Embed Size (px)
Citation preview
Re
view of w indow restrictors used in he alth and social care
Pre pared by the Health and Safety Executive
RR1150 Research Report
© Crown copyright 2019
Prepared 2015
First published 2019
You may reuse this information (not including logos) free of charge in
any format or medium, under the terms of the Open Government Licence. To view the licence visit ww w.nationalarchives.gov.uk/doc/open-government-licence/, write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email [email protected].
Some images and illustrations may not be owned b y the Crown so
can not be reproduced without permission of the copyright owner. Enquiries should be sent to [email protected].
Serious injuries and fatalities have occurred when people
have fallen from windows in health and social care
premises. A vulnerable person may fall unintentionally when they are in a confused mental state, such as a person with dementia, or as a deliberate act of self-harm. Window restrictors may be used as part of managing the risk of
vulnerable people falling from windows. However, there is a lack of evidence-based advice on the minimum force that w indow restrictors should withstand for use in health and social care premises to protect vulnerable people.
This report describes research to identify the force that c ould reasonably be applied by an individual determined to
open a window that is above waist height. The researchers r eviewed: incidents involving window restrictors; standards for design, production and installation of window r estrictors; and ergonomic data. The researchers suggest
that for windows that are above waist height, window r estrictors and their fixings should be capable of withstanding at least 850 N. This is based on an adult
e xerting a static push force with both hands, pushing outwards on a handle at shoulder height in a non-braced, f orward leaning posture. Where adults can use excessive force, body weight, impact or momentum to try to break or
open a window, it would not be appropriate to rely on a force guide of 850 N.
HSE Information Sheet ‘Falls from windows or balconies in
health and social care’ HIS5 (2012) gives related information for providers of health and social care services.
This report and the work it describes were funded by the Health and
Safety Executive (HSE). Its contents, includingany opinions and/or
conclusions expressed, are those of the authors a lone and do not
necessarily reflect HSE policy.
2
ipiscing elit
3
ReL voierew m of wi psindum ow d roelsotrric stors it a umesed t in he
caolth ns aencd t esoctuiael rc aarde
Rob ert White and Elizabeth Yeomans Health and Safety Executive Harpur Hill
Buxton Der byshire SK17 9JN

KEY MESSAGES
Serious injuries and fatalities have occurred when people have fallen from windows in health and social care premises. A vulnerable person may fall unintentionally when they are in a confused mental state, such as a person with dementia, or as a deliberate act of self-harm. These premises may use windowrestrictors as part of managing the risk of vulnerable people falling from windows. A window restrictor is a device used to limit how wide a window can open. However, there is a lack of evidence-based advice on the minimum force that window restrictors should withstand for use in health and social care premises to protect vulnerable people.
This report describes research to identify the force that an individual who is determined to open a window that is above waist height could reasonably apply. The research involved reviewing: incidents involving windowrestrictors; current standards for the design, production and installation of window restrictors; and ergonomic data on maximum forces that people can apply to open windows above waist height. The research identified the following.
As a guide, it is suggested that window restrictors (and their fixings) are capable of withstanding push forces of at least 850 N in order to protect vulnerable people in health and social care premises. This applies to windows that are above waist height. The research bases this finding on ergonomic data where an adult male exerts a static push force with both hands, pushing outwards on a handle at shoulder height in a non -braced, forward leaning posture.
In some situations people may be able to use excessive force, body weight, impact or momentum to try to break or open a window, for example, by throwing a chair at a window. Whether this is likely to occur would need to be considered on a case-by-case basis. In these circumstances, the suggested force guide of 850 N would not be appropriate to rely on. Additionally, the potential of falls from windows because the glazing breaks, or other window components fail, may become more significant if excessive force is used.
Many commercial available window restrictors have a manufacturers stated minimum strength of 600 N based on the requirements of the superseded British Standard BS 6375-2:1987. The current British and European standards for window restrictors appear to consider normal day-to-day use, not what would be required to prevent the determined effort of a vulnerable individual to open a window as a means of exit. They have a lower minimum strength requirement than earlier superseded standards.
Other aspects of window restrictors are also an important consideration. Incidents
have occurred where: the window restrictor became ineffective because of degradation, wear and / or poor maintenance during service; the way in which the window was restricted was defeated or disabled; or the window restrictor allowed too large an opening.
4

EXECUTIVE SUMMARY
Background
Serious injuries and fatalities have occurred when people have fallen from windows in health and social care premises. A vulnerable person may fall unintentionally when they are in a confused mental state, such as a person with dementia, or as a deliberate act of self -harm. These premises may use windowrestrictors as part of managing the risk of vulnerable people falling from windows. A window restrictor is a device used to limit the opening of a window.
However, there is a lack of evidence-based advice on the minimum force that window restrictors should withstand for use in health and social care premises to protect vulnerable people.
Aim
This report describes research to identify the level of force that a determined individual could reasonably apply when attempting to open a window and to compare that with the level of force currently used in the design of window restrictors. The research was carried out in 2014.
Methods
The research comprised a review of the following.
1) Incidents involving window restrictors, commenting on causes and identifying any links or patterns between these occurrences.
2) Current standards for window restrictors including any associated standards and guidance, such as that relating to burglar resistance and fire safety.
3) Designs and technology currently used in the production of window restrictors.
4) Closest equivalent ergonomic data concerning the maximum forces that an individual could apply to open windows above waist height.
Findings and Conclusions
1. Incident Review
In a number of cases, incidents occurred because there was no window restrictor. In other instances, there was a window restrictor, but the window itself or its components failed. In the incidents where therewas a window restrictor, but this was inadequate, the following types of failure were identified:
• The window restrictor was not strong enough to withstand the forces that the individual was applying.
5

• The window restrictor became ineffective because of degradation, wear and / or poor maintenance during service.
• The way in which the window was restricted was defeated or disabled.
• The window restrictor allowed too large an opening to prevent the incident occurring.
2. Current Standards
The current standards for window restrictors in Britain and Europe appear to consider normal day-to-day use, not deliberate attempts to defeat a window restrictor. The Department of Healths 2013 best practice guidance on healthcare buildings1 recognises this:
window restrictors tested to current British Standards may be inadequate in preventing a determined effort to force a window open beyond the 100 mm restriction. The relevant tests for restrictors cited in BS EN 14351-1 and BS EN 13126-5 have been developed to prevent accidental falling from windows. BS EN 14351-1 recommends that restrictors must be able to hold a window in place for 60 seconds when a static load of 350 newtons is applied to that window.
However, these static loads may not be sufficient to prevent determined patients who want to force the window beyond its 100 mm restriction. None of the British and European Standards dealwith deliberate attempts to defeat the restrictor using impact forces, which may be the situation encountered in hospitals and care homes;”
Older, superseded, standards had higher requirements for restrictor strength. Many manufacturers still supply to the superseded British Standard BS 6375-2:1987. Manufacturers often quote a minimum strength of 600 N for their restrictors based on the requirements of this standard.
3. Designs and Technology
The designs used as a basis for commercially available window restrictors are broadly consistent. The nature of the restriction is either tension (using flexible or rigid links) or compression (using brackets or track-based stops). The design of most restrictors allows retrospective fitting. However, track-based stops willgenerally be specified as an option during procurement of the windows.
1 Department of Health (2013) Health Building Note 00-10 Part D: Windows and associated hardware. Available at https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_da ta/file/273867/20131223_HBN_00-10_PartD_FINAL_published_version.pdf (Accessed 26/4/13.)
6

4. Ergonomics Data and Analysis
A review of available ergonomics data indicated that adult males could easily achieve forces well in excess of 350 N from a range of postures. Therefore , to offer sufficient protection in circumstances where individuals can brace against objects, use body weight, momentum or impact, or use the body to wedge or lever the window, restrictors would need to be able to withstand forces significantly in excess of that specified under the tests cited in the current standards.
Setting a reasonable strength criterion for window restrictors is not a straightforward matter. Ergonomics data replicating the scenario of applying determined effort against a restrictor is not available. The static pushing forces that an adult male can apply may be a good starting point. Strength data for adult males is likely to exceed the capabilities of other groups (such as the young or elderly). The maximum static push force that adult males can exert with both hands, pushing outwards on a handle at shoulder height in a non -braced, forward leaning posture is 833 N. A window restrictor that can withstand 833 N of push force may offer protection for 99% of the population. However, because of the difficulty extrapolating these maximum force figures to the general population and to this particular situation, we suggest that a guide figure of withstanding 850 N push force would be appropriate to offer a further margin of safety.
In some situations people may be use excessive force, body weight, impact or momentum to try to break or open a window. For example, if:
the force is applied from an alternative posture such as one foot forward, the other back, leaning forward significantly;
the person is able to brace themselves against a supporting structure when applying the force;
the force is applied with another part of the body such as a push with the shoulder;
the force applied is an impact force rather than a gradually applied force such as a shove; and;
the force applied is an impact force using an object such as throwing a chair at the window.
Whether this is likely to occur would need to be considered on a case -by-case basis. In these circumstances, the suggested force guide of 850 N would not be appropriate to rely on. Additionally, the potential of falls from windows because the glazing breaks, or other window components fail, may become more significant if excessive force is used.
7
CONTENTS
KEY MESSAGES ................................................................................................................. 4
EXECUTIVE SUMMARY ..................................................................................................... 5
1 INTRODUCTION ..................................................................................................10
2 FATAL INCIDENTS INVOLVING WINDOW RESTRICTORS...................................11 2.1 RIDDOR Database ...............................................................................................11 2.2 HSE press releases ..............................................................................................11 2.3 Reports from HSEs laboratory ...........................................................................12 2.4 BBC News articles ...............................................................................................13 2.5 Summary .............................................................................................................15
3 CURRENT DESIGNS OF WINDOW RESTRICTORS ...............................................17 3.1 Devices which are loaded in tension ..................................................................17 3.2 Devices which are loaded in compression..........................................................18 3.3 Summary of restrictor designs............................................................................18
4 CURRENT STANDARDS AND GUIDANCE APPLICABLE TO WINDOW RESTRICTORS ..................................................................................................................20 4.1 British and European standards .........................................................................20 4.2 Guidance for hospitals and other buildings........................................................24 4.3 Assessment of standards and guidance .............................................................28
5 MAXIMUM FORCES THAT CAN BE APPLIED BY DETERMINED ADULTS TO OPEN WINDOWS AND THE FORCES THAT CAN BE APPLIED ABOVE WAIST HEIGHT.............30 5.1 Static strength anthropometric data for adult populations ...............................30 5.2 Static strength anthropometric data for older adults ........................................31 5.3 Impact forces ......................................................................................................32 5.4 Impact performance levels for glazing ...............................................................33 5.5 Summary .............................................................................................................33
6 IMPLICATIONS ....................................................................................................36 6.1 The current situation ..........................................................................................36 6.2 Conclusions .........................................................................................................36
7 REFERENCES........................................................................................................38
APPENDIX 1 – HSE’S INFORM!TION ON ‘RISK OF FALLING FROM WINDOWS’...........43 Risks from glazing ...........................................................................................................43 Falls from windows and balconies..................................................................................43 Further information ........................................................................................................43
8

