Embed Size (px)
Citation preview

Revenue Management for Risk-Adjusted Health Plans: Advanced Strategies
Free Webinar Series: May 5, 2016
1
Richard Lieberman Richard Bernstein, MD, FACP
Chief Data Scientist
Mile High Healthcare Analytics

TODAY’S AGENDA
• 30-Days in 30 Seconds
• Dr. Bernstein will provide insights about digital detailing for revenue management
• Richard Lieberman will present a brief overview of some legal developments related to risk adjustment compliance
• We will then present some findings from a different way of looking at retrospective medical record reviews
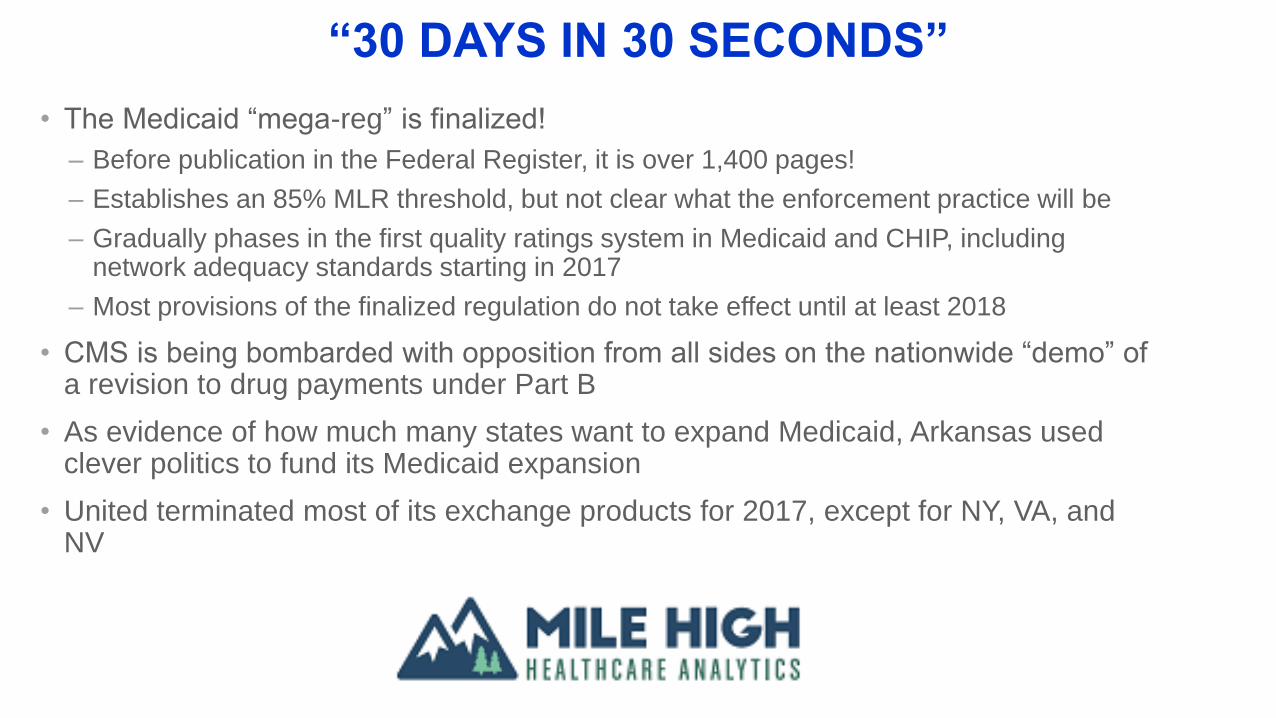
“30 DAYS IN 30 SECONDS”
• The Medicaid “mega-reg” is finalized!
– Before publication in the Federal Register, it is over 1,400 pages!
