Embed Size (px)
Citation preview

International Journal of
Radiation Oncologybiology physics
www.redjournal.org
Physics Contribution
Retrospective Reconstructions of Active BoneMarrow Dose-Volume HistogramsCristina Veres, MSc,*,y,z Rodrigue S. Allodji, PhD,*,y,z
Damien Llanas, MSc,*,y,z Jeremi Vu Bezin, MSc,*,y,z
Jean Chavaudra, PhD,y Jean Pierre Mege, PhD,y
Dimitri Lefkopoulos, PhD,y Eric Quiniou, PhD,jj Eric Deutsh, MD,y,x
Florent de Vathaire, PhD,*,y,z and Ibrahima Diallo, PhD*,y,z
*Radiation Epidemiology Group, Center for Research in Epidemiology and Population Health,Institut National de la Sante et de la Recherche Medicale, UMR 1018, Villejuif, France; yInstitutGustave Roussy, Villejuif, France; zUniversity Paris-Sud XI, Villejuif, France; xInstitut National de laSante et de la Recherche Medicale, UMR 1030, Villejuif, France; and jjInstitut National de la Sante etde la Recherche Medicale UMR 759, Orsay, France
Received May 6, 2014, and in revised form Aug 14, 2014. Accepted for publication Aug 19, 2014.
Summary
Published data regarding thepercentage volume of activebone marrow (ABM) irradi-ated to various dose levelsare extremely rare. Such in-formation might, however,offer new perspectives onstudies aiming at assessingradiation-related leukemia. Amethod has been developedto allow retrospective evalu-ations of the percentage vol-ume of the ABM irradiatedto various doses levels.Wepresent here the dose recon-struction method and a sum-mary of the doses-volumedata for ABM.
Reprint requests to: Dr Ibrahima Diallo, PhD
Group, Center for Research in Epidemiology and
Int J Radiation Oncol Biol Phys, Vol. 90, No. 5
0360-3016/$ - see front matter � 2014 Elsevie
http://dx.doi.org/10.1016/j.ijrobp.2014.08.335
Purpose: To present a method for calculating dose-volume histograms (DVH’s) to theactive bone marrow (ABM) of patients who had undergone radiation therapy (RT) andsubsequently developed leukemia.Methods and Materials: The study focuses on 15 patients treated between 1961 and1996. Whole-body RT planning computed tomographic (CT) data were not available.We therefore generated representative whole-body CTs similar to patient anatomy. Inaddition, we developed a method enabling us to obtain information on the density dis-tribution of ABM all over the skeleton. Dose could then be calculated in a series ofpoints distributed all over the skeleton in such a way that their local density reflectedage-specific data for ABM distribution. Dose to particular regions and dose-volumehistograms of the entire ABM were estimated for all patients.Results: Depending on patient age, the total number of dose calculation points gener-ated ranged from 1,190,970 to 4,108,524. The average dose to ABM ranged from 0.3to 16.4 Gy. Dose-volume histograms analysis showed that the median doses (D50%)ranged from 0.06 to 12.8 Gy. We also evaluated the inhomogeneity of individual pa-tient ABM dose distribution according to clinical situation. It was evident that the co-efficient of variation of the dose for the whole ABM ranged from 1.0 to 5.7, whichmeans that the standard deviation could be more than 5 times higher than the mean.Conclusions: For patients with available long-term follow-up data, our method pro-vides reconstruction of dose-volume data comparable to detailed dose calculations,which have become standard in modern CT-based 3-dimensional RT planning. Our
, Radiation Epidemiology
Population, Inserm UMR
1018, F-94800 Villejuif, France. Tel: þ331 42 11 49 18. E-mail: ibrahim.
Conflict of interest: none.
, pp. 1216e1224, 2014r Inc. All rights reserved.

Volume 90 � Number 5 � 2014 ABM dose-volume metrics 1217
Table 1 Summary of the number ofmalignant neoplasms
Type of FMNNo. ofpatients
No. ofPTVs
CNS 2 5STS 2 2Renal tumors 4 5Hepatoblastoma 1 1Lymphomas 4 7Nasopharynx tumor 1 2Testis tumor 1 1
Abbeviations: CNS Z central nervous syst
strategy of using dose-volume histograms offers new perspectives to retrospectiveepidemiological studies. � 2014 Elsevier Inc.
Introduction
Interpretation of the results of studies of leukemia risk aftertreatment with radiation therapy (RT) and chemotherapy isnot clear; a complication is the almost systematic co-treatment with powerful chemotherapeutic drugs andfrequent failure to account for RT dose heterogeneity. Amajor reason for the latter complication is the weaknessesof methods used to estimate doses to active bone marrow(ABM), for epidemiological studies. To date, most of thesemethods have been limited to evaluations of a weightedaverage dose to the total ABM (1-4). Dose-volume-histograms (DVH), which have become a standard inmodern computed tomography (CT)-based 3-dimensionalRT planning, might provide better information, toimprove the ability of epidemiological studies of leukemiarisk after cancer treatment to account for RT dose hetero-geneity. To our knowledge, no previous dosimetric studyhas presented detailed data for ABM RT dose-volumeevaluations from different RT regimens involved in retro-spective studies of leukemia risk after cancer treatment.These data may be of interest for practitioners, especiallyas the estimation of the leukemia risk of modern RT re-quires development of dose-response relationships capableof accounting for RT dose heterogeneity, which in turn,requires DVH to ABM of past RT regimens given to pa-tients for whom long-term follow-up data are alreadyavailable.
