Embed Size (px)
Citation preview

708 www.thelancet.com/gastrohep Vol 3 October 2018
Review
Emerging non-invasive approaches for diagnosis and monitoring of portal hypertensionXiaolong Qi*†, Annalisa Berzigotti*, Andres Cardenas, Shiv Kumar Sarin†
Clinically significant portal hypertension is associated with an increased risk of developing gastro-oesophageal varices and hepatic decompensation. Hepatic venous pressure gradient measurement and oesophagogastroduodenoscopy are the gold-standard methods for assessing clinically significant portal hypertension (hepatic venous pressure gradient ≥10 mm Hg) and gastro-oesophageal varices, respectively. However, invasiveness, cost, and feasibility limit their widespread use, especially if repeated and serial evaluations are required to assess the efficacy of pharmacotherapy. Although new techniques for non-invasive portal pressure measurement have been pursued for many decades, only recently have new tools been assessed and validated for larger clinical application. This Review focuses on the recent advances in non-invasive approaches for the diagnosis and serial monitoring of portal hypertension and varices for clinical practice.
IntroductionDevelopment of portal hypertension in cirrhosis is associated with hyperdynamic circulation and serious clinical consequences, such as variceal haemorrhage, ascites, hepatic encephalopathy, and renal dys-function.1–3 Grading of portal hypertension in cirrhosis, based on the level of portal pressure, is helpful to stratify patients who are more likely than others to have a worse clinical course. According to clinical practice guidelines, measure ment of portal pressure is not only important for prognosis, but is also pivotal for clinical management.1–3
The most reliable method for assessment of portal pressure in chronic liver disease is the measurement of the hepatic venous pressure gradient (HVPG) through hepatic vein catheterisation (via transjugular, trans-femoral, or transbrachial routes; figure 1).4 With this method, patients with compensated cirrhosis can be stratified into those with subclinical portal hypertension (HVPG >5 mm Hg but <10 mm Hg) or clinically significant portal hypertension (HVPG ≥10 mm Hg).1,2 When clinically significant portal hypertension develops, complications such as varices (figure 1) appear and patients are at a high risk of hepatic decompen-sation.1,3 In the Baveno VI consensus conference held in 2015,2 non-invasive tests were accepted as a standard of care to reduce the number of unnecessary endoscopies. According to the Baveno VI recom mendations, the combination of liver stiffness of less than 20 kPa measured by transient elastography and a platelet count of more than 150 000 per µL was recommended to exclude patients with cirrhosis with high-risk varices or varices needing treatment, and to safely circumvent oesophagogastroduodenoscopy.2
Whether patients with portal hypertension can be reliably identified by non-invasive methods, and if hepatic vein catheterisation and oesophagogastro-duoden o scopy can be avoided in some patients, is an area of intense investigation.2 Whether these approaches can also be used to monitor the efficacy of medical therapy is also unclear. Treatment efficacy is established
by pre-therapy and post-therapy HVPG measurement;1–3 patients who achieve an HVPG reduction of at least 20% from baseline or achieve a portal pressure of 12 mm Hg or less on non-selective β-blockers are at reduced risk of variceal haemorrhage and have improved clinical outcomes.1,2 Given these observations, several studies have suggested that simple, non-invasive methods can be used for the diagnosis and monitoring of portal hypertension in patients with cirrhosis. However, there are many challenges to inte grating non-invasive screening methods into clinical practice, and more data are needed to establish consensus on standard practice and implementation. Challenges include the high heterogeneity across published studies in terms of the methods used and the underlying causes of disease in the populations studied; technical challenges in applying these approaches to patients with obesity and other underlying comorbidities; and uncertainty regarding the effect of medical therapy on the output of non-invasive screening methods.
In this Review, we focus on emerging non-invasive approaches in the diagnosis of clinically significant portal hypertension and gastro-oesophageal varices (summarised in appendix) and discuss the role of these approaches in clinical practice for monitoring changes in portal pressure and the develop ment and regression of clinically significant portal hypertension and varices (summarised in figure 2). The limitations, gaps in knowledge, and opportunities for future research are also discussed.
Emerging non-invasive diagnostic approaches for portal hypertensionNon-invasive methods for the diagnosis of clinically relevant portal hypertension include serum tests, anatomical imaging markers, and physical surrogates of tissue properties reflective of hypertension.1,2 For example, a low platelet count alone could indicate the presence of portal hypertension, but with limited accuracy.1 Imaging evidence of portosystemic collateral circulation or a hepatofugal flow within the portal
Lancet Gastroenterol Hepatol 2018; 3: 708–19
*Joint first authors
†Joint senior authors
CHESS Group, Hepatic Hemodynamic Lab, Institute of Hepatology, Nanfang Hospital,
Southern Medical University, Guangzhou, China
(Prof X Qi MD); CHESS Frontier Center, Lanzhou University,
Lanzhou, China (Prof X Qi); Hepatology Group, Swiss Liver
Center, University Clinic for Visceral Surgery and Medicine, Inselspital, University of Bern,
Bern, Switzerland (A Berzigotti MD); GI/Liver Unit,
Institute of Digestive Diseases and Metabolism, Hospital
Clinic, University of Barcelona, Barcelona, Spain
(A Cardenas MD); and Department of Hepatology, Institute of Liver and Biliary
Sciences, New Delhi, India (S K Sarin MD)
Correspondence to: Prof Xiaolong Qi, CHESS Group,
Hepatic Hemodynamic Lab, Institute of Hepatology,
Nanfang Hospital, Southern Medical University, Guangzhou
510515, China [email protected]
See Online for appendix

www.thelancet.com/gastrohep Vol 3 October 2018 709
Review
system on Doppler ultrasound, CT, or MRI are considered adequate to diagnose clinically significant portal hypertension.1,2 Liver stiffness by transient elastography, alone or combined with platelet count and spleen size, has shown excellent diagnostic performance
to identify clinically significant portal hypertension, and the combination of liver stiffness and platelet count is recommended to rule out high-risk varices in patients with compensated cirrhosis, according to the Baveno VI consensus.2 Several papers subsequently validated these
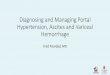
Figure 1: Gold-standard approaches for diagnosis and monitoring of portal hypertensionThe gold standard for assessing clinically significant portal hypertension (left image) is hepatic venous pressure gradient measurement and for gastro-oesophageal varices (right image) is oesophagogastroduodenoscopy. A balloon catheter is required for a reliable assessment of hepatic venous pressure gradient.
Balloon catheter Hepatic vein
Cirrhotic liver
Portalvein
Stomach
Gastro-oesophageal varices
Oesophagogastroduodenoscopy(gold standard for gastro-oesophageal varices)
Hepatic venous pressure gradient(gold standard for clinically significant
portal hypertension)
Figure 2: Non-invasive approaches for diagnosis and monitoring of portal hypertension and underlying liver physiologyMethods aim to detect changes occurring during cirrhosis and portal hypertension development (in liver, spleen, intra-hepatic and extra-hepatic vessels), properties of the liver and spleen parenchyma (stiffness; indocyanine green [ICG] and contrast dye clearance), or circulating proteins associated with fibrogenesis and portal hypertension. 2D-SWE=two-dimensional real-time shear wave elastography. ELF=enhanced liver fibrosis. ICG-r15=indocyanine green 15 min retention test. MRE=magnetic resonance elastography. pSWE=point shear wave elastography. Pro-C5=the formation marker procollagen type V. SHAPE=subharmonic aided pressure estimation. TE=transient elastography. vWF-Ag=von Willebrand factor antigen.
