Embed Size (px)
Citation preview

ww.sciencedirect.com
Journal of Hospital Infection 78 (2011) 81e85
Available online at w
Journal of Hospital Infection
journal homepage: www.elsevierhealth.com/journals / jhin
Review of a three-year meticillin-resistant Staphylococcus aureus screeningprogramme
J. Collins a,*, M. Raza a, M. Ford a, L. Hall b, S. Brydon c, F.K. Gould a
aDepartment of Microbiology, Newcastle upon Tyne Hospitals NHS Foundation Trust, UKb Infection Prevention and Control Team, Newcastle upon Tyne Hospitals NHS Foundation Trust, UKc Information Services, Newcastle upon Tyne Hospitals NHS Foundation Trust, UK
a r t i c l e i n f o
Article history:Received 22 October 2010Accepted 22 February 2011by J.A. ChildAvailable online 20 April 2011
Keywords:Meticillin-resistant Staphylococcus aureusNose, throat and perineumUniversal screeningTargeted approach
* Corresponding author. Address: Microbiology DeHigh Heaton, Newcastle upon Tyne, NE7 7DN, UK. Tel191 2231224.
E-mail address: [email protected] (J. Co
0195-6701/$ e see front matter � 2011 The Healthcadoi:10.1016/j.jhin.2011.02.012
s u m m a r y
The Newcastle upon Tyne Hospitals NHS Foundation Trust (NuTH) implemented a seek anddestroy (S&D) programme in 2006 to minimise meticillin-resistant Staphylococcus aureus(MRSA) colonisation and/or infection of patients. Using a phased introduction, all patientspecialties were included in the scheme by September 2008, well in advance of the mandatoryDepartment of Health, England (DoH) requirement for all patients to be screened. NuTHscreens nose, throat and perineum samples from approximately 15000 patients per monthusing a chromogenic culture method, showing a mean MRSA prevalence of 2.4%. Provision ofseven-day microbiology and infection control services ensured that the turnaround time toprescribing decolonisation therapy was <24 h. Analysis of 168073 results identified thenecessity for inclusion of all three screening sites to maximise recovery of MRSA. Appraisal ofthe S&D policy demonstrated that MRSA detection rates did not increase despite an expo-nential increase in workload owing to mandatory inclusion of low risk areas in the screeningprogramme. Review of data during a typical one-month period indicated that only seven day-case patients would not have been identified as MRSA carriers using our targeted S&Dapproach compared with the DoH universal screening. Detection of these additional patientsincurred total laboratory costs of £20,000 and generated a further 4200 associated negativescreens in one month alone. Our study indicates that a screening strategy based upon clinicalrisk is more pragmatic and more cost-effective than the universal programme currentlyrequired in England.
� 2011 The Healthcare Infection Society. Published by Elsevier Ltd. All rights reserved.
Introduction
Healthcare-associated infections (HAIs), including those causedby meticillin-resistant Staphylococcus aureus (MRSA), have becomea global concern. Many strategies have been implemented toreduce significantly the risk of acquisition.1e11 The Department ofHealth, England (DoH) reported that about 9% of patients inhospitals in the UK acquire HAI, costing the National Health Service(NHS) about £1 billion per annum.12 Concurrently, estimates fromthe Office for National Statistics up to 2005 had shown a rise in
partment, Freeman Hospital,.: þ44 191 2231226; fax: þ44
llins).
re Infection Society. Published by
MRSAmortality rates.13 As a consequence, in 2006 all NHS Trusts inEngland were advised by the Chief Medical Officer to review theirpolicies for screening and decolonisation of patients with MRSA. Atargeted approach across all patient pathways was initially sug-gested by the DoH as themost effective measure for minimising therisk of infection.14
UK national protocols were subsequently modified in 2009 toencompass mandatory screening of all elective and day-casepatients, with the proviso of including emergency patients byDecember 2010.15e18 Each healthcare establishment has to providedocumentary evidence of compliance. As the DoH guidance doesnot stipulate how to provide such a commitment, local decisionswere advocated. This has resulted in a plethora of laboratoryprocedures to detect MRSA colonisation. Most testing algorithmsincorporate either chromogenic culture with or without priorenrichment or rapid molecular methods.19 Even though molecular
Elsevier Ltd. All rights reserved.