– Establishes an 85% MLR threshold, but not clear what the enforcement practice will be
– Gradually phases in the first quality ratings system in Medicaid and CHIP, including network adequacy standards starting in 2017
– Most provisions of the finalized regulation do not take effect until at least 2018
• CMS is being bombarded with opposition from all sides on the nationwide “demo” of a revision to drug payments under Part B
• As evidence of how much many states want to expand Medicaid, Arkansas used clever politics to fund its Medicaid expansion
• United terminated most of its exchange products for 2017, except for NY, VA, and NV

“30 DAYS IN 30 SECONDS”
• CMS on May 2nd published the performance measures for determining Medicare
physician pay under the new system that the agency is designing
• CMS is scaling back the federal exchange market's quality star ratings initiative from a
full-fledged national program to a five-state pilot for the 2017 plan year
– Quality star ratings for qualified health plans will be publicly reported nationwide for the first
time in 2018, a year later than was originally expected
Richard H Bernstein, MD, FACP
5/5/2016
Digital Detailing:A Scalable Way to Improve Population
Health, RAF Scores, and Quality
The First Steps for Population Health Management
1. Know the population by diagnosis, risk level, and gaps in care
(Easy, with sound data analytics)
2. Get doctors to list all the diagnoses
(HARD: Are they educable?)
4 WAYS TO OPTIMIZE CAPTURING VALID DIAGNOSES
7
1.Retrospective Assessments
2.Prospective Assessments
3.Multiphasic Testing Events &Targeted Visits
4.Concurrent Assessments: Peer Detailing & Digital Detailing
1. RETROSPECTIVE ASSESSMENTS
8
1. Use data analytics to target chart retrieval.
2. Capture un/under- or mis-coded historical diagnoses. Report unsupported diagnoses (RADV risk).
3. Use coding experts to assure documentation meets Correct Coding criteria.
4. Limitation: Often no feedback to providers; documentation errors may be repeated.
2a. PROSPECTIVE ASSESSMENTS
9
1. Use data analytics to target visits (RA, Gaps) in the office, at home, or alternative sites, e.g., retail settings
2. Perform comprehensive health assessments (including health risk assessments)
3. Capture un- and under-coded diagnoses; PoC testing
4. Avoid RADV risk from over-aggressive coding
2b. PROSPECTIVE ASSESSMENTS
10
To satisfy CMS, results must complete the Circle of Care:• Generate recommended care plans• Information shared with care managers, PCP, and
member• Show that new HCCs result in new or modified care
plan
3. CAPTURE DIAGNOSES THROUGH TARGETED SCREENING
11
1. Use data analytics to implement targeted lab studies and procedures in the home, in the office, or at health fairs.
2. Examples: Screening for peripheral artery disease, osteoporosis, diabetic retinopathy, etc.
3. Document diagnoses (when qualified provider involved); close quality gaps
4a. CONCURRENT ASSESSMENTS:Peer-to-Peer (P2P) Detailing
12
1. Use data analytics & chart sampling: identify most common under- and mis-coded HCCs
2. Develop peer educational program to correct coding behavior by clinicians and billing staff
3. Track improvement; provide feedback based on small chart sample
4. Limitation: scalability, one-and-done, asynchronous
4b. CONCURRENT ASSESSMENTS:Digital Detailing
13
1. Use data analytics to push EHR alerts at the time of member visits (ideal synchronous learning)
2. Incorporate chart review, “peer champions,” & incentives based on response to alerts (accept & reject)
3. Educate doctors re: 100% of un-, under-, and mis-coded diagnoses
14
Support:
1. Risk Adjustment recommendations for chart documentation and provide…
2. Defense against RADV audit challenges3. Ongoing education to providers by a process that fits
their workflow (point of care EHR alerts)
4. Managed Care Plans, QHP, ACOs and Medical Groups with appropriate risk-adjusted capitation revenue
4 DIGITAL DETAILING GOALS
15
1. Clinical algorithms filter data to identify members with HCC scoring opportunities and quality gaps
Data sources:- Claims - Eligibility- Rx - CMS files (MMR, MOR)- Lab - RAPS/EDS
2. Risk Adjustment specialists confirm clinical algorithms with evidence from the chart to generate alerts
DATA ANALYTICS
16
Excised malignant neoplasms may only be documented as active if further treatment is indicated.
Dr. Smith (Oncology) documented Breast Cancer on 12/15/2015, noting: “Continue Arimidex.” If patient still on Arimidex, consider documenting this diagnosis, rather than “history of cancer.”
