Embed Size (px)
Citation preview

Journal of Surgical Oncology 8: 149-153 (1976)
Reticulum Cell Sarcoma of the Cecum and Macroglobulinemia: A Case Report ....................................................................................... ....................................................................................... MITCHELL LEVY,M.D., ALEX M. STONE, M.D., and NORBERT PLATT, M.D.
A case report is presented of an 81-yr old male who developed a reticulum cell sarcoma of the cecum while on immunosuppressive therapy for 13 yr for a primary diagnosis of macroglobulinemia. The considerable overlap between immunoproliferative disorders and the increased incidence of malig- nancies in patients receiving immunosuppressive therapy are discussed. .......................................................................................... ..........................................................................................
Key words: reticulum cell sarcoma, immunoproliferative disorders, immunosuppression
INTRODUCTION
Waldenstrom called attention to the fact that there is considerable overlapping be- tween multiple myeloma, macroglobulinemia, and other diseases. He suggested that they may represent a spectrum of “proliferative diseases of immunocytes,” (Waldenstrom, 1961). There also may be a higher incidence of unrelated nonlymphomatous malignancies in patients with immunoproliferative disorders. Patients afflicted with macroglobulinemia have disordered immune responses. This in itself may play a role in the appearance of other malignant conditions in patients so afflicted. In 1973, Penn and Starzl reported an increase in malignancies in patients receiving immunosuppressive therapy..
This case report documents an 8 1-yr old with a 13-yr history of macroglobulinemia, who, while under therapy with immunosuppressive agents, developed a malignant lympho- sarcoma of the cecum. Although colonic lymphosarcomas have been well documented in the surgical literature, their relationship to other immunoproliferative disorders and im- munosuppression has not been stressed.
From the Departments of Surgery and Pathology, Long Island Jewish-Hillside Medical Center, New Hyde Park, New York, and The Departments of Surgery and Pathology, Health Sciences Center, State University of New York at Stony Brook Address reprint requests to: Mitchell Levy, M.D., Department of Surgery, Long Island Jewish-Hillside Medical Center, New Hyde Park, New York 11040.
149 @ 1976 Alan R Liss, Inc., 150 Fifth Avenue, New York, N.Y. 10011

150 Levy, Stone, and Platt
CASE HISTORY
(LIJ No. 164664)
An 81-yr old white male was admitted to the Long .nd Jewish-Hillside Medical Center on June 1, 1974, complaining of weakness, abdominal pain, and an 18-lb weight loss. History dates back to 13 yr prior to admission when a diagnosis of Waldenstrom’s macroglobulinemia was made at this institution. He was treated with courses of Cytoxan, Leukeran, and Prednisone, and had done well over the 13 yr, necessitating no hospital care except for intermittent blood transfusions. 1 mo prior to this admission, he developed anorexia, weight loss, weakness, and right lower quadrant abdominal pain. There was no history of diarrhea, constipation, or rectal bleeding. There was no vomiting.
On physical examination, blood pressure was lOO/SO and pulse rate was 80 per min. The temperature was 98°F. The patient was a pale-looking, elderly white male in no acute distress. Examination of the head and neck was normal. Both chest fields were clear to auscultation. Cardiac examination revealed an ejection systolic murmur consistent with anemia. Abdominal exam revealed a 10-cm, hard, freely movable, tender mass in the right lower quadrant. The liver and spleen were not palpable. Rectal exam was normal. Exami- nation of the groins revealed inguinal adenopathy . Neurological exam was within normal limits. There was 2+ ankle edema bilaterally.
Pertinent laboratory data upon admission revealed a hemoglobin of 8.6 g and a
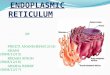
Fig. 1. Barium enema demonstrating intraluminal filling defect of the cecum.