J. Collins et al. / Journal of Hospital Infection 78 (2011) 81e8582
techniques have superior sensitivity and specificity, higher costgenerally prevents their use in extensive screening regimes.20,21
Such systems have also only been validated for use with materialcollected from the anterior nares, though some authors support thenecessity for screening additional body sites to increase the likeli-hood of detection.22e27
With regard to control strategies, international protocolssuggest that extensive active surveillance cultures (ASCs) shouldonly be advocated for use in intensive care units and that routinescreening of all other hospital admissions be discouraged.28
However, despite conflict of opinion, universal ASCs were intro-duced in England as a tool to minimise HAI caused by MRSA.29
The Newcastle upon Tyne Foundation Hospitals NHS Trust(NuTH) initiated a locally devised seek and destroy (S&D) pro-gramme for MRSA in August 2006.14 As the microbiology depart-ment had processed screening swabs formore than three years therewas a considerable dataset, covering about 300 000 patients, avail-able for retrospective analysis. A review of local data was deemedessential to assess the outcomes against the recently implementednational screening initiative. The primary aims were: (i) to compareuniversal ASCs with a more targeted screening programme basedupon patient-related risk defined by specialty; (ii) to determine localMRSA prevalence; (iii) to examine the sensitivity of various bodysites for MRSA detection when using chromogenic culture methods.
Methods
NuTH is a large multi-sited teaching hospital with approxi-mately 1800 beds. The infection prevention and control team (IPCT)used a phased approach for the introduction of S&D; prioritisingusing evidence-based risk assessment of MRSA acquisition.14 Table Ishows the order of implementation, assigned risk categoryaccording to hospital specialty, and the number of MRSA screenssubmitted to the laboratory each month.
The S&D programme required admission, transfer and dischargescreens from those patients residing in hospital for more than 48 h.Known previously positive patients were pre-emptively isolated andtopical eradication therapy was administered on advice from theIPCT. Each routine screen consisted of nose, throat and perineum
Table IPhased implementation of the seek and destroy policy; indicating relevant patient specialt
Phase Implementation date Risk categorya No. of MRSA screens/month
1 August 2006 High 4000 CrEldMeReSuUr
2 September 2007 Medium 8000 AdCaCaHaInfNeOr
3 September 2008 Low 10 500 BuDeEaGyNeOpPaW
4 April 2009 Mandatory 15 000 Da
MRSA, meticillin-resistant Staphylococcus aureus.a Risk category determined by hospital patient specialty.
specimens. In those patients with open wounds, invasive devices orurinary catheters, additional specimens were required to ensurecompleteness of screening.
Sampleswere collected by nursing staff using cotton tip applicatorswhich were then forwarded to the laboratory in Amie’s Charcoaltransport media (Medical Wire and Equipment, Corsham, UK). Allswabs were inoculated on to chromID MRSA (bioMérieux, Marcyl’Etoile, France) asper local standardoperatingprocedureandobservedfor the presence of green colonies after a minimum of 20 h incubationat 37 �C in air. Such colonies were confirmed as MRSA by demonstra-tion of latex agglutination using Slidex Staph-plus (bioMérieux) fol-lowed by verification of meticillin resistance using standard methods(British Society for Antimicrobial Chemotherapy, Birmingham,UK).30,31 The IPCT, however, began individual patient management assoon as suspect colonies were detected by the laboratory.
Each chromID MRSA plate was divided into three to accom-modate nose, throat and perineum (NTP) samples. As a specific,rather than a pooled, result was documented in the laboratoryinformation management system (LIMS), this allowed simpleanalysis of individual MRSA surveillance swabs.
