Embed Size (px)
Citation preview

REVIEW Open Access
Overview of healthcare system in the CzechRepublicJudita Kinkorovaacute1 and Ondřej Topolčan2
Abstract
The healthcare system in the Czech Republic underwent and still is undergoing dramatic changes since the Velvetrevolution in 1989 History of the Czech healthcare system main healthcare laws and the current status ofhealthcare documented in the main healthcare indicators is described based on the several main sources as wellas delivery of health services and the role of the main actors in healthcare system The material is based mainly onCzech Health Statistics 2009 and HiT Summary Health Care Systems in Translation 2005 public information ofMinistry of Health CR
Keywords Czech Republic Healthcare system Politics Financing Predictive Preventive and Personalised MedicineRecommendations
IntroductionCountry descriptionThe Czech Republic is centrally located in the heart ofEurope with the area of 78865 square kilometres [1]and with an estimated population of 10542080 in 2011(Figure 1) ethnically and linguistically Czech (94)Other ethnic groups include Germans Roma Vietna-mese and Poles Czech Republic has a democratic par-liamentary system of government and a well-developedeconomy The Czech Republic has been a member ofthe Organisation for Economic Co-operation and Devel-opment (OECD) since December 1995 a member of theNorth Atlantic Treaty Organisation (NATO) since Feb-ruary 1999 and a member of the European Union (EU)since May 2004 [1]
History government and political system [2]After World War II the political system in Czechoslova-kia was greatly affected by the introduction of a Soviet-style Communist regime as it was in the other countriesof central and east Europe In February 1948 the Com-munist Party became the only autonomous politicalentity
After the revolutionary events so-called ldquoVelvet revo-lutionrdquo of November 1989 which brought about thedownfall of the Communist regime the entire countryfaced the uneasy task of resuming its pre-Communisttraditions and building a democratic political system Awide diversity of political parties was established evenbefore the break-up of Czechoslovakia on December 311992 The constitution of the Czech Republic whichbecame valid on the day of the birth of the new stateexplicitly defined civil rights the relationship betweenthe executive and legislative branches of power and theindependence of the judiciary
Population and demographyWith an estimated population of 10542080 at 30 June2011 compared to 93 million at the beginning of thetwentieth century the population growth of the CzechRepublic was limited and characterised by low fertilityrates and loss of population in and around World War Iand World War II Population growth resumed until1994 when the population was 103 million From 1994to 2005 natural growth was negative and the populationdecreased to 102 million Since 2006 natural growthhas been positive but the most important factor for therecent population of the Czech Republic has been immi-gration approximately 300000 during the last decade[1] Correspondence Kinkorovatccz
1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech RepublicFull list of author information is available at the end of the article
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
copy 2012 Kinkorovaacute and Topolčan licensee BioMed Central Ltd This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (httpcreativecommonsorglicensesby20) which permits unrestricted use distribution andreproduction in any medium provided the original work is properly cited
In 1994 the number of deaths exceeded the number ofbirths for the first time since 1918 and the population iscontinuing to decline Population by age in 2009 isshown in Figure 2Life expectancy at birth in the Czech Republic is con-
tinuously increasing having reached 772 in 2009 [3]The most frequent cause of death was and still is cir-
culatory system disease followed by malignant neo-plasms Despite the decrease of external causes (injuryor poisoning) these as a group are the third largestcause of death in 2009 The forth most common causeof death are respiratory system diseases followed by dis-eases of digestive system diabetes mellitus diseases ofthe blood and of the blood forming organs tuberculosisand infectious and parasitic diseasesVaccination coverage in the Czech Republic is very
high greater than 97 in all relevant immunisation cate-gories [4] Vaccination against tuberculosis diphtheriatetanus poliomyelitis and others are part of the compul-sory childhood vaccination schedule
The evolution of the Czech population (in 2009) ischaracterised by the number of live births decreasedthe number of deaths increased the natural populationincrease remained positive but was lower than in theprevious year Migration increase about 28 thousandpersons in 2009 The total population of the CzechRepublic increased but its age structure grew older [5]
History of healthcare systemHistory of healthcare system in Bohemia as a part ofAustro-Hungarian Monarchy has the roots in 1883when Otto von Bismarck established the health insur-ance as a part of the Bismarckrsquos model of social securityand health insurance system After Czechoslovakiarsquosindependence in 1918 the Bismarckrsquos healthcare systeminherited from the Monarchy was expanded and welldefined After the World War II Czechoslovakiabecomes a part of Soviet empire of influence which hadimportant negative impact on the healthcare system In1952 a soviet style centralised system of unified
Figure 1 Location of the Czech Republic in the Europe Taken from UN cartographic section
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 2 of 8
healthcare system so-called Semashko model was intro-duced The new system effectively solved the post-warproblems of the early 1950s In 1960s the modifiedSemashkorsquos healthcare system reached a turning pointand as a centralised and rigid in many aspects it provedunable to respond flexibly to new health problems aris-ing from life style changes and environmental factors[5]The new era of healthcare system in Czechoslovakia
started after so-called ldquoVelvet revolutionrdquo in 1989 Cze-choslovakia like other former soviet sphere countriesopted for the introduction of a Bismarckian type offinancing system which served as a transitional bridgetoward more market-oriented mechanisms and institu-tions [6] In 1990 and 1991 during the democratisationprocess a dramatic liberalisation of the healthcare sys-tem took place The principle of free choice of health-care facility was introduced In 1991 new laws wereapproved especially the General Health Insurance Act(No 5501991 Coll) and the Act on the General HealthInsurance Fund (No 5511991 Coll) Since then thehealthcare system has moved towards a compulsory
health insurance model with a number of insurersfinancing healthcare providers on the basis of contractsFrom the early 1990s considerable changes have been
implemented in the Czech healthcare system Themajority of the planned changes have taken place andthe implementation process has been remarkablysmooth A complete reconstruction of the healthcarefacilities and authorities has been achieved and a healthinsurance system has been created At the same timethere was an almost complete privatisation of primaryhealthcare the pharmaceutical industry pharmacieshealthcare support firms spa facilities etc [7]The healthcare system underwent a number of impor-
tant changes since 2005 five of them are listed below
1 the implementation between 2005 and 2006 of anew risk adjustment scheme for redistributing socialhealth insurance contributions among the healthinsurance funds2 the introduction in 2008 of user fees for doctorvisits hospital stays prescription pharmaceuticals eg and out-of-pocket payments
Figure 2 Population by age to 1 July 2009 Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 3 of 8
3 the inclusion in 2008 of the State Institute forDrug Control (Staacutetniacute uacutestav pro kontrolu lečivSUacuteKL) in the process of setting maximum prices forpharmaceuticals for transparency of price settings4 the introduction in 2008 of a programme to sup-ply accredited providers with additional financialsupport for training nurses and physicians5 an initiative to improve the quality of highly spe-cialised care by identifying high performing health-care facilities and allowing for special contractualconditions between these facilities and the healthinsurance funds
Organisation of health system in the CzechRepublicCzech health system is based on five pillars1 solidarity
- solidarity between healthy people and the sick isfostered in healthcare systems by separation betweenthe provision of healthcare and its financing- solidarity of the economically active with the eco-nomically inactive people means that every insuredperson pays an insurance premium as a percentageof their income regardless of what healthcare theyreceive or will receive
2 high degree of self-administration3 multisource financing with major share of public
health insurance Healthcare is funded from publichealth insurance direct payments the national budgetand regional budgets4 equal availability of healthcare for all insured per-
sons The healthcare system strives to create conditionsin which there are no differences in the availability ofhealthcare5 obligatory vaccination against infectious diseasesThese pillars are legally supported by following
selected laws
- Resolution of the Presidium of the Czech NationalCouncil 21993 promulgating the Charter of Funda-mental Rights and Freedoms as part of the Czechconstitutional order- Act 481997 Coll on public health insuranceamending some related laws- Act 201966 Coll on public healthcare amendingsome related laws- Act 5921992 Coll on premiums for generalhealth insurance amending some related laws- Act no 2582000 Coll on public health protectionand amendments to several related acts as amended[8]
Healthcare is in the Czech Republic is provided bystructured network of several types of healthcare someof them are listed below [68]
Outpatient careOutpatient care is provided by primary care physiciansor specialists If a person is taken ill they usually con-tact a primary care physician working near their homeThese are general practitioners for adults general practi-tioners for children and young people dentists andgynaecologistsWhen choosing a physician you should bear in mind
that you can only register with a physician who has con-cluded a contract with your insurance companyIf healthcare is to be reimbursed from public health