.................................................................................APPENDIX 2 – ERGONOMIC DATA 44
9
1 INTRODUCTION
A window restrictor is a mechanism used to restrict or limit the opening of a window. Window restrictors are commonly used in health and social care as part of managing the risk of vulnerable people falling from windows.
There have been a number of incidents whererestrictors have failed to provide the anticipated level of protection. Between 2005 and 2010, there were 21 fatalities, reported under RIDDOR (The Reporting of Injuries, Diseases and Dangerous Occurrences Regulations) relating to falls from windows in health and social care. Between November 2011 and May 2012, 5 fatal notifications were received. Of these, a number related to the failure to provide suitably robust restrictors.
Attempts to open restricted windows may include an element of determination. Dementia, senility and confusion can lead to individuals trying to force their way through a window in an attempt to escape from abuilding. Alternatively, falls can result from deliberate acts of self-harm or suicide. The Health and Safety Executive(HSE) have prepared an information sheet on this topic (which has been included as Appendix 1).
It is possible that the requirements in standards and guidance relating to window restrictors are based on day-to-day use by the general population rather than vulnerable adults who are determined to escape.
This work aims to identify the level of force that could reasonably be applied by a determined adult attempting to open a window and to compare that with the level of force currently being used in the design of window restrictors.
In order to achieve that comparison, the research comprised the following activities:
1. A review of incidents involving window restrictors, commenting on causes and identifying any links or patterns between these occurrences;
2. A review of designs and technology currently used in the production of window restrictors;
3. A critical review of current standards for window restrictors including any associated standards and guidance (such as that relating to burglar resistance and fire safety);
4. A review of closest equivalent ergonomic data concerning the maximum forces that could be applied to open windows above waist height.
This report summarises the findings of each of these reviews and makes recommendations based upon those findings.
10
2 FATAL INCIDENTS INVOLVING WINDOW RESTRICTORS
To gain a fuller understanding of the role of window restrictors during incidents it was necessary to undertake a qualitative analysis of the cause of each incident. Reports containing descriptive text relating to the incident are likely to provide more useful information than statistical data. The following sources of potentially useful descriptive text were identified: the HSE RIDDOR database, HSE press releases, incident reports by HSEs laboratory (the Health and Safety Laboratory, HSL) and BBC News Reports.
2.1 RIDDOR DATABASE
Under the Reportable Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) there is a statutory obligation to report incidents, dangerous occurrences and near misses occurring at work (or in connection to work). A search of HSEs RIDDOR database was attempted. However, there was not sufficient detail contained within the text fields of individualreports to differentiate between relevant cases and other types of incident involving work at height. Therefore, it was not possible to obtain useful descriptions of incidents from the RIDDOR database.
2.2 HSE PRESS RELEASES
HSE produce press releases summarising incident events, their causes and outcomes. Sharing this information could reduce the likelihood of similar incidents occurring. By definition the information within these releases is in the public domain and therefore freely available.
HSE provided a number of press releases, dated between 2010 and 2013, relating to fatal incidents where window restrictors, or the absence thereof , may have been a contributory factor. Eight of these press releases formed the starting point of the review of incidents. Table 1 summarises the details of these incidents.
11
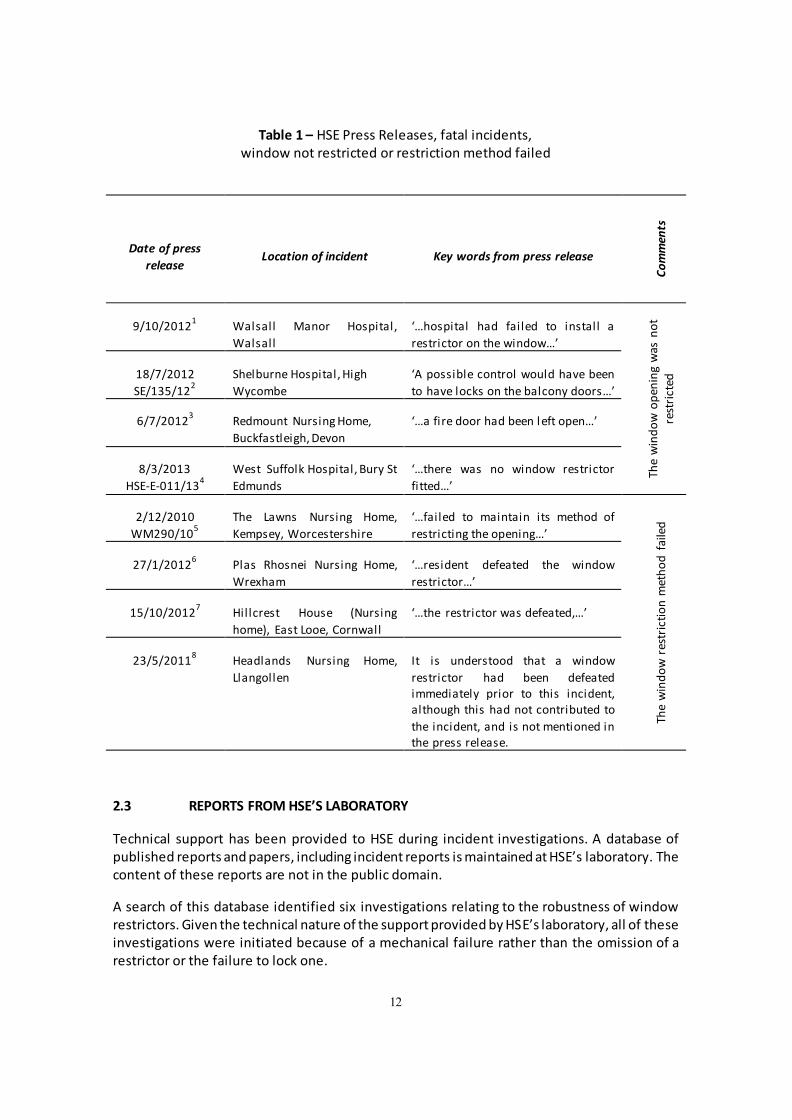
Table 1 – HSE Press Releases, fatal incidents, window not restricted or restriction method failed
Date of press
release Location of incident Key words from press release
Co
mm
ents
9/10/20121
Walsall Manor Hospital,
Walsall
/hospital had failed to install a
restrictor on the window/
to
n s aw g
in d
en te icp ro t w
serod
inw
e hT
18/7/2012
SE/135/122
Shelburne Hospital, High
Wycombe
! possible control would have been
to have locks on the balcony doors/
6/7/20123
Redmount Nursing Home,
Buckfastleigh, Devon
/a fire door had been l eft open/
8/3/2013
HSE-E-011/134
West Suffolk Hospital, Bury St
Edmunds
/there was no window restrictor
fitted/
2/12/2010
WM290/105
The Lawns Nursing Home,
Kempsey, Worcestershire
/failed to maintain its method of
restricting the opening/
The
win
do
w r
estr
icti
on
met
ho
d f
aile
d
27/1/20126
Plas Rhosnei Nursing Home,
Wrexham
/resident defeated the window
restrictor/
15/10/20127
Hillcrest House (Nursing
home), East Looe, Cornwall
/the restrictor was defeated,/
23/5/20118
Headlands Nursing Home,
Llangollen
It is understood that a window
restrictor had been defeated immediately prior to this incident, although this had not contributed to
the incident, and is not mentioned in the press release.
2.3 REPORTS FROM HSE’S L!BOR!TORY
Technical support has been provided to HSE during incident investigations. A database of published reports and papers, including incident reports is maintained at HSEs laboratory. The content of these reports are not in the public domain.
A search of this database identified six investigations relating to the robustness of window restrictors. Given the technical nature of the support provided by HSEs laboratory, all of these investigations were initiated because of a mechanical failure rather than the omission of a restrictor or the failure to lock one.
12
In four cases the window restrictor had failed. These included the incident that occurred at Plas Rhosnei, Wrexham which has previously been described in Table 1 and Reference 6.
In two instances part of a window or window opening mechanism had failed. This was not the part of the window designed to restrict the opening. However the opening of these windows was intended to be restricted, and the windowfailure allowed this restriction to be overcome.
2.4 BBC NEWS ARTICLES
An internet search was undertaken to identify news reports relating to the performance of window restrictors. A single news source, in this case the British Broadcasting Corporation (BBC), was used to eliminateduplication. The BBC was selected as a reputable, public service news provider with national coverage.
The internet search was undertaken using two key word combinations BBC + window + restrictor and BBC + hospital + window. These searches identified eleven articles of potential interest.
In most cases, the articles do not contain detailed information about the incidents. The articles are listed in Table 2, where comments about each incident have been included. Three of the incidents listed in HSE press releases were also reported by the BBC, and this has been cross referenced in the table. It should be noted that where incidents were reported by duplicate sources there may be minor discrepancies between reports.
13
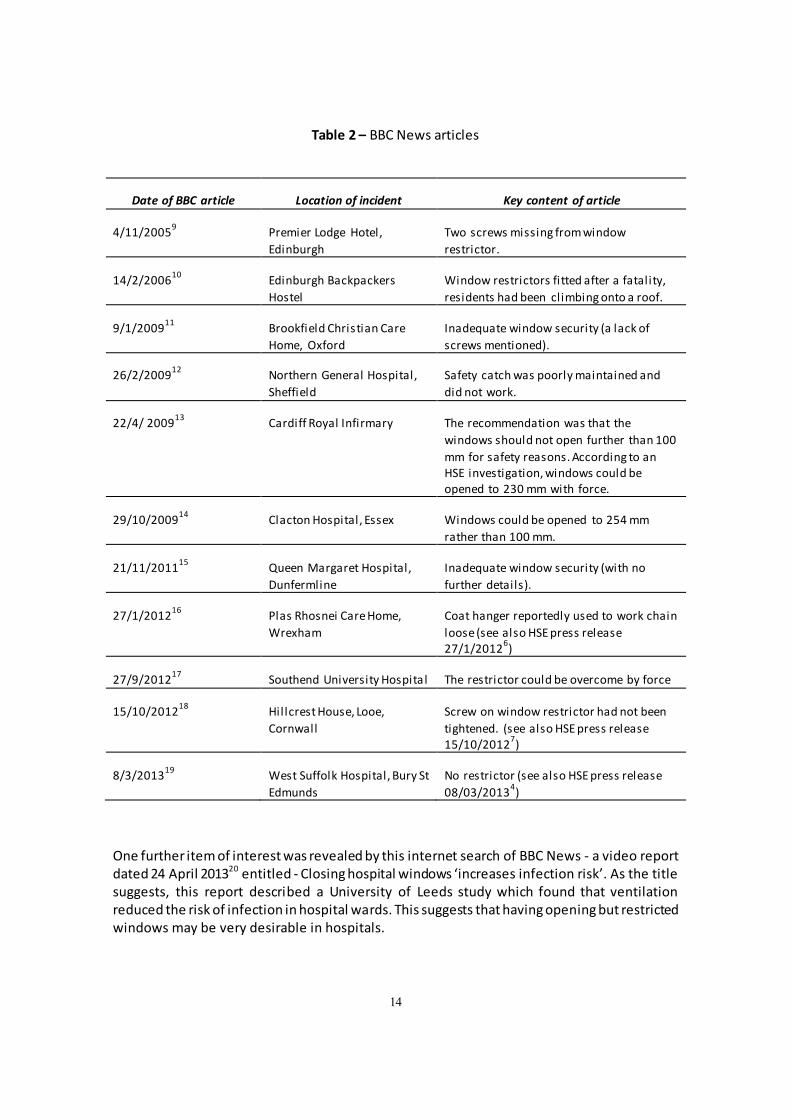
Table 2 – BBC News articles
Date of BBC article Location of incident Key content of article
4/11/20059
Premier Lodge Hotel,
Edinburgh
Two screws missing from window
restrictor.
14/2/200610
Edinburgh Backpackers
Hostel
Window restrictors fitted after a fatality,
residents had been climbing onto a roof.
9/1/200911
Brookfield Christian Care
Home, Oxford
Inadequate window security (a lack of
screws mentioned).
26/2/200912
Northern General Hospital,
Sheffield
Safety catch was poorly maintained and
did not work.
22/4/ 200913
Cardiff Royal Infirmary The recommendation was that the
windows should not open further than 100
mm for safety reasons. According to an HSE investigation, windows could be opened to 230 mm with force.
29/10/200914
Clacton Hospital, Essex Windows could be opened to 254 mm
rather than 100 mm.
21/11/201115
Queen Margaret Hospital,
Dunfermline
Inadequate window security (with no
further details).
27/1/201216
Plas Rhosnei Care Home,
Wrexham
Coat hanger reportedly used to work chain
loose (see also HSE press release 27/1/2012
6)
27/9/201217
Southend University Hospital The restrictor could be overcome by force
15/10/201218
Hillcrest House, Looe,
Cornwall
Screw on window restrictor had not been
tightened. (see also HSE press release 15/10/2012
7)
8/3/201319
West Suffolk Hospital, Bury St
Edmunds
No restrictor (see also HSE press release
08/03/20134)
One further item of interest was revealed by this internet search of BBC News - a video report dated 24 A pril 201320 entitled - �losing hospital windows increases infection risk. !s the title suggests, this report described a University of Leeds study which found that ventilation reduced the risk of infection in hospital wards. This suggests that having opening but restricted windows may be very desirable in hospitals.
14
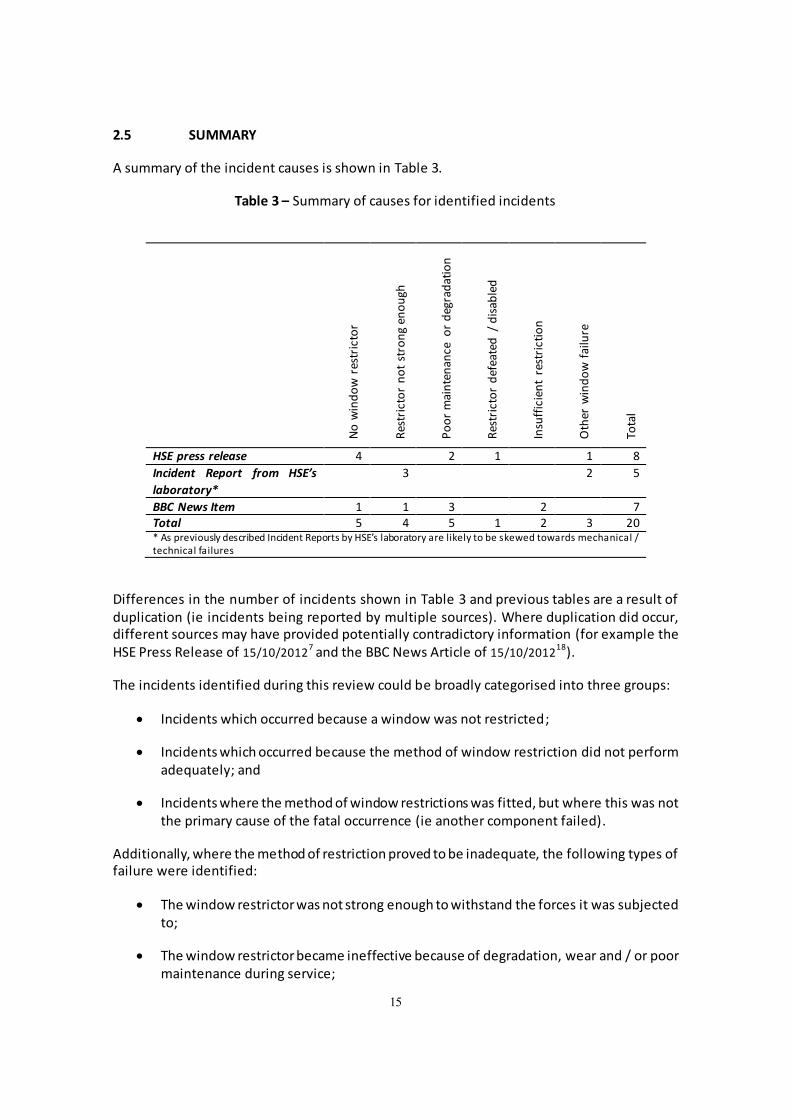
2.5 SUMMARY
A summary of the incident causes is shown in Table 3.
Table 3 – Summary of causes for identified incidents
rot
icrtser w
o
din
w o
N
hg
uo
ne g n
orts t o
n r ot
icrtseR P
oo
r m
ain
ten
ance
or
deg
rad
atio
n
dle
bais
d/
d
etafee
d r ot
icrtseR In
suff
icie
nt
rest
rict
ion
e riluaf
w
od
inw r e
htO
l atoT
HSE press release 4 2 1 1 8
Incident Report from HSE’s
laboratory*
3 2 5
BBC News Item 1 1 3 2 7 Total 5 4 5 1 2 3 20 * As previously described Incident Reports by HSE s laboratory are likely to be skewed towards mechanical / technical failures
Differences in the number of incidents shown in Table 3 a nd previous tables are a result of duplication (ie incidents being reported by multiple sources). Where duplication did occur, different sources may have provided potentially contradictory information (for example the HSE Press Release of 7 18
15/10/2012 and the BBC News Article of 15/10/2012 ).
The incidents identified during this review could be broadly categorised into three groups:
Incidents which occurred because a window was not restricted;
Incidents which occurred because the method of window restriction did not perform adequately; and
Incidents where the method of window restrictions was fitted, but where this was not the primary cause of the fatal occurrence (ie another component failed).
Additionally, where the method of restriction proved to be inadequate, the following types of failure were identified:
The window restrictor was not strong enough to withstand the forces it was subjected to;
The window restrictor became ineffective because of degradation, wear and / or poor maintenance during service;
15

The way in which the window was restricted was defeated or disabled; and
The window restrictor did not provide sufficient restriction (ie it allowed too large an opening to prevent the incident).
Window restrictors were fitted in 75% of the incidents identified. Where window restrictors were fitted the main causes of failure were poor maintenance (or degradation in service) (5 occurrences), a failure of the restrictor due to insufficient strength (4) and a failure of the window, frame or other component (3).
16
3 CURRENT DESIGNS OF WINDOW RESTRICTORS
This section identifies typical methods and mechanisms used to restrict the opening of windows.
An internet search was performed for devices that can be used to restrict the opening of a window using the key words window + restrictor. The intention of this search was not to identify individual devices or manufacturers but to identify common design themes.
The devices which were identified by this search could be divided into two broad categories:-
a) Devices which are loaded in tension.
b) Devices which are loaded in compression.
3.1 DEVICES WHICH ARE LOADED IN TENSION
These devices connect the opening part of a window (leaf) and the fixed part (frame). The tension within the devices prevents movement beyond a certain limit. This type of device can be easily retro-fitted and various types of device are available as after-market modifications.
Of the devices identified that were loaded in tension, two sub-categories existed. In both cases the limit of opening occurred when a connection between the fixed and opening parts of the window was placed in tension. This connection could either be flexible or rigid:
3.1.1 Flexible connection
These window restrictors typically rely on a flexible wire (although other flexible connections such as chain could also be used, as documented in the HSE Press Release of 16
27/1/2012 ) . Closure was possible when the connection flexed into a U shape. These devices could typically be disengaged by completely disconnecting the wire (or chain) at one end, often by unlocking it with a key. Examples of these devices can be seen by consulting device manufacturers web pages (References 21 to 24).
3.1.2 Rigid Connection
A rigid connection typically relies on two solid components, one of which is slotted with the other having a feature which is captured within this slot. This captured feature will generally be free to slide along the length of the slot up to a set limit.
One of these components will be attached to the window frame, whilethe other is attached to the opening leaf of the window. Typically this device could be disengaged by unhooking or unlocking the feature from the slot in some way. Examples of these devices can be seen by consulting device manufactures web pages (References 25 to 29).
3.1.3 Strength of devices loaded in tension
Further investigation identified that several manufacturers were quoting figures relating to the strength of window restrictors designed to be loaded in tension. These figures ranged from 600 N to 5296 N.
17

