Embed Size (px)
Citation preview

Retropharyngeal Cystic Hygroma ASHOK VERMA, SATISH MEHTA BISHAN RADOTRA ~ S. B. S. MANN
A case of cystic hygroma of retropharyngea! space is being reported in a 5 years male child. The patient presented wi th a painless swelling on right side of the neck, dysphagia, change in voice and respiratory stridor. Surgical excision was done under general anaesthesia and the histopatho- Iogy of which was consistent w i th cystic hygroma.
Cystic hygromas are thin walled cysts lined with flat endothelium and filled wi th yel lowish fluid. These are said to owe their origin to sequestration of portions of primitive embryonic lymphatic sac. Lymphangioma constitutes 5.6% of all the benign tumours of infancy and chi ldhood (Leonidas, 1970). 50-60% of cystic hygromas are present at birth and 80-90% pre- sent by 2 years of age. About 75% of these are seen in the neck, 20% in the axilla and 5% on the trunk and extremities (Sowenson, 1978).
Unusual sites like parotid, lips, nose, larynx, preauricular, medias- tinum, retroperitoneal, mesentry, inguinal region etc. have been reported in the literature. But no case of cystic hygroma involving the retropharyngeal space has been reported in the reviewed literature.
Case Report :
K. S. 5 years male child reported to Outpatient Department of Ear, Nose ~ Throat of Nehru Hospital, Post Graduate Institute of Medical Education ~ Research, Chandigarh with the fo l lowing complaints :
Ashok Verma, Senior Resident, Deptt. of E.N.T. Satish Mehta, Junior Resident, Deptt. of E.N.T. Bishan Rodotra, Senior Resident, Deptt. of Pathology. S. B. S. Mann, Associate Professor, Deptt. of E.N.T. Postgraduate Institute of Medical Educa- tion 8 Research, Chandigarh-160012
Request for reprints : Dr. S. B. S. Mann, Associate Professor, Department of E.N.T., Postgraduate Institute of Medical Education El- Research, Chandigarh-160 012 (India)
Painless gradually progressive swell ing on right side of the neck for the past 5 months.
- - Diff iculty in swal lowing, change in voice and diff iculty in brea- thing of two days duration.
On examination the child was of average built having respiratory stridor with respiratory rate of 46/ min, pu lse : 96/min, blood pres- sure was 100/70 mm of Hg. The child was afebrile. Local examina- t ion revealed a swell ing on (R) side of the neck under the sterno- mastoid muscle, the swell ing was non-tender, cystic, f luctuant and non-transil luminant. No pulsation and bruit was present over the swell ing. Trachea was markedly shifted to left side. Oral cavity examination revealed a smooth bulge in the post pharyngeal wall, extending from the nasopharynx down to the level of the larynx. The overlying mucosa was normal.
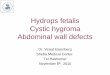
The child was admitted wi th the provisional diagnosis of retro- pharyngeal abscess extending to the parapharyngeal space. X-ray soft tissues neck (Lateral view) revealed an increase in the prever- tebral soft tissue shadow extendin.o. from base of skull to the 7th cervical vertebra. The trachea was shifted forwards and supraglottic airway was occluded (Fig. 1).
About 80 cc of l ight yel low fluid was aspirated from the swell ing and the patient was relieved of stridor. After 5-6 hours the patient again developed stridor. Emer- sency tracheostomy and explora- t ion was done under General Ana- esthesia. Transverse collar incision was given and skin flaps including the platysma were elevated. Tra- chea was lying deep to the left
sternomastoid muscle, which was incised horizontally to expose it. Tracheostome was made in the 3rd and 4th tracheal rings. A cystic swell ing was seen under the (Rt.)
Fig. 1. Pr'e-operative X-ray soft tissue of neck lateral view showing increase in the pre-vertebral shadow extending from base of skull to the seventh cervical vertebra.
sternomastoid muscle which was extending posteriorly on to the vertebral column pushing the oeso- phagus forwards and to the left, superiorly to the base of the skull and inferiorly to the superior media- stinum about 1 cm below the upper border of sternum. The cyst got ruptured while dissecting it from the surrounding tissues and multiple small cysts were seen, which were removed and sent for histopathological examination. Right recurrent laryngeal nerve was identified and saved.