Recommend: Malignant Neoplasm of Female Breast (C50.919)
Reference to RAF (risk adjustment factor) is NOT included in alerts, e.g., “History of” cancer codes RAF = 0.000
HCC 12 - Breast, Prostate and other cancers and tumors RAF = 0.154
DIGITAL DETAILING ALERT EXAMPLE:Issue: “History of” vs. Active Cancer
17
Besides HCC-related EMR alerts, Digital Detailing can create alerts to providers about:
•Quality Gaps in Care, e.g., mammography, retinal eye exams
•RADV Risk, e.g., “rheumatoid arthritis” with no serologic, imaging, Rx, or other evidence of RA
OTHER DIGITAL DETAILING ALERTS:Issues: Quality Gaps and RADV
Incomplete Diagnosis Accurate, Supported Diagnosis
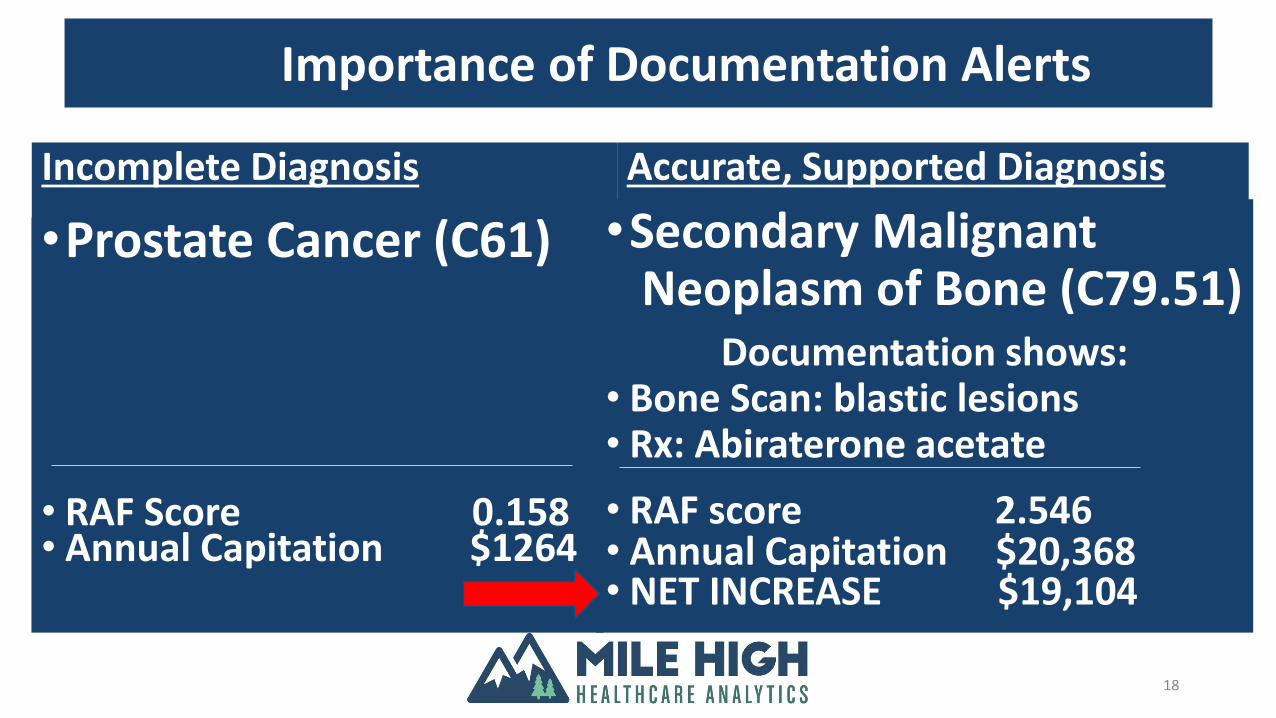
•Prostate Cancer (C61)
• RAF Score 0.158• Annual Capitation $1264
•Secondary Malignant Neoplasm of Bone (C79.51)
Documentation shows: • Bone Scan: blastic lesions • Rx: Abiraterone acetate
• RAF score 2.546• Annual Capitation $20,368• NET INCREASE $19,104
18
Importance of Documentation Alerts
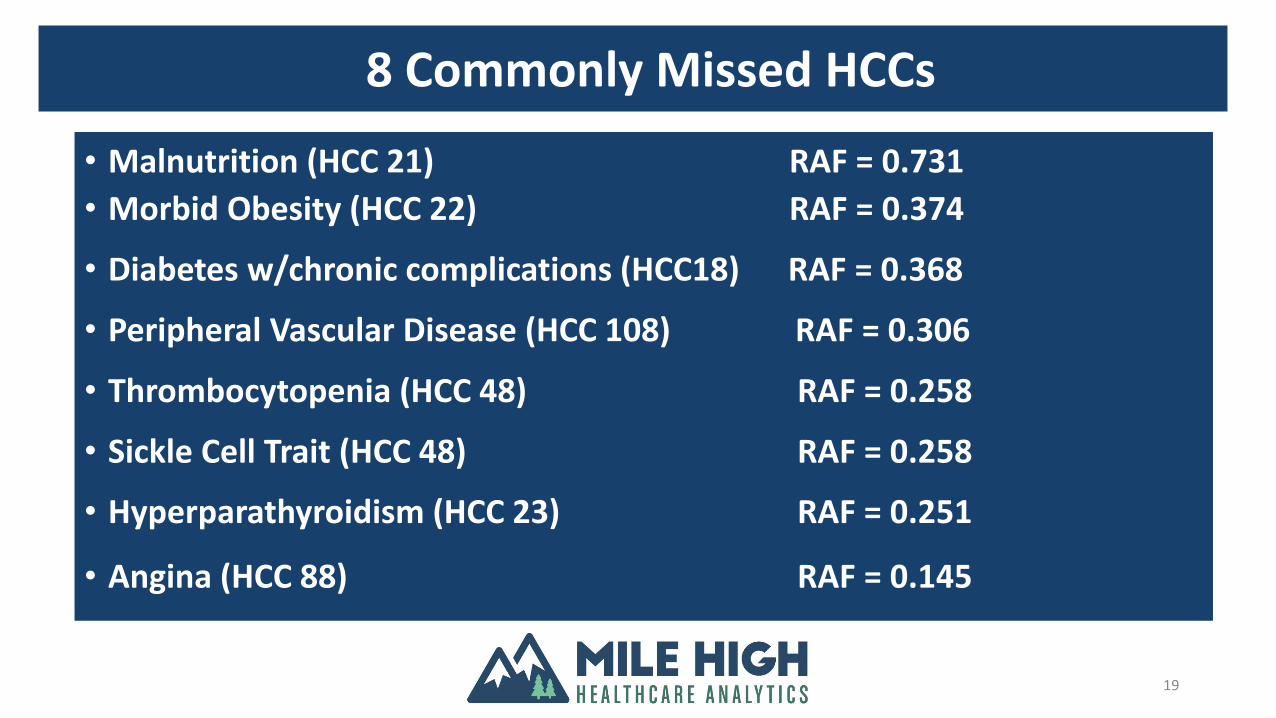
19
• Malnutrition (HCC 21) RAF = 0.731
• Morbid Obesity (HCC 22) RAF = 0.374
• Diabetes w/chronic complications (HCC18) RAF = 0.368
• Peripheral Vascular Disease (HCC 108) RAF = 0.306
• Thrombocytopenia (HCC 48) RAF = 0.258
• Sickle Cell Trait (HCC 48) RAF = 0.258
• Hyperparathyroidism (HCC 23) RAF = 0.251
• Angina (HCC 88) RAF = 0.145
8 Commonly Missed HCCs
