-
7/28/2019 Revascularization of Immature Permanent Incisors After
Severe Extrusive Luxation Injury
1/7
Revascularization of Immature Permanent Incisors after
Severe Extrusive Luxation Injury
Zafer C. Cehreli, DDS, PhD; Sezgi Sara, DDS; Burak Aksoy,
DDS
Posted on January 19, 2012
Tags:childrenendodonticsinjurytreatment
Cite this as: J Can Dent Assoc 2012;78:c4
Abstract
Pulp necrosis is an uncommon sequel to extrusive luxation in
immature teeth with incomplete
apical closure. In this report, we describe the management of
severely extruded immaturemaxillary incisors and the outcome of
revascularization to treat subsequent pulp necrosis. An8.5-year-old
boy with severe dentoalveolar trauma to the anterior maxillary
region as a result of a
fall was provided emergency treatment consisting of reduction of
the dislodged labial cortical
bone and repositioning of the central incisors, which had
suffered extrusive luxation. When he
presented with spontaneous pain involving the traumatized
incisors a week later, the teeth weretreated via a
revascularization protocol using sodium hypochlorite irrigation
followed by 3 weeks
of intracanal calcium hydroxide, then a coronal seal of mineral
trioxide aggregate and resin
composite. Complete periradicular healing was observed after 3
months, followed by progressivethickening of the root walls and
apical closure. Follow-up observations confirmed the efficacy
of
the regenerative treatment as a viable alternative to
conventional apexification in endodontically
involved, traumatized immature teeth.
Introduction
Extrusion is an injury characterized by partial axial
displacement of a tooth.1
Clinically, the
affected tooth appears elongated, is usually displaced in the
palatal direction and demonstratesexcessive mobility.
2,3Radiographically, extruded teeth appear to have an increased
periodontal
ligament space. Based on severance of the periodontal ligament
that has not yet been exposed to
desiccation or disarticulation of the tooth from the blood
supply, Andreasen4
described extrusive
luxation as partial avulsion. According to Lee and
colleagues,3
this term is useful in terms oftreatment approach, as the pulpal
outcome of severe extrusion may be comparable to that of a
replanted tooth.
The stage of apical development is a key factor in pulp healing
after extrusive luxation.3,5,6
In
teeth with open apices, the pulp has greater potential for
healing, commonly followed by pulp
canal obliteration; in patients with closed apices, the
likelihood of pulp revascularization is low,usually leading to pulp
necrosis.
1,3,5,6Once pulp necrosis is diagnosed, endodontic therapy
should
http://www.jcda.ca/Article/tagged-with/tag/en_childrenhttp://www.jcda.ca/Article/tagged-with/tag/en_childrenhttp://www.jcda.ca/Article/tagged-with/tag/en_endodonticshttp://www.jcda.ca/Article/tagged-with/tag/en_endodonticshttp://www.jcda.ca/Article/tagged-with/tag/en_injuryhttp://www.jcda.ca/Article/tagged-with/tag/en_injuryhttp://www.jcda.ca/Article/tagged-with/tag/en_treatmenthttp://www.jcda.ca/Article/tagged-with/tag/en_treatmenthttp://www.jcda.ca/Article/tagged-with/tag/en_treatmenthttp://www.jcda.ca/Article/tagged-with/tag/en_treatmenthttp://www.jcda.ca/Article/tagged-with/tag/en_injuryhttp://www.jcda.ca/Article/tagged-with/tag/en_endodonticshttp://www.jcda.ca/Article/tagged-with/tag/en_children
-
7/28/2019 Revascularization of Immature Permanent Incisors After
Severe Extrusive Luxation Injury
2/7
be initiated to eliminate infection and facilitate healing and
retention of the tooth.3
If root
development is incomplete, apexification is indicated to induce
formation of a calcific barrier at
the apex. However, this technique has several disadvantages,
including up to 24 months oftreatment, which often requires
multiple visits and renewal of the intracanal dressing.
7,8Apical
closure is unpredictable,9
and the tooth is susceptible to root fracture after prolonged
exposure to
calcium hydroxide (Ca(OH)2).
