Embed Size (px)
Citation preview

R A D I O L O G I CC L I N I C S
O F N O R T H A M E R I C A
Radiol Clin N Am 45 (2007) 461–483
461
Review of CT Angiography of AortaTongfu Yu, MDa, Xiaomei Zhu, MDa, Lijun Tang, MDa,Dehang Wang, MDa,*, Nael Saad, MB, BChb
- CT techniquesExamination protocolsProtocols for administration of contrast
mediumPostprocessing techniques
- Anatomy- Congenital anomalies
Interrupted aortic archCoarctation of the aortaRight aortic arch
- Aortic aneurysmAortic ruptureInfectionManagement of abdominal aortic
aneurysmCT techniques
- Aortic dissection
CT findings- Intramural hematoma
CT findings- Atherosclerotic disease
CT findings- Traumatic aortic injury
Incomplete ruptureComplete ruptureTraumatic aortic dissectionTraumatic acute intramural hematoma
- Postoperative changesMigrationPseudoaneurysmEndoleak
- Stenosis- Summary- References
During the past decade CT angiography (CTA)has become a standard noninvasive imaging mo-dality for the depiction of vascular anatomy andpathology. The quality and speed of CTAexaminations have increased dramatically as CTtechnology has evolved from one-channel spiralCT systems to multichannel (4-, 8-, 10- and 16-slice) spiral CT systems. Sixty-four multidetectorrow CT (MDCT) became available in 2004 [1–4].The imaging modality most commonly used for di-agnosis of aortic disease is CT, followed by transeso-phageal echocardiography, MR imaging, andaortography. If multiple imaging is performed, the ini-tial imaging technique most frequently used is CT [5].
0033-8389/07/$ – see front matter ª 2007 Elsevier Inc. All righradiologic.theclinics.com
CT techniques
Examination protocols
CTA of the aorta using four-slice scanners producesimages with a lower spatial resolution and a rela-tively longer scan time than those produced usingscanners with 16 or more slices. The spatial resolu-tion needed to render diagnostic images of thesmaller branches of the aorta and of intimal tearsbecomes feasible with the latter scanners. Thescan should cover the area from a level 3 cm abovethe aortic arch to the level of the femoral heads.Typical protocols for 4-, 16- and 64-slice scannersfor aortic CTA are given in Table 1.
a Radiological Department of the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu210029, Chinab Department of Imaging Sciences, University of Rochester Medical Center, Rochester, NY, USA* Corresponding author.E-mail address: [email protected] (D. Wang).
ts reserved. doi:10.1016/j.rcl.2007.04.010

Yu et al462
Table 1: Scan protocols for CT angiography of the entire aorta with a range of 100 cm for differentscanners
ScannerRotationtime (s) Collimation
Tablefeed(mm/s)
Slicethickness(mm)
Sliceinterval(mm) Duration (s)
Numberofimages
4-slice 0.5 4 � 2.5 mm 30 3 1.5 33 6670.8 4 � 2.5 mm 19 3 1.5 53 667
16-slice 0.5 16 � 1.5 mm 48 2 1.2 21 83364-slice 0.33 32 � 0.6 mm � 2 48 1 0.8 21 1250
Currently the standard tube voltage for CTA is120 kV. The tube current should be approximately120 mAs, and automated dose modulation shouldbe used. A tube voltage of 100 kV increases the con-trast-to-noise ratio because of effective X-ray ab-sorption by iodine at lower tube voltages, whichimproves the quality of images and reduces the ra-diation exposure to patients by 35% in comparisonwith 120 kV at a constant tube current [6]. CTA ofthe abdominal aorta performed at a low voltage re-sults in higher attenuation in the aorta with reducedradiation dose and without degrading the diagnos-tic image quality. The volume of iodinated contrastmedium can be reduced by lowering the voltageduring CTA [7,8].
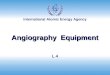
The beating of the heart results in both circularand perpendicular motion of the aorta that ismost pronounced near the heart. Pseudodissectionof the thoracic aorta, a well-known pitfall, occurspredominantly at the right anterior and left poste-rior aortic circumference (Fig. 1) [9]. Multiplanarreconstruction of images from contrast-enhancedor unenhanced helical CT provides evidence of mo-tion artifacts [10]. Hofmann and colleagues [11]recommended the use of retrospective ECG gatingfor imaging of the heart, the aortic root, and the as-cending aorta, especially when motion artifacts
may influence the diagnosis critically (eg, when aor-tic dissection is suspected); however, an ECG-gatedscan increases the radiation dose to the patient.Morgan-Hughes and colleagues [12] suggestedthat in patients who have slower heart rates (% 70beats per minute), a reconstruction windowshould be centered at 75% of the R-R intervaland that in patients who have faster heart rates(> 70 beats per minute) the construction windowshould be centered at 50% of the R-R interval.ECG-assisted MDCT shows a significant reductionof motion artifacts for the entire thoracic aortacompared with non–ECG-assisted MDCT [9].
Protocols for administration of contrastmedium
High-quality CTA of the aorta requires sufficientcontrast enhancement. An intra-arterial targetthreshold higher than 200 Hounsfield units(HU) produces adequate aortic enhancement fora diagnostic study [13]. As blood and the contrastmedia travel downstream, gradual mixing of thecentral and peripheral parts of the lumen occurs;to compensate for this dilution effect, a high-contrast delivery rate should be used to reachthe target threshold. In addition, the reductionin the volume of contrast material for a given
Fig. 1. (A) The motion of the heart transfers motion to the right anterior and left posterior walls of the ascend-ing aorta (white arrows), which mimics aortic dissection. (B) Sagittal multiplanar reformation reconstructionshows evidence of motion artifact.

Review of CT Angiography of Aorta 463
iodine dose may reduce adverse hemodynamiceffects, especially in large patients [14]. Therefore,contrast media with a high iodine concentration(350–400 mg/mL) should be used at a flow rateof 3 to 4 mL/s to reach the target threshold [3].Uniform vascular contrast enhancement witha reduced volume of contrast medium, which isdesirable in CTA and essential for steady-statequantification of blood volume, can be achievedby using an exponentially decelerated methodfor injecting contrast medium [15].
Another challenge of aortic CTA is scan synchro-nization, which is determined by several factorsincluding the transit of contrast medium bolus inthe aorta, the start of the scan, and the table feed.Factors that influence the pattern of the arterialenhancement include the volume of contrastmedium, the injection rate, and the iodine concen-tration [16,17]. Adjusting the volume of contrastmedium according to the patient’s weight can resultin a predictable degree of aortic enhancement, butin clinical practice a fixed amount is applied [18].A saline chaser usually is used in CTA performedby 16-row CT, especially in CTAs examining thevessels of the thorax. A saline chaser can facilitatethe use of a smaller volume of contrast medium,decrease the streak artifacts in the superior venacava, and produce a uniform enhancement patternwithout affecting the maximal enhancement in themain arteries [19–21]. The time to peak aortic en-hancement depends mainly on the injection rate;increasing the injection rate leads to a proportionalincrease in arterial enhancement regardless of theiodine concentration and volume of the contrastmedium [22]. Effective opacification of the thoracicaorta is achieved better by injecting a contrast me-dium with a high iodine concentration at injectionrates of 3 mL/s or more [23].
The start of the scan can be determined by one ofthree methods: using a fixed delay time, using a delaytime determined by a peak enhancement timeobtained from a test bolus, or triggered by bolustracking [13]. Awai and colleagues [24] showedthat in a protocol using a fixed injection duration,the time of arterial phase CT scanning may remainunchanged; thus, the scanning protocol can be spec-ified easily because the aortic peak enhancementtime and the period during which contrast enhance-ment is 200 HU or greater are almost constant. Theauthors did not specify the time value for a fixedinjection duration, however [24]. Because scantimes become shorter with the use of faster MDCTscanners, bolus timing is essential to make the fulluse of the contrast media. Automated bolus trackingis used more often than the test-bolus technique be-cause it is easier to use, is more efficient, and reducesthe total contrast medium dose [25]. Also, with the
bolus-tracking protocol, scanning is performedduring the plateau of attenuation, which may offera more homogenous enhancement in the aortaand less pooling of contrast material in the rightside of the heart [26]. Another important consider-ation with regards to synchronization of the con-trast bolus and the scan is the table feed. The tablefeed of 64-slice scanners, sometimes up to 7 cm/s,may result in the scan overriding the bolus if a prox-imal stenosis is present. A lower table feed may re-sult in the bolus overtaking the scan if there isperipheral vasodilatation. These two circumstanceswill affect the quality of the aortic CTA. Thomasand Bernhard [25] recommend using a fixed tablefeed of 40 to 48 mm/s combined with bolus track-ing to perform aortic CTA.
Postprocessing techniques
CTA of the aorta using modern CT scanners pro-duces several hundred images per study. This vol-ume of data makes a comprehensive review of allaxial images virtually impossible, and postprocess-ing techniques providing three-dimensional volu-metric images are a prerequisite for efficientinterpretation of the CTA and for reporting the find-ings to referring physicians. An important point forall postprocessing techniques is that they should notbe rendered from the entire data set, because doingso would reduce the spatial resolution substantially.The aorta should be divided into segments to exploitthe high Z-axis resolution inherent in the data set.Volume rendering is not without its disadvantages,however: skeletal structures may overlap vessels,and vessel wall calcifications may obscure underly-ing stenotic lesions. Maximum intensity projection(MIP) is a projection without depth information.MIP images of vessels are similar to digital subtrac-tion angiography images, with the advantage thatany desired projection can be visualized from a sin-gle data acquisition set. Overlapping bones thatcompletely obscure the view of the artery may be re-solved by thin-slab MIP images or bone-removaltechniques. Thin-slab MIP images are performedin a short time and depict a particular vascular seg-ment but lack a comprehensive overview of the en-tire vascular bed. A threshold of 200 to 300 HU isselected for bone removal, and a few referencepoints are set in bones at different positions. Despitethe relatively long postprocessing time, the authorsof this article consider MIP with bone removal thebest way of displaying CTAs because of the excellentimage quality. Curved multiplanar reformation isa technique that can be used if the vascular lumentravels along the long axis. Curved multiplanar ref-ormation is an excellent adjunct to MIP reconstruc-tions whenever extensive calcifications obscure theview of the lumen on MIP images.

