Embed Size (px)
DESCRIPTION
Reverend Bayes Sample Sizes and Statistical Analysis. Statisticians. Statisticians are generally ‘power’ mad, that is they want to minimise uncertainty around any effect estimate. Two camps: Frequentists and Bayesians. Frequentists. - PowerPoint PPT Presentation
Citation preview

Reverend BayesSample Sizes
and Statistical Analysis

Statisticians Statisticians are generally ‘power’
mad, that is they want to minimise uncertainty around any effect estimate.
Two camps: Frequentists and Bayesians.

Frequentists The philosophy underlying most of
our statistics is frequentist. Frequentists produce the ‘null’
hypothesis. The experiment is set up to ‘prove’ the null hypothesis of ‘no difference’.
See themselves as more ‘objective’ and ‘scientific’ than Bayesians.

Frequentist Null hypothesis This is nonsense! If we truly believed in the null
hypothesis we would not undertake a trial. We would just chose the cheapest treatment or give treatments according to patient preferences.
We usually have an ‘idea’ about the likely effect of a treatment.

Reverend Bayes A minister who lived in the 18th
Century but dabbled in statistics. Produced Baye’s theorem, which
includes prior beliefs in statistical calculations.
Was not published ‘till 20 years after his death - truly ‘publish or perish’.

God and statistics Frequentists believe the ‘truth is
out there’ and we are getting sample estimates of the truth.
Bayes believed only God can know the ‘truth’ and as mere mortals we can only gain probability estimates of the truth, which is why he developed Bayes theorum.

Bayesians Until recently Bayes’ approach only
used in diagnostic testing in health research.
Widely used in other areas. Not widely used partly because of
computational difficulties but also many think it is ‘unscientific’.
More recently computational problems have been largely solved and increased interest in using the method.

Bayesian statistics The Bayesian approach is
attractive as it is similar to everyday decision making.
One uses prior experience to make a judgement and use new data to inform future decisions.

Bayesians vs Frequentists When we seek to observe a 50%
increase or decrease in essence this is a Bayesian approach as we have a prior belief that A may be 50% more effective than B.
If we had a belief in the null hypothesis then the sample size would be infinite to ‘prove’ no difference.

Prior beliefs Bayesians want to be more explicit
about prior beliefs and include these in a design and analysis.
Data would have to be particularly strong to overturn a prior belief or weaker to confirm.

Bayesian Problems Bayesians argue that one should
keep doing a study until the confidence in the results are credible enough to stop the trial.
Problem that one cannot really plan a trial unless we have a prior sample size.

Not Scientific Prior beliefs may be so incorrect
that they could mislead research. Strong prior belief was HRT prevented heart disease. Shown to be untrue. Small trials showing this to be a fallacy would not overturn this strong belief.

GRIT Trial – Bayesian trial The design of this trial included prior
beliefs on the effectiveness of early or late delivery of babies.
Data were analysed every 6 months (without p values) and presented to clinicians in order for them to change their minds and either randomise more patients or stop randomising.

Bayesian analysis Expect to see more studies using
Bayesian methods in the future. Rapid area of statistical and
economic research.

Statistical Outcomes Two measures of effect.
Dichotomous = yes/no; dead/alive; passed/failed.
Continuous = blood pressure; weight; exam scores.

Binary outcomes Basically in a RCT we can compare
the percentages in the two groups. If the percentages are significantly
different this is due to the intervention.

Continuous outcomes Scores, such as blood pressure,
quality of life, test scores are compared. Usually the mean scores are compared although sometimes the medians are used.
Usually, mean scores have a ‘normal’ or near normal distribution.


Standard deviation This is calculated by taking the
differences of individual scores from the mean squaring these differences and dividing by the number of observations.
The square root is the SD of this.

Effect sizes The effect size is the difference between
means divided by the standard deviation.
If students in Group A have a mean score of 60 vs 50 in Group B and the standard deviation is 20 the effect size is 0.5 (10/20).
Few new health care treatments get effect sizes GREATER than 0.5.

Relative Risks etc Binary outcomes are often described in
relative risk or odds ratios. Relative risk is: if 10/100 events in group A versus 5/100 in group B. A vs B RR = 2 (10%/5%) B vs A RR = 0.5 (5%/10%).
Odds ratios produce similar results for rare events.
Confidence intervals passing through 1 = not statistically significant.

Sample sizes for trials The bigger the better – size
matters in trials. Most trials approach sample size
estimation using a frequentist approach.

Background Many trials are ‘underpowered’ that is
they are too small to detect a difference that is important.
This is commonly referred to as a Type II error.
At least 30% of trials published in major general journals are underpowered.
This is worse among other journals.

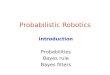
Meta-analysis of Hip Protectors (Ranked by Size)
Energy absorbing or unknow types
‘Shell’ type Protectors
Community
Community
Nursing Home
Community
Community

Hip protector trials All trials (bar ours of course) were
underpowered to detect large (e.g., 50%) reductions in hip fractures.
Small positive trials tended to be published giving an overestimated effect of benefit.

Sample size estimation Text books usually recommend the
following approach to sample size estimation. Define a clinically important difference
in outcome between treatments; Design an experiment that is
sufficiently large to show that such a difference is ‘statistically significant’.

Clinical Significance The first problem is definition of
what is ‘clinically significant’. This is usually unclear.
Any difference of death, for example, is pretty clinically significant.
To power a trial to reduce mortality by 1 death would require an almost infinitely large study.

