Embed Size (px)
Citation preview
IJDA, 3(3), July-September, 2011 627
Full Mouth Rehabilitation with Group FunctionOcclusal scheme in a patient with severe
Dental Fluorosis
Sudhir N1, Hari Parkash2
Professor1
Department of Prosthodontics and Implantology,Kamineni Institute of Dental Sciences,Narketpally, Nalgonda Dist., Andhra Pradesh.
Email for correspondence:[email protected]
INTRODUCTION:
With nearly 14% of total fluoride available in theEarth’s crust present in India, Dental Fluorosis isendemic and is still a serious problem in nearly 15states of our country. The highest incidence is seenin Andhra Pradesh, Haryana, Karnataka, Punjab,Rajasthan and Tamilnadu.1 Fluoride in water is akinto a double edged sword, while it is required inconcentrations of 0.5mg/L of ground water in tropicalcountries where the drinking water consumption ismore for calcification of the bones and teeth, largerconcentrations than this can lead to debilitatingdental manifestations that range from mild,moderate to severe. Severe dental fluorosis causes
pitting/mottling of the enamel with increasedpredisposition to decay, fracture, wear, premature lossleading to degeneration of occlusal stability andhence the masticatory mechanism. It compromisesnot only the oral health of the patient but also theirpsychological bearing due to the mutilation anddiscoloration of affected teeth and impaired function.In many a cases of such severe dental fluorosis Fullmouth rehabilitation is not only curative but alsopreventive and therefore essential.
Of the various treatment procedures inProsthodontics, the most demanding is the Fullmouth Rehabilitation for, it is the culmination of allvalid and legible theory and its practical applicationto provide harmonious occlusal contacts andarticulation and synchronize the very delicately
Article InfoReceived: April 12, 2011Review Completed: May, 16, 2011Accepted: June, 17, 2011Available Online: October, 2011© NAD, 2011 - All rights reserved
REVIEW
ABSTRACT:
Full mouth rehabilitation continues to be the biggest challenge toany clinician in Restorative dentistry. It requires efficient diagnosisand elaborate treatment planning to develop ordered occlusalcontacts and harmonious articulation in order to optimizestomathognathic function, health and esthetics which thentranslates to patient's comfort and satisfaction. Thoroughknowledge of the various concepts of articulation is thereforeintegral to any full mouth rehabilitation that is taken up to addressthe patient's problem related to restoration of multiple teeth thatare either decayed, worn, broken, discolored, missing or sufferdevelopmental deficits.
This case report describes the Full mouth rehabilitation of a 22year old girl who reported with multiple decayed and discoloredfluorosed teeth with proclined anteriors. The case was treated withindividual Porcelain fused to metal crowns and a bridge withGroup function occlusal scheme using Simultaneous full archtechnique which is although exacting, exhaustive and demandingprovides for a structured stable and predictable articulation.
Several techniques of Full mouth rehabilitations are available anda clinician should ascribe to one after a comprehensive diagnosisof the patient's clinical condition and prospective considerationof his/her oral health, function, comfort and esthetic requirements.
Key words: Full mouth rehabilitation, Group function, Fluorosis
INDIAN JOURNAL OF DENTAL ADVANCEMENTS
Jour nal homepage: www. nacd. in
Professor and Director2,I.T.S. Centre for Dental Studies and Research,Muradnagar, Ghaziabad. Uttar Pradesh.
doi:10.5866/3.3.627

IJDA, 3(3), July-September, 2011628
balanced Stomatognathic system. Full mouthrehabilitations are taken up for various clinicalconditions that require extensive prostheticrestorations involving nearly the entire complimentof teeth such as advanced attrition or abrasion andcaries causing mutilation of teeth; periodontalinvolvement with drifted, elongated, extruded teethwith loss of contacts; Temporo mandibular disorders,discolored or malformed teeth secondary todevelopmental disorders including severe dentalfluorosis.2 Conformative means of occlusalrehabilitation at the intercuspal position or ICP hasto be weighed against the more radicalReorganization of occlusion at the Centric relationcontact position or CRCP, as it requires exhaustiveplanning and structured treatment procedures.However, in most cases requiring Full mouthrehabilitations, reorganizing the occlusion is the onlymeans by which we can predict a self-sustained, self-maintaining masticatory mechanism ensuringhealth, harmony and comfort.
