Embed Size (px)
Citation preview

Reverse the New Anticoagulants?
Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care
University Medical Center Brackenridge / Dell Seton Medical Center at the University of Texas
Seton Healthcare Family
Clinical Adjunct Faculty
University of Texas College of Pharmacy

Disclosure
• No financial conflicts of interest to disclose
related to this subject manner
• Discuss off-label uses of laboratory and
medication therapy

Learning Objectives
• Describe how to assess for the
presence of TSOA
• Discuss available options for TSOA
reversal
VIIa VII
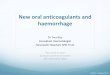
Target Specific Oral Anticoagulants (TSOA)
Direct Thrombin Inhibitor
• Dabigatran (Pradaxa®- 2010)
Factor Xa Inhibitor
• Rivaroxaban (Xarelto® - 2011)
• Apixaban (Eliquis® - 2012)
• Edoxaban (Savaysa® - 2015)
• Betrixaban (Portola® - in development)
XII XIIa
Damaged Surface
XI XIa
IX IXa VIIIa
X Xa
Tissue Factor
Va
Fibrinogen Fibrin
(I) (Ia)
Prothrombin Thrombin
(II) (IIa)
Intrinsic Pathway
Extrinsic
Pathway

Approach to Reversal
1. Recognize TSOA coagulopathy
2. Determine if drug present / assess urgency
3. Pharmacologic reversal

Recognizing Dabigatran Coagulopathy
Van Ryn, et al. J Thromb Haemost 2010;103:1116.
Assay Relationship Pearl
Diluted thrombin time (Hemoclot®) Diluted plasma, constant thrombin concentration
Quantitative, direct, linear Not routinely available
Use in clinical trials
Ecarin clotting time (ECT) Ecarin converts prothrombin to meizothrombin
Quantitative, direct, linear
Thrombin clotting time (TT) Directly assess the activity of thrombin
Qualitative, direct, linear Lacks standardization in
reagents; very sensitive
Activated partial thromboplastin time
(aPTT) Measures intrinsic pathway
Qualitative, indirect,
curvilinear
Normal suggests little to no
dabigatran acitivity

Recognizing Factor Xa Inhibitor Coagulopathy
Garcia D, et al. J Thromb Haemost 2013;11:245.
Cuker A, et al. J Thromb Thrombolysis 2015;39:288.
Assay Relationship Pearl
Chromogenic anti-FXa assay Factor Xa cleaves chromogenic substrate
directly proportional to activity
Quantitative, direct, linear No data on threshold values
Requires local calibration
and validation
Prothrombin time Clotting time triggered with tissue factor
Rivaroxaban: qualitative
Apixaban: insensitive
Edoxaban: qualitative, can’t rule
out
Dependent on reagent
May see modest elevations

Recognizing TSOA Coagulopathy Is Difficult…
• Lack of optimal and readily available assay
• Limited medical history
• Example: RCT of idarucizumab for dabigatran reversal
– Efficacy outcome: ECT & dTT reversal at central laboratory
– Patients given study drug & excluded from efficacy analysis
• ~25% normal dTT
• ~11% normal ECT
• Pharmacologic reversal should be guided by bleeding
Pollack CV, et al. N Eng J Med 2015;373:511.

Approach to Reversal
1. Recognize TSOA coagulopathy
2. Determine if drug present / assess urgency
3. Pharmacologic reversal

Applying Pharmacokinetics Characteristic Dabigatran Rivaroxaban Apixaban Edoxaban
Half-life by renal function, hrs
Clcr: > 80 mL/min
Clcr: 50-79 mL/min
Clcr: 30-49 mL/min
Clcr: < 30 mL/min
12-14
17
19
28
5-9
9
9
10
8-15
15
18
17
8.5
9
9
9.5
Renal elimination, % 80 36 27 50
Protein binding, % 35 92-95 87 55
Typical duration of
anticoagulation, days
1-3
AKI >3-5 d
1-2
> in AKI?
1-2
> AKI?
1-2
> AKI?
Drug – drug interactions
examples
P-glycoprotein
inhibitors
P-glycoprotein inhibitors
Cytochrome 3A4 inhibitors
P-glycoprotein
inhibitors
Nutescu EA, et al. Am J Health Syst Pharm 2013;70:1914.

