Embed Size (px)
DESCRIPTION
Cardiomyopathy of different etiologies
Citation preview

7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 1/9
Review Article
Cardiomyopathy in Young Adults
Introduction
Cardiomyopathy are commonly divided into three types: dilated, hypertrophic and restrictive
forms. The estimated prevalence of dilated cardiomyopathy is 920 cases per 100,000 persons, 50
to 200 cases per 100,000 persons of hypertrophic cardiomyopathy while restrictive
cardiomyopathy is the rarest encountered form1. In young adults, peripartum cardiomyopathy
constitutes a rare but potentially life-threatening condition when left untreated. In this review
article, we will present an overview of peripartum cardiomyopathy, its management, prognosisand prevention.
Case illustration
A 33 year old female was brought to the hospital because of her generalized edema and
shortness of breath. The patient history reveals that the symptoms originated 5 months earlier. At
5 months postpartum, an ulcer appeared on the anterior medial left leg. The ulcer was red, tender
and oozing clear liquid. She was taken to the nearest health clinic where she was diagnosed with
diabetes mellitus and discharged with ‗sugar pills‘, the names of which the patient could not
recall. However, the ulcer remained unchanged. Financial difficulties had hindered the patient
from seeking medical care and by the fourth month of illness, the edema had spread to both of
her upper and lower extremities along with a new onset of dyspnea. At this point, she was taken
to a hospital in order to receive treatment.
Medical history reveals that the patient was diagnosed with gestational hypertension at
the second trimester of pregnancy. Tetanus vaccination status has never been administered. The
patient and family denied a history of seizure or hemorrhage during labor. She gave birth at 36
weeks of gestation to a viable 3,3kg male infant who is healthy and thriving presently. On the
eleventh month postpartum, patient was taken to the hospital and a full investigation was
performed. On physical examination, she was conscious but in moderate pain. Vital signs were
at normal range. Generalized edema was observed throughout the body with pitting edema on
both of her lower extremities. Massive ascites with abdominal circumference of 106cm was also
observed. Laboratory result showed normocytic normochromic anemia (Hb 11, 50 g/dL, Ht
36,84%). Urine analysis revealed cloudy appearance with the presence of high leukocyte
esterase, 16 leukocytes (N: 0-10) and 1+ bacteria. Erythrocyte sedimentation rate was elevated at

7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 2/9
20mm/hr along with total bilirubin of 1.4g/dL (N: 0.20-1.0g/dL). Albumin value was 3.01
(N:3.50-5.00g/dL) and potassium levels were 2.8g/dL (N: 3.6-5.0g/dL). Abdominal ultrasound
revealed massive ascites and other abdominal organs are within normal size range. Chest
roentgenogram revealed a CTR ratio of greater than 50% and increased bronchopulmonary
vasculature. Lung bases are cloudy and filled with fluid. A twelve-lead standard
electrocardiogram (ECG) showed tachycardia and right axis deviation. Echocardiography
revealed severe left ventricular systolic dysfunction with ejection fraction of 30% and dilated left
ventricle.
Disease Classification
Cardiomyopathy is classified into two forms2:
1). Primary form – disease are caused by damage to the heart muscle asa result of idiopathic or genetic mutations. Examples includehypertrophic cardiomyopathy, arrhythmogenic right ventricularcardiomyopathy, isolated ventricular non-compaction, mitochondrial
myopathy, eosinophilic endomyocardial disease and endomyocardialfibrosis.
2). Secondary form – disease are caused by damage to the heart muscle
as a result of insult from other factors such as drugs, autoimmunecondition, infections, granulomatous infiltrations, metabolic problems,
connective tissue disorders and neuromuscular disorders .
In many cases, cardiomyopathy is classified into three morphologic
types: dilated, restrictive and hypertrophic due to the differences in their
pathophysiology and anatomic features.
Case Definition
Peripartum cardiomyopathy is defined as cardiac failure that occurs (all most be present)3:
1) In the last month of pregnancy or within five months of delivery
2) No identifiable cause of cardiac failure3) No recognizable heart disease before the last month of pregnancy
4) An ejection fraction of less than 45% or the combination of an M-mode fractional
shortening of less than 30% and an end-diastolic dimension greater than 2.7cm/m2.