insurance the insured must first register with a primarycare physician (the local basic healthcare provider) Aphysician may only refuse to register an insured personif the registration brought to the physician so muchwork that it would not permit provision of quality careto the patient or other patients in the physicianrsquos careA patient can visit a specialist physician in the Czech
Republic without a referral from the primary carephysician
Institutional (inpatient) careIf the nature of an illness demands this a primary carephysician or outpatient specialist can refer a patient forhospital treatment or arrange for their admittanceInpatient care is provided in hospitals and specialised
institutions such as psychiatric hospitals and rehabilita-tion centres hospices sanatoria long-term carehospitals
Ambulance and emergency rescue serviceEmergency rescue service is available to deal with casesof acute illness or accident when a patient cannot get toa physician and immediate treatment is needed andtransport of the patient to a healthcare facility underpermanent care to prevent further aggravation of theirhealth conditions or threat to the life
Balneological careBalneological care can be regarded as an essential partof the curative process It is recommended by onersquosattending physician and confirmed by a reviewing physi-cian Entitlement to balneological care is claimed on apre-printed form by the registering general physician orattending physician in case of hospitalisation
Long-term careLong-term care for older or disabled people is providedin two overlapping settings with different systems of
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 4 of 8
organisation and funding residential long-term carefacilities and other social services financed from centralregional or municipal budgets and healthcare facilitiesfor long-term inpatient care financed primarily throughthe social health insurance
Mental healthcareMental healthcare is provided both in the ambulatorysettings and in inpatient facilities which include hospitalpsychiatric departments psychiatric hospitals and psy-chiatric institutes
Dispensing medicaments and medical devicesIn the Czech Republic there is an extensive network ofpharmacies dispensing medicaments and medicaldevices both on prescription and over the counter
Preventive carePreventive examinations and vaccination against infec-tious diseases are performed by primary care physicians
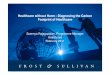
FinancingIn 2010 as in the preceding years the predominant partof health expenditure was financed by the public healthinsurance system covering 766 of the total (in Figure3 is shown expenditure on health services by sources of
financing) The State and territorial budgets covered72 and private expenditure covered 162 The shareof private expenditure in the total expenditure on healthrose particularly after 2008 due to new regulation feesin health services In 2010 the private expenditure onhealth slightly decreased partly as a result of softeningof the regulation fees and of stagnant purchasing powerof the population The total expenditure on healthincreased from 2009 by 821 million CZK and in 2010 itamounted in absolute value to 290 412 million CZK ie27 613 CZK per 1 inhabitant This total expenditurerepresents 769 of the GDP in 2010 Public expendi-ture ie that of the public budgets and of the publichealth insurance system totally 243 283 million CZKby 1 646 million CZK more than in the preceding year(all data are preliminary) [9]Healthcare in the Czech Republic is provided primar-
ily on the basis of statutory health insurance which iscurrently provided by nine health insurance fundsThe largest health insurance fund - the General
Health Insurance Fund GHIF - has 77 district branchesAny person with a permanent residence in the CzechRepublic is entitled to health insuranceHealthcare services are covered by the health insur-
ance funds The following services are fully or partiallycovered by health insurance [8]
Figure 3 Expenditure on health services by sources of financing Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 5 of 8
1 outpatient and institutional (inpatient) care2 emergency and ambulance services3 preventive care4 dispensary care5 supply of medicaments medical supplies (eg hear-
ing aids bandages)6 balneological care care in specialised childrenrsquos hos-
pitals and sanatoria7 industrial healthcare8 transport of the sick reimbursement of travel
expenses9 deceased examination and autopsyThere are many procedures which insured persons co-
finance These are procedures or medical devices pro-vided outside the legal framework Some cases in pointare dental procedures some balneological care andsome medicaments Some medicaments are reimbursedin full by insurance companies whereas some are co-financed by the patients In every category of medica-ments there must be at least one reimbursed in full byan insurer Costs of medicaments and medical devicesduring hospitalisation are reimbursed in full by theinsurer and the insured person does not pay directly
International comparisonThis part contains comparison of the shares of expendi-ture on health in gross domestic product (GDP) inselected countries in Europe (Figure 4) The source ofthese data is the Database OECD Health Data 2011Ageing of the population is a phenomenon that charac-
terises in the long term the demographic evolution ofmost European countries As a result of the decreasingnatality the share of persons older than 64 years increasesThe age preference index defined as the number of
persons aged 65 years or more per 100 children exceedsthe value 100 in increasing numbers of countries Itmeans that there are more seniors than children This isalready so in 35 of EU member countries most mark-edly in Germany and in Italy On the opposite pole arethe ldquoyoungestrdquo countries Albania Ireland and Icelandwhere the share of seniors is only about one half of itsvalue in Germany and ItalyThe Czech Republic belongs to countries with a low
share of children up to 15 years old (142 in 2009)With its share of persons in the age group of 65 ormore years (150 in 2009) the CR still does not reachthe European Union average that exceeded 17 in 2007In 2006 the Czech Republic joined the group of coun-tries with more persons over 64 than children The agepreference index in 2009 reached the value 107Another common feature of most European countries
is the decreasing mortality connected with growinglength of human life The average value of standardiseddeath rate (that eliminates the influence of the age
structure of the population further SDR) shows a long-term decreasing trend in European Union (EU) as well asin EU-15 (member countries before May 2004) and inEU-12 (new member countries that joined EU in 2004and 2007) The average values of the total SDR in EU-12exceed the averages in EU-15 by 23 in men and byalmost 12 in women The SDR values in the CzechRepublic in spite of the marked decrease in the past twodecreases still exceed not only the averages of EU-15 (byalmost 40 in men and by ca 30 in women) but alsoof the whole EU by 15 both in men and women
Current status of the PPPM in the Czech RepublicThere is no conception of PPPM (predictive preventiveand personalised medicine) in the Czech Republic offi-cially proposed by policy makers as eg Ministry ofHealth of the Czech Republic (MoH) and NationalInstitute of Public Health (SZUacute) Ministry of Labour andSocial Affairs (MoLSA) and other governmental bodiesThe main document regarding the national health policyis ldquoMinistry of Health Departmental Program forResearch and Development III (DPR III)rdquo [10] withsome aspects regarding basic principles of PPPM As anexample of this approach the SZUacute is responsible for pre-ventive services covering
1 compulsory vaccination and preventive examina-tions for children of specific age groups2 compulsory vaccination and periodic examinationsby general practitioner very two years3 well organised cancer screening programmes (egcolo-rectal cancer breast cancer cervical cancer)4 mammography for women 45-69 every two yearspreventive gynaecological examinations includingcytology from the age of 155 regular vaccination covering 99 of the popula-tion (tuberculosis tetanus diphtheria pertussispoliomyelitis measles mumps and rubella cervicalcancer from 2001 also hepatitis B and Haemophilusinfluenzae type B [5]
Several additional preventive care services are deliv-ered to the Czech citizens reducing alcohol harm treat-ing drug addiction tackling obesity especially inchildren prevention of smoking sexual health educa-tion life style health risksThe current situation in the Czech Republic is charac-
terised by raising awareness and recognition of PPPMpromotion of education and up to date informationEducation of PPPM is one of the initial activities The
only educational centres are universities and researchinstitutes The concept of PPPM national education isstill under preparation at both non-professional (gen-eral) and professionals in personalised medicine
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 6 of 8
Following steps will include graduate post graduateand continuing education programmes for young andexperienced researchers and medical staff those who willbe taking the PPPM forward in the coming years
RecommendationsBasic principles of PPPM should be incorporated intobasic strategic documents of policy makers (MoH SZUacuteMoLSA) with ethical legal and social issues involved
Educational programmes for students and profes-sionals at all levels in conventional and molecular diag-nostics biomedicine biotechnologies ethics andeconomics for universities research units private andpublic hospitals and publicndashpatients and their familymembers with all necessary materials should be system-atically preparedAll relevant partners like policy makers stakeholders
pharmacy biomedical industry universities research
Figure 4 Proportion of total expenditure on health services in gross domestic product (GDP) Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 7 of 8
centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8

In 1994 the number of deaths exceeded the number ofbirths for the first time since 1918 and the population iscontinuing to decline Population by age in 2009 isshown in Figure 2Life expectancy at birth in the Czech Republic is con-
tinuously increasing having reached 772 in 2009 [3]The most frequent cause of death was and still is cir-
culatory system disease followed by malignant neo-plasms Despite the decrease of external causes (injuryor poisoning) these as a group are the third largestcause of death in 2009 The forth most common causeof death are respiratory system diseases followed by dis-eases of digestive system diabetes mellitus diseases ofthe blood and of the blood forming organs tuberculosisand infectious and parasitic diseasesVaccination coverage in the Czech Republic is very
