Embed Size (px)
Citation preview

Reversible Posterior LeukoencephalopathySyndrome Complicating Cytotoxic Chemotherapy
for Hematologic Malignancies
C.S. Tam,1 J. Galanos,1 J.F. Seymour,1 A.G. Pitman,2 R.J. Stark,1,3,4 and H.M. Prince1*1Hematology Service, Peter MacCallum Cancer Centre, Melbourne, Victoria, Australia
2Department of Diagnostic Imaging, Peter MacCallum Cancer Centre, Melbourne, Victoria, Australia3Department of Neurology, Monash University, The Alfred Hospital, Commercial Road, Melbourne, Victoria, Australia4Department of Medicine, Monash University, The Alfred Hospital, Commercial Road, Melbourne, Victoria, Australia
Reversible posterior leukoencephalopathy syndrome (RPLS) is an uncommon but dis-
tinctive clinicoradiological entity comprising of headache, seizures, visual disturbance,
and altered mental function, in association with posterior cerebral white matter edema.
With appropriate management, RPLS is reversible in the majority of cases. Previous
reported associations of RPLS include hypertension, eclampsia, renal failure, and use
of immunosuppressive drugs; reports in the adult hematology setting are rare. We report
two cases of adults undergoing treatment for hematological malignancies who devel-
oped RPLS, and we emphasize the importance of early recognition and institution of
appropriate management in reducing the risk of development of permanent neurological
disability. Am. J. Hematol. 77:72–76, 2004. ª 2004 Wiley-Liss, Inc.
Key words: posterior leukoencephalopathy; hypertensive encephalopathy; eclampsia;
cyclosporine encephalopathy; cytotoxic chemotherapy
INTRODUCTION
Reversible posterior leukoencephalopathy syndrome(RPLS) is a term first used by Hinchey et al. [13] todescribe an uncommon but distinct clinicoradiologicalentity of headache, seizures, visual disturbance, andaltered mental function associated with symmetricalposterior hemispheric edema. The syndrome is char-acterized by its reversibility upon control of hyper-tension and other primary instigating factors [13].Imaging demonstrates evidence of white matteredema, usually affecting the parieto-occipital regionin a strikingly symmetrical distribution [13,21]. Theetiology of RPLS is not fully understood but isbelieved to be related to failure of cerebral autoregu-lation leading to development of vasogenic edema[13,21,23]. RPLS is most commonly seen in patientswith hypertensive encephalopathy, eclampsia, renalfailure, or use of cyclosporine or tacrolimus [13].Despite increasing awareness of RPLS as a complica-tion of treatment of childhood cancers [8,22,24,25],this syndrome is rarely reported in the adult oncologysetting. We report two patients who developed
RPLS during cytotoxic chemotherapy for hematologi-cal malignancies.
CASE ONE
A 65-year-old man was admitted for managementof advanced-stage multiple myeloma, with rapid pro-gression of disease after brief response to previoustherapy with high-dose cyclophosphamide (4 g/m2).Salvage chemotherapy with DT-PACE (dexa-
methasone, thalidomide, cisplatin, adriamycin, cyclo-phosphamide, and etoposide) [20] was commenced,
*Correspondence to: Associate Professor H. Miles Prince,Hematology Service, Peter MacCallum Cancer Centre, LockedBag 1, A’Beckett Street, Victoria 8006, Australia.E-mail: [email protected]
Received for publication 6 November 2003; Accepted 31 March2004
Published online in Wiley InterScience (www.interscience.wiley.com).DOI: 10.1002/ajh.20147
American Journal of Hematology 77:72–76 (2004)
ª 2004 Wiley-Liss, Inc.

with intravenous fluids for tumor lysis prophylaxis.The patient developed significant fluid overloaddespite regular administration of frusemide, withweight gain of 10% above admission body weightand moderate elevation of blood pressure (150/80mmHg, from baseline of 120/70 mmHg).On day 8, the patient developed sudden onset
headache, cortical blindness, and ocular paresis, inassociation with hypertension of 180/100 mmHg.Computerized tomography (CT) scan of the brainrevealed widespread bilateral occipital lobe whitematter edema; diagnostic lumbar puncture was notperformed at this time because of the risk of cerebralherniation. The patient’s conscious state rapidly dete-riorated, and he became comatose 2 hr post headacheonset, with recurrent left-sided focal seizures.Medical control of hypertension was instituted, and
the patient’s conscious state improved rapidly. By thethird day post onset, all neurological deficits hadresolved completely, with no recurrence of seizureactivity. A magnetic resonance (MR) scan of the
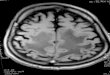
head revealed bilateral posterior white matter edemacharacteristic of RPLS (Fig. 1).Repeat MR scan of the head 2 weeks later showed
near-complete resolution of previous extensiveabnormalities. The patient remained free of recurrentneurological symptoms but died from sepsis 2 monthslater.