It is notable that only one manufacturer referred to testing their product using windows manufactured from different materials. In this case, the device under test failed because of a screw pulling out of a PVCu window, at a load of 800 N. It is not clear whether other manufacturers have considered this type of failureor whether their strength figures are based on testing of restrictors fixed to stronger materials likesteel or hardwood or restrictors tested in isolation (i.e. without fixing to a window or similar).
When assessing the strength of a window restrictor it is important to consider its attachment method, and the material to which it is attached.
3.2 DEVICES WHICH ARE LOADED IN COMPRESSION.
A second group of window restrictors function by providing stops – components that block window movement, by supporting compressive loads.
These could be simple fixed brackets which the opening part of a window would strike at a particular point of opening. Such devices are commercially available ( Reference 30 is a web page describing one), but blocks or brackets can also be specially made and fitted as physical constraints on window opening.
A second variant of compressive stop is sometimes used on hinged windows with modern metal mechanisms. Stops are integrated into the tracks by window manufacturers and act on the sliding stays. It is usually possible to request that restrictors are fitted to these windows, when placing an order. Fitting this type of device to an existing window may be more complicated than fitting other types of restrictor, and would involve acquiring new or replacement parts from the window manufacturer, or fitting an additional mechanism with a stop incorporated.
3.2.1 Strength of devices loaded in compression
No evidencewas found of bracket-typestop manufacturers claiming to support any particular loads, although the strength of these devices is likely to depend largely on the fixing methods.
Two manufacturers of stay mechanism were identified, both of whom claimed that their devices were capable of supporting a 600 N force. However, it is possible that there is a limit to the size of window for which these devices would be suitable, since the larger the window , the greater the force that the restrictor would have to contend with. See the manufacturers web pages, References 31 and 32.
The websites of four prominent suppliers and fitters of domestic windows were reviewed. Each of these suppliers offered opening restrictors as an option, but none of them commented on the strength of these devices. Relevant web pages can be found in References 33 to 37.
3.3 SUMMARY OF RESTRICTOR DESIGNS
Window restrictors are based on four broadly consistent designs:
Tension – Flexible.
Tension – Rigid.
18

Compression - Bracket.
Compression – Track based.
Where restrictor strength was quoted by manufacturers, a minimum figure of 600 N was most commonly used. This was based on the requirements of BS 6375-2:198738
19
4 CURRENT STANDARDS AND GUIDANCE APPLICABLE TO
WINDOW RESTRICTORS
This section identifies relevant standards, regulations and guidance which are relevant to the procurement and supply of window restriction devices. Where clauses and recommendations are particularly relevant (for example test methods and requirements) , that text has been reproduced here.
4.1 BRITISH AND EUROPEAN STANDARDS
With a few exceptions, compliance with a British or European Standard is voluntary rather than a legal obligation. A failure to comply with a British Standard does not necessarily make a product unsafe. However, in certain circumstances, compliance with a standard may be interpreted as evidence of the application of good practice.
4.1.1 BS 6375-2:198738
BS 6375-2:1987 “Performance of windows – Part 2: “Specification for operation and strength characteristics”, was the standard which was most commonly quoted by window restrictor suppliers. This standard was replaced in 200939.
The standard defines a restricted opening device” as an item of hardware or a part of an item of hardware that, for safety, limits the initial opening of a sash to a predetermined amount”. In a test specification it quotes 100 mm as an example of a predetermined opening distance. It specifies that window restrictors should be tested with a 600 N force, as quoted below.
A.7 Test 6. Strength of restricted opening and location devices and maximum opening stops
Open the sash until the restricted opening device is engaged and apply a force of 600 N for 5 s as follows:
a) perpendicular to the plane of the sash, except for sliding windows;
b) in the plane of the sash for sliding windows;
c) either at the mid-span position shown in Figure 4 or, for horizontalsliding windows, at the position indicated in Figure 4;
d) in the direction of opening the sash.
Note that this test is carried out with the restrictor installed on a window.
4.1.2 BS 6375-2:200939
The 2009 version defers to two further standards on the subject of safety devices:-
5.3 Load-bearing capacity of safety devices
20
When fitted in accordance with the manufacturer’s instructions and tested in accordance with BS EN 14609 b ut with the safety device engaged, safety devices shall be capable of achieving the performance requirements given in BS EN 14351, when applied to the casement or sash in the most unfavourable position and/or direction.
The standard states in a summary table that the requirements of the referenced standard and test method for window restrictors correspond to: 350 N threshold value”.
The standard does not mention opening limits for restrictors or safety devices.
4.1.3 BS EN 1460940
BS EN 14609:2004 is entitled “Windows – Determination of the resistance to static torsion”. It describes a test procedure applicable to window restrictors, but does not specify strength requirements for restrictors.
4.1.4 BS EN 14351:200641
BS EN 14351:2006 is entitled “Windows and doors – Product standard, performance characteristics. This standard was amended in 2010 and remains current.
This standard does specify a force requirement of 350 N supported for one minute applied in the most unfavourable way. Determination of the most unfavourable way is left to the manufacturer. The strength requirement appears to have been reduced from that specified by BS 6375-2:1987. The wording is as follows:
4.8 Load-bearing capacity of safety devices
Safety devices (e.g. retaining and reversing catches, restrictors, and fixing devices for cleaning procedures), if provided and engaged in accordance with the manufacturer's published instructions, shall be able to hold the leaf, casement or sash in place for 60 s when 350 N are applied to the leaf, casement or sash in the most unfavourable way (i.e. position, direction). This threshold strength shall be demonstrated by means of tests carried out as described in EN 14609 or EN 948 (reference methods), or by calculation.
4.1.5 DD CEN/TS 13126-5:200442
This was a draft for development for the proposed BS EN 13126 P art 5: 2004. It was entitled “Building hardware, fittings for windows and door height windows – Requirements and test methods – Part 5: devices that restrict the opening of windows”; This draft was superseded by the 2011 r evision of the standard:
7.4.2 Restricted opening device strength test
For restricted opening devices and maximum opening stops :
— apply a load of 500N (+50N, -0N) in the opening direction,
It also defines 100 mm as being the maximum opening limit for a window restrictor. The following two paragraphs are taken from Clause 5.2, Other requirements:
21

The restricted opening device shall not permit the movable casement of the test apparatus to be opened beyond the intended limit of the specimen. No gap greater than 100 mm shall occur between the movable casement and the fixed outer frame when the static load of 7.4.1 is applied to allow a 100 mm diameter sphere to pass.
NOTE Restricted opening devices may include design features which permit opening beyond the initial limit, after the restriction has been released. Automatic reengagement when the movable casement is fully closed is not obligatory.
4.1.6 BS EN 13126-5:201143
BS EN 13126-5:2011 is entitled “Building Hardware – Hardware for windows and door height windows – Requirements and test methods Part 5: Devices that restrict the opening of windows and door height windows”. This standard replaces the 2004 draft for development.
The 2011 version of the standard divides restrictors into two separate groups with different requirements, depending on which group protection is aimed at. The two groups are safety limiting restrictors and child safety limiting restrictors. Safety limiting restrictors have a maximum initialopening of 100 mm while child safety limiting restrictors have a more rigorous requirement, with a maximum initial opening of 89 mm
Child safety limiting restrictors have a minimum strength requirement of 350 N for initial opening and a minimum mechanical strength requirement of 500 N.
The clause relating to the strength test of (non-child) safety limiting restrictors is as follows:
7.4.2 Restrictor strength test procedure
Use sample A1.
Open the sash and engage the restrictor in the intended stop position to be tested.
Restrictors shall be manually operated, where necessary, to hold a window open.
Apply a force of 350 N without shock, for 60 s, to the sash in the direction of opening. This force shall be applied perpendicular ± 5º to the plane of the sash, in the same plane as the specimen and at the mid point of the locking rail. (See Figure A.6)
Acceptance criteria are in accordance with EN 13126-1 and 5.4.3 of this standard.
4.1.7 BS EN 16281:201344
A standard related to child safety quotes a window restrictor strength requirement of 350 N. BS EN 16821:2013 is entitled “Child protective products – Consumer fitted child resistant locking devices for windows and balcony doors – Safety requirements and test methods”. This is the wording, and the window restrictor strength requirement:
5.5.4 Mechanical protective function test (opening test)
22
Apply a force of 350 N on the sash in the opening direction without shock, for (60 +10 / -0) s. The force shall be applied at the most onerous position. Check whether test probe A can pass between the frame and the sash.
This same standard has requirements for the security of the lock, against children, but allowing use by adults. This is the wording:
4.1 Child protective functions
4.1.1 General
The release mechanism of the locking device shall be protected against unintentional opening by young children. It shall either:
a) require the use of a specifically designed removable device or removable tool (e.g. a key); or
b) comply with the child panel test requirements in 4.1.2.
The removable device or removable tool shall be removable in the restricted and closed/locked position of the window or balcony door.
It is recommended that locking devices be capable of easy operation by adults including people with special needs.
The panel test refers to the proportion of a panel (200 children, between 42 months and 51 months, with even distribution of age and sex) that are able to defeat the device within 5 minutes.
4.1.8 BS 8213-1:200445
A simpler definition of child-proof is included in BS 8213-1:2004, “Windows, doors and rooflights – Part 1: design for safety in use and during cleaning of windows, including door-height windows and roof windows – Code of practice”; It states in Annex B:
Safety restrictors should operate so that they:
b) are releasable only by manipulation not normally possible by a child under 5 years;
The same standard defines safety [window] restrictors, and sets an opening limit as follows:
3.14 safety restrictor (restricted opening device)
mechanicaldevice which is intended to limit the initial movement of an opening light so that a clear opening of not more than 100 mm is achieved at any point.
4.1.9 BS 8220-2:200046
This standard which covers security products is referenced in the NHS estates document HTM 5550 .BS 8220-2:2000 “Guide for security of buildings against crime – Part 2 shops and offices”, refers to Part 1 in relation to window locks.
23
Many of the various types of locks and fastenings for hinged, pivoted and sliding windows are described and illustrated in BS 8220-1, where guidance is also given on their optimum positioning and on fitment precautions.
4.1.10 BS 8220-1:199547
BS 8220-1:1995, “Guide for security of buildings against crime – Part 1: Dwellings” refers to two other standards which may be relevant to window restriction:
Manipulation testing, which cannot be replicated mechanically was added and following an extensive test programme as PAS 011, tests and acceptance criteria established, which now form the basis of BS 7950.
4.1.11 BS 7950:199748
PAS 011:1994 was a publically available specification (i .e. a specification that was available without cost) which covered the security performance of domestic windows. This specification has been superseded and is no longer available. PAS 011 was replaced by BS 7950:1997, Specification for enhanced security performance of windows for domestic applications”. BS 7950:1997 has itself been replaced by PAS 024:2012.
This standard lists tools and methods that could be used to overcome the security features of a window. It is intended to guard against break-in (from the outside). The tools listed include such things as credit cards, screwdrivers, paint scrapers and chisels.
It is likely that persons within a hospital would have access to some devices of this type, but not all. It may be possible to draw up a more appropriate l ist of items, primarily designed for a different purpose, but with the possibility of being used as a tool. Examples of such devices are a fork, a knitting needle, a walking stick and a nail file.
4.1.12 PAS 024:201249
BS 7950 has been superseded by PAS 024:2012 (“Enhanced security performance requirements for doorsets and windows in the UK – External doorsets and windows intended to offer a level of security suitable for dwellings and other buildings exposed to comparable risk”) which is similar, but includes additional tool sets and test methods.
4.2 GUIDANCE FOR HOSPITALS AND OTHER BUILDINGS
NHS Estates and the Department of Health have developed guidance relating to the construction and maintenance of their properties.
4.2.1 HTM 5550
National Health Service (NHS) Estates have a set of guidance which includes several references to window restrictors. Health Technical Manual (HTM) 55 was published in 1998. It s guidance on windows has been summarised below. This guidance has been superseded by the Health Building Note 00 – 10 Part D51.
Restrictors should be types that can only be disengaged by means of a special tool or key. Socket-head securing screws may be suitable.
24

This implies that ordinary, readily available slotted or Phillips headed screws are unsuitable.
The specified limit of opening in this guidance is 100 mm as transcribed below:
restrictor devices:
These shall check the opening of an opening light of whatever type, at an aperture of not more than 100 mm. To permit the window to be opened more widely, the catch shall be capable of being unfastened. The catch shall re-engage automatically
Note: Automatic reengagement of a catch is not possible on the common wire type window restrictors described in Section 3.1.1.
The guidance deals with security against break-in by referring to BS 8220 parts 147 and 246.
4.2.2 Health Building Note 00-10 Part D: Windows and associated hardware51
Since the initial draft of this report was written, HTM 55 has been superseded by this guidance. It is therefore the most up to date guidance at the time of writing, relating to buildings operated by the NHS.
It acknowledges the need for natural ventilation as follows:
3.10 Opening lights should be used to provide normal ventilation except where:
• the level of outside noise is unacceptable;
• unpleasant smells are generated either inside or outside the building;
• inflows of air are undesirable (such as in a laboratory).
It also suggests (if it doesnt create a risk of falling) that vents or high level opening lights are considered whererestricted opening lights may provide insufficient ventilation. The wording is as follows:
3.13 Louvres or additional high-level opening lights may be considered when restricted openings cannot provide sufficient natural ventilation in hot weather – but only if risk assessment identifies that there is no risk of falling (see also the section on the safe opening and closing of windows in Approved Document K).
This guidance includes the following two clauses relating to windows providing a view:
3.16 The ideal viewing zone will be determined by the eye level of occupants, depending upon whether they are standing up, sitting or lying down. The following factors will affect the ideal viewing zone (see also BS 8206-2):
• security and safety;
• outlook and privacy;
• under-sill requirements for mechanicalservices or furniture.
3.17 These factors will determine:
25