Approach to Reversal
1. Recognize TSOA coagulopathy
2. Determine if drug present / assess urgency
3. Pharmacologic reversal
• Coagulation factor replacement / hemostatic agents
• Antidotes

PCC Considerations
Nutescu EA, et al. Am J Health Syst Pharm 2013;70:82.
Enriquez A, et al. Eurospace 2015; doi:10.1093/eurospace/euv030.
Frontera JA, et al. Neurocrit Care 2016:24:6-46.
• PCC recommended for TSOA reversal from multiple guidelines → if antidotes not available
– Dabigatran: activated or 4 factor PCC 50 unit/kg
– Anti-factor Xa: activated or 4 factor PCC 50 unit/kg
• Not considered standard of care in RCT
“Do what you can, with what you have, where you are”
-Theodore Roosevelt

Approach to Reversal
1. Recognize TSOA coagulopathy
2. Determine if drug present / assess urgency
3. Pharmacologic reversal • Coagulation factor replacement / hemostatic agents
• Antidotes

Hopeful Future: TSOA Antidotes Drug Mechanism Which TSOA Early Results Current Status
Idarucizumab
(Praxbind®)
From
Boehringer
Monoclonal
antibody;
binds dabigatran
(>350 affinity)
Dabigatran
Reversed coagulation markers
within 5 minutes
Sustained for >12 hours in
• Phase III study
ongoing
• FDA approved
Andexanet
From Portola
Modified factor Xa;
binds anti-Xa
(similar affinity)
Xa inhibitors
(direct and
indirect)
Plasma anti-Xa reduced >90%
within 2 minutes
Dose dependent response
• Phase III study
ongoing
Ciraparantag /
Aripazine
From
Perosphere
Synthetic
molecule; direct
binding
Universal Baseline hemostasis achieved
in 10-30 minutes
• Phase II study
ongoing
Mo Y, et al. Pharmacotherapy 2015;35:198.
Ansell JE, et al. N Eng J Med 2014;371:2141.

Idarucizumab: RE-VERSE AD Study Population Intervention Endpoints
Pollack
Phase 3
Multicenter
Single arm
Patients on dabigatran
A: life threatening hemorrhage
B: urgent (<8 hr) surgical or
invasive procedure
Goal = 300 pt; interim = 90 pt
5 g
intravenous
idarucizumab
(2.5 g / 50 mL x 2)
10 endpoint:
- Maximum percent dabigatran reversal (dTT or ECT)
2o endpoint:
- Proportion of patients with normalization by 4 hours
- Reduction in concentration of unbound dabigatran
- Clinical outcomes
Pollack CV, et al. N Eng J Med 2015;373:511.
• Demographics – Group A = 51 patients; Group B = 39
– Age 76.5 y, eCrCl 58 mL/min; time from dabigatran 15.4 hr
– Type of bleeding: ICH (20%), trauma (10%), GI (22%)

Pollack CV, et al. N Eng J Med 2015;373:511.
Unbound Dabigatran Levels

Pollack CV, et al. N Eng J Med 2015;373:511.
ECT Reversal
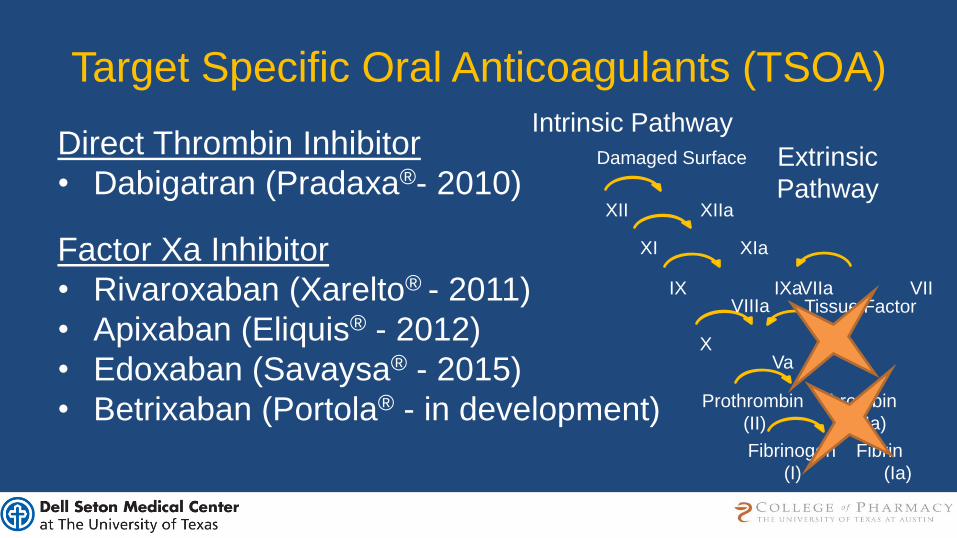
Idarucizumab Reverses Dabigatran…
• 100% maximum percentage reversal & normalized labs in 88-98%
• Unbound dabigatran levels <20 ng/mL: – 93% of pts at 12 hours
– 79% at 24 hours
• Clinical outcomes – Investigator-reported time to hemostasis: 11.4 hours
– Urgent procedures: 92% normal intraoperative hemostasis
– Mortality: 20% (5 fatal bleeding events)
– Thrombotic events: 5 patients; only 1 within 72 hours
• Remains to be defined – Repeat dosing?
– Overdose?
Pollack CV, et al. N Eng J Med 2015;373:511.