In this study, we report development of a method thatallows retrospective evaluations of the percentage of vol-ume of the ABM irradiated to various dose levels. Wepresent the dose reconstruction method and a summary ofthe dose-volume data for the ABM of 15 cases ofsubsequent leukemia occurring after childhood cancer RT.Practical figures for the average dose and dose heteroge-neity that can be kept in mind are also provided.
PTVs, doses delivered to PT
Region involved
Head, thorax, abdomenThorax, pelvisThorax, abdomenabdomenHead, Thorax, AbdomenHead, Neck, thoraxPelvis
em; FMN Z first malignant neop
Methods and Materials
Patients
The present analysis focused on 15 patients whose subse-quent leukemia was diagnosed after a latency period of atleast 2 years since the date of the RT.
Radiation therapy techniques
For reconstruction of the RT, we collected each patient’sclinical parameters, including sex, age, height, weight, andany available data on external measurements that could beobtained from treatment planning charts. We abstractedeach patient’s RT parameters, including target-volume lo-cations, prescribed dose, number of fields, field configura-tion(s), field size(s), type of treatment machine, beamenergies, and other parameters.
Segmentation of ABM compartments
Whole-body RT planning CT data for the patients were notavailable. Therefore, to enable computation of entire ABMdose distribution reconstructions for each individual, weused a surrogate anatomy, whole-body RT planning CTsfrom 6 patients (4 males and 2 females). First, each of the15 patients was matched to the closest whole-body scan ofthe same sex, age, and similar weight and height, lying inthe relevant treatment position. Then, when the informationwas available for patient external dimensions, the matchedwhole-body scans were rescaled accordingly.
In each representative patient CT, the skeleton wassegmented into 19 fragments according to age-specificdistribution of ABM tabulated by the International Com-mission on Radiological Protection (ICRP) (5). For dose
Vs, and fractionation regimens for the different types of first
PTV irradiation details
Total dose (Gy) Dose per fraction (Gy) Duration (weeks)
25.4 [25.0, 55.2] 1.7 [0.8, 1.8] 6 [3, 7]24.5 [24.0, 25.0] 1.3 [1.0, 1.6] 3 [3, 4]20.0 [9.0, 30.0] 1.6 [1.5, 2.3] 3 [1, 5]
42.0 1.8 620.0 [20.0, 34.8] 1.7 [0.9, 1.8] 4 [2, 8]20.0 [19.6, 20.4] 1.1 [1.1, 1.1] 6 [6, 6]
20.0 2.5 3
lasm; PTV Z planning target volume; STS Z soft tissue sarcoma.

Fig. 1. Scatter plot of the 4 different distributions of dose calculation points involved in the evaluation of the ABM dosedistribution in the population under study. The skeleton segmentation into 19 compartments and the density of points per regionare based on the age-specific distribution ofABMas defined by the ICRP report 89, such that the distribution of the pointswithin agiven subregion is homogeneous. ABMZ active bone marrow; ICRPZ International Commission on Radiological Protection.
Fig. 2. Scatter plot of the inhomogeneous dose distribution in the ABM for three selected patients with different first cancertypes. ABM Z active bone marrow.
Veres et al. International Journal of Radiation Oncology � Biology � Physics1218

Volume 90 � Number 5 � 2014 ABM dose-volume metrics 1219
computation purposes, we distributed at random throughoutthe skeleton a series of points in such a way that theirdensity in a region reflects the proportion of ABM in thatparticular region. ABM distribution based on ICRP dataassumes that the distribution of ABM is homogeneouswithin each fragment.
Dose calculations
Photon beamsFor irradiations with photon beams, the absorbed dose to agiven voxel in the representative patient (Di) was calculatedusing Equation 1.
DiZXN
jZ0fDðdmax;Ad;SSDÞ �PDDðd;As;SSDÞ
�OARðx;d;AdÞgjwith i as the calculation point within the organ volume, j is[1,.,n] radiation fields, SSD is source to skin distance,PDD(d, As, SSD) is the percentage of depth dose at depthd in tissue for field size As at surface at SSD, D(dmax, Ad,SSD) is the absorbed dose on the beam central axis at depthdmax in tissue with surface at SSD for field size Ad atcalculation point, and OAR(x, d, Ad) is the off-axis ratio atoff-axis distance x and depth d in tissue for field size Ad atcalculation point.
Reference values for PDD (6) were used. For out-of-fielddose evaluations, extended values for off-axis-ratio (OAR)were derived from in-water phantom measurements ach-ieved and gathered since the mid-1980s (7, 8) especially forthis purpose. Internal tissue heterogeneity corrections werenot applied to dose calculations for this study.
For electrons beams, dose distributions computed withhomemade software were used. All details regardingmethods and accuracy of this procedure can be obtainedfrom previous publications (8).
Accumulated doseThe local radiation dose (ie point dose) was defined as thecumulative absorbed dose to ABM during the periodranging from the date of the initial RT for the firstmalignant neoplasm (FMN) to the date of the subsequentleukemia diagnosis minus 2 years. Possible additionaldoses due to imaging procedures were not accountedfor.
Dose and dose-volume metrics
DVHs were computed for patients’ ABM. This was madepossible because the dose calculation points generated atrandom in the whole ABM volume are presented in sucha way that each point is representative of an ABM vol-ume element. We evaluated DV, the absorbed dose infraction V of the ABM volume. Without a preciseknowledge of the relevant values of dose-volume datasuitable for the risk associated with ABM irradiation, wedecided to provide descriptive data on the near minimum
D98%, the near-maximum D2%, and the median absorbeddose D50%.