CASE REPORT:
A 22 year old girl moderately built with goodgeneral health and no systemic ailments reported tothe Department of Prosthodontics and Implantology,All India Institute of Medical Sciences, New Delhi. Shecomplained of discolored and forwardly placedanterior teeth and multiple decayed teeth with“chipping off” in the posteriors. The patient gave ahistory of residence since her birth at a village inHaryana which had high fluoride levels in the groundwater and informed of the same problem with heryounger siblings. On clinical and radiographicexamination it was seen that she suffered fromgeneralized dental fluorosis with severe mottling ofthe enamel and dark brown discoloration (DeansFluorosis Index: Severe). Multisurface caries withocclusal wear in all the posterior teeth, missing 24which was extracted 1 year back due to caries,marked overjet, attrited incisal facets on 11,12,21,22,31,32,41,42, and lower incisal imbrication.Patient was given various treatment options and sheconsented for a Full mouth rehabilitation. Compositerestorations (Solare P, GC corp, Japan) were made inall the carious teeth and RCT was done in 11,12,21,22.Diagnostic impressions were made with irreversiblehydrocolloid (Neocolloid, Zhermack, Italy) and the
maxillary cast oriented to the articulator axis with afacebow record (Quick mount facebow, Whip mix,U.S.A.). A leaf gauge was used to deprogramme themandible and was maneuvered into centric closureand a thin trapezoidal Aluwax sheet was used torecord the same without any tooth contact(perforation) and the relation used to transfer themandibular cast to a semi adjustable articulator( Whip mix #8500, U.S.A.). Protrusive occlusalregistration was made with fast settingpolyvinylsiloxane bite registration material (BluMousse, Parkell, U.S.A.) and the articulator adjusted.Diagnostic occlusal assessment was done and anyinterference during centric closure noted andremoved in the patient’s mouth. A permissiveocclusal splint fabricated in clear auto-polymerizingresin on the articulated casts was then given both asa definitive deprogrammer and also to assess thepossibility of increasing the vertical dimension by2mm if and when required, given her occlusal wear.A diagnostic wax up was made on the articulatedmodels and two Putty Silicone indices (Aquasil,Dentsply, U.S.A.) were made on the Diagnostic waxup models, one complete for fabrication of thetemporaries and the other sectioned to aid as a guideduring tooth preparation. When after using the splintfor 6weeks, the patient reported of no discomfort, aReorganized approach to the full mouthrehabilitation with individual porcelain fused tometal crowns and a PFM bridge in relation to 23, 2425 and Group function occlusal scheme through asimultaneous full arch technique was planned. Themaxillary and mandibular teeth were preparedsimultaneously and impressions made with poly vinylsilicones (Aquasil Putty and Aquasil LV, Dentsply,U.S.A.). Complete arch dies were prepared and thecasts mounted using renewed facebow, centric andthe protrusive interocclusal records. Temporization( Tooth Shade Acrylic, Duralay, U.S.A.) was doneindirectly using the Putty Silicone index from thediagnostic wax up. Metal coping trial was made toconfirm fit and marginal integrity. Ceramic (IPSClassic, Ivoclar Vivadent )was fired onto the copingsand was followed by the bisque try-in. Final occlusaladjustments to the modified incisal guidance duringprotrusion were made and Unilateral group functionon the working sides was adjusted and confirmed.The crowns and the bridge were finally stained and
Full Mouth Rehabilitation with Group Function Sudhir & Hari Parkash

IJDA, 3(3), July-September, 2011 629
glazed and cemented with a glass ionomer (GC FujiI) luting cement. Patient was then put on a strict oralhygiene regimen and recall schedule.
DISCUSSION:
Fixed Prosthodontic procedures fall in one of twocategories, Conformative or Re-organized.Conformative occlusal approach is generallyfollowed when relatively small amount of restorativetreatment is required and is designed around thepatients existing Inter Cuspal Position, ICP (orMaximum Intercuspation, MI) which may or may notcoincide with the Centric Relation. It is limited tolocalized occlusal adjustments involving the tooth tobe prepared or its immediate vicinity such as removalof deflecting contact, shortening of the opposingcusp, elimination of non-working side interferences.Reorganized approach is needed when the presentICP is unacceptable and needs to be changed orwhen extensive restorations are required to optimizethe patient’s occlusion. Herein, the ICP is developedat the Centric Relation position of the Mandible orthe ICP is made coincident with the CRCP (CentricRelation Contact Position). This provides an even andstable occlusion and ensures there are no pathogenicdeflective contacts. Therefore, most of all full mouthrehabilitations tread the Reorganized approach as itrestores the structural and functional integrity of thedental arches that are compromised extensively bydecayed, missing, broken, worn, discolored teeth orteeth suffering from developmental defects or faultyfixed prosthodontic work. Once the decision of fullmouth rehabilitation is arrived at, two questions needto be answered, what sequence of tooth preparationand restoration is to be followed and what occlusalscheme to give. Choices range from Simultaneous fullarch or Segmental/ Quadrant or Sequentialsimultaneous techniques and Group function orCanine guided occlusal schemes. Each comes withits own merits and demerits. The choice is balancedbetween what is best for the patient given the clinicalcondition and patient’s expectation and theoperators experience and understanding.Irrespective of the choice, the treatment protocolshould essentially include preliminary proceduresdirected towards eliminating pain, infection, cariouslesions and teeth with poor prognosis by aninterdisciplinary team of specialists followed by a fullanalysis of occlusion as it exists.