high greater than 97 in all relevant immunisation cate-gories [4] Vaccination against tuberculosis diphtheriatetanus poliomyelitis and others are part of the compul-sory childhood vaccination schedule
The evolution of the Czech population (in 2009) ischaracterised by the number of live births decreasedthe number of deaths increased the natural populationincrease remained positive but was lower than in theprevious year Migration increase about 28 thousandpersons in 2009 The total population of the CzechRepublic increased but its age structure grew older [5]
History of healthcare systemHistory of healthcare system in Bohemia as a part ofAustro-Hungarian Monarchy has the roots in 1883when Otto von Bismarck established the health insur-ance as a part of the Bismarckrsquos model of social securityand health insurance system After Czechoslovakiarsquosindependence in 1918 the Bismarckrsquos healthcare systeminherited from the Monarchy was expanded and welldefined After the World War II Czechoslovakiabecomes a part of Soviet empire of influence which hadimportant negative impact on the healthcare system In1952 a soviet style centralised system of unified
Figure 1 Location of the Czech Republic in the Europe Taken from UN cartographic section
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 2 of 8
healthcare system so-called Semashko model was intro-duced The new system effectively solved the post-warproblems of the early 1950s In 1960s the modifiedSemashkorsquos healthcare system reached a turning pointand as a centralised and rigid in many aspects it provedunable to respond flexibly to new health problems aris-ing from life style changes and environmental factors[5]The new era of healthcare system in Czechoslovakia
started after so-called ldquoVelvet revolutionrdquo in 1989 Cze-choslovakia like other former soviet sphere countriesopted for the introduction of a Bismarckian type offinancing system which served as a transitional bridgetoward more market-oriented mechanisms and institu-tions [6] In 1990 and 1991 during the democratisationprocess a dramatic liberalisation of the healthcare sys-tem took place The principle of free choice of health-care facility was introduced In 1991 new laws wereapproved especially the General Health Insurance Act(No 5501991 Coll) and the Act on the General HealthInsurance Fund (No 5511991 Coll) Since then thehealthcare system has moved towards a compulsory
health insurance model with a number of insurersfinancing healthcare providers on the basis of contractsFrom the early 1990s considerable changes have been
implemented in the Czech healthcare system Themajority of the planned changes have taken place andthe implementation process has been remarkablysmooth A complete reconstruction of the healthcarefacilities and authorities has been achieved and a healthinsurance system has been created At the same timethere was an almost complete privatisation of primaryhealthcare the pharmaceutical industry pharmacieshealthcare support firms spa facilities etc [7]The healthcare system underwent a number of impor-
tant changes since 2005 five of them are listed below
1 the implementation between 2005 and 2006 of anew risk adjustment scheme for redistributing socialhealth insurance contributions among the healthinsurance funds2 the introduction in 2008 of user fees for doctorvisits hospital stays prescription pharmaceuticals eg and out-of-pocket payments
Figure 2 Population by age to 1 July 2009 Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 3 of 8
3 the inclusion in 2008 of the State Institute forDrug Control (Staacutetniacute uacutestav pro kontrolu lečivSUacuteKL) in the process of setting maximum prices forpharmaceuticals for transparency of price settings4 the introduction in 2008 of a programme to sup-ply accredited providers with additional financialsupport for training nurses and physicians5 an initiative to improve the quality of highly spe-cialised care by identifying high performing health-care facilities and allowing for special contractualconditions between these facilities and the healthinsurance funds
Organisation of health system in the CzechRepublicCzech health system is based on five pillars1 solidarity
- solidarity between healthy people and the sick isfostered in healthcare systems by separation betweenthe provision of healthcare and its financing- solidarity of the economically active with the eco-nomically inactive people means that every insuredperson pays an insurance premium as a percentageof their income regardless of what healthcare theyreceive or will receive
2 high degree of self-administration3 multisource financing with major share of public
health insurance Healthcare is funded from publichealth insurance direct payments the national budgetand regional budgets4 equal availability of healthcare for all insured per-
sons The healthcare system strives to create conditionsin which there are no differences in the availability ofhealthcare5 obligatory vaccination against infectious diseasesThese pillars are legally supported by following
selected laws
- Resolution of the Presidium of the Czech NationalCouncil 21993 promulgating the Charter of Funda-mental Rights and Freedoms as part of the Czechconstitutional order- Act 481997 Coll on public health insuranceamending some related laws- Act 201966 Coll on public healthcare amendingsome related laws- Act 5921992 Coll on premiums for generalhealth insurance amending some related laws- Act no 2582000 Coll on public health protectionand amendments to several related acts as amended[8]
Healthcare is in the Czech Republic is provided bystructured network of several types of healthcare someof them are listed below [68]
Outpatient careOutpatient care is provided by primary care physiciansor specialists If a person is taken ill they usually con-tact a primary care physician working near their homeThese are general practitioners for adults general practi-tioners for children and young people dentists andgynaecologistsWhen choosing a physician you should bear in mind
that you can only register with a physician who has con-cluded a contract with your insurance companyIf healthcare is to be reimbursed from public health
insurance the insured must first register with a primarycare physician (the local basic healthcare provider) Aphysician may only refuse to register an insured personif the registration brought to the physician so muchwork that it would not permit provision of quality careto the patient or other patients in the physicianrsquos careA patient can visit a specialist physician in the Czech
Republic without a referral from the primary carephysician
Institutional (inpatient) careIf the nature of an illness demands this a primary carephysician or outpatient specialist can refer a patient forhospital treatment or arrange for their admittanceInpatient care is provided in hospitals and specialised
institutions such as psychiatric hospitals and rehabilita-tion centres hospices sanatoria long-term carehospitals
Ambulance and emergency rescue serviceEmergency rescue service is available to deal with casesof acute illness or accident when a patient cannot get toa physician and immediate treatment is needed andtransport of the patient to a healthcare facility underpermanent care to prevent further aggravation of theirhealth conditions or threat to the life
Balneological careBalneological care can be regarded as an essential partof the curative process It is recommended by onersquosattending physician and confirmed by a reviewing physi-cian Entitlement to balneological care is claimed on apre-printed form by the registering general physician orattending physician in case of hospitalisation
Long-term careLong-term care for older or disabled people is providedin two overlapping settings with different systems of
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 4 of 8
organisation and funding residential long-term carefacilities and other social services financed from centralregional or municipal budgets and healthcare facilitiesfor long-term inpatient care financed primarily throughthe social health insurance
Mental healthcareMental healthcare is provided both in the ambulatorysettings and in inpatient facilities which include hospitalpsychiatric departments psychiatric hospitals and psy-chiatric institutes
Dispensing medicaments and medical devicesIn the Czech Republic there is an extensive network ofpharmacies dispensing medicaments and medicaldevices both on prescription and over the counter
Preventive carePreventive examinations and vaccination against infec-tious diseases are performed by primary care physicians
FinancingIn 2010 as in the preceding years the predominant partof health expenditure was financed by the public healthinsurance system covering 766 of the total (in Figure3 is shown expenditure on health services by sources of
financing) The State and territorial budgets covered72 and private expenditure covered 162 The shareof private expenditure in the total expenditure on healthrose particularly after 2008 due to new regulation feesin health services In 2010 the private expenditure onhealth slightly decreased partly as a result of softeningof the regulation fees and of stagnant purchasing powerof the population The total expenditure on healthincreased from 2009 by 821 million CZK and in 2010 itamounted in absolute value to 290 412 million CZK ie27 613 CZK per 1 inhabitant This total expenditurerepresents 769 of the GDP in 2010 Public expendi-ture ie that of the public budgets and of the publichealth insurance system totally 243 283 million CZKby 1 646 million CZK more than in the preceding year(all data are preliminary) [9]Healthcare in the Czech Republic is provided primar-
ily on the basis of statutory health insurance which iscurrently provided by nine health insurance fundsThe largest health insurance fund - the General
Health Insurance Fund GHIF - has 77 district branchesAny person with a permanent residence in the CzechRepublic is entitled to health insuranceHealthcare services are covered by the health insur-
ance funds The following services are fully or partiallycovered by health insurance [8]
Figure 3 Expenditure on health services by sources of financing Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 5 of 8
1 outpatient and institutional (inpatient) care2 emergency and ambulance services3 preventive care4 dispensary care5 supply of medicaments medical supplies (eg hear-
