Embed Size (px)
Citation preview

Retrograde Femoral (Seldinger) Aortography:Surgical Complications in 26 Cases
BERNARD SEIDENBERG, M.D., F.A.C.S., ELLIOTr S. HuRwIrr, M.D., F.A.C.S.
From the Surgical Division, Montefiore Hospital and Medical Center,and Long Island Jewish Hospital, New York City
VISUALIZATION of the aorta and itsbranches with radiopaque contrast mate-rial has become an essential component inthe diagnostic evaluation of many diseasestates. The Seldinger technic of retrogradecatheter aortography,6 usually via the femo-ral artery, has earned wide acceptance andhas been associated with a very low inci-dence of complications. Currently it is astandard procedure. This report presentsour experience with surgical complicationsinherent both in the method and in thedisease states for which this type of investi-gation is indicated. About 1,500 aortogramshave been performed in the past 3 years,resulting in 26 serious complications, mostof which required surgical intervention.The purpose is to analyze these complica-tions so as to provide: an alert to poten-tial dangers of this important procedure,methods to reduce incidence, and propermanagement.
In June 1963 McGraw4 reported five ma-jor complications in 372 arteriograms donevia the percutaneous transfemoral route.Three were acute arterial occlusions, oneresulting in amputation and another asso-ciated with acute myocardial infarction andcardiac arrest. The fourth was a false aneu-rysm, and the fifth involved penetration of
Submitted for publication March 3, 1965.Presented before the New York Surgical So-
ciety, February 10, 1965.Aided by a grant from the Westchester League
for Cardiac Children.
the aortic wall with resultant dissection,multiple embolization and death. Lang3surveyed 11,402 retrograde percutaneousaortograms and found seven deaths, 81 seri-ous complications and 325 minor complica-tions. The most common complication inthis series was arterial thrombosis, usuallyat the site of the needle puncture.
Material and MethodsAbout two thirds of the aortograms were
performed in the radiology department andone third in cardiac catheterization labora-tories. In the radiology department mostprocedures were evenly distributed be-tween aortograms for visualization of therenal arteries in hypertensive patients andaortic arch studies for cerebral vascular in-sufficiency. The remaining studies, ten percent of the total, were for other forms of se-lective arteriography. Therefore, two thirdsof these procedures were for hypertensionor arteriosclerosis. The other one third wasfor evaluation of cardiac disease for surgi-cal correction. Some earlier studies wereperformed by surgeons; in recent yearstrained senior personnel or residents op-erated under direct supervision. In mostcases the femoral artery was the site ofpercutaneous puncture and passage of aguide wire followed by the catheter. In theradiology department, when the patienthad peripheral vascular disease with inter-mittent claudication or non-palpable pulsesbelow the femoral arteries, the axillary ar-
221

222 SEIDENBERG AND HURWN"ITT
tery was uised. The catheter was passedeither into the ascendiing aorta for stuidiesof the arch or inlto the descenidiing aorta forrenal artery or peripheral arterial visuali-zation. In the cardiac catlheterizationi labo-ratory the femoral artery was used for leftheart catheterization in almost all instances.
After a clean arterial puncture is per-formed with a Cournand needle, the guidewire is inserted through the needle andpassed into the iliac artery and the aortaunder fluoroscopic television monitor. Theneedle is removed and the catheter passedover the gtuide wvire into the aorta, againunder television control. If there is im-pedance to the passage of either the guidewire or catheter which cannot be overcomeby gentle manipulation, the procedure isterminated in at that level. A gray Odmancatheter is used for aortic arch visualiza-tion and a polyethylene TE 240 catheter forthe renal arteries. Red or green cathetersare used for selective arteriograms only.The procedure is performed under estab-lished principles of surgical asepsis. Fol-lowing aortography or left heart catheteri-zation, the catheter is removed and pres-sure maintained over the arterial puncturesite for at least 15 minutes. For the first 2 or3 minutes the pressure occludes the artery,and then pressure is reduced to the pointwhere hemostasis is maintained and at thesame time a peripheral pulse is palpable.After 15 minutes pressure is slowly re-leased. If hemostasis is complete a pressuredressing is applied and pressure is appliedwith a weighted sand bag for at least 4hours. The patient is observed frequentlyduring the next 24 hours for evidence ofbleeding or hematoma at the punctture site.