Epidemiological Significance A more common justification of
sample size is observed effect sizes from epidemiological studies (which may be overestimates).
Or from meta-analyses of smaller trials (which again may over-estimate due to publication bias).

Statistical significance What is statistical significance?
Tradition in medical research states that p = 0.05 or lower is significant. Difference between p = 0.05 and p = 0.06 is trivial, one is significant and the other is not.
Other disciplines, economics, sometimes use p = 0.10.

P values Originally Pearson constructed p
values as a guide not as a cut off. The idea was that given what was known about a treatment (side-effects etc) the p value would add extra information as to whether one should accept the finding.
But p value = 0.05 has become set in stone.

Fallacy of P values If there is a treatment effect that is not
statistically significant p = 0.20 and the null hypothesis is accepted (I.e. there is no difference) you would have only a 20% chance of being correct and 80% of making the wrong decision.
Really one should go for a treatment that the data favours irrespective of the p value.

Significance BOTH clinical and statistical
significance are often arbitary constructs.
‘Economic significance’ can be less arbitrary.
One can ascertain an economic difference that makes sense.
To demonstrate cost neutrality is a significant endpoint.

Economic Significance For example, a randomised trial of two
methods of endometrial resection was powered to detect a 15% difference in ‘satisfaction’.
Important clinical outcome was re-treatment rates.
An economic difference of significance was about 8% in retreatment rates as this would be cost saving.
Torgerson & Campbell BMJ 2000;697.

Endometrial Resection The trial was only sufficiently
powerful to show a 12% difference in retreatment rates.
Trial showed a 4% difference (95% CI of –4% to 11%) but could not exclude an 8% difference.
Pinion et al. BMJ 1994;309:979-83.

Forget theory What normally happens is Clinician
says to statistician I can get 70 patients in a trial in a year.
Stato says ‘needs to be bigger’ clinician has a couple of mates who can add 140 more. Statistician calculates difference that 210 participants can show.

What should be done? For a continuous outcome (e.g. Quality of
Life, blood pressure) we should aim to detect AT LEAST half a standardize effect size, which needs 128 participants.
Ideally we need to detect a somewhat smaller difference.
For dichotomous outcome we should have enough power to detect a halving or doubling.

Attrition and clustering Do not forget to boost sample size to
take into account loss to follow-up.
Depending on patient group this might range from 5-30%.
Finally, if it is a cluster trial total sample size needs to be inflated.

How to calculate a sample size This is easy. Lots of tables or
programmes will do this. For continuous outcomes a simple formulae is: take standardised difference and divide the square of this into 32 (80% power) or 42 (90% power).
E.g., 0.5 squared is 0.25 32/0.25 = 128 or 42/0.25 = 168.

For binary outcomes Look at sample size tables or use
programme, but rule of thumb about 800 is needed for 80% power to show 10% difference between 40% and 50% or 50% and 60%. To see 5% difference quadruple sample size.

Cluster trials For cluster trials we need to inflate
the sample size to take into account the ICC of the clusters. 1+(cluster size X ICC) = design effect.
For example, a RCT of adult literacy classes mean size = 8. ICC from a previous trial shows ICC of reading = 0.3.

Cluster sample size We want to detect 0.5 difference
which for an individual RCT = 128 for 80% power. Cluster size = 8 take 1 =7.
7 x 0.3 = 2.1 + 1 = 3.1 = 397 participants or t 50 clusters of a mean of 8 per cluster.

Analysis The first analysis that many people
do is compare groups at baseline. Typical many comparisons are
made, for example, a paper of a trial in the most recent JAMA (Feb 4, 2004) shows this typical baseline comparison table.

Baseline Tests (n = 24 tests)

Baseline testing Of the 24 comparisons 3 were
‘statistically’ significant (I.e, p < 0.05).
What should we do with this information?
Has randomisation failed? It is useless information and an
exercise in futility.

Baseline testing Assuming randomisation has not
been subverted, which in this case looks unlikely, then any differences will have occurred ‘by chance’ they are random differences.

What is wrong with baseline testing? Baseline testing will ALWAYS throw
up chance differences. This can mislead the credulous into believing there is something ‘wrong’ with the study. Also it can mislead some statisticians into ‘correcting’ these baseline imbalances in the analysis.

Baseline variables: What should be done?
Before the study starts specify in advance important co-variates to be used in the analysis (e.g., centre, age) and adjust for these IRRESPECTIVE of whether or not randomisation balances them out.

Interim Data Analysis This is where the trial is analysed
BEFORE completion. This is done usually for ethical reasons so
that a trial can be stopped early if there is an overwhelming benefit or harm.
Women’s Health Initiative trial undertook an interim analysis and the trial was stopped because of harm.

Dangers of Interim Analysis
Sample size calculations assume 1 analysis. Repeated looks at the data WILL showed a significant differences, by chance, even when no difference exists.
The temptation is to stop the trial early when a statistical significance is achieved.
This could be a chance finding.

Interim Analysis To avoid premature stopping of a trial
interim analyses are usually undertaken by an independent committee with experience trialists.
Statistical significance is adjusted to take repeated looks of data into account (so p = 0.01 is significant rather than p = 0.05).

Analysis All point estimates should be
bounded by confidence intervals as well as the exact p value. A single principal analysis should be stated in advance (e.g., the primary outcome was a reduction in ALL fractures) secondary analysis are for research interest only.

Summary Sample size estimation is EASY.
The difficult bit is determining the likely effect size to inform the calculations.
Analyses are more straightforward from RCTs than non-RCTs because you do not need to adjust for baseline co-variates.