Embed Size (px)
Citation preview
4REVIEW
135 Global clinical experience with Boron neutron capture therapy Galeş N. Laurenţia, Anghel M. Rodica
ORIGINAL PAPERS141 A study regarding the interrelation
between a good state of mind as an indicator of health state and psychotherapy in children with Attention Deficit Hyperactivity DisorderMitu Ana Mihaela, Daviţoiu Ana Maria, Truţă Elena, Stănciulescu Luminiţa, Ionică M.
THERAPEUTICAL PRACTICE
146
Treatment in oropharyngeal cancer- an updatePalade O.D., Lazăr Andra Sorina, Oprea Alina, Toader Miorița, Toader C.
CASE REPORT
149 Acute myeloid leukaemia in a 19 year old patient previously treated for osteosarcoma - case report and review of the literatureDrăgan C., Meilin Murat, Trifa A., Tevet Mihaela, Lupu Anca Roxana
152 Intoxication with DiazinonDumitraşcu Monica, Macovei R.A., Caragea Genica, Avram Ruxandra, Ionică M.
156 Correlation of histological findings with bacterial culture in children with Helicobacter pylori gastritisNăstase Gabriela, Anghel Mălina, Galoș Felicia, Stoicescu M., Munteanu M., Bălgrădean Mihaela
159 An atypical cause of nauseaIlie Mădălina, Turculeţ C., Diaconu Camelia, Tincu R., Constantinescu G., Stănciulescu Luminiţa, Macovei R., Enache V., Popa B., Ene D.
163 Compressing Dermoid Cyst of the NeckPalade O.D., Rebega Cătălina, Cobzeanu M.D., Oprea Alina, Toader Mioriţa, Toader C.
165 A rare case of isolated oesophageal Crohn’s diseaseIlie Mădălina, Constantinescu G., Diaconu Camelia, Stănciulescu Elena-Luminița, Enache V., Macovei R., Popa B.

Vol. XIX Number IV December 2015
National Institute of Infectious Diseases "Prof. Dr. Matei Balş"
Romanian Society of Pharmacology, Therapeuticsand Clinical Toxicology
Romanian Academy ofMedical Sciences
University of Medicine and Pharmacy "Carol Davila"
Journal published in cooperation with:
CNCSIS Category: B+ Code: 605
NLM (National Medical Library)SCOPUSEBSCOhostIndexCopernicusgetCITED
Academic Medical Database:

Founders
Emanoil Manolescu Mircea Angelescu Liviu Ioan Miclea
Editor-in-Chief TherapeuticsAdrian Streinu-Cercel (Professor, Member of Academy of Medical Science, Head of Department of Infectious Diseases, National
Institute of Infectious Diseases "Prof. Dr. Matei Balş", University of Medicine and Pharmacy Carol Davila Bucharest)
Editor-in-Chief Clinical Pharmacology and ToxicologyVictor A. Voicu (Professor, Member of Romanian Academy, Head of Department of Pharmacology, Toxicology and Clinical Psychopharmacology,
University of Medicine and Pharmacy Carol Davila Bucharest)
Associate EditorMonica Luminos (Associate Professor, National Institute of Infectious Diseases "Prof. Dr. Matei Balş", University of Medicine and Pharmacy
Carol Davila Bucharest)Doina Pleșca (Professor, Children's Clinical Hospital, Dean of University of Medicine and Pharmacy Carol Davila Bucharest)
International Scientific BoardLaure Aurelian (Professor, Senior Associate, The Johns Hopkins School of Public Health) • Hege Christensen (Professor, School of Pharmacy,
Uni-versity of Oslo, Norway) • Jaime Kapitulnik (Professor, The Hebrew University of Jerusalem, Israel) • Momir Mikov (Senior Lecturer, School of Pharmacy, University of Otago, New Zealand) • Stanislav Yanev (Professor, Head of Department Drug and Toxicology, Bulgarian Academy of Science, Bulgaria) • Olavi Pelkonen (Professor, Head of the Department of Pharmacology and Toxicology, University of Oulu, Finland) • Olivier Patey (Professor, Chef de service des maladies infectieuses et tropicales CHI, Villeneuve-Saint Georges, France) • George C. Rodgers (Professor of Pediatrics, Pharmacology and Toxicology, University of Louisville, Kentucky, USA) • Robert Smith (Professor, Brown Medical School, U.K.) • Jean Paul Stahl (Professor, Rédacteur en chef de Médecine et Maladies Infectieuses, Elsevier Maison, Grenoble, France) • Michel Urbain (Chief of Research Department, Societe de Etude et de Research Biologique, Paris, France) • Andrei Iagăru (Associate Professor, Department of Nuclear Medicine, Stanford University, USA) • Serafim Kastanakis (Professor, University of Crete, Greece)
Romanian Scientific BoardEduard Apetrei (Professor, University of Medicine and Pharmacy Carol Davila Bucharest, Member of Romanian Academy of Medical Science) •
Ştefan Sorin Aramă (Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Constantin Arion (Professor, University of Medicine and Pharmacy Carol Davila Bucharest, Member of Romanian Academy of Medical Science) • Anca Buzoianu (Professor, University of Medicine and Pharmacy Iuliu Haţieganu Cluj-Napoca) • Carmen Dorobăţ (Professor, University of Medicine and Pharmacy Gr.T. Popa, Iassy) • Constantin Dumitrache (Professor, Member of Romanian Academy, University of Medicine and Pharmacy Carol Davila Bucharest) • Leonida Gherasim (Professor, University of Medicine and Pharmacy Carol Davila Bucharest, Member of Romanian Academy of Medical Science) • Daniela Ion (Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Ion Fulga (Professor, Head of Department of Pharmacotherapy and Pharmacology, University of Medicine and Pharmacy Carol Davila Bucharest) • Sorin Leucuţa (Professor, University of Medicine and Pharmacy Oradea) • Radu Macovei (Professor, Head of Department of ICU-Toxicology, University of Medicine and Pharmacy Carol Davila Bucharest) • Mihai Gafencu (Assistant Professor, University of Medicine and Pharmacy Victor Babeş Timişoara) • Nicolae Miu (Professor, University of Medicine and Pharmacy Iuliu Haţieganu Cluj-Napoca) • Ostin C. Mungiu (Professor, Head of Department of Pharmacology and Clinical Toxicology, University of Medicine and Pharmacy Gr.T. Popa, Iassy) • Lucian Negruţiu (Professor, University of Medicine and Pharmacy Victor Babeş Timişoara) • Florian Popa (Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Irinel Popescu (Professor, Head of Department of Surgery and Liver Transplant, University of Medicine and Pharmacy Carol Davila Bucharest, Member of Academy of Medical Science) • Laurenţiu Mircea Popescu (Professor, Member of Romanian Academy, Head of Department of Celular Biology, University of Medicine and Pharmacy Carol Davila Bucharest) • Florica Stăniceanu (Professor, Univeristy of Medicine and Pharmacy Carol Davila Bucharest) • Dan Tulbure (Professor, Head of Department of ICU, University of Medicine and Pharmacy Carol Davila Bucharest) • Doina Ţăţulescu (Professor, University of Medicine and Pharmacy Iuliu Haţieganu Cluj-Napoca) • Coriolan Ulmeanu (Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Doina Velican (Researcher, Member of Romanian Academy of Medical Science) • Florin Căruntu (Associate Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Adrian Gabriel Popescu (Associate Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Anca Drăgănescu (Pediatrician, INBI Prof. Dr. Matei Bals, Bucharest) • Paraschiva Postolache (Associate Professor, University of Medicine and Pharmacy Gr.T. Popa, Iassy) • Alexandru Rafila (Associate Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Adriana Hristea (Associate Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Gabriela Leşanu (Lecture, University of Medicine and Pharmacy Carol Davila Bucharest) • Ion Lică (Lecture, University of Medicine and Pharmacy Carol Davila Bucharest) • Raluca Papacocea (Lecture, University of Medicine and Pharmacy Carol Davila Bucharest) • Adrian Lungu (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Maria Dorina Pașca (Associate Professor, University of Medicine and Pharmacy Targu Mures) • Voichiţa Lăzureanu (Assistant Professor, University of Medicine and Pharmacy Victor Babeş Timişoara) • Anca Macovei (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Anca Streinu-Cercel (Associate, University of Medicine and Pharmacy Carol Davila Bucharest) • Andrei Tica (Professor, University of Medicine and Pharmacy Craiova) • Laura Bălănescu (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Mihail Tudosie (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Ionel Alexandru Checheriță (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Mihai Săndulescu (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Toma Papacocea (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest) • Alexandru Ulmeanu (Assistant Professor, University of Medicine and Pharmacy Carol Davila Bucharest)
Issue EditorElisabeta Otilia Benea (Associate Professor, University of Medicine and Pharmacy Carol Davila Bucharest) Oana Săndulescu Ana-Maria Tudor
English Proofreading EditorAlexandra Mărdărescu
Publishing EditorMihaela Cristina Negulescu
Editorial Office Institutul Naţional de Boli Infecţioase Prof. Dr. Matei Balş, Pavilionul IV, Etaj 41 Dr. Calistrat Grozovici Str., Sector 2, Bucureşti, C.P. 021105, O.P. 10
E-mail: [email protected], [email protected] [email protected]
Published by SC Editura Rp. SRLCUI RO9954898, RC J40/7184/1997Address: 6 Codrii Neamțului Str., Bl. PM 26bis, Sc. A, Et. 8, Ap. 36, sector 3, Bucharest, Romania Tel/Fax: 031.80.40.513; 0724.356.578 E-mail: [email protected]: www.terapeutica.ro
ISSN 2066-0170

XIX, Vol.19, Number 4/2015 135
Laurenția Galeș258 Șos. Fundeni, 2 District, Bucharest, Romaniae-mail: [email protected]
Abstract. Boron neutron capture therapy (BNCT) represents a top therapeutic method that relies on knowledge in the area of nuclear technology as well as on medicine experience in treating malignant tumour. Various pre-clinical experiments have been initially applied in order to demonstrate the effectiveness of BNCT concept. Once they demonstrated the concept, pre-clinical experiments continued by focusing on a better establishment of the irradiation parameters in each facility, in view of acquiring dosimetry systems, a treatment plan and, most importantly, the development of boron compounds that fit, as best as possible, the ideal BNCT requirements. The first clinical trials focusing on Boron neutron capture therapy were initiated by Dr. Sweet şi Brownell (Massachusetts Institute of Technology - MIT Boston) and Farr (Brookhaven National Laboratory – BNL) in 1951. Between 1951 and 1961, patients with glioblastoma from USA were irradiated, both at BNL as well as MIT. Based on the support provided by EORTC the first BNCT clinical studies were also initiated in Europe. Consequently, EORTC formed a study group for BNCT. A first phase I trial included 25 patients with optimally operated glioblastomas in 5 neurosurgery centres. Another EORTC protocol studied BSH and BPA administration in patients with different types of solid tumours in order to identify new targets for BNCT. Simultaneously, another study following BNCT and BPA in cutaneous metastases of malignant melanoma was implemented. A fourth protocol was initiated for BNCT with BSH in glioblastoma multifome. A third tumour type approached through BNCT was recurrent head and neck cancer. The first studies were established by Kato in Japan. In September 2003, Hiratsuka treated a recurrent papillary thyroid cancer with BNCT, in Japan. Yanagie and collaborators also used BNCT in Japan in recurrent rectal cancers. Other BNCT experiments evaluated treatment methods for locally recurrent breast cancers. Multiple liver metastases of the colorectal adenocarcinoma were among thy first liver tumours that raised researchers’ interest, from the area of BNCT. In February 2005, in Kyoto, Japan, at KUR the first patient with hepatocarcinoma was treated with BNC. The project “Study, research and application in the oncological clinical practice of treatment with neutron capture by B-10” participated in 2005 at the CEEX governmental competition- “Research Excellency Programmes”. The project was selected for financing and benefitted from a grant offered by the Romanian Government, PC-D01-PT11-94 - 2005.Although there are still considerable inconveniences, BNCT may be regarded as a promising method for cancer treatment.