• size of the window;
• shape of the window;
• height of sill;
• height of transom;
• height of head.
It contains expanded sections on safety, prepared with assistance from the Health and Safety Executive. The new sections are in response to a letter from a Coroner who had presided over an inquest into a fatal incident during which a window was forced open beyond the 100 mm-open position to which it should have been restricted.
Sections 3.25 to 3.28 i ndicate that a safety risk assessment concerning falling from windows must be undertaken for all buildings (old and new). It should consider factors such as the people at risk, the consequences of a fall, and the methods of restriction or risk prevention. It defines window restrictors as devices that can hold a window at an opening of less than 100 mm, can resist a significant opening force, and cannot be overridden except with a removable device or key. It also draws attention to safety screens as an alternative to window restrictors, to the HSE guidance (Appendix 1), and to three Safety Alerts on this topic.
The Health Building Note51 contains an important note on page 7 stating that current standards (BS EN 14351-141 and BS EN 13126-543) concern accidental falling from windows and may not demand sufficient strength to prevent determined patients from forcing windows open. It suggests testing window restrictors with loads in excess of those prescribed by these standards (350 N and 500 N respectively).
4.2.3 “Estates and Facilities !lert – Integral side stay mechanism window restrictors fitted with plastic spacer and used in many window applications“52
This document is a safety alert rather than guidance. However it contains important information relating to the deterioration and failure of plastic spacers used in window friction hinges, with integral restrictors. This information was published following an incident.
4.2.4 “Department of Health, Environmental Design Guide, !dult Medium SecureServices, First Published 2011” 53
This publication specifies a maximum window opening of 125 mm. It prescribes testing windows for security against escape using the following tools for striking the window – a hardwood baton, a rubber mallet and a paving maul (similar to a rubber mallet). These tests are of a violent nature and may be more appropriate for simulating the actions of strong individuals in a hospital, rather than infirm individuals in a nursing home.
It also mentions a pen lid test on the beading, frame and glazing, stating that a specific testing regime should be developed appropriate to the situation.
A low security version of this document is also produced, but does not specify any test against escape. A high security version is also available, but this is only applicable to Ashworth, Broadmoor and Rampton hospitals.
26

4.2.5 “The Building Regulations 2010, Volume 2, Buildings other than Dwelling Houses” 54
The Building Regulations are a statutory instrument covering all aspects of building. The issue of emergency evacuation and residential care homes is addressed in section 2.3.8. The regulations state that a proportion of residents at a care home are likely to require some assistance to evacuate. A system of progressive evacuation, by incorporating protected areas, is suggested.
In a care home for the elderly it would seem inappropriateto use windows as an escape route, as patients may struggle to climb up to a window opening. The presence of window restrictors would therefore not become an issue in the event of an evacuation.
27

4.3 ASSESSMENT OF STANDARDS AND GUIDANCE
The strength and maximum opening requirements of the various relevant standards and guidance are summarised in Table 4.
Table 4 – Summary of strength and opening requirements
Document Year Ref Status Min
Strength (N)
Max
opening (mm)
Other
BS 6375 -2 1987 38 Supersede d
600 100*
2009 39 Current 350 -
BS EN 14609 2004 40 Current - -
BS EN 14351 2006 41 Current 350 -
BS EN 13126 -5 2011 43 Current 350 100 Safety l imiting
350/500 89 Child safety l imiting
DD CEN/TS 13126 -5 2004 42 Draft 500 100
BS EN 16821 2013 44 Current 350 -
BS 8213 -1 2004 45 Current - 100
BS 8220 -1 1995 47 Current - -BS 8220 -2 2000 46 Current - -
BS 7950 1997 48 Supersede
d
- -
PAS 024 2012 49 Current - -
HTM 55 1998 50 Supersede d
- 100
Health building note 00-10:D 2013 51 Current - 100 Excess of 350 N and 500 N
Environmental Design Guide 2011 53 Current # 125
Building Regulations Vol 2 2010 54 Current * BS 6375-2 : 1987 Quotes 100 mm as an example of a restricted opening not as a limit of opening. # The Department of Health: Environmental Design Guide specifies impact testing using a variety of domestic items.
Current standards show a general consensus on both the minimum strength of the restrictor (350 N) and the maximum opening of a restricted window (100 mm). It is notable that older superseded specifications have higher strength requirements and that this requirement appears to have been revised downward over time.
It is interesting to note that the latest version of BS EN 13126 quotes higher strength requirements for window restrictors which are protecting children. This would appear to suggest that while the standard considers deliberate actions by children and accidental actions by adults, there is a general failure to consider the actions of determined adults. None of the British and European standards appear to deal with deliberate attempts to defeat the restrictor, as may be encountered in hospitals and care homes. This is acknowledged in NHS guidance51.
Department of Health guidance states that current British and European Standards concern accidental falling from windows and may not demand sufficient strength to prevent determined patients from forcing windows open. It suggests testing window restrictors with loads in excess of those prescribed by current standards.
28

More recent guidance (Health building Note 00-10 Part D: Windows and associated hardware54) also states that special tools or devices should be needed to open windows beyond the restriction. In addition, the more recent guidance comments on other factors such as the need for natural ventilation and viewing zones. It states that individual risk assessments should be carried out concerning the risk of falling from windows.
29

5 MAXIMUM FORCES THAT CAN BE APPLIED BY DETERMINED ADULTS TO OPEN WINDOWS AND THE FORCES THAT CAN BE
APPLIED ABOVE WAIST HEIGHT
If a person is trying to open a window more than the window restrictors will allow, it is likely that they will push against the window or the window handle. The maximum push forces that can be applied by a person to an object depend on a number of factors. These include the posture adopted to apply the push force (e.g. standing, sitting, kneeling, braced against a supporting structure), what part of the body is used (e.g. one hand, both hands, shoulder, knee, foot), and the height, size and shape of the object that is being pushed against. The force that can be applied also depends on and whether the force is static (force applied gradually) or is an impact force (force applied at speed like a shove, punch or kick).
Posture is an important factor when applying push force. Studies by Pheasant55 measuring strength in different postures generally show that the differences between postures are greater than the differences between individuals (i.e. muscle strength) . For example, the maximum push force is greater for pushes using both hands rather than one hand and for pushes against an object at waist height compared to shoulder or chest height according to Peebles and Norris56. Other issues reported by Pheasant57 include the body weight itself, how the body weight is positioned, whether the body is supported or braced against another object, and the slip resistance between the feet and the floor
It is generally accepted that, on average, women are not as strong as men (female to male ratio of 61% according to Pheasant57).For this reason, where push strength data for both male and females is available, the male data is used to determine maximum forces. Strength generally declines with age over the age of 50. As some incidents involving the failure of window restrictors have occurred in hospitals and nursing homes, we have considered push force data, specifically measured on older age groups as well as adult data where this is available.
5.1 STATIC STRENGTH ANTHROPOMETRIC DATA FOR ADULT POPULATIONS
As would be expected more static push force can be applied using both hands than one hand. Peebles and Norriss survey56 of two handed push force suggests that the mean maximum standing push strength for adult males is 304 N. This is the forward force exerted on a round handle 1240 mm from the floor which is close to the average UK male chest height. While the raw data are not available, it is calculated that the greatest (i.e. 99th percentile) push strengths measured in this survey were about 457 N. Another survey by Chaffin & Anderson58, of the two handed strength of adult males found a similar mean maximum push force from an upright standing posture of 303 N (480 N for 99th percentile) when applied on a handle positioned at chest height and a mean of 311 N (765 N for 99th percentile) when applied at waist height.
It is worth noting that force measurements for these surveys were for one or two handed push forces on an object such as a round handle, vertical or horizontal bar, which may relate to push forces on a window opening handle. However, there are no comparable data for one or two handed staticpalm pushes on a vertical surface from a standing posture which would replicate someone pushing on the glass or frame of a window.
30

The data suggests that greater maximum push forces can be applied from postures other than standing where the whole body can be used either braced against a supporting object (like a wall opposite) or by leaning towards the object or surface. Leaning forward means that the centre of gravity of the body falls in front of the feet which enables the weight to exert some push force in addition to the force that is exerted by muscles contracting according to Kroemer59. For example, the mean static push strength for adult males pushing outwards with both hands on a handle placed at shoulder level where the body is leaning forward into the push was 418 N (833 N for 99th percentile) in Ch affin and Andersons survey 58. Another much smaller survey61 published by the Department of Trade and Industry (10 male participants aged 31-50) measured static push strength where the participants were encouraged to adopt a free posture (ie whatever standing, non-braced posture in which they felt they could apply most force). The mean maximum static two handed standing push force with a free posture was 537 N (1042 N for 99th percentile). Kroemer59 reports that adopting a posture where a part of the body is braced against a supporting structure which stops the feet from sliding on the floor and enables maximum static push forces to be exerted. Examples of braced postures include bracing the back against a wall opposite to the object or surface to push, or resting the back foot against a foot rest and pushing forward on to the object or surface).
Postures that might be used to try to overcome a window restrictor include leaning forward towards the window with one foot forward and the other back and pushing with both hands; and pushing against the window with one shoulder. Depending on where the windowis, it may be possible for an individual to brace themselves against a wall or a piece of furniture.
Considerably more push force can be applied if the individual is able to brace against a supporting structure whilst adopting a two handed static push or a shoulder push. For example, Peebles and Norriss survey56 found that a two handed static palm push on a vertical surface with the arms at shoulder height and the back braced against a supporting structure resulted in a mean maximum push force of 1311 N (2262 N for 99th percentile). This is more than four times the comparable non-braced mean maximum standing push force (311 N mean at waist height). Similarly, a push with the shoulder with body weight behind the push, on a vertical surface at 60% of shoulder height, resulted in a mean maximum push force of 871 N (1293 N for 99th percentile). In Peebles and Norriss survey56 the mean maximum static push force for a two handed push with the back foot braced was 703 N (1073 N for 99th percentile).
5.2 STATIC STRENGTH ANTHROPOMETRIC DATA FOR OLDER ADULTS
Surveys carried out specifically on older adults look at different age groups. One survey by Smith, Norris & Peebles60 of UK older males indicates that the mean maximum one handed push force on an object from a standing posture was 283 N for a 60-65 a ge group, 225 N for ages 66-70 and 199 N for a 71-75 a ge group where the object was 1000 mm from the floor (average elbow height for men 65 years or older). The same survey found that mean maximum push forces using one hand on an object at greater heights were lower for all age groups (236 N at 1300 mm and 220 N at 1600 for the 60-65 a ge group).
A similar survey of two handed standing push forces carried out on groups of older males in the Netherlands found that a mean maximum push force of 424 N when applied on an object at elbow height for the 60-64 age group. As would be expected, the maximum push force was
31
generally lower for older age groups with the 80 plus age group mean maximum push force being 295 N according to Smith, Norris & Peebles60.
Maximum push forces for older adults in postures other than standing were only found for pushes with the shoulder. The Department of Trade and Industry UK survey61 found that the mean maximum push strength with the shoulder at 90% of shoulder height for males was 510 N for the 61-70 age group, 339 N for the 71-80 age group and 281 N for the 81-90 a ge group.
The population samples provided for the older adult data reported above were generally taken from people living independently, rather than residents or patients in care homes or hospitals, so the maximum forces for dependent older peoplecould differ. Also, the survey sample sizes for each older age group were small, which adds uncertainty when extrapolating the data to the entire population.
See Tables A1, A2 and A3 in Appendix 1 for more information on static push force anthropometric data for adult and older people.
5.3 IMPACT FORCES
If an individual is determined to open a window, they may apply a dynamic impact force on the window rather than a gradually applied (static) force. Impact forces are greater than static forces. However, determining the maximum human impact force depends on several complex factors including:
Method of impact;
Orientation, size and position of the impact object or surface;
Characteristics and capabilities of the individual, such as strength, skill, body mass, etc.;
Position and posture of the individual;
Psychological influences on the individual, such as intentions (e.g. to get out of the building), perceptions of safety, possible self-injury, etc. , and
Environmental and situational factors that may be present when an individual is trying to open a window more than the restrictors are designed to allow.
Ferreira (2003) carried out a small literature review on human impact forces for work related to the forces that could be applied to emergency stop controls. He found limited information regarding maximal human impact forces. Previous investigations have focused upon sports-related (boxing, martial arts) applications; for example, determining the maximal impact forces of a punch. For example, Smith et al.62 designed a boxing dynamometer to measure punching forces and found mean maximal straight punch forces for elite, intermediate and novice boxers of 4800 N , 3722 N and 2381 N for the rear hand although this may underestimate the maximal human impact force that could be inflicted on a rigid object.
Only one study (Hopkinson et al63) could be found that addressed human impact forces with respect to industry standards and impact tests. To validate safety standards for vertically mounted glass, researchers measured impact force data from 8 adults (5 males, 3 females with a mean age of 24) with an adjustable vertically-mounted force plate. The impact data was collected for six impact methods. The mean maximum impacts recorded included 4883 N for
32