CASE TWO
A 60-year-old man was admitted for managementof relapsed lymphoblastic lymphoma.Chemotherapy with high-dose methotrexate (1 g/m2
over 24 hr) and cytarabine (1.5 g/m2 every 12 hr � 4doses) was administered, complicated by acute renalfailure and severe methotrexate toxicity. Use of intra-venous hydration resulted in significant fluid over-load (weight gain of 12% body weight). Serumcreatinine peaked at 0.34 mmol/L on day 4 andremained between 0.15 and 0.25 mmol/L over thesubsequent week.
Fig. 1. (Top) Fluid-attenuated inversion recovery (FLAIR) magnetic resonance sequences of Patient 1, showingwidespread hyperintense signals in occipital white matter and left hippocampus at presentation (left, arrows). Repeatscan 2 weeks later (right) showing complete resolution of occipital white matter abnormality and persistence of lefthippocampal infarct. (Bottom) FLAIR magnetic sequences of Patient 2, showing multiple symmetrical foci of hyperintensesignal within occipital white matter at presentation (left, arrows). Repeat scan 4 months later (right) showing completeresolution of white matter abnormalities.
Case Report: Posterior Leukoencephalopathy in Hematology 73

On day 8, the patient developed headache andblurring of vision, in association with hypertensionof 150/90 mmHg. On day 9, he deteriorated withincreasing vagueness, dysarthria, and gait unsteadi-ness; that evening he had a generalized tonic–clonicseizure.MR scan showed symmetric occipital white matter
abnormalities consistent with RPLS (Fig. 1). Medicalcontrol of hypertension and correction of fluid over-load was instituted, with rapid resolution of thepatient’s neurological deficits. Diagnostic lumbarpuncture performed 24 hr post RPLS onset showednormal opening pressure and normal cerebral spinalfluid microscopy and biochemistry. A repeat MRscan performed 4 months later showed complete reso-lution of changes.The subsequent clinical course was complicated by
recurrent lymphoma requiring further chemotherapy.Meticulous attention to blood pressure control andfluid management resulted in no recurrence of RPLS,despite development of severe tumor lysis syndrome,multiple episodes of septic shock, and eventual pro-gression to dialysis-dependent end-stage renal failure.Five months post RPLS, the patient underwent
autologous stem cell transplantation complicated bysevere neutropenic sepsis and eventual death frommultiorgan failure. Five days before death, thepatient developed confusion progressing to coma, inassociation with severe hypertension refractory tointravenous antihypertensive therapy with atenolol,glycerine trinitrate, and hydralazine. Although therewas a strong clinical suspicion for recurrent RPLS, noneuroimaging was obtained at the time and thepatient’s family declined a postmortem examination.
DISCUSSION
RPLS is characterized by subacute onset of head-ache, altered conscious state and behavior, and visualdisturbance ranging from blurred vision to total cor-tical blindness; seizures are common and may heraldthe onset [13]. Focal deficits of cranial nerves andlimbs are uncommon [10,13,15,21]. Characteristicradiological changes are those of white matteredema, with often strikingly symmetrical hyperin-tense signals predominantly in the posterior hemi-spheres on T2-weighted MR scanning; this is bestvisualized on fluid-attenuated inversion recovery(FLAIR) sequences [13,21]. The majority of patientspreviously reported have complete or near-completeresolution of clinical and radiological changes withindays to weeks [13].RPLS is typically seen in patients with hyperten-
sive encephalopathy, eclampsia, renal failure, anduse of immunosuppressant drugs [13]. Many other
associations have been reported, including microan-giopathy [2], sickle cell disease [10], intravenousimmunoglobulin use [28], large-volume red cell trans-fusion [16], stem cell re-infusion [12], use of erythro-poietin or G-CSF [5,17], hypercalcemia [18], andacute intermittent porphyria [19,26].In the pediatric oncology literature, there is increas-
ing awareness of RPLS as a complication of cancertreatment [22,24,25], particularly in the setting ofhematopoietic stem cell transplantation where it isthe most common severe neurological complication[8].In adult oncology literature, however, RPLS is rarely