All infection control data were captured from the LIMS via thecommercial software tool Impromptu licensed by Cognos, Inc.(Ottawa, Canada). Monthly spreadsheets and pivot tables wereused to manipulate the information into a workable format. Datawere retrieved from all four phases of the S&D programme toallow comparisons of high, medium, low and mandatory riskgroups. A total of 168 073 NTP sets were evaluated over a three-year period. Results from patients who only submitted dualscreening swabs or NTP plus additional body sites were notincluded in this evaluation.
Results
Efficacy and cost-effectiveness of the universal screening andtargeted approach
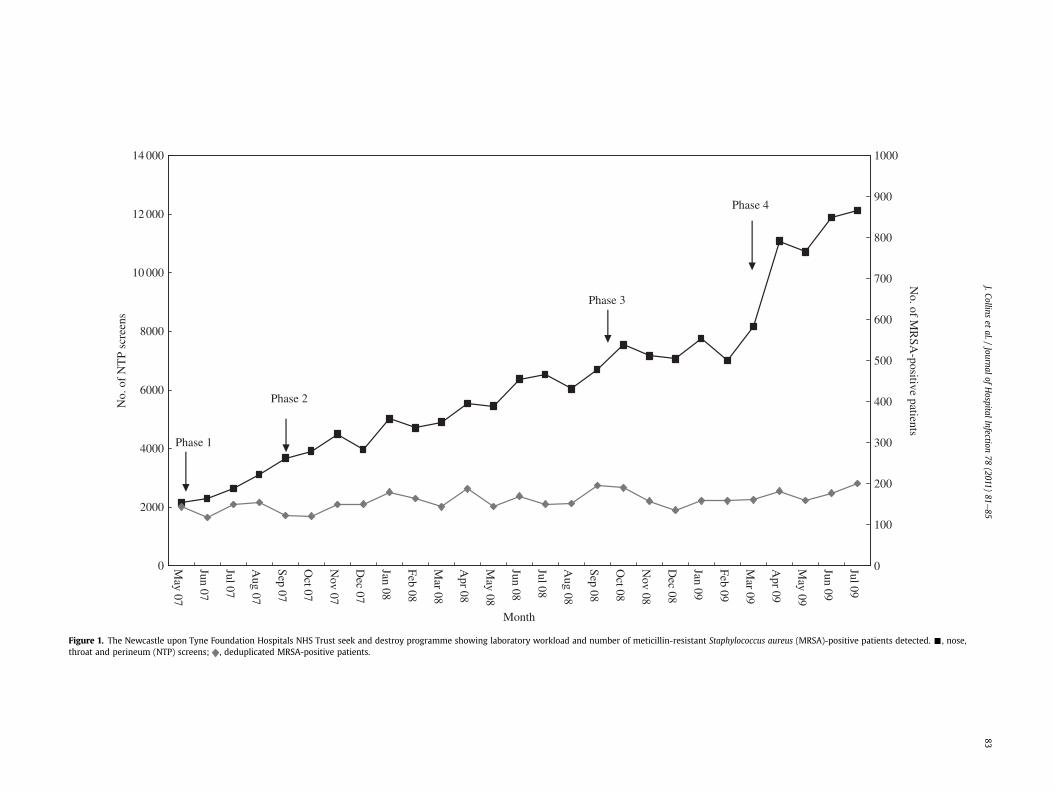
The number of patients screened for MRSA in our organisationhas increased each month since S&D was initiated in August 2006,with the most recent figures exceeding 12000 NTP screens permonth. Despite this increase, the number of MRSA-positive patients
y, average number ofMRSA screens performed eachmonth and percentage positivity
Patient specialty % MRSA positive Prevalence/risk category (%)
itical care 5.2 4.4erly care 8.0dicine 4.8nal 3.5rgery 2.7ology 2.4missions 1.1 1.6ncer services 1.5rdiology 1.0ematology 1.9ectious diseases 2.0urology 1.8thopaedics 1.8rns/plastics 3.9 1.7rmatology 5.7r, nose, throat 0.5naecology 0.5onatology 1.2hthalmology 1.1ediatrics 0.2omen’s services 0.2y cases & elective admissions 1.2 1.2
0
2000
4000
6000
8000
10 000
12 000
14 000
May 07
Jun 07
Jul 07
Aug 07
Sep 07
Oct 07
Nov 07
Dec 07
Jan 08
Feb 08
Mar 08
Apr 08
May 08
Jun 08
Jul 08
Aug 08
Sep 08
Oct 08
Nov 08
Dec 08
Jan 09
Feb 09
Mar 09
Apr 09
May 09
Jun 09
Jul 09
Month
No.