Analysis of the occlusion requires the transfer ofthe maxillary and mandibular diagnostic casts to acapable articulator which provides for a moreconvenient and relatively definite means ofassessment. This requires a Facebow record to orientthe maxillary cast to the opening and closing axis ofthe articulator and a set of interocclusal records, onethe centric relation record and the other theprotrusive and laterotrusive records which are usedto transfer the mandibular cast to the articulator andadjust the lateral and horizontal condylar guidances.
Deprogramming of the mandible from a learnedpattern of neuromuscular memory to change it froma tooth guided (ICP) to a joint guided (CRCP)movement facilitates easier maneuver into Centricclosure and therefore identifying any prematuritiesand deflecting contacts. . Permissive occlusal splintsare excellent deprogramming devices and also ofdiagnostic value in cases where the verticaldimension is planned to be increased. Guiding themandible into centric closure is achieved by one ofmany methods like chin point guidance3, Dawson’sbimanual manipulation4 Tongue to palate maneuvre3.Many recording media are available for interocclusalregistration like plaster, thermoplastic waxes, zincoxide eugenol pastes, silicones and polyethers. Forits ease of manipulation and non-compressibilityafter setting, Aluwax is a relatively convenientmaterial for registration. Centric records can be madewith bimanual manipulation and a wax record inpatients who exhibit easy movement along theretruded arc. Anterior stop techniques such as tonguespatula, modified leaf gauge5 acrylic jig6 or Jones biteframe4 can be used in patients showing difficulty inmovement along the retruded arc. Analyze theocclusion on the articulated casts, identify andremove sequentially any prematurities andinterferences before the Diagnostic wax up is startedafter the preparation on the gypsum teeth. Wax isbuilt up and contoured to the selected scheme ofocclusion and the anterior guidance modified thereinin form and position.7 Putty Silicone indices are madeon the Diagnostic wax up models, one complete forfabrication of the temporaries8 and the othersectioned to aid as a guide during tooth preparation.
The Simultaneous full arch technique requiresrestoring both the arches at once with complete arch
Full Mouth Rehabilitation with Group Function Sudhir & Hari Parkash
IJDA, 3(3), July-September, 2011630
prepared dies and provides the convenience offlexibility in an occlusal plane, occlusal scheme,embrasures, crown contours and esthetics which arerestricted in the Quadrant/segmental technique.However it is arduous and requires a full archanesthesia. Canine guided occlusion is preferred inmost full mouth rehabilitations because of therelative ease of fabrication and various studies9,10,11,12
support its practice. However in cases where thecanines are missing or are compromised bydevelopmental deficits such as short roots,malocclusion, marked jaw size discrepancy andperiodontal disease, Group function provides for amore stable and self-maintaining scheme ofocclusion and distributes the force over greaternumber of teeth on the mediotrusive side. Groupfunction or Unilateral balanced occlusion has itsorigin in the works of Schuyler,13 Pankey, Mann,14
Ramfjord15 etc. This ensures that there is distributionof contacts on all the posterior teeth in centricposition thereby applying forces along their longaxes. Disocclusion occurs in the posteriors duringprotrusion and during lateral movementsdisocclusion on the non-working side occurs againstthe canine and buccal cusps of maxillary andmandibular premolars and molars on the workingside. Group function on the working side distributesthe occlusal load onto several teeth and the absenceof contacts on the non-working side preventsdestructive oblique forces on the teeth. Howeverdeveloping Group function requires greater clinicaland technical precision and is relatively difficult toachieve.
CONCLUSION:
Optimum oral health should be the primeobjective of all rehabilitation procedures because theultimate goal will always be to restore the mouth tohealth and function and preserve this statusthroughout the life of the patient.