Results
Patients
Among the 15 patients, 11 were male. The median age atdiagnosis of the FMN was 4.7 years (range, 1.1-15.9 years),and the median calendar year at diagnosis of the FMN was1985 (range, 1961-1996). The FMNs consisted of renaltumors (nZ4), lymphomas (nZ4), soft tissue sarcomas(nZ2), central nervous system (CNS) tumors (nZ2),hepatoblastomas (nZ1), nasopharynx tumors (nZ1), andtestis tumors (nZ1). The median age at diagnosis of thesubsequent leukemia was 17.4 years (range, 6.6-51.0 years), and the median calendar year at diagnosis was1994 (range, 1977-2008). Patients could also have under-gone chemotherapy.
Radiation therapy techniques
Information on the different RT regimens for the patientsunder study is summarized in Table 1. Although the size ofthe population under study was small, the different kinds oftumors led to different target volumes (planning targetvolume [PTV]), locations, and doses.
Thus, depending on FMN type and individual patientclinical situation, the PTV can be a subvolume of the patienthead, neck, thorax, abdomen, or pelvis, or any combinationof these. Several PTVs can belong to the same individual;among them, some can be a boost or a recurrence.
Among the PTVs, 21 were prescriptions for initial FMNand 2 were for a recurrence. The total prescribed dose to aPTV ranged from 9.0 Gy to 55.2 Gy. The dose fraction-ation schedule for a PTV was 0.8 Gy to 2.5-Gy fractions,5 days per week during 1 to 8 weeks. A total of 51 beamswere involved in the RT of the 15 patients. Among these,28 were delivered using source-to-axis distance (SAD) and23 using source-to-skin distance (SSD) techniques,respectively. The predominant beam qualities were high-energy X-photons from linear accelerators (nZ25) and g-photons from cobalt-60 machines (nZ16). Electron beamsand 200- kV x-rays were involved in the treatment of a fewpatients.
ABM compartmental distribution
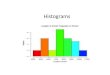
Figure 1 presents the 4 different distributions of dosecalculation points involved to assess the ABM dose dis-tribution in the population under study. The skeletonsegmentation into 19 compartments and the density of thepoints within a given region were based on data for age-specific distribution of ABM as defined by ICRP report89 (5). Considering Figure 1, one can remark that theconcentration of points in a given area varies with age. For

Table 3 Absorbed dose (DV) in fraction V of the ABM volume
Parameter
Sex
F M F M F M M M
Age, y 1.1 1.5 1.8 1.8 2.4 3.2 3.3 4.7Type of FMN Kidney STS Kidney Liver STS Kidney Kidney HLDose to PTV, Gy 20 25 33 42 24 30 18.6 20Year of RT 1978 1985 1967 1986 1961 1978 1973 1990
D50% [D98% � D2%]