ing aids bandages)6 balneological care care in specialised childrenrsquos hos-
pitals and sanatoria7 industrial healthcare8 transport of the sick reimbursement of travel
expenses9 deceased examination and autopsyThere are many procedures which insured persons co-
finance These are procedures or medical devices pro-vided outside the legal framework Some cases in pointare dental procedures some balneological care andsome medicaments Some medicaments are reimbursedin full by insurance companies whereas some are co-financed by the patients In every category of medica-ments there must be at least one reimbursed in full byan insurer Costs of medicaments and medical devicesduring hospitalisation are reimbursed in full by theinsurer and the insured person does not pay directly
International comparisonThis part contains comparison of the shares of expendi-ture on health in gross domestic product (GDP) inselected countries in Europe (Figure 4) The source ofthese data is the Database OECD Health Data 2011Ageing of the population is a phenomenon that charac-
terises in the long term the demographic evolution ofmost European countries As a result of the decreasingnatality the share of persons older than 64 years increasesThe age preference index defined as the number of
persons aged 65 years or more per 100 children exceedsthe value 100 in increasing numbers of countries Itmeans that there are more seniors than children This isalready so in 35 of EU member countries most mark-edly in Germany and in Italy On the opposite pole arethe ldquoyoungestrdquo countries Albania Ireland and Icelandwhere the share of seniors is only about one half of itsvalue in Germany and ItalyThe Czech Republic belongs to countries with a low
share of children up to 15 years old (142 in 2009)With its share of persons in the age group of 65 ormore years (150 in 2009) the CR still does not reachthe European Union average that exceeded 17 in 2007In 2006 the Czech Republic joined the group of coun-tries with more persons over 64 than children The agepreference index in 2009 reached the value 107Another common feature of most European countries
is the decreasing mortality connected with growinglength of human life The average value of standardiseddeath rate (that eliminates the influence of the age
structure of the population further SDR) shows a long-term decreasing trend in European Union (EU) as well asin EU-15 (member countries before May 2004) and inEU-12 (new member countries that joined EU in 2004and 2007) The average values of the total SDR in EU-12exceed the averages in EU-15 by 23 in men and byalmost 12 in women The SDR values in the CzechRepublic in spite of the marked decrease in the past twodecreases still exceed not only the averages of EU-15 (byalmost 40 in men and by ca 30 in women) but alsoof the whole EU by 15 both in men and women
Current status of the PPPM in the Czech RepublicThere is no conception of PPPM (predictive preventiveand personalised medicine) in the Czech Republic offi-cially proposed by policy makers as eg Ministry ofHealth of the Czech Republic (MoH) and NationalInstitute of Public Health (SZUacute) Ministry of Labour andSocial Affairs (MoLSA) and other governmental bodiesThe main document regarding the national health policyis ldquoMinistry of Health Departmental Program forResearch and Development III (DPR III)rdquo [10] withsome aspects regarding basic principles of PPPM As anexample of this approach the SZUacute is responsible for pre-ventive services covering
1 compulsory vaccination and preventive examina-tions for children of specific age groups2 compulsory vaccination and periodic examinationsby general practitioner very two years3 well organised cancer screening programmes (egcolo-rectal cancer breast cancer cervical cancer)4 mammography for women 45-69 every two yearspreventive gynaecological examinations includingcytology from the age of 155 regular vaccination covering 99 of the popula-tion (tuberculosis tetanus diphtheria pertussispoliomyelitis measles mumps and rubella cervicalcancer from 2001 also hepatitis B and Haemophilusinfluenzae type B [5]
Several additional preventive care services are deliv-ered to the Czech citizens reducing alcohol harm treat-ing drug addiction tackling obesity especially inchildren prevention of smoking sexual health educa-tion life style health risksThe current situation in the Czech Republic is charac-
terised by raising awareness and recognition of PPPMpromotion of education and up to date informationEducation of PPPM is one of the initial activities The
only educational centres are universities and researchinstitutes The concept of PPPM national education isstill under preparation at both non-professional (gen-eral) and professionals in personalised medicine
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 6 of 8
Following steps will include graduate post graduateand continuing education programmes for young andexperienced researchers and medical staff those who willbe taking the PPPM forward in the coming years
RecommendationsBasic principles of PPPM should be incorporated intobasic strategic documents of policy makers (MoH SZUacuteMoLSA) with ethical legal and social issues involved
Educational programmes for students and profes-sionals at all levels in conventional and molecular diag-nostics biomedicine biotechnologies ethics andeconomics for universities research units private andpublic hospitals and publicndashpatients and their familymembers with all necessary materials should be system-atically preparedAll relevant partners like policy makers stakeholders
pharmacy biomedical industry universities research
Figure 4 Proportion of total expenditure on health services in gross domestic product (GDP) Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 7 of 8
centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8

healthcare system so-called Semashko model was intro-duced The new system effectively solved the post-warproblems of the early 1950s In 1960s the modifiedSemashkorsquos healthcare system reached a turning pointand as a centralised and rigid in many aspects it provedunable to respond flexibly to new health problems aris-ing from life style changes and environmental factors[5]The new era of healthcare system in Czechoslovakia
started after so-called ldquoVelvet revolutionrdquo in 1989 Cze-choslovakia like other former soviet sphere countriesopted for the introduction of a Bismarckian type offinancing system which served as a transitional bridgetoward more market-oriented mechanisms and institu-tions [6] In 1990 and 1991 during the democratisationprocess a dramatic liberalisation of the healthcare sys-tem took place The principle of free choice of health-care facility was introduced In 1991 new laws wereapproved especially the General Health Insurance Act(No 5501991 Coll) and the Act on the General HealthInsurance Fund (No 5511991 Coll) Since then thehealthcare system has moved towards a compulsory
health insurance model with a number of insurersfinancing healthcare providers on the basis of contractsFrom the early 1990s considerable changes have been
implemented in the Czech healthcare system Themajority of the planned changes have taken place andthe implementation process has been remarkablysmooth A complete reconstruction of the healthcarefacilities and authorities has been achieved and a healthinsurance system has been created At the same timethere was an almost complete privatisation of primaryhealthcare the pharmaceutical industry pharmacieshealthcare support firms spa facilities etc [7]The healthcare system underwent a number of impor-
tant changes since 2005 five of them are listed below
1 the implementation between 2005 and 2006 of anew risk adjustment scheme for redistributing socialhealth insurance contributions among the healthinsurance funds2 the introduction in 2008 of user fees for doctorvisits hospital stays prescription pharmaceuticals eg and out-of-pocket payments
Figure 2 Population by age to 1 July 2009 Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 3 of 8
3 the inclusion in 2008 of the State Institute forDrug Control (Staacutetniacute uacutestav pro kontrolu lečivSUacuteKL) in the process of setting maximum prices forpharmaceuticals for transparency of price settings4 the introduction in 2008 of a programme to sup-ply accredited providers with additional financialsupport for training nurses and physicians5 an initiative to improve the quality of highly spe-cialised care by identifying high performing health-care facilities and allowing for special contractualconditions between these facilities and the healthinsurance funds
Organisation of health system in the CzechRepublicCzech health system is based on five pillars1 solidarity
- solidarity between healthy people and the sick isfostered in healthcare systems by separation betweenthe provision of healthcare and its financing- solidarity of the economically active with the eco-nomically inactive people means that every insuredperson pays an insurance premium as a percentageof their income regardless of what healthcare theyreceive or will receive
2 high degree of self-administration3 multisource financing with major share of public
health insurance Healthcare is funded from publichealth insurance direct payments the national budgetand regional budgets4 equal availability of healthcare for all insured per-
sons The healthcare system strives to create conditionsin which there are no differences in the availability ofhealthcare5 obligatory vaccination against infectious diseasesThese pillars are legally supported by following
selected laws
- Resolution of the Presidium of the Czech NationalCouncil 21993 promulgating the Charter of Funda-mental Rights and Freedoms as part of the Czechconstitutional order- Act 481997 Coll on public health insuranceamending some related laws- Act 201966 Coll on public healthcare amendingsome related laws- Act 5921992 Coll on premiums for generalhealth insurance amending some related laws- Act no 2582000 Coll on public health protectionand amendments to several related acts as amended[8]
Healthcare is in the Czech Republic is provided bystructured network of several types of healthcare someof them are listed below [68]
Outpatient careOutpatient care is provided by primary care physiciansor specialists If a person is taken ill they usually con-tact a primary care physician working near their homeThese are general practitioners for adults general practi-tioners for children and young people dentists andgynaecologistsWhen choosing a physician you should bear in mind