Keywords: radiotherapy, BNCT, clinical applications
Galeş N. Laurenția, Anghel M. Rodica1
GLOBAL CLINICAL EXPERIENCE WITH BORON NEUTRON CAPTURE THERAPY (BNCT)
REVIEWTherapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 135 - 140© Copyright reserved 2015
Introduction
BNCT represents a top therapeutic method that relies on nuclear technology knowledge,
chemistry, biology as well as on medicine experience in treating malignant tumours.
In 1936, GL Locher (Pensylvania SUA) suggested, for the first time, that neutron capture reactions could have applicability in cancer therapy. [1,2]
Various pre-clinical experiments were initially
applied in order to demonstrate the effectiveness of BNCT concept. Once they demonstrated the concept, pre-clinical experiments continued by focusing on a better establishment of the irradiation parameters in each facility, in order to develop dosimetry systems, a treatment plan and, most importantly, the development of boron compounds that fit, as best as possible, the ideal BNCT requirements. Furthermore, pre-clinical experiments were carried out for different tumours than head tumours, some of them already being continued in the area of clinical research.
Experimental BNCT irradiation on pre-clinical models:
BNCT irradiation on murine subjects for head and neck tumours formed the subject of several researches
1 UMF Carol Davila Bucureşti

Therapeutics, Pharmacology and Clinical Toxicology136
in Osaka, Japan and Bariloche, Argentina[3,4], that obtained an important rate of complete remission. In Argentina, studies were carried out with the purpose to evaluate feasibility of BNCT sequential irradiation (two successive applications), thus constituting the first researches of this kind.
Other animal subjects were used for BNCT irradiation of pancreatic tumours[5], thyroid tumours [6], mesothelioma intrathoracic tumours[7], or multiple lung metastases (Taormiona Projaect in Pavia, Bariloche in Argentina), prostate tumours [8], ocular melanoma [9], osteosarcoma (TAORMINA), etc.
For primitive tumours of the liver or metastatic ones o series of pre-clinical trials was applied in order to identify the optimal dosimetry and treatment plan [10,11,12] as well as an experimental irradiation of laboratory animals (Pavia, Bariloche). [13, 14]
BNCT based clinical trials The first clinical trials on neutron Boron capture
therapy were initiated by Sweet and Brownell (Massachusetts Institute of Technology - MIT Boston) [15, 16, 17] and Farr (Brookhaven National Laboratory – BNL) [15, 18] in 1951. Between 1951 and 1961, patients with glioblastoma from USA were irradiated, both at BNL as well as MIT however without conclusive results which rendered, at the time, the trials a failure. In 1967-1985 Prof. Hatanaka from Japan obtained impressive outcomes, which triggered more research in the field.[19] Studies were resumed both in USA (in 1994 at Brookhave and Massachusetts Institute of Technology for glioblastomas and malignant melanoma, by using BPA) [20,21] as well as in Europe (in 1997 la Petten – glioblastoma- BPA and BSH).[22] Subsequently, similar studies began in Finland (1999- glioblastoma, ENT and malignant melanoma- BPA)[23], Czech Republic (2000- glioblastoma- BPA and BSH)[24], Sweden (glioblastoma- BPA and BSH) [25] and Italy (2001- liver metastases- BPA), Argentina (2003- malignant melanoma_ BPA) [26] and Taiwan (2010- ENT- BPA).[27] In Japan since 1968 until now patients with glioblastoma, malignant melanoma, head and neck cancer, pulmonary cancer, thyroid and liver cancer patients have been irradiated with therapies based on both BPA and BSH.
Hatanaka and later on, his collaborator, Nakagawa [28] irradiated over 200 patients suffering from glioblastoma, predominantly using BSH. They reported promising results on a long term due to the extended survival period achieved by certain of their patients. Thus, survival rates were: at 2 years- 11,4%, at 5 years- 10,4% and at 10 years- 5,7%.[19, 28] Results were not confirmed by sub-group tests performed by Laramore on American patients treated by Hatanaka.[29] Despite this, the Japanese experience with BNCT therapy in glioblastomas was positive, enabling further development of this treatment technique. The difference between the first American and Japanese studies lied in the Japanese practice, namely an initial debulking surgery and subsequent irradiation with thermal neutrons following craniotomy (direct brain irradiation) considering the low penetrability of thermal neutrons. [30, 31]
Once studies were resumed in the United States,
approximately 53 patients were irradiated at BNL and 20 at MIT, by using BPA and epithermal neutrons, with higher tissue penetrability. [32, 33] The results were comparable to those from the conventional irradiation. [30, 34, 35]
More recent protocols are currently trying to improve BNCT technique by prolonged BPA infusion for better tumour penetrability (Sweden) [36, 37], by mixing BPA with BSH (Japan)[38, 39, 40, 41, 42], mixing thermal and epithermal neutrons [43] or combining with X-ray irradiation boost. [38] So far the outcomes seem superior to the classical BNCT irradiation.
Based on the support provided by EORTC, the first BNCT clinical studies were also initiated in Europe. Consequently, EORTC formed a study group for BNCT. A first phase I trial included 25 patients with optimally operated glioblastomas in 5 neurosurgery centres. They received 4 daily consecutive BNCT fractions at European High Flux Reactor în Petten. These studies aimed at determining immediate and late toxicities and to compare them with toxicities occurring to conventional radiotherapy of 60 Gy in six weeks. Another EORTC protocol focused on BSH and BPA administration in patients with different types of solid tumours in order to identify new targets for BNCT. Hence, another study on the administration of BNCT combined with BPA was in cutaneous metastases of malignant melanoma. A fourth protocol was initiated for BNCT with BSH in glioblastoma multifome. [44]
In Europe, a smaller number of patients with glioblastoma was treated: in Petten, Holland (27 patients), [22, 24], Essen Germany (24 petients)[45], Helsinki Finland (20 patients)[23], Studsvik Sweden (52 patients) and Rez Czech Republic (5 patients). [22]
After brain tumours, the most predominant in terms of number of irradiated patients was malignant melanoma, the experiments having begun back in the 1980s. The first patients were irradiated by Mishima in 1985 and the outcomes turned even better than those in brain tumours, as complete remissions were registered and some of the patients having no sign of illness four years after the irradiation. [46, 47, 27, 48, 49] Busse et All also treated patients with brain metastases occurring to malignant melanoma or cutaneous melanoma.[20, 30, 50]. Patients with malignant melanoma were also irradiated in settings in Argentina.[51] The overall conclusion was that BNCT in irradiation of malignant melanomas obtained better outcomes compared to glioblastomas, BNCT constituting an experimental treatment method recommended in inoperable tumours that cannot benefit from stereotractic radiosurgery.[52]
A third tumour approached through BNCT was recurrent mouth and throat cancer. The first studies were carried out by Kato in Japan [53-55], followed by other Japanese researchers including Kankaanranta in Finland.[56] Kato irradiated 26 patients with recurrent head and neck tumours that had received both radiotherapy and chemotherapy. Histological patterns were heterogeneous, this including even salivary gland sarcoma or adenocarcinoma. The mean period of survival was 13.6 months but with a survival rate of 24% at six years. Significant adverse events occurred, such as cerebral necrosis, osteomyelitis, mucositis.[53]
XIX, Vol.19, Number 4/2015 137
Kankaanranta and collaborators deployed a clinical study that included 30 patients with recurrent head and neck cancers that received BNCT with BPA therapy in Helsinki.[56] 29 of patients were evaluable for the rate of response, which led to 13 complete remissions and 9 partial remissions, a 76% rate of response with 20% rate of survival, with no progression at 2 years and 30% global survival at 2 years.[35, 56, 57] The most frequent adverse events were oral mucositis, pain and fatigue. Three patients presented osteoradionecrosis and 1 patient showed soft tissue necrosis. [56]
In Japan, Fuwa N. et All tried to improve results from BPA administration both intravenously as well as though the arteries in the case of ENT cancers. They irradiated 5 patients that had no other therapeutic option. For two of the BNCT irradiation had to be applied two times. The medical team obtained one complete remission and 4 partial remissions, but except for one patient the rest died to a recurrent illness. For such cases the authors suggest conventional irradiation mixed with a BNCT boost.[58]
In August 2010, the first patient with recurrent ENT cancer was irradiated in Taiwan.[27]
The role of BNCT in ENT cancers continues to be relatively inconclusive considering the low number of patients treated so far.[59]
In September 2003 Hiratsuka treated with BNCT therapy the first recurrent papillary thyroid carcinoma, in Japan. In 2009 the patient was alive with no signs of recurrence and with well tolerated treatment.[60, 61]
In Japan, Yanagie and collaborators used BNCT for recurrent rectal cancers but with no reports on long term results.[62]
Other BNCT experiments assessed treatment methods for locally recurrent breast cancer.[63]
BNCT experience in liver tumoursPrimitive liver tumours are one of the most
frequent tumours in the world. Of these, 25-30% are hepatocarcinomas and the rest come from intrahepatic bile ducts. The mortality rate to this cancer type is very high, but varies, at global levels. The incidence of these tumours is increasing worldwide, along with the increase of viral hepatitis B and C. The liver represents is the most common metastatic site in malignant tumours (colorectal, breast cancers, pulmonary, etc). For example, 10-25% of colorectal patients have liver metastases at the time of diagnosis and of them only 25% can be resected with curative intent. For most patients, therapeutic options are limited, with little satisfactory results.
Multiple liver metastases of colorectal adenocarcinoma were the first to raise interest of researchers in the area of BNCT. [22, 24] Thus, through the TAORMINA project, two patients underwent irradiation at the Pavia University reactor.[64] They received BPA- fructosis 300 mg/kg i.v. for two hours through the colic vein, after which hepatectomy was performed. The liver was irradiated with BNCT, outside the body, with thermal neutrons of 4 x 1012 cm-2 fluency, for 10 minutes. Consequently, during the second surgical phase, the liver was transplanted back to the patient.[65] The first patient, aged 48 was treated in 2001. He presented 14 bilolobar metastases and 63% residual liver
function, with no vascular abnormalities. The procedure spanned on 21 hours, of which, 5 hours and a half anhepatic. 7 days after the procedure the patient went through another surgery, this time for blood collection in the peritoneal cavity. The first three weeks succeeding BNCT the patients presented liver and kidney failure and rhabdomyolysis, with accentuated asthenia and brain dysfunction, probably through cell lisis. Kidney dialysis was necessary for two weeks. After the first month the patient reached full recovery, with an increase in the liver residual function of 73%.[64] 20 month after BNCT the first local recurrence resurfaced, the patient undergoing surgery and adjuvant chemotherapy that he previously had refused. 33 month after BNCT the patient presented a new hepatic and extrahepatic relapse that was non-responsive to chemotherapy. 40 month post BNCT a new immunochemotherapy protocol is initiated but with no response which led to the patient’s death in August 2005. In 2003 the procedure was applied to a second 39 year old patient. He presented 11 liver metastases, 58% residual liver function, dilated cardiomyopathy and a hepatic artery vascular abnormality. The procedure lasted 18 hours and 40 minutes, of which 6 hours and 10 minutes anhepatic. The first post BNCT month went similarly as with the previous case, this meaning the same evolution in the liver, kidney, brain functions. 30 days postoperatively, surgery was needed in order to correct a hepatic artery thrombosis but it failed. The patient died 33 days after BNCT to cardiac failure and pulmonary oedema caused by the hepatic artery thrombosis.