REFERENCES:1. Teotia SP, Teotia.M. Endemic fluorosis in India : A
challenging national health problem. J.Assoc PhysiciansIndia 1994;32:347-352
2. Nathan LD. Advances in functional occlusion rehabilitation.J Prosthet Dent 1956;6: 252-258
3. Stewart RK. Clinical removable Partial Prosthodontics. IEAPublishers, St. Louis, 1997.
4. Peter.E.Dawson. Evaluation, diagnosis and treatment ofocclusal problems. The C.V.Mosby Company, 1989.
5. Woelfel and Lee. Suggested modification for the leaf wafersystem. J Prosthet Dent 1991;65:287-291.
6. Lodge Le and Mahan PD. Study of mandibular movementfrom centric occlusion to maximum intercuspation. JProsthet Dent 1967;18:19-30.
7. Irad DZ and Francis AP. Full mouth reconstruction fixed-removable. Dent Clin North Am 1987;31-35.
8. Martin D and H. Cardash. Transferring anterior occlusalguidance to the articulator. J Prosthet Dent 1983;61:282-285.
9. Lucia CV. The Gnathological concepts of articulation. DentClin North Am 1962;183-197.
10. D.Amico. Functional occlusion of the natural teeth of man.J Prosthet Dent 1961;2:899-901.
11. Stallard H and Stuart CE. Conceots of occlusion. Dent ClinNorth Am 1963;11:591-606.
12. Mann A, Chan C and Miralles R. Influence of group functionand canine guidance on EMG activity of elevator muscles.J Prosthet Dent 1987;57:494-500.
13. Schuyler CH. Freedom in centric. Dent Clin North Am1969;13:681-686.