Cranium 0.08 [0.04�0.2] 0.04 [0.03�0.06] 0.1 [0.05�0.3] 0.5 [0.2�1.2] 0.3 [0.1�0.5] 0.06 [0.04�0.1] 0.06 [0.03�0.1] 0.2 [0.04�0.9]Mandible 0.1 [0.07�0.4] 0.05 [0.04�0.07] 0.2 [0.1�0.4] 0.9 [0.3�1.6] 0.4 [0.3�1.2] 0.1 [0.07�0.2] 0.09 [0.04�0.1] 0.7 [0.4�1.1]Scapulae 0.6 [0.2�1.3] 0.1 [0.09�0.3] 0.9 [0.4�2.2] 1.5 [0.6�2.2] 1.7 [0.8�10.7] 0.5 [0.2�1.9] 0.3 [0.08�0.6] 2 [0.9�12.7]Clavicles 0.3 [0.2�0.7] 0.1 [0.09�0.1] 0.6 [0.4�1.2] 0.9 [0.4�1.6] 1.6 [0.8�2.9] 0.3 [0.2�0.6] 0.2 [0.08�0.3] 13.2 [1.6�20.9]Sternum 1.2 [0.3�18.5] 0.1 [0.09�0.3] 2.1 [1�13.6] 1.4 [0.4�5.2] 7.8 [2.2�31.3] 1.4 [0.3�28.5] 0.4 [0.2�2.4] 18.8 [15.3�21]Ribs 1.6 [0.3�22.5] 0.3 [0.09�1.1] 3.6 [0.4�50.3] 2 [0.5�37.1] 2.9 [0.9�28.6] 1.9 [0.2�35.5] 0.7 [0.1�21.3] 2.1 [0.5�21.3]Cervical vertebrae 0.2 [0.07�0.3] 0.07 [0.05�0.09] 0.2 [0.1�0.4] 0.4 [0.3�1.1] 0.6 [0.3�1] 0.1 [0.08�0.2] 0.1 [0.05�0.2] 1.5 [0.6�21.2]Thoracic vertebrae 1.8 [0.2�18] 0.3 [0.08�0.7] 2.4 [0.4�39.8] 1.1 [0.4�39.6] 6.5 [0.9�27.4] 2 [0.2�30.1] 0.8 [0.1�17.3] 20.1 [2�21.4]Lumbar vertebrae 17.4 [16.7�18.3] 2 [0.6�7.4] 34.4 [32.1�42.6] 21.1 [1.6�41.6] 2.5 [1�24.6] 29.3 [26.6�30.3] 17.6 [3.5�18.3] 0.6 [0.2�1.6]Sacrum 17.2 [2.4�17.9] 24.6 [7.4�27.7] 34.3 [5.6�40.8] 1.2 [0.7�3.4] 0.7 [0.4�1.1] 4.8 [1.8�27.7] 10 [1.7�18.1] 0.1 [0.07�0.3]Os coxae 3.6 [1.3�21.1] 25.2 [0.04�27] 20 [2�45.8] 1.3 [0.6�2.6] 0.5 [0.2�1.1] 1.8 [0.6�29.4] 1.4 [0.2�19.3] 0.07 [0.04�0.2]Femora UH 1.2 [0.3�3.7] 24.8 [1.6�27.7] 2.5 [0.5�19.9] 0.9 [0.4�1.9] 0.3 [0.2�0.4] 0.5 [0.1�1.5] 0.4 [0.08�1.3] 0.03 [0.02�0.05]Femora LH 0.1 [0.07�0.3] 0.5 [0.4�1.5] 0.3 [0.2�0.5] 0.6 [0.2�1.1] 0.1 [0.08�0.2] 0.1 [0.09�0.2] 0.1 [0.06�0.2] 0.01 [0.01�0.02]TFP 0.07 [0.03�0.1] 0.2 [0.09�0.4] 0.1 [0.05�0.2] 0.2 [0.2�1.1] 0.06 [0.03�0.1] 0.06 [0.03�0.1] 0.07 [0.06�0.2] 0.01 [0.008�0.01]AFB 0.04 [0.03�0.05] 0.06 [0.04�0.09] 0.04 [0.03�0.06] 0.2 [0.2�0.2] 0.02 [0.02�0.03] 0.03 [0.03�0.03] 0.06 [0.06�0.06] 0.008 [0.008�0.009]Humeri, UH 1 [0.4�3.5] 0.3 [0.1�0.7] 1.2 [0.5�3.8] 1.6 [0.6�2.2] 1.3 [0.6�3.3] 0.8 [0.4�4] 0.2 [0.07�1.2] 0.8 [0.5�2]Humeri, LH 1.3 [0.7�5.1] 0.9 [0.5�1.4] 2.3 [0.8�5.8] 3.7 [1.9�21.2] 0.8 [0.5�3.7] 1.7 [0.6�5] 0.2 [0.1�1.7] 0.3 [0.1�0.8]Ulnae-radii 1.2 [0.4�2.7] 2.2 [0.9�15.3] 1.7 [0.7�3] 1.5 [0.6�17.5] 0.5 [0.3�2.1] 0.6 [0.3�3.5] 0.2 [0.09�0.8] 0.06 [0.02�0.2]Wrist-hand 0.4 [0.2�1.4] 3 [0.7�19.7] 0.7 [0.4�2.2] 1.2 [0.7�1.8] 0.2 [0.2�0.4] 0.2 [0.1�0.5] 0.1 [0.07�0.2] 0.02 [0.01�0.03]Whole ABM 0.3 [0.03�19.3] 0.2 [0.03�26.2] 0.5 [0.04�40.4] 0.7 [0.2�35.6] 0.4 [0.02�23.6] 0.6 [0.03�30] 0.3 [0.04�18.2] 0.2 [0.008�20.6]
Abbreviations: ABM Z active bone marrow; AFB Z ankle and foot bones; FMN Z first malignant neoplasm; HL Z Hodgkinlymphoma; LH Z lower half; LS Z Lymphosarcoma; PTV Z planning target volume; RT Z radiation therapy; STS Z soft tissuesarcoma; TFP Z tibiae fibulae patellae; UH Z upper half.
Table 2 Average doses to the 19 subregions and to the whole ABM for the 15 patients under study
Parameter
Sex
F M F M F M M
Age, y 1.1 1.5 1.8 1.8 2.4 3.2 3.3Type of FMN Kidney STS Kidney Liver STS Kidney KidneyDose to PTV 20 25 33 42 24 30 18.6Year of RT 1978 1985 1967 1986 1961 1978 1973