recognized outside the hematopoietic stem cell trans-plantation setting. No single chemotherapeutic agent ortherapeutic regimen has been identified to date as beingconsistently associated with RPLS. Implicated drugshave included single-agent cisplatin [15] or cytarabine[27], as well as combinations of adriamycin [4,7,9,11,14], cyclophosphamide [4,7,9,11,14], vincristine[4,7,9,11], corticosteroids [4,7,9,11,14], ifosfamide [9],etoposide [9], and cytarabine [9]. Most publishedreports of RPLS complicating combination chemother-apy for adult hematological malignancies involved theuse of intrathecal chemotherapy, with methotrexate,cytarabine, or both [7,9,11,14]; there is therefore pre-vious uncertainty about the contributory role ofintrathecal chemotherapy in RPLS development.Neither of our patients, however, received intrathecalchemotherapy. Furthermore, in the pediatric literaturethere are examples of continued administration ofintrathecal chemotherapy to patients who developedRPLS following initial regimens that involved intrathe-cal treatment, with no recurrence of neurological symp-toms [24]. There is therefore little evidence of etiologiclink between RPLS and intrathecal administration ofcytotoxic drugs.One constant feature in all reported cases of RPLS
complicating cytotoxic chemotherapy is the presenceof systemic hypertension [4,7,9,11,14,15]. Hyperten-sion is also a feature in the vast majority of RPLSreported [5,7,9–11,13–16,19,21,23–26]. In contrast toencephalopathy caused by isolated malignant hyper-tension, patients with RPLS often present with onlymoderate levels of hypertension (systolic blood pres-sure 130–200 mmHg, diastolic blood pressure gener-ally > 90 mmHg); in the majority of cases this stillrepresents a significant increase above baseline levels.One hypothesis for the pathogenesis of RPLS consis-tent with this observation involves dysfunctionof cerebral vascular autoregulation. Under normalcircumstances, sympathetic innervation of cerebralvessels assists in regulating intracerebral blood flowagainst fluctuations in systemic perfusion pressure [3];in RPLS, failure of autoregulation due to unknown
74 Case Report: Tam et al.

mechanisms result in hyperperfusion of the brainfollowing only modest rises in blood pressure, withresultant breakdown of blood–brain barrier andinterstitial edema [3,13,26]. Posterior hemispheric pre-dilection may be explained by poor sympatheticinnervation of vertebrobasilar system relative to thecarotid system [6]. Evidence supporting vascularpathogenesis of RPLS includes demonstrations ofvasospasm during acute-phase RPLS [11,16] andMR brain–water diffusion studies suggesting thatwhite matter edema in RPLS is largely vasogenic inorigin [21,23,25].In the majority of reported cases, RPLS is fully
reversible within a period of days to weeks, withremoval of the inciting factor and control of the bloodpressure [13]. However, permanent neurological dis-ability can occur, often in associationwith complicatingcerebral infarction or hemorrhage [1,11]; fatalities havealso been reported [4,9]. The MR findings of hyper-intense signals on diffusion-weighted images andrestricted diffusion on apparent diffusion coefficientmap are occasionally seen and are suggestive ofcytotoxic edema; these findings may be predictive ofirreversible infarction [1,10,11,25].As a result of our experience, our institution now
considers patients with one or more of (i) significantfluid overload (>10% baseline weight), (ii) meanblood pressure >25% of baseline, and (iii) creatinine>0.16 mmol/L to be at high risk for RPLS; all suchpatients receive early neuroimaging to evaluate anyunexplained neurological change. In addition, meti-culous attention is paid to changes in weight andblood pressure in any patient who receives a regimenrequiring more than 3 L of intravenous fluid daily.RPLS may be an under-appreciated complication ofcytotoxic therapy; early diagnosis requires a highclinical index of suspicion, appreciation that initialneurological deficits are variable and often subtle,and timely evaluation of cerebral white matter withneuroimaging.
REFERENCES
1. Ay H, Buonanno FS, Schaefer PW, et al. Posterior leukoencepha-
lopathy without severe hypertension: utility of diffusion-weighted
MRI. Neurology 1998;51:1369–1376.
2. Bakshi R, Shaikh ZA, Bates VE, Kinkel PR. Thrombotic throm-
bocytopenic purpura: brain CT and MRI findings in 12 patients.
Neurology 1999;52:1285.
3. Beausang-Linder M, Bill A. Cerebral circulation in acute arterial
hypertension—protective effects of sympathetic nervous activity.
Acta Physiol Scand 1981;111:193–199.
4. Cain MS, Burton GV, Holcombe RF. Fatal leukoencephalopathy
in a patient with non-Hodgkin’s lymphoma treated with CHOP
chemotherapy and high-dose steroids. Am J Med Sci 1998;315:
202–207.
5. Delanty N, Vaughan C, Frucht S, Stubgen P. Erythropoietin-
associated hypertensive posterior leukoencephalopathy. Neuro-
logy 1997;49:686–689.
6. Edvinsson L, Owman C, Sjoberg NO. Autonomic nerves, mast
cells, and amine receptors in human brain vessels. A histochemical
and pharmacological study. Brain Res 1976;115:377–393.
7. Edwards MJ, Walker R, Vinnicombe S, Barlow C, MacCallum P,
Foran JM. Reversible posterior leukoencephalopathy syndrome
following CHOP chemotherapy for diffuse large B-cell lymphoma.
Ann Oncol 2001;12:1327–1329.