Yu et al464
CT angiography is noninvasive, is substantiallyless expensive than conventional digital subtractionangiography, and allows three-dimensional visuali-zation of vessels from any angle from a single set ofdata acquisition [26,27]. Another advantage of CTAover digital subtraction angiography is the ability toshow the shape, size, and density of the vascularwall and the adjacent organs. Compared withCTA, the major disadvantages of conventional angi-ography are cost, failure to detect intramural hema-toma (IMH), and excessive time required for theexamination [10]. CTA also has some disadvan-tages, which include lack of dynamic informationand a somewhat poor visualization of small collat-erals. Because of the use of contrast media, the mostcommon complications during general CT exami-nations are allergic reactions and contrast extravasa-tion, and quite a few cases of iatrogenic intravenousair embolism have been reported in the literature[28].
Anatomy
The aorta consists of an ascending segment, a trans-verse segment or arch, and a descending segment.The ascending aorta is approximately 5 cm longand has two distinct segments. The lower segmentis the aortic root, which begins at the level of theaortic valve and extends to the sinotubular junc-tion. This portion of the ascending aorta is the wid-est and measures about 3.5 cm in diameter. Theascending aorta extends to the origin of the innom-inate artery. The aortic arch begins at the innomi-nate artery and ends at the ligamentum or ductusarteriosum. The innominate, left carotid, and leftsubclavian arteries arise from the aortic arch. Thepoint at which the aortic arch joins the descendingaorta is called the ‘‘aortic isthmus.’’ The aortic arch isusually on the left side. The descending aorta beginsat the ligamentum or ductus, and its proximal por-tion may appear slightly dilated, ending at thetwelfth intercostal space [29].
The thoracic portion of the aorta is a continuationof the aortic arch as it descends through the thoraciccavity to the diaphragm. The descending aorta in thethoracic cavity gives off branches to the organs andmuscles of the thoracic region. These branches in-clude pericardial arteries, bronchial arteries for sys-temic circulation to the lungs; esophageal arteries,which supply the esophagus as it passes throughthe mediastinum; segmental posterior intercostalarteries supplying the intercostal muscles and otherstructures of the thoracic wall; and superior phrenicarteries supplying blood to the diaphragm.
The abdominal portion of the aorta is the seg-ment of the aorta between the diaphragm and thelevel of the fourth lumbar vertebra, where it divides
into the right and left common iliac arteries. Threemajor unpaired arteries supply blood to the ab-dominal organs. The first, a short and thick celiactrunk, divides immediately into three arteries: theleft gastric, splenic, and common hepatic arteries.The next unpaired vessel is the superior mesentericartery. It arises anteriorly from the abdominal por-tion of the aorta, just below the celiac trunk, supply-ing blood to the small intestine (except fora portion of the duodenum), the cecum, the appen-dix, the ascending colon, and the proximal twothirds of the transverse colon. The third unpairedvessel is the inferior mesenteric artery. It arises justbefore the iliac bifurcation. The inferior mesentericartery supplies the distal one third of the transversecolon, the descending colon, the sigmoid colon,and the rectum. Variations of the abdominal aortabranches are common, and sometimes a multiplic-ity of variations may be present. Knowledge of thesevariations allows clinicians to identify and protectthese branches during surgical procedures [30].
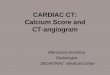
The abdominal aorta also gives rise to someimportant paired arteries. Small inferior phrenic ar-teries that supply the diaphragm are the first vesselsarising from the abdominal portion of the aorta.The next major paired vessels are the paired renalarteries that carry blood to the kidneys. Smallersuprarenal arteries, located just above the renalarteries, supply the adrenal glands. The gonadal ar-teries are small, paired vessels that arise from theabdominal portion of the aorta, just below therenal arteries. Several lumbar arteries branch poste-riorly from the abdominal portion of the aortathroughout its length and supply the muscles andthe spinal cord in the lumbar region. In addition,an unpaired middle sacral artery arises from theposterior terminal portion of the abdominal por-tion of the aorta to supply the sacrum and coccyx.The abdominal portion of the aorta terminates inthe posterior pelvis as it bifurcates into the rightand left common iliac arteries. These vessels passdownward approximately 5 cm on their respectivesides and terminate by dividing into the internaland external iliac arteries (Fig. 2) [31].
Congenital anomalies
A multitude of congenital anomalies may affect var-ious portions of the aorta. Examples of these anom-alies are described in the following sections.
Interrupted aortic arch
Interrupted aortic arch is defined as a separationbetween the ascending and descending aortas[32–36], and the classification is based on the siteof interruption. Interrupted aortic arch has beenclassified into three types (A, B, and C) based on

Review of CT Angiography of Aorta 465
Fig. 2. The anatomy of the aorta.
the site of aortic interruption. In type A, the inter-ruption occurs distal to the origin of the left subcla-vian artery. In type B, the interruption occurs distalto the origin of the left common carotid artery. Intype C, the interruption occurs proximal to the ori-gin of the left common carotid artery.
In any of the three types, the right subclavianartery may arise normally or abnormally; the twomost common abnormal sites are distal to the leftsubclavian artery (aberrant right subclavian artery)and from the right ductus arteriosus (isolated rightsubclavian artery). Type B interruptions account forabout two thirds of cases, type A occurs in aboutone third of cases, and type C occurs in less than1% of cases. CTA examination can show the directsigns of the three types and even the subtypes [29].
In addition to the type of interrupted aortic arch,evaluation of the distance between the proximaland distal segments, the size of a patent ductus arte-riosus, the narrowest dimension of the left ventric-ular outflow tract, and other cardiac structuralabnormalities are important for surgical planning.Three-dimensional reconstruction of the aorta andthe branches is very useful in this regard. A right-sided descending aorta with aortic interruption isalmost always associated with DiGeorge syndrome.
Coarctation of the aorta
There are two types of coarctation of the aorta: tu-bular and localized coarctation. The latter is more
common. In classic coarctation, the narrowing is lo-cated just distal to the left subclavian artery and hasmale predilection (Fig. 3) [32–35,37]. Coarctationat or immediately proximal to the left subclavian ar-tery is rare and compromises the left subclavian ar-tery. An aberrant right subclavian artery may arise ator below the coarctation. An external indentation
Fig. 3. Sagittal reformatted CT image demonstratinga membranous septation (arrow) distal to the leftsubclavian artery in a patient who has a classic aorticcoarctation.

Yu et al466
that involves all but the ventral portion of the coarc-tation corresponds internally to the ridge. The aortajust distal to the coarctation typically is dilated.Uniform narrowing of the aortic arch (tubular hy-poplasia) can be seen frequently in neonates andusually is associated with other cardiac anomalies.Localized coarctation and tubular hypoplasia maycoexist or may occur independently. Localized co-arctation can be asymptomatic and detected inci-dentally, but it occasionally may present withheadaches caused by hypertension or claudicationcaused by decreased blood flow. Depending onthe severity, surgical correction is needed when pa-tients are 3 to 5 years of age. Polson and colleagues[38] reported that coarctation of the aorta is associ-ated with hypertension and abnormalities of bloodpressure control that persist after repair and suggestthat infants who have coarctation already showsigns of pathologic adjustment of autonomic car-diovascular homeostasis. Proper imaging is of vitalimportance for the depiction and quantification ofascending aortic ectasia, aortic arch hypoplasia, re-coarctation, or the formation of a local aneurysmor pseudoaneurysm at the previous site of coarcta-tion [39,40]. MDCT and MR imaging are similarlyuseful for noninvasive evaluation of the thoracicaorta in patients who have coarctation. CTA can de-fine the extent and location of the coarctation aswell as associated cardiac anomalies. It is importantto measure the diameter of the aorta, especially af-ter treatment to assess stability of the repair anddetect complications early. The slices for the mea-surements should be manually adjusted separatelyfor each aortic level to get an oblique plane that isstrictly perpendicular to the course of the aorta. Ha-ger and colleagues [41] suggested that in explainingthe diameter differences, one should consider thenature of the changes in the diameter of an agingaorta, which grows roughly 1 mm per year.
A diverticulum of Kommerell is characterized byan ectatic infundibulum at the origin of an anoma-lous right subclavian artery that originates distal tothe left subclavian artery in a left-sided arch config-uration. In this anomaly, the infundibular originmay become aneurysmal and often exhibits circum-ferential atherosclerotic changes. The vessel, whichmost often courses posterior to the esophagus,may create an extrinsic compression on the esoph-agus and result in the clinical syndrome of dyspha-gia lusorum [42].
Right aortic arch
Patients who have a right-sided aortic arch are usu-ally asymptomatic. An aberrant left subclavianartery in association with a right-sided aortic archis the most common type of right-arch anomaly.It is rare and is associated with congenital heart
disease. Five percent of patients who have an aber-rant left subclavian artery develop compressionsymptoms caused by a tight vascular ring. Mirrorimaging branching, which is the second most com-mon right-arch anomaly, frequently is symptomaticand is associated with congenital heart disease(Fig. 4). The third most common, but rare, presen-tation is a right aortic arch with isolated left subcla-vian artery associated with congenital subclaviansteal syndrome presenting with diminished pulsein left upper extremity. CTA can visualize the rightaortic arch and various branching patterns directlyand evaluate the associated heart disease correctly.
Aortic aneurysm
Aneurysm of the aorta is defined as a permanent lo-calized dilatation of the aorta, at least 50% greaterthan normal and involving all three wall layers[43]. The lesser degree of dilatation generally isreferred to as ‘‘ectasia.’’ Most aneurysms of thethoracic aorta are atherosclerotic in origin. Othercauses are infection (mycotic aneurysms) and cysticmedial necrosis (annuloaortic ectasia) [44]. Fre-quent comorbidities include hypertension, coro-nary artery disease, obstructive pulmonary disease,and congestive heart failure. Atherosclerotic aneu-rysms typically are fusiform in shape and aremore common in the descending aorta, witha high incidence of concomitant abdominal aorticaneurysm. In Marfan syndrome, aneurysms mostcommonly occur in the proximal portion of the as-cending aorta, involving the aortic root and result-ing in a pear-shaped aorta [45]. Importantimaging features of aortic aneurysms are the maxi-mum diameter, the length, and involvement of ma-jor branch vessels. The aneurysmal thoracic aortagrows at an average rate of 1 mm per year witha high risk for natural complications (rupture ordissection) at 6 cm for the ascending aorta and7 cm for the descending aorta [46]. The yearly riskof any occurrence of rupture, dissection, or deathin a patient who has a thoracic aneurysm largerthan 6 cm in diameter is greater than 14% [46].As is the case with abdominal aortic aneurysms(AAAs), the risk of rupture for thoracic aneurysmsincreases with size, and the 5-year rupture rate isfivefold higher for aneurysms larger than 6 cm in di-ameter [47]. In asymptomatic patients, risk/benefitanalysis in a large population study supports thatthoracic aneurysms larger than 6.5 cm be repairedelectively, with the threshold for Marfan’s diseaseor familial TAAs being more than 6 cm [46]. Craw-ford and DeNatale [48] classified thoracoabdomi-nal aneurysms based on the anatomic location.Type I involves the descending thoracic aorta belowthe subclavian vessels and the upper abdominal