128 Indian Journal of Otolaryngology, Volume 39, No. 3, September, 1987

RETROPHARYNGEAL CYSTIC H Y G R O M A - - V E R M A et al
Postoperatively the patient was kept on Ryle's tube feeding for 3 days. Decannulat ion was done on 15th post-operat ive day. Post- operative X-ray soft tissue neck was done which revealed normal pre- vertebral soft tissue shadow Airway and speech wasnormal too.
H i s t o p a t h o l o g i c a l R e p o r t :
Sections prepared from the spe- cimen showed dilated cystic spaces lined by single layer of endothelial cells and containing homogeneous eosinopoil ic material and erythro- cytes. The wal ls of these spaces also contained smooth muscle fibres. The intervening stroma was
loose oedematous and contained nerve fibres. Two small lymph
Fig. 2. Cystic hygroma composed of many large dilated spaces and occasion- ally scattered collections of lymphocytes. Islands of smooth muscle are seen in the walls of spaces. H 8- E × 55.
nodes present in the specimen showed reactive hyperplasia (Fig. 2).
Discuss ion :
Cystic hygroma involving the neck is quite common in infancy and chi ldhood. Unusual sites like larynx (Alexander, 1985) media- st inum (Rudolph, 1982) ilium bone (Bickel, W.H., 19-4,7) genaralised lymphangioma with chvlo thorax (Leonadis, 1970) mesentery (Alex- ander, 1965) and inguinal region (Najman, 1967) have been des- cribed. No reference could be found of cystic hygroma involving retropharyngeal space. The impor- tance to recognise this condi t ion lies in the differential diagnosis of retropharyngeal cold abscess.
References
1. Bickel, W.H. and Broders, A.C. : (1947) : Primary lymphangioma of ilium report of a case. J. Bone Joint Surg., 29 : 517.
2. Bitl, A.H. Et Jr. Sumner D.S. (1965) : A unified concept of lymphangioma and cystic hygroma. Surg. GynaecoL Obstet. 120 : 79.1965
3. Camishion R.C., Templeton J.V. (1962) : Cervico-mediastinal cystic hygroma. Paediatrics, 29 : 831.
4. Goestsch, E. (1938) : Hygroma colli cysticum and hygroma axillare : Pathologic and clinical study and report of 12 cases. Arch. Surg., 36 : 394, 1938
5. Harkings, G.A. and Sabiston, D.C. (1960) : Lymphangioma in infancy and childhood. Surgery, 47 : 811.
6. Murphishi, G., Archiuve, E.L., Krause, J.R. (1970) : Generalised lymphan- gioma in infancy with chylothorax. Paediatrics, 46 : 566.
7. Najman, E. Fabecic--Sabadi, R. and Temmer, B. (1967) : Lymphangioma in the inguinal region with cystic lymphangiomatosis of bone. J. Paediat., 71 : 561.
8. Ninh, T.N., Ninh, T.A. (1974) : Cystic hygroma--a report of 126 cases. J. Paediatr. Surg., 9 : 191.
9. Pfahler, G.E. and Perlman, H.H. (1950) : Cystic hygroma of neck and mediastinum successfully treated by roentgen rays. Amer. J. Roetge- nol. 63 : 539.
10. Portman, U.V. (1945) : Cystic hy- groma--report of 3 cases. Cleve- land Clin. Quart., 12 : 98.
11. Rosen Quist, C.J. and Wolfe, D.C. (1968) : Lymphangioma of bone. J. Bone Joint Surg. (Amer) 50-A : 158.
12. Singh, S., Buboo, M.L., Pathak, I.C. (1971) : Cystic hygroma in children. Report of 32 cases including lesions of rare sites, Surgery, 69 : 941.
Indian Journal of Otolaryngology, Volume 89, No. 3, September, 1987 129