8. Faraci M, Lanino E, Dini G, et al. Severe neurologic complica-
tions after hematopoietic stem cell transplantation in children.
Neurology 2002;59:1895–1904.
9. Greenwood MJ, Dodds AJ, Garricik R, Rodriguez M. Posterior
leukoencephalopathy in association with the tumour lysis syn-
drome in acute lymphoblastic leukaemia—a case with clinico-
pathological correlation. Leuk Lymphoma 2003;44:719–721.
10. Henderson JN, Noetzel MJ, McKinstry RC, White DA,
Armstrong M, DeBaun MR. Reversible posterior leukoencepha-
lopathy syndrome and silent cerebral infarcts are associated with
severe acute chest syndrome in children with sickle cell disease.
Blood 2003;101:415–419.
11. Henderson RD, Rajah T, Nicol AJ, Read SJ. Posterior leukoen-
cephalopathy following intrathecal chemotherapy with MRA-
documented vasospasm. Neurology 2003;60:326–328.
12. Higman MA, Port JD, Beauchamp NJ Jr, Chen AR. Reversible
leukoencephalopathy associated with re-infusion of DMSO pre-
served stem cells. Bone Marrow Transplant 2000;26:797–800.
13. Hinchey J, Chaves C, Appignani B, et al. A reversible posterior
leukoencephalopathy syndrome. N Engl J Med 1996;334:494–500.
14. Honkaniemi J, Kahara V, Dastidar P, et al. Reversible posterior
leukoencephalopathy after combination chemotherapy. Neurora-
diology 2000;42:895–899.
15. Ito Y, Arahata Y, Goto Y, et al. Cisplatin neurotoxicity present-
ing as reversible posterior leukoencephalopathy syndrome. AJNR
Am J Neuroradiol 1998;19:415–417.
16. Ito Y, Niwa H, Iida T, et al. Post-transfusion reversible posterior
leukoencephalopathy syndrome with cerebral vasoconstriction.
Neurology 1997;49:1174–1175.
17. Kastrup O, Diener HC. Granulocyte-stimulating factor filgrastim
and molgramostim induced recurring encephalopathy and focal
status epilepticus. J Neurol 1997;244:274–275.
18. Kastrup O, Maschke M, Wanke I, Diener HC. Posterior reversible
encephalopathy syndrome due to severe hypercalcemia. J Neurol
2002;249:1563–1566.
19. Kupferschmidt H, Bont A, Schnorf H, et al. Transient cortical
blindness and bioccipital brain lesions in two patients with acute
intermittent porphyria. Ann Intern Med 1995;123:598–600.
20. Lee C-K, Barlogie B, Munshi N, et al. DTPACE: an effective,
novel combination chemotherapy with thalidomide for pre-
viously treated patients with myeloma. J Clin Oncol 2003;21:
2732–2739.
21. Mukherjee P, McKinstry RC. Reversible posterior leukoencepha-
lopathy syndrome: evaluation with diffusion-tensor MR imaging.
Radiology 2001;219:756–765.
22. Pavlakis SG, Frank Y, Chusid R. Hypertensive encephalopathy,
reversible occipitoparietal encephalopathy, or reversible posterior
leukoencephalopathy: three names for an old syndrome. J Child
Neurol 1999;14:277–281.
23. Schwartz RB, Bravo SM, Klufas RA, et al. Cyclosporine neuro-
toxicity and its relationship to hypertensive encephalopathy: CT
and MR findings in 16 cases. AJR Am J Roentgenol 1995;165:
627–631.
24. Shin RK, Stern JW, Janss AJ, Hunter JV, Liu GT. Reversible
posterior leukoencephalopathy during the treatment of acute lym-
phoblastic leukemia. Neurology 2001;56:388–391.
Case Report: Posterior Leukoencephalopathy in Hematology 75

25. Suminoe A, Matsuzaki A, Kira R, et al. Reversible posterior
leukoencephalopathy syndrome in children with cancers. J Pediatr
Hematol Oncol 2003;25:236–239.
26. Utz N, Kinkel B, Hedde JP, Bewermeyer H. MR imaging
of acute intermittent porphyria mimicking reversible posterior
leukoencephalopathy syndrome. Neuroradiology 2001;43:
1059–1062.
27. Vaughn DJ, Jarvik JG, Hackney D, Peters S, Stadtmauer EA.
High-dose cytarabine neurotoxicity: MR findings during the
acute phase. AJNR Am J Neuroradiol 1993;14:1014–1016.
28. Voltz R, Rosen FV, Yousry T, Beck J, Hohlfeld R. Reversible
encephalopathy with cerebral vasospasm in a Guillain-Barre
syndrome patient treated with intravenous immunoglobulin.
Neurology 1996;46:250–251.
76 Case Report: Tam et al.