Review of CT Angiography of Aorta 467
Fig. 4. (A) Axial CT image demonstrating a right aortic arch (asterisk). (B) The right common carotid (black arrow)and the right subclavian (white arrow) arteries have separate origins at the aortic arch. There is a common trunk(arrowhead) of the left common carotid and left subclavian arteries. (C) Coronal reformatted image demon-strates a saccular aneurysm of the ascending aorta. The origin of the common trunk of the left common carotidartery and left subclavian artery is also seen (arrow).
aorta. Type II involves most of the descending aortaand most of the abdominal aorta below the dia-phragm. Type III involves the lower portion of thethoracic aorta. Type IV aneurysms begin at the dia-phragm and extend caudally. Type II and type IIIAAAs are the most difficult to repair. Type II aneu-rysms have the highest risk for spinal cord injuryand renal failure. Overall, up to 13% of all patientsin whom an aortic aneurysm is diagnosed havemultiple aneurysms; 25% to 28% of those whohave thoracic aortic aneurysms have concomitantabdominal aortic aneurysms.
The incidence and prevalence of AAA, a commonpathology in the elderly, is increasing [49]. Al-though most AAAs remain asymptomatic, their in-crease in size may lead to spontaneous rupture,which is associated with a mortality rate rangingfrom 66% to 95%. Forty percent to 50% of patientswho have ruptured AAA die before they reach thehospital, and the overall mortality rate is greaterthan 90% [50]. Several studies indicated the neces-sity of mass screening for AAA [51,52]. AAA screen-ing of men aged 65 to 75 years reduces AAA-relatedmortality [53]. Indeed, the Screening AAAs Very Ef-fectively (SAAAVE) Act was passed by Congress andreceived Presidential approval. It went into effect at
the beginning of 2007 and offers an ultrasoundscreening as part of the ‘‘Welcome to Medicare’’physical examination for patients older than 65years who join Medicare. Most AAAs are asymptom-atic, not detectable on physical examination, and si-lent until discovered during radiologic testing forother reasons. Tobacco use, hypertension, a familyhistory of AAA, and male sex are clinical risk factorsfor the development of an aneurysm [54]. In con-trast, pseudoaneurysms of the abdominal aortausually are iatrogenic (eg, prior graft repair of anAAA or a complication of inferior vena cava filterplacement or orthotopic heart transplant proce-dure) (Fig. 5) [55–57].
Aortic rupture
Rupture of an AAA involves complete loss of aorticwall integrity and is a surgical emergency requiringimmediate repair (Fig. 6). The mortality rate ap-proaches 90% if rupture occurs outside the hospital[54]. AAA rupture is a complicated and multifacto-rial event, dependent upon the maximum diameter,expansion rate, diastolic pressure, wall stress andstrength, asymmetry, saccular index, intraluminalthrombus, and change in stiffness. Clearly, one can-not rely on one or two simple factors alone to

Yu et al468
Fig. 5. (A) Axial CT image in a patient who has a chronic aortic pseudoaneurysm. The thick pseudocapsule formedby blood and fibrotic tissue is invading the thoracic vertebrae resulting in bone resorption. (B) Sagittal reformat-ted CT image demonstrates a narrow neck connecting the aorta and the sac of the pseudoaneurysm (arrow).
determine the risk of rupture accurately [58]. Thesite of rupture usually involves the posterior wallof the aorta [59]. The CT features of retroperitonealrupture are discontinuity of the rim of calcificationin the aneurysm wall, well-defined soft tissue den-sity adjacent to the aorta, concealed psoas muscle,and displaced viscera. Extravasation of contrast me-dium from aortic lumen is a definite sign of aorticrupture [60,61]. Contained rupture is characterizedmore frequently by a relatively well-defined soft tis-sue density adjacent to the aorta. Rupture of an aor-tic aneurysm is preventable in most cases by closesurveillance and the recognition of physical and im-aging findings that place patients at a higher risk forrupture. Early detection reduces mortality becauserepair is elective rather than emergent [62].
Infection
Infection is estimated to complicate about 0.7% to2.6% of aortic aneurysms [63]. The infectious agent
Fig. 6. Axial CT image demonstrating an abdominalaortic aneurysm that has ruptured retroperitoneallywith resultant hematoma (asterisk).
can reach the artery either by contiguous spread ofan adjacent infectious process (Fig. 7) or by trau-matic and/or iatrogenic inoculation. Risk factorsfor development of a mycotic aneurysm include ar-terial trauma, various immunocompromised states(diabetes mellitus, malignancy, alcoholism, colla-gen vascular disease, AIDS, steroid use), concurrentsepsis, endocarditis, and congenital cardiovasculardefects [64]. Cross-sectional imaging is a valuabletool that helps identify adjacent findings such asa periaortic soft tissue mass, stranding, and/or fluid(Fig. 8). Compared with the natural history of arte-riosclerotic aneurysm, relatively rapid progressionof disease was a feature that was present when se-quential examinations were obtained [65]. In addi-tion to demonstrating the size and extent of theaneurysm, a CT scan also demonstrates leak andperianeurysmal hemorrhage. Because almost 90%of arteriosclerotic aneurysms are located in the
Fig. 7. Axial CT image in a patient who has tuberculo-sis in the posterior segment of the lower lobe of theleft lung. A pseudoaneurysm (asterisk) of thedescending thoracic aorta has developed because ofnecrosis of the aortic wall.

Review of CT Angiography of Aorta 469
infrarenal aorta, the majority of infected aneurysmsare found in this location.
Management of abdominal aortic aneurysm
Surgical intervention is worthwhile when the aneu-rysm is at least 5.5 cm in diameter, or greater than4.5 cm with an increase of 0.5 cm in the 6 monthsbefore intervention [66]. Asymptomatic patientswho have an AAA should be medically optimizedbefore repair. Symptomatic aneurysms require ur-gent surgical attention. There is a paradigm shiftin the treatment of AAAs with endovascular aorticrepair. Endovascular aortic repair has been shownto have lower morbidity and mortality rates thanopen surgical repair, in addition to a reduced hospi-tal stay [66].
CT techniques
Three-dimensional CTor volume rendering (VR) CTreconstruction is an invaluable tool for evaluatingaortic aneurysm size, location, extent, visceral aorticbranches, and aortoiliac tortuosity [67] in additionto performing measurements for preoperative plan-ning of stent-graft repair [68]. Characteristics andmeasurements of the abdominal aorta and itsbranches that make it suitable for endovascular stentgrafting include an aneurysm neck (the portion ofthe infrarenal abdominal aorta between the lowestrenal artery and the proximal aspect of the aneu-rysm) that is cylindrical in shape, at least 1.5 cm inlength, free of thrombus and excessive plaque, andrelatively straight in orientation to the long axis ofthe aneurysm. Iliac artery features are similar tothose of the neck, including a small degree of tortu-osity and disease-free lumens. The maximal diame-ter of the neck and iliac arteries suitable forendovascular aortic repair varies according to thecommercial graft device used [69]. Some authorsconsider VR images more reliable than axial CTimages for the detection of renal and iliac arteryinvolvement in an AAA [70].
Fig. 8. Axial CT image demonstrating a mycotic aneu-rysm of the descending thoracic aorta with periaorticsoft-tissue mass (arrowhead) and fluid (arrow).
Aortic dissection
Aortic dissection is a potentially catastrophic car-diovascular disease associated with high morbidityand mortality that mandates emergent treatment.Advances in the understanding of this diseasehave established that survival generally is better inpatients who have lesions limited to the descendingaorta than in patients who have lesions involvingthe ascending aorta. Acute aortic dissection is themost common cause of aortic emergency. Factorspredisposing patients to aortic dissection includehypertension (the most important), Marfan syn-drome (Fig. 9), Turner syndrome, other connectivetissue diseases, congenital aortic valvular defects,aortic coarctation, aortic aneurysm, infection andother causes of aortitis, and pregnancy. Cocaineuse also has been associated with aortic dissection.
Aortic dissection is classified according to the ex-tent of involvement of the aorta. The Stanford sys-tem classifies the dissection into two types. TypeA, which accounts for about 75% of the total dissec-tions, affects only the ascending aorta or the aorticarch, regardless of the site of the intimal tear; Type Baffects the descending aorta [71]. Because the Stan-ford system is based on whether the dissectionneeds to be corrected surgically, it has supersededthe original DeBakey system that classified aorticdissection into three types (with types I and IIequivalent to type A in the Stanford system)(Fig. 10).
Aortic dissection may be acute or chronic, de-pending on its clinical manifestation. Dissectionis considered acute if the onset of symptoms oc-curred less than 2 weeks at the time of presentationand is considered chronic if the onset of symptomsoccurred more than 2 weeks before presentation.Seventy-five percent of deaths from aortic dissectionoccur within 2 weeks of the initial manifestation ofsymptoms. Mean plasma levels of thrombin-anti-thrombin complex and D-dimer decrease in corre-lation with the morphologic regressive changes.Serial measurement of D-dimer and thrombin-anti-thrombin complex is useful to predict morphologicchanges in chronic aortic dissection and has beenproposed as a method to follow-up patients whohave aortic dissection [72]. Aortic dissection withextension into a common carotid artery (Fig. 11)can cause ischemic stroke, and acute aortic dissec-tion sometimes can result in acute aortic obstruc-tion, which frequently causes life-threateningorgan ischemia [65,73].
Acute type A aortic dissection can have fatal com-plications including extension to the pericardium,the pleural space, the coronary arteries, and/or theaortic valvular ring, so it should be repaired imme-diately [73]. A risk-prediction model with control