falling forward, 5521 N for running forward, 6109 N for a fist strike, 6942 N for strike with an elbow, 6796 N for strike with a foot and 7836 N for strike with a knee. See Table A4 in Appendix 1 for more details.
These forces are considerably greater than static forces although since this study used only 8 subjects and a substantial range of forces were recorded, caution must be exercised when extrapolating these results to a larger population. Also, it is worth noting that the impact forces reported by Hopkinson et al.63 are considerably higher than those reported in earlier sports-related literature. Ferreira (2003) suggests that it is questionable whether the heaviest subject in this study (83.9 k g) could deliver nearly twice the force over an elite boxer. This shows the difficulties in comparing studies and using these results to extrapolate to other scenarios. For example, Hopkinson et al.63 used a force plate which was vertical and padded to protect the participants. However, it is likely that the subjects would perceive that they could strike a padded surface harder than a glass surface without causing themselves injury or the window to break. In addition, to overcome window restrictors, the force would be applied to a window that was partially open rather than vertical which may reduce the force that could be applied.
5.4 IMPACT PERFORMANCE LEVELS FOR GLAZING
It would not seem appropriate to have window restrictors which are able to withstand greater force than the glazing. The maximum impact forces described above are likely to exceed the impact performance requirements for safety glass for use in buildings as specified in BS 6206:198164. The highest classification of safety glass requires glass either to not break or to break safely when subjected to impact energies of 538 J . This is generated under the test conditions by dropping a lead-shot filled leather bag weighing 45 kg from a height of 1219 mm so that it swings like a pendulum against the test safety glass.
5.5 SUMMARY
As described in 4.1.4, BS EN 14351-1 (2006) Windows and doors – product standard, performance characteristics 41, states that window restrictors should be able to withstand 350 N of force applied to the window casement or sash. This is in line with force requirements for child safety. This level of force reflects the 58th percentile for static, un-braced maximum push force at waist height for an adult male pushing with both hands which suggests that 42 out of 100 adults could apply greater force in this posture and potentially could defeat window restraints meeting the 350 N British Standard requirement. Similarly, the 35th percentile for adult male maximum two-handed push strength in a static standing, leaning forward posture is 350 N which suggests that only 35 out of 100 adult males would be stopped by window restrictors which could only withstand 350 N. For braced postures, even the weakest 1 or 2 per cent of the adult male population could defeat window restrictors designed to this standard.
If a window restrictor were designed to resist a static, gradually applied, push force of 640 N, it may offer protection for 95% of the adult population (765 N for 99%). This is based on the anthropometricdata on maximum push forces from a standing (non-braced) posture at elbow (or waist) height. Using the data specifically for older age groups (60 or older), would suggest a lower force of 500 N may offer protection to 95% of this age group (527 N for 99%). However,
33
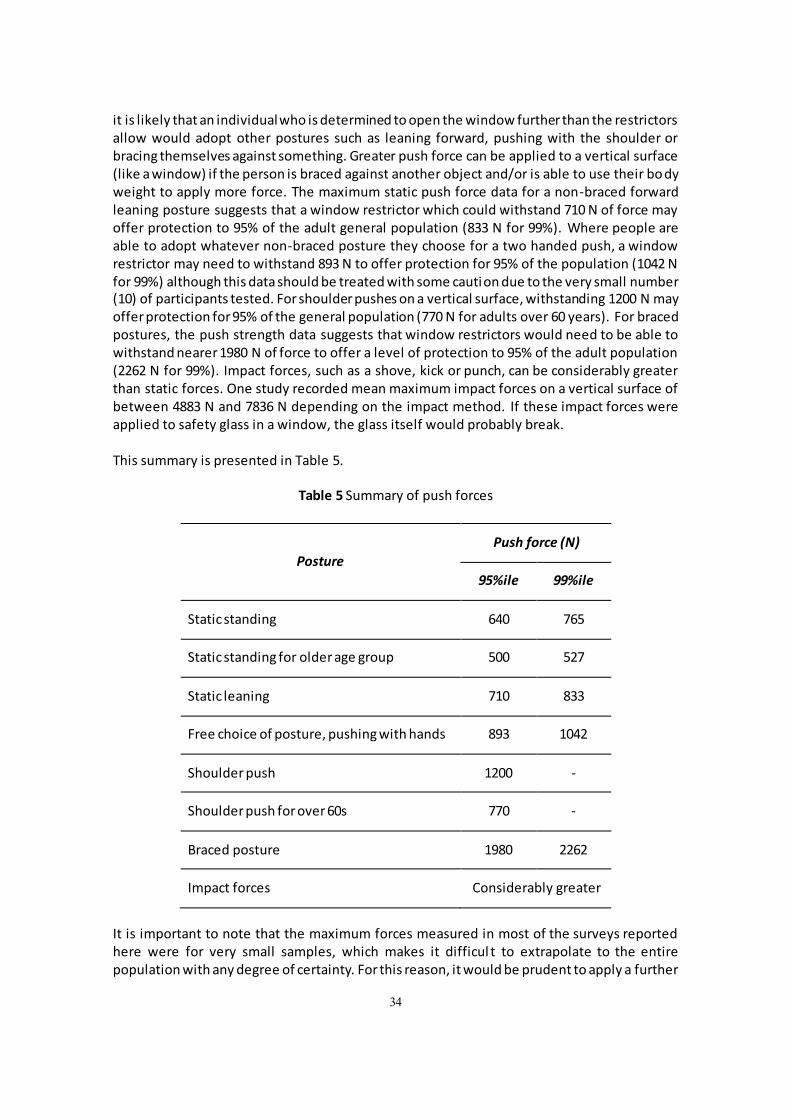
it is likely that an individual who is determined to open the window further than the restrictors allow would adopt other postures such as leaning forward, pushing with the shoulder or bracing themselves against something. Greater push force can be applied to a vertical surface (like a window) if the person is braced against another object and/or is able to use their bo dy weight to apply more force. The maximum static push force data for a non-braced forward leaning posture suggests that a window restrictor which could withstand 710 N of force may offer protection to 95% of the adult general population (833 N for 99%). Where people are able to adopt whatever non-braced posture they choose for a two handed push, a window restrictor may need to withstand 893 N to offer protection for 95% of the population (1042 N for 99%) although this data should be treated with some caution due to the very small number (10) of participants tested. For shoulder pushes on a vertical surface, withstanding 1200 N may offer protection for 95% of the general population (770 N for adults over 60 years). For braced postures, the push strength data suggests that window restrictors would need to be able to withstand nearer 1980 N of force to offer a level of protection to 95% of the adult population (2262 N for 99%). Impact forces, such as a shove, kick or punch, can be considerably greater than static forces. O ne study recorded mean maximum impact forces on a vertical surface of between 4883 N and 7836 N depending on the impact method. If these impact forces were applied to safety glass in a window, the glass itself would probably break.
This summary is presented in Table 5.
Table 5 Summary of push forces
Posture
Push force (N)
95%ile 99%ile
Static standing 640 765
Static standing for older age group 500 527
Static leaning 710 833
Free choice of posture, pushing with hands 893 1042
Shoulder push 1200 -
Shoulder push for over 60s 770 -
Braced posture 1980 2262
Impact forces Considerably greater
It is important to note that the maximum forces measured in most of the surveys reported here were for very small samples, which makes it difficul t to extrapolate to the entire population with any degree of certainty. For this reason, it would be prudent to apply a further
34

margin of safety (above the 99th percentile values) to the requirements of window restrictors in order to ensure that the entire population is protected.
35
6 IMPLICATIONS
6.1 THE CURRENT SITUATION
A review of incident descriptions indicates that there are issues associated with falls from windows in the Health and Care sectors. Insufficient strength of restrictors is one of the most significant causes of failure.
A review of standards indicates that the minimum strength requirement of 350 N and the maximum opening of 100 mm appear to have general agreement between standards. This suggests that minimum load requirements have been standardised over time (although many manufacturers still claim to meet a higher strength requirement taken from BS 6375 -2:198738 which was superseded in 2009.
This review also suggested that the issue of determined adults attempting to deliberately defeat a window restrictor has not been given adequate consideration by these standards. These standards do not necessarily offer sufficient protection against situations that are likely to occur in health or social care.
The available strength data (summarised in Table 5) indicates that forces well in excess of 350 N can easily be achieved from a range of postures. Therefore to offer sufficient protection in circumstances where individuals can brace against objects, use body weight, momentum or impact, or use the body to wedge or lever the window, then restrictors would need to be able to withstand forces significantly in excess of that currently specified.
6.2 CONCLUSIONS
At present, BS EN 14351: 200641 is considered to provide a level of protection sufficient to avoid inadvertent breakage during normal use. However, it doesnt appear to consider the forces that could foreseeably be generated by a determined action. Given the use of window restrictors in the care and health sectors, this is a potentially significant omission. However, because of the wide range in forces that can be generated by people, setting a reasonable strength criterion for window restrictors is not a straightforward matter.
In order to be able to select a useful force criterion from the data avai lable, it is necessary to take account of how the force capability data was generated. For the health or social care context, it may be considered reasonable and workable to adopt the scenario of normal use but factoring in an element of determination. By this we mean that the person is any child or adult, and that they purposefully attempt to open the window using its intended method of operation without resorting to a means of exerting a force that unduly involves using body weight, body momentum or impact on any part of the window, or using the body to wedge or lever the window open. Repetition of the force, is a likely behaviour, and also needs to be considered.
Ergonomics data corresponding exactly with this scenario is not available. However the static pushing forces that can be applied by an adult male may be a good starting point. Any strength requirements based on adults males is likely to exceed the capabilities of weaker persons (such as the young or elderly). From Table 5, the maximum static push force that adult males can
36
exert with both hands, pushing outwards on a handle, at shoulder height in a non-braced, forward leaning posture is 833 N.
A restricted window that can withstand 833 N of push force may offer protection for 99% of the population in these circumstances, based on Kremer59. However, because of the difficulty extrapolating these maximum force figures to the general population and to this particular situation, we suggest that a guide figure of 850 N would be appropriate to apply a further margin of safety.
Therefore, as a guide, it is suggested that window restrictors (and their fixings) should be capable of withstanding push forces of at least 850 N.
It is important to note that people may be able to exert greater forces (and defeat window restrictor installations capable of withstanding 850 N) if, for example:
the force is applied from an alternative posture e.g. one foot forward, the other back, leaning forward significantly;
the person is able to brace themselves against a supporting structure when applying the force;
the force is applied with another part of the body e.g. push with the shoulder;
the force applied is an impact force rather than a gradually applied force e.g. a shove; and;
the force applied is an impact force using an object e.g. throwing a chair at the window.
It should be recognised that in some situations some patients may use excessive force, body weight, impact or momentum to try to break or open a window. Whether this is likely to occur in the environment wherethe windowrestrictors are to be installed needs to be consideredon a case by case basis. In these circumstances, clearly the suggested force guide of 850 N would not be appropriate to rely on and the potential vulnerability of the glazing and other window components may become more significant.
37
7 REFERENCES
1. HSE Press Release, dated 9 October 2012, (No reference number), URL: http://www.hse.gov.uk/press/2012/rnn-wm-walsall-nhs.htm accessed 24/4/13.
2. HSE Press Release, dated 18 July 2012, Release number SE/135/12, URL: http://www.hse.gov.uk/press/2012/rnn-se-13512.htm accessed 24/4/13.
3. HSE Press Release, dated 6 July 2012, (No reference number),
http://www.hse.gov.uk/press/2012/rnn-sw-yourhealth.htm accessed 24/4/13.
4. HSE Press Release, dated 8 March 2013, Release number HSE-E-011/13, URL: http://www.hse.gov.uk/press/2013/rnn-e-01113.htm accessed 24/4/13.
5. HSE Press Release, dated 2 December 2010, Release number WM290/10, URL:
http://news.hse.gov.uk/2010/12/02/worcestershire-care-home-fined-after-investigation-into-fatal-fall-from-window/ accessed 24/4/13.
6. HSE Press Release, dated 27 Januray 2012, (No reference number), URL:
http://www.hse.gov.uk/press/2012/coi-w-wrexhamcarehome.htm accessed 24/4/13.
7. HSE Press Release, dated 15 October 2012, (No reference number), URL:
http://www.hse.gov.uk/press/2012/rnn-sw-hillcresthouse.htm accessed 24/4/13.
8. HSE Press Release, dated 23 May 2011, (No reference number), URL:
http://www.hse.gov.uk/press/2011/coi-w-headlandsnursing.htm accessed 24/4/13.
9. Firm fined for hotel death fall, BBC Scotland News article, dated 4 November 2005, URL: http://news.bbc.co.uk/1/hi/scotland/4407978.stm accessed 25/4/13.
10. Hostel death plunge preventable, BBC Scotland News article, dated 14 February 2006,
URL: http://news.bbc.co.uk/1/hi/scotland/4713514.stm accessed 25/4/13.
11. Home fined over residents death, BBC Oxfordshire News article, date 9 January 2009,
URL: http://news.bbc.co.uk/1/hi/england/oxfordshire/7820109.stm accessed 25/4/13.
12. Trust fined after window plunge, BBC News article, dated 26 February 2009, URL:
http://news.bbc.co.uk/1/hi/england/south_yorkshire/7913033.stm accessed 25/4/13.
13. Window advice over OAP death fall, BBC Wales News article, dated 22 April 2009, URL:
http://news.bbc.co.uk/1/hi/wales/8012965.stm accessed 25/4/13.
14. Hospital fall trust fined £10,000, BBC Essex News article, dated 29 October 2009, URL: http://news.bbc.co.uk/1/hi/england/essex/8332372.stm accessed 25/4/13.
38