Figure 1

7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 3/9
Clinical Presentation
The early stages of cardiomyopathy are commonly asymptomatic. As the disease progresses
which may take months to years after the initial insult, patients commonly classic symptoms of
congestive heart failure some of which may be alone or in combination of 4:
I. Dyspnea with or without exertion
II. Palpitations and Diaphoresis
III. Angina
IV. Ascites
V. Peripheral Edema
VI. Pulmonary Edema
VII. Unexplained Fatigue
VIII. Syncope
IX. In some cases, sudden death
Laboratory evaluation may also be beneficial in differentiating between the three forms of
cardiomyopathy5:
Table 1.
Dilated Restrictive Hypertrophic
ChestRoentgenogram
1). Moderate to marked
cardiac silhouetteenlargement2).Pulmonary venoushypertension
Mild cardiac silhouetteenlargement
Mild to moderate cardiacsilhouette enlargement
ElectrocardiogramST-segment and T-wave
abnormalitiesLow voltage,
conduction defectsST-segment and T-wave
abnormalities
EchocardiogramLeft ventriculardilatation and
dysfunction
1). Increased left
ventricular wallthickness2). Normal or mildlyreduced systolicfunction
1). Asymmetric septal
hypertrophy2). Systolic anterior
motion (SAM) of themitral valve

7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 4/9
Dilated Cardiomyopathy
Alcohol 1)Consuming >90g/day
2)Polymorphism ofgene ALDH2 encodingalcohol metabolizing
enzyme
Peripartum 1)Develop at the last
trimester to within fivemonths postpartum
2)Inflammatorymyocarditis, immune
activation and gestationalhypertension
NeuromuscularDisease
Duchenne MuscularDystrophy associatedwith myocyte death.
Drugs1)Antineoplastic
Agents2)Anthracyclin
derivative3)Damage to inner
mitochondrialmembrane
Tako-TsuboDCM/Stress
1)Ballooning of coronaryepicardial coronary
vessels2)Associated withsudden stress or
adrenergic surge oncardiac muscle
Arrythmogenicdysplasia Right
VentricularCardiomyopathy/
Dysplasia 1)Autosomal dominant
mutationof Plakophilin-2(PKP-2) gene
2)Abnormalities indesmosomes causing
detachment and myocyteapoptosis and fibrofatty
replacement
Left Ventricularnoncompaction1)Result from arrest ofnormal embryogenesis2)Presence of multipledeep trabeculations orsinusoids that form in
the myocardium
Cardiac
catheterization
1). Left ventricular
dilatation anddysfunction2). Elevated left and
open right sided filling pressures
3).Diminished cardiacoutput