In February 2005, the first patient with hepatocarcinoma was treated in Kyoto, Japan, at KUR. The patient was diagnosed in June 2004 when resection was performed. In November 2004 he presented multiple bilobar recurrence which led to a transarterial chemoembolization. In December 2004 another relapse was identified. A combination of 250 mg/kg BPA was administered in 60 minutes as well as BSH 1g/kg, a share of it associated with lipiodol. After six hours the patient was irradiated for 62 minutes with a lateral right beam and for 21 minutes with a posterior beam. In terms of adverse events, fever and cytolysis occurred but disappeared after one week. Sadly, one month after BNCT administration, progressive disease was identified having the patient die 10 month post BNCT.
BNCT experience in primitive or secondary liver tumours is, for the time being, limited requiring a complicated methodology that impedes its administration on a large scale, hence the formulation and release of clear conclusions. [67]
ConclusionsAlthough BNCT is an innovative and promising
treatment method, still several aspects continue to be critical which prevent it from being applied on a larger scale. The first problematic aspect regards the boron delivery compound. The second aspect has to do with the neutron flux. The third concerns dosimtery and last but not least, clinical experience is essential. In what concerns the latter aspect, a multidisciplinary team can be difficult to form. Furthermore, researchers have to deploy numerous and complex clinical trials that include
Therapeutics, Pharmacology and Clinical Toxicology138
a larger number of patients before ranking BNCT therapy in cancer treatments.
Thanks to the support provided by EORTC the first clinical studies on BNCT in Europe were deployed.
The project “Study, research and application in the oncological clinical practice of treatment with neutron capture by B-10” participated in 2005 at the CEEX governmental competition- “Research Excellency Programmes”. The project was selected for financing and benefitted from a grant offered by the Romanian Government, PC-D01-PT11-94 - 2005. Research was carried out by a 5 partners’ consortium: “Prof Dr. Al. Trestioreanu” Oncology Institute, Bucharest (IOB), “Fundeni” Clinical Hospital (ICF), “Pitesti” Nuclear Research Department (SCN), “Horia Hulubei” National Institute for R&D in Physics and Nuclear Engineering (IFN-HH) and “Victor Babes” Institute’s Foundation.
The project was conducted over four years in 6 stages. Despite the mentioned inconveniences one can
conclude that BNCT is a promising treatment method for cancer and research in this domain represents the first stage in the implementing process of an effective oncology therapy in Romania. One of the physical accomplishments of BNCT could be the application of Cyclotron/Laser from the Magurele platform as long as a neutron flux is obtained as well as an irradiation medical site.
References
1. Barth RF., Soloway A.H., Fairchild R.G., Boron Neutron Capture Therapy for Cancer – Scientific American 1990; 263 (4): 100-7.
2. Locher G.L., Biological effects and therapeutic possibilities of neutrons – Am J Roentgenol 1936; 36 (1): 1-13.
3. Kamida A, Obayashi S, Kato I, et al. Effects of boron neutron capture therapy on human oral squamous cell carcinoma in a nude mouse model. - Int J Radiat Biol. 2006 Jan; 82(1): 21-9.
4. Kreimann EL, Itoiz ME, Longhino J, et al. Boron neutron capture therapy for the treatment of oral cancer in the hamster cheek pouch model. Cancer Res. 2001 Dec 15; 61(24): 8638-42.
5. Yanagie H, Maruyama K, Takizawa T, et al. Application of boron-entrapped stealth liposomes to inhibition of growth of tumour cells in the in vivo boron neutron-capture therapy model.- Biomed Pharmacother. 2006 Jan; 60(1): 43-50.
6. Pisarev M.A., Dagrosa M.A., Juvenal G.J. Boron Neutron Capture in Cancer: Past, Present and Future Arq Bras Endocrinol Metab 2007; 51 (5): 852-856.
7. Suzuki M, Sakurai Y, Masunaga S, Kinashi Y, Nagata K, Maruhashi A, Ono K A Preliminary Experimental Study of Boron Neutron Capture Therapy for Malignant Tumors Spreading in Thoracic Cavity – Jpn J Clin Oncol 2007; 37 (4): 245-249.
8. Yasui L, Kroc T, Gladden S, et al. Boron neutron capture in prostate cancer cells. Appl Radiat Isot. 2012 Jan; 70(1): 6-12.
9. Packer S, Coderre J, Saraf S, et al. Boron neutron capture therapy of anterior chamber melanoma with p-boronophenylalanine – Br. J. Cancer 1997, 76 (12): 1623-9.
10. Benzi V., Mezzetti F., Rocchi F., Sumini M. Feasibility analysis of a Plasma Focus neutron source for BNCT treatment of transplanted human liver – Nuclear Instruments and Methods in Physics research B 213 (2004) 611-15.
11. Suzuki M, Sakurai Y, Masunaga S, et al. - Dosimetric study of boron neutron capture therapy with borocaptate sodium (BSH)/lipiodol emulsion (BSH/lipiodol-BNCT) for treatment of multiple liver tumors – Int J Radiation Oncology Biol Phys, 2004, 58 (3): 892-896.
12. Kotiluoto P., Auterinen I – MCNP study for epithermal neutron irradiation of an isolated liver at the Finnish BNCT facility – Applied Radiation and Isotopes 2004, 61: 781-785.
13. Suzuki M, Masunaga S, Kinashi Y, et al. Intra-arterial administration of sodium borocaptate (BSH)/lipiodol emulsion delivers B-10 to liver tumors highly selectively for boron neutron capture therapy: experimental studies in the rat liver model - Int J Radiat Oncol Biol Phys. 2004 May 1; 59(1): 260-6.
14. Nano R, Barni S, Chiari P, et al. Efficacy of boron neutron capture therapy on liver metastases of colon adenocarcinoma: Optical and ultrastructural study in the rat – Oncology Reports 2004, 11: 149-153.
15. Godwin JT, Farr LE, Sweet WH, Robertson JS. Pathological study of eight patients with glioblastoma multiforme treated by neutron-capture therapy using boron 10. Cancer 1955; 8: 601–15.
16. Asbury AK, Ojemann, Nielson SL, Sweet WH. Neuropathologic study of fourteen cases of malignant brain tumor treated by boron-10 slow neutron capture therapy. J Neuropathol Exp Neurol 1972; 31: 278–303.
17. Sweet WH. Practical problems in the past in the use of boron-slow neutron capture therapy in the treatment of glioblastoma multiforme. Proceedings of the First International Symposium on Neutron Capture Therapy; 1983 Oct 12–14. Brookhaven National Laboratory Reports 51730. p. 376–8.
18. Farr LE, Sweet WH, Robertson JS, et al. Neutron capture therapy with boron in the treatment of glioblastoma multiforme. Am J Roentgenol 1954; 71: 279–91.
19. Nakagawa Y, Hatanaka H. Boron neutron capture therapy: clinical brain tumor studies. J Neuro-Oncol, 33: 105-15, 1997.
20. Busse P, Zamenhof R, Harling O, et al. The Harvard-MIT BNCT program: overview of the clinical trials and translational research. In: Hawthorne MF, Shelly K, Wiersema RJ, editors. Frontiers in neutron capture therapy. Vol. 1. New York: Kluwer Academic/Plenum Publishers; 2001. p. 37–60.
XIX, Vol.19, Number 4/2015 139
21. Palmer MR, Goorley JT, Kiger WS, et al. Treatment planning and dosimetry for the Harvard-MIT phase I clinical trial of cranial neutron capture therapy. Int J Radiat Oncol Biol Phys 2002; 53: 1361–79.
22. Wittig A., Hideghety K., Paquis P., et al. Sauerwein, W.; Moss, R.; Wittig, A., eds. "Current clinical results of the EORTC – study 11961". Research and Development in Neutron Capture Therapy Proc. 10th Intl. Congress on Neutron Capture Therapy. pp. 1117–22, 2002.
23. Joensuu H, Kankaanranta L, Seppälä T, et al. Boron neutron capture therapy of brain tumors: clinical trials at the Finnish Facility using boronophenylalanine. J Neurooncol 2003; 62: 123–34.
24. Burian J, Marek M, Rataj J, et al. Report on the first patient group of the phase I BNCT trial at the LVR-15 reactor. In: Sauerwein W, Moss R Wittig A, editors. Research and Development in Neutron Capture Therapy, Bologna: Monduzzi Editore; 2002. p. 1107–12.
25. Capala J, H.-Stenstam B, Sköld K, et al. Boron neutron capture therapy for glioblastoma multiforme: clinical studies in Sweden. J Neurooncol 2003; 62: 135–44.
26. Zonta, A.; Pinelli, T.; Prati, U.; et al. "Extra-corporeal liver BNCT for the treatment of diffuse metastases: What was learned and what is still to be learned". Applied Radiation and Isotopes 2009; 67 (7–8): S67–75.
27. Mishima, Y. Cancer Neutron Capture Therapy; Mishima, Y., Ed.; Plenum Press: New York, 1996, p 1-26.
28. Nakagawa Y, Pooh K, Kobayashi T, et al. Clinical review of the Japanese experience with boron neutron capture therapy and a proposed strategy using epithermal neutron beams. J Neuro-Oncol, 62: 87-99, 2003.
29. Laramore G.E., Wootton P., Livesey J.C., et al, Boron neutron capture therapy: a mechanism for achieving a concomitant tumor boost in fast neutron radiotherapy – Int. J. Radiat. Oncol. Biol. Phys., 1994, 28, 1135.
30. Barth R.F., Coderre J.A., Vicente H, et al. Boron Neutron Capture Therapy of Cancer: Current Status and Future Prospects – Clinical Cancer Research 2005; 11 (11): 3987-4002.
31. Yamamoto T, Matsumura A., External Beam BNCT for Glioblastoma Multiforme in Neutron Capture Therapy: Principles and Applications – Sauerwein W.A.G., Wittig A, Moss R, Nakagawa Y – Springer 2012; 377-388.
32. Diaz A.Z. Assessment of the results from the phase I/II boron neutron capture therapy trials at the Brookhaven National Laboratory from a clinician’s point of view – Journal of Neuro-Oncology 2003; 62 (1-2): 101-9.
33. Coderre J.A., Elowitz E.H., Chadha M et al Boron neutron capture therapy for glioblastoma multiforme using p-boronophenilalanine and epithermal neutrons: trial design and early clinical results - J. Neurooncol 1997; 33: 141-52.
34. Busse P.M., Harling O.K., Palmer M.R., et al A critical examination of the results from the Harvard-MIT NCT program phase I clinical trial of neutron capture therapy for intracranial disease - Journal of Neuro-Oncology 2003; 62 (1-2):111-21.
35. Barth RF, Vicente MG, Harling OK, et al, Current status of boron neutron capture therapy of high grade gliomas and recurrent head and neck cancer – radiat Oncol 2012, 29; 7: 146.
36. Henriksson, R.; Capala, J.; Michanek, A.; et al. "Boron neutron capture therapy (BNCT) for glioblastoma multiforme: A phase II study evaluating a prolonged high-dose of boronophenylalanine (BPA)". Radiotherapy and Oncology 2008; 88 (2): 183–91.
37. Sköld, K.; Gorlia, T.; Pellettieri, L.; et al. "Boron neutron capture therapy for newly diagnosed glioblastoma multiforme: An assessment of clinical potential". British Journal of Radiology 2010; 83 (991): 596–603.
38. Kawabata S, Miyatake S-I, Kuroiwa T, et al Boron Neutron Capture Therapy for Newly Diagnosed Glioblastoma – Journal of Radiation Research 2009; 50 (1): 51-60.
39. Miyatake S-I, Kawabata S, Yokoyama K, et al, Survival benefit of Boron neutron capture therapy for recurrent malignant gliomas – Journal of Neuro-Oncology 2008; 91 (2): 199-206.
40. Yamamoto T, Nakai K, Matsumura A – Boron neutron capture therapy for glioblastoma, Cancer Letters, 2008; 262: 143.
41. Yamamoto, T.; Nakai, K.; Nariai, T.; et al."The status of Tsukuba BNCT trial: BPA-based boron neutron capture therapy combined with X-ray irradiation". Applied Radiation and Isotopes 2011; 69 (12): 1817–8.