15. Tribute to hospital fall woman Josephine Mowat, BBC Edinburgh, Fife & East Scotland, dated 21 November 2011, URL: http://www.bbc.co.uk/news/uk-scotland-edinburgh-east-fife-15818940 accesssed 25/4/13.
16. Care Home Wrexham Ltd fined after mans window fall, ��� North East Wales News
article, dated 27 January 2012, URL: http://www.bbc.co.uk/news/uk-wales-north-east-wales-16768483 accessed 25/4/13.
17. Robin �lowes accidentally fell to his death from window, ��� Essex News article,
dated 27 S eptember 2012, URL: http://www.bbc.co.uk/news/uk-england-essex-19742365 accessed 25/4/13.
18. Hillcrest House care home fined for Looe window fall death, BBC Cornwall News
article, dated, 15 October 2012, URL: http://www.bbc.co.uk/news/uk-england-cornwall-19955166 accessed 25/4/13.
19. West Suffolk Hospital fined after patient fell from window, BBC Suffolk News article,
dated 8 M arch 2013, URL: http://www.bbc.co.uk/news/uk-england-suffolk-21719416 accessed 25/4/13.
20. �losing hospital windows increases infection risk, ��� News video, dated 24 !pril
2013, URL: http://www.bbc.co.uk/news/health-22269697 accessed 25/4/13.
21. Jackloc Cable Restrictor Test, report by Wintech Building Envelope Testing, Number
R12026-2, Date 1/2/2012.
22. Webpage for Penkid window restrictor, URL: http://www.fingershield.co.uk/Penkid
accessed 25/4/13.
23. Webpage for Fenster Window Safety Restrictor, URL:
http://www.fenster.uk.com/wsr.html accessed 25/4/13.
24. Webpage for Sashjack Ltd Locit, URL:
http://www.busipages.com/sashjack/sashsecure.html accessed 25/4/13.
25. Technical sheet for ERA window restrictor, URL: http://www.era-
security.com/media/downloads/window-restrictor.pdf accessed 25/4/13.
26. Technical sheet for MILA ventilation arm, URL:
http://www.mila.co.uk/Portals/0/pdf/rsd_ventilation_arm.pdf accessed 25/4/13.
27. Webpage for J Banks Res-lok surface fix restrictor, URL:
http://www.jbanks.co.uk/locks_hardware/windowfittings/res-lok_FF.html accessed 25/4/13.
28. MACO Multi-vent window restrictor operating instructions, URL:
http://www.maco.de/maco/cont/ShowFile.aspx?id=6699 accessed 25/4/13.
39
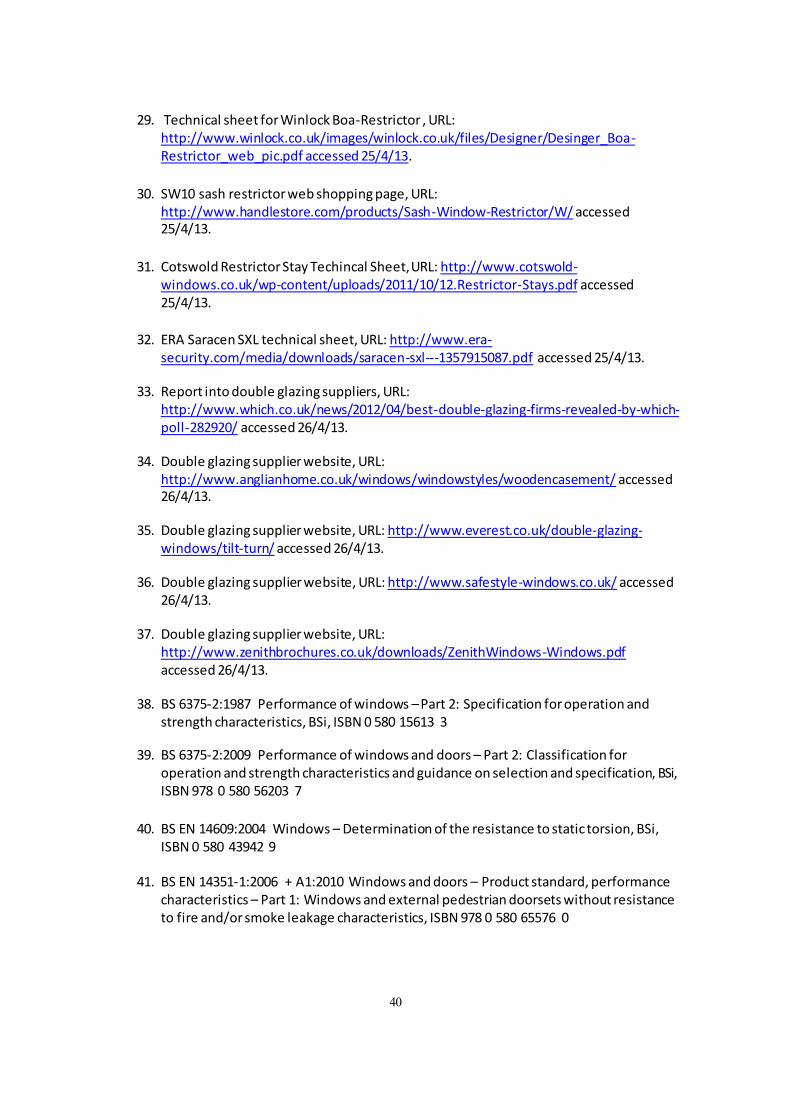
29. Technical sheet for Winlock Boa-Restrictor , URL: http://www.winlock.co.uk/images/winlock.co.uk/files/Designer/Desinger_Boa-Restrictor_web_pic.pdf accessed 25/4/13.
30. SW10 s ash restrictor web shopping page, URL:
http://www.handlestore.com/products/Sash-Window-Restrictor/W/ accessed 25/4/13.
31. Cotswold Restrictor Stay Techincal Sheet, URL: http://www.cotswold-
windows.co.uk/wp-content/uploads/2011/10/12.Restrictor-Stays.pdf accessed 25/4/13.
32. ERA Saracen SXL technical sheet, URL: http://www.era-
security.com/media/downloads/saracen-sxl---1357915087.pdf accessed 25/4/13.
33. Report into double glazing suppliers, URL: http://www.which.co.uk/news/2012/04/best-double-glazing-firms-revealed-by-which-poll-282920/ accessed 26/4/13.
34. Double glazing supplier website, URL: http://www.anglianhome.co.uk/windows/windowstyles/woodencasement/ accessed 26/4/13.
35. Double glazing supplier website, URL: http://www.everest.co.uk/double-glazing-windows/tilt-turn/ accessed 26/4/13.
36. Double glazing supplier website, URL: http://www.safestyle-windows.co.uk/ accessed 26/4/13.
37. Double glazing supplier website, URL: http://www.zenithbrochures.co.uk/downloads/ZenithWindows-Windows.pdf accessed 26/4/13.
38. BS 6375-2:1987 Performance of windows – Part 2: Specification for operation and strength characteristics, BSi, ISBN 0 580 15613 3
39. BS 6375-2:2009 Performance of windows and doors – Part 2: Classification for operation and strength characteristics and guidance on selection and specification, BSi, ISBN 978 0 580 56203 7
40. BS EN 14609:2004 Windows – Determination of the resistance to static torsion, BSi, ISBN 0 580 43942 9
41. BS EN 14351-1:2006 + A1:2010 Windows and doors – Product standard, performance characteristics – Part 1: Windows and external pedestrian doorsets without resistance to fire and/or smoke leakage characteristics, ISBN 978 0 580 65576 0
40
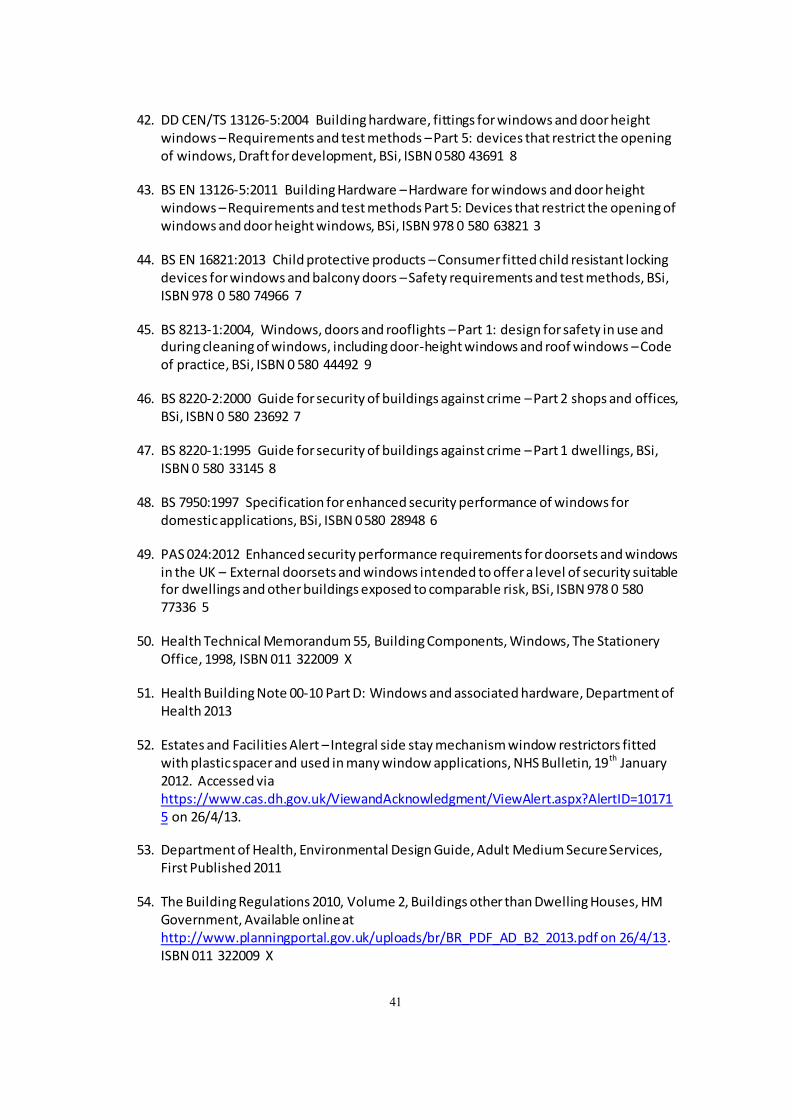
42. DD CEN/TS 13126-5:2004 Building hardware, fittings for windows and door height windows – Requirements and test methods – Part 5: devices that restrict the opening of windows, Draft for development, BSi, ISBN 0580 43691 8
43. BS EN 13126-5:2011 Building Hardware –Hardware for windows and door height windows – Requirements and test methods Part 5: Devices that restrict the opening of windows and door height windows, BSi, ISBN 978 0 580 63821 3
44. BS EN 16821:2013 Child protective products – Consumer fitted child resistant locking devices for windows and balcony doors –Safety requirements and test methods, BSi, ISBN 978 0 580 74966 7
45. BS 8213-1:2004, Windows, doors and rooflights – Part 1: design for safety in use and during cleaning of windows, including door-height windows and roof windows –Code of practice, BSi, ISBN 0 580 44492 9
46. BS 8220-2:2000 Guide for security of buildings against crime – Part 2 shops and offices, BSi, ISBN 0 580 23692 7
47. BS 8220-1:1995 Guide for security of buildings against crime – Part 1 dwellings, BSi, ISBN 0 580 33145 8
48. BS 7950:1997 Specification for enhanced security performance of windows for domesticapplications, BSi, ISBN 0580 28948 6
49. PAS 024:2012 Enhanced security performance requirements for doorsets and windows in the UK – External doorsets and windows intended to offer a level of security suitable for dwellings and other buildings exposed to comparable risk, BSi, ISBN 978 0 580 77336 5
50. Health Technical Memorandum 55, Building Components, Windows, The Stationery Office, 1998, ISBN 011 322009 X
51. Health Building Note 00-10 Part D: Windows and associated hardware, Department of Health 2013
52. Estates and Facilities Alert – Integral side stay mechanism window restrictors fitted with plastic spacer and used in many window applications, NHS Bulletin, 19th January 2012. Accessed via https://www.cas.dh.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=10171 5 on 26/4/13.
53. Department of Health, Environmental Design Guide, Adult Medium SecureServices, First Published 2011
54. The Building Regulations 2010, Volume 2, Buildings other than Dwelling Houses, HM Government, Available onlineat http://www.planningportal.gov.uk/uploads/br/BR_PDF_AD_B2_2013.pdf on 26/4/13. ISBN 011 322009 X
41
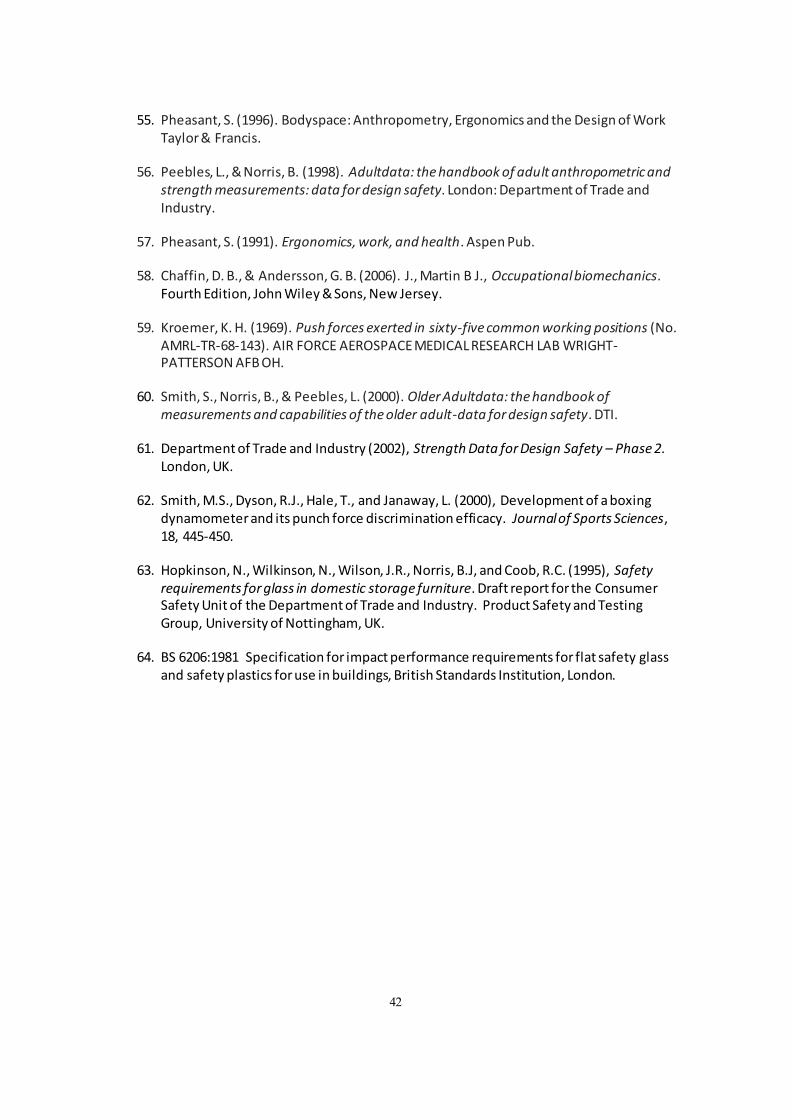
55. Pheasant, S. (1996). Bodyspace: Anthropometry, Ergonomics and the Design of Work Taylor & Francis.
56. Peebles, L., & Norris, B. (1998). Adultdata: the handbook of adult anthropometric and strength measurements: data for design safety. London: Department of Trade and Industry.
57. Pheasant, S. (1991). Ergonomics, work, and health. Aspen Pub.
58. Chaffin, D. B., & Andersson, G. B. (2006). J., Martin B J., Occupationalbiomechanics. Fourth Edition, John Wiley & Sons, New Jersey.
59. Kroemer, K. H. (1969). Push forces exerted in sixty-five common working positions (No. AMRL-TR-68-143). AIR FORCE AEROSPACE MEDICAL RESEARCH LAB WRIGHT-PATTERSON AFB OH.
60. Smith, S., Norris, B., & Peebles, L. (2000). Older Adultdata: the handbook of measurements and capabilities of the older adult-data for design safety. DTI.
61. Department of Trade and Industry (2002), Strength Data for Design Safety – Phase 2. London, UK.
62. Smith, M.S., Dyson, R.J., Hale, T., and Janaway, L. (2000), Development of a boxing dynamometer and its punch force discrimination efficacy. Journalof Sports Sciences, 18, 445-450.
63. Hopkinson, N., Wilkinson, N., Wilson, J.R., Norris, B.J, and Coob, R.C. (1995), Safety requirements for glass in domestic storage furniture. Draft report for the Consumer Safety Unit of the Department of Trade and Industry. Product Safety and Testing Group, University of Nottingham, UK.
64. BS 6206:1981 Specification for impact performance requirements for flat safety glass and safety plastics for use in buildings, British Standards Institution, London.
42
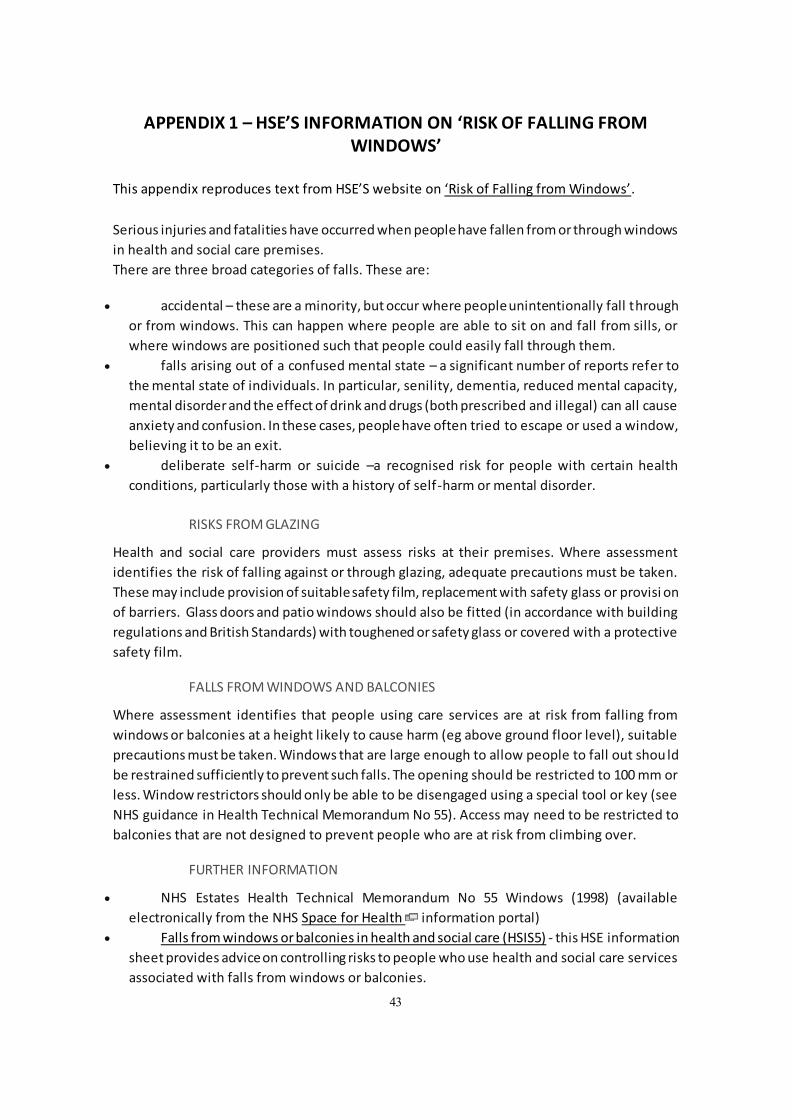
APPENDIX 1 – HSE’S INFORMATION ON ‘RISK OF FALLING FROM WINDOWS’
This appendix reproduces text from HSES website on Risk of Falling from Windows.
Serious injuries and fatalities have occurred when peoplehave fallen from or through windows in health and social care premises. There are three broad categories of falls. These are:
accidental – these are a minority, but occur where peopleunintentionally fall through