10,11
Because of these concerns, the traditional
Ca(OH)2-basedapexification procedure has been modified by the
introduction of an artificial apical barrier usingmineral trioxide
aggregate (MTA).
1215Obturation of open apices with MTA plugs significantly
reduces treatment time and results in favourable healing of
periradicular tissues.12,14,16,17
However, MTA plugs cannot stimulate physiologic apical closure
and thickening of radiculardentin, leaving the tooths structural
integrity compromised.
18,19
Revascularization is an emerging regenerative endodontic
treatment approach that aims to allowcontinuation of root
development and tissue regeneration in immature necrotic teeth.
20,21The
root canal is disinfected with sodium hypochlorite, followed by
placement of an intracanal
medicament, such as calcium hydroxide or a combination of
ciprofloxacin, metronidazole and
minocycline.
22
After disinfection, the antibiotic paste is removed and apical
bleeding is inducedto form a blood clot below the coronal level.
The root canal orifice is then sealed with MTA, and
the tooth crown is restored permanently.
This protocol has been successful, as evidenced by increased
root length, thickening of the root
walls and apical closure of varying degrees.2328
In the following case, we describe the
management of severely extruded immature maxillary incisors and
the outcome ofrevascularization in the treatment of pulp necrosis
subsequent to the trauma.
Case Report
A healthy 8.5-year-old boy was admitted to the pediatric
dentistry clinic 6 hours after a fall in hisschoolyard. Reportedly,
an emergency examination had been carried out by a hospital
pediatrician, who found the patient to be free of neurologic and
general physical symptoms andreferred him for management of
dentoalveolar trauma.
The child was unable to close his mouth or speak properly
because of severely displaced
maxillary central incisors, evident on extraoral view (Fig. 1a).
Intraoral examination showed
severe extrusive luxation of the incisors along with a fractured
labial cortical bone (Fig. 1b). The
teeth were excessively mobile and the maxillary right central
incisor showed pronounceddisplacement in the palatal direction. The
palatal segment of the alveolar bone was slightly
mobile on palpation, but did not appear to be dislodged. The
neighbouring lateral incisors
displayed normal mobility. The attached gingiva distal to the
right lateral incisor was lacerated(Fig. 1b). A periapical
radiograph revealed increased apical periodontal ligament space in
bothincisors, along with palatal displacement of the right central
incisor (Fig. 1c). In both teeth, root
development was incomplete, and wide root canals and open apices
were evident.
Following removal of the blood clot with copious saline
irrigation (Fig. 1d), the dislodged buccal
cortical bone was gently repositioned. The extruded incisors
were then meticulously repositionedby conventional digital
maneuver, with no sign of resistance caused by a clot blockage. A
semi-
-
7/28/2019 Revascularization of Immature Permanent Incisors After
Severe Extrusive Luxation Injury
3/7
rigid splint made of 0.9-mm monofilament fishing line was bonded
to the lateral and central
incisors using acid-etch composite resin (Fig. 1e). After
suturing of soft tissue lacerations, a
radiograph was taken to confirm correct reduction and
repositioning (Fig. 1f). The patient wasprescribed amoxicillin and
ibuprofen, and scheduled for a follow-up visit.
-
7/28/2019 Revascularization of Immature Permanent Incisors After
Severe Extrusive Luxation Injury
4/7
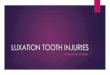
Figure 1: Initial examination of patient. a) Extraoral view,
demonstrating the extent of jaw
closure; b) intraoral and c) radiographic views of extruded
incisors; d) intraoral view following
removal of the blood clot with saline irrigation; e) view of the
incisors after reduction, splintingand suturing; f) radiographic
view of the incisors after repositioning, revealing the wide
root
canals and open apices.
A week later, the patient returned with severe spontaneous pain
involving the traumatized
incisors. The teeth were tender on palpation, and radiographic
examination revealed periapical
radiolucency. Because of the patients incomplete root
development and wide open apices,traditional endodontic therapy
using Ca(OH)2-based apexification or placement of an apical
barrier with MTA would seriously compromise the structural
integrity of the tooth. Therefore,regenerative endodontic treatment
of the affected incisors was considered. After comprehensive
discussion of the risks and possible outcomes of this treatment
and the treatment plan in case offailure, the consent of the
patient and parents was obtained and treatment was initiated at
the
same visit.