Changes in liver size and shapeUltrasound, CT, MR: liver size, volume, lobe ratio,morphologyMR: T1 relaxation time, relative liver enhancement
Increased liver stiffness due to increase in fibrosisElastography: TE, pSWE, 2D-SWE, MRE
Intrahepatic microcirculation derangement andintrahepatic shuntingContrast-enhanced ultrasonography: hepaticmicrovascular network connectivity, intrahepatictransit time, SHAPE
Increased spleen size and stiffness due tocongestionDoppler ultrasound: splenic arterial resistive indexElastography: TE, pSWE, 2D-SWE, MREUltrasound, CT, MR: spleen diameter, volume
Dilatation of portal vein system, compensatoryvasodilation of hepatic artery and splenic artery, formation of portosystemic collateralsDoppler ultrasound: blood velocity of portal veinand splenic artery, portovascular resistance,splenoportal index, hepatic veins flow patternUltrasound, CT, MR: portal vein system diameter,presence and type of portosystemic collaterals, hepatic arterial fraction, azygos blood flow
Decreased splenic clearance of iodine contrast dyeCT: splenic clearance
Decreased capacity of ICG clearance Serum biomarker: ICG-r15
Increased release and circulating amount ofproteins associated with intrahepaticendothelial dysfunction and remodelling ofextracellular matrixSerum biomarker: vWF-Ag, Pro-C5, osteopontin,CD163, ELF, fibrotic markers
Hepatic vein
Cirrhotic liver
Portalvein
Splenic vein
Spleen

710 www.thelancet.com/gastrohep Vol 3 October 2018
Review
recommendations, and they have also been endorsed by the American Association for the Study of Liver Diseases in the 2016 practice guidance on portal hypertension.1 Spleen stiffness, also measured by transient elastography, is another promising parameter but has several technical concerns.1 Novel ultrasound elastography techniques, such as point shear wave elastography and two-dimensional shear wave elasto-graphy, that enable visualisation of the area of stiffness in the liver or spleen are now available.1,2 Magnetic resonance elastography is another alternative for measuring liver and spleen stiffness; because the entire liver and spleen are scanned, this technique provides a measurement of stiffness in larger areas, making it theoretically superior to ultrasound-based elasto-graphical methods. However, evidence is scarce as to whether this method can be used alone to diagnose clinically significant portal hypertension.1
Laboratory tests and serum markersSeveral novel laboratory parameters have been tested for detection of clinically significant portal hypertension in patients with cirrhosis, but their clinical utility remains uncertain. A recent study showed that the ratio of von Willebrand factor antigen concentration to platelet count (called the VITRO score) was useful for the detection of clinically significant portal hypertension, with an area under the receiver operating characteristic curve (AUROC) of 0∙86.5 In another study, measurement of soluble CD163 in serum, an indicator of active hepatic inflammation, combined with the Enhanced Liver Fibrosis score (comprising hyaluronic acid, tissue inhibitor of metalloproteinase-1, and procollagen-III aminopeptide) was also successful in identifying patients with cirrhosis with clinically significant portal hypertension, with an AUROC of 0·91.6 The indocyanine green 15 min retention test, which measures liver parenchymal function and hepatic blood flow based on clearance of an injected dye, has been validated as a potential screening tool for clinically significant portal hypertension, with excellent sensitivity in the three Child-Pugh classes, particularly Child-Pugh class A (AUROC 0∙7776).7 However, this test is more complex than a simple blood test, requiring administration of dye, and its generalisability is uncertain given that most of the patients tested in the study had alcohol-related liver disease.7 Since clinically significant portal hypertension is invariably present in patients with decompensated cirrhosis, studies aimed at evaluating the diagnostic value of these tests should be done in patients with fully compensated liver disease.
Indices of liver fibrosis (including the aspartate amino transferase-to-alanine aminotransferase ratio, aspartate aminotransferase-to-platelet ratio index, fibrosis index, Fibrosis-4 [FIB-4], Forns’ index, Kings’ score, and the Lok index) are used to evaluate the presence and grade of fibrosis and to diagnose cirrhosis.
These approaches were assessed in one study to evaluate the presence of clinically significant portal hypertension, but all had limited accuracy.8 In a cohort of patients with alcoholic cirrhosis, measurement of the collagen formation marker procollagen type V identified clinically significant portal hypertension with a sensitivity of 79·7% and a specificity of 64·0%, with a cutoff of 330 ng/mL.9 However, the utility of this biomarker in patients with cirrhosis due to other causes remains to be assessed. Osteopontin levels have also been shown to correlate with both liver fibrosis and portal hypertension.10 Overall, non-invasive and readily available blood parameters show modest clinical utility, and many are still in the exploratory phases of testing and are not yet ready to enter clinical practice.
Doppler ultrasound and contrast-enhanced ultrasoundDoppler ultrasound studies are especially useful in evaluating the patency of and blood flow through portal and splanchnic beds, and for visualisation of morphological abnormalities associated with portal hypertension (eg, dilatation of the portal vein system, splenomegaly, and presence of portosystemic collaterals). The damping index, which measures alterations in the Doppler hepatic vein waveform, reflects clinically significant portal hypertension and correlates with HVPG grade and variations in HVPG in response to therapy.11 A technique for measuring splenic arterial resistance by combining the splenic Doppler pulsatility index with measurement of portal blood flow proved to be a reliable measure of splenic and portal venous resistance, and showed a stronger correlation with HVPG than other Doppler parameters.12 In one study, this technique (deemed the splenic arterial resistive index) showed a higher diagnostic performance compared with liver stiffness measurement by shear wave elastography.13 However, spleen stiffness, which might better reflect portal hypertension, was not measured in this study. Taken together, the available data are not sufficiently robust to recommend any of the existing Doppler measurements as a reliable surrogate of HVPG.14,15
Contrast-enhanced ultrasound techniques have recently provided notable results. In a pilot study, use of subharmonic aided pressure estimation using perflubutane microbubbles (Sonazoid, GE Healthcare, Oslo, Norway) showed good agreement with HVPG,16 and this method is being validated in a large multicentre study in the USA (NCT02489045; table). Another pilot study of 15 patients used machine learning to evaluate hepatic microvascular network connectivity using dynamic contrast-enhanced ultrasound with continuous infusion of sulphur hexafluoride micro-bubbles (SonoVue, Bracco, Milan, Italy), showing an inverse correlation between the resulting clustering coefficient and HVPG.17 However, this calculation depended on the ability to acquire data of optimal

www.thelancet.com/gastrohep Vol 3 October 2018 711
Review
quality, which contributed to the small size of the study cohort and limits widespread applicability of the technique. This method is being tested in the CLEVER study, a multicentre study of patients with chronic liver disease (FP7-IAPP-GA-2013-612273-CLEVER), and results from the first 152 consecutive patients enrolled showed a poor technical success rate (56%) but an excellent correlation between the portal pressure estimation and HVPG (r=0∙914 in training set and r=0∙843 in validation set; both p<0∙0001).18 The method was robust enough to identify not only patients with clinically significant portal hypertension but also those with an HVPG of more than 16 mm Hg. Because this HVPG threshold is associated with an increased risk of mortality,4 contrast-enhanced ultrasound could represent a novel tool for risk stratification in compensated cirrhosis beyond the simpler concept of presence or absence of clinically significant portal hypertension.