or from windows. This can happen where people are able to sit on and fall from sills, or
where windows are positioned such that people could easily fall through them.
falls arising out of a confused mental state – a significant number of reports refer to
the mental state of individuals. In particular, senility, dementia, reduced mental capacity,
mental disorder and the effect of drink and drugs (both prescribed and illegal) can all cause
anxiety and confusion. In these cases, peoplehave often tried to escape or used a window,
believing it to be an exit.
deliberate self-harm or suicide –a recognised risk for people with certain health
conditions, particularly those with a history of self-harm or mental disorder.
RISKS FROM GLAZING
Health and social care providers must assess risks at their premises. Where assessment
identifies the risk of falling against or through glazing, adequate precautions must be taken.
These may include provision of suitablesafety film, replacement with safety glass or provisi on
of barriers. Glass doors and patio windows should also be fitted (in accordance with building
regulations and British Standards) with toughened or safety glass or covered with a protective
safety film.
FALLS FROM WINDOWS AND BALCONIES
Where assessment identifies that people using care services are at risk from falling from
windows or balconies at a height likely to cause harm (eg above ground floor level), suitable
precautions must be taken. Windows that are large enough to allow people to fall out shou ld
be restrained sufficiently to prevent such falls. The opening should be restricted to 100 mm or
less. Window restrictors should only be able to be disengaged using a special tool or key (see
NHS guidance in Health Technical Memorandum No 55). Access may need to be restricted to
balconies that are not designed to prevent people who are at risk from climbing over.
FURTHER INFORMATION
NHS Estates Health Technical Memorandum No 55 Windows (1998) (available
electronically from the NHS Space for Health information portal)
Falls from windows or balconies in health and social care (HSIS5) - this HSE information
sheet provides advice on controlling risks to people who use health and social care services
associated with falls from windows or balconies.
43
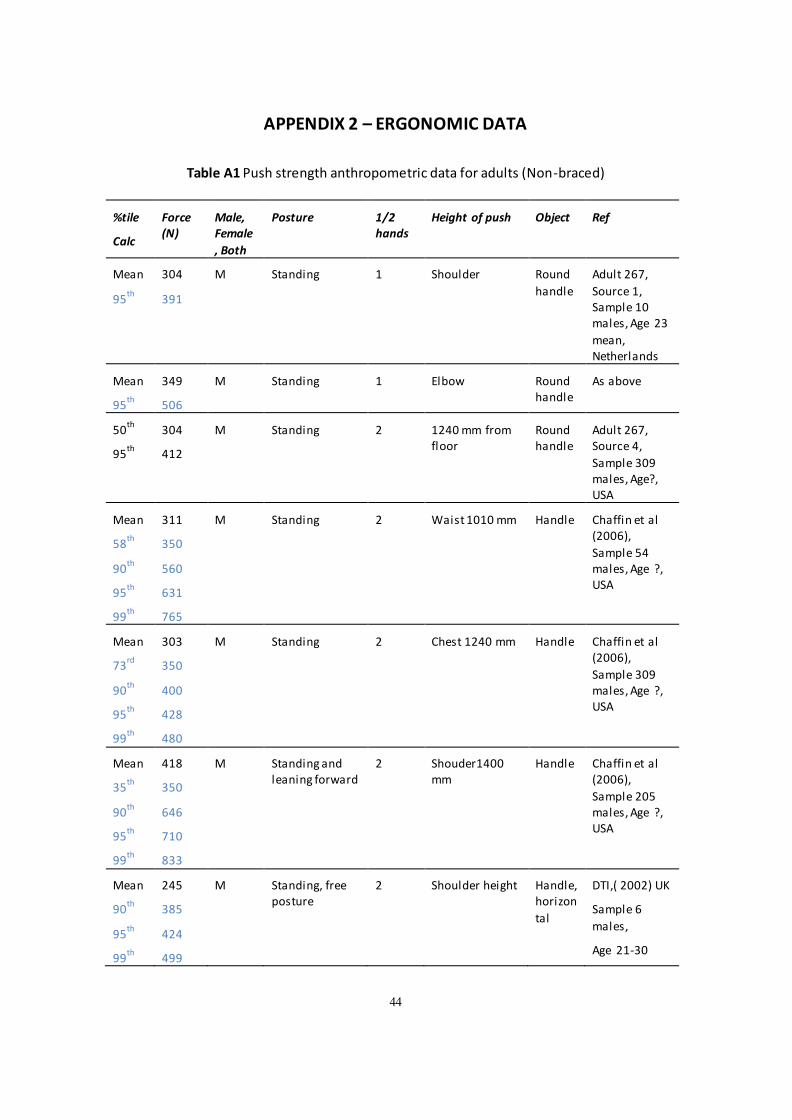
APPENDIX 2 – ERGONOMIC DATA
Table A1 Push strength anthropometric data for adults (Non-braced)
%tile
Calc
Force (N)
Male, Female
, Both
Posture 1/2 hands
Height of push Object Ref
Mean
th 95
304
391
M Standing 1 Shoulder Round
handle
Adult 267,
Source 1, Sample 10 males, Age 23
mean, Netherlands
Mean
th 95
349
506
M Standing 1 Elbow Round handle
As above
50th
th 95
304
412
M Standing 2 1240 mm from floor
Round handle
Adult 267, Source 4,
Sample 309 males, Age?, USA
Mean
th 58
th 90
th 95
99th
311
350
560
631
765
M Standing 2 Waist 1010 mm Handle Chaffin et al (2006),
Sample 54 males, Age ?, USA
Mean
rd 73
th 90
th 95
th 99
303
350
400
428
480
M Standing 2 Chest 1240 mm Handle Chaffin et al (2006),
Sample 309 males, Age ?, USA
Mean
th 35
th 90
th 95
th 99
418
350
646
710
833
M Standing and leaning forward
2 Shouder1400 mm
Handle Chaffin et al (2006),
Sample 205 males, Age ?, USA
Mean
th 90
th 95
th 99
245
385
424
499
M Standing, free posture
2 Shoulder height Handle, horizon
tal
DTI,( 2002) UK
Sample 6
males,
Age 21-30
44
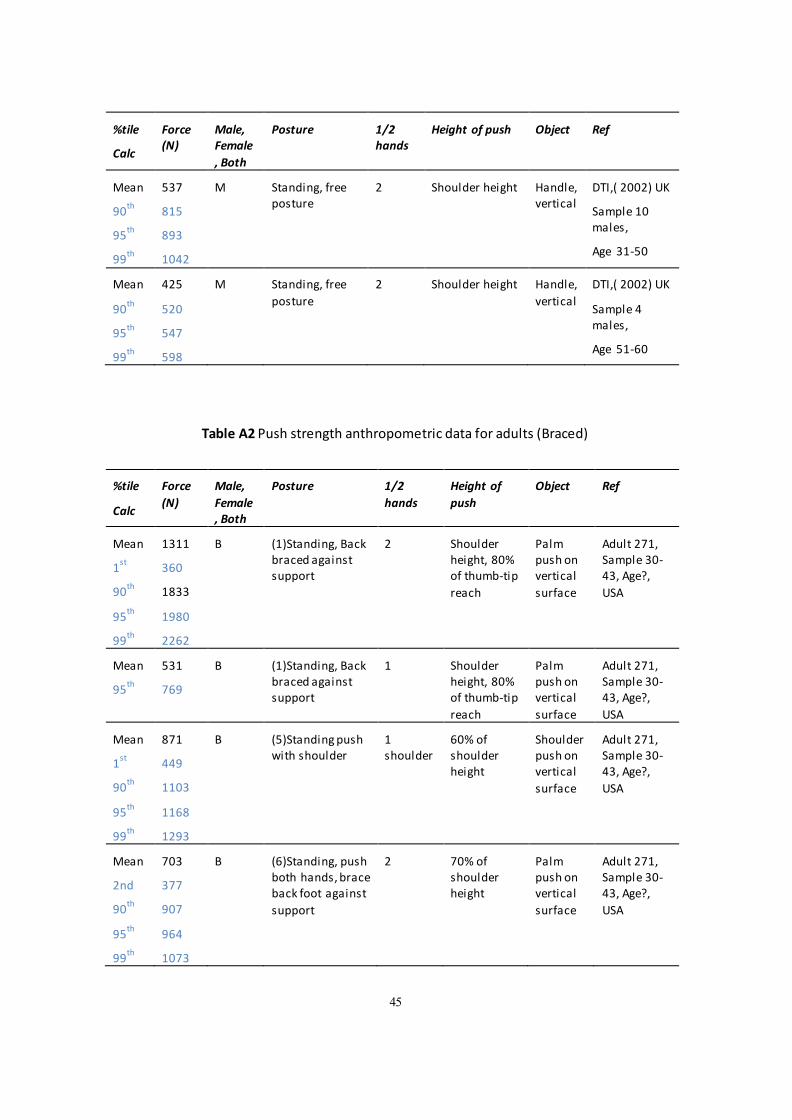
%tile
Calc
Force (N)
Male, Female
, Both
Posture 1/2 hands
Height of push Object Ref
Mean
th 90
th 95
th 99
537
815
893
1042
M Standing, free posture
2 Shoulder height Handle, vertical
DTI,( 2002) UK
Sample 10 males,
Age 31-50
Mean
th 90
th 95
th 99
425
520
547
598
M Standing, free
posture
2 Shoulder height Handle,
vertical
DTI,( 2002) UK
Sample 4 males,
Age 51-60
Table A2 Push strength anthropometric data for adults (Braced)
%tile
Calc
Force
(N)
Male,
Female , Both
Posture 1/2
hands
Height of
push
Object Ref
Mean
st 1
th 90
th 95
th 99
1311
360
1833
1980
2262
B (1)Standing, Back braced against support
2 Shoulder height, 80% of thumb-tip
reach
Palm push on vertical
surface
Adult 271, Sample 30-43, Age?,
USA
Mean
th 95
531
769
B (1)Standing, Back braced against support
1 Shoulder height, 80% of thumb-tip
reach
Palm push on vertical
surface
Adult 271, Sample 30-43, Age?,
USA
Mean
1st
90th
95th
99th
871
449
1103
1168
1293
B (5)Standing push with shoulder
1 shoulder
60% of shoulder height
Shoulder push on vertical
surface
Adult 271, Sample 30-43, Age?,
USA
Mean
2nd
90th
95th
99th
703
377
907
964
1073
B (6)Standing, push both hands, brace back foot against
support
2 70% of shoulder height
Palm push on vertical
surface
Adult 271, Sample 30-43, Age?,
USA
45
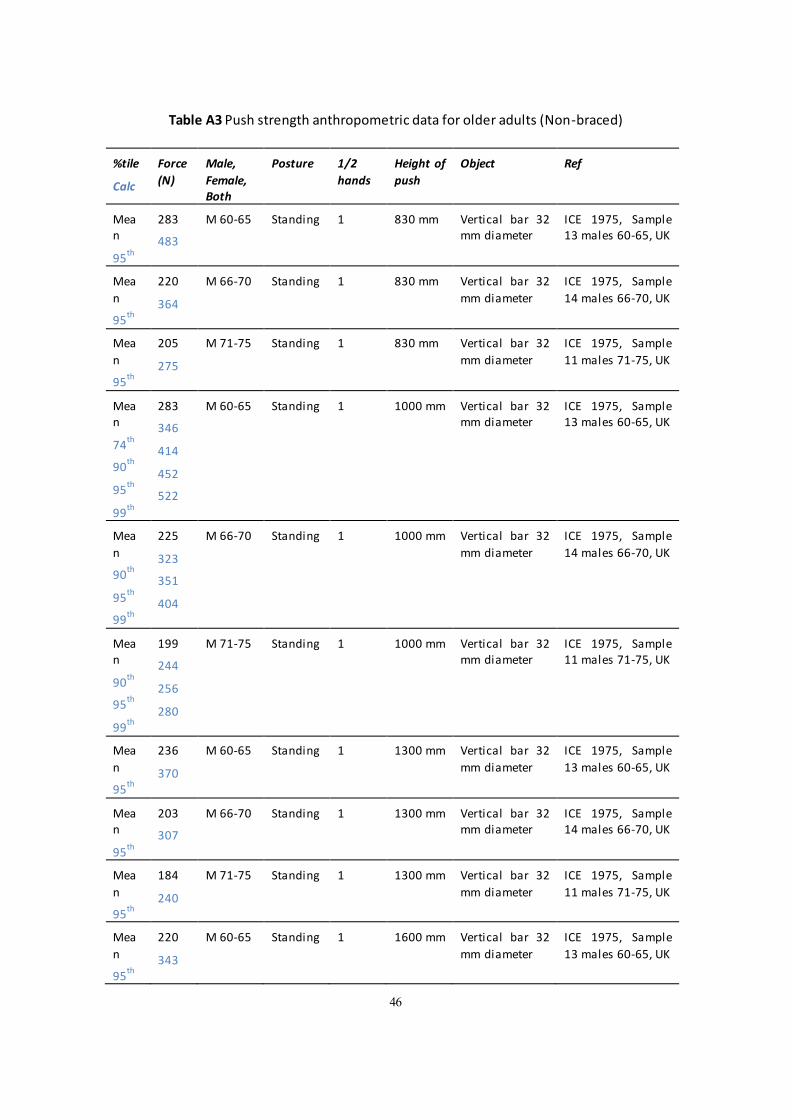
Table A3 Push strength anthropometric data for older adults (Non-braced)
%tile
Calc
Force
(N)
Male,
Female, Both
Posture 1/2
hands
Height of
push
Object Ref
Mea n
th 95
283
483
M 60-65 Standing 1 830 mm Vertical bar 32 mm diameter
ICE 1975, Sample 13 males 60-65, UK
Mea
n th
95
220
364
M 66-70 Standing 1 830 mm Vertical bar 32
mm diameter
ICE 1975, Sample
14 males 66-70, UK
Mea
n th
95
205
275
M 71-75 Standing 1 830 mm Vertical bar 32
mm diameter
ICE 1975, Sample
11 males 71-75, UK
Mea n
th 74
th 90
th 95
th 99
283
346
414
452
522
M 60-65 Standing 1 1000 mm Vertical bar 32 mm diameter
ICE 1975, Sample 13 males 60-65, UK
Mea
n th
90 th
95 th
99
225
323
351
404
M 66-70 Standing 1 1000 mm Vertical bar 32
mm diameter
ICE 1975, Sample
14 males 66-70, UK
Mea n
th 90
th 95
th 99
199
244
256
280
M 71-75 Standing 1 1000 mm Vertical bar 32 mm diameter
ICE 1975, Sample 11 males 71-75, UK
Mea
n th
95
236
370
M 60-65 Standing 1 1300 mm Vertical bar 32
mm diameter
ICE 1975, Sample
13 males 60-65, UK
Mea n
th 95
203
307
M 66-70 Standing 1 1300 mm Vertical bar 32 mm diameter
ICE 1975, Sample 14 males 66-70, UK
Mea
n th
95
184
240
M 71-75 Standing 1 1300 mm Vertical bar 32
mm diameter
ICE 1975, Sample
11 males 71-75, UK
Mea
n th
95
220
343
M 60-65 Standing 1 1600 mm Vertical bar 32
mm diameter
ICE 1975, Sample
13 males 60-65, UK
46
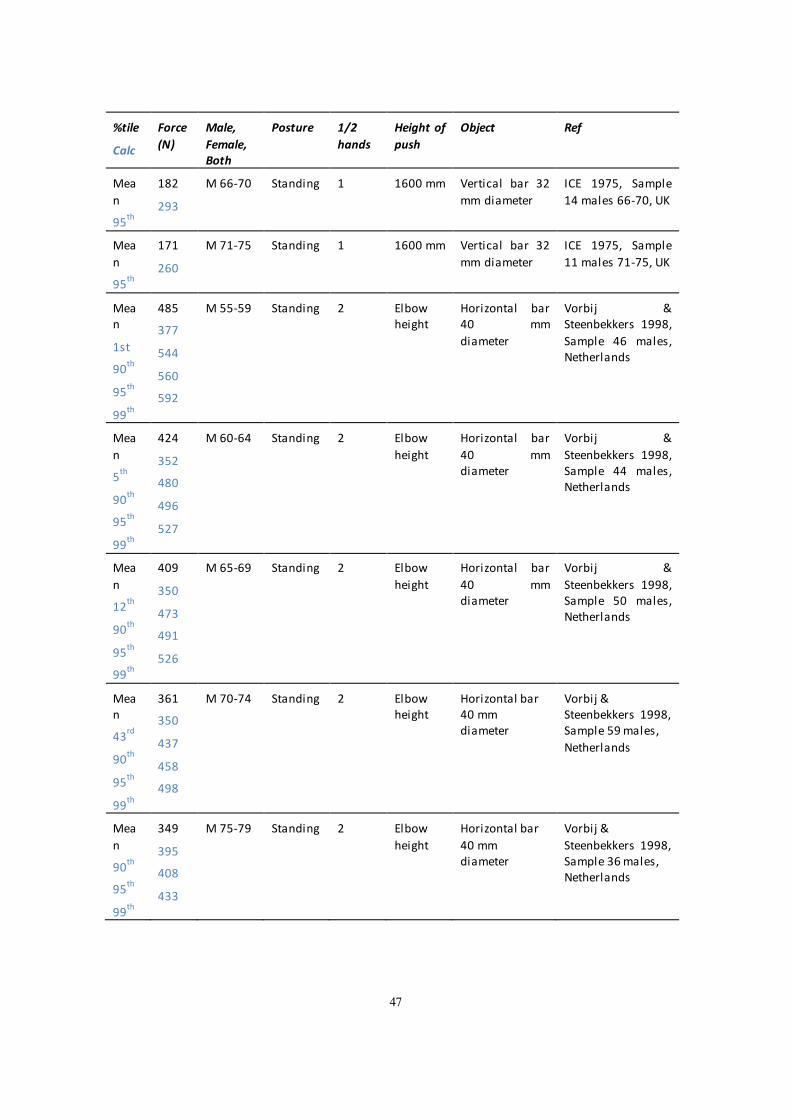
%tile
Calc
Force
(N)
Male,
Female, Both
Posture 1/2
hands
Height of
push
Object Ref
Mea
n th
95
182
293
M 66-70 Standing 1 1600 mm Vertical bar 32
mm diameter
ICE 1975, Sample
14 males 66-70, UK
Mea
n th
95
171
260
M 71-75 Standing 1 1600 mm Vertical bar 32
mm diameter
ICE 1975, Sample
11 males 71-75, UK
Mea n
1st th
90 th
95 th
99
485
377
544
560
592
M 55-59 Standing 2 Elbow height
Horizontal 40
diameter
bar mm
Vorbij & Steenbekkers 1998,
Sample 46 males, Netherlands
Mea
n th
5 th
90 th
95 th
99
424
352
480
496
527
M 60-64 Standing 2 Elbow
height
Horizontal
40 diameter
bar
mm
Vorbij &
Steenbekkers 1998, Sample 44 males, Netherlands
Mea
n th
12 th
90 th
95 th
99
409
350
473
491
526
M 65-69 Standing 2 Elbow
height
Horizontal
40 diameter
bar
mm
Vorbij &
Steenbekkers 1998, Sample 50 males, Netherlands
Mea n
rd 43
th 90
th 95
th 99
361
350
437
458
498
M 70-74 Standing 2 Elbow height
Horizontal bar 40 mm diameter
Vorbij & Steenbekkers 1998, Sample 59 males,
Netherlands
Mea
n th
90 th
95 th
99
349
395
408
433
M 75-79 Standing 2 Elbow
height
Horizontal bar
40 mm diameter
Vorbij &
Steenbekkers 1998, Sample 36 males, Netherlands
47
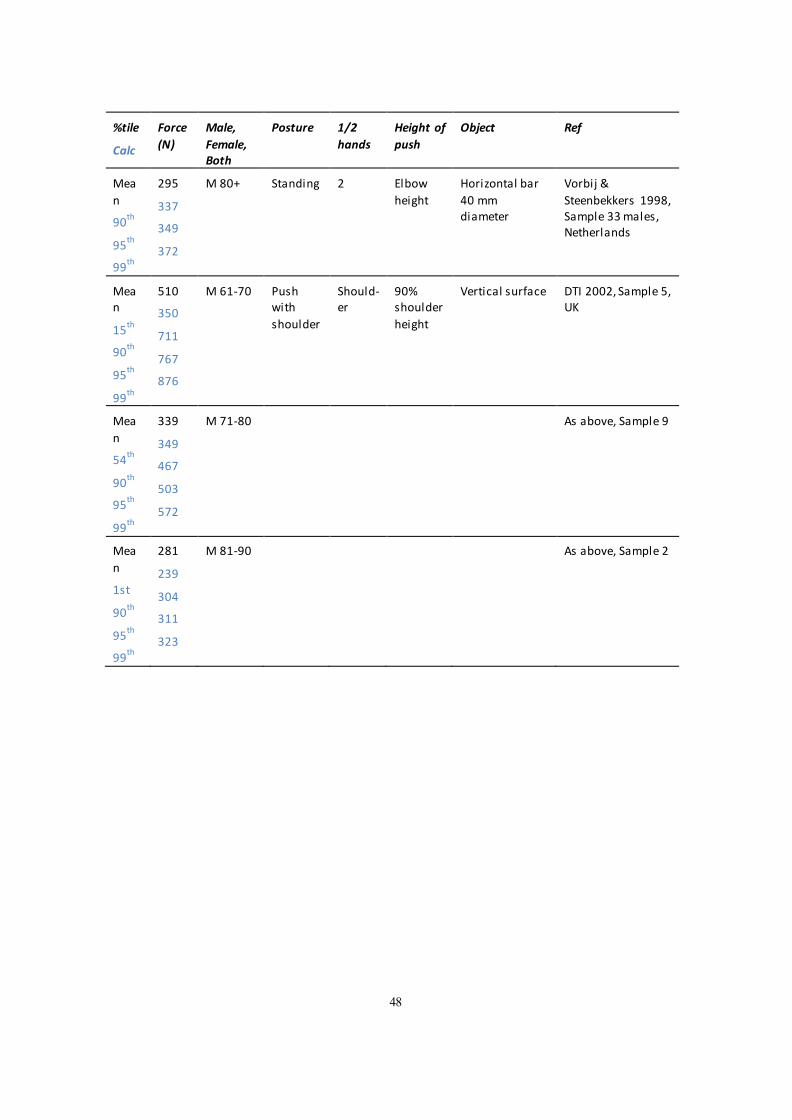
%tile
Calc
Force
(N)
Male,
Female, Both
Posture 1/2
hands
Height of
push
Object Ref
Mea
n th
90 th
95 th
99
295
337
349
372
M 80+ Standing 2 Elbow
height
Horizontal bar
40 mm diameter
Vorbij &
Steenbekkers 1998, Sample 33 males, Netherlands
Mea n
th 15
th 90
th 95
th 99
510
350
711
767
876
M 61-70 Push with
shoulder
Should-er
90% shoulder
height
Vertical surface DTI 2002, Sample 5, UK
Mea
n th
54 th
90th
95 th
99
339
349
467
503
572
M 71-80 As above, Sample 9
Mea
n
1st th
90th
95 th
99
281
239
304
311
323
M 81-90 As above, Sample 2
48
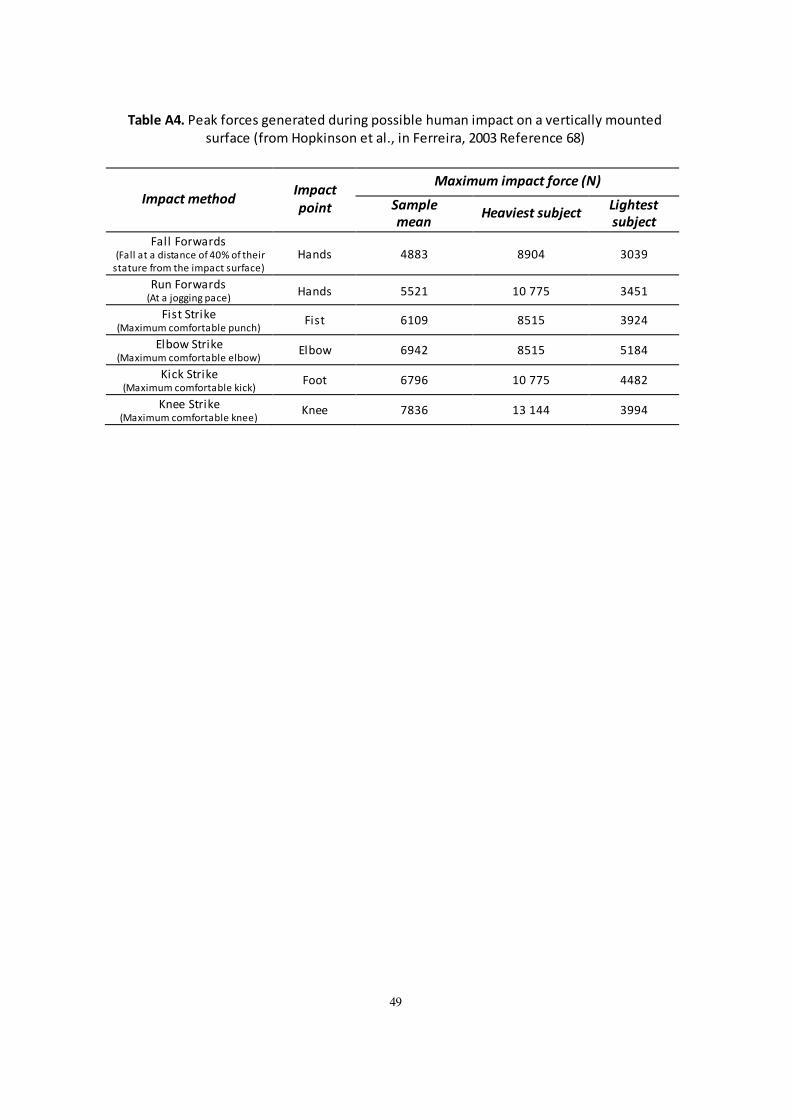
Table A4. Peak forces generated during possible human impact on a vertically mounted surface (from Hopkinson et al., in Ferreira, 2003 Reference 68)
Impact method Impact point
Maximum impact force (N)
Sample mean
Heaviest subject Lightest subject
Fall Forwards (Fall at a distance of 40% of their
stature from the impact surface) Hands 4883 8904 3039
Run Forwards (At a jogging pace)
Hands 5521 10 775 3451
Fist Strike (Maximum comfortable punch)
Fist 6109 8515 3924
Elbow Strike (Maximum comfortable elbow)
Elbow 6942 8515 5184
Kick Strike (Maximum comfortable kick)
Foot 6796 10 775 4482
Knee Strike (Maximum comfortable knee)
Knee 7836 13 144 3994
49