After anesthesia, the pulp chambers were accessed. Isolation was
achieved using cotton rolls and
gauze, as a rubber dam could not be placed in the presence of
the trauma splint. Each root canalorifice was gently irrigated with
10 mL of 2.5% sodium hypochlorite (NaOCl) without
instrumentation. Ca(OH)2 powder (Merck, Darmstadt, Germany) was
mixed with sterile saline in
a 3:1 ratio to produce a thick, homogeneous paste. The mixture
was placed in the pulp chamber
using a plastic carrier and loosely packed into the coronal
portion of the root canals with moistcotton pellets. Finally, the
access cavity was sealed with Cavit (3M ESPE, Seefeld, Germany)
(Fig. 2a). A week later, the patient was recalled for removal of
the trauma splint and, 3 weeks
later, for evaluation of the intracanal medication.
After 3 weeks, both teeth were asymptomatic. They were
anesthetized using 2% mepivacaine
(Citanest, AstraZeneca, UK) without a vasoconstrictor, isolated
with a rubber dam and
reaccessed. The Ca(OH)2 paste was removed with copious 2.5%
NaOCl irrigation, and the root
-
7/28/2019 Revascularization of Immature Permanent Incisors After
Severe Extrusive Luxation Injury
5/7
canals received a final irrigation with 10 mL sterile saline and
were dried. Apical bleeding was
induced by gentle irritation using size 15 K-files. After a
blood clot had formed, MTA (Dentsply
Tulsa Dental, Tulsa, OK) was prepared according to the
manufacturers instructions and gentlyadapted over the blood clot. A
wet cotton pellet was placed over the MTA, and the access
cavity
was temporarily restored with conventional glass ionomer cement.
Final resin composite
restorations were placed 1 week later (Fig. 2b), and the patient
was scheduled for regular follow-up visits.
The teeth remained asymptomatic during the 18-month evaluation
period. At 3 months, the teethshowed complete periapical healing
and, thereafter, root development and closure of the apices
continued (Fig. 2c).
To quantify the increase in root width and length, the
radiographs obtained immediately after
treatment and 18 months later were converted to 32-bit TIFF
files using ImageJ analysis program
(v.1.44p, National Institutes of Health, Bethesda, MD). The
TurboReg plug-in (Biomedical
Imaging Group, Swiss Federal Institute of Technology, Lausanne,
Switzerland)29
was used to
mathematically align the two images as described by Bose and
colleagues.
28
Because the 18-month radiograph showed less distortion, it was
used as the source image, while the
postoperative radiograph, which required correction, was used as
the target image.28
Followingalignment of the images using TurboReg (Fig. 2d), a
scale was added, and root lengths and root
wall thicknesses were measured.28
This revealed an increase of 18.16% and 17.14% in the root
lengths and 40.54% and 75.64% in the root widths of the right
and left incisors, respectively.
-
7/28/2019 Revascularization of Immature Permanent Incisors After
Severe Extrusive Luxation Injury
6/7
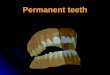
Figure 2:a) Radiographic view of the teeth after intracanal
application of calcium hydroxide
(Ca(OH)2) paste; periradicular radiolucencies are evident in
both roots. b) Periapical radiograph
showing the coronal mineral trioxide aggregate (MTA) barrier and
final composite restoration. c)Radiographic view at 18 months
follow-up, demonstrating narrowing of root canal in the apical
third and thickening of the lateral walls. A normal bony
architecture at the periradicular region is
evident. d) Image b after correction (alignment) with ImageJ and
the TurboReg plugin using c asthe source image for mathematical
correction.
At 12 months, a positive response to a cold test was first
observed, but the response of both teethto electric pulp testing
(EPT) was inconsistent. At 18 months, response to cold testing was
still
positive and both teeth showed a consistent, delayed response to
EPT. The patient has beenattending regular follow-up appointments;
his teeth have remained asymptomatic, with normal
mobility and gingiva in good condition.