of
NT
P sc
reen
s
0
100
200
300
400
500
600
700
800
900
1000N
o. of MR
SA-positive patients
Phase 1
Phase 2
Phase 3
Phase 4
Figure 1. The Newcastle upon Tyne Foundation Hospitals NHS Trust seek and destroy programme showing laboratory workload and number of meticillin-resistant Staphylococcus aureus (MRSA)-positive patients detected. -, nose,throat and perineum (NTP) screens; , deduplicated MRSA-positive patients.
J.Collinset
al./Journal
ofHospital
Infection78
(2011)81
e85
83

Table IIPercentage of healthcare and non-healthcare MRSA acquisition for each patient riskcategory
Patient riskcategory
% healthcare-acquiredMRSA
% non-healthcare-acquiredMRSA
High 76.5 62.5Medium 17.8 18.9Low 5.7 18.6
MRSA, meticillin-resistant Staphylococcus aureus.
J. Collins et al. / Journal of Hospital Infection 78 (2011) 81e8584
detected remained relatively constant throughout the four phases ofscreening at an average of 159 patients (range: 118e201) per monthduring the 27months of study. Figure 1 illustrates themonthly totalsand highlights the relative proportion of colonised patients.
To assess the effectiveness of universal screening against theexisting NuTH S&D policy, it was necessary to appraise the clinicalspecialty of each colonised patient. Data from a typical month, June2009, were selected for this additional analysis. Results showedthat NTP specimens were received from 11 895 patients, of which3707 were elective/day-case. After deduplication there were177 patients identified as MRSA positive screened via S&D and44 screened as elective/day-case patients, establishing prevalenceas 2.2% and 1.2% respectively. Review of historical data in LIMSidentified that 23 of the elective/day-case patients were known tobe previously positive. Of the 21 new MRSA-positive patients, onlyseven day-case patients would not have been detected by ourexisting S&D screening regime.
Use of targeted screening rather than the universal programmewould equate to an estimated monthly saving, based on totallaboratory costs of £20,000 of which about £4,000 representedlaboratory consumables. Each screen has an associated consumablecost of £0.90 and total laboratory cost of £4.54.
Local prevalence of MRSA
MRSA prevalence within each clinical specialty was calculatedusing laboratory data combined with admission figures providedby NuTH Information Services. Patients colonised and/or infectedwith MRSA were reviewed over a 33-month period (April 2007until December 2009). Data were deduplicated, ensuring thatpositive patients were only represented once each quarterly periodregardless of the source of the organism. The percentage of MRSA-positive patients within each specialty is given in Table I. Asexpected, elderly care had the highest prevalence of 8%, but it isinteresting to note that all other specialties in this evaluation areconsiderably lower than the 7% prevalence assumed in theDepartment of Health Impact Assessment.32 Additional analysisshowed that 76% of all healthcare-acquired MRSA occurred withinthe high risk clinical specialties, as compared to 5.7% in the desig-nated low risk areas. Results for healthcare and non-healthcareacquisition are given in Table II.
Comparison of swab combinations
The data for sensitivity of various body sites e nose (N), throat(T) and perineum (P) e are given in Table III. This evaluation
Table IIIRecovery of MRSA using chromogenic culture media for individual and combined body s
Body site Posio
N T P N þ T N þ P T þ P
% MRSA 59 6 49 80 84 75
MRSA, meticillin-resistant Staphylococcus aureus; N, nose; T, throat; P, perineum.
demonstrated that the recovery rate, when using chromogenicculture, was at best only 59% for a single nasal swab; other bodysites were even less sensitive and only 13% of patients werecolonised in all three sites.