ComplicationsThere were 26 major complications in
this series, 23 of which were related tothe arterial puncture. Fourteen occurred incases done in the radiology department and12 in the cardiac catheterization labora-
Annals of SurgeryFebruary 1966
tories. Common etiologic factors suggestspecific measures for minimizing their oc-currence. Twenty of the 26 patients re-quired surgical correction of the complica-tion, either as an emergency procedure orto prevent untoward sequelae.
Uncontrolled Bleeding. There were fiveinstances of uncontrolled bleeding from thefemoral arterial puncture site, four in car-diac catheterizations and one in a studyfrom the radiology department. All re-quired immediate surgical repair of thehole in the femoral artery. The high inci-dence of this complication in cardiac cathe-terizations is most likely due to manipula-tion of the catheter during left heart cathe-terization which results in enlarging thepuncture site. There is more catheter ma-nipulation by the cardiac team than duringaortography in the radiology department.One instance of uncontrolled bleeding ex-perienced in the radiology department oc-curred in a patient with malignant hyper-tension, blood pressure 300/160. This pa-tient bled enormously and required 8 unitsof blood before blood volume was restoredand the puncture wound closed surgically.To limit this complication it is advisable tominimize manipulation of the catheter andto perform manipulations with gentlenessand caution. Surgical repair of the bleed-ing puncture site was required in all cases,and complete recovery without impairmentof arterial circulation to the extremity re-sulted.Thrombosis. The most common compli-
cation was arterial thrombosis, usually oc-curring at the site of needle puncture. Thedistribution between the two departmentsof this complication is about equal, fivein radiology and six in the catheterizationlaboratory. Of the five occurring in theradiology department, four patients werebeing studied for arteriosclerotic cerebralvascular insufficiency. No one factor can beindicted for the high incidence of this com-plication. It is intrinsic in the method and

RETROGRADE FEMORAL AORTOGRAPHY
can be minimized only by careful technicand selection of the appropriate artery forpuncture. Multiple punctures predispose todamage of the arterial wall; excessive andforceful manipulation of the guide wire or
the catheter results in arterial injury andspasm; and excessive digital pressure may
result in thrombosis of the already trau-matized arterial wall. Most studies are per-
formed in patients with hypertension or
arteriosclerosis and there is usually diseasein the vessels used. Again, catheter ma-
nipulation required during cardiac cathe-terization traumatizes the arterial wall andpredisposes to thrombosis. The signs ofthrombosis usually appeared immediatelyor within 4 hours after the procedure. Pa-tients complained of pain and coldness inthe foot and leg, and previously palpablepulses were absent below the femoral ar-
tery. All but one patient with ischemicsigns due to thrombosis underwent surgi-cal correction by thrombectomy or throm-boendarterectomy, with closure of the ar-
teriotomy or application of a roof patch.Nine of ten surgically repaired patients re-
covered, with return of peripheral pulses.One patient went on to midleg amputationbecause late thrombectomy, performed 36hours after the onset of ischemia, failed tore-establish circulation. One patient was
not repaired surgically because of cardiacdisease and did not lose the extremity butdeveloped significant claudication. Earlysurgical intervention in ischemia secondaryto thrombosis of the femoral artery resultedin restoration of blood flow and freedomfrom sequelae.