Ultrasound elastographyLiver stiffness reflects liver fibrosis, which is the main component of intrahepatic resistance and portal pressure (Δ portal pressure=resistance × blood flow). A meta-analysis of 11 studies showed that liver stiffness measured using transient elastography correlated well with HVPG (r=0·783 [95% CI 0·737–0·823]) and was accurate for detection of clinically significant portal
hypertension with a sensitivity of 87·5% and specificity of 85·3%.19 Studies that used a low cutoff value of 13·6–18·0 kPa was proposed to decrease false negative results and increase sensitivity compared to those that used a cutoff of 21–25 kPa;19 however, the performance of transient elastography was adversely affected by obesity, narrow intercostal spaces, and the presence of ascites. Additionally, the diagnostic accuracy of liver stiffness for portal hypertension (and that of point shear wave elastography and two-dimensional real-time shear wave elastography) is limited in patients with active alcohol use, recent food consumption (eg, within 2 h), flares of aminotransferases, cholestasis, or con-gestive heart failure, all factors known to increase liver stiffness.20 Additionally, the correlation between liver stiffness and HVPG decreases markedly at HVPG values over 10–12 mm Hg,20 consistent with the concept that portal hypertension is aggravated in part by extrahepatic factors, such as splanchnic vasodilation, hyperdynamic circulation, and portosystemic col late-rals, which do not likewise affect liver stiffness.1,20 The implication of this finding for clinical practice is that liver stiffness might correctly identify patients with clinically significant portal hypertension, but it cannot be used for risk stratification.
Among point shear wave elastography techniques, Virtual Touch tissue quantification, commonly defined
Study lead author and country ClinicalTrials.gov number
For portal hypertension with hepatic venous pressure gradient as reference
MR and MRE Bendtsen F, Denmark NCT03443934
Multiparametric MR Taouli B, USA NCT03436550
Acoustic radiation force impulse Zizer E, Germany NCT03315767
Haemodynamics-based mathematical model Jiang W, China NCT03277651
Radiomics-based hepatic venous pressure gradient Qi X, China NCT03138915
Quantitative MR Aithal GP, UK NCT03114813
Hepatic vein waveform Ali Shah SH, Pakistan NCT02975323
Virtual imaging-hepatic venous pressure gradient Qi X, China NCT02842697
Liver stiffness, spleen stiffness by two-dimensional real-time shear wave elastography
Grgurevic I, Croatia NCT02653846
Surrogate markers (ICG test, liver stiffness, spleen stiffness) Garcia-Tsao G, USA NCT02508298
Subharmonic aided pressure estimation algorithm Forsberg F, USA NCT0248904513C-methacetin breath test García-Pagán JC, Spain NCT0214377813C-methacetin breath test Ashkenazi E, Israel NCT01851252
Acoustic radiation force impulse Garcia-Tsao G, USA NCT01644656
For gastro-oesophageal varices with oesophagogastroduodenoscopy as reference
Radiomics-based surrogate of endoscopy Qi X, China NCT03373123
Serum ammonia El-Kalla F, Egypt NCT03212872
Biochemical data-based score Guo X, China NCT02593799
Spleen stiffness by transient elastography Davide FESTI, Italy NCT02180113
Liver and spleen stiffness measurement by transient elastography Wong GL, China NCT02024347
MR=magnetic resonance. MRE=magnetic resonance elastography. ICG=indocyanine green.
Table: Trials of non-invasive diagnosis and monitoring of portal hypertension

712 www.thelancet.com/gastrohep Vol 3 October 2018
Review
as acoustic radiation force impulse (Siemens, Erlangen, Germany), seems to be a good predictor of clinically significant portal hypertension with a cutoff of 2·17 m/s.21 Additionally, measurement of liver stiffness by super-sonic shear imaging is increasingly used. A meta-analysis that included four studies found that liver stiffness measured by this technique showed promising performance for diagnosis of clinically significant portal hypertension, with an AUROC of 0∙84, sensitivity of 79%, and specificity of 82%.22 These techniques have also improved the measurement of liver stiffness in patients with obesity and ascites, although further clinical validation and reliable, universally agreed upon criteria for measurement are needed. The reliability of two-dimensional real-time shear wave elastography measurement was highlighted in two studies which proposed that low measurement variability with a larger region of interest and optimal depths of measurement could contribute to more reliable results.23,24
Spleen stiffness measured by elastographical methods is also a promising predictor of portal hypertension. In a meta-analysis of nine studies, spleen stiffness showed good correlation with HVPG (r=0·72 [95% CI 0∙63–0∙80]) and ability to discriminate clinically significant portal hypertension with an AUROC of 0·92, sensitivity of 88%, and specificity of 84%.25 However, spleen stiffness can be falsely increased by multiple pathological changes related to portal hypertension, such as blood congestion, increased resistance to splenic vein outflow, and inc reased angiogenesis and fibrogenesis.20 Spleen stiffness seems to have a better diagnostic performance than liver stiffness for identifying portal hypertension in the context of cirrhosis,26 which has also been shown by use of point shear wave elastography, but not with transient elastography or two-dimensional real-time shear wave elastography.24,27,28
Stepwise algorithms based on liver stiffness and spleen stiffness measured by two-dimensional real-time shear wave elastography were proposed to rule-in and rule-out clinically significant portal hypertension.29,30 Using a combination of these two algorithms, studies showed that invasive HVPG measurement could be safely avoided in 87% of patients; however, more patients were misclassified in an external validation.29,30 This poor performance might be explained by inclusion of a higher proportion of patients with clinically significant portal hypertension and with different underlying causes of disease in the validation cohort. For studies done with transient elastography, it should be noted that spleen stiffness measurement has a suboptimal technical success rate because the probes used are designed for the liver. Technical improvements in transient elastography devices (eg, a dedicated probe for measuring spleen stiffness) will soon be available for clinical evaluation. This technique might find special use for patients with non-cirrhotic forms of portal hypertension, who, by definition, have normal or near-normal liver stiffness.
MRIHaemodynamic parameters measured with MRI seem to correlate with HVPG. In one study, the azygos flow measured by two-dimensional cine phase-contrast MRI correlated with HVPG (AUROC 0∙96 [95% CI 0∙91–1∙00]) in patients with cirrhosis related to hepatitis C virus (HCV) infection and alcohol use.31 In a multicentre study, a predictive model, based on MRI measured longitudinal relaxation time (T1) and splenic artery velocity, significantly correlated with HVPG (both p<0·001) and provided a good prediction of HVPG in a validation cohort.32 Hepatic arterial fraction estimates in healthy volunteers suffer from error propagation from multivessel flow measurements. However, these measurements are less prone to non-physiological results in patients with chronic liver disease, in whom hepatic arterial flows tend to be higher. In a pilot study, caval subtraction phase-contrast MRI measurement of hepatic arterial fraction appeared to be a valuable haemodynamic marker when tested against an invasive microsphere standard in a rodent model, showing a positive correlation with HVPG.33
Shear wave velocity by magnetic resonance elasto-graphy, a measure of liver stiffness, was independently associated with HVPG in a cohort of 23 patients (R²=0∙377, p=0∙02).34 However, these imaging techniques remain difficult to implement in clinical practice because of the absence of validation in larger cohorts, the requirement for specialised equipment, high cost, and issues around patient tolerance. In our opinion, the use of these imaging techniques in the near future will be restricted to further clinical studies aimed at their optimisation, rather than entering into clinical use.
Combination approachesApproaches based on the combination of unrelated non-invasive tests have been proposed.1,20 Examples include platelet count-to-spleen ratio, liver stiffness measurement and spleen diameter-to-platelet ratio score, portal hypertension score, and the Baveno criteria for portal hypertension and varices. Combining non-invasive tests increases accuracy and reduces indeterminate findings. In the ANTICIPATE study,35 investigators set out to devise point-of-care risk assessment in 518 patients with advanced chronic liver disease using various non-invasive tests.35 The study showed high discriminative value of the proposed nomograms (which included the combination of liver stiffness and platelet count, liver stiffness measurement and spleen diameter-to-platelet ratio score, and platelet count-to-spleen ratio) for identi fication of clinically significant portal hypertension.35 Calibration of these models was also excellent, suggesting the potential for these approaches to be applied in practice and to facilitate individualised medical care.