Discussion
The introduction and subsequent expansion of the S&D pro-gramme at NuTH has required an investment of about £1.6 millionsince August 2006. This encompassed microbiology consumables,decolonisation therapy, expansion of the laboratory footprint, plusadditional laboratory and infection control staff to allow intro-duction of a dedicated seven-day service specifically for infectionprevention and control.
Current sample turnaround times of 21e22 h for all microbi-ology MRSA results and prompt administration of eradicationtherapy indicate success of implementation. It is important tohighlight that in some laboratories, which have adopted rapidmolecular techniques, median turnaround time for processingsamples from emergency patients is also 21e22 h.33 This isconsiderably longer than stated by manufacturers but pertains tothe necessity for batch processing in the clinical laboratoryenvironment.20
Although molecular methods are only validated for use withmaterial collected from nasal specimens, single surveillanceswabs when using chromogenic culture for detection of MRSA arenot advocated.22,26,27 Despite this, the DoH best practice guidancesuggests screening nasal specimens as a minimum requirementfor MRSA surveillance. Both Bignardi and Ringberg et al.demonstrated that in their laboratory setting, throat swabs weremore effective than nasal swabs for detection of MRSA colonisa-tion. However results from this evaluation did not corroborateprevious findings.22,27 Single throat swabs only recovered MRSAfrom 46% of known positive patients, whereas nasal swabsdetected 59%. Our study indicates that to optimise detectiontriple screening swabs (nose, throat and perineum) were neces-sary. Use of dual combinations of either nose and throat, or noseand perineum, led to false-negative screening result in up to 20%of patients. It must be noted that variation among different bodysites in MRSA detection may reflect actual prevalence as well asadequacy of sample collection and sensitivity of detectionmethods.
Compliance with the national screening programme for elec-tive/day-case patients increased the number of patients assessedeach month at NuTH from approximately 7300e11500 with nocorresponding rise in MRSA detection rate. This denotes that ourlocally devised existing S&D strategy of screening high andmediumrisk groups detected the majority of patients colonised/infectedwith MRSA without the need to screen unnecessarily all the lowrisk patient groups. Comparative analysis of S&D against thenational programme has shown that fewer than ten day-casepatients each month would go undetected, against the expense ofscreening on average an additional 4200 patients each month. Day-case patients are considered a low risk group in terms of MRSAprevalence, and even if detected as colonised, full eradicationtherapy could not be given prior to any clinical procedure.
ites
tive in anyne site
Positive in anytwo sites
Positive in allthree sites
Positive in any threesites (N or T or P)
59 28 13 100

J. Collins et al. / Journal of Hospital Infection 78 (2011) 81e85 85
The difference in total laboratory costs for the targeted S&Dscreening as compared with the DoH universal strategy calculatedfor a one-month period was estimated at £20,000.
In addition to the cost of laboratory consumables required toidentify so few additional MRSA positive patients, valuable nursingtime is lost when having to order and collect an estimated 13000extra surveillance swabs each month.
Evidence gained from similar control strategies supports theeffectiveness of targeted active surveillance cultures.1,6,7 Prevalencerates in clinical specialties that fall below the community baselinecouldbeproposedas a contraindication for screening.Our evaluationhighlighted that six clinical areas had MRSA rates equal to or lowerthan those of patients admitted directly from the community:cardiology, ENT, gynaecology, neonatology, ophthalmology, paedi-atrics, andwomen’s services. Determining local prevalence shouldbeadvocated as a primary tool for assessing the requirement to screen.