Mean � SD dose (Gy) to ABM and mean dose evaluated in each of the 19 subregionsCranium 0.09 � 0.04 0.04 � 0.009 0.1 � 0.05 0.5 � 0.3 0.3 � 0.09 0.07 � 0.02 0.06 � 0.02Mandible 0.2 � 0.1 0.05 � 0.008 0.2 � 0.08 0.9 � 0.4 0.4 � 0.2 0.1 � 0.02 0.09 � 0.03Scapulae 0.6 � 0.3 0.2 � 0.05 1 � 0.4 1.3 � 0.5 2.3 � 2.3 0.7 � 0.4 0.3 � 0.1Clavicles 0.4 � 0.2 0.1 � 0.009 0.7 � 0.2 0.9 � 0.4 1.7 � 0.6 0.4 � 0.1 0.2 � 0.08Sternum 2.7 � 3.7 0.2 � 0.06 3.3 � 3.3 1.6 � 1.2 12.4 � 10.5 3.6 � 6.2 0.7 � 0.6Ribs 5 � 6.9 0.4 � 0.3 8.7 � 13.3 5.9 � 9 6.2 � 7.8 6.4 � 10.7 2.2 � 4.8Cervical vertebrae 0.2 � 0.06 0.07 � 0.01 0.2 � 0.06 0.5 � 0.2 0.6 � 0.2 0.1 � 0.05 0.1 � 0.03Thoracic vertebrae 6.1 � 7.1 0.3 � 0.2 9.1 � 12.8 6.6 � 11.5 9.7 � 8.6 9 � 11.7 2.5 � 4.3Lumbar vertebrae 17.4 � 0.4 2.6 � 1.9 35.4 � 2.9 20.2 � 15.5 4.9 � 5.9 29.1 � 1.1 14.5 � 4.9Sacrum 15.5 � 4.1 23.6 � 4.2 32.9 � 7.6 1.4 � 0.7 0.7 � 0.2 7.9 � 6.8 10.4 � 6.3Os coxae 7.7 � 6.9 22.2 � 6.7 20.5 � 14.6 1.4 � 0.6 0.6 � 0.2 4.1 � 6.5 3.6 � 5.4Femora UH 1.4 � 1 17.4 � 10.4 3.6 � 4.1 0.9 � 0.5 0.3 � 0.07 0.6 � 0.4 0.5 � 0.4Femora LH 0.1 � 0.07 0.7 � 0.3 0.3 � 0.09 0.5 � 0.3 0.1 � 0.03 0.1 � 0.03 0.1 � 0.05TFP 0.07 � 0.02 0.2 � 0.1 0.1 � 0.05 0.3 � 0.2 0.06 � 0.02 0.06 � 0.02 0.08 � 0.03AFB 0.04 � 0.005 0.06 � 0.02 0.04 � 0.008 0.2 � 0.002 0.02 � 0.005 0.03 � 0.001 0.06 � 0.001Humeri UH 1.1 � 0.7 0.3 � 0.2 1.5 � 0.9 1.5 � 0.4 1.6 � 0.9 1.2 � 0.9 0.3 � 0.3Humeri LH 1.8 � 1.3 0.9 � 0.2 2.5 � 1.3 7.9 � 6.6 1.4 � 0.9 2 � 1.4 0.5 � 0.4Ulnae-radii 1.3 � 0.7 4 � 4.2 1.7 � 0.7 3.1 � 4.2 0.7 � 0.5 1 � 0.8 0.3 � 0.2Wrist-hand 0.5 � 0.3 5.9 � 5.8 0.9 � 0.5 1.2 � 0.3 0.2 � 0.06 0.3 � 0.1 0.1 � 0.04Whole ABM* 3.2 � 5.9 4.2 � 8.7 6.5 � 12.4 2.8 � 7 2 � 4.9 4.5 � 9.2 2.5 � 5.3
Abbreviations: ABM Z active bone marrow; AFB Z ankle and foot bones; FMN Z first malignant neoplasm; HL Z Hodgkinlymphoma; LH Z lower half; LS Z Lymphosarcoma; PTV Z planning target volume; RT Z radiation therapy; STS Z soft tissuesarcoma; TFP Z tibiae fibulae patellae; UH Z upper half.
Veres et al. International Journal of Radiation Oncology � Biology � Physics1220

Sex
M M M M F M M M
4.7 5.1 6.8 7.9 13.6 14.0 15.3 15.9HL Brain LS HL HL Brain Nasopharynx Testis20 55.2 34.8 20 20 55 20.4 201990 1994 1979 1996 1996 1990 1966 1996
Mean � SD dose (Gy) to ABM and mean dose evaluated in each of the 19 subregions0.3 � 0.3 15.8 � 21.8 23.8 � 15.4 0.6 � 0.3 0.3 � 0.2 31 � 15.5 7.4 � 8.1 0.06 � 0.020.7 � 0.2 15.4 � 18.7 15.4 � 13.1 0.9 � 0.2 0.7 � 0.3 26.4 � 19.1 9.5 � 7 0.08 � 0.023.5 � 3.6 0.4 � 0.1 0.7 � 0.3 15.5 � 7.2 7.2 � 7.4 4.4 � 3.8 0.7 � 0.3 0.05 � 0.0111.5 � 7.3 0.6 � 0.1 0.9 � 0.2 19.4 � 3.4 14 � 8.2 8.7 � 6 1.5 � 0.3 0.1 � 0.0718.6 � 2 0.3 � 0.1 0.4 � 0.1 22.3 � 4.8 13.6 � 7.2 1.4 � 3.4 0.5 � 0.3 0.1 � 0.067.1 � 8 0.3 � 0.4 0.5 � 0.5 14.9 � 11.7 10.6 � 8 6.9 � 10.7 0.6 � 1.5 0.05 � 0.035.2 � 6.8 32.8 � 22.9 22.9 � 13 3.8 � 4.3 7.1 � 8.2 35.7 � 11.3 8.6 � 5.8 0.1 � 0.0318 � 5.4 0.4 � 0.5 0.5 � 0.7 23.8 � 8.5 16.6 � 6.4 26.1 � 7.7 0.8 � 1.7 0.09 � 0.050.7 � 0.4 0.09 � 0.02 0.09 � 0.02 35.5 � 7.4 17.5 � 4.8 29.5 � 16.6 0.05 � 0.01 0.04 � 0.010.1 � 0.04 0.06 � 0.003 0.06 � 0.004 20.4 � 3.5 1 � 0.5 30.6 � 11 0.03 � 0.006 0.1 � 0.10.09 � 0.05 0.08 � 0.2 0.06 � 0.01 11.4 � 8.5 0.6 � 0.8 9 � 11.5 0.03 � 0.01 1.5 � 3.80.03 � 0.01 0.09 � 0.3 0.04 � 0.009 6.9 � 7.7 0.1 � 0.04 0.03 � 0.2 0.02 � 0.02 0.09 � 0.070.01 � 0.002 0.04 � 0.004 0.02 � 0.003 0.3 � 0.1 0.06 � 0.006 0.01 � 0.002 0.01 � 0.002 0.03 � 0.010.01 � 0.001 0.03 � 0.002 0.01 � 0.002 0.3 � 0.06 - - - -