www.thelancet.com/gastrohep Vol 3 October 2018 713
Review
Emerging approaches for the diagnosis of gastro-oesophageal varicesTreatment with non-selective β-blockers for primary prophylaxis of variceal haemorrhage in patients with compensated cirrhosis is indicated in those with large varices, with or without red signs, or in those with Child-Pugh class C cirrhosis and small varices.1,2 Oesophagogastroduodenoscopy is the gold-standard diagnostic test for identifying the presence and grade of gastro-oesophageal varices (figure 1). However, it has some drawbacks such as invasiveness, cost, patient discomfort, and inter-observer variability.1,3 An HVPG of 10 mm Hg or more is considered the threshold for the formation of varices, and a value of 12 mm Hg or more is associated with increased risk of bleeding.1,3 Non-invasive tests have proven valuable for diagnosing varices that require treatment. In the 2015 Baveno VI consensus, the combination of liver stiffness of less than 20 kPa (by transient elastography), and platelet count of more than 150 000 per µL, is recommended for excluding high-risk varices or varices needing treatment, and for safely circumventing oesophago-gastro duodenoscopy in patients with compensated cirrhosis.2 With these cutoffs, approx imately 20–30% of oesophagogastroduo deno scopies can be avoided in these patients. The liver stiffness measurement and spleen diameter-to-platelet ratio score and spleen stiffness by acoustic radiation force impulse are promising in this setting, but further studies are required.1
Laboratory tests and serum markersThe indocyanine green 15 min retention test has been shown to predict an HVPG of 12 mm Hg or more.7 This test has been validated with a sensitivity varying from 90–92% in all three Child-Pugh classes.7 Concentrations of soluble CD163 were also significantly higher in patients with varices needing treatment, large varices, and those with high risk of variceal haemorrhage.36 Nevertheless, the diagnostic performance of soluble CD163 was modest for predicting the presence of varices needing treatment and risk of bleeding.36 A predictive score for large gastro-oesophageal varices based on platelet count, alpha fetoprotein, and prothrombin-international normalised ratio showed a good diagnostic performance in patients with HCV-related cirrhosis using an optimal cutoff of 0·27.37 However, it should be noted that none of these tests have been validated in patients in whom HCV has been successfully eradicated.
Ultrasound, Doppler ultrasound, and contrast-enhanced ultrasonographyIn a cohort of patients with hepatitis B virus (HBV) infection, a classification analysis model combining ultrasound qualitative signs and a spleen diameter of more than 162 mm detected gastro-oesophageal varices
with a sensitivity of 97∙5% and a specificity of 82∙6%.38 However, intra-observer and inter-observer variability should be considered when establishing the presence of ultrasound qualitative signs, as diagnostic accuracy of a combination of ultrasound signs was unsatisfactory in studies addressing compensated cirrhosis of different aetiologies.14,38
Portal hypertension is characterised by systemic and splanchnic haemodynamic changes.20 Parameters measured by Doppler ultrasound including haemo-dynamic liver index (portal vein diameter divided by mean portal vein velocity), portal vascular resistance ([0∙066 × splenic artery pulsatility index – 0∙044] × portal blood flow), and splenoportal index (spleen long diameter × spleen short diameter divided by mean portal vein velocity) seem to be useful in detecting gastro-oesophageal varices. These three Doppler indices showed statistical significance at specific cutoff values for identifying the presence of gastro-oesophageal varices in 60 patients with cirrhosis.39 In patients with HBV-related cirrhosis, intrahepatic transit time (the difference between hepatic vein arrival time and hepatic artery arrival time) measured by contrast-enhanced ultrasonography offered considerable diagnostic value for detecting the presence of gastro-oesophageal varices (AUROC 0∙883) and high-risk varices (AUROC 0∙915).40 Additionally, the intrahepatic transit time negatively correlated with the grade of gastro-oesophageal varices (R=–0·737, p<0·001).40 Use of other contrast-enhanced ultrasonography measures are also potentially useful for identifying the presence of varices. For example, in a study of 81 patients with cirrhosis, the thickness of double-layer mucosa and submucosa in the lower oesophagus (Tm), and the maximum anteroposterior diameter of the lower oesophagus showed excellent predictive performance; a Tm value of 7∙65 mm was identified as the cutoff value for diagnosing large oesophageal varices.41 Despite these promising data, none of the Doppler-related or contrast-enhanced ultrasonography-related parameters has fully entered clinical practice; due at least in part to the substantial inter-observer variability of Doppler parameter measurements.14,15
Ultrasound elastographyIn a recent meta-analysis of 15 studies, liver stiffness assessed by transient elastography identified the presence of gastro-oesophageal varices with a summary sensitivity of 84%, and moderate summary specificity of 62%.42 The pooled sensitivity and specificity for detecting large gastro-oesophageal varices was 78% and 76%, respectively.42 The superior sensitivity and moderate specificity of liver stiffness have also been shown in other studies,43,44 supporting this technique as a reliable screening tool. The reliability is particularly supported if liver stiffness is combined with other methods such as platelet count. However, this method

714 www.thelancet.com/gastrohep Vol 3 October 2018
Review
has not been rapidly taken up in clinical practice, mostly because of heterogeneity in the populations studied, leading to the identification of different cutoff values.42–45 The diagnostic performance of liver stiffness for varices and varices needing treatment is similar using point shear wave elastography and two-dimensional real-time shear wave elastography.21 In a meta-analysis of four studies, two-dimensional real-time shear wave elastography detected the presence of varices with a summary sensitivity of 80% and summary specificity of 80%.22 Data using point shear wave elastography and two-dimensional real-time shear wave elastography in this context are still scarce, and their use in practice is not universal. Spleen stiffness has been reported to have superior predictive accuracy compared with liver stiffness for detection of gastro-oesophageal varices in the setting of chronic liver disease.46 In a randomised controlled study of patients with cirrhosis,47 a novel screening strategy combining liver stiffness and spleen stiffness was superior to endoscopic screening (recommended by the Baveno VI criteria) for ruling out gastro-oesophageal varices.47 Still, these results need to be supported in larger studies.