that you can only register with a physician who has con-cluded a contract with your insurance companyIf healthcare is to be reimbursed from public health
insurance the insured must first register with a primarycare physician (the local basic healthcare provider) Aphysician may only refuse to register an insured personif the registration brought to the physician so muchwork that it would not permit provision of quality careto the patient or other patients in the physicianrsquos careA patient can visit a specialist physician in the Czech
Republic without a referral from the primary carephysician
Institutional (inpatient) careIf the nature of an illness demands this a primary carephysician or outpatient specialist can refer a patient forhospital treatment or arrange for their admittanceInpatient care is provided in hospitals and specialised
institutions such as psychiatric hospitals and rehabilita-tion centres hospices sanatoria long-term carehospitals
Ambulance and emergency rescue serviceEmergency rescue service is available to deal with casesof acute illness or accident when a patient cannot get toa physician and immediate treatment is needed andtransport of the patient to a healthcare facility underpermanent care to prevent further aggravation of theirhealth conditions or threat to the life
Balneological careBalneological care can be regarded as an essential partof the curative process It is recommended by onersquosattending physician and confirmed by a reviewing physi-cian Entitlement to balneological care is claimed on apre-printed form by the registering general physician orattending physician in case of hospitalisation
Long-term careLong-term care for older or disabled people is providedin two overlapping settings with different systems of
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 4 of 8
organisation and funding residential long-term carefacilities and other social services financed from centralregional or municipal budgets and healthcare facilitiesfor long-term inpatient care financed primarily throughthe social health insurance
Mental healthcareMental healthcare is provided both in the ambulatorysettings and in inpatient facilities which include hospitalpsychiatric departments psychiatric hospitals and psy-chiatric institutes
Dispensing medicaments and medical devicesIn the Czech Republic there is an extensive network ofpharmacies dispensing medicaments and medicaldevices both on prescription and over the counter
Preventive carePreventive examinations and vaccination against infec-tious diseases are performed by primary care physicians
FinancingIn 2010 as in the preceding years the predominant partof health expenditure was financed by the public healthinsurance system covering 766 of the total (in Figure3 is shown expenditure on health services by sources of
financing) The State and territorial budgets covered72 and private expenditure covered 162 The shareof private expenditure in the total expenditure on healthrose particularly after 2008 due to new regulation feesin health services In 2010 the private expenditure onhealth slightly decreased partly as a result of softeningof the regulation fees and of stagnant purchasing powerof the population The total expenditure on healthincreased from 2009 by 821 million CZK and in 2010 itamounted in absolute value to 290 412 million CZK ie27 613 CZK per 1 inhabitant This total expenditurerepresents 769 of the GDP in 2010 Public expendi-ture ie that of the public budgets and of the publichealth insurance system totally 243 283 million CZKby 1 646 million CZK more than in the preceding year(all data are preliminary) [9]Healthcare in the Czech Republic is provided primar-
ily on the basis of statutory health insurance which iscurrently provided by nine health insurance fundsThe largest health insurance fund - the General
Health Insurance Fund GHIF - has 77 district branchesAny person with a permanent residence in the CzechRepublic is entitled to health insuranceHealthcare services are covered by the health insur-
ance funds The following services are fully or partiallycovered by health insurance [8]
Figure 3 Expenditure on health services by sources of financing Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 5 of 8
1 outpatient and institutional (inpatient) care2 emergency and ambulance services3 preventive care4 dispensary care5 supply of medicaments medical supplies (eg hear-
ing aids bandages)6 balneological care care in specialised childrenrsquos hos-
pitals and sanatoria7 industrial healthcare8 transport of the sick reimbursement of travel
expenses9 deceased examination and autopsyThere are many procedures which insured persons co-
finance These are procedures or medical devices pro-vided outside the legal framework Some cases in pointare dental procedures some balneological care andsome medicaments Some medicaments are reimbursedin full by insurance companies whereas some are co-financed by the patients In every category of medica-ments there must be at least one reimbursed in full byan insurer Costs of medicaments and medical devicesduring hospitalisation are reimbursed in full by theinsurer and the insured person does not pay directly
International comparisonThis part contains comparison of the shares of expendi-ture on health in gross domestic product (GDP) inselected countries in Europe (Figure 4) The source ofthese data is the Database OECD Health Data 2011Ageing of the population is a phenomenon that charac-
terises in the long term the demographic evolution ofmost European countries As a result of the decreasingnatality the share of persons older than 64 years increasesThe age preference index defined as the number of
persons aged 65 years or more per 100 children exceedsthe value 100 in increasing numbers of countries Itmeans that there are more seniors than children This isalready so in 35 of EU member countries most mark-edly in Germany and in Italy On the opposite pole arethe ldquoyoungestrdquo countries Albania Ireland and Icelandwhere the share of seniors is only about one half of itsvalue in Germany and ItalyThe Czech Republic belongs to countries with a low
share of children up to 15 years old (142 in 2009)With its share of persons in the age group of 65 ormore years (150 in 2009) the CR still does not reachthe European Union average that exceeded 17 in 2007In 2006 the Czech Republic joined the group of coun-tries with more persons over 64 than children The agepreference index in 2009 reached the value 107Another common feature of most European countries
is the decreasing mortality connected with growinglength of human life The average value of standardiseddeath rate (that eliminates the influence of the age
structure of the population further SDR) shows a long-term decreasing trend in European Union (EU) as well asin EU-15 (member countries before May 2004) and inEU-12 (new member countries that joined EU in 2004and 2007) The average values of the total SDR in EU-12exceed the averages in EU-15 by 23 in men and byalmost 12 in women The SDR values in the CzechRepublic in spite of the marked decrease in the past twodecreases still exceed not only the averages of EU-15 (byalmost 40 in men and by ca 30 in women) but alsoof the whole EU by 15 both in men and women
Current status of the PPPM in the Czech RepublicThere is no conception of PPPM (predictive preventiveand personalised medicine) in the Czech Republic offi-cially proposed by policy makers as eg Ministry ofHealth of the Czech Republic (MoH) and NationalInstitute of Public Health (SZUacute) Ministry of Labour andSocial Affairs (MoLSA) and other governmental bodiesThe main document regarding the national health policyis ldquoMinistry of Health Departmental Program forResearch and Development III (DPR III)rdquo [10] withsome aspects regarding basic principles of PPPM As anexample of this approach the SZUacute is responsible for pre-ventive services covering
1 compulsory vaccination and preventive examina-tions for children of specific age groups2 compulsory vaccination and periodic examinationsby general practitioner very two years3 well organised cancer screening programmes (egcolo-rectal cancer breast cancer cervical cancer)4 mammography for women 45-69 every two yearspreventive gynaecological examinations includingcytology from the age of 155 regular vaccination covering 99 of the popula-tion (tuberculosis tetanus diphtheria pertussispoliomyelitis measles mumps and rubella cervicalcancer from 2001 also hepatitis B and Haemophilusinfluenzae type B [5]
Several additional preventive care services are deliv-ered to the Czech citizens reducing alcohol harm treat-ing drug addiction tackling obesity especially inchildren prevention of smoking sexual health educa-tion life style health risksThe current situation in the Czech Republic is charac-
terised by raising awareness and recognition of PPPMpromotion of education and up to date informationEducation of PPPM is one of the initial activities The
only educational centres are universities and researchinstitutes The concept of PPPM national education isstill under preparation at both non-professional (gen-eral) and professionals in personalised medicine
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 6 of 8
Following steps will include graduate post graduateand continuing education programmes for young andexperienced researchers and medical staff those who willbe taking the PPPM forward in the coming years
RecommendationsBasic principles of PPPM should be incorporated intobasic strategic documents of policy makers (MoH SZUacuteMoLSA) with ethical legal and social issues involved
Educational programmes for students and profes-sionals at all levels in conventional and molecular diag-nostics biomedicine biotechnologies ethics andeconomics for universities research units private andpublic hospitals and publicndashpatients and their familymembers with all necessary materials should be system-atically preparedAll relevant partners like policy makers stakeholders
pharmacy biomedical industry universities research
Figure 4 Proportion of total expenditure on health services in gross domestic product (GDP) Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 7 of 8
centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8

3 the inclusion in 2008 of the State Institute forDrug Control (Staacutetniacute uacutestav pro kontrolu lečivSUacuteKL) in the process of setting maximum prices forpharmaceuticals for transparency of price settings4 the introduction in 2008 of a programme to sup-ply accredited providers with additional financialsupport for training nurses and physicians5 an initiative to improve the quality of highly spe-cialised care by identifying high performing health-care facilities and allowing for special contractualconditions between these facilities and the healthinsurance funds