42. Miyatake S, Kajimoto Y, Kawabata S et al, Modified boron neutron capture therapy for malignant gliomas performed using epithermal neutron and two boron compounds with different accumulation mechanisms: an efficacy study based on findings on neuroimages – J Neurosurg, 2005, 103: 1000.
43. Yamamoto T.; Matsumura A, Nakai K. et al, Current clinical results of the Tsukuba BNCT trial – Applied Radiat isotopes, 2004, 61, 1089.
44. Sauerwein W, Zurlo A; EORTC Boron Neutron Capture Therapy Group. The EORTC Boron Neutron Capture Therapy (BNCT) Group: achievements and future projects. Eur J Cancer. 2002 Mar; 38 Suppl 4: S31-4.
45. Vos MJ, Turowski B, Zanella FE et al, Radiologic findings in patients treated with boron neutron capture therapy for glioblastoma multiforme within EORTC trial 11961 – Int J Rad Oncdol Biol Phys, 2005, 61, 392.
46. Mishima Y., Ichihashi M., Hatta S., et al., 1989 – New thermal neutron capture therapy for malignant melanoma. Melanogenesis-seeking 10B molecular-melanoma cell interaction from in vitro to first clinical trial, Pigment Cell Res, 1989; 2, 226.
Therapeutics, Pharmacology and Clinical Toxicology140
47. Mishima Y, Honda C, Ichibashi M et al, Treatment of malignant melanoma by single neutron capture therapy with melanoma-seeking 10B-compound. Lancet,1989; 1, 388.
48. Hiratsuka J., Clinical results of BNCT for head and neck melanoma. 16th Intl' Congress on Neutron Capture Therapy, Helsinki, Finland, June 14–19, 2014.
49. Larsson B, Crawford J, Weinreich R, Advances in neutron capture therapy, medicine and physics, Amsterdam, Elsevier, 1997, 1: 10-25.
50. Coderre J.A., Turcotte J.C., Riley K.J., et al. Boron neutron capture therapy: cellular targeting of high linear energy transfer radiation – Technol Cancer Res Treat 2003, 2:1-21.
51. Gonzalez SJ, Bonomi MR, Santa Cruz GA, et al. First BNCT treatment of a skin melanoma in Argentina: dosimetric analysis and clinical outcome. Appl Radiat Isot 2004; 61:1101–5.
52. Hiratsuka J, Fukuda H Malignant melanoma in Neutron Capture Therapy: Principles and Applications – Sauerwein W.A.G., Wittig A, Moss R, Nakagawa Y – Springer 2012 – 433-448.
53. Kato, I.; Fujita, Y.; Maruhashi, A.; et al."Effectiveness of boron neutron capture therapy for recurrent head and neck malignancies". Applied Radiation and Isotopes 2009; 67 (7–8): S37–42.
54. Wang, L.W.; Wang, S.J.; Chu, P.Y.; et al. "BNCT for locally recurrent head and neck cancer: Preliminary clinical experience from a phase I/II trial at Tsing Hua Open-Pool Reactor". Applied Radiation and Isotopes 2011; 69 (12): 1803–6.
55. Kato I, Ono K, Sakurai Y, et al. Effectiveness of BNCT for recurrent head and neck malignancies. Appl Radiat Isot 2004;61:1069–73.
56. Kankaanranta L, Seppälä T, Koivunoro H, et al Boron Neutron Capture Therapy in the Treatment of Locally Recurrent Head-and-Neck Cancer: A Final Analysis of a Phase I/II Trial - International Journal of Radiation Oncology Biology Physics, 2012, 82 (1): e67-75.
57. Savolainen S, Kortesniemi M, Timonen M, et al. Boron neutron capture therapy (BNCT) in Finland: technological and physical prospects after 20 years of experiences. Phys Med. 2013 May; 29(3): 233-48.
58. Fuwa N, Suzuki M, Sakurai Y, et al. Treatment results of boron neutron capture therapy using intra-arterial administration of boron compounds for recurrent head and neck cancer. - Br J Radiol. 2008 Sep; 81(969): 749-52.
59. Aihara T, Morita N, BNCT for Advanced or Recurrent Head and Neck Cancer in Neutron Capture Therapy: Principles and Applications – Sauerwein W.A.G., Wittig A, Moss R, Nakagawa Y – Springer 2012 – 417-424.
60. Hiratsuka J, Morita N, Aihara T, et al., First clinical trial of neutron capture capture therapy for thyroid cancer, in Nakagawa Y, Kobayashi T, Fukuda H eds, Proceedings of ICNCT-12, Kagawa, Japan, 7-9.
61. Pisarev M, Dagrosa M, Juvenal GJ, Studies on the Possible Application of BNCT to Thyroid Cancer in Neutron Capture Therapy: Principles and Applications – Sauerwein W.A.G., Wittig A, Moss R, Nakagawa Y – Springer 2012 – 425-432.
62. Altieri, S.; Bortolussi, S.; Barth, et al. "Thirteenth International Congress on Neutron Capture Therapy". Applied Radiation and Isotopes 2009; 67 (7–8): S1–2.
63. Yanagie H, Application of Neutron Capture Therapy for Locally Recurrent Breast Cancer in Neutron Capture Therapy: Principles and Applications – Sauerwein W.A.G., Wittig A, Moss R, Nakagawa Y – Springer 2012 – 449-460.
64. Zonta, A.; Prati, U.; Roveda, L.; et al."Clinical lessons from the first applications of BNCT on unresectable liver metastases". Journal of Physics: Conference Series 2006; 41 (1): 484–95.
65. Pinelli T, Zonta A, Altieri S, et al. TAOrMINA: from the first idea to the application to the human liver. In: M.W. Sauerwein, R. Moss and A. Wittig, editors. Research and Development in Neutron Capture Therapy, Bologna: Monduzzi Editore, International Proceedings Division; 2002. p. 1065–72.
66. Suzuki M, Sakurai Y, Hagiwara S, et al First attempt of boron neutron capture therapy (BNCT) for hepatocellular carcinoma. Jpn J Clin Oncol. 2007 May; 37(5): 376-81.
67. Zonta A, Roveda L, Altieri S Liver metastases in Neutron Capture Therapy: Principles and Applications – Sauerwein W.A.G., Wittig A, Moss R, Nakagawa Y – Springer 2012 – 461-504.

XIX, Vol.19, Number 4/2015 141
Elena Truță8 Calea Floreasca, 014461 BUcharest, Romaniae-mail: [email protected]
Abstract. Throughout one year: 2013 – 2014, a lot of 50 children from the residential institution “SOS Satele Copiilor” Bucharest, was included in our research The children were distributed in two groups: Group A which consisted of 25 children (12 girls, 13 boys) who were not diagnosed with ADHD and Group B which consisted of 25 children (14 boys, 11 girls) who were diagnosed with ADHD. Initially, the two groups were subjected to a psychodiagnostic battery of tests, one of them being: “ Evaluating the Health State of children with ADHD questionnaire” elaborated by the study team, particularly for this research, with the purpose of highlighting the direct link between children’s health status and their ADHD symptoms. Subsequently, the children from group B benefited from a psychotherapy protocol which combined the strategies of the short term psychodynamic psychotherapy. The emotional wellbeing average values of the children from group B and group A were significantly different at the beginning of our program, whileat the end the difference were highly reduced based on the statistical analysis.
Key words: ADHD, emotional wellbeing, health state assessment questionnaire.
Mitu Ana Mihaela1, Daviţoiu Ana Maria2, Truţă Elena3,Stănciulescu Luminiţa3, Ionică M.4
A STUDY REGARDING THE INTERRELATION BETWEEN A GOOD STATE OF MIND AS AN INDICATOR OF HEALTH STATE AND PSYCHOTHERAPY IN CHILDREN WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER
ORIGINAL PAPERTherapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 141 - 145© Copyright reserved 2015
Background
Attention Deficit and Hyperactivity Disorder (ADHD) is defined by The American Academy
of Paediatrics as being the most common childhood neurobehavioral disorder which can profoundly affect the academic performances, the wellbeing and the social interactions of the child (***., 2014).
The studies performed on children that were diagnosed with ADHD marked out that ADHD is one of the most common psychiatric disorder seen in childhood whose symptoms persist during teenage and adulthood in more than 50% of the cases studied (Mannunza S., et al, 2003; Barkley R.A., et al, 2002).
The clinical diagnosis is based on medical, psychological, behavioural and educational comprehensives evaluations. The diagnosis criteria are forecasted by DSM – V and ICD – 10 (***., 2013; ***., 2004).
The ratio of ADHD diagnoses in children is five
boys to one girl. This is explained by the fact that during childhood the boys’ behavioural manifestations resemble to hyperactivity and violence, whereas the girls’ behavioural manifestations resemble to chronic tiredness and attention problems; those symptoms can be easily ignored and therefore girls are less diagnosed and treated for ADHD (Judd F., et al, 2008).
The aetiology of ADHD is multifactorial and it includes:
• external factors (problems during pregnancy and during birth, premature birth and low birth weight, infections, CNS diseases or disorders , exposure to toxic substances, smoking during pregnancy);
• genetic factors (they are the main cause of the development of this disorder (65 -90%) without fully explaining its’ existence, brothers and parents have a three to five times increased risk to develop ADHD;
• social factors (family and school conditions considerably influence this manifestations emphasis and development).
The studies performed on families, twins and adopted children marked out that ADHD has a familial component
1 Psychology Cabinet “Ana Mihaela Mitu”2 Clinical Emergency Children Hospital “Victor Gomoiu” Bucharest3 Clinical Emergency Hospital Bucharest4 Scientific Research Centre for Military Health; University “Politehnica” Bucharest

Therapeutics, Pharmacology and Clinical Toxicology142
and a hereditary component, the hereditary component being the main risk factor (Lanham J.S., 2005). The risk of being diagnosed with ADHD is 4 to 10 times bigger for close relatives. Studies performed on twins that were diagnosed with ADHD during childhood and teen years have highlighted the inheritable component of the diseases in 76% of the studied cases (Faraone S.V., et al., 2005).
The same studies reveal that genetics are the base of the persistence of the behavioural manifestations during adulthood (van den Berg S.M., et al, 2006).
It is believed that the molecular genetic studies will elucidate the mechanism by which ADHD diagnosed in childhood persists or remits during adulthood. In this way new ways to extend disease prevention in adulthood could be developed. In this sense one of the assumptions is issued by Halperin which leaves from the premises that there is a connection between ADHD and premature cortical dysfunctions, while remission of symptoms is closely related to the maturation of executive control. Cortical and subcortical balance functions induce remission or persistent ADHD symptoms (Halperin J.M., et al, 2006, Halperin J.M., et al, 2008). Discovered genetic variations in dopamine D4 (DR4) and D5 (DR5), in dopamine transporter (DAT1), in dopamine beta hydroxylase genes (DB4), in 5-hydroxytryptamine receptor 1B (HTR1B) and the serotonin transporter (5HTT), synaptosomal associated protein (SNAP 25), explain 3.2% of ADHD variation symptoms (Faraone S.V., et al, 2005; Franke B., et al, 2009).
Other changes in genes like Cadherin – 12 genes (CDH 12) (Daviţoiu A.M., 2015) were recently identified
Health State is a complex concept with many sides, namely it is a state of good physical, material, social, emotional, and personal development. It is used as a measure of discretion in several areas: medicine, economics, and philosophy. Health State is currently the term mostly used by numerous disciplines . However it is poorly used, and it should be removed from the dictionary (??) (Felce D. & Perry J., 1995). It is the phrase located on everyone's lips, but nobody knows what to do with it (Campbell A., 1974).