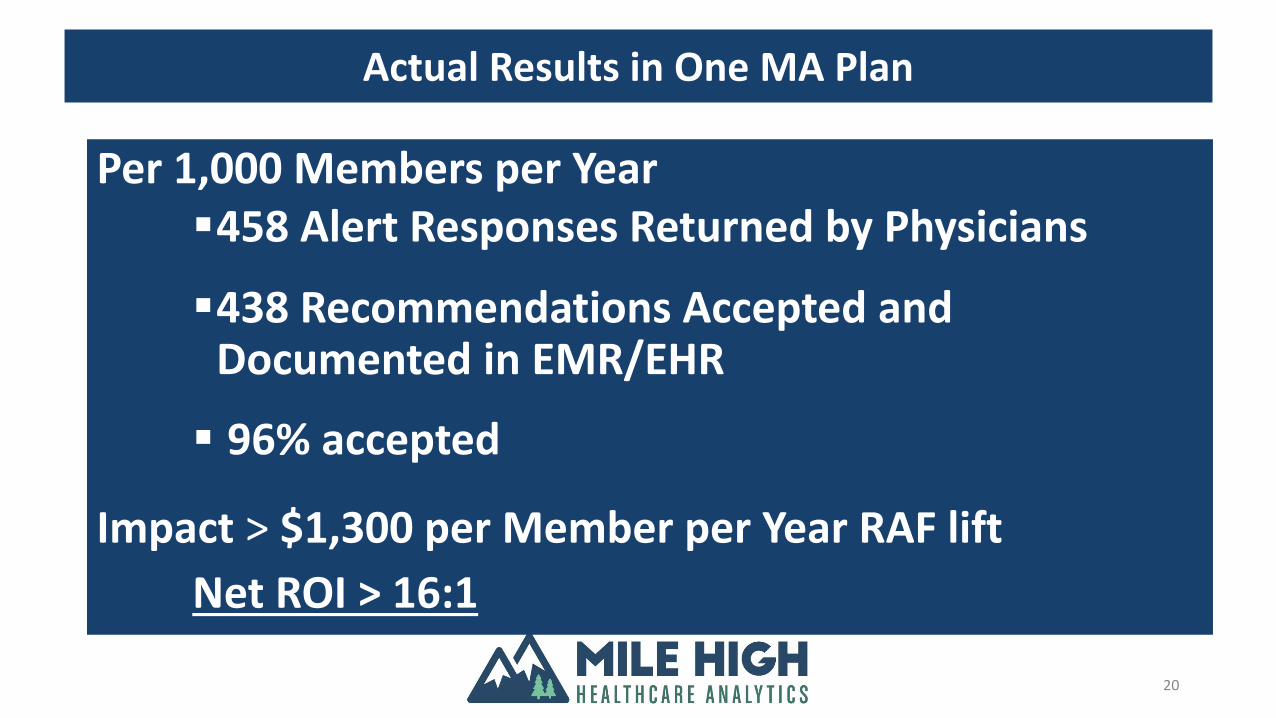
20
Per 1,000 Members per Year458 Alert Responses Returned by Physicians
438 Recommendations Accepted and Documented in EMR/EHR
96% accepted
Impact > $1,300 per Member per Year RAF lift
Net ROI > 16:1
Actual Results in One MA Plan
Improving Provider Documentation is Possible!
21
Digital Detailing Alerts:1. Target Under-,Mis-,Uncoded Dxs2. Change MD coding practices to better support all
valid diagnoses3. Form a foundation for population health
management
(And, yes, there is evidence that doctors are educable)
Richard Lieberman
An Expanding Paradigm Governing Revenue Management
ISSUES TO CONSIDER FOR 2016 AND BEYOND
• Accuracy of data transmitted by providers:
• CMS decided in 2014 not to finalize a proposed requirement
that any chart reviews conducted by an MA organization be
designed to find not just additional diagnoses to submit to
CMS but also unsupported diagnoses that had previously
been submitted to CMS—a “look both ways” requirement
• However, this is not the position that is being pursued by the
Justice Department
• The new risk adjustment model is going to put downward
pressure on risk scores for many plans
• EDPS is no longer just a compliance activity!
THE GOVERNMENT’S POSITION APPEARS TO BE EVOLVING….
• In a brief filed by the United States as Amicus Curiae in the US Circuit Court of Appeals for
the 9th Circuit on April 18, 2016 (Case Number No. 13-56746), the Justice Department