Organisation of health system in the CzechRepublicCzech health system is based on five pillars1 solidarity
- solidarity between healthy people and the sick isfostered in healthcare systems by separation betweenthe provision of healthcare and its financing- solidarity of the economically active with the eco-nomically inactive people means that every insuredperson pays an insurance premium as a percentageof their income regardless of what healthcare theyreceive or will receive
2 high degree of self-administration3 multisource financing with major share of public
health insurance Healthcare is funded from publichealth insurance direct payments the national budgetand regional budgets4 equal availability of healthcare for all insured per-
sons The healthcare system strives to create conditionsin which there are no differences in the availability ofhealthcare5 obligatory vaccination against infectious diseasesThese pillars are legally supported by following
selected laws
- Resolution of the Presidium of the Czech NationalCouncil 21993 promulgating the Charter of Funda-mental Rights and Freedoms as part of the Czechconstitutional order- Act 481997 Coll on public health insuranceamending some related laws- Act 201966 Coll on public healthcare amendingsome related laws- Act 5921992 Coll on premiums for generalhealth insurance amending some related laws- Act no 2582000 Coll on public health protectionand amendments to several related acts as amended[8]
Healthcare is in the Czech Republic is provided bystructured network of several types of healthcare someof them are listed below [68]
Outpatient careOutpatient care is provided by primary care physiciansor specialists If a person is taken ill they usually con-tact a primary care physician working near their homeThese are general practitioners for adults general practi-tioners for children and young people dentists andgynaecologistsWhen choosing a physician you should bear in mind
that you can only register with a physician who has con-cluded a contract with your insurance companyIf healthcare is to be reimbursed from public health
insurance the insured must first register with a primarycare physician (the local basic healthcare provider) Aphysician may only refuse to register an insured personif the registration brought to the physician so muchwork that it would not permit provision of quality careto the patient or other patients in the physicianrsquos careA patient can visit a specialist physician in the Czech
Republic without a referral from the primary carephysician
Institutional (inpatient) careIf the nature of an illness demands this a primary carephysician or outpatient specialist can refer a patient forhospital treatment or arrange for their admittanceInpatient care is provided in hospitals and specialised
institutions such as psychiatric hospitals and rehabilita-tion centres hospices sanatoria long-term carehospitals
Ambulance and emergency rescue serviceEmergency rescue service is available to deal with casesof acute illness or accident when a patient cannot get toa physician and immediate treatment is needed andtransport of the patient to a healthcare facility underpermanent care to prevent further aggravation of theirhealth conditions or threat to the life
Balneological careBalneological care can be regarded as an essential partof the curative process It is recommended by onersquosattending physician and confirmed by a reviewing physi-cian Entitlement to balneological care is claimed on apre-printed form by the registering general physician orattending physician in case of hospitalisation
Long-term careLong-term care for older or disabled people is providedin two overlapping settings with different systems of
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 4 of 8
organisation and funding residential long-term carefacilities and other social services financed from centralregional or municipal budgets and healthcare facilitiesfor long-term inpatient care financed primarily throughthe social health insurance
Mental healthcareMental healthcare is provided both in the ambulatorysettings and in inpatient facilities which include hospitalpsychiatric departments psychiatric hospitals and psy-chiatric institutes
Dispensing medicaments and medical devicesIn the Czech Republic there is an extensive network ofpharmacies dispensing medicaments and medicaldevices both on prescription and over the counter
Preventive carePreventive examinations and vaccination against infec-tious diseases are performed by primary care physicians
FinancingIn 2010 as in the preceding years the predominant partof health expenditure was financed by the public healthinsurance system covering 766 of the total (in Figure3 is shown expenditure on health services by sources of
financing) The State and territorial budgets covered72 and private expenditure covered 162 The shareof private expenditure in the total expenditure on healthrose particularly after 2008 due to new regulation feesin health services In 2010 the private expenditure onhealth slightly decreased partly as a result of softeningof the regulation fees and of stagnant purchasing powerof the population The total expenditure on healthincreased from 2009 by 821 million CZK and in 2010 itamounted in absolute value to 290 412 million CZK ie27 613 CZK per 1 inhabitant This total expenditurerepresents 769 of the GDP in 2010 Public expendi-ture ie that of the public budgets and of the publichealth insurance system totally 243 283 million CZKby 1 646 million CZK more than in the preceding year(all data are preliminary) [9]Healthcare in the Czech Republic is provided primar-
ily on the basis of statutory health insurance which iscurrently provided by nine health insurance fundsThe largest health insurance fund - the General
Health Insurance Fund GHIF - has 77 district branchesAny person with a permanent residence in the CzechRepublic is entitled to health insuranceHealthcare services are covered by the health insur-
ance funds The following services are fully or partiallycovered by health insurance [8]
Figure 3 Expenditure on health services by sources of financing Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 5 of 8
1 outpatient and institutional (inpatient) care2 emergency and ambulance services3 preventive care4 dispensary care5 supply of medicaments medical supplies (eg hear-
ing aids bandages)6 balneological care care in specialised childrenrsquos hos-
pitals and sanatoria7 industrial healthcare8 transport of the sick reimbursement of travel
expenses9 deceased examination and autopsyThere are many procedures which insured persons co-
finance These are procedures or medical devices pro-vided outside the legal framework Some cases in pointare dental procedures some balneological care andsome medicaments Some medicaments are reimbursedin full by insurance companies whereas some are co-financed by the patients In every category of medica-ments there must be at least one reimbursed in full byan insurer Costs of medicaments and medical devicesduring hospitalisation are reimbursed in full by theinsurer and the insured person does not pay directly
International comparisonThis part contains comparison of the shares of expendi-ture on health in gross domestic product (GDP) inselected countries in Europe (Figure 4) The source ofthese data is the Database OECD Health Data 2011Ageing of the population is a phenomenon that charac-
terises in the long term the demographic evolution ofmost European countries As a result of the decreasingnatality the share of persons older than 64 years increasesThe age preference index defined as the number of
persons aged 65 years or more per 100 children exceedsthe value 100 in increasing numbers of countries Itmeans that there are more seniors than children This isalready so in 35 of EU member countries most mark-edly in Germany and in Italy On the opposite pole arethe ldquoyoungestrdquo countries Albania Ireland and Icelandwhere the share of seniors is only about one half of itsvalue in Germany and ItalyThe Czech Republic belongs to countries with a low
share of children up to 15 years old (142 in 2009)With its share of persons in the age group of 65 ormore years (150 in 2009) the CR still does not reachthe European Union average that exceeded 17 in 2007In 2006 the Czech Republic joined the group of coun-tries with more persons over 64 than children The agepreference index in 2009 reached the value 107Another common feature of most European countries
is the decreasing mortality connected with growinglength of human life The average value of standardiseddeath rate (that eliminates the influence of the age
structure of the population further SDR) shows a long-term decreasing trend in European Union (EU) as well asin EU-15 (member countries before May 2004) and inEU-12 (new member countries that joined EU in 2004and 2007) The average values of the total SDR in EU-12exceed the averages in EU-15 by 23 in men and byalmost 12 in women The SDR values in the CzechRepublic in spite of the marked decrease in the past twodecreases still exceed not only the averages of EU-15 (byalmost 40 in men and by ca 30 in women) but alsoof the whole EU by 15 both in men and women
Current status of the PPPM in the Czech RepublicThere is no conception of PPPM (predictive preventiveand personalised medicine) in the Czech Republic offi-cially proposed by policy makers as eg Ministry ofHealth of the Czech Republic (MoH) and NationalInstitute of Public Health (SZUacute) Ministry of Labour andSocial Affairs (MoLSA) and other governmental bodiesThe main document regarding the national health policyis ldquoMinistry of Health Departmental Program forResearch and Development III (DPR III)rdquo [10] withsome aspects regarding basic principles of PPPM As anexample of this approach the SZUacute is responsible for pre-ventive services covering
1 compulsory vaccination and preventive examina-tions for children of specific age groups2 compulsory vaccination and periodic examinationsby general practitioner very two years3 well organised cancer screening programmes (egcolo-rectal cancer breast cancer cervical cancer)4 mammography for women 45-69 every two yearspreventive gynaecological examinations includingcytology from the age of 155 regular vaccination covering 99 of the popula-tion (tuberculosis tetanus diphtheria pertussispoliomyelitis measles mumps and rubella cervicalcancer from 2001 also hepatitis B and Haemophilusinfluenzae type B [5]