Discussion
Pulp necrosis is a relatively uncommon sequel to extrusive
luxation in immature teeth with wide-
open apices,5
because of the high likelihood of revascularization and
subsequent root
development in these teeth. However, the risk increases
significantly in the case of severeextrusion
3and, if pulp necrosis occurs, it is likely to be an early
event.
3,5,30
Regenerative endodontic techniques may enhance continued root
development21
and, therefore,offer an alternative approach to the management
of traumatized immature permanent teeth with
pulp necrosis and periradicular infection.24,31
A growing body of evidence supports the
possibility of residual viable pulpal tissue in the wide root
canal or apical region of necroticimmature teeth, which may survive
the infection and allow continued apical development.
25,32,33
Stem cells from the apical papilla may also survive infection,
because of their proximity to the
periapical tissues.26,32,33
Following proper endodontic disinfection, these cells may
differentiate
under the influence of surviving epithelial cells of Hertwigs
root sheath and initiate continued
-
7/28/2019 Revascularization of Immature Permanent Incisors After
Severe Extrusive Luxation Injury
7/7
root development.26,33
Once the regenerative process is induced, the presence of a wide
apical
foramen and root canal enhances the ingrowth of small blood
vessels and regenerated tissues.26
In the revascularization protocol, infected root canals should
be treated as conservatively as
possible.20,25,31
This is best achieved by copious irrigation with 2.5%5.25% NaOCl
and no
instrumentation. At the same appointment, intracanal medication
is put in place to disinfect theroot canal and left for 34 weeks.
Previous reports have demonstrated the effectiveness of a
triple antibiotic paste consisting of metronidazole,
ciprofloxacin and minocycline in the
disinfection of infected root canals,22,34
including those of immature teeth with apicalperiodontitis.
25,35The main disadvantage of this paste is minocycline-induced
crown
discoloration,36,37
which might be reduced, but not prevented by prior sealing of
the coronal
dentin with bonding agents.37
Ca(OH)2 has also been used successfully for disinfection of root
canals before
revascularization.23,26,28
Bose and colleagues28
showed that placement of Ca(OH)2 in the coronal
half of the root canal contributed to a significant increase in
root length and wall thickness,
comparable to that achieved with the triple antibiotic
paste.
In the current case, the teeth were asymptomatic after treatment
with Ca(OH)2: continuing rootdevelopment was observed, symptoms of
infection were absent and no crown discoloration
occurred. In a retrospective study, Chueh and colleagues26
showed a high rate of progressive
calcification of the root canal space in teeth medicated with
Ca(OH)2, suggesting that rootdevelopment induced by regenerative
endodontic treatment may not follow a natural pattern.
Thus, despite the absence of root canal obliteration in the
current case, progressive calcification
may occur in the longer run.
Previous studies of the revascularization procedure in
traumatized, immature incisors have
reported a lack of sensitivity to both cold testing and EPT.
24,30,38
In the absence of histologic datafrom humans, the reasons for
both positive and negative responses to thermal and
electricalstimuli should be interpreted with caution, as lack of
response could merely be a result of the
thickness of the MTA and restorative materials preventing
stimulation of vital tissues within the
root canal.39
The use of a collagen matrix to control the thickness of the
coronal MTA barrier30
and placement of the MTA barrier close to the cementoenamel
level
39might increase the
likelihood of a positive response, provided that the regenerated
tissue in the root canal contains
nerves. Based on these considerations, the inconsistent
responses of the extruded incisors to EPTin contrast to cold
testing might have resulted from the thick MTA barriers, which
occupied
almost half the length of the root canal.
The favourable short-term results in this case of severe
extrusive luxation show that regenerative
endodontic treatment of pulpally involved traumatized immature
teeth is a viable alternative to
apexification or artificial apical barrier techniques. Although
the nature of the regenerated tissue
within the root canal is yet to be elucidated in humans, it is
evident that this technique can allowfor continued root development
and apical closure. More clinical data is required to confirm
the
predictability of this approach.