1). Normal or mildlyreduced systolicfunction
2). Elevated left- andright-sided filling
pressures
1). Vigorous systolic
function2). Dynamic leftventricular outflow
obstruction3). Elevated left- and
right-sided filling pressures
Etiology and Pathogenesis
The major cause of dilated cardiomyopathy is myocardial damage due to prolonged or
continuous unknown infection, metabolic problems or exposure to toxic agents. On the otherhand, about one third of these patients have familial forms of dilated cardiomyopathy most
commonly caused by mutations in genes encoding for sarcomeric proteins of the heart5. As a
result, these abnormal proteins cause contractile dysfunction by impairing the production and/ortransmission of force of heart pump. Multiple etiologies are related to the development of dilated
cardiomyopathy and they can be seen as listed below:
Figure 2
7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 5/9
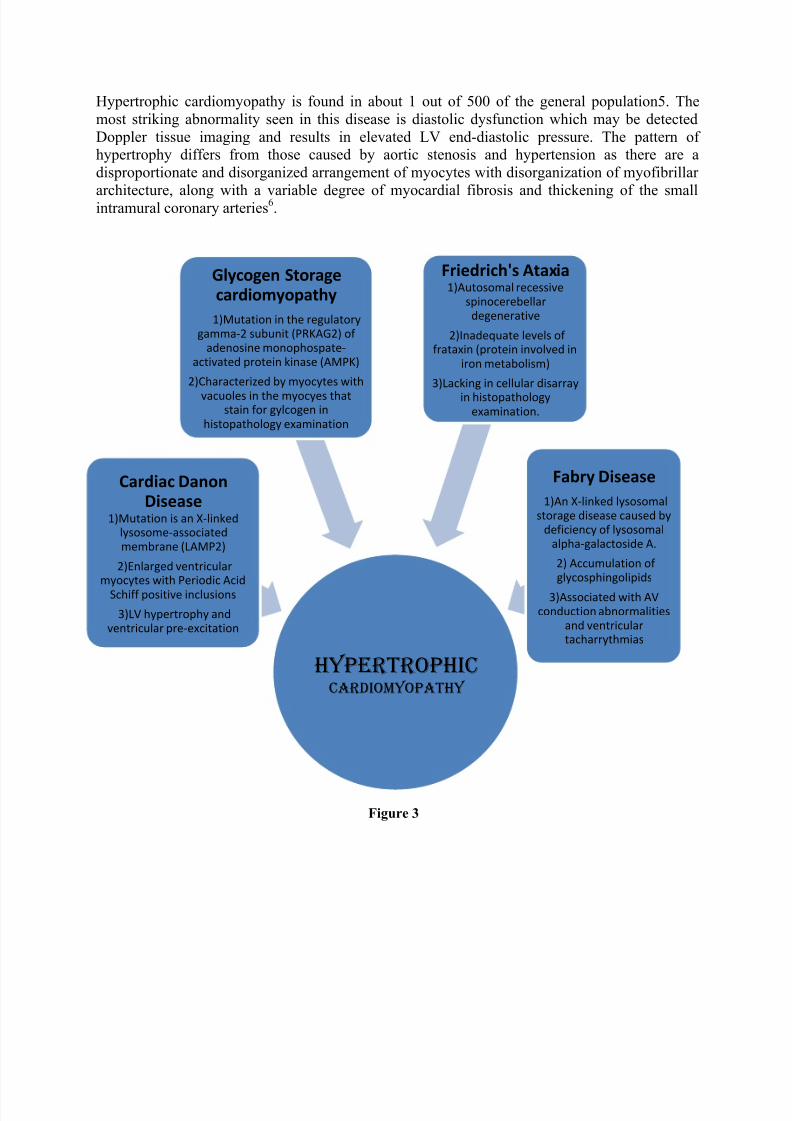
Hypertrophic Cardiomyopathy
Cardiac DanonDisease
1)Mutation is an X-linkedlysosome-associatedmembrane (LAMP2)
2)Enlarged ventricularmyocytes with Periodic Acid
Schiff positive inclusions
3)LV hypertrophy andventricular pre-excitation
Friedrich's Ataxia1)Autosomal recessive
spinocerebellardegenerative
2)Inadequate levels offrataxin (protein involved in
iron metabolism)
3)Lacking in cellular disarray
in histopathologyexamination.
Fabry Disease
1)An X-linked lysosomalstorage disease caused by
deficiency of lysosomalalpha-galactoside A.
2) Accumulation ofglycosphingolipids
3)Associated with AVconduction abnormalities
and ventriculartacharrythmias
Glycogen Storagecardiomyopathy
1)Mutation in the regulatorygamma-2 subunit (PRKAG2) of
adenosine monophospate-activated protein kinase (AMPK)
2)Characterized by myocytes with
vacuoles in the myocyes thatstain for gylcogen in
histopathology examination
Hypertrophic cardiomyopathy is found in about 1 out of 500 of the general population5. The
most striking abnormality seen in this disease is diastolic dysfunction which may be detected
Doppler tissue imaging and results in elevated LV end-diastolic pressure. The pattern ofhypertrophy differs from those caused by aortic stenosis and hypertension as there are a
disproportionate and disorganized arrangement of myocytes with disorganization of myofibrillar
architecture, along with a variable degree of myocardial fibrosis and thickening of the smallintramural coronary arteries6.