Yu et al470
Fig. 9. (A) Axial CT image in a patient who has a type A aortic dissection. The true lumen (arrowhead) is smallerand of higher density than the false lumen (arrow). (B) Coronal reformatted image demonstrates extension ofthe dissection flap into the innominate and right common carotid arteries (arrow).
for age and gender showed hypotension/shock(odds ratio [OR] 23.8; P < .0001), absence ofchest/back pain on presentation (OR 3.5; P 5.01), and branch vessel involvement (OR 2.9; P 5.02), collectively named ‘‘the deadly triad,’’ to beindependent predictors of in-hospital death forpatients who have type B dissection.
Type B aortic dissections usually are managedconservatively with aggressive blood pressure con-trol. Complicated type B aortic dissections (eg,
containing rupture, occlusion of major branch, ex-tension, or enlargement) may require surgical man-agement, which at times may be emergent (eg,rupture, enlargement); other complications (eg, in-tractable pain, visceral malperfusion) may allowmore time for medical/interventional management.Early and midterm results show endovascular repairto be effective in treatment of acute type B aorticdissections [74,75]. Surgical repair should be per-formed if the aortic diameter enlarges or if a new
Fig. 10. The DeBakey and Stanford systems for classifying aortic dissection.

Review of CT Angiography of Aorta 471
Fig. 11. (A) Sagittal reformatted CT image demonstrating a type A aortic dissection involving the entire length ofthe aorta in a patient who has Marfan syndrome. (B) Axial CT image at the level of the main pulmonary arteryshowing involvement of the ascending and descending thoracic aorta. The larger cavity is the false lumen witha lower density (arrows); the true lumen is smaller with a higher density (arrowheads).
complication appears during the chronic phase[76]. Patients who have type B or surgically treatedtype A dissections may develop vascular complica-tions such as mesenteric or peripheral arterial ische-mia, which cannot be managed medically. Aorticfenestration is a method for decompressing thehypertensive false lumen by creating a hole in thedistal part of the dissection flap to address thiscomplication [77]. In type B aortic dissections, theaffected aortas have shown a high incidence of en-largement during the follow-up period. Eijun andcolleagues [78] reported that age greater than 60years and the presence of blood flow in the falselumen during the follow-up period are the onlytwo significant risk factors predisposing to an in-crease in the diameter of the aorta, and the thoracicaorta grows at a faster rate than the abdominalaorta. These results suggest that the segment withthe largest diameter does not always show the fast-est rate of growth. Familiarity with these results isuseful for following-up patients who have type Baortic dissection [75–76].
CT findings
CT scans performed before and after the injection ofcontrast medium are mandatory in patients sus-pected of having aortic dissection. UnenhancedCT is useful in evaluating the aorta in patients sus-pected of having an aortic dissection. Occasionally,on unenhanced CT scans one may see a calcified in-tima with internal displacement (Fig. 12). Thisfinding may be confused with an aneurysm withcalcified mural thrombus. The density of the lumenis useful to differentiate the two conditions: an
aortic dissection has a hypodense lumen and anaortic aneurysm with a calcified mural thrombushas a hyperdense lumen.
An intimal flap separating the true lumen fromthe false lumen is the hallmark of aortic dissectionon contrast-enhanced CT (Figs. 12 and 13). Distin-guishing the true and false lumens on CTA is of par-amount importance when endovascular therapy isconsidered, because the endograft must be de-ployed in the true lumen. This consideration isless significant with open surgical repair. CT charac-teristics that aid in the identification of the false lu-men include the presence of slender linear areas oflow attenuation within the false lumen correspond-ing to residual ribbons of the media incompletelysheared away during the dissection process. Thismanifestation known as the ‘‘cobweb sign’’ is spe-cific to the false lumen. Two other useful indicatorsof the false lumen are a larger cross-sectional areaand the beak sign. The beak sign is the cross-sec-tional imaging manifestation of the wedge of hema-toma that cleaves a space for the propagation of thefalse lumen [79]. On most contrast-enhanced CTscans, the lumen that is continuous with the undis-sected portion of the aorta usually can be identifiedas the true lumen. Circumferential dissection of theintimal layer can produce an intimo-intimal intus-susception, an unusual type of aortic dissection,which subsequently invaginates like a windsock.This type of intimal tear usually begins near the cor-onary orifices. An aortic aneurysm with intralumi-nal thrombus may be difficult to distinguish froma dissection with a thrombosed false lumen. Thefact that a dissection generally has a spiral shape

Yu et al472
Fig. 12. (A) Unenhanced axial CT image demonstrates displacement of the calcified intima (arrow), which corre-sponds to the intimal flap (arrowhead) on (B) the contrast-enhanced CT. The true lumen (TL) is brightly enhanc-ing; the false lumen (FL) is partially enhancing to a lesser degree because of slower flow and thrombosis.
with a smooth inner border, whereas a thrombustends to maintain a constant circumferential rela-tionship with the aortic wall with an irregular innerborder, can help in differentiating between the two.Furthermore, intimal calcification occurring in anaortic aneurysm typically is located at the peripheryof the aorta.
CTA in patients suspected of having an aorticdissection or IMH helps identify the site of an entrytear (the most proximal split in the intimal flap oran ulcerlike projection within the IMH on enhancedCT). Involvement of an aortic arch branch vessel,pericardial effusion, and aortic arch anomalies
also should be examined carefully. Any remnantentry tear may increase the possibility of enlarge-ment of the false lumen as a late complication.
Intramural hematoma
IMH may be an early stage or a variant of aortic dis-section [80]. In contrast to typical aortic dissection,in which there is an intimal tear, IMH is caused bya spontaneous hemorrhage from the vasa vasorumof the medial layer, which weakens the media with-out an intimal tear. IMH accounts for approxi-mately 13% of acute aortic dissection. Because
Fig. 13. (A) Axial CT image in a patient who has an acute type B aortic dissection. The right kidney is less en-hanced than the left kidney because of slower blood flow through the right renal artery that originates fromthe false lumen of the aorta (arrow). (B) Axial CT image in a different patient demonstrating a chronic type Baortic dissection. Long-standing decreased perfusion to the left kidney resulting from obstruction of the left re-nal artery origin (arrowhead) by the dissection flap has caused atrophy of the left kidney. The right kidney showscompensatory hypertrophy.

Review of CT Angiography of Aorta 473
IMH and typical dissection have similar clinicalmanifestations and risk factors, IMH is commonlyclassified according to the Stanford system for clas-sification of aortic dissection. Some authors recom-mend that IMH of Stanford type A should betreated surgically [81]; others have suggested that,because of the high mortality and morbidity associ-ated with aortic surgery, conservative medical treat-ment with frequent imaging follow-up may bea rational management option [82]. Song andcolleagues [82] hypothesized that the absence ofan intimal tear and the lack of continuous bloodflow in IMH probably indicates a better clinical out-come than in typical aortic dissection. Gerber andcolleagues [65] suggested that one indication forendovascular repair may include an IMH in thedescending aorta with or without a penetratingatherosclerotic ulcer (PAU).
The difficulty with this pathology is that the exactorigin of the intramural bleeding cannot always beverified easily [83]. Ganaha and colleagues [83]suggested that both symptoms and radiologic find-ings (eg, recurrent pain, pleural effusion, and thesize and depth of the ulcerlike projection) may bepredictive of disease progression. Early diagnosisand prompt treatment are critical in improvingthe outcome of patients who have IMH.
The growth patterns of type B aortic dissectionand type B IMH are somewhat different. In patientswho have type B IMH, the affected aortas do nothave a high incidence of enlargement during thefollow-up period but tend to increase in size after1 year. An initial diameter of 40 mm or greaterand the presence of blood flow in the false lumenare important risk factors for enlargement duringthe follow-up period [84]. Several investigatorshave attempted to assess the usefulness of CT find-ings for predicting the progression of aortic IMH toaortic dissection. The maximum aortic diameter(> 50 mm), estimated on the basis of the initialCT scan, is the most important predictive factor ofprogression in type A IMH. Findings in type AIMH, such as thick hematoma with compressionof the true lumen, pericardial effusion, or, less im-portant, pleural effusion, were useful for predictingprogression to aortic dissection [80]. A large hema-toma may indicate active bleeding from the rup-tured vasa vasorum, which may result in increasedweakening of the intima of the affected aorta. Ifthe IMH progresses to typical dissection, especiallyin type A IMH, emergent treatment is mandatory.Patients who have type A IMH develop ulcerlikeprojections significantly more often than do pa-tients who have type B IMH. These ulcerlike projec-tions, which represent new areas of intimaldisruption, can progress to aneurysm formationor overt aortic dissection [85,86].
CT findings
It is important to perform unenhanced CT as thefirst imaging evaluation when aortic dissection issuspected, because contrast material within the ves-sel may obscure IMH. On unenhanced CT scans,characteristic findings include a cuff or crescent ofhigh attenuation and internal displacement of inti-mal calcification. The crescent-shaped area of highattenuation in the aortic wall corresponds to a he-matoma in the medial layer, which may or maynot compress the aortic lumen. The density of theIMH often is higher than that of the normal lumen.Intimal calcifications also may be displaced byIMH.
IMH is characterized by the absence of both anintimal flap and blood flow within its substance.Unlike the false lumen in typical aortic dissection,which has various degrees of enhancement fromone patient to another, the crescent-shaped areaof IMH does not enhance after administration ofcontrast material (Fig. 14). The relationship ofIMH and the thrombosed false lumen with the aor-tic wall is an important factor in their differentia-tion. IMH maintains a constant circumferentialrelationship with the aortic wall, but the throm-bosed false lumen tends to spiral longitudinallyaround the aorta.
Atherosclerotic disease
Atherosclerosis arterial occlusive disease (PAU) isa significant disease in the elderly and has beenshown to progress rapidly after menopause inwomen [87]. Atheromatosis of the thoracic aortahas been recognized as a major source of strokeor systemic embolism [88]. Complex atheroscle-rotic aortic debris is a marker for generalized ath-erosclerosis and well-established atheroscleroticand cardioembolic mechanisms of cerebral ische-mia [89]. Therefore it is important to demonstratethe changes atherosclerosis makes to the mainarteries.
A PAU is an ulceration of atheromatous plaquethat has eroded the inner, elastic layer of the aorticwall, reached the medial layer, and produced a he-matoma in the media. Involvement of the mediasometimes can be complicated by aneurysmal dila-tation or, less frequently, by rupture (Figs. 15 and16) [90]. Some authors have theorized that mostsaccular aneurysms are caused by a PAU [85]. Un-like typical aortic dissection, PAUs most often occurin elderly patients who have severe underlying ath-erosclerosis. Sometimes, a PAU with IMH may oc-cur in a nonemergent or nondissection setting.These ulcers typically involve the aortic arch and de-scending thoracic aorta and rarely occur in the as-cending aorta, where rapid blood flow from the