The differences in the definition of health state come from the description and interpretation of psychological processes through the concepts and different ways of communications (Dissart K. & Deller S.C., 2000).
The position an individual or group in society hold as well as social and political factors affect the meaning of the concept of health state. The strength of the concept is just its multidisciplinary specific, but as his general meaning overshadows the original one the power of analytics decreases. (Veenhoven R., 2000).
In the 60s, in the US, it was thought that the economic development alone positively affected the health state. It was found, however, that economic development was not enough to impact the health state. Although economy was considered as a burden, the population faced a high rate of violence, crime, public disorder and degradation of the environment. When assessing the health state social factors should be taken into account. Therefore, the policy of increasing the health state will use methods tuned to correct the existing social and economic relations (Zamfir C., 1990).
When we define health state we often ask, who is being evaluated: the individual, the society or some specific groups (children with ADHD, women’s health) (Escobar S., et al, 2005)?
A second question that arises is: What health state we wanted to define? Objective (individual standard of living) or subjective health state (subjective way in which each measures his own life - contentment, happiness, and fulfillment)?
According to Allardt a better life is defined as: "to have" (material needs), "to love" (social needs) and "to be" (personal development).
According to Veenhoven there are four basic qualities of health state: the ability of individuals to overcome life's problems, adaptive potential, how each individual judges their own life, life satisfaction and subjective well-being .
The literature mentions a link between the health state level and manifestation of ADHD symptoms.
Health state is a multidimensional concept which includes the comprehension of an individual’s development within communities, as well as the matter of how much psychological processes are influenced by environmental factors and the man’s meaning of his personal life, that is the result of the global evaluation from the standpoint of his own life (Katschnig H., et al, 2008).
Health State refers to both, the objective conditions under which human life unfolds and the subjective way in which each individual perceives his/her own life - the state of satisfaction, happiness and fulfilment (Lanham J.S., 2005).
The study’s interests are the psychological perspective (subjective) regarding health state which refers to the perceptions, estimations and strategies that the individual applies to his current living status and to the comparison made with his personal needs, values and expectations.
In terms of the impact ADHD has on the health state of an individual, summing- education, life style, individual evolution, researches demonstrated that the majority of children with ADHD struggle with: learning difficulties (45.5% vs. 13% at healthy children), failing or dropping out of school (70.9% vs. 21.3%), sleep disorder, low self esteem, smoking, drugs use (52% vs. 24%) (Møller V., et al, 2008).
In the case of ADHD, there is increasingly more evidence in literature showing that the prognosis and health state depend on the patient's mental balance and psychological processes that can modulate or stimulate the upper portion of the brainstem.
Zigmond and his team conducted a review of studies on patients with ADHD who received psychological intervention, assessing symptoms reduction rates. They watched the most commonly used types of psychological interventions: psycho-education, behavioural training, individual psychotherapy and group interventions, highlighting their positive impact on physical and mental health (Zigmond T., et al, 2009).
Emotional wellbeing, as an indicator of health state’s quality, comprises: positive emotions, negative emotions, self-esteem and personal beliefs (Gregory D., et al, 2009). This indicator is included in our questionnaire, where we focused on measuring the harm (the perception of
XIX, Vol.19, Number 4/2015 143
harm?), self-esteem and personal beliefs. Negative affects are based on the intensity with
which feelings are felt as: guilt, the desire to cry, fear and lack of joy of life. Frustrations or lack of understanding can generate violence or retirement into solitude. This section aims at finding solutions for the prevention of child failure to adapt to everyday challenges. Moreover they often seek to redress by appealing to false solutions - alcohol, tobacco, drugs, excess of every kind, violence.
Self-esteem is defined our reactions and the way they are generated by our perception of the self. A good self-image is characterized by: low aggressiveness, confidence, optimism, acceptance of differences.
Personal beliefs concern the way in which children have the capacity to appreciate the power of learning, memory, attention, intention, willingness to take a decision, assign values to objects and experiences. They are all able to give meaning to existence and to ensure the overall feeling of wellbeing. A source of comfort and security, they rely on a sense of belonging to the intelligible world, enhancing motivation for a harmonious adaptation and willingness to act independently, confirming thus the child’s personality.
Materials and method The study was conducted between 2013 and 2014.
Children from the orphanage "SOS Children's Villages" Bucharest were included. Psychological evaluation and psychotherapeutic treatments were conducted with the childrens’ and their legal representative’s consent. The study included 50 children divided in two groups: Group A included 25 children (12 boys and 13 girls) without a diagnosis of ADHD and Group B consists of 25 children (14 boys and 11 girls) diagnosed with ADHD.
Inclusion criteria: children aged 7 - 15 years; children with diagnosed and undiagnosed ADHD.
Exclusion criteria: psychiatric diagnoses with (autism, psychosis, mental deficiency), associated neurological disorders (paresis, cerebral palsy).
Statistical analysis was conducted based on the Student test.
Psychological assessment was performed with a "Battery of psycho diagnostic tests" presented below.
• An adapted form of the “Sheet investigation for the diagnosed children’s parents and for hyperactive teenagers” conducted by a group of specialists from the Medical Center of Masschusetts was used for the purpose of this study (Barkley R.A., et al, 2002). This is intended for interviewing parents of hyperactive children. The interview contains questions covering five areas: the child’s and family’s personal data, development factors (prenatal history, postnatal and infant development period, medical history and treatment), social relationships and activities, current behavioural problems, school behaviour. The questionnaire was applied to the parents once, at the beginning of the study.
• “Semi-structured clinical interview for children and adolescents with ADHD” applied at the beginning of the study .
• “Health State Assessment Questionnaire for
children with ADHD”. This questionnaire was developed by us and was specifically adapted for children with ADHD. The purpose of this questionnaire is to highlight the direct link between health state and the severity of ADHD symptoms. It includes 21 items systematized by the following criteria: health state (11 items) and ADHD symptoms (10 items). The criterion " health state " defined as a multidimensional concept includes the following areas: physical wellbeing ; emotional wellbeing; social wellbeing, material wellbeing, development and activity. The criterion "ADHD Symptoms" structured to measure the severity of symptoms, as perceived by the patient, includes: predominantly hyperactive and attention problems, predominantly hyperactive- impulsive. If the values of the two fields are equal they are considered mixed symptoms. The test was applied before and after the treatment.
The questionnaire presents an objective method for assessing and addressing the group with ages between 7 and 14 years. It was built, analyzed, pre-tested and completed in a study conducted in the "SOS Children's Villages" orphanage from 2013 to 2014, on a sample of 25 patients diagnosed with ADHD. The method used for the clinical trial included the current questionnaire
Group A included 25 children (12 boys and 13 girls) who weren’t diagnosed with ADHD and Group B consisted in 25 children (14 boys and 11 girls) diagnosed with ADHD.
Group A, was used as a reference to evaluate the quality of life. Children from this group were assessed with the “Health State Assessment Questionnaire”, once, at the beginning of the study.
Group B, was used as an experimental group in the process of evaluating the quality of life. The children evaluated benefited from a “protocol of psychotherapy“ which combined short psychodynamic therapy strategies. The therapeutic approach was centred on building personal identity in children. The therapy’s goal was to help children feel confident, to help them see the world around them as it really is. The used therapeutic techniques and objectives were adapted each child’s particularities , given the fact that each is unique and we cannot extrapolate the same contingency plan for a child to another just because the two are suffering from the same type of mental disorder.
The protocol covered 14 individual therapy sessions for each child with ADHD included in the study and 8 sessions of group therapy (three groups). We tried to make the foster parents understand the characteristics of children with ADHD and prepare them to help the patients manage and mitigate the difficulties created by these characteristic features, during special sessions. Strategies were developed to increase pro-social behaviours and eliminate the inappropriate remains.
The protocol consisted of 8 sessions of group therapy for each caregiver included in the study. The groups were composed of 6 - 8 participants. Please note that the meetings with the foster parents started before the children’s therapeutic sessions, and in this way, by the
Therapeutics, Pharmacology and Clinical Toxicology144
time the children began the treatment the caregivers could apply what they had learned.
Results and discussions25 children aged 7 to 15 were diagnosed with ADHD
at different ages. They were divided into two groups (7 - 10 years) and (11 - 15 years). In the age group (7 - 10 years) there were 19 diagnosed children, representing (76%). The cause of a medical evaluation of such a high rate within this age group could be integration into the school system and difficulties to adapt to it. The highest ratio of ADHD diagnoses- attention deficit hyperactive form was identified in children diagnosed at this age. . These data are consistent with literature. Childrens’ consultation at this age group was frequently performed at the teacher’s requests whoe worries revolved around impulse or hyperactive manifestations like: motor restlessness , continuous tendency to run and jump , inability to remain seated during working hours and the accidents that happenoften, especially during breaks.
In the age group 11 - 15 years there were 6 diagnosed children (24%). For the diagnosis of ADHD, the following were highlighted: poor school performance in the context of the subject’s cognitive possibilities , failure or drop out, orientation towards risky behaviours.
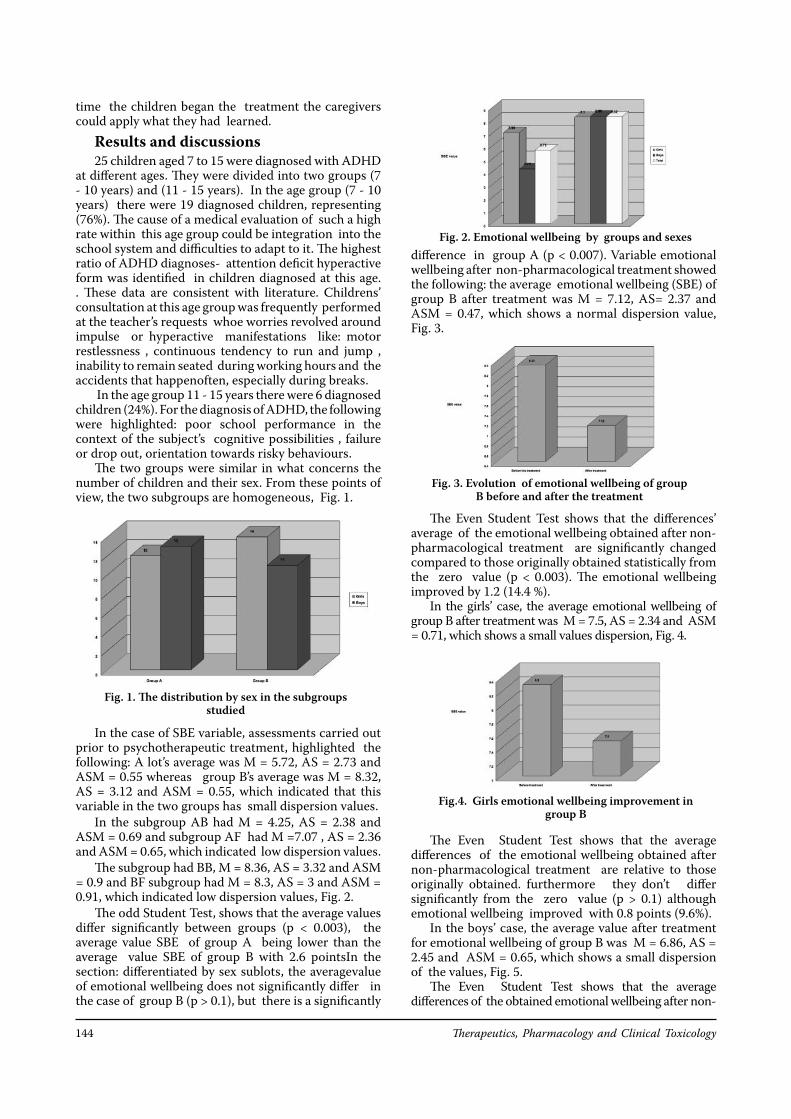
The two groups were similar in what concerns the number of children and their sex. From these points of view, the two subgroups are homogeneous, Fig. 1.