said:
• CMS has made clear that MA organizations must exercise “due diligence” to ensure the
accuracy of submitted data. The certification required under 42 C.F.R. § 422.504(l) is thus best
understood to carry with it a representation that a plan has acted with reasonable diligence and
implemented measures to find errors. If a plan has not exercised such diligence—especially
where it has implemented record-review procedures specifically designed not to reveal
unsupported diagnosis codes—the plan’s certification under § 422.504(l) is “false or fraudulent”
under 31 U.S.C. § 3729(a)(1)(A) & (B).
• “Even apart from the regulatory duty to exercise “due diligence,” if an MA organization knows
that it has submitted unsupported diagnoses, see 31 U.S.C. § 3729(b)(1), its certification that
the information it has submitted is “accurate, complete, and truthful” is false or fraudulent under
the False Claims Act”
THE ACA PUT TEETH INTO THE FALSE CLAIMS ACT
• The False Claims Act is the government’s primary tool
to combat fraud and recover losses due to fraud
• The ACA created a 60-day window from when a
provider detects an overpayment to when the
government must be reimbursed for the overpayment
• In the case of risk adjustment “overpayments” this 60-
day window begins after the final reconciliation data
sweep (January 31st of the year after the payment year)
THE INDUSTRY DOESN’T NECESSARY AGREE!