Tacconelli recently posed two relevant questions: ‘How arehealthcare professionals to decide which is the best and most costeffective approach to preventing transmission of MRSA within thehospital?’ and ‘Where is the evidence?’34 This review suggests thata targeted approach to screening for MRSA colonisation is morepragmatic and cost-effective than universal ASCs. Data from ourthree-year study justifies the proposal for re-evaluation of the 100%compliance target specified by the DoH. It also implies that theinitial advice issued by the DoH in 2006 to implement a targetedapproach was the most effective model for MRSA screening. Theinterim results from the NHS Scotland pathfinder project alsosuggest that the outcome of universal screening remains conten-tious.35 Reilly et al. identified several organisational issues,including difficulties in achieving complete uptake of screening.
Resources saved by revision of the current English nationalMRSA surveillance strategy from a universal to a targeted approachcould be redirected to assist in the reduction of HAI caused by othersentinel organisms.
Acknowledgements
The authors gratefully acknowledge the support of Dr A. Gas-coigne (Director of Infection Prevention and Control) and his team,and also the microbiology staff who assisted throughout theevaluation.
Conflict of interest statementNone declared.
Funding sourcesNone.
References
1. Harbarth S, Hawkey PM, Tenover F, Stefani S, Pantosti A, Struelens MJ. Updateon screening and clinical diagnosis of methicillin-resistant Staphylococcusaureus (MRSA). Int J Antimicrobiol Agent 2011;37:110e117.
2. Yang Y, McBride MV, Rodvold KA, et al. Hospital policies and practices onprevention and treatment of infections caused by methicillin-resistant byStaphylococcus aureus. Am J Health Syst Pharm 2010;67:1017e1024.
3. Struelens MJ, Hawkey PM, French GL, Wittle W, Tacconelli E. Laboratory toolsand strategies for methicillin-resistant Staphylococcus aureus screening andtyping: state of the art and unmet needs. Clin Microbiol Infect 2009;15:112e119.
4. French GL. Methods for screening for methicillin-resistant Staphylococcusaureus carriage. Clin Microbiol Infect 2009;15(Suppl. 7):10e16.
5. Stürenburg E. Rapid detection of methicillin-resistant Staphylococcus aureusdirectly from clinical samples: methods, effectiveness and cost considerations.Ger Med Sci 2009;7. Doc06.
6. Harris AD, Furuno JP, Roghmann MC, et al. Targeted MRSA surveillance and itspotential use to guide empiric antibiotic therapy. Antimicrob Agents Chemother2010;54:3143e3148.
7. Vos MC, Behrendt MD, Melles DC, et al. 5 years of experience implementinga methicillin-resistant Staphylococcus aureus search and destroy policy at thelargest university medical center in the Netherlands. Infect Control Hosp Epi-demiol 2009;30:977e984.
8. Haung SS, Yokoe DS, Hinrichsen VL, et al. Impact of routine intensive care unitsurveillance cultures and resultant barrier precautions on hospital-wide methi-cillin-resistant Staphylococcus bacteraemia. Clin Infect Dis 2006;43:971e978.
9. Simmons S. Effects of selective patient screening for MRSA on overall MRSAhospital-acquired infection rates. Crit Care Nurs Q 2011;34:18e24.
10. Pearson A. Historical and changing epidemiology of healthcare-associatedinfections. J Hosp Infect 2009;73:296e304.
11. Mears A, White A, Cookson B, et al. Healthcare-associated infections in acutehospital: which interventions are effective? J Hosp Infect 2009;71:307e313.
12. Donaldson L, Beasley C. Saving lives. A delivery programme to reduce healthcareassociated infection including MRSA. London: Department of Health; June 2005.
13. Office for National Statistics. http://www.statistics.gov.uk/cci/nugget.asp?id¼1067. Date last accessed,1 October 2010.
14. Donaldson L, Beasley C. Screening for MRSA colonisation: a summary of bestpractice. PL CMO(2006)4. London: Department of Health; 2006.
15. Department of Health (England). The NHS in England: the operating frameworkfor 2008/09 and 2009/10. London: Department of Health; 2007.
16. Beasley C, Flory D. MRSA screening e operational guidance. London: NHSFinance, Performance and Operations; July 2008.