In the case of SBE variable, assessments carried out prior to psychotherapeutic treatment, highlighted the following: A lot’s average was M = 5.72, AS = 2.73 and ASM = 0.55 whereas group B’s average was M = 8.32, AS = 3.12 and ASM = 0.55, which indicated that this variable in the two groups has small dispersion values .
In the subgroup AB had M = 4.25, AS = 2.38 and ASM = 0.69 and subgroup AF had M =7.07 , AS = 2.36 and ASM = 0.65, which indicated low dispersion values.
The subgroup had BB, M = 8.36, AS = 3.32 and ASM = 0.9 and BF subgroup had M = 8.3, AS = 3 and ASM = 0.91, which indicated low dispersion values , Fig. 2.
The odd Student Test, shows that the average values differ significantly between groups (p < 0.003), the average value SBE of group A being lower than the average value SBE of group B with 2.6 pointsIn the section: differentiated by sex sublots, the averagevalue of emotional wellbeing does not significantly differ in the case of group B (p > 0.1), but there is a significantly
difference in group A (p < 0.007). Variable emotional wellbeing after non-pharmacological treatment showed the following: the average emotional wellbeing (SBE) of group B after treatment was M = 7.12, AS= 2.37 and ASM = 0.47, which shows a normal dispersion value, Fig. 3.
The Even Student Test shows that the differences’ average of the emotional wellbeing obtained after non-pharmacological treatment are significantly changed compared to those originally obtained statistically from the zero value (p < 0.003). The emotional wellbeing improved by 1.2 (14.4 %).
In the girls’ case, the average emotional wellbeing of group B after treatment was M = 7.5, AS = 2.34 and ASM = 0.71, which shows a small values dispersion, Fig. 4.
The Even Student Test shows that the average differences of the emotional wellbeing obtained after non-pharmacological treatment are relative to those originally obtained. furthermore they don’t differ significantly from the zero value (p > 0.1) although emotional wellbeing improved with 0.8 points (9.6%).
In the boys’ case, the average value after treatment for emotional wellbeing of group B was M = 6.86, AS = 2.45 and ASM = 0.65, which shows a small dispersion of the values, Fig. 5.
The Even Student Test shows that the average differences of the obtained emotional wellbeing after non-
Fig. 2. Emotional wellbeing by groups and sexes
Fig. 3. Evolution of emotional wellbeing of group B before and after the treatment
Fig.4. Girls emotional wellbeing improvement in group B
Fig. 1. The distribution by sex in the subgroups studied
XIX, Vol.19, Number 4/2015 145
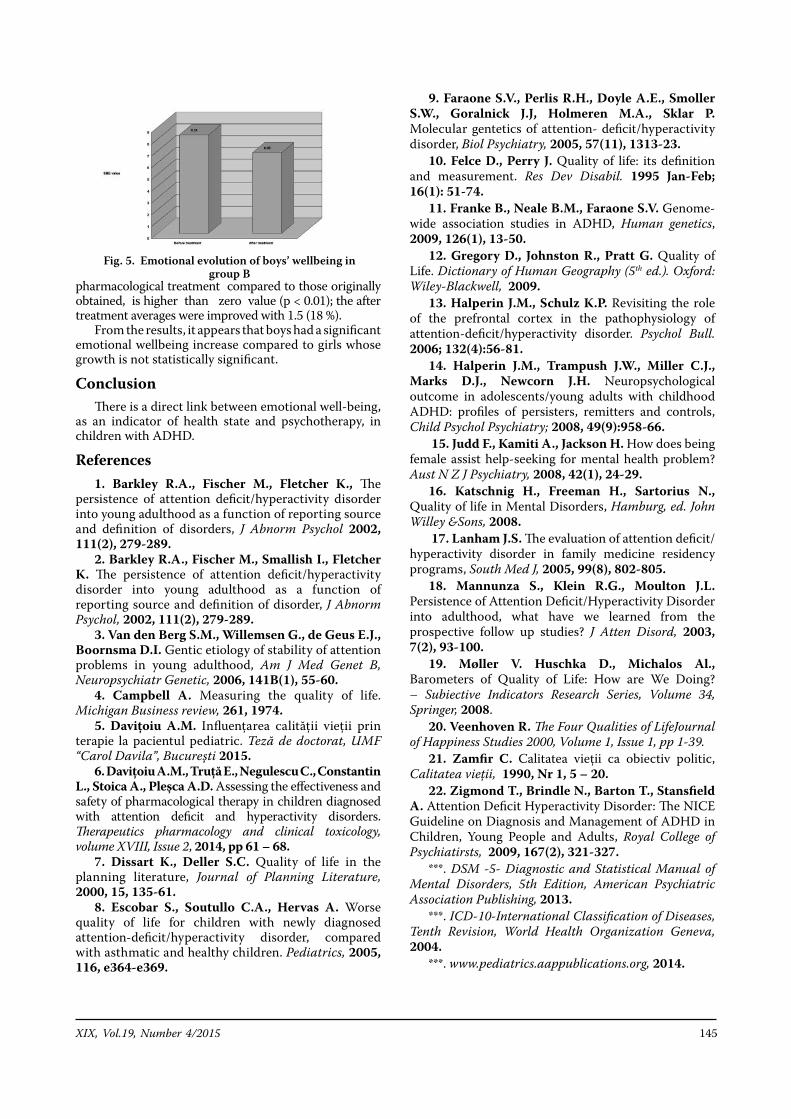
pharmacological treatment compared to those originally obtained, is higher than zero value (p < 0.01); the after treatment averages were improved with 1.5 (18 %).
From the results, it appears that boys had a significant emotional wellbeing increase compared to girls whose growth is not statistically significant.
ConclusionThere is a direct link between emotional well-being,
as an indicator of health state and psychotherapy, in children with ADHD.
References 1. Barkley R.A., Fischer M., Fletcher K., The
persistence of attention deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorders, J Abnorm Psychol 2002, 111(2), 279-289.
2. Barkley R.A., Fischer M., Smallish I., Fletcher K. The persistence of attention deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder, J Abnorm Psychol, 2002, 111(2), 279-289.
3. Van den Berg S.M., Willemsen G., de Geus E.J., Boornsma D.I. Gentic etiology of stability of attention problems in young adulthood, Am J Med Genet B, Neuropsychiatr Genetic, 2006, 141B(1), 55-60.
4. Campbell A. Measuring the quality of life. Michigan Business review, 261, 1974.
5. Daviţoiu A.M. Influenţarea calităţii vieţii prin terapie la pacientul pediatric. Teză de doctorat, UMF “Carol Davila”, Bucureşti 2015.
6. Daviţoiu A.M., Truţă E., Negulescu C., Constantin L., Stoica A., Pleşca A.D. Assessing the effectiveness and safety of pharmacological therapy in children diagnosed with attention deficit and hyperactivity disorders. Therapeutics pharmacology and clinical toxicology, volume XVIII, Issue 2, 2014, pp 61 – 68.
7. Dissart K., Deller S.C. Quality of life in the planning literature, Journal of Planning Literature, 2000, 15, 135-61.
8. Escobar S., Soutullo C.A., Hervas A. Worse quality of life for children with newly diagnosed attention-deficit/hyperactivity disorder, compared with asthmatic and healthy children. Pediatrics, 2005, 116, e364-e369.
9. Faraone S.V., Perlis R.H., Doyle A.E., Smoller S.W., Goralnick J.J, Holmeren M.A., Sklar P. Molecular gentetics of attention- deficit/hyperactivity disorder, Biol Psychiatry, 2005, 57(11), 1313-23.
10. Felce D., Perry J. Quality of life: its definition and measurement. Res Dev Disabil. 1995 Jan-Feb; 16(1): 51-74.
11. Franke B., Neale B.M., Faraone S.V. Genome-wide association studies in ADHD, Human genetics, 2009, 126(1), 13-50.
12. Gregory D., Johnston R., Pratt G. Quality of Life. Dictionary of Human Geography (5th ed.). Oxford: Wiley-Blackwell, 2009.
13. Halperin J.M., Schulz K.P. Revisiting the role of the prefrontal cortex in the pathophysiology of attention-deficit/hyperactivity disorder. Psychol Bull. 2006; 132(4):56-81.
14. Halperin J.M., Trampush J.W., Miller C.J., Marks D.J., Newcorn J.H. Neuropsychological outcome in adolescents/young adults with childhood ADHD: profiles of persisters, remitters and controls, Child Psychol Psychiatry; 2008, 49(9):958-66.
15. Judd F., Kamiti A., Jackson H. How does being female assist help-seeking for mental health problem? Aust N Z J Psychiatry, 2008, 42(1), 24-29.
16. Katschnig H., Freeman H., Sartorius N., Quality of life in Mental Disorders, Hamburg, ed. John Willey &Sons, 2008.
17. Lanham J.S. The evaluation of attention deficit/hyperactivity disorder in family medicine residency programs, South Med J, 2005, 99(8), 802-805.
18. Mannunza S., Klein R.G., Moulton J.L. Persistence of Attention Deficit/Hyperactivity Disorder into adulthood, what have we learned from the prospective follow up studies? J Atten Disord, 2003, 7(2), 93-100.
19. Møller V. Huschka D., Michalos Al., Barometers of Quality of Life: How are We Doing? – Subiective Indicators Research Series, Volume 34, Springer, 2008.
20. Veenhoven R. The Four Qualities of LifeJournal of Happiness Studies 2000, Volume 1, Issue 1, pp 1-39.
21. Zamfir C. Calitatea vieţii ca obiectiv politic, Calitatea vieţii, 1990, Nr 1, 5 – 20.
22. Zigmond T., Brindle N., Barton T., Stansfield A. Attention Deficit Hyperactivity Disorder: The NICE Guideline on Diagnosis and Management of ADHD in Children, Young People and Adults, Royal College of Psychiatirsts, 2009, 167(2), 321-327.
***. DSM -5- Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, American Psychiatric Association Publishing, 2013.
***. ICD-10-International Classification of Diseases, Tenth Revision, World Health Organization Geneva, 2004.
***. www.pediatrics.aappublications.org, 2014.
Fig. 5. Emotional evolution of boys’ wellbeing in group B
Therapeutics, Pharmacology and Clinical Toxicology146
Miorița Toader30-32 Iancu de Hunedoara Blvd., 011743 Bucharest, Romaniae-mail: [email protected]
Abstract. Oropharyngeal cancer is a common malignancy which includes a wide variety of histopathologic tumors. Unfortunately it affects not only the elderly population, but also young patients, its incidence rising alarmingly in the last decade. The gold standard for the treatment of ororpharyngeal cancer is the multidisciplinary approach. The authors present a literature review of the current therapeutic regimens, with an emphasis on the surgical techniques.
Keywords: oropharyngeal cancer, transoral laser microsurgery, robotic surgery, chemoradiation
1 University of Medicine and Pharmacy “Grigore T. Popa” Iasi2 Emergency Clinical Hospital for Children “Grigore Alexandrescu”, Bucharest3 National Institute of Cerebrovascular Disease, Bucharest
Palade O.D.1, Lazăr Andra Sorina1, Oprea Alina2, Toader Miorița2, Toader C.3
TREATMENT IN OROPHARYNGEAL CANCER- AN UPDATE
Therapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 146 - 148© Copyright reserved 2015
Introduction
In 2002, the crude incidence rates of carcinoma of the head and neck, including oropharyngeal
cancers, in Europe were 36/100 000/year in the male population and 7/100 000/ year for females. This fact became a driving force for the development of new surgical treatment techniques as well as adjustment of the chemotherapy and radiation therapy protocols, in order to battle the disease.