Figure 3
7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 6/9
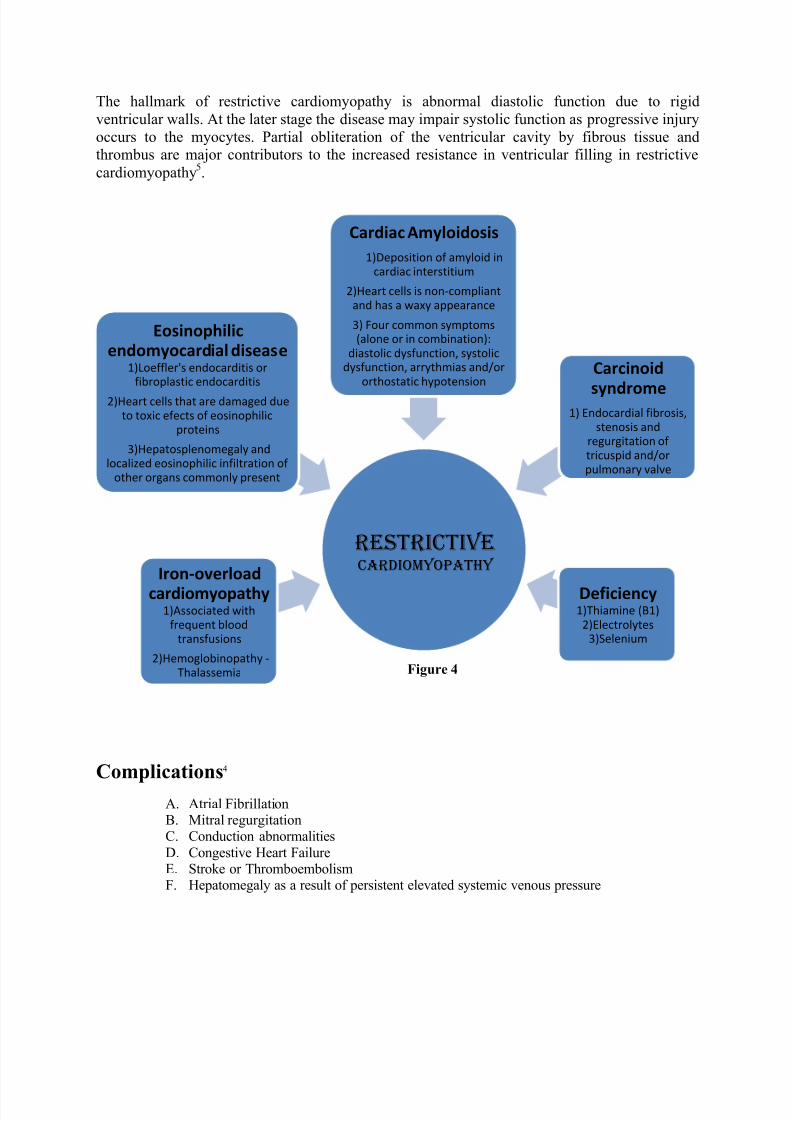
The hallmark of restrictive cardiomyopathy is abnormal diastolic function due to rigid
ventricular walls. At the later stage the disease may impair systolic function as progressive injury
occurs to the myocytes. Partial obliteration of the ventricular cavity by fibrous tissue andthrombus are major contributors to the increased resistance in ventricular filling in restrictive
cardiomyopathy5.
Complications4
A. Atrial FibrillationB. Mitral regurgitationC. Conduction abnormalities
D. Congestive Heart FailureE. Stroke or ThromboembolismF. Hepatomegaly as a result of persistent elevated systemic venous pressure
restrictiveCardiomyopathy
Eosinophilicendomyocardial disease
1)Loeffler's endocarditis orfibroplastic endocarditis
2)Heart cells that are damaged dueto toxic efects of eosinophilic
proteins
3)Hepatosplenomegaly andlocalized eosinophilic infiltration of
other organs commonly present
Iron-overload
cardiomyopathy1)Associated with
frequent bloodtransfusions
2)Hemoglobinopathy -Thalassemia
Cardiac Amyloidosis
1)Deposition of amyloid incardiac interstitium
2)Heart cells is non-compliantand has a waxy appearance
3) Four common symptoms(alone or in combination):
diastolic dysfunction, systolicdysfunction, arrythmias and/or
orthostatic hypotensionCarcinoid
syndrome1) Endocardial fibrosis,
stenosis andregurgitation oftricuspid and/orpulmonary valve
Deficiency 1)Thiamine (B1)
2)Electrolytes3)Selenium
Figure 4

7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 7/9
Management
In general, all patients suffering from congestive heart failure should be treated promptly. It is importantto treat the fluid retention with diuretics before initiating an ACE inhibitor or ARB (if patient is intolerant
of ACE-inhibitor)6. Beta-blockers should then be started after the ACE inhibitor has been uptitrated. If
the patient remains asymptomatic, an aldosterone antagonist, ARB or digoxin may be added as ―tripletherapy‖. Anticoagulation and antiplatelet therapy may be considered in patients with depressed left
ventricular function because these patients are at an increased risk of thromboembolism or stroke6.