Yu et al474
Fig. 14. (A) Axial CT image in a patient who has a type A IMH involving the ascending and descending thoracicaorta. Curvilinear hypodensities correspond to the IMH (arrows). (B) Axial CT image in a patient who has a type BIMH (arrow) with calcified aortic adventitia (arrowhead). (C) Axial CT image in a patient who has a type B IMHwith extensive hematoma (arrow) circumferentially within the wall of aorta.
left ventricle provides protection against atheroscle-rosis. They therefore can be distinguished easilyfrom type A aortic dissection or type A IMH. Rarely,type B aortic dissection can occur as a late compli-cation of a PAU.
The initial therapy for PAU is medical manage-ment similar to management for type B aortic dis-section. Surgery is performed in patients whohave hemodynamic instability, persistent pain, aor-tic rupture, distal embolization, or rapid enlarge-ment of the aortic diameter. It is important toemphasize that surgical repair of a PAU generallyis more complicated and extensive than surgicalrepair of typical type B aortic dissection, becausemuch of the aortic wall may have been damagedby ulceration and may have to be replaced. Conse-quently, aortic grafting for PAU may be associatedwith higher morbidity (eg, increased risk of para-plegia) because of a greater compromise of theblood supply to the spinal cord during surgery.
Patients who are asymptomatic and are found in-cidentally to have a PAU should undergo the sameCT follow-up as those who have thoracic aortic an-eurysms, because one third of ulcerlike lesions mayprogress, resulting in mild interval aortic enlarge-ment [85]. When rupture and mediastinal hemor-rhage occur, it is difficult to differentiate betweena ruptured aneurysm and a complicated
atherosclerotic ulcer by imaging findings. In bothcases, immediate surgical treatment is required. Tat-sumi and colleagues [91] suggested that fluorodeox-yglucose positron emission tomography/CT maydetect the metabolic activity of atheroscleroticchanges, which may be useful for monitoring theprogress of the atherosclerotic lesions. PAUs typi-cally are located in the descending and abdominalaorta, which are severely atherosclerotic. In con-trast, in classic aortic dissection, most intimal dis-ruptions also are related to mechanical stress andusually occur at the ascending aorta or aortic arch.The progression of intimal disruption may bemore common in IMH than in PAU [79].
CT findings
In PAU, extensive atherosclerosis and IMH ofvariable extent are visible on unenhanced CT scans.Frequently the IMH is focal because of medial fibro-sis caused by atherosclerosis. Displaced intimalcalcifications are often present.
At CTA, the ulcerlike projection appears as a local-ized blood-filled pouch protruding into the throm-bosed lumen of the aorta, showing the samedegree of contrast enhancement as the aortic lumen.The appearance of the lesion is similar to that ofa peptic ulcer (Fig. 16). Lesions can be single ormultiple. PAU often is associated with thickening

Review of CT Angiography of Aorta 475
Fig. 15. The four stages in the formation of a penetrating atherosclerotic ulcer. (A) Aortic atheroma. (B) Benignintimal plaque ulceration contained in the intima. (C) Medial hematoma with potential adventitial false aneu-rysm. (D) Transmural rupture.
of the aortic wall, which appears enhanced. Athero-matous ulcers that are confined to the intimal layersometimes have a radiologic appearance similar tothat of PAU. Therefore, particular care should betaken in making a diagnosis of PAU if the lesionsare discovered incidentally in an asymptomaticpatient and if associated focal IMH is absent [92].
Traumatic aortic injury
MDCT angiography is very sensitive in detectingtraumatic vascular injuries. To make full use ofMDCT, a well-adjusted scanning protocol consist-ing a thin collimation and bolus tracking after in-jection of intravenous contrast medium is needed.Chest CTA is an excellent initial imaging tool be-cause of its high sensitivity and ease of performancein the trauma patient suspected of having an aorticinjury. Sometimes, however, artifacts and otherlimitations require the use of conventional
aortography for further evaluation [93]. Aortictransaction is the cause of 16% of all deaths frommotor vehicle collisions. Eighty-five percent of pa-tients sustaining an aortic transaction die beforereaching the hospital. Of the remaining survivors,50% die within 24 hours [94].
Acute aortic injury may result in incomplete rup-ture, complete rupture, traumatic aortic dissection,and acute traumatic IMH [95]. CT findings of aorticinjury include blood within the mediastinum, de-formities of the aortic contour, intimal flaps,thrombus or debris protruding into the aorticlumen, the presence of a pseudoaneurysm, or anabrupt tapering of the diameter of the descendingaorta compared with the ascending aorta (pseudo-coarctation) [96].
Incomplete rupture
A combination of traction, torsion, and hydrostaticforces created by differential deceleration of

Yu et al476
Fig. 16. Aortic changes caused by atherosclerosis in different stages. (A) Aortic atheroma. (B) Benign intimal pla-que ulceration (white arrow) contained in the intima. (C) Medial hematoma (white arrow) with potential adven-titial false aneurysm.
thoracic structures can result in aortic rupture. In-complete rupture of the aorta is caused by a limitedpartial circumferential tear in the intima and/or themedia of the aortic wall [97,98]. CT findings typi-cally consist of a saccular outpouching demarcatedfrom the aortic lumen by a collar, usually witha periaortic hematoma (Fig. 17). Because of thefresh hematoma, the density usually is a little high-er than that of the soft tissue adjacent to the aorta inthe unenhanced CT scan. A thin layer of the adven-titia and neighboring tissue form the outer wall ofthe pseudoaneurysm, which requires emergenttreatment by stent grafting or open surgical repairto avoid progression to a complete rupture that car-ries a higher mortality rate.
Complete rupture
In severe aortic injury, the forces mentioned previ-ously can cause complete transection when thetear extends from the intima and media into the ad-ventitial layer [97–99]. This injury results in mas-sive mediastinal and pleural hemorrhage, usuallyleading to hypovolemic shock and, ultimately,death. In approximately 90% of patients who sus-tain blunt traumatic aortic injuries and survive tobe transferred to a hospital, the complete rupture
occurs at the anteromedial aspect of the aortic isth-mus distal to the origin of the left subclavian artery(Fig. 18). The typical appearance of the rupturedisthmus on contrast-enhanced CT is a sleeve of sub-adventitial contrast medium. CT also accuratelyshows hemomediastinum and hemothorax, whichmay be indirect signs of a blunt traumatic aortic in-jury. Although thoracic aortic transections remaina highly lethal injury, hemodynamically stable pa-tients have a low operative mortality, and spinalcord injury is decreased by the use of adjuvant per-fusion techniques that maintain distal aortic perfu-sion during cross-clamping of the aorta [100].
Traumatic aortic dissection
Aortic dissection is less common in the setting ofblunt thoracic trauma than with the complete or in-complete rupture of the aorta [101,102]. Acute hy-pertension and steepness of the pulse wave alongwith the rapid deceleration force sustained by theaorta may cause intimal tears and assist in the distalpropagation of the dissection [102]. The CT signs oftraumatic aortic dissection are similar to those ofthe nontraumatic type, with other associated trau-matic injuries, including pulmonary contusions[103].

Review of CT Angiography of Aorta 477
Fig. 17. (A) Axial CT image demonstrating a contained traumatic aortic transection. A pseudoaneurysm (arrow)has formed at the site of the aortic wall disruption, and the arch is surrounded by a hematoma (arrowheads). (B)A three-dimensional volume-rendered image from a right lateral projection shows the pseudoaneurysm (arrow)at the aortic isthmus.
Traumatic acute intramural hematoma
An IMH is referred to as a dissection that lacks anintimo-medial tear, which is the hallmark of a typ-ical dissection [104,105]. In patients who havetraumatic acute IMH, the thickening of the aorticwall generally is circular. Acute IMH weakens theaorta and may progress either to rupture of theaortic wall externally, leading to a pseudoaneur-ysm, or to inward disruption of the intimal layer,
leading to a communicating aortic dissection.MDCT angiography has been reported to ap-proach a sensitivity of 100% and a negative pre-dictive value of 100% in detecting IMH [106].IMHs usually are hyperattenuating on unen-hanced CT and hypoattenuating compared withthe vessel lumen on contrast-enhanced CT. Identi-fication of the intima can be used to differentiatean acute IMH from a mural thrombus. A mural
Fig. 18. (A) Axial CT image demonstrating a traumatic aortic transection. A pseudoaneurysm (arrow) has formedat the site of the aortic wall disruption, and the arch is surrounded by a hematoma (arrowheads). (B) Axial CTimage at the level of the pulmonary artery (PA) shows extensive mediastinal hematoma with extravasated con-trast material (arrow) indicating a noncontained aortic transection. Ao, descending thoracic aorta.