0.008 � 0.001 0.03 � 0.001 0.01 � 0.001 - - - - -0.9 � 0.4 0.3 � 0.06 0.6 � 0.2 12.2 � 8.9 1 � 0.7 1.2 � 1.3 0.5 � 0.3 0.06 � 0.010.3 � 0.2 0.1 � 0.04 0.2 � 0.09 1.9 � 1.3 0.6 � 0.3 0.08 � 0.04 0.1 � 0.6 0.07 � 0.0080.08 � 0.05 0.06 � 0.02 0.07 � 0.04 0.6 � 0.4 - - - -0.02 � 0.003 0.09 � 0.2 0.04 � 0.01 - - - - -
3 � 6.5 3.6 � 12.1 4.7 � 11.3 12.7 � 12.6 6.8 � 8.5 16.4 � 16.5 1.3 � 3.9 0.3 � 1.7
Table 2 (Continued)
Sex
M M M F M M M
5.1 6.8 7.9 13.6 14.0 15.3 15.9Brain LS HL HL Brain Nasoph Testis55.2 34.8 20 20 55 20.4 201994 1979 1996 1996 1990 1966 1996
Dose (Gy)D50% [D98%�D2%]
2.8 [0.4�58.7] 34.3 [1.5�43.3] 0.6 [0.2�1.3] 0.2 [0.08�0.8] 27.2 [7.3�60.4] 2.9 [0.7�24.3] 0.07 [0.04�0.1]5.1 [1.5�53.4] 7.5 [2.6�35.9] 0.9 [0.6�1.3] 0.7 [0.3�1.4] 20 [1.6�53.9] 5.8 [0.9�23.6] 0.08 [0.05�0.1]0.4 [0.3�0.6] 0.7 [0.3�1.2] 19.1 [3.2�23.3] 3 [0.5�20.4] 2.9 [0.6�14.1] 0.7 [0.2�1.3] 0.04 [0.03�0.08]0.5 [0.4�0.7] 1 [0.5�1.2] 20.6 [9.7�22] 19 [0.6�21] 8.1 [0.9�23.9] 1.4 [1�2.1] 0.08 [0.04�0.2]0.2 [0.1�0.5] 0.4 [0.2�0.6] 21.6 [9.9�37.9] 17.5 [2.7�20.9] 0.6 [0.3�19.6] 0.4 [0.2�1.2] 0.1 [0.05�0.2]0.2 [0.1�2.1] 0.3 [0.2�3] 12.1 [3.2�43.5] 9.4 [1.2�21] 0.8 [0.1�34.9] 0.2 [0.05�6.7] 0.05 [0.02�0.2]50 [2.7�54.5] 32.2 [3.7�37.2] 2.3 [0.9�17.5] 1.8 [0.5�21] 30 [26.6�55.8] 6 [2.4�21.9] 0.09 [0.07�0.2]0.3 [0.1�2.4] 0.2 [0.1�3.3] 21.5 [2.8�40.7] 20.2 [2.8�21.1] 26 [0.3�46.6] 0.2 [0.06�8.5] 0.06 [0.03�0.2]
0.09 [0.07�0.1] 0.09 [0.06�0.1] 40.4 [22.5�41.2] 19.6 [3.1�20.6] 33.8 [0.5�55.4] 0.05 [0.03�0.08] 0.04 [0.03�0.06]0.06 [0.05�0.07] 0.06 [0.05�0.07] 21.4 [5�22.5] 0.9 [0.3�2.4] 33.9 [0.03�43.3] 0.03 [0.02�0.04] 0.08 [0.03�0.6]0.05 [0.05�0.8] 0.06 [0.04�0.08] 12.9 [0.3�21.3] 0.4 [0.1�2.2] 0.2 [0.02�33.2] 0.03 [0.02�0.05] 0.09 [0.02�15.4]0.05 [0.04�0.9] 0.04 [0.03�0.06] 2.9 [0.2�20.4] 0.1 [0.06�0.2] 0.02 [0.01�0.1] 0.02 [0.01�0.03] 0.07 [0.02�0.3]0.04 [0.03�0.05] 0.02 [0.02�0.03] 0.3 [0.2�0.6] 0.06 [0.04�0.07] 0.01 [0.009�0.02] 0.01 [0.008�0.02] 0.03 [0.01�0.05]0.03 [0.03�0.04] 0.01 [0.01�0.02] 0.3 [0.2�0.4] - - - -0.03 [0.03�0.03] 0.01 [0.01�0.01] - - - - -0.03 [0.2�0.4] 0.5 [0.3�1] 6.8 [2.2�25.5] 0.9 [0.4�3.2] 0.8 [0.1�4.6] 0.5 [0.1�1.1] 0.06 [0.04�0.08]0.1 [0.06�0.2] 0.2 [0.08�0.4] 1.7 [1�2.8] 0.6 [0.2�1.2] 0.07 [0.03�0.2] 0.08 [0.04�0.4] 0.07 [0.03�0.08]0.05 [0.04�0.1] 0.06 [0.03�0.2] 0.5 [0.2�1.6] - - - -0.04 [0.03�0.9] 0.04 [0.03�0.06] - - - - -0.1 [0.03�54] 0.1 [0.01�37.7] 7.3 [0.2�41] 1.2 [0.06�20.9] 12.8 [0.01�53.8] 0.07 [0.01�19.4] 0.06 [0.02�3.7]
Table 3 (Continued)
Volume 90 � Number 5 � 2014 ABM dose-volume metrics 1221

Veres et al. International Journal of Radiation Oncology � Biology � Physics1222
example, from 10 years of age, feet and hand bones arefree of ABM. From the age of 15, the lower parts of theupper and lower limbs also become free of ABM. More-over, a visual comparison of the lower half of the femursshows the decrease in ABM concentration with age in thatarea.