CT and MRICross-sectional imaging methods like CT and MRI are widely used in patients with cirrhosis for several indications, and can provide images diagnostic of gastro-oesophageal varices. A meta-analysis of 17 studies showed that the summary sensitivity and specificity of CT for assessing the presence of varices of any size were 87% and 80%, respectively;48 and for high-risk gastro-oesophageal varices, the values were 87% and 88%.48 The accuracy of CT was also substantiated in another meta-analysis, which reported similar sensitivity and specificity values.49 However, different CT technologies might result in heterogeneity between studies.49 A prediction model based on radiological indices from CT was developed for oesophageal varices in patients with cirrhosis, showing good sensitivity (95%) but poor specificity (26%).50 In a small cohort of 21 patients with cirrhosis, splenic clearance assessed by CT perfusion imaging showed excellent performance for detecting an HVPG of 12 mm Hg or more (sensitivity 94%; specificity 100%).51 In a retrospective single-centre study, investigators used CT imaging features, including the size of the para-umbilical vein and spleen and the presence of ascites, to devise a simple prediction score.52 The weighted score showed an association with a first variceal haemorrhage and was validated in a prospective cohort, but data for its diagnostic performance were not reported.52
MRI-based parameters have also been assessed for predicting the presence of gastro-oesophageal varices. In a retrospective study of 178 patients with chronic liver disease, relative liver enhancement and portal vein hyperintensity on 20 min delayed T1-weighted gadoxetic
acid-enhanced MRI, were identified as independent predictors of an HVPG of 12 mm Hg or more.53 However, these data require validation. Spleen volume measured by routine MRI, and liver stiffness and spleen stiffness by magnetic resonance elastography, showed inde pendent associations with the presence of gastro-oesophageal varices, among which spleen stiffness was the most reliable for discriminating severe varices.54 In a cohort of patients with HBV, liver volume parameters were evaluated by MRI for predicting severity of gastro-oesophageal varices.55 Total liver volume, left medial liver lobe volume, and right liver lobe volume negatively correlated with endoscopic grade of gastro-oesophageal varices.55
Combination approachesThe Baveno VI criteria for diagnosis of gastro-oesophageal varices, which combines liver stiffness and platelet count, have been extensively validated, suggesting that patients with gastro-oesophageal varices could be identified and unnecessary oesophagogastro-duodenoscopies could be safely avoided in many patients.56–58 According to one study, the model for end-stage liver disease score combined with the Baveno VI criteria provided a 12% increase over the Baveno VI criteria alone in the number of patients spared from undergoing duo denoscopy, with comparably high sensitivity and negative predictive value.57 Additionally, based on a recent retrospective analysis, a non-invasive prediction model combining spleen stiffness with Baveno VI criteria could be useful to rule-out high-risk gastro-oesophageal varices, making it possible to avoid an estimated 22% more unnecessary oesophagogastro-duodenoscopies compared with Baveno VI criteria alone.59 An expanded Baveno VI criteria that combines liver stiffness of less than 25 kPa and platelet count of more than 110 000 per µL could spare more endoscopies than the original criteria with a minimal risk of missing varices needing treatment.60 This model, initially established in patients with Child-Pugh class A cirrhosis, was substantiated in patients with HCV and alcoholic hepatitis, and non-alcoholic steatohepatitis (NASH),60,61 but not in patients with other disease aetiologies. In patients with HCV, a stepwise algorithm that combined liver stiffness by transient elastography of 17 kPa or more and spleen diameter of 15 cm or more had an overall accuracy of 98∙33 (SD 3∙33) for the prediction of gastro-oesophageal varices and discrimination between different grades of varices.62
The platelet count-to-spleen diameter ratio was further validated as a reliable predictor for oesophageal varices in patients with cirrhosis.63 In patients with HCV-related cirrhosis, a new model was established on the basis of platelet count-to-spleen diameter ratio and portal vein diameter measured by CT, showing modest results for detection of large gastro-oesophageal varices (86∙9% sensitivity, 57∙1% specificity).64 In a retrospective

www.thelancet.com/gastrohep Vol 3 October 2018 715
Review
cohort, the ratio of the right liver lobe diameter in the medioclavicular line to serum albumin concentration predicted the presence of varices with a sensitivity of 92∙45% and a specificity of 47∙52%, however, this approach has not been validated.65 On the basis of point shear wave elastography, a prediction model combining spleen diameter and platelet count was developed and showed excellent performance for detection of high-risk varices (AUROC 0∙946 [95% CI 0∙895–0∙977]).66 In a cohort of patients with HBV infection, right liver lobe and spleen volume measured with MRI could also detect gastro-oesophageal varices in combination with serum markers.67,68 However, the costs and accessibility of MRI in clinical practice are drawbacks. In our opinion, combinations of simpler methods (eg, ultra-sound elastography and laboratory tests), should be preferred over the use of a single modality, since this improves the likelihood of achieving a definite diagnosis while avoiding invasive procedures.
Non-invasive monitoring of portal hypertension, HVPG changes, and varicesMeasurement of HVPG provides prognostic information, and responders to medical therapy are best identified in terms of the degree of reduction in HVPG.1,2 A reduction in HVPG of at least 20% from baseline or to 12 mm Hg or less indicates a decreased risk of development of varices, first variceal haemorrhage, and death.1,2 However, HVPG is not routinely monitored in clinical practice.1 In patients with compensated cirrhosis, surveillance endoscopy should be repeated at different intervals according to the presence or absence of varices on the first endoscopy, ongoing liver injury, and cofactors of disease.2 Information is scarce on how non-invasive tests could be used to monitor portal hypertension and varices. Imaging evidence of new portosystemic collaterals and progressive splenomegaly during follow-up is associated with development or growth of varices.1 By contrast, non-invasive methods that accurately mirror changes in HVPG are not widely available.
In patients with cirrhosis who are taking non-selective β-blockers, reduced portal vein velocity and increased hepatic vein damping index significantly correlated with HVPG reduction in response to therapy.11 However, these data are not sufficiently robust to allow translation to clinical practice. In another study with patients taking non-selective β-blockers, liver stiffness measured by transient elastography did not mirror changes in HVPG.69 There was a mean reduction in liver stiffness of 1∙2 kPa; responders to medical therapy showed a slight increase in liver stiffness (2∙7 kPa, SD 10∙7) whereas non-responders showed a slight decrease (–1∙9 kPa, SD 12∙2), without a statistically significant difference between the two groups (p=0∙331).69 However, in a cohort of patients with HCV, liver stiffness measured by transient elastography showed
high accuracy (AUROC of 0·888) for identification of clinically significant portal hypertension, 1 year after sustained virological response.70 Importantly, patients whose liver stiffness value remained above 21 kPa invariably had clinically significant portal hypertension, whereas an adequate prediction was not possible in patients with lower values, many of whom had HVPG of more than 10 mm Hg despite a liver stiffness less than 21 kPa.70
Moreover, interpretation of liver stiffness values in practice can be difficult in some cases. For instance, in one study, a statistically significant decrease of liver stiffness correlated with an increase of variceal size, suggesting that reduction of liver stiffness might indicate collateral formation.71 This finding needs to be validated in an appropriately designed study. In another study, spleen stiffness values strongly correlated with HVPG measured prior to transjugular intrahepatic portosystemic shunt (TIPS; r²=0·72; p<0·001) and decreased significantly after TIPS implantation, suggesting that spleen stiffness could mirror changes in portal pressure.72 However, measurement of spleen stiffness using transient elastography is limited to about 70% of cases for technical reasons (eg, a lower maximum value of stiffness), which could be overcome by using point shear wave elastography and two-dimensional real-time shear wave elastography.20 Spleen stiffness could also be useful as a follow-up test for identifying gastro-oesophageal varices in patients, regardless of intake of non-selective β-blockers, because
Search strategy and selection criteria
We searched PubMed and Web of Science for studies published from Jan 1, 2015, to May 1, 2018, with the search strategy: (“clinically significant portal hypertension” OR “CSPH”) AND (“hepatic venous pressure gradient” OR “HVPG”) AND (“diagnosis“ OR “predict“ OR “monitor“) OR (“varices“ OR “variceal“) AND (“esophagogastroduodenoscopy“ OR “endoscopy“ OR “EGD”) AND (“diagnosis“ OR “predict“ OR “monitor“). Additionally, we searched ClinicalTrials.gov for ongoing and completed studies as of May 1, 2018, on non-invasive diagnosis of portal hypertension and gastro-oesophageal varices with HVPG and oesophagogastroduodenoscopy as standard references, respectively. Duplicated results from databases were removed. Inclusion criteria were: studies focused on non-invasive diagnosis and monitoring of portal hypertension, varices and high-risk varices; and studies using HVPG measurement and oesophagogastroduodenoscopy as the reference standard for diagnosis of clinically significant portal hypertension and gastro-oesophageal varices, respectively. Exclusion criteria were: reviews, commentaries, and case reports; studies published in languages other than English; and studies done in children. See appendix for full list of studies covered in this Review.

716 www.thelancet.com/gastrohep Vol 3 October 2018
Review
its diagnostic accuracy is not hampered by use of these drugs.73 However, spleen stiffness in comparison to HVPG has not been assessed in this setting.
In a study of ten patients, spleen stiffness measured by magnetic resonance elastography was evaluated before and after TIPS,74 with values significantly decreasing after the procedure and correlating linearly with reduction in HVPG (r2=0·659, p=0·013).74 These data are encouraging but require validation in larger cohorts.