Yu et al478
thrombus lies on top of the intima, which fre-quently is calcified, whereas an IMH is subintimal[105]. Periaortic hematoma near the level of theaortic isthmus is an indirect sign of aortic injuryand has been identified as a common and sugges-tive finding of aortic rupture. Periaortic hematomanear the level of the diaphragmatic crura is an in-sensitive but relatively specific sign for thoracicaortic injury after blunt trauma [107].
Postoperative changes
Endovascular stent grafting is an established thera-peutic option for abdominal aortic aneurysms. Re-cently, it has emerged as a less invasive therapeuticalternative for aneurysms and dissections of the de-scending thoracic aorta [108]. Endograft therapyfor thoracic aortic disease can be performed safelyin elderly patients with no significant increase inperioperative morbidity or mortality comparedwith younger patients. If the proximal landingzone, defined as the distance from the origin ofthe left subclavian artery to the entry tear of thedissection or the proximal aspect of the descendingaortic aneurysm, is less than 5 mm, covering theleft subclavian artery with graft fabric lengthensthe proximal fixation site and should minimizeproximal endoleaks. Because of the collateralblood flow from the right vertebral artery, circleof Willis, carotid arteries, and the vessels aroundthe thoracic wall and the shoulder, the coverageof the left subclavian artery does not result in is-chemic disease [109,110]. Kern and colleagues[111] advocate endograft therapy, when anatomi-cally possible, as the treatment of choice for tho-racic aortic disease in elderly patients. Reductionin sac diameter after endovascular aneurysm repairis considered a definite indication of treatmentsuccess. If the diameter remains static, it is unclearwhether the treatment has succeeded (because ithas arrested growth) or failed (because there hasbeen no shrinkage). Although early results com-pare favorably with those of conventional opensurgery, several procedure-related complicationshave been described, such as stent-graft dislodg-ment, migration, stent fracture, collapse of thestent, changes in the size and shape of the aorta,and arterial wall injury [112–115].
Migration
Because the attachment sites are not sutured, theremay be movement at the aortic or iliac attachmentsor at points of connection within modular grafts.
Pseudoaneurysm
Arterial wall injury can result in acute retrogradeaortic dissection or pseudoaneurysm formation,
mandating urgent surgical repair. Although pseu-doaneurysm formation at conventional anasto-motic sites is a recognized complication, it rarelyis seen with endografts [114].
Endoleak
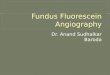
Persistent blood flow in the aortic aneurysm sacoutside the stent graft is called an ‘‘endoleak’’(Fig. 19). The term was coined to distinguish thisperigraft blood flow from aortic rupture with retro-peritoneal or intraperitoneal leak. There are fourtypes of endoleak. Type I endoleak is related tothe stent graft device itself and is caused by an insuf-ficient seal between the proximal portion of the en-dograft and the aortic wall or between the distalportion of the endograft and the iliac artery wall.Type II endoleak is retrograde flow from collateralbranches (lumbar, inferior mesenteric, and acces-sory renal arteries). Type III endoleak is cause byfabric tears, graft wall defect, or modular disconnec-tion or disintegration. Type IV endoleak is flowthrough the graft assumed to be associated withgraft wall porosity, that is, endotension [65]. Themost common branches causing type II endoleakare the fourth lumbar arteries and the inferior mes-enteric artery. Endoleak is recognized by the accu-mulation of contrast medium in the aneurysm sacoutside the stent graft. Contrast-enhanced MDCTperformed during the arterial phase is the methodof choice for detecting endoleaks, although someslow-filling side branch endoleaks may not beseen until a later phase after contrast medium injec-tion. If the sac remains pressurized because ofblood flow, it may enlarge and rupture.
Stenosis
Aortic stenosis, or narrowing of the aortic lumen,has many causes. It may be caused by coarctationor pseudocoarctation of the aorta, midaortic dys-plastic syndrome, atherosclerosis, Takayasu arteri-tis, aortic dissection, various intra-aortic andperiaortic diseases, or surgical aortic repair [116].The impedance of blood flow through the stenoticsegment may lead to the development of collateralarterial pathways that vary according to the locationof stenosis [117]. The site of aortic stenosis varies ac-cording to the disease or condition that caused thestenosis. Stenosis of the proximal descendingthoracic aorta is typical of congenital coarctation,stenosis of the thoracoabdominal aortic junctionoccurs in dysplastic midaortic syndrome, and steno-sis of the abdominal aorta often is secondary toatherosclerosis [115]. In Takayasu arteritis—aorticdissection caused by intra-aortic and periaortic dis-eases or aortic stenosis—stenosis can occur in anypart of the vessel. Thickening of the vessel wall in

Review of CT Angiography of Aorta 479
Fig. 19. Endoleak after endovascular aortic repair. (A) Axial CT image demonstrates an irregular isodensityaround the circular stent within the descending thoracic aorta corresponding to the endoleak (white arrow).The native wall of aorta is thickened (white arrowhead), and the aorta is a little dilated. (B) Sagittal reformattedand (C) three-dimensional volume-rendered images also demonstrate the endoleak (arrows).
Takayasu arteritis is an early sign of the disease andleads to stenosis, thrombosis, and sometimes to an-eurysm formation [118].
Summary
CTA has become a standard noninvasive imagingmethod for depicting vascular anatomy and pathol-ogy during the past decade. It is the most frequentlyused technique when multiple imaging is needed.The quality and speed of CTA is superior to thatof other imaging modalities, and it is cheaper andless invasive. CTA of the aorta has proven to be su-perior to conventional arteriography in diagnosticaccuracy in several applications. It allows three-di-mensional visualization from any angle and inany direction. Proper imaging is of vital importancein diagnosing several cardiac anomalies, such asinterrupted aortic arch, coarctation of the aorta,abdominal aortic aneurysm, aortic rupture, aortic
dissection, IMH, atherosclerotic arterial occlusivedisease, and traumatic aortic injury. For example,in aortic dissection, an intimal flap that separatesthe true lumen from the false lumen is a typicalfinding on contrast CT scan. Accurate differentia-tion between the true and false lumen is importantfor placement of an endovascular stent. In trau-matic aortic injury, multidetector CTA is useful fordetecting complications of vascular emergencies ofthe aorta.
References
[1] Schoenhagen P, Halliburton SS, Stillman AE,et al. Non-invasive imaging of coronary arteries:current and future role of multidetector row CT.Radiology 2004;232:7–17.
[2] Lepor NE, Madyoon H, Friede G. The emerginguse of 16- and 64-slice computed tomographycoronary angiography in clinical cardiovascularpractice. Rev Cardiovasc Med 2005;6:47–53.

Yu et al480
[3] Flohr TG, Schoepf UJ, Kuettner A, et al. Ad-vances in cardiac imaging with 16-section CTsystems. Acad Radiol 2003;10:386–401.
[4] Kuettner A, Beck T, Drosch T, et al. Imagingquality and diagnostic accuracy of non-invasivecoronary imaging with 16-detector slice spiralcomputed tomography with 188ms temporalresection. Heart 2005;91:938–41.
[5] Suzuki T, Mehta RH, Ince H, et al. Clinical pro-files and outcomes of acute type B aortic dissec-tion in the current Era: lessons from theInternational Registry of Aortic Dissection(IRAD). Circulation 2003;108:312–7.
[6] Wintersperger B, Jakobs T, Herzog P, et al. Aorto-iliac multidetector-row CT angiography withlow kV settings: improved vessel enhancementand simultaneous reduction of the radiationdose. Eur Radiol 2005;15:334–41.
[7] Kalva SP, Sahani DV, Hahn PF, et al. Using theK-edge to improve contrast conspicuity and tolower radiation dose with a 16-MDCT: a phan-tom and human study. J Comput Assist Tomogr2006;30:391–7.
[8] Strocchi S, Vite C, Callegari L, et al. Optimisa-tion of multislice computed tomography proto-cols in angio-CT examinations. Radiol Med(Torino) 2006;111:238–44.
[9] Roos JE, Willmann JK, Weishaupt D, et al.Thoracic aorta: motion artifact reduction withretrospective and prospective electrocardiogra-phy-assisted multi-detector row CT. Radiology2002;222:271–7.
[10] Yoshida S, Akiba H, Tamakawa M, et al. Thoracicinvolvement of type A aortic dissection and intra-mural hematoma: diagnostic accuracy—com-parison of emergency helical CT and surgicalfindings. Radiology 2003;228:430–5.
[11] Hofmann LK, Kelly HZ, Philip C, et al. Electro-cardiographically gated 16-section CT of thethorax: cardiac motion suppression. Radiology2004;233:927–33.
[12] Morgan-Hughes GJ, Owens PE, Marshall AJ,et al. Thoracic aorta at multi-detector row CT:motion artifact with various reconstructionwindows. Radiology 2003;228:583–8.
[13] Macari M, Israel GM, Berman P, et al. Infrarenalabdominal aortic aneurysms at multi-detectorrow CT angiography: intravascular enhance-ment without a timing acquisition. Radiology2001;220:519–23.
[14] Shigeki I, Mitsuru I, Masataka A, et al. Multi-phase contrast-enhanced CT of the liver witha multislice CT scanner: effects of iodine con-centration and delivery rate. Radiat Med 2005;23(1):61–9.
[15] Bae KT, Tran HQ, Heiken JP. Uniform vascularcontrast enhancement and reduced contrastmedium volume achieved by using exponen-tially decelerated contrast material injectionmethod. Radiology 2004;231:732–6.
[16] Brink JK. Contrast optimization and scan tim-ing for single and multidetector-row computed
tomography. J Comput Assist Tomogr 2003;27:s3–8.
[17] Feyter PJ, Krestin GP, editors. Computedtomography of the coronary arteries. Abingdon(UK): Taylor & Franics; 2005.
[18] Cademartiri F, Luccichenti G, Marano R, et al.Spiral CT-angiography with one, four, and six-teen slice scanners. Technical note. RadiolMed (Torino) 2003;106:269–83.
[19] Hopper KD, Mosher TJ, Kasales CJ, et al.Thoracic spiral CT: delivery of contrast materialpushed with injectable saline solution ina power injector. Radiology 1997;205:269–71.
[20] Cademaritiri F, mollet N, van der Lugt A, et al.Non-invasive 16-row multislice coronary angi-ography: usefulness of saline chaser. Eur Radiol2004;14:178–83.
[21] Tatsugami F, Matsuki M, Kani H, et al. Effect ofsaline pushing after contrast material injectionin abdominal multidetector computed tomog-raphy with the use of different iodine concen-trations. Acta Radiol 2006;47(2):192–7.
[22] Han JK, Kim AY, Lee KY, et al. Factors influenc-ing vascular and hepatic enhancement at CT:experimental study on injection protocol usinga canine model. J Comput Assist Tomogr 2000;24:400–6.
[23] Fenchel S, Fleiter TR, Aschoff AJ, et al. Effect ofiodine concentration of contrast media on con-trast enhancement in multislice CT of the pan-creas. Br J Radiol 2004;77:821–30.
[24] Awai K, Hiraishi K, Hori Sl. Effect of contrastmaterial injection duration and rate on aorticpeak time and peak enhancement at dynamicCT involving injection protocol with dose tai-lored to patient weight. Radiology 2004;230:142–50.
[25] Thomas A, Bernhard M. New trends in multide-tector computed tomography angiography ofperipheral arteries. Advances in MDCT—an in-ternational literature review service. 2005;2(2):1–6.
[26] Cademartiri F, Nieman K, Lugt AV, et al. Intrave-nous contrast material administration at 16-de-tector row helical CT coronary angiography: testbolus versus bolus-tracking technique. Radiol-ogy 2004;233:817–23.
[27] Catalano C, Fraioli F, Laghi A, et al. Infrarenalaortic and lower-extremity arterial disease: diag-nostic performance of multi-detector row CTangiography. Radiology 2004;231:555–63.
[28] Imai S, Tamada T, Gyoten M, et al. Iatrogenicvenous air embolism caused by CT injector—from a risk management point of view. RadiatMed 2004;22:269–71.
[29] Goo HW, Park Is, Ko JK, et al. CT of congenitalheart disease: normal anatomy and typicalpathologic conditions. Radiographics 2003;23:S147–65.
[30] Ucerler H, Asli Aktan Ikiz Z. Multiplicity of thevariations in ventral branches of abdominalaorta. Ital J Anat Embryol 2006;111(1):15–22.