• In January 2016, United Health Group filed a complaint in the US District Court for the
District of Columbia (United Health Group v. Burwell and CMS, Case number 1:16-cv-
00157). The plaintiff’s position is:
• Seeking judicial review of a regulation promulgated by CMS that governs the reporting and
returning of “overpayments” from CMS to insurance plans in the Medicare Advantage Program
• The regulation should be vacated because it constitutes an unlawful and unreasonable
interpretation of the statute. Congress mandated that plans return to CMS any overpayments
that a plan has “identified”—an actual knowledge standard. The regulation, by contrast, CMS
required plans to instead return any overpayment that the plan not only has identified, but also
any overpayment that the plan “should have identified through the exercise of reasonable
diligence”—a negligence standard.
• CMS’s interpretation violates the plain meaning of the statute, or at a minimum is an
unreasonable interpretation of any statutory ambiguity, and is therefore contrary to law.
SO WHAT IS THE POINT OF ALL OF THIS LEGAL GOBBLEDYGOOK?
• Risk adjustment compliance is likely to change just as the new models and data collection methods are putting additional downward pressure on risk scores and premiums
• Risk-adjusted plans are entitled to be paid accurate premiums that fully account for the underlying morbidity of the members they enroll
• But, plans must ensure that submitted data is accurate, not that it solely maximizes the plan’s risk score and premium
MEDICAL RECORD SUBSTANTIATION OF RISK SCORES IS VITAL
• Receiving accurate Medicare-Advantage premiums requires
comprehensive medical record documentation created at the point-of-
care
• Use of encounter data in risk score calculations increases the need to
link diagnosis coding to treatment
• 10 percent of risk score in 2016 is driven by encounter data; 25 percent in
2017
• RADV audits are used to uncover inadequate linkages between claims
submission coding and underlying clinical documentation
• CMS is moving toward the creation of MA Part C RACs to assume the
responsibility for RADV audits
ROLE OF CHART REVIEW PROJECT COMPONENT
• Mile High Healthcare Analytics (MHHA) engaged a vendor to review a convenience
sample of charts for a group of PCPs