Traditionally, surgery and radiation therapy have been the standards for treatment of oropharyngeal cancers. A pooled analysis of 6,400 patients from 51 reported series who were treated for base-of-tongue oropharyngeal carcinoma between 1970 and 2000 demonstrated local control rates of 79% (surgery ± radiation) and 76% (radiation), (P = .087); locoregional control was 60% versus 69% (P = .009); 5-year survival was 49% for surgery with or without radiation therapy versus 52% (P = .2) for radiation therapy with or without neck dissection. Similar findings showed equivalent overall and cause-specific survival between surgery versus radiation for tonsil carcinoma; however, 23% overall and cause-specific survival for severe complications in the surgery group versus 6% overall and cause-specific survival in the radiation therapy group (P < .001).[4]
Surgical techniques of oropharyngeal cancer treatment
For patients with early-stage disease, single-modality treatment, usually radiation therapy alone is preferred, however, new surgical techniques, including transoral
surgery and transoral robotic surgery, are currently growing. Nonrandomized comparisons are starting to suggest superior quality of life with minimally invasive surgical techniques.[4]
Surgical innovation may occur by applying new technology to a procedure or with new anatomic approaches to accomplish existing surgical goals. New technologies from different fields like optics, ultrasonography, radiology and robotics as well as new instruments, drugs and materials, have been introduced in medicine and changed the head and neck surgery techniques.
Important technical improvements facilitating visualization, both in the areas of lighting and magnification, have been realized which is an important part of surgical visualization. The application of surgical loupes for open procedures improves visualization considerably by magnifying vital structures.
Magnification and superior illumination combined with endoscopic telescopes with a camera system provide an excellent two-dimensional view. Current telescope technology allows for high-definition images and digital magnification. [5]
Improvements in intraoperative monitoring, especially with respect to anaesthesia, cardiac and respiratory systems monitoring, have been critical in enhancing the safety of surgical procedures in general, as well as in head and neck surgical approaches.
New techniques are also facilitated by improvements in instrumentation. In some cases, reducing the size of standard instruments or altering the mechanism of action will assist the use of standard instrument designs through smaller incisions or remote locations. Laparoscopic instrumentation offers a set of innovative tools that may be used and potentially modified. Additionally, the development of manual and robotic articulating instrumentation offers the potential to improve dexterity in less accessible areas. With robotic technology, tremor filtration, scaling, and augmented movement can also be achieved [6].
THERAPEUTICAL PRACTICE

XIX, Vol.19, Number 4/2015 147
Haemostasis is crucial to performing safe surgery. Improvements in cautery, vessel ligation, surgical clips, and haemostatic dressings have allowed surgery to be accomplished more quickly, with less blood loss, and without surgical drains. [5]
Different approaches are used for oropharyngeal surgeries. Transoral approach may be used for limited tumours since it doesn't produce external scars, and transcervical/visor flap approach may be considered for large tumours of the base of tongue or tonsil but both provide a poor exposure. Mandibulectomy is indicated for larger lesions, but has a risk of malocclusion and plate extrusion. Mandibulotomy spares mandible and may be approached laterally or midline with a lip-splitting incision. Osteotomy is performed to create a favourable repair followed by rigid fixation. The technique provides exceptional exposure and less risk of malocclusion. Lateral Pharyngotomy may be considered for small base of tongue or posterior pharyngeal wall tumours. The technique has limited exposure field, but spares mandible and avoids lip-splitting incision. Transhyoid Pharyngotomy may be considered for small base of tongue or posterior pharyngeal wall tumours without significant superior or tonsillar extension. The surgeon enters pharynx above or through hyoid bone. The technique spares mandible, avoids lip-splitting incision, but has a poor exposure superiorly. Each of these technologies have benefits and drawbacks that need to be understood, particularly when incorporated into more complicated approaches.[5]Transoral laser microsurgery
Laser is an acronym for light amplification by stimulated emission of radiation. Since their development in 1960, lasers as surgical tools have evolved and now play an important role in the diagnosis and treatment of cancer. It is precise, decreases the risk of infection, and reduces healing time, bleeding, swelling, and scarring.
Several laser systems, such as the diode, ruby, Ho:YAG, Er:YAG, Nd:YAG, and yellow light lasers, as well as dye lasers for photodynamic therapy, have been used. However, the argon and CO2 lasers were the first laser systems to be clinically used.
Most small tumours of the posterior pharyngeal wall can be completely resected without any difficulties. If tumour extension has occurred toward the hypopharynx or nasopharynx is present, the resection is extended accordingly.[7]
Excisions made by transoral laser microsurgery diminishes morbidity by lowering postoperative complications, such as swelling, pain and scarring, and makes assessment of cancer relapse easier.Endoscopic CO2 Laser resection
The CO2 laser has currently the highest value in otorhinolaryngology. Advantages are that no tracheotomy is required, the preservation of the suprahyoid musculature allows more normal swallowing, no reconstruction needed, and hospital stay is decreased with patients returning to an oral diet as early as the first day postoperative. This approach has given extraordinary results for all areas in which it has been applied.
The technique involves using a bivalve laryngopharyngoscope, an operating microscope,
and a CO2 laser as the dissecting instrument. Under microscopic vision, tumour margins are taken up to 10 mm and as opposed to conventional open procedures, the tumour is often cut through to provide a direct view of tumour depth and/or to assess cartilage invasion, in this fashion making complete resection possible. Cartilage may be exposed or resected during the surgery and to avoid perichondritis antibiotics are given prophylactically.[1] [6]
TORS- Transoral robotic surgeryThe Da Vinci Surgical System is a sophisticated
robotic platform which offers a minimally invasive option for major surgery and is designed to expand the surgeon’s capabilities. With Da Vinci, small incisions are used to insert miniaturized wristed instruments and a high-definition 3D camera. The surgeon views a magnified, high-resolution 3D image of the surgical site inside the body. At the same time, the latest robotic and computer technologies scale, filter and seamlessly translate surgeon's hand movements into exact micro-movements of the instruments. The system cannot move or operate on its own the surgeon being in control 100%. The system holds up to three EndoWrist instruments and one 3D camera that may be used by the surgeon to access the target anatomy.
Recently, many reports have reported the importance of TORS in head and neck cancer treatment. The objective of transoral robotic surgery TORS is the removal of pharyngeal and laryngeal cancers and to improve functional and aesthetic outcomes with the same survival rate. [8]
Transoral robotic surgery gives the surgeon access to operate through the mouth – avoiding a large incision through the jaw and throat. TORS allows a clearer and wider view of the surgical field and better 3D visualization of structures in comparison to TOLS (transoral laser surgery), this enabling a way in to the tumour via a smaller approach than the external one.
It has been demonstrated that the Da Vinci Robot enables transoral removal of the tumour while preserving key structures and nerves. In addition, it has been showed that it further allows a complete resection with negative surgical margins and without complications. Another advantage of TORS is the use of miniaturized tools. This allows mimicking standard surgical instruments and arm movements, with tremor filtration. It also offers an advantage through an excellent frontal view and the reach of blind corners of the pharyngolaryngeal complex, due to the possibility to use a 30° telescope. [3] [9]
The possible complications in TORS are bleedings that might be life-threatening, difficulty in swallowing or breathing, with the need of airway security by tracheotomy or tracheostomy, or use of ventilator for a long time, loss of taste, tongue paralysis, difficulty opening mouth, narrowing of throat, vocal cord damage with changes in speech or voice quality, abnormal salivation pathway, difficulty speaking, injury to teeth, lips, or nerves in the tongue.[2]
Negative outcomes of transoral robotic surgery system may be linked with longer operative and anaesthesia times. There is also the risk of the da Vinci robotic surgical system malfunction. This can lead to serious damage or the need to switch to another type

Therapeutics, Pharmacology and Clinical Toxicology148
of surgery. Switching to another procedure technique could also result in a longer operation time, a longer time under anaesthesia and greater risk of complications.[2]Radical neck dissection
Lymph node metastasis reduces the survival rate of patients with squamous cell carcinoma by half. The survival rate is less than 5% in patients who have a recurrent metastasis in the neck after previously undergoing surgery. Therefore, the control of the neck is one of the most important aspects in the successful management of these tumours.[10]
The number of lymph nodes involved by cancer has been found to correlate with the incidence of cancer recurrence in the neck and survival rates. Patients with four or more involved nodes have significantly worse prognosis than patients with only one node involved.
In a landmark paper from Memorial Sloan-Kettering, Strong reported a series of 204 patients treated by radical neck dissection alone. The recurrence rate in the neck was 36.5% in patients with histologically positive nodes at one level of the neck and 71% in patients with positive nodes at multiple levels. The presence of tumour spread beyond the capsule of a lymph node is a major determinant for prognosis and need for postoperative chemo radiation. [2] [10]
It has also been shown that the recurrence rate in the neck after radical neck dissection is significantly higher when extracapsular spread of tumour is verified. The efficacy of a therapeutic radical neck dissection must be measured in relationship with the adjuvant use of radiation therapy. Studies have shown that the combined use of radical neck dissection and postoperative radiation therapy can reduce recurrence in the ipsilateral neck and prevent recurrence in the contralateral side in patients with cervical lymph node metastases who have one or more of the factors associated with increased risk of recurrence. These include multiple histologically positive nodes and extracapsular extension of tumour.[2]Radiation and chemotherapy
The probability of tumour control correlates with both the dose of radiation and the size of the malignancy. Radiation cell kill is essentially an exponential function of dosage. Thus, the necessary dosage of radiation is approximately proportional to the number of cells in the tumour (tumour volume). Control of microscopic disease in head and neck cancers usually requires a dosage of approximately 50 Gy, while positive margins require 60 Gy, and adequate control of large (stages T3 and T4) tumours requires dosages in the range of 70 Gy.[11]
Altered fractionation achieves better local control and higher overall survival than conventionally fractionated radiation but has not yet been compared with conventional chemoradiation. In the postoperative setting, the addition of concurrent chemotherapy to radiation improves survival in cases with extracapsular extension and/or microscopically involved surgical margins.
External beam radiotherapy was the most frequently used form of radiotherapy but intensity-modulated radiation therapy (IMRT) has evolved over the past decade to become a standard technique for head and neck radiation therapy. IMRT allows a dose-painting
technique also known as a simultaneous-integrated-boost (SIB) technique with a dose per fraction slightly higher than 2 Gy, which allows shortening of overall treatment time increasing the biologically equivalent dose to the tumour offering a better tumour control by reducing the constraints on the tumour dose that are due to critical organs that limit the tumour boost doses in conventional radiation therapy. Therefore, the use of intensity-modulated radiation therapy in advanced head and neck cancer may offer sparing of vital organs, including major salivary glands, minor salivary glands dispersed within the oral cavity, mandible, pharyngeal musculature, inner and middle ears, temporomandibular joints, temporal brain lobes, and optic pathways.[11]
Chemotherapy may be given with a curative intent, or it may aim to prolong life or to reduce symptoms - palliative chemotherapy. Concurrent chemoradiation is superior to radiation therapy alone and is used for locally advanced disease, emphasizing organ preservation and functionality.
In a randomized trial of locally advanced head and neck cancer patients, curative-intent radiation therapy alone (213 patients) was compared with radiation therapy plus weekly Cetuximab (211 patients). At a median follow up of 54 months, patients treated with Cetuximab and radiation therapy demonstrated significantly higher progression-free survival (hazard ratio for disease progression or death, 0.70; P = .006). [9]
Depending on pathological findings after primary surgery, PORT or postoperative chemoradiation has proven its use in the adjuvant setting for T4 disease, perineural invasion, lymphovascular invasion, positive margins or margins less than 5 mm, extracapsular extension of a lymph node, two or more involved lymph nodes.References
1. Courtney M. Townsend, Sabiston Textbook of surgery: the biological basis of modern surgical practice, 2012, pp. 805-835.
2. Eugene N. Myers, master techniques in otolaryngology-head and neck surgery, Wolters Kluwer Health I Lippincott Williams & Willdns., 2014.