Several additional preventive care services are deliv-ered to the Czech citizens reducing alcohol harm treat-ing drug addiction tackling obesity especially inchildren prevention of smoking sexual health educa-tion life style health risksThe current situation in the Czech Republic is charac-
terised by raising awareness and recognition of PPPMpromotion of education and up to date informationEducation of PPPM is one of the initial activities The
only educational centres are universities and researchinstitutes The concept of PPPM national education isstill under preparation at both non-professional (gen-eral) and professionals in personalised medicine
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 6 of 8
Following steps will include graduate post graduateand continuing education programmes for young andexperienced researchers and medical staff those who willbe taking the PPPM forward in the coming years
RecommendationsBasic principles of PPPM should be incorporated intobasic strategic documents of policy makers (MoH SZUacuteMoLSA) with ethical legal and social issues involved
Educational programmes for students and profes-sionals at all levels in conventional and molecular diag-nostics biomedicine biotechnologies ethics andeconomics for universities research units private andpublic hospitals and publicndashpatients and their familymembers with all necessary materials should be system-atically preparedAll relevant partners like policy makers stakeholders
pharmacy biomedical industry universities research
Figure 4 Proportion of total expenditure on health services in gross domestic product (GDP) Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 7 of 8
centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8

organisation and funding residential long-term carefacilities and other social services financed from centralregional or municipal budgets and healthcare facilitiesfor long-term inpatient care financed primarily throughthe social health insurance
Mental healthcareMental healthcare is provided both in the ambulatorysettings and in inpatient facilities which include hospitalpsychiatric departments psychiatric hospitals and psy-chiatric institutes
Dispensing medicaments and medical devicesIn the Czech Republic there is an extensive network ofpharmacies dispensing medicaments and medicaldevices both on prescription and over the counter
Preventive carePreventive examinations and vaccination against infec-tious diseases are performed by primary care physicians
FinancingIn 2010 as in the preceding years the predominant partof health expenditure was financed by the public healthinsurance system covering 766 of the total (in Figure3 is shown expenditure on health services by sources of
financing) The State and territorial budgets covered72 and private expenditure covered 162 The shareof private expenditure in the total expenditure on healthrose particularly after 2008 due to new regulation feesin health services In 2010 the private expenditure onhealth slightly decreased partly as a result of softeningof the regulation fees and of stagnant purchasing powerof the population The total expenditure on healthincreased from 2009 by 821 million CZK and in 2010 itamounted in absolute value to 290 412 million CZK ie27 613 CZK per 1 inhabitant This total expenditurerepresents 769 of the GDP in 2010 Public expendi-ture ie that of the public budgets and of the publichealth insurance system totally 243 283 million CZKby 1 646 million CZK more than in the preceding year(all data are preliminary) [9]Healthcare in the Czech Republic is provided primar-
ily on the basis of statutory health insurance which iscurrently provided by nine health insurance fundsThe largest health insurance fund - the General
Health Insurance Fund GHIF - has 77 district branchesAny person with a permanent residence in the CzechRepublic is entitled to health insuranceHealthcare services are covered by the health insur-
ance funds The following services are fully or partiallycovered by health insurance [8]
Figure 3 Expenditure on health services by sources of financing Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 5 of 8
1 outpatient and institutional (inpatient) care2 emergency and ambulance services3 preventive care4 dispensary care5 supply of medicaments medical supplies (eg hear-
ing aids bandages)6 balneological care care in specialised childrenrsquos hos-
pitals and sanatoria7 industrial healthcare8 transport of the sick reimbursement of travel
expenses9 deceased examination and autopsyThere are many procedures which insured persons co-
finance These are procedures or medical devices pro-vided outside the legal framework Some cases in pointare dental procedures some balneological care andsome medicaments Some medicaments are reimbursedin full by insurance companies whereas some are co-financed by the patients In every category of medica-ments there must be at least one reimbursed in full byan insurer Costs of medicaments and medical devicesduring hospitalisation are reimbursed in full by theinsurer and the insured person does not pay directly
International comparisonThis part contains comparison of the shares of expendi-ture on health in gross domestic product (GDP) inselected countries in Europe (Figure 4) The source ofthese data is the Database OECD Health Data 2011Ageing of the population is a phenomenon that charac-
terises in the long term the demographic evolution ofmost European countries As a result of the decreasingnatality the share of persons older than 64 years increasesThe age preference index defined as the number of
persons aged 65 years or more per 100 children exceedsthe value 100 in increasing numbers of countries Itmeans that there are more seniors than children This isalready so in 35 of EU member countries most mark-edly in Germany and in Italy On the opposite pole arethe ldquoyoungestrdquo countries Albania Ireland and Icelandwhere the share of seniors is only about one half of itsvalue in Germany and ItalyThe Czech Republic belongs to countries with a low
share of children up to 15 years old (142 in 2009)With its share of persons in the age group of 65 ormore years (150 in 2009) the CR still does not reachthe European Union average that exceeded 17 in 2007In 2006 the Czech Republic joined the group of coun-tries with more persons over 64 than children The agepreference index in 2009 reached the value 107Another common feature of most European countries
is the decreasing mortality connected with growinglength of human life The average value of standardiseddeath rate (that eliminates the influence of the age
structure of the population further SDR) shows a long-term decreasing trend in European Union (EU) as well asin EU-15 (member countries before May 2004) and inEU-12 (new member countries that joined EU in 2004and 2007) The average values of the total SDR in EU-12exceed the averages in EU-15 by 23 in men and byalmost 12 in women The SDR values in the CzechRepublic in spite of the marked decrease in the past twodecreases still exceed not only the averages of EU-15 (byalmost 40 in men and by ca 30 in women) but alsoof the whole EU by 15 both in men and women
Current status of the PPPM in the Czech RepublicThere is no conception of PPPM (predictive preventiveand personalised medicine) in the Czech Republic offi-cially proposed by policy makers as eg Ministry ofHealth of the Czech Republic (MoH) and NationalInstitute of Public Health (SZUacute) Ministry of Labour andSocial Affairs (MoLSA) and other governmental bodiesThe main document regarding the national health policyis ldquoMinistry of Health Departmental Program forResearch and Development III (DPR III)rdquo [10] withsome aspects regarding basic principles of PPPM As anexample of this approach the SZUacute is responsible for pre-ventive services covering
1 compulsory vaccination and preventive examina-tions for children of specific age groups2 compulsory vaccination and periodic examinationsby general practitioner very two years3 well organised cancer screening programmes (egcolo-rectal cancer breast cancer cervical cancer)4 mammography for women 45-69 every two yearspreventive gynaecological examinations includingcytology from the age of 155 regular vaccination covering 99 of the popula-tion (tuberculosis tetanus diphtheria pertussispoliomyelitis measles mumps and rubella cervicalcancer from 2001 also hepatitis B and Haemophilusinfluenzae type B [5]
Several additional preventive care services are deliv-ered to the Czech citizens reducing alcohol harm treat-ing drug addiction tackling obesity especially inchildren prevention of smoking sexual health educa-tion life style health risksThe current situation in the Czech Republic is charac-
terised by raising awareness and recognition of PPPMpromotion of education and up to date informationEducation of PPPM is one of the initial activities The
only educational centres are universities and researchinstitutes The concept of PPPM national education isstill under preparation at both non-professional (gen-eral) and professionals in personalised medicine
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 6 of 8
Following steps will include graduate post graduateand continuing education programmes for young andexperienced researchers and medical staff those who willbe taking the PPPM forward in the coming years
RecommendationsBasic principles of PPPM should be incorporated intobasic strategic documents of policy makers (MoH SZUacuteMoLSA) with ethical legal and social issues involved
Educational programmes for students and profes-sionals at all levels in conventional and molecular diag-nostics biomedicine biotechnologies ethics andeconomics for universities research units private andpublic hospitals and publicndashpatients and their familymembers with all necessary materials should be system-atically preparedAll relevant partners like policy makers stakeholders
pharmacy biomedical industry universities research
Figure 4 Proportion of total expenditure on health services in gross domestic product (GDP) Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 7 of 8
centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8

1 outpatient and institutional (inpatient) care2 emergency and ambulance services3 preventive care4 dispensary care5 supply of medicaments medical supplies (eg hear-
ing aids bandages)6 balneological care care in specialised childrenrsquos hos-
pitals and sanatoria7 industrial healthcare8 transport of the sick reimbursement of travel
expenses9 deceased examination and autopsyThere are many procedures which insured persons co-