Future perspectivesAlthough many studies of non-invasive diagnostic tests have shown promising results for identifying patients with portal hypertension and gastro-oesophageal varices, many challenges remain. Heterogeneity is high across studies of non-invasive diagnostic tools because of different populations and disease aetiologies, and more prospective studies involving broader populations are needed. Body-mass index (BMI) is clearly associated with discordant findings when comparing transient elastography versus magnetic resonance elastography in the assessment of the severity of liver disease.75 Since the prevalence of obesity-related liver disease (eg, NASH) is increasing worldwide, studies focusing on methods less dependent on BMI are urgently needed. The increasing proportion of patients with HCV-related cirrhosis who achieve sustained virological response represents another challenge. Whether and how non-invasive methods can help in diagnosis and follow-up of portal hypertension in this population is unknown and requires dedicated collaborative efforts. As for the best method to use in the remaining disease aetiologies, there is still a paucity of data, despite a substantial number of studies assessing and validating various non-invasive combinations.
At present, there is no simple non-invasive test for the diagnosis and monitoring of the development and progression of portal hypertension. Importantly, even restricting need to clinically significant portal hyper-tension, a 100% reliable rule-in test for patients with compensated cirrhosis is lacking. As new techniques, such as point shear wave elastography and two-dimensional real-time shear wave elastography evolve, it will be essential for investigators and practitioners to come to a consensus on standard practice and inter-pretation of test results. Reliable non-invasive tests to monitor changes in HVPG are crucial; there is no question that this is an unmet need in hepatology. At present, no method can replace repeated measure-ment of HVPG, and a good haemodynamic response remains the only indicator of the efficacy of drugs for primary and secondary prophylaxis of variceal haemorrhage, and of low risk of progression from compensated to decompensated cirrhosis.76 An enhance-ment of the standardised training and skills in measuring HVPG worldwide is needed. However, since
HVPG measure ments are not available in all centres, a reliable and validated non-invasive surrogate would allow physicians to assess the response to therapy in all cases, which would undoubtedly improve patient outcomes.
The availability of novel tests to analyse the data obtained by new methods is an opportunity in the field to improve the diagnosis and monitoring of patients. Substantiating the robustness of non-invasive tests in large cohorts is key to safely applying these tests in clinical practice. The need for data in patients with NASH, cholestatic liver disease, and patients with sustained virological response to antiviral drugs for HCV can be addressed by large international consortia, that can nowadays easily interact through internet-based platforms. It is important to stress the remaining unmet need for both cross-sectional studies and longitudinal studies that include patients with different disease aetiologies, cirrhosis stages, and therapeutic interventions. The field of hepatology now has the opportunity to plan such studies with scientifically robust designs and adequate statistical power.
Additionally, precision medicine approaches based on liver imaging indices of risk should be developed and prospectively validated.77 The large amount of data already available allows for the design of models that account for several different non-invasive and clinical tests, with improved predictive accuracy and potential to improve patient outcomes. Finally, emerging multi-disciplinary approaches such as machine learning, radiomics algorithms, and three-dimensional compu-tational model ling have shown a satisfactory predictive accuracy compared with reference standards.78–80 Theses novel techniques are being tested in ongoing prospective studies (NCT03373123, NCT03138915, NCT02842697) with encouraging results, and could prove to be useful in the field of portal hypertension. Although diagnostic studies are less commonly prospectively registered, more data are expected in the coming years since many clinical trials are underway (table).
ConclusionsA wide spectrum of novel non-invasive tests for portal hypertension assessment has emerged in the past decade and is rapidly finding its place in clinical practice. Liver stiffness measurement by transient elastography in combination with other simple parameters can be used to identify patients with a high likelihood of having clinically significant portal hypertension and to select low-risk patients that can safely avoid oesophago gastroduodenoscopy. New techniques such as contrast-enhanced ultrasonography, shear wave elastography and magnetic resonance elastography, and new parameters such as spleen stiffness are encouraging. Machine learning and radiomics algorithms are entering the field and are likely to bring precision medicine closer to reality

www.thelancet.com/gastrohep Vol 3 October 2018 717
Review
for these patients. However, the road to a non-invasive measurement of HVPG is still long. Despite many encouraging results, we still lack a faultless non-invasive method to stratify the risk of portal hypertension and to monitor HVPG changes in response to medical therapy. The development and validation of novel approaches for diagnosis and monitoring of portal hypertension will require rigorously designed studies in well characterised cohorts of patients with compensated cirrhosis and well-defined aetiologies, with use of HVPG and oeso-phago gastroduodenoscopy as gold-standard references.ContributorsXQ was responsible for the concept and design of the Review. XQ, AB, SKS, and AC were responsible for data acquisition and literature research, drafting of the manuscript, critical revision of the manuscript, and final approval of the manuscript.
Declaration of interestsWe declare no competing interests.
AcknowledgmentsWe thank Jidong Jia and Juan Gonzalez Abraldes for constructive comments on the manuscript. We also thank Sizhe Chen for the literature research and help and critical revision of the manuscript.
References1 Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J.
Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017; 65: 310–35.
2 de Franchis R; Baveno V Faculty. Expanding consensus in portal hypertension. Report of the Baveno VI Consensus Workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol 2015; 63: 743–52.
3 Tripathi D, Stanley AJ, Hayes PC, et al. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut 2015; 64: 1680–704.
4 Bosch J, Abraldes JG, Berzigotti A, García-Pagan JC. The clinical use of HVPG measurements in chronic liver disease. Nat Rev Gastroenterol Hepatol 2009; 6: 573–82.
5 Hametner S, Ferlitsch A, Ferlitsch M, et al. The VITRO score (Von Willebrand factor antigen/thrombocyte ratio) as a new marker for clinically significant portal hypertension in comparison to other non-invasive parameters of fibrosis including ELF test. PLoS One 2016; 11: e0149230.
6 Sandahl T D, Mcgrail R, Møller HJ, et al. The macrophage activation marker sCD163 combined with markers of the Enhanced Liver Fibrosis (ELF) score predicts clinically significant portal hypertension in patients with cirrhosis. Aliment Pharmacol Ther 2016; 43: 1222–31.
7 Pind M L, Bendtsen F, Kallemose T, Møller S. Indocyanine green retention test (ICG-r15) as a noninvasive predictor of portal hypertension in patients with different severity of cirrhosis. Eur J Gastroenterol Hepatol 2016; 28: 948–54.
8 Wang L, Feng Y, Ma X, et al. Diagnostic efficacy of noninvasive liver fibrosis indexes in predicting portal hypertension in patients with cirrhosis. PLoS One 2017; 12: e0182969.
9 Leeming DJ, Veidal SS, Karsdal MA, et al. Pro-C5, a marker of true type V collagen formation and fibrillation, correlates with portal hypertension in patients with alcoholic cirrhosis. Scand J Gastroenterol 2015; 50: 584–92.
10 Bruha R, Jachymova M, Petrtyl J, et al. Osteopontin: a non-invasive parameter of portal hypertension and prognostic marker of cirrhosis. World J Gastroenterol 2016; 22: 3441–50.
11 Kim M, Baik S, Park D, et al. Damping index of Doppler hepatic vein waveform to assess the severity of portal hypertension and response to propranolol in liver cirrhosis: a prospective nonrandomized study. Liver Int 2007; 27: 1103–10.
12 Bolognesi M, Sacerdoti D, Merkel C, et al. Noninvasive grading of the severity of portal hypertension in cirrhotic patients by echo-color-Doppler. Ultrasound Med Biol 2001; 27: 901–07.
13 Lee CM, Jeong WK, Lim S, et al. Diagnosis of clinically significant portal hypertension in patients with cirrhosis: splenic arterial resistive index versus liver stiffness measurement. Ultrasound Med Biol 2016; 42: 1312–20.
14 Maruyama H, Yokosuka O. Ultrasonography for noninvasive assessment of portal hypertension. Gut Liver 2017; 11: 464–73.