151
hematocrit of 23.4%. RBC count was 2,410,000. WBC was 10,000. Differential revealed 4 bands, 8 metamyelocytes, 2 myelocytes, 50 polymorphonuclear leukocytes, 30 lympho- cytes, 3 monocytes, 2 eosinophils, and 1 basophil. Serum immunodiffusion revealed:
Reticulum Cell Sarcoma and Macroglobulinemia
IgG IgA I!@ normal 600- 1,200 1 6 5 4 1 0 50-110 patient 780 27 2,650
A barium enema (Fig. 1) demonstrated a large, intraluminal filling defect of the
After preoperative preparation, the patient was explored on June 3, 1974. A large, cecum.
noncircumferential, hard mass was found in the cecum (Fig. 2). The mass was not fixed to the retroperitoneum or other visceral structures. There were multiple, large, mesenteric lymph nodes palpable. An extended right hemicolectomy was performed.
Fig. 2. Photograph of gross specimen, Reticulum cell sarcoma of the cecum.
Pathological examination of the specimen (Fig. 3 and 4) revealed a reticulum cell sarcoma of the cecum with transmural extension into the pericolic fat with involvement of the regional lymph nodes.
cumbed 3 wk postoperatively to complications of pulmonary embolism combined with upper GI bleeding.
The postoperative course was initially uncomplicated, however, the patient suc-
DISCUSSION
This 81-yr old male developed a reticulum cell sarcoma of the cecum while on im-
It has been pointed out that there is considerable overlapping between macroglobu- munosuppressive therapy for 13 yr with a primary diagnosis of macroglobulinemia.

152 Levy, Stone, and Platt
Fig. 3. Reticulum cell sarcoma of the cecum (hematoxylin and eosin, x 25).
Fig. 4. Reticulum cell sarcoma of the cecum (hematoxylin and eosin, x 400).

153
linemia, reticulum cell sarcoma, and lymphatic leukemia (Waldenstrom, 1961). It is thought by some authors that these disease states represent different stages in the spectrum of pro- liferative diseases of immunocytes (Waldenstrom, 1961; Okano et d., 1966). There has been much debate as to whether malignancies of all types are more frequent in patients with primary macroglobulinemia. Weitzel found malignancies in 11 out of 57 cases stu- died (20%) (Weitzel, 1958).
Recently, there have been several reports of patients developing primary malignan- cies while undergoing immunosuppression, usually prior to or after rend transplantation (Penn and Starzl, 1973; Penn, 1970). It has been recently shown that the overall incidence of all malignancies was far greater (1 3/2,000) in this group than that seen in the popula- tion at large (8.2/100,000) under the age of 40 (McKhann, 1969). Furthermore, 50% of the patients developed primary tumors of the reticuloendothelial system and, in particu- lar, reticulum cell sarcoma (Penn and Starzl, 1973). These were all patients who were seen in the Transplant Service in Denver, Colo., and had undergone transplantation. It was un- clear whether this increase in malignancy was due to the fact that: (1) the immunosup- pressive agents were carcinogenic or mutagenic; ( 2 ) patients under treatment with immuno- suppressive agents were unable to suppress the growth of malignancies which were present but suppressed in the normal host; (3) patients treated with immunosuppressive agents after receiving homograft transplants were unable to suppress the growth of inadvertently transplanted oncogenic cells whch were effectively suppressed in the host prior to trans- plant (Penn and Starzl, 1973).
This unusual case is presented because of the possible relationships of the develop- ment of a malignancy in patients with an immunological disease further compounded by immunosuppressive therapy, and to emphasize the importance of aggressive follow-up in this type of patient population.
Reticulum Cell Sarcoma and Macroglobulinemia
REFERENCES
1. McKhann, C. F. (1969). Primary malignancy in patients undergoing immunosuppression for renal
2. Okano, H., Azar, H. A., and Osserman, E. F. (1 966). Plasmacytic reticulum cell sarcoma. Am. J. Clin.
3. Penn, 1. (1970). Malignant Tumors in Organ Transplant Recipients. Springer-Verlag, New York. 4. Penn, I., and Starzl, T. E. (1973). Immunosuppression and cancer. Transplant Proc. 5:l. 5. Waldenstrom, J. G. (1961). Studies on conditions associated with disturbed gamma globulin forma-
6. Weitzel, R. A. (1958). Carcinoma coexistent with malignant disorders of plasma cells. Cancer 11:
transplantation. A request for information. Transplant 8:2.
Pathol. 46:546.
tion (gammopathies). Harvey Lect. 56:21 l .
546.