Preferably, warfarin is prescribed in cases of heart failure, chronic or paroxysmal atrial fibrillation, or in patients who have a history of pulmonary emboli, including stroke and transient ischemic attack. Lowdose aspirin (75-81mg) is used for the prevention of myocardial infarction and death.
Heart Failure treatment during pregnancy
In peripartum cardiomyopathy, treatment are focused on halting the sequel of heart failure. Pregnant
patients are prescribed medications such as hydralazine and nitrates which can reduce afterload along
with digoxin, beta-blockers and loop diuretics6. The use of angiotensin-converting enzyme and
angiotensin receptor blocker are contraindicated in pregnancy because they have been associated withfetopathy such as fetal hypotension, oligohydramnios-anuria and renal tubular dysplasia 7,8. Pregnant
women should also receive anticoagulation therapy as the risk of thromboembolic complications increases
due to higher concentrations of factors II, VII, VIII, X and plasma fibrinogen. The therapy are given and
should be continued up to 6 weeks postpartum or until a normal left ventricular function is confirmed 3.
Warfarin is not used in pregnancy as they can cause spontaneous cerebral hemorrhage when used in the
second and third trimester of pregnancy9,10, however unfractionated or low-molecular-weight heparin can
safe to use in pregnancy.
Heart Failure treatment postpartum
Treatment for postpartum cardiomyopathy is identical to those who are nonpregnant and includes the use
of ACE inhibitors and ARB. Dosage is one-hald the maximum antihypertensive dose. Selective and non-selective beta-blockers are recommended for peripartum cardiomyopathy6 as they have been proven toimprove symptoms, ejection fraction and survival rates. Dosage goal for non-selective beta-blockers such
as carvedilol is 25mg twice a day up to 50mg twice a day for larger patients. Selective beta-blockers suchas metaprolol succinate 100mg can also be given once a day. Diuretics may be used for symptomatic
relief of edema and the use of sprinolactone or digoxin are used in patients who have New York HeartAssociation class III or IV symptoms.
Other proposed therapies include calcium channel antagonists11
, statins12
, monoclonal antibodies13
,
interferon beta14,immunoadsorption15, therapeutic apheresis16, and cardiomyoplasty17.
Prognosis
Prognosis of patients with peripartum cardiomyopathy are based on T-Troponin levels, ORS duration and
ejection fraction. A troponin-T concentration of more than 0.04ng/mL are predictive of persistent left
ventricular dysfunction, a QRS duration of 120ms or more is a risk factor for death and sudden death 18,

7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 8/9
while ejection fractions of less than 30% are more indicative of poor left ventricle recovery. Other factors
associated with the lack or recovery include an initial left ventricular end-diastolic dimension of greater
than 5.6cm, left ventricular thrombus and African American race6.
A study on peripartum cardiomyopathy by Elkayam et al19 reported a two year follow-up that out of 100
patients who had the disease, 54 of them had recovered normal left ventricular fucntion at the end of 2
years, nine people that died and four of them which recieved a heart transplant.
Prevention
Since peripartum cardiomyopathy is a rare form of idiopathic primary myocardial disease with a yet
indefinite etiologic cause, prevention are mainly targeted at halting more damage to the dilated heart and
these includes medications such as diuretics, beta-blockers ARB and ACE inhibitors. In patients whose
left ventricular function has fully recovered, subsequent pregnancy still carries a low risk for developing
another sequel of cardiomyopathy20
. On the other hand, if left ventricular function has not recovered, the
risk of worsening heart failure and long-term systolic dysfunction are high and subsequent pregnancy
should be avoided.