15 Maruyama H, Shiha G, Yokosuka O, et al. Non-invasive assessment of portal hypertension and liver fibrosis using contrast-enhanced ultrasonography. Hepatol Int 2016; 10: 267–76.
16 Eisenbrey JR, Dave JK, Halldorsdottir VG, et al. Chronic liver disease: noninvasive subharmonic aided pressure estimation of hepatic venous pressure gradient. Radiology 2013; 268: 581–88.
17 Amat-Roldan I, Berzigotti A, Gilabert R, Bosch J. Assessment of hepatic vascular network connectivity with automated graph analysis of dynamic contrast-enhanced US to evaluate portal hypertension in patients with cirrhosis: a pilot study. Radiology 2015; 277: 268–76.
18 Berzigotti A, Piscaglia F, Amat-Roldan I, et al. Non-invasive measurement of HVPG using graph analysis of dynamic contrast-enhanced ultrasound: the CLEVER study. J Hepatol 2018; 68: S76–77.
19 You MW, Kim KW, Pyo J, et al. A meta-analysis for the diagnostic performance of transient elastography for clinically significant portal hypertension. Ultrasound Med Biol 2016; 43: 59–68.
20 Berzigotti A. Non-invasive evaluation of portal hypertension using ultrasound elastography. J Hepatol 2017; 67: 399–411.
21 Attia D, Schoenemeier B, Rodt T, et al. Evaluation of liver and spleen stiffness with acoustic radiation force impulse quantification elastography for diagnosing clinically significant portal hypertension. Ultraschall Med 2015; 36: 603–10.
22 Deng H, Qi X, Zhang T, et al. Supersonic shear imaging for the diagnosis of liver fibrosis and portal hypertension in liver diseases: a meta-analysis. Expert Rev Gastroenterol Hepatol 2017; 12: 91–98.
23 Thiele M, Madsen BS, Procopet B, et al. Reliability criteria for liver stiffness measurements with real-time 2d shear wave elastography in different clinical scenarios of chronic liver disease. Ultraschall Med 2017; 38: 648–54.
24 Procopet B, Berzigotti A, Abraldes JG, et al. Real-time shear-wave elastography: applicability, reliability and accuracy for clinically significant portal hypertension. J Hepatol 2015; 62: 1068–75.
25 Song J, Huang J, Huang H, et al. Performance of spleen stiffness measurement in prediction of clinical significant portal hypertension: a meta-analysis. Clin Res Hepatol Gastroenterol 2018; 42: 216–26.
26 Takuma Y, Nouso K, Morimoto Y, et al. Portal hypertension in patients with liver cirrhosis: diagnostic accuracy of spleen stiffness. Radiology 2016; 279: 609–19.
27 Zykus R, Jonaitis L, Petrenkienė V, et al. Liver and spleen transient elastography predicts portal hypertension in patients with chronic liver disease: a prospective cohort study. BMC Gastroenterol 2015; 15: 183.
28 Elkrief L, Rautou PE, Ronot M, et al. Prospective comparison of spleen and liver stiffness by using shear-wave and transient elastography for detection of portal hypertension in cirrhosis. Radiology 2015; 275: 589–98.
29 Jansen C, Bogs C, Verlinden W, et al. Shear-wave elastography of the liver and spleen identifies clinically significant portal hypertension: a prospective multicentre study. Liver Int 2017; 37: 396–405.
30 Elkrief L, Ronot M, Andrade F, et al. Non-invasive evaluation of portal hypertension using shear-wave elastography: analysis of two algorithms combining liver and spleen stiffness in 191 patients with cirrhosis. Aliment Pharmacol Ther 2018; 47: 621–30.
31 Gouya H, Grabar S, Vignaux O, et al. Portal hypertension in patients with cirrhosis: indirect assessment of hepatic venous pressure gradient by measuring azygos flow with 2D-cine phase-contrast magnetic resonance imaging. Eur Radiol 2016; 26: 1981–90.
32 Palaniyappan N, Cox E, Bradley C, et al. Non-invasive assessment of portal hypertension using quantitative magnetic resonance imaging. J Hepatol 2016; 65: 1131–39.

718 www.thelancet.com/gastrohep Vol 3 October 2018
Review
33 Chouhan MD, Mookerjee RP, Bainbridge A, et al. Caval subtraction 2D phase-contrast MRI to measure total liver and hepatic arterial blood flow: proof-of-principle, correlation with portal hypertension severity and validation in patients with chronic liver disease. Invest Radiol 2017; 52: 170–76.
34 Gharib AM, Han M, Meissner EG, et al. Magnetic resonance elastography shear wave velocity correlates with liver fibrosis and hepatic venous pressure gradient in adults with advanced liver disease. Biomed Res Int 2017; published online April 5. DOI:10.1155/2017/2067479.
35 Abraldes JG, Bureau C, Stefanescu H, et al. Noninvasive tools and risk of clinically significant portal hypertension and varices in compensated cirrhosis: the “Anticipate” study. Hepatology 2016; 64: 2173–84.
36 Fouad R, Hamza I, Khairy M, et al. Role of serum soluble CD163 in the diagnosis, risk of bleeding, and prognosis of gastro-esophageal varices in cirrhotic patients. J Interferon Cytokine Res 2017; 37: 112–18.
37 Farid K, Omran MM, Farag RE, et al. Development and evaluation of a novel score for prediction of large oesophageal varices in patients with hepatitis c virus-induced liver cirrhosis. Br J Biomed Sci 2017; 74: 138–43.
38 Zhang C, Xu J, Li J, et al. Predict esophageal varices via routine trans-abdominal ultrasound: a design of classification analysis model. J Gastroenterol Hepatol 2016; 31: 194–99.
39 Bintintan A, Chira R I, Bintintan VV, et al. Value of hepatic elastography and Doppler indexes for predictions of esophageal varices in liver cirrhosis. Med Ultrason 2015; 17: 5–11.
40 Li J, Feng JC, Peng XY, et al. Usefulness of contrast-enhanced ultrasonography for predicting esophageal varices in patients with hepatitis B virus (HBV)-related cirrhosis. Med Sci Monit 2017; 23: 2241–49.
41 Qiu L, Zhang X, Liu D, et al. Contrast-enhanced ultrasonography diagnostic evaluation of esophageal varices in patients with cirrhosis. Ultrasound Q 2016; 32: 136–43.
42 Pu K, Shi JH, Wang X, et al. Diagnostic accuracy of transient elastography (FibroScan) in detection of esophageal varices in patients with cirrhosis: a meta-analysis. World J Gastroenterol 2017; 23: 345–56.
43 Qu Y, Li T, Ye Q, et al. A beginning or the end? A meta-analysis to assess the diagnostic accuracy of transient elastography for the prediction of esophageal varices. Saudi J Gastroenterol 2016; 22: 345–52.
44 Li T, Qu Y, Yang B, et al. Evaluation of large esophageal varices in cirrhotic patients by transient elastography: a meta-analysis. Rev Esp Enferm Dig 2016; 108: 464–72.
45 Alhamoudi WK, Abdelrahman AA, Helmy A, et al. The role of Fibroscan in predicting the presence of varices in patients with cirrhosis. Eur J Gastroenterol Hepatol 2015; 27: 1307–12.
46 Ma X, Le W, Hao W, et al. Spleen stiffness is superior to liver stiffness for predicting esophageal varices in chronic liver disease: a meta-analysis. PLoS One 2016; 11: e0165786.
47 Wong GL, Kwok R, Hui AJ, et al. A new screening strategy for varices by liver and spleen stiffness measurement (LSSM) in cirrhotic patients: a randomized trial. Liver Int 2018; 38: 636–44.