finance These are procedures or medical devices pro-vided outside the legal framework Some cases in pointare dental procedures some balneological care andsome medicaments Some medicaments are reimbursedin full by insurance companies whereas some are co-financed by the patients In every category of medica-ments there must be at least one reimbursed in full byan insurer Costs of medicaments and medical devicesduring hospitalisation are reimbursed in full by theinsurer and the insured person does not pay directly
International comparisonThis part contains comparison of the shares of expendi-ture on health in gross domestic product (GDP) inselected countries in Europe (Figure 4) The source ofthese data is the Database OECD Health Data 2011Ageing of the population is a phenomenon that charac-
terises in the long term the demographic evolution ofmost European countries As a result of the decreasingnatality the share of persons older than 64 years increasesThe age preference index defined as the number of
persons aged 65 years or more per 100 children exceedsthe value 100 in increasing numbers of countries Itmeans that there are more seniors than children This isalready so in 35 of EU member countries most mark-edly in Germany and in Italy On the opposite pole arethe ldquoyoungestrdquo countries Albania Ireland and Icelandwhere the share of seniors is only about one half of itsvalue in Germany and ItalyThe Czech Republic belongs to countries with a low
share of children up to 15 years old (142 in 2009)With its share of persons in the age group of 65 ormore years (150 in 2009) the CR still does not reachthe European Union average that exceeded 17 in 2007In 2006 the Czech Republic joined the group of coun-tries with more persons over 64 than children The agepreference index in 2009 reached the value 107Another common feature of most European countries
is the decreasing mortality connected with growinglength of human life The average value of standardiseddeath rate (that eliminates the influence of the age
structure of the population further SDR) shows a long-term decreasing trend in European Union (EU) as well asin EU-15 (member countries before May 2004) and inEU-12 (new member countries that joined EU in 2004and 2007) The average values of the total SDR in EU-12exceed the averages in EU-15 by 23 in men and byalmost 12 in women The SDR values in the CzechRepublic in spite of the marked decrease in the past twodecreases still exceed not only the averages of EU-15 (byalmost 40 in men and by ca 30 in women) but alsoof the whole EU by 15 both in men and women
Current status of the PPPM in the Czech RepublicThere is no conception of PPPM (predictive preventiveand personalised medicine) in the Czech Republic offi-cially proposed by policy makers as eg Ministry ofHealth of the Czech Republic (MoH) and NationalInstitute of Public Health (SZUacute) Ministry of Labour andSocial Affairs (MoLSA) and other governmental bodiesThe main document regarding the national health policyis ldquoMinistry of Health Departmental Program forResearch and Development III (DPR III)rdquo [10] withsome aspects regarding basic principles of PPPM As anexample of this approach the SZUacute is responsible for pre-ventive services covering
1 compulsory vaccination and preventive examina-tions for children of specific age groups2 compulsory vaccination and periodic examinationsby general practitioner very two years3 well organised cancer screening programmes (egcolo-rectal cancer breast cancer cervical cancer)4 mammography for women 45-69 every two yearspreventive gynaecological examinations includingcytology from the age of 155 regular vaccination covering 99 of the popula-tion (tuberculosis tetanus diphtheria pertussispoliomyelitis measles mumps and rubella cervicalcancer from 2001 also hepatitis B and Haemophilusinfluenzae type B [5]
Several additional preventive care services are deliv-ered to the Czech citizens reducing alcohol harm treat-ing drug addiction tackling obesity especially inchildren prevention of smoking sexual health educa-tion life style health risksThe current situation in the Czech Republic is charac-
terised by raising awareness and recognition of PPPMpromotion of education and up to date informationEducation of PPPM is one of the initial activities The
only educational centres are universities and researchinstitutes The concept of PPPM national education isstill under preparation at both non-professional (gen-eral) and professionals in personalised medicine
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 6 of 8
Following steps will include graduate post graduateand continuing education programmes for young andexperienced researchers and medical staff those who willbe taking the PPPM forward in the coming years
RecommendationsBasic principles of PPPM should be incorporated intobasic strategic documents of policy makers (MoH SZUacuteMoLSA) with ethical legal and social issues involved
Educational programmes for students and profes-sionals at all levels in conventional and molecular diag-nostics biomedicine biotechnologies ethics andeconomics for universities research units private andpublic hospitals and publicndashpatients and their familymembers with all necessary materials should be system-atically preparedAll relevant partners like policy makers stakeholders
pharmacy biomedical industry universities research
Figure 4 Proportion of total expenditure on health services in gross domestic product (GDP) Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 7 of 8
centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8

Following steps will include graduate post graduateand continuing education programmes for young andexperienced researchers and medical staff those who willbe taking the PPPM forward in the coming years
RecommendationsBasic principles of PPPM should be incorporated intobasic strategic documents of policy makers (MoH SZUacuteMoLSA) with ethical legal and social issues involved
Educational programmes for students and profes-sionals at all levels in conventional and molecular diag-nostics biomedicine biotechnologies ethics andeconomics for universities research units private andpublic hospitals and publicndashpatients and their familymembers with all necessary materials should be system-atically preparedAll relevant partners like policy makers stakeholders
pharmacy biomedical industry universities research
Figure 4 Proportion of total expenditure on health services in gross domestic product (GDP) Taken from Czech health statistics 2009 [1]
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 7 of 8
centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8

centres hospitals patient and patientsrsquo organisationsshould be involved in process of establishing PPPM inthe Czech RepublicCzech professionals should be more involved in inter-
national PPPM programmes and research and otheractivities eg Framework Programme 7 (FP7) and bemore active in preparation of the following programmeHORIZON 2020Czech professionals should more participate at all
international activities like congresses conferencesworkshops Joint programming be more active inpublishing
ConclusionsSince 1989 the Czech healthcare system has undergomajor and important changes with the aim to start andaccelerate process of democratisation and humanisationof the healthcare system and make it more efficient Thenext important step was to separate financing of health-care from the state budgetThe key challenge to health reform in the upcoming
period is to improve high quality of healthcare to allinhabitants of the Czech RepublicThe process of transformation is on-going process
well-coordinated with the basic principles of EU strategyin healthcare in the member states
AcknowledgementsThe article has been prepared with the support of the EU project CZ1072300200040 - Molecular genetics of tumor and cardiovascular diseasesOpen AccessThis article is distributed under the terms of the Creative CommonsAttribution License which permits any use distribution and reproduction inany medium provided the original author(s) and the source are credited
Author details1Technology Centre of the Academy of Sciences of the Czech Republic(Technology Centre ASCR) Ve Struhaacutech 27 Praha 6 160 00 Czech Republic2Charles University Prague E Beneše 13 Plzeš 305 99 Czech Republic
Received 20 December 2011 Accepted 23 January 2012Published 28 February 2012
References1 Czech Republic in Figures 2010 Czech Statistical Office [http www
czsoczcsu2010edicniplannsfengp1410-10]2 Political System of the Czech Republic About the Czech Republic Embassy
of the Czech Republic in Sofia [httpwww mzvczsofiaenabout_the_czech_republicpolitical_system_of_ the_czech_republicindexhtml]
3 Healthcare statistics 2011 Eurostat European Commission [httpeppeurostateceuropaeustatistics_explainedindexphpHealthcare_statistics]
4 Health and health systems European Health Report 2009 WHO RegionalOffice for Europe 2009 [httpwwweurowho int__dataassetspdf_file000982386E93103pdf]
5 Bryndovaacute L Pavlokovaacute K Roubal T Rokosovaacute M Gaskins M van Ginneken ECzech Republic Health system review Health Systems in Transition 2009[httpwwweurowhoint__dataassetspdf_file001097633E92968pdf]
6 Mihaacutelyi P Post-socialist health systems in transition Czech RepublicHungary and Poland (2000) Central European University Working Paper No42000 Available at SSRN httpssrncomabstract0253857
7 Rokosovaacute M Haacuteva P Schreyoumlgg J Busse R Health care systems intransition Czech Republic Copenhagen WHO Regional Office for Europe onbehalf of the European Observatory on Health Systems and Policies 2005[httpwwweurowhoint__dataassetspdf_file000375144E86823pdf]
8 General Principles of the Health System in the Czech Republic Ministryof Health of the Czech Republic (MoH) [httpwww mzcrczprevenceczechczechhtml]
9 Czech Health Statistics Yearbook 2010 Institute of Health Informationand Statistics of the Czech Republic Czech Health Statistics Yearbook2010
10 Ministry of Health Departmental Program for Research andDevelopment III (DPR III) Ministry of Health of the Czech Republic [httpigamzcrczpublicWeb]
doi101007s13167-012-0139-9Cite this article as Kinkorovaacute and Topolčan Overview of healthcaresystem in the Czech Republic The EPMA Journal 2012 34
Submit your next manuscript to BioMed Centraland take full advantage of
bull Convenient online submission
bull Thorough peer review
bull No space constraints or color figure charges
bull Immediate publication on acceptance
bull Inclusion in PubMed CAS Scopus and Google Scholar
bull Research which is freely available for redistribution
Submit your manuscript at wwwbiomedcentralcomsubmit
Kinkorovaacute and Topolčan The EPMA Journal 2012 34httpwwwepmajournalcomcontent314
Page 8 of 8