50
4
Published by the Health & Safety Executive 12/19
5
Review of window restrictors used in health and social care
Serious injuries and fatalities have occurred when people have fallen from windows in health and social care
premises. A vulnerable person may fall unintentionally when they are in a confused mental state, such as a person with dementia, or as a deliberate act of self-harm. Window restrictors may be used as part of managing the risk of
vulnerable people falling from windows. However, there is a lack of evidence-based advice on the minimum force that window restrictors should withstand for use in health and social care premises to protect vulnerable people.
This report describes research to identify the force that could reasonably be applied by an individual determined to
open a window that is above waist height. The researchers reviewed: incidents involving window restrictors; standards for design, production and installation of window restrictors; and ergonomic data. The researchers suggest
that for windows that are above waist height, window restrictors and their fixings should be capable of withstanding at least 850 N. This is based on an adult
exerting a static push force with both hands, pushing outwards on a handle at shoulder height in a non-braced, forward leaning posture. Where adults can use excessive force, body weight, impact or momentum to try to break or
open a window, it would not be appropriate to rely on a force guide of 850 N.
HSE Information Sheet ‘Falls from windows or balconies in health and social care’ HIS5 (2012) gives related information for providers of health and social care services.
This report and the work it describes were funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy.
RR1150
www.hse.gov.uk





