17. Beasley C, Flory D. MRSA screening e operational guidance 2. London: NHSFinance, Performance and Operations; December 2008.
18. Beasley C, Flory D. MRSA screening e operational guidance 3. London: NHSFinance, Performance and Operations; March 2010.
19. Gurran C, Holliday MG, Perry JD, Ford M, Morgan S, Orr KE. A novel selectivemedium for the detection of methicillin-resistant Staphylococcus aureusenabling result reporting in under 24 h. J Hosp Infect 2002;52:148e151.
20. Wolk DM, Picton E, Johnson D, et al. A multicentre evaluation of the CepheidXpertTM MRSA test as a rapid screening method for detection of MRSA fromnares swabs. J Clin Microbiol 2009;47:758e764.
21. Jeyaratnam D, Whitty C, Phillips K, et al. Impact of rapid screening tests onacquisition of methicillin resistant Staphylococcus aureus: cluster randomisedcrossover trial. BMJ 2008;336:927e930.
22. Bignardi G, Lowes S. MRSA screening: throat swabs are better than nose swabs.J Hosp Infect 2009;71:373e388.
23. Harbarth S, Schrenzel J, Renzi G, Akakpo C, Ricou B. Is throat screeningnecessary to detect methicillin-resistant Staphylococcus aureus colonization inpatients upon admission to an intensive care unit? J Clin Microbiol 2007;45:1072e1073.
24. Bitterman Y, Laor A, Itzhaki S, Weber G. Characterisation of the best anatomicalsites for MRSA colonisation. Eur J Clin Microbiol Infect Dis 2010;29:391e397.
25. Mertz D, Frei R, Periat N, Zimmerli M, Battegay M. Exclusive Staphylococcusaureus throat carriage: at risk populations. Arch Int Med 2009;169:172e178.
26. Batra R, Eziefula AC, Wyncoll D, Edgeworth J. Throat and rectal swabs may havean important role in MRSA screening of critically ill patients. Intensive Care Med2008;34:1703e1706.
27. Ringberg H, Petersson CA, Walder H, Johansson HPJ. The throat: an importantsite for MRSA colonisation. Scand J Infect Dis 2006;38:888e893.
28. Weber SG, Huang SS, Oriola S. Legislative mandates for use of active surveil-lance cultures to screen for methicillin-resistant Staphylococcus aureus andvancomycin-resistant enterococci: positive statement from the Joint SHEA andAPIC Task Force. Am J Infect Control 2007;35:73e85.
29. McGinigle KL, Gourlay ML, Buchana IB. The use of active surveillance culturesin adult intensive care unit to reduce methicillin-resistant Staphylococcusaureus related morbidity, mortality and costs: a systemic review. Clin Infect Dis2008;46:1717e1725.
30. van Griethuysen A, Bes M, Etienne J, Zbinden R, Kluytmans J. Internationalmulticenter evaluation of latex agglutination tests for identification of Staph-ylococcus aureus. J Clin Microbiol 2001;39:86e89.
31. Andrews JM. BSAC Working Party on Susceptibility Testing. BSAC standardiseddisc susceptibility testing method (version 8). J Antimicrob Chemother2009;64:454e489.
32. Department of Health (England). Impact assessment of screening elective patientsfor MRSA. Version 0.3; November 2008.
33. Tacconelli E, de Angelis G, de Waure C, Cataldo M, la Torre G, Cauda R. Rapidscreening tests for meticillin-resistant Staphylococcus at hospital admission:systematic review and meta-analysis. Lancet Infect Dis 2009;9:546e554.
34. Tacconelli E. Screening and isolation for infection control. J Hosp Infect2009;73:371e377.
35. Reilly JS, Stewart S, Christie P, et al. Universal screening for methicillin-resistantStaphylococcus aureus: interim results from the NHS Scotland pathfinderproject. J Hosp Infect 2010;74:35e41.





