48 Deng H, Qi X, Guo X. Computed tomography for the diagnosis of varices in liver cirrhosis: a systematic review and meta-analysis of observational studies. Postgrad Med 2016; 129: 318–28.
49 Tseng YJ, Zeng XQ, Chen J, et al. Computed tomography in evaluating gastroesophageal varices in patients with portal hypertension: a meta-analysis. Dig Liver Dis 2016; 48: 695–702.
50 Gaduputi V, Patel H, Sakam S, et al. Value of portal venous system radiological indices in predicting esophageal varices. Clin Exp Gastroenterol 2015; 8: 89–93.
51 Talakić E, Schaffellner S, Kniepeiss D, et al. CT perfusion imaging of the liver and the spleen in patients with cirrhosis: is there a correlation between perfusion and portal venous hypertension. Eur Radiol 2017; 27: 4173–80.
52 Calame P, Ronot M, Bouveresse S, et al. Predictive value of CT for first esophageal variceal bleeding in patients with cirrhosis: value of para-umbilical vein patency. Eur J Radiol 2017; 87: 45–52.
53 Asenbaum U, Ba-Ssalamah A, Mandorfer M, et al. Effects of portal hypertension on gadoxetic acid-enhanced liver magnetic resonance: diagnostic and prognostic implications. Invest Radiol 2017; 52: 462–69.
54 Morisaka H, Motosugi U, Ichikawa S, et al. Association of splenic MR elastographic findings with gastroesophageal varices in patients with chronic liver disease. J Magn Reson Imaging 2015; 41: 117–24.
55 Zhou H, Zhang J, Zhang X, et al. Liver volume measured on magnetic resonance imaging in cirrhosis patients with hepatitis B: Association with severity of esophageal varices. Int J Clin Exp Med 2017; 10: 9495–501.
56 Maurice J, Brodkin E, Arnold F, et al. Validation of the Baveno VI criteria to identify low risk cirrhotic patients not requiring endoscopic surveillance for varices. J Hepatol 2016; 65: 899–905.
57 Jangouk P, Turco L, Oliveira A, et al. Validating, deconstructing and refining Baveno criteria for ruling out high-risk varices in patients with compensated cirrhosis. Liver Int 2017; 37: 1177–83.
58 Llop E, Lopez M, de la Revilla J, et al. Validation of noninvasive methods to predict the presence of gastroesophageal varices in a cohort of patients with compensated advanced chronic liver disease. J Gastroenterol Hepatol 2017; 32: 1867–72.
59 Colecchia A, Ravaioli F, Marasco G, et al. A combined model based on spleen stiffness measurement and Baveno VI criteria to rule out high risk varices in advanced chronic liver disease. J Hepatol 2018; published online May 3. DOI:10.1016/j.jhep.2018.04.023.
60 Augustin S, Pons M, Maurice JB, et al. Expanding the Baveno VI criteria for the screening of varices in patients with compensated advanced chronic liver disease. Hepatology 2017; 66: 1980–88.
61 Ding NS, Nguyen T, Iser DM, et al. Liver stiffness plus platelet count can be used to exclude high-risk oesophageal varices. Liver Int 2015; 36: 240–45.
62 Tag-Adeen M, Alsenbesy M, Ghweil AA, et al. Liver stiffness measurement and spleen diameter as predictors for the presence of esophageal varices in chronic hepatitis C patients. Medicine (Baltimore) 2017; 96: e8621.
63 Jamil Z, Malik M, Durrani AA. Platelet count to splenic diameter ratio and other noninvasive markers as predictors of esophageal varices in patients with liver cirrhosis. Turk J Gastroenterol 2017; 28: 347–52.
64 Elalfy H, Elsherbiny W, Abdel Rahman A, et al. Diagnostic non-invasive model of large risky esophageal varices in cirrhotic hepatitis C virus patients. World J Hepatol 2016; 8: 1028–37.
65 Lalosevic MS, Stojkovic M, Naumovic T, et al. Clinical scores for the prediction of esophageal varices in patients with liver cirrhosis. Acta Gastroenterol Belg 2016; 79: 14–17.
66 Park Y, Kim SU, Park SY, et al. A novel model to predict esophageal varices in patients with compensated cirrhosis using acoustic radiation force impulse elastography. PLoS One 2015; 10: e0121009.
67 Li H, Chen TW, Li ZL, et al. Albumin and magnetic resonance imaging-liver volume to identify hepatitis B-related cirrhosis and esophageal varices. World J Gastroenterol 2015; 21: 988–96.
68 Chen XL, Chen TW, Zhang XM, et al. Platelet count combined with right liver volume and spleen volume measured by magnetic resonance imaging for identifying cirrhosis and esophageal varices. World J Gastroenterol 2015; 21: 10184–91.
69 Reiberger T, Ferlitsch A, Payer BA, et al. Non-selective β-blockers improve the correlation of liver stiffness and portal pressure in advanced cirrhosis. J Gastroenterol 2012; 47: 561–68.
70 Mauro E, Crespo G, Montironi C, et al. Portal pressure and liver stiffness measurements in the prediction of fibrosis regression after SVR in recurrent hepatitis C. Hepatology 2018; 67: 1683–94.
71 Piecha F, Paech D, Sollors J, et al. Rapid change of liver stiffness after variceal ligation and TIPS implantation. Am J Physiol Gastrointest Liver Physiol 2017; 314: G179–87.
72 Buechter M, Manka P, Theysohn JM, et al. Spleen stiffness is positively correlated with HVPG and decreases significantly after TIPS implantation. Dig Liver Dis 2018; 50: 54–60.
73 Wong GL, Kwok R, Chan HL, et al. Measuring spleen stiffness to predict varices in chronic hepatitis B cirrhotic patients with or without receiving non-selective beta-blockers. J Dig Dis 2016; 17: 538–46.
74 Guo J, Schott E, Braun J, et al. In vivo abdominal magnetic resonance elastography for the assessment of portal hypertension before and after transjugular intrahepatic portosystemic shunt implantation. Invest Radiol 2015; 50: 347–51.

www.thelancet.com/gastrohep Vol 3 October 2018 719
Review
75 Caussy C, Chen J, Alquiraish MH, et al. Association between obesity and discordance in fibrosis stage determination by magnetic resonance vs transient elastography in patients with nonalcoholic liver disease. Clin Gastroenterol Hepatol 2018; published online Jan 17. DOI:10.1016/j.cgh.2017.10.037.
76 Bhardwaj A, Kedarisetty CK, Vashishtha C, et al. Carvedilol delays the progression of small oesophageal varices in patients with cirrhosis: a randomised placebo-controlled trial. Gut 2017; 66: 1838–43.
77 Dong J, Qi X. Liver imaging in precision medicine. EBioMedicine 2018; 32: 1–2
78 Wang K, Lu X, Zhou H, et al. Deep learning Radiomics of shear wave elastography significantly improved diagnostic performance for assessing liver fibrosis in chronic hepatitis B: a prospective multicentre study. Gut 2018; published online May 5. DOI:10.1136/gutjnl-2018-316204.
79 Qi X, Li Z, Huang J, et al. Virtual portal pressure gradient from anatomic CT angiography. Gut 2015; 64: 1004–05.
80 Wang T, Liang F, Zhou Z, Qi X. Global sensitivity analysis of hepatic venous pressure gradient (HVPG) measurement with a stochastic computational model of the hepatic circulation. Comput Biol Med 2018; 97: 124–36.
© 2018 Elsevier Ltd. All rights reserved.










![Safe use of medication in patients with cirrhosis ......by portal hypertension can lead to fluid accumulation in the abdomen (i.e. ascites) [5,7]. Portal hypertension can further result](https://img.pdfslide.net/doc/110x75/5feafbb23acda067bb72703e/safe-use-of-medication-in-patients-with-cirrhosis-by-portal-hypertension.jpg)