References
1. Epidemiology of cardiomyopathy. Clinical Key Elsevier 2012. Retrieved 17 January 2013
2. Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies:a positionstatement from the European Society Of Cardiology Working Group on Myocardial andPericardial Diseases. European Heart Journal 2008; 29:270 – 276
3. Ramaraj R, Sorell VL. Peripartum cardiomyopathy: disease causes, diagnosis and treatment.Cleveland Clinic Journal of Medicine 2009;76 (5)
4. Baughman KL et al: Braunwald‘s Heart Disease. Elsevier, Philadelphia, Pennsylvania, 2005
5. Wynne J, Braunwald E: Cardiomyopathy and Myocarditis. Harrison‘s Cardiovascular Medicine.McGraw-Hill, 2010.
6. Amos AM, Jaber WA, Russell SD. Improved outcomes in peripartum cardiomyopathy withcontemporary. American Heart Journal 2006; 152:509 – 513.
7. Pearson GD, Veille JC, Rahimtoola S, et al. Peripartum cardiomyopathy: National Heart, Lung,and Blood Institute and Office of Rare Diseases (National Institutes of Health) workshop
recommendations and review. JAMA 2000; 283:1183 – 1188.
8. Andrade SE, Raebel MA, Brown J, et al. Outpatient use of cardiovascular drugs during pregnancy. Pharmacologic Epidemiology Drug Safety 2008; 17:240 – 247.
9. Ray JG, Vermeulen MJ, Koren G. Taking ACE inhibitors during early pregnancy: is it safe?Canadian Family Physician 2007; 53:1439 – 1440.

7/18/2019 Review Article Cardiomyopathy
http://slidepdf.com/reader/full/review-article-cardiomyopathy 9/9
10. Clark NP, Delate T, Witt DM, Parker S, McDuffie R. A descriptive evaluation of unfractionated
heparin use during pregnancy. Journal of Thrombolysis 2008
11. Narin C, Reyhanoglu H, Tulek B, et al. Comparison of different dose regimens of enoxaparin indeep vein thrombosis therapy in pregnancy. Advanced Therapy 2008; 25:585 – 594.
12. Yuan Z, Kishimoto C, Shioji K. Beneficial effects of low-dose benidipine in acute autoimmunemyocarditis: suppressive effects on inflammatory cytokines and inducible nitric oxide synthase.Circulation Journal 2003; 67:545 – 550.
13. Li WM, Liu W, Gao C, Zhou BG. Immunoregulatory effects of atorvastatin on experimental
autoimmune myocarditis in Lewis rats. Immunology Cell Biology 2006; 84:274 – 280.
14. Yuan HT, Liao YH, Wang Z, et al. Prevention of myosin-induced autoimmune myocarditis inmice by anti-L3T4 monoclonal antibody. Canadian Journal of Physiology and Pharmacology
2003; 81:84 – 88.
15. Kuhl U, Pauschinger M, Schwimmbeck PL, et al. Interferon-beta treatment eliminatescardiotropic viruses and improves left ventricular function in patients with myocardial persistenceof viral genomes and left ventricular dysfunction. Circulation 2003; 107:2793 – 2798.
16. Felix SB, Staudt A. Non-specific immunoadsorption in patients with dilated cardiomyopathy:mechanisms and clinical effects. International Journal of Cardiology 2006; 112:30 – 33.
17. Bosch T. Therapeutic apheresis — state of the art in the year 2005. Therapeutic Apheresis and
Dialysis 2005; 9:459 – 468.
18. Liu Z, Yuan J, Yanagawa B, Qiu D, McManus BM, Yang D. Coxsackie virus induced
myocarditis: new trends in treatment. Expert Review of Anti Infective Therapy 2005; 3:641 – 650.
19. Elkayam U, Akhter MW, Singh H, et al. Pregnancy-associated cardiomyopathy:clinicalcharacteristics and a comparison between early and late presentation. Circulation 2005;111:2050 – 2055.
20. Fett JD, Christie LG, Murphy JG. Brief communication: Outcomes of subsequent pregnancy after peripartum cardiomyopathy: a case series from Haiti. Annals of Internal Medicine 2006; 145:30 – 34.
Figures:
1. Figure 1. Revised by Malcolm J. ―Types of Cardiomyopathies". The Merck Manual Home HealthHandbook 2008





