False Aneurysm. There were five in-stances of false aneurysm. Only one fol-lowed cardiac catheterization, four were
from the radiology department. The eti-ology is quite clear. Three occurred in pa-tients with severe hypertension who hadretrograde aortograms for evaluation ofrenal arteries. The other instance in theradiology department and one in the car-
diac catheterization department were dueto inadequate management of the arterialpuncture site. In one, digital pressure was
released before the usual 15-minute period,no bleeding was seen and further pressurewas not employed. This patient developeda hematoma after several days and a pul--sating mass 6 weeks later. In another pa-tient arterial puncture was unsuccessfuland a catheter was not passed; apparentlythe usual digital pressure was not main-tained for the recommended period oftime. This patient developed a pulsatingfalse aneurysm 7 weeks postcatheterization.As soon as the diagnosis of false aneurysm
was made in these five instances, the aneu-
rysms were resected and the arteries re-
paired. One patient was admitted to thehospital in shock 6 weeks after a renalaortogram following rupture of a falseaneurysm in the left groin. This patienthad malignant hypertension. The aneurysmwas evacuated and the puncture site in thefemoral artery was sutured. The patientdied suddenly on the second postoperativeday with signs of cerebral hemorrhage, theonly mortality in the series of complica-tions. The other four patients recoveredfollowing surgical correction, with circula-tion in the affected extremity restored.Massive Hematoma. There were two pa-
tients early in the series of Seldinger pro-
cedures done in the radiology departmentwho developed massive hematomas in thegroin; one had hypertension, and in theother selective celiac axis arteriogram was
done for a possible pancreatic tumor. Al-though operation was considered at first,the hematomas resolved without formationof false aneurysms. It is likely that thesehematomas resulted from inadequate dig-ital pressure over the arterial puncture site.More careful adherence to technical stepsavoided this complication in the past 2years. Halpern 1 described prevention ofhematomas by diffusing escaped bloodaway from the vessels, by rotary motion
Volume 163Number 2 223

SEIDENBERG AND HURWITT Annals of SurgeryFebruary 1966
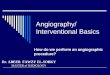
W... ''''''''''''''-:1' :~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~..FIG. 1. Aortic perforation. (Left) Roentgenogram of chest before Seldinger aortogram.
(Right) Roentgenogram immediately following intramural passage of catheter in descendingaorta demonstrating acute widening of mediastinum.
during application of digital pressure. Thismaneuver diffuses the ecchymosis and pre-
vents false aneurysms.
Catheter and Guide Wire Complica-tions. Three such complications occurred.In two aortic perforation and dissectionoccurred in patients with arteriosclerosis;one had an abdominal aortic aneurysm andperipheral arterial occlusive disease of thelower extremities, and the other had theLeriche syndrome. Both complications oc-
curred in the department of radiology. A53-year-old patient had a retrograde femo-ral arteriogram performed for evaluationof the peripheral circulation and the rela-tion of an aortic aneurysm to the renal ar-
teries. The patient tolerated the procedurewell, without any obvious difficulty. Whenhe was operated upon 2 days later an ex-
tensive periaortic hematoma was found,presumably due to perforation of the aortaby the guide wire or the catheter duringthe Seldinger aortogram. The second com-
plication was more serious. A 43-year-old
woman was being evaluated for arterio-sclerotic obstruciton at the aortic bifurca-tion, and right axillary retrograde aorto-gram was performed. The catheter passedinto the descending aorta and 2 to 3 cc.
of 50 per cent Hypoque were injectedmanually to demonstrate free entry of thecontrast medium into the lumen of theaorta. Under television control it was ob-vious that there was an intramural injec-tion. The patient complained of severe
chest pain and developed a shock-like col-lapse; x-ray (Fig. 1) of the chest showedmassive widening of the mediastinum. Theprocedure was immediately abandoned,and the team mobilized for operation withcardiopulmonary bypass. Meanwhile thepatient was treated supportively and ob-served in the recovery room, with chestx-rays repeated at short intervals. Vitalsigns stabilized and the widened medias-tinum also showed no progression over thenext 8 hours. Twenty-four hours later theprocess still appeared to be stable and the
224

Volume 163Number 2
RETROGRADE FEMORAL AORTOGRAPHY
TABLE 1. Analysis of Surgical Complicationsand Results of Therapy
Total CompleteType Cases Recovery Failure
1. Uncontrolled bleeding 5 5 02. Thrombosis 11 9 2*3. False aneurysm 5 4 1**
4. Massive hematoma 2t 2 05. Aortic perforation 2t 2 06. Fractured guide wire 1 1 0
26 23 3
* One claudication with no surgical correction. Onemidleg amputation following failure of late throm-bectomy.