Review of CT Angiography of Aorta 481
[31] Van De Graaff. Human anatomy. 6th edition.New York: The McGraw�Hill Companies;2001. p. 574–83.
[32] Kawano T, Ishii M, Takagi J, et al. Three-dimen-sional helical computed tomographic angiogra-phy in neonates and infants with complex heartdisease. Am Heart J 2000;139:654–60.
[33] Moon Y, Kim YM, Kim TH, et al. Congenitalanomalies of aortic arch: CT angiography. J Ko-rean Radiol Soc 2001;44:51–8.
[34] Freedom RM, Mawson JB, Yoo SJ, et al. Congen-ital heart disease: textbook of angiocardiogra-phy. Armonk (NY): Futura; 1997.
[35] Didier D, Ratib O, Beghetti M, et al. Morpho-logic and functional evaluation of congenitalheart disease by magnetic resonance imaging.J Magn Reson Imaging 1999;10:639–55.
[36] Roche KJ, Krinsky G, Lee VS, et al. Interruptedaortic arch: diagnosis with gadolinium-en-hanced 3D MRA. J Comput Assist Tomogr 1999;23:197–202.
[37] Haramati LB, Glickstein FS, Issenberg HF, et al.MR imaging and CT of vascular anomalies andconnections in patients with congenital heartdisease: significance in surgical planning. Ra-diographics 2002;22:337–49.
[38] Polson JW, McCallion N, Waki H, et al. Evi-dence for cardiovascular autonomic dysfunc-tion in neonates with coarctation of the aorta.Circulation 2006;113:2844–50.
[39] Marx GR. ‘‘Repaired’’ aortic coarctation inadults: not a ‘‘simple’’ congenital heart defect.J Am Coll Cardiol 2000;35:1003–6.
[40] Kaminishi Y, Kono Y, Kato M, et al. Late pseu-doaneurysm formation after patch angioplastyof coarctation of the aorta; report of a case.Kyobu Geka 2006;59:407–9.
[41] Hager A, Kaemmerer H, Rapp-Bernhardt U, et al.Diameters of the thoracic aorta throughout lifeas measured with helical computed tomography.J Thorac Cardiovasc Surg 2002;123:1060–6.
[42] Malloy PC, Richard HM 3rd. Thoracic angiogra-phy and intervention in trauma. Radiol ClinNorth Am 2006;44(2):239–49, viii.
[43] Gotway MB, Dawn SK. Thoracic aorta imagingwith multislice CT. Radiol Clin North Am2003;41(3):521–43.
[44] Mitchell RS, Dake MD, Sembra CP, et al. Endo-vascular stent-graft repair of thoracic aortic an-eurysms. J Thorac Cardiovasc Surg 1996;111(5):1054–62.
[45] Tatli S, Mortele KJ, Breen EL, et al. Local stagingof rectal cancer using combined pelvic phased-array and endorectal coil MRI. J Magn ResonImaging 2006;23(4):534–40.
[46] Elefteriades JA. Natural history of thoracic aorticaneurysms: indications for surgery, and surgicalversus nonsurgical risks. Ann Thorac Surg 2002;74:S1877–80 [discussion: S1892–8].
[47] Perko MJ, Norgaard M, Herzog TM, et al. Unop-erated aortic aneurysms: a survey of 170 pa-tients. Ann Thorac Surg 1995;59:1204–9.
[48] Crawford ES, DeNatale RW. Thoracoabdominalaortic aneurysm: observations regarding thenatural course of the disease. J Vasc Surg1986;3(4):578–82.
[49] Hello CL, Koskas F, Cluze LP, et al. Frenchwomen from multiplex abdominal aortic aneu-rysm Families should be screened. Ann Surg2005;242:739–44.
[50] Beebe HG, Kritpracha B. Screening and preoper-ative imaging of candidates for conventional re-pair of abdominal aortic aneurysm. Semin VascSurg 1999;12:300–5.
[51] Ashton HA, Buxton MJ, Day NE, et al. Multi-centre Aneurysm Screening Study Group. Multi-centre Aneurysm Screening Study (MASS) intothe effect of abdominal aortic aneurysm screen-ing on mortality in men: a randomized con-trolled trial. Lancet 2002;360:1531–9.
[52] Beard JD. Screening for abdominal aortic aneu-rysm. Br J Surg 2003;90:515–6.
[53] Fleming C, Whitlock EP, Beil TL, et al. Screeningfor abdominal aortic aneurysm: a best-evidencesystematic review for the U.S. preventive servicestask force. Ann Intern Med 2005;142:203–11.
[54] Upchurch GR, Schaub TA. Abdominal aortic an-eurysm. Am Fam Physician 2006;73:1198–204.
[55] Kapoor V, Kanal El, Fukui MB, et al. Vertebralmass resulting from a chronic-contained rup-ture of an abdominal aortic aneurysm repairgraft. AJNR Am J Neuroradiol 2001;22:1775–7.
[56] Medina CR, Indes J, Smith C. Endovascular treat-ment of an abdominal aortic pseudoaneurysmas a late complication of inferior vena cava filterplacement. J Vasc Surg 2006;43(6):1278–82.
[57] Palanichamy N, Gregoric ID, La Francesca S,et al. Mycotic pseudo-aneurysm of the ascend-ing thoracic aorta after cardiac transplantation.J Heart Lung Transplant 2006;25(6):730–3.
[58] Kleinstreuer C, Li LH. Analysis and computerprogram for rupture-risk prediction of abdomi-nal aortic aneurysms. Biomed Eng Online2006;5:19.
[59] Ando M, Igari T, Yokoyama H, et al. CT featuresof chronic contained rupture of an abdominalaortic aneurysm. Ann Thorac Cardiovasc Surg2003;9:274–8.
[60] Dorrucci V, Dusi R, Rombola G, et al. Con-tained rupture of an abdominal aortic aneu-rysm presenting as obstructive jaundice: reportof a case. Surg Today 2001;31:331–2.
[61] Tuma MA, Hans SS. Rupture of abdominal aor-tic aneurysm with tear of inferior vena cava ina patient with prior endograft. J Vasc Surg2002;35:798–800.
[62] Patel SN, Kettner NW. Abdominal aortic aneu-rysm presenting as back pain to a chiropracticclinic: a case report. J Manipulative PhysiolTher 2006;29(5):409, e1–7.
[63] Oderich GS, Panneton JM, Bower TC, et al.Infected aortic aneurysms: aggressive presenta-tion, complicated early outcome, but durableresults. J Vasc Surg 2001;34:900–8.