14. Mann AW and Pankey LD. The PM philosophy of occlusalrehabilitation. Dent Clin North Am 1963;7:621-629.
15. Ash MM and Ramfjord SP. An introduction to functionalocclusion, 1982, W.B. Saunders.
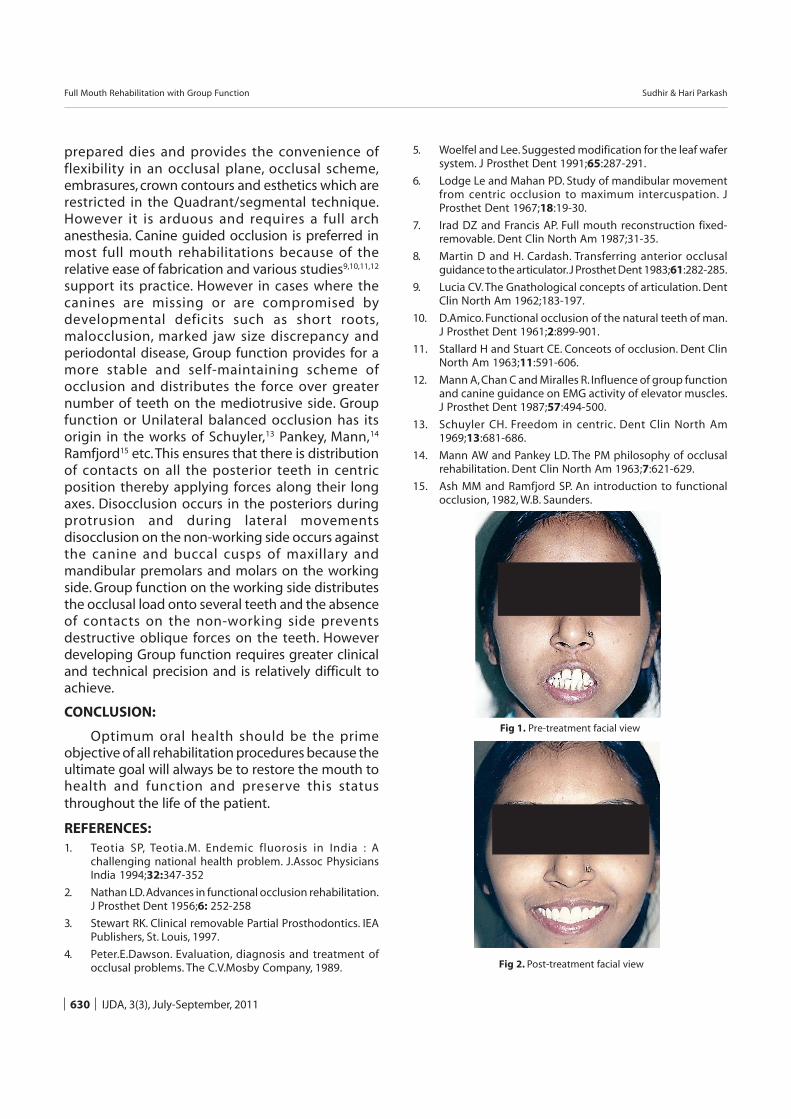
Fig 1. Pre-treatment facial view
Fig 2. Post-treatment facial view
Full Mouth Rehabilitation with Group Function Sudhir & Hari Parkash
IJDA, 3(3), July-September, 2011 631
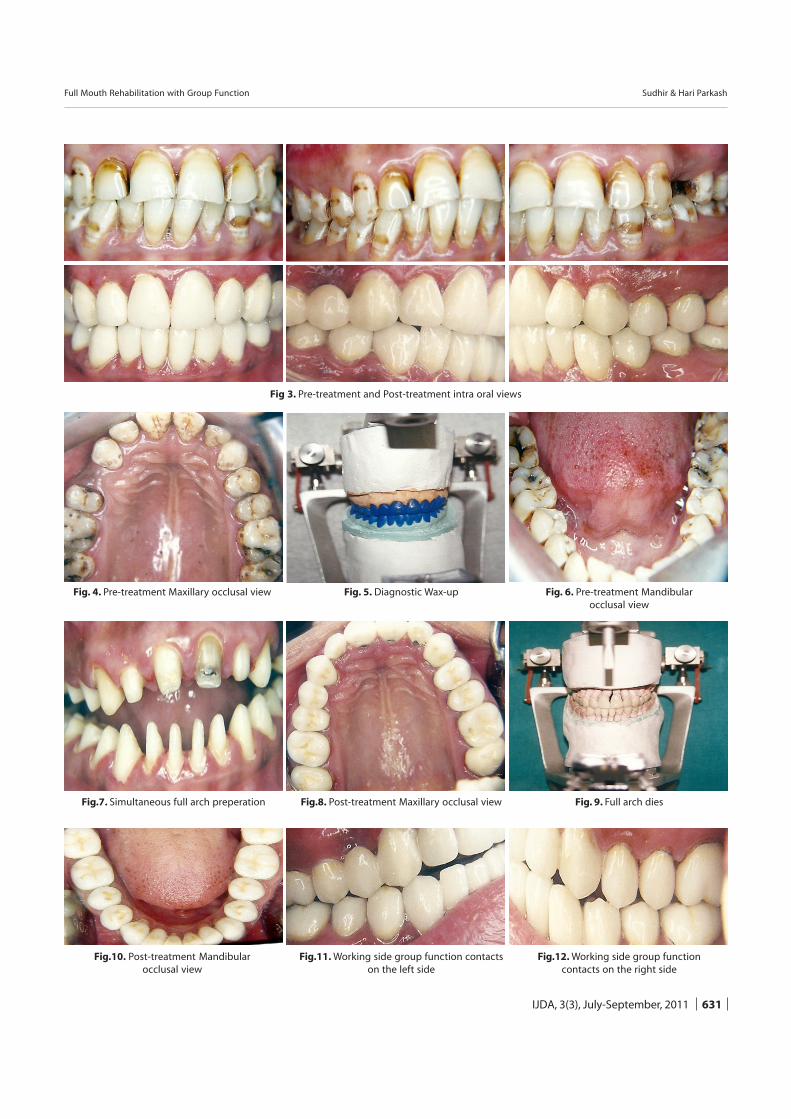
Fig 3. Pre-treatment and Post-treatment intra oral views
Fig.10. Post-treatment Mandibularocclusal view
Fig.11. Working side group function contactson the left side
Fig.12. Working side group functioncontacts on the right side
Fig.7. Simultaneous full arch preperation Fig.8. Post-treatment Maxillary occlusal view Fig. 9. Full arch dies
Fig. 4. Pre-treatment Maxillary occlusal view Fig. 5. Diagnostic Wax-up Fig. 6. Pre-treatment Mandibularocclusal view
Full Mouth Rehabilitation with Group Function Sudhir & Hari Parkash
![Full Mouth Rehabilitation with Modified Andrew’s Bridge ... · fixed prostheses [4,5]. In this clinical report, because of prevailing limitations, a full mouth rehabilitation after](https://img.pdfslide.net/doc/110x75/5f42560028e9b16b6a577f0b/full-mouth-rehabilitation-with-modified-andrewas-bridge-fixed-prostheses-45.jpg)




























