
D C
Fig. 2. (A–D) Percutaneous transvenous snare technique of intracardiac catheter fragment retrieval removal approach.
Fig. 3. Catheter fragment and catheter after removal.
538 Reddy et al.

13. Vazquez M: Vascular access for dialysis: recent lessons and newinsights. Curr Opin Nephrol Hypertension 18:116–121, 2009
14. Aitken DR, Minton JP: The ‘‘pinch-off sign’’: a warning of impendingproblems with permanent subclavian catheters. Am J Surg 148:633–636,1984
15. Schwab SJ, Beathard G: The hemodialysis catheter conundrum:hate living with them, but can’t live without them. Kidney Int 56:1–17,1999
16. Ndzengue A, Kessaris N, Dosani T, Mustafa N, Papalois V, HakimNS: Mechanical complications of long-term Tesio catheters. J VascAccess 10:50–54, 2009
17. Field M, Pugh J, Asquith J, Davies S, Pherwani AD: A stuck hemodial-ysis central venous catheter. J Vasc Access 9:301–303, 2008
18. Hassan A, Khaffa M, Al-Akira M, Lord R, Davenport A: Six cases ofretained central venous haemodialysis access catheters. Nephrol DialTransplant 21:2005–2008, 2006 Links
19. Liu T, Hanna N, Summers D: Retained central venous haemodialysisaccess catheters. Nephrol Dial Transplant 22:960–961, 2007
20. Thein H, Ratanjee SK: Tethered hemodialysis catheter with retainedportions in central vein and right atrium on attempted removal. Am JKidney Dis 46:35–39, 2005 Links
21. Foley PT, Carter RM, Uberoi R: Endovascular removal of long-termhemodialysis catheters. Cardiovasc Intervent Radiol 30:1079–1081, 2007
22. Carrillo RG, Garisto JD, Salman L, Merrill D, Asif A: A novel tech-nique for tethered dialysis catheter removal using the LASER sheath.Semin Dial 22:688–691, 2009
RETAINED FRACTURED CATHETER FRAGMENT 539







![Tunneled Peritoneal Catheter Placement in …downloads.hindawi.com/journals/bmri/2019/4132396.pdfof life []. Treatments with tunneled peritoneal catheter insertion, peritoneovenous](https://img.pdfslide.net/doc/110x75/5f8b6407216452101b766e47/tunneled-peritoneal-catheter-placement-in-of-life-treatments-with-tunneled-peritoneal.jpg)




