ABM dose distribution
Figure 2 illustrates the inhomogeneity of the dose to theABM for 3 selected patients with different locations of theRT fields. The sampling for the assessment of the ABMdose distribution within each subregion was such that,depending on patient age, for the entire ABM, the totalnumber of dose calculation points in an individual variedfrom 1,190,970 in a 1.1-year-old female patient at RT to4,108,524 in a 15.9-year-old male patient. The number ofdose calculation points per subregion ranged from 9400 inthe clavicle of a 1.1-year-old patient to 759,825 in the oscoxae of a 15.9-year-old patient. Such a sampling appearsto be suitable for DVH computation and for deriving dose-volume metrics for the whole ABM and also for anysubregion.
The lowest average dose to the whole ABM (0.3 Gy) andthe highest average dose (16.4 Gy) were obtained for atestis cancer patient and a brain cancer patient, respectively(Table 2). It can also be noted that, depending on the in-dividual clinical situation, in a comparison of the standarddeviations and the means, the coefficient of variation of thedose for the whole ABM ranged from 1.0 to 5.7.
For the whole ABM, the lowest and highest values forD50% (Table 3) are 0.06 Gy and 12.8 Gy, respectively. Theshapes of the DVH curves (Fig. 3) from a modern treatmentplanning system (TPS) and those derived with our methodare in a reasonable agreement. For the selected clinicalexample, depending on the ABM segment location relativeto beam edge, the discrepancies in the values of D50% rangefrom 1% to 31% for the 6 segments directly involved inirradiation. The largest discrepancy corresponds to thescapulae, located outside the direct beam and receiving thelowest dose. For the 13 remaining segments, the TPS couldnot evaluate the dose because the distances from the beamedge became too large.
Discussion
Owing to the inhomogeneity of the ABM distributionthroughout the whole skeleton, anatomic data for the pa-tient’s whole body is indispensable for the assessment ofdose distributions. Unfortunately, 3D anatomic data were notavailable for the patients treated during the study period. Itappeared relevant, in such a situation, to match each actualpatient to the closest available phantom. Previous work (9)on inherent uncertainties in such a method has shown thatthe mean relative difference between organ volumes in theactual patient and the matched phantom data is
approximately 13% (range, approximately 0%-43%) for or-gans located in the head, 14% (range, 2%-49%) for kidneys,and 31% (range, 2%-69%) for lungs. This uncertainty isfurther compounded when using a straightforward model fordose calculation. Compared with calculations made with amodern TPS, the shapes of the DVHs from both systemswere in reasonable agreement, and the discrepancies in thevalues of D50% ranged from 1% to 31%. A noticeableadvantage of our approach is its capability to provide esti-mated DVHs for the whole 19 ABM compartments, what-ever the distance to the beam edge, whereas calculations areachievable with the TPS for only 6 compartments closest tothe irradiated volume. Indeed, several authors (10, 11) havereported that TPS generally underestimates the out-of-fielddose and that this underestimation worsened for increasingdistances from the field edge.
In the population under study, the RT modalities werevariable and included soft x-rays, gamma radiation fromcobalt machines, and megavoltage x-rays and electronsbeams. The doses were estimated to be between 1,190,970and 4,108,524 points, distributed throughout the skeleton,so that their concentration in every subregion would reflectthe age-specific data on ABM distribution, tabulated by theICRP report 89 (5). However, bone marrow injury is one ofthe most common dose-limiting side effects of conventionalcancer treatments. Acute bone marrow injury occurs shortlyafter chemotherapy and/or radiation therapy due to induc-tion of hematopoietic cell apoptosis. A recent review (12)provides a detailed survey of some of the recent findingsregarding the underlying mechanisms through which radi-ation therapy and chemotherapy cause bone marrow injury.The authors also stated that the mechanisms by whichirradiation and/or chemotherapy induce bone marrowdamage have not yet been clearly defined. Therefore, for apatient who undergoes chemotherapy, the actual distribu-tion of ABM may differ from the population-averaged age-specific values used in the present work. Consequently, 1limitation of the present work is that we could not evaluatethe impact of chemotherapy as a related source of uncer-tainty. The inability to accurately take into account indi-vidual clinical situation and the related variability in ABMdistribution remains a concern.
In the present study, the average dose to the whole ABMis in the range of 0.3 to 16.4 Gy (mean, 4.7 Gy), and in agiven patient, heterogeneity of radiation is such that thecoefficient of variation of the dose is 1.0 to 5.7. These re-sults are, on the whole, consistent with those previouslyreported by several authors. Indeed, Travis et al (13) re-ported that median cumulative dose of radiation to ABMfor low-dose total body irradiation was 5.2 Gy. Blettner andBoice (14) reported that the mean value of the weightedaverage dose to the whole ABM from radiation therapy forcervical cancer was 7.1 Gy. Tucker et al (1) and Allard et al(4) obtained 10 Gy and 2.4 Gy, respectively, in differentchildhood cancer patient populations.
Consensus lies in the fact that among the main sources ofuncertainty in retrospective dose estimates, the completeness

Fig. 3. Intercomparison of dose-volume histograms ob-tained with a modern treatment planning system (solidlines) and using equation 1 (dashed lines). (A) The selectedclinical example, a 4.7 years aged male patient treated forHodgkin lymphoma is shown and (B) the dose-volumehistograms are depicted for the 6 compartments of theABM surrounding the irradiated volume.