• For each instance where the medical record offered evidence of an HCC, the quality of
the medical record documentation was categorized as follows:
– Correctly documented condition
– Incompletely/inaccurately documented condition – opportunity to improve documentation and
ensure code stand up to audits
– Suspect identified that was not documented by the provider; from labs, chart info, etc. that
needs to be confirmed by provider in next face to face visit – these are big opportunities for
risk score improvement and appropriate care management/condition identification to improve
health status
29
MEDICAL RECORDS ONLY TELL PART OF THE STORY
• In a shared-risk contract, facility claims (both inpatient and outpatient) supply a
significant number of HCCs to augment the overall person-based risk score
• This project linked diagnoses from facility claims to the data abstracted the PCP charts
• MHHA calculated a disease-based risk score, summing only the HCC weights for each
member’s chart abstracted (demographic weights excluded)
– This approach facilitates PCP-to-PCP comparisons
30
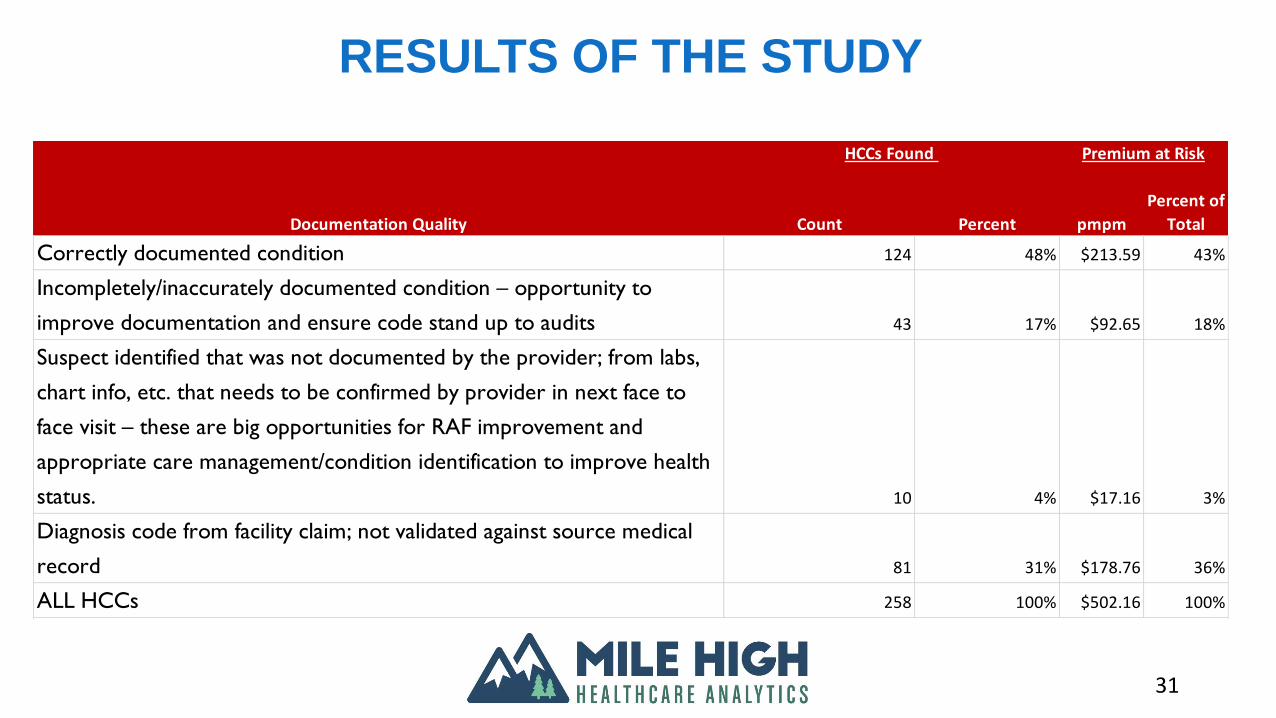
RESULTS OF THE STUDY
31
Count Percent pmpm
Percent of
Total
Correctly documented condition 124 48% $213.59 43%
Incompletely/inaccurately documented condition – opportunity to
improve documentation and ensure code stand up to audits 43 17% $92.65 18%
Suspect identified that was not documented by the provider; from labs,
chart info, etc. that needs to be confirmed by provider in next face to
face visit – these are big opportunities for RAF improvement and
appropriate care management/condition identification to improve health
status. 10 4% $17.16 3%
Diagnosis code from facility claim; not validated against source medical
record 81 31% $178.76 36%
ALL HCCs 258 100% $502.16 100%
HCCs Found
Documentation Quality
Premium at Risk
OMINOUS SIGNS FROM AGGREGATE FINDINGS• While 79 percent of the HCC-specific risk score is substantiated by medical
records (48% from PCP charts), there remains 17 percent of the risk score that is at risk in the event of a RADV audit
– This at-risk amount translates to over $92 pmpm based on 2013 Part A/B standardized premium payments in the county where the IPA operates