Does Idarucizumab Improve Outcomes?
• Considerations – Lack of control group
– Broad inclusion (mortality: 20% vs. 10-20% previously)
• How important is neutralizing the anticoagulant effect? – Warfarin vs. dabigatran in intracranial hemorrhage
• In-hospital mortality dabigatran 20% (n=101) vs. warfarin 22% (n=2,290)
• Propensity score adjustment 0.93 (0.62-1.37)
Bauer K. N Eng J Med 2015;373:569.
et al. Circulation 2013;128:2325.
Alonso A, et al. Stroke 2014;45:2286.
Granger, et al. Circulation 2012;125:159.
Majeed,

Hopeful Future: TSOA Antidotes Drug Mechanism Which TSOA Early Results Current Status
Idarucizumab
(Praxbind®)
From
Boehringer
Monoclonal
antibody;
binds dabigatran
(>350 affinity)
Dabigatran
Reversed coagulation markers
within 5 minutes
Sustained for >12 hours in
• Phase III study
ongoing
• FDA approved
Andexanet
From Portola
Modified factor Xa;
binds anti-Xa
(similar affinity)
Xa inhibitors
(direct and
indirect)
Plasma anti-Xa reduced >90%
within 2 minutes
Dose dependent response
• Phase III study
ongoing
Ciraparantag /
Aripazine
From
Perosphere
Synthetic
molecule; direct
binding
Universal Baseline hemostasis achieved
in 10-30 minutes
• Phase II study
ongoing
Mo Y, et al. Pharmacotherapy 2015;35:198.
Ansell JE, et al. N Eng J Med 2014;371:2141.

Andexanet Study Population Intervention Endpoints
Siegal
Phase 2
Placebo
controlled
Elderly (50-75), healthy
volunteers
Received rivaroxaban and
apixaban for ~4 days
Andexanet: 400-800 mg bolus
-or-
Andexanet: 400-800 mg bolus & 4-8 mg/min for 2 hr
-or-
Placebo
10 endpoint:
- % change in anti-factor
Xa activity
Siegal DM, N Eng J Med 2015. epub
ahead of print
Phase 3 trial primary outcome good or excellent clinical
hemostasis

Conclusions • Identify TSOA coagulopathy:
– Dabigatran: TT, aPTT, and maybe rapid TEG
– Factor Xa inhibitors: protime and chromogenic anti-Xa
• Establish time from last dose (3-5 half-lives)
– Prolonged with end-organ dysfunction?
– Drug-drug interactions?
• Reversal options in a transition period – Dabigatran: ? dialysis and / or aPCC ? → idarucizumab
– Xa inhibitors: 4 factor or activated PCC → andexanet
• This transition will:
– Challenge our approach to reversal
– Improve outcomes?

Reverse the New Anticoagulants?
Mitchell J Daley, PharmD, BCPS Clinical Pharmacy Specialist, Critical Care
University Medical Center Brackenridge / Dell Seton Medical Center at the University of Texas
Seton Healthcare Family
Clinical Adjunct Faculty
University of Texas College of Pharmacy