Volume 90 � Number 5 � 2014 ABM dose-volume metrics 1223
of RT records is the most critical point (15). For all patientsincluded in the present study, the RT records contain mostcritical information on sizes and locations of irradiation fields,prescribed dose, and patient clinical characteristics. Typicalfigures for the effect of the remaining sources of uncertaintiescan be obtained in recent publications (16, 17). The depth ofthe ABMwas derived from representative anatomies that mayexhibit discrepancies in ABM depth compared to actual pa-tient data. Based on percentage of depth dose data for thepredominant beam qualities involved in our study, in single-beam setting, a 1-cm difference in depth shifts the dose esti-mate by approximately 10%. However, given that most RTregimens involved at least 2 opposed beams on each singletarget volume, the in-field dose distribution is homogenized,and consequently, the effect of discrepancies in ABM depth isconsiderably decreased and may not exceed 3% of the localdose. Because our calculations were based on data from in-water measurements and given that no corrections weremade for tissue inhomogeneity, the presence of dense bonymaterial all around some parts of the ABM was a majorconcern. Indeed, high electron density inhomogeneity inducesa dose enhancement due to backscatter upstream and a dose
disturbance downstream from the inhomogeneity. For corticalbone, the differences between dose to medium and dose towater has been reported to be approximately 10% (18).
Conclusions
For patients with available long-term follow-up data, ourmethod allows reconstructions of whole-body DVHs com-parable to detailed dose calculations that have become astandard in modern CT-based 3D treatment planning.Regarding the need for better accounting of RT dose het-erogeneity, our method allows DVHs to offer new per-spectives for retrospective epidemiological studies ofsubsequent leukemia risk.
References
1. Tucker MA, Meadows AT, Boice JD Jr, et al. Leukemia after therapy
with alkylating agents for childhood cancer. J Natl Cancer Inst 1987;
78:459-464.
2. Hawkins MM, Wilson LM, Stovall MA, et al. Epipodophyllotoxins,
alkylating agents, and radiation and risk of secondary leukemia after
childhood cancer. Br Med J 1992;304:951-958.
3. Haddy N, Le Deley MC, Samand A, et al. Role of radiotherapy and
chemotherapy in the risk of secondary leukaemia after a solid tumour
in childhood. Eur J Cancer 2006;42:2757-2764.
4. Allard A, Haddy N, Le Deley MC, et al. Role of radiation dose in the
risk of secondary leukemia after a solid tumor in childhood treated
between 1980 and 1999. Int J Radiat Oncol Biol Phys 2010;78:1474-
1482.
5. International Commission on Radiological Protection. Basic
Anatomical and Physiological Data For Use in Radiological Protec-
tion: Reference Values. Oxford, UK: ICRP Publication; 2002.
6. Bewley DK, Bradshaw AL, Burns JE, et al. Central axis depth
dose data for use in radiotherapy. A survey of depth doses and related
data measured in water or equivalent media. Br J Radiol 1983;17:
1-147.
7. Francois P, Beurtheret C, Dutreix A. Calculation of the dose delivered
to organs outside the radiation beams. Med Phys 1988;15:879-883.
8. Diallo I, Lamon A, Shamsaldin A, et al. Estimation of the radiation
dose delivered to any point outside the target volume per patient
treated with external beam radiotherapy. Radiother Oncol 1996;38:
269-271.
9. Alziar I, Bonniaud G, Couanet D, et al. Individual radiation therapy
patient whole-body phantoms for peripheral dose evaluations: method
and specific software. Phys Med Biol 2009;54:375-383.
10. Huang JY, Followill DS, Wang XA, et al. Accuracy and sources of
error of out-of field dose calculations by a commercial treatment
planning system for intensity-modulated radiation therapy treatments.
J Appl Clin Med Phys 2013;14:186-197.
11. Howell RM, Scarboro SB, Kry SF, et al. Accuracy of out-of-field dose
calculations by a commercial treatment planning system. Phys Med
Biol 2010;55:6999-7008.
12. Shao L, Wang Y, Chang J, et al. Hematopoietic stem cell senescence
and cancer therapy-induced long-term bone marrow injury. Transl
Cancer Res 2013;2:397-411.
13. Travis LB, Weeks J, Curtis RE, et al. Leukemia following low-dose
total body irradiation and chemotherapy for non-Hodgkin’s lym-
phoma. J Clin Oncol 1996;14:565-571.
14. Blettner M, Boice JD Jr. Radiation dose and leukaemia risk: general
relative risk techniques for dose-response models in a matched case-
control study. Stat Med 1991;10:1511-1526.

Veres et al. International Journal of Radiation Oncology � Biology � Physics1224
15. Stovall M, Weathers R, Kasper C, et al. Dose reconstruction for
therapeutic and diagnostic radiation exposures: use in epidemiological
studies. Radiat Res 2006;166:141-157.
16. Ng A, Brock KK, Sharpe MB, et al. Individualized 3D reconstruction
of normal tissue dose for patients with long-term follow-up: a step
toward understanding dose risk for late toxicity. Int J Radiat Oncol
Biol Phys 2012;84:e557-e563.
17. Lamart S, Stovall M, Simon SL, et al. Radiation dose to the esophagus
from breast cancer radiation therapy, 1943-1996: an international
population-based study of 414 patients. Int J Radiat Oncol Biol Phys
2013;86:694-701.
18. Siebers JV, Keall PJ, Nahum AE, et al. Converting absorbed dose to
medium to absorbed dose to water for Monte Carlo based photon beam
dose calculations. Phys Med Biol 2000;45:983-995.