** Death.t No surgical correction.
patient showed no further untoward effect.After 6 days of observation the patient was
discharged from the hospital. A monthlater chest x-ray films (Fig. 2) showedthat the mediastinum had returned to nor-
mal and an thromboendarterectomy of theaorta was performed with good result.There was no periaortic dissection belowthe diaphragm. This non-operative manage-ment of an aortic perforation has been thesubject of a separate report,2 and is in-cluded here because of its unique features,even though the axillary and not the femo-ral artery was involved.One instance of a fractured guide wire
and perforation of the iliac artery in a 3-year-old girl was encountered early in theseries in the cardiac catheterization labora-tory. Passage of the guide wire was ob-structed at the level of the aortic bifurca-tion. The wire was not passed any furtherand the catheter was passed over the wire.On removal of the wire it was noticed thatthe flexible tip was missing. X-rays afterthe procedure showed the wire in the retro-peritoneal space, and operation was per-formed. The guide wire was found outsideof the lumen of the vessel and was re-
moved; a large perivascular retroperitonealhematoma was evacuated. This patient re-
covered without sequelae from this com-
plication. Guide wire fractures are easily
A
FIG. 2. Aortic perforation. Roentgenogram ofchest 1 month later revealing spontaneous resolu-tion of widened mediastinum.
eliminated by carefully inspecting eachwire before use. Correct passage of theguide wire is essentially without sensation.Any resistance requires immediate cessa-
tion of the procedure. The same care isrequired in passing the catheter into theartery and aorta. It is not difficult for a
catheter tip to penetrate an arterioscleroticulcer of the intima in a diseased aorta.This is the reason for manual injection ofa small test dose of contrast substance be-fore the pressure injection for aortographyis performed. The test confirms the intra-mural position of the catheter and avoidsdissection or perforation by injection of a
large volume. This complication was de-scribed by Templeton; 7 a dissecting aneu-
rysm of thoracic aorta was successfullytreated by excision and replacement witha Dacron prosthesis.
Conclusions
Deaths and serious complications may
follow diagnostic procedures. The Seldingertechnic of retrograde catheter aortographyis an essential diagnostic modality today.Complications inherent in the method and
225

SEIDENBERG AND HURWITT Annals of Surgery226 February 1966
in the diseases being studied are presentedin the hope that accidents may be limitedto a minimum and that proper manage-ment may be instituted. These proceduresare usually done in high-risk patients. Com-plications may be limited to a minimum byexperienced personnel who exercise judg-ment and caution and adhere to technicaldetails.
It is doubtful that these complicationscan be eliminated entirely. Twenty-threeof 20 patients recovered following prompt,adequate treatment of the complication(Table 1). One death occurred severaldays after repair of a false aneurysm in apatient with malignant hypertension. Mid-leg amputation in another patient mighthave been avoided if thrombectomy hadbeen performed within the first 8 to 12hours following occlusion; late throm-bectomy failed to re-establish patency ofthe femoralpopliteal vessels. Claudicationwith limb survival preferable to operationin the remaining patient because of ad-vanced cardiac disease.
SummaryTwenty-six surgical complications follow-
ing the Seldinger technic of retrograde(femoral) catheter aortography have beenreported. Some were inherent in the pro-
cedure, while others were related to thedisease for which the investigation wasperformed. Aortograms were performed inthe radiology department and the cardiaccatheterization laboratories and complica-tions are discussed accordingly.
Suggestions are presented for minimizingoccurrence of these complications. Theseexperiences demonstrate that aggressivecorrection of vascular complications resultsin a high percentage of recoveries. Aortog-raphy requires hospitalization and cannotbe done safely on an out-patient basis. Fa-cilities should be available for vascular op-erative treatment whenever indicated.
References1. Halpern, M.: Percutaneous Transfemoral Ar-
teriography; An Analysis of the Complicationsin 1000 Consecutive Cases. Amer. J. of Roent-genol., 92:918, 1964.
2. Hurwitt, E. S. and Seidenberg, B.: The Non-Operative Management of Two Cases ofCatheter Perforation of the Aorta. Amer. J.Surg., 110:452, 1965.
3. Lang, E. K.: A Survey of the Complicationsof Percutaneous Retrograde Arteriography:Seldinger Technique. Radiology, 81:257, 1963.
4. McGraw, J. Y.: Arteriography of PeripheralVessels, A Review with Report of Complica-tions. Angiology, 14:306, 1963.
5. Seldinger, S. I.: Catheter Replacement of theNeedle in Percutaneous Arteriography: ANew Technique. Acta Radiol., 39:368, 1953.
6. Templeton, J. Y., Johnson, R. G. and Griffith,J. R.: Dissecting Aneurysm of Thoracic Aortaas Complication of Aortography. J. Thor.Surg., 40:209, 1960.