• An additional $17.16 pmpm could be added to the MA premium payment if medical records captured all of the HCCs that were evident from lab tests, medication records, or other chart components not eligible as sources for HCC substantiation
• If the results of these 106 members are generalizable to the entire enrollment, there is a premium pickup opportunity of almost $4 million
– But in excess of $21 million of premium revenue is at risk from suboptimal medical record documentation
32
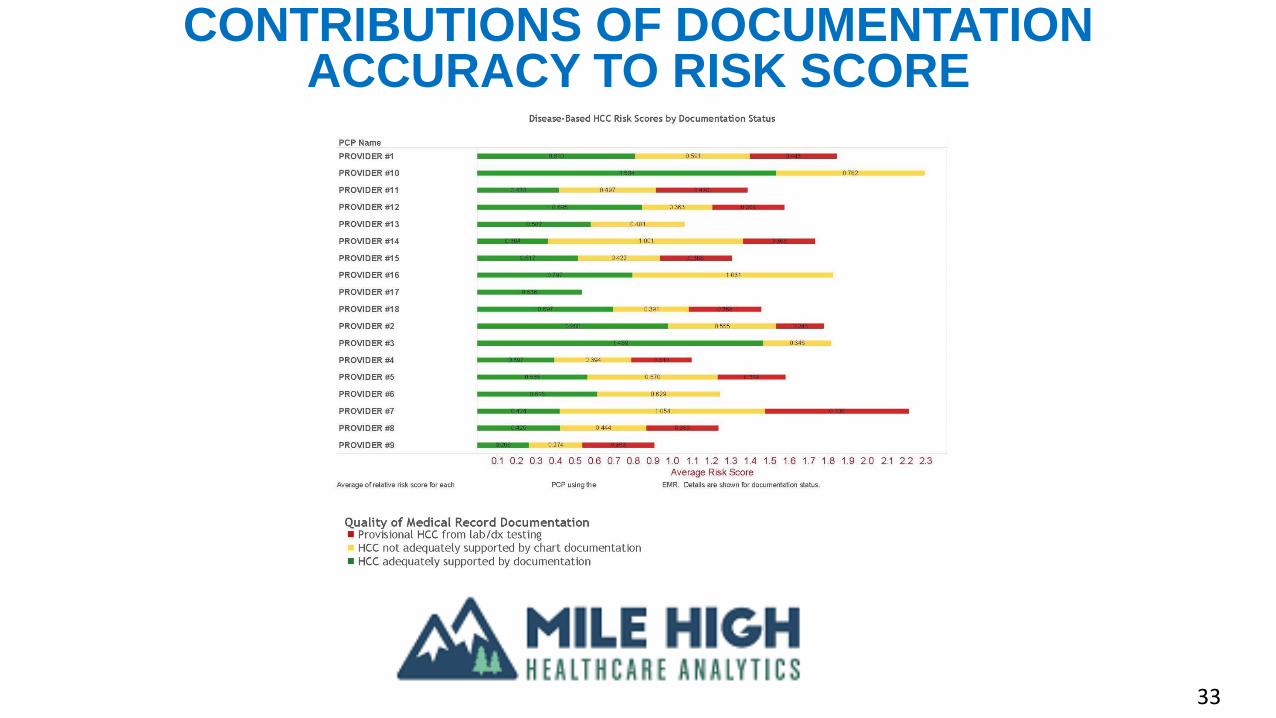
CONTRIBUTIONS OF DOCUMENTATION ACCURACY TO RISK SCORE
33
OBSERVATIONS FROM PCP ASSESSMENTS
• Looking at the data at the PCP-level, only 30 percent of the HCC-specific risk score
comes from documentation that adequately substantiates the HCC
• Another 38 percent of the risk score is inadequately documented in the PCP medical
records
• There are substantial opportunities to increase risk score is suspect conditions were
correctly documented
34

PLEASE VISIT OUR NEW WEBSITE!
35
WWW.HEALTHCAREANALYTICS.EXPERT
LEARN ABOUT OUR NEWEST QUALITY IMPROVEMENT TOOL: QISIM
36

UPCOMING CONFERENCES
• Mile High Healthcare Analytics will be at:
– On May 24th, at the Risk Adjustment Forum in Cedar Creek, TX. Richard will be speaking on,
“RAPS TO EDS Transition: Analysis and Implications for the Industry”
– On June 13th, Richard will be co-teaching the CMS & HHS Risk Adjustment 101 Workshop in
Paradise Point, San Diego CA
– On June 27th, we will be at The 6th Annual Star Ratings Master Class, The Star Ratings
Strategic Planning Forum, in Scottsdale, AZ
37

NEXT WEBINAR
• Mile High Healthcare Analytics will continue our free
webinar series. We will continue to present key risk
adjustment and performance improvement topics to health
plans and provider groups.
• Our next webinar will be held on:
– Thursday June 9, 2016: Beyond the Quality Measurement
Scorecard
• Please watch http://www.healthcareanalytics.expert/news-
and-events/free-webinar-series/ to learn about our webinar
topics
CONTACT INFORMATION
Richard Lieberman
720-446-7785 (voice)
www.healthcareanalytics.expert
Richard Bernstein, MD, FACP
40
For further information about any of the 4 approaches, contact:
Richard H Bernstein, MD, FACPBernstein Associates, [email protected]
M: 973-495-3138
CONTACT INFORMATION

THANK YOU FOR JOINING US!!
Our new website is up! Please visit us at:
www.healthcareanalytics.expert