Yu et al482
[64] Sungjin Oh, Young WY, Gil JJ, et al. Spontane-ous disruption of mycotic aneurysm involvinginnominate artery. J Korean Med Sci 2003;18:589–91.
[65] Gerber M, Immer FF, Do DD, et al. Endovascu-lar stent-grafting for diseases of the descendingthoracic aorta. Swiss Med Wkly 2003;133:44–51.
[66] Drury D, Michaels JA, Jones L, et al. Systematicreview of recent evidence for the safety and effi-cacy of elective endovascular repair in the man-agement of infrarenal abdominal aorticaneurysm [review]. Br J Surg 2005;92(8):937–46.
[67] Wolf YG, Tillich M, Lee WA, et al. Impact of aor-toiliac tortuosity on endovascular repair of ab-dominal aortic aneurysms: evaluation of 3Dcomputer-based assessment. J Vasc Surg 2001;34:594–9.
[68] Kato K, Ishiguchi T, Maruyama K, et al. Accu-racy of plastic replica of aortic aneurysm using3D-CT data for transluminal stent-grafting: ex-perimental and clinical evaluation. J ComputAssist Tomogr 2001;25:300–4.
[69] Whitaker SC. Imaging of abdominal aortic an-eurysm before and after endoluminal stent-graftrepair [review]. Eur J Radiol 2001;39(1):3–15.
[70] Fukuhara R, Ishiguchi T, Ikeda M, et al. Evalua-tion of abdominal aortic aneurysm for endovas-cular stent-grafting with volume-rendered CTimages of vessel lumen and thrombus. RadiatMed 2004;22:332–41.
[71] Khan IA, Nair CK. Clinical diagnostic and man-agement perspectives of aortic dissection. Chest2002;122:311–28.
[72] Iyano K, Kawada T, Aiba M, et al. Correlation ofhemostatic molecular markers and morphologyof the residual false lumen in chronic aortic dis-section. Ann Thorac Cardiovasc Surg 2004;10:106–12.
[73] Shimazaki Y, Minowa T, Watanabe T, et al.Acute aortic dissection with new massive cere-bral infarction—a successful repair with ligatureof the right common carotid artery. Ann ThoracCardiovasc Surg 2004;10:64–6.
[74] Daitoku K, Fukui K, Tamo W, et al. Emergencysmall-sized stent placement following aortictrue lumen obliteration of Stanford type B acuteaortic dissection. Kyobu Geka 2006;59:445–8.
[75] Xu SD, Huang FJ, Yang JF, et al. Endovascular re-pair of acute type B aortic dissection: early andmid-term results. J Vasc Surg 2006;43(6):1090–5.
[76] Sueyoshi E, Sakamoto I, Hayashi K, et al.Growth rate of aortic diameter in patientswith type B aortic dissection during the chronicphase. Circulation 2004;110(Suppl II):256–61.
[77] Hartnell GG, Gates J. Aortic fenestration: a why,when, and how-to guide. Radiographics 2005;25(1):175–89.
[78] Eijun S, Ichiro S, Kuniaki H, et al. Growth rateof aortic diameter in patients with Type B aortic
dissection during the chronic phase. Circula-tion 2004;110(Suppl 2):256–61.
[79] LePage M, Quint LE, Sonnad SS, et al. Aorticdissection: CT features that distinguish true lu-men from false lumen. AJR Am J Roentgenol2001;177:207–11.
[80] Choi SH, Choi SJ, Kim JH, et al. Useful CT find-ings for predicting the progression of aortic in-tramural hematoma to overt aortic dissection.J Comput Assist Tomogr 2001;25:295–9.
[81] Rerkpattanapipat P, Jacobs LE, Makornwattana P,et al. Meta-analysis of 143 reported cases of aorticintramural hematoma. Am J Cardiol 2000;86:664–8.
[82] Song JK, Kim HS, Kang DH, et al. Different clin-ical features of aortic intramural hematoma ver-sus dissection involving the ascending aorta.J Am Coll Cardiol 2001;37:1604–10.
[83] Ganaha n, Fumikiyo n, Miller n, et al. Prognosisof aortic intramural hematoma with and with-out penetrating atherosclerotic ulcer: a clinicaland radiological analysis. Circulation 2002;106:342–8.
[84] Sueyoshi E, Sakamoto I, Uetani, et al. MCTanalysis of the growth rate of aortic diameter af-fected by acute type B intramural hematoma.AJR Am J Roentgenol 2006;186(6 Suppl 2):S414–20.
[85] Quint LE, Williams DM, Francis IR, et al. Ulcer-like lesions of the aorta: imaging features andnatural history. Radiology 2001;218:719–23.
[86] Sueyoshi E, Matsuoka Y, Imada T, et al. New de-velopment of an ulcerlike projection in aorticintramural hematoma: CT evaluation. Radiol-ogy 2002;224:536–41.
[87] Welty FK. Cardiovascular disease and dyslipide-mia in women. Arch Intern Med 2001;161:514–22.
[88] Casella G, Greco C, Perugini E, et al. [Athero-matosis of the thoracic aorta and risk of stroke].G Ital Cardiol (Rome) 2006;7(5):309–16 [inItalian].
[89] Petty GW, Khandheria BK, Meissner I, et al.Population-based study of the relationship be-tween atherosclerotic aortic debris and cerebro-vascular ischemic events. Mayo Clin Proc 2006;81(5):609–14.
[90] Castaner Eva, Andreu M, Gallardo X, et al. CT innontraumatic acute thoracic aortic disease: typ-ical and atypical features and complications.Radiographics 2003;23:S93–110.
[91] Tatsumi M, Cohade C, Nakamoto Y, et al. Fluo-rodeoxyglucose uptake in the aortic wall at PET/CT: possible finding for active atherosclerosis.Radiology 2003;229:831–7.
[92] Hayashi H, Matsuoka Y, Sakamoto I, et al. Pen-etrating atherosclerotic ulcer of the aorta: imag-ing features and disease concept. Radiographics2000;20:995–1005.
[93] Bruckner BA, DiBardino DJ, Cumbie TC, et al.Critical evaluation of chest computed tomog-raphy scans for blunt descending thoracic

Review of CT Angiography of Aorta 483
aortic injury. Ann Thorac Surg 2006;81(4):1339–46.
[94] Trerotola SO. Can helical CT replace aortogra-phy in thoracic trauma. Radiology 1995;197:13–5.
[95] Alkadhi H, Wildermuth S, Desbiolles L, et al.Vascular emergencies of the thorax after bluntand iatrogenic trauma: multi–detector row CTand three-dimensional imaging. Radiographics2004;24:1239–55.
[96] Kuhlman JE, Pozniak MA, Collins J, et al. Ra-diographic and CT findings of blunt chesttrauma: aortic injuries and looking beyondthem. Radiographics 1998;18:1085–106.
[97] Wintermark M, Wicky S, Schnyder P. Imaging ofacute traumatic injuries of the thoracic aorta.Eur Radiol 2002;12:431–42.
[98] Macura KJ, Corl FM, Fishman EK, et al. Patho-genesis in acute aortic syndromes: aortic aneu-rysm leak and rupture and traumatic aortictransaction. AJR Am J Roentgenol 2003;181:303–7.
[99] Richens D, Field M, Neale M, et al. The mecha-nism of injury in blunt traumatic rupture of theaorta. Eur J Cardiothorac Surg 2002;21:288–93.
[100] Crestanello JA, Zehr KJ, Mullany CJ, et al. Theeffect of adjuvant perfusion techniques on theincidence of paraplegia after repair of traumaticthoracic aortic transections. Mayo Clin Proc2006;81(5):625–30.
[101] Mimasaka S, Yajima Y, Hashiyada M, et al. Acase of aortic dissection caused by blunt chesttrauma. Forensic Sci Int 2003;132:5–8.
[102] Bashar AH, Kazui T, Washiyama N, et al. Stan-ford type A aortic dissection after blunt chesttrauma: case report with a reflection on themechanism of injury. J Trauma 2002;52:380–1.
[103] Yokoyama S, Maeda Y, Maisawa K, et al. Ascend-ing aortic dissection associated with pulmonarycontusion caused by blunt trauma. Kyobu Geka2006;59(5):383–6.
[104] Vilacosta I, Roman JA. Acute aortic syndrome.Heart 2001;85:365–8.
[105] Macura KJ, Corl FM, Fishman EK, et al. Patho-genesis in acute aortic syndromes: aortic dissec-tion, intramural hematoma, and penetratingatherosclerotic aortic ulcer. AJR Am J Roentgenol2003;181:309–16.
[106] Dyer DS, Moore EE, Ilke DN, et al. Thoracic aor-tic injury: how predictive is mechanism and is
chest-computed tomography a reliable screen-ing tool? A prospective study of 1,561 patients.J Trauma 2000;48:673–82 [discussion: 682–3].
[107] Wong H, Gotway MB, Sasson AD, et al. Peri-aortic hematoma at diaphragmatic crura at heli-cal CT: sign of blunt aortic injury in patientswith mediastinal hematoma. Radiology 2004;231:185–9.
[108] Fattori R, Napoli G, Lovato L, et al. Descendingthoracic aortic diseases: stent-graft repair. Radi-ology 2003;229:176–83.
[109] Lawlor Dk, Michael O, Thomas LF, et al. Endo-vascular management of traumatic thoracic aor-tic injuries. Can J Surg 2005;48(4):293–7.
[110] Fu WG, Dong ZH, Wang YQ, et al. Strategies forthe insufficiency of the proximal landing zoomduring endovascular thoracic aortic repair. ChinMed J (Engl) 2005;118(13):1066–71.
[111] Kern JA, Matsumoto AH, Tribble CG, et al. Tho-racic aortic endografting is the treatment ofchoice for elderly patients with thoracic aorticdisease. Ann Surg 2006;243(6):815–20 [discus-sion: 820–3].
[112] Bethuyne N, Bove T, Van den Brande P, et al.Acute retrograde aortic dissection during endo-vascular repair of a thoracic aortic aneurysm.Ann Thorac Surg 2003;75:1967–9.
[113] Kato N, Hirano T, Kawaguchi T, et al. Aneurys-mal degeneration of the aorta after stent-graftrepair of acute aortic dissection. J Vasc Surg2001;34:513–8.
[114] Chen FH, Shim WH, Chang BC, et al. False an-eurysms at both ends of a descending thoracicaortic stent-graft: complication after endovascu-lar repair of a penetrating atherosclerotic ulcer.J Endovasc Ther 2003;10:249–53.
[115] Mestres G, Maeso J, Fernandez V, et al. Symp-tomatic collapse of a thoracic aorta endopros-thesis. J Vasc Surg 2006;43(6):1270–3.
[116] Carmen Sebastia, Sergi Quiroga, Rosa Boye’,et al. Aortic stenosis: spectrum of diseases de-picted at multisection CT. Radiographics 2003;23:S79–91.
[117] Yurdakul M, Tola M, Ozdemir E, et al. Internalthoracic artery-inferior epigastric artery as a col-lateral pathway in aortoiliac occlusive disease.J Vasc Surg 2006;43(4):707–13.
[118] Quemeneur T, Hachulla E, Lambert M, et al. Ta-kayasu arteritis. Presse Med 2006;35(5 Pt 2):847–56.