3. R. E. Harris, Global Epidemiology of Cancer. 4. Hans-Olov Adami, Textbook of Cancer
Epidemiology, 2008. 5. G. W. Randolph, Surgery of Thyroid and
Parathyroid glands, 2013. 6. M. A. A. D. M. Jochen A.Werner, "Transoral
Laser Microsurgery in Carcinomas of the Oral Cavity, Pharynx, and Larynx," Cancer Control, September/October 2002, Vol. 9, No.5.
7. J. G. Strong MS, "Laser surgery in the larynx: clinical experience with continuous CO2 laser".
8. [Online]. Available: http://www.davincisurgery.com/da-vinci-surgery/da-vinci-surgical-system/.
9. P. R. R. P. G. C. a. G. S. G. MERCANTE, "Transoral robotic surgery (TORS) for tongue base tumours," Acta Otorhinolaryngol Ital, 2013.
10. M. F. Antonio Riera March and M. M. Chief Editor: Arlen D Meyers, "Radical Neck Dissection," http://emedicine.medscape.com/article/849895-overview.
11. M. B. H. H. M. F. F. Paul W. Flint, Cummings Otolaryngology Head & Neck Surgery, 2010, pp. 1369-1373.

XIX, Vol.19, Number 4/2015 149
Drăgan Cornel19-21 Șos. Ștefan cel Mare, 020125 Bucharest, Romania e-mail: [email protected]
Abstract. As patients with osteosarcoma become long-term survivors, increasing attention revolved around the burden of late effects. Recent studies showed an increase in the incidence of secondary malignant neoplasms in patients with osteosarcoma compared with the general population. The risk of developing leukaemia was reported to be in an increasing rate in the last decade. [1] Case report. In this report we present the case of a 19 year old patient diagnosed in the Haematology Department of Colentina Clinical Hospital in February 2015 with Acute Myeloid Leukaemia following the treatment (chemo- and radio-therapy) for an osteogenic osteosarcoma performed 3 years earlier. The cytogenetic examination revealed an abnormal karyotype with 91 chromosomes (XXY). The molecular biology exam did not find mutations in the FLT3ITD, FLT3D835 and NPM1 A genes. After the first induction course of chemotherapy the patient achieved complete remission, which was consolidated by 3 more courses of chemotherapy and an allogeneic stem cell transplant. Conclusion. Taking into consideration the prior treatment for osteosarcoma consisting in radiotherapy and chemotherapy we identified a secondary Acute Myeloid Leukaemia, this representing a major negative prognostic factor, along with the cytogenetic abnormalities found. These factors strongly indicate that the first complete remission should be consolidated by allogeneic stem cell transplant. Particularities of this case are the association of the two malignancies in a young patient, the presence of an abnormal karyotype (hyperploid), and also a good response to the induction therapy, thus achieving complete remission after the first induction course, and of course, sustaining that response.
Key words: secondary leukemia, osteosarcoma, cytogenetics, complete remission.
1 Hematology Department, Colentina Clinical Hospital, Bucharest 2 Genetic Center Laboratories 3 Hematology Clinic, Colțea Clinical Hospital, Bucharest
Drăgan C.1, Meilin Murat1, Trifa A.2, Tevet Mihaela1, Lupu Anca Roxana3
ACUTE MYELOID LEUKAEMIA IN A 19 YEAR OLD PATIENT PREVIOUSLY TREATED FOR OSTEOSARCOMA - CASE REPORT AND REVIEW OF THE LITERATURE
CASE REPORTTherapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 149 - 151© Copyright reserved 2015
Introduction
It has been observed that the survival rate for patients with osteosarcoma (OS) has improved substantially
with the introduction of multi-agent chemotherapy. As the number of paediatric cancer survivors increases, there is a concern about the development of secondary malignant neoplasms (SMN). [1] Osteosarcoma (OS) is the most common malignant bone tumour that affects adolescents and young adults. It is treated by surgery and pre- and postoperative chemotherapy. Various SMNs have been reported in OS patients. [2] Secondary Acute Myeloid Leukaemia (sAML) has also been reported in literature as a rare complication of OS. [3] However, the exact offending drug is difficult to prove as there is no consistent data. From the cited literature, sAML usually develops 2 years after completion of therapy. [4]
Different molecular and pathogenic agents may be involvedin the development of second malignant neoplasms in long-term survivors of osteosarcomas. Some authors believe that the treatment with topoisomerase II inhibitors may have a role in the development of sAML, while others talk about cisplatin-associated sAML.
Case reportIn this report we present the case of a 19 year old
patient admitted in the Haematology Department of Colentina Clinical Hospital in February 2015 for fever (38°C), extreme fatigue, intense pallor.
The patient had been diagnosed with osteogenic osteosarcoma of the right femur 3 years before which was operated and treated with chemotherapy (COSS EURAMOS protocol – Cisplatin, Doxorubicin, Methotrexate) and radiotherapy, achieving complete remission.
The symptoms which led him to our Department started approximately one month prior to the presentation atthe hospital, and worsened over time.
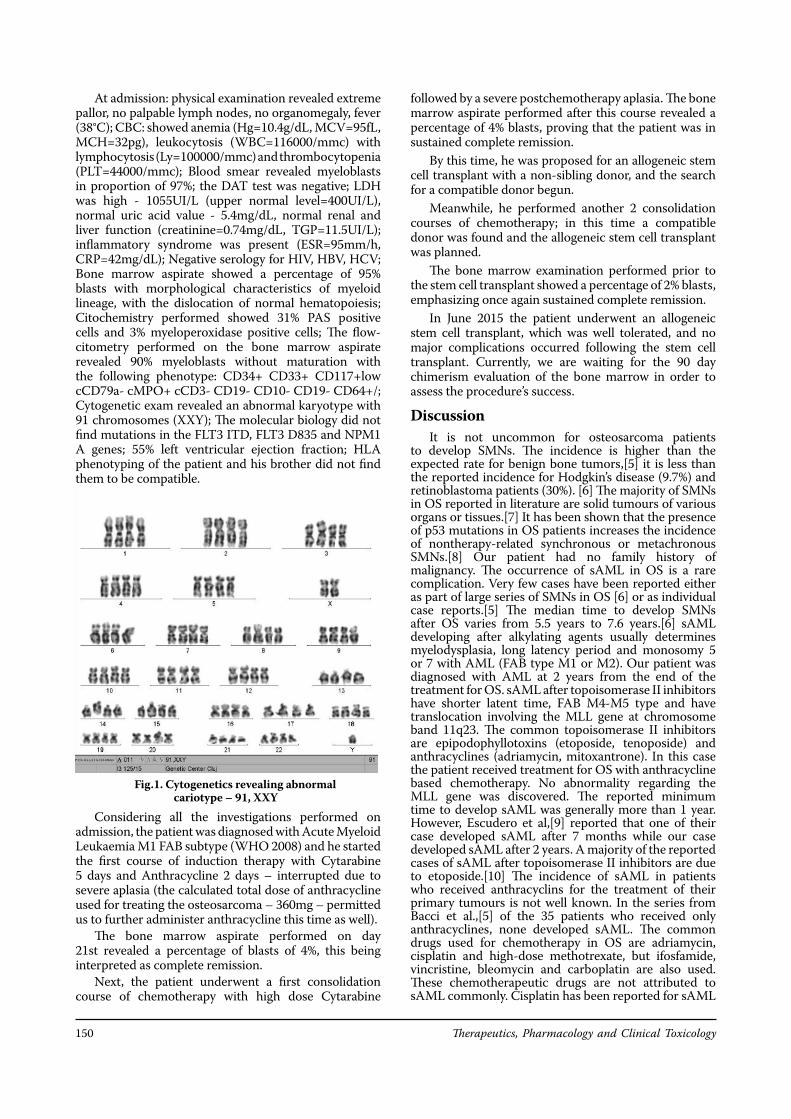
Therapeutics, Pharmacology and Clinical Toxicology150
At admission: physical examination revealed extreme pallor, no palpable lymph nodes, no organomegaly, fever (38°C); CBC: showed anemia (Hg=10.4g/dL, MCV=95fL, MCH=32pg), leukocytosis (WBC=116000/mmc) with lymphocytosis (Ly=100000/mmc) and thrombocytopenia (PLT=44000/mmc); Blood smear revealed myeloblasts in proportion of 97%; the DAT test was negative; LDH was high - 1055UI/L (upper normal level=400UI/L), normal uric acid value - 5.4mg/dL, normal renal and liver function (creatinine=0.74mg/dL, TGP=11.5UI/L); inflammatory syndrome was present (ESR=95mm/h, CRP=42mg/dL); Negative serology for HIV, HBV, HCV; Bone marrow aspirate showed a percentage of 95% blasts with morphological characteristics of myeloid lineage, with the dislocation of normal hematopoiesis; Citochemistry performed showed 31% PAS positive cells and 3% myeloperoxidase positive cells; The flow-citometry performed on the bone marrow aspirate revealed 90% myeloblasts without maturation with the following phenotype: CD34+ CD33+ CD117+low cCD79a- cMPO+ cCD3- CD19- CD10- CD19- CD64+/; Cytogenetic exam revealed an abnormal karyotype with 91 chromosomes (XXY); The molecular biology did not find mutations in the FLT3 ITD, FLT3 D835 and NPM1 A genes; 55% left ventricular ejection fraction; HLA phenotyping of the patient and his brother did not find them to be compatible.
Considering all the investigations performed on admission, the patient was diagnosed with Acute Myeloid Leukaemia M1 FAB subtype (WHO 2008) and he started the first course of induction therapy with Cytarabine 5 days and Anthracycline 2 days – interrupted due to severe aplasia (the calculated total dose of anthracycline used for treating the osteosarcoma – 360mg – permitted us to further administer anthracycline this time as well).
The bone marrow aspirate performed on day 21st revealed a percentage of blasts of 4%, this being interpreted as complete remission.
Next, the patient underwent a first consolidation course of chemotherapy with high dose Cytarabine
followed by a severe postchemotherapy aplasia. The bone marrow aspirate performed after this course revealed a percentage of 4% blasts, proving that the patient was in sustained complete remission.
By this time, he was proposed for an allogeneic stem cell transplant with a non-sibling donor, and the search for a compatible donor begun.
Meanwhile, he performed another 2 consolidation courses of chemotherapy; in this time a compatible donor was found and the allogeneic stem cell transplant was planned.
The bone marrow examination performed prior to the stem cell transplant showed a percentage of 2% blasts, emphasizing once again sustained complete remission.
In June 2015 the patient underwent an allogeneic stem cell transplant, which was well tolerated, and no major complications occurred following the stem cell transplant. Currently, we are waiting for the 90 day chimerism evaluation of the bone marrow in order to assess the procedure’s success.
DiscussionIt is not uncommon for osteosarcoma patients
to develop SMNs. The incidence is higher than the expected rate for benign bone tumors,[5] it is less than the reported incidence for Hodgkin’s disease (9.7%) and retinoblastoma patients (30%). [6] The majority of SMNs in OS reported in literature are solid tumours of various organs or tissues.[7] It has been shown that the presence of p53 mutations in OS patients increases the incidence of nontherapy-related synchronous or metachronous SMNs.[8] Our patient had no family history of malignancy. The occurrence of sAML in OS is a rare complication. Very few cases have been reported either as part of large series of SMNs in OS [6] or as individual case reports.[5] The median time to develop SMNs after OS varies from 5.5 years to 7.6 years.[6] sAML developing after alkylating agents usually determines myelodysplasia, long latency period and monosomy 5 or 7 with AML (FAB type M1 or M2). Our patient was diagnosed with AML at 2 years from the end of the treatment for OS. sAML after topoisomerase II inhibitors have shorter latent time, FAB M4-M5 type and have translocation involving the MLL gene at chromosome band 11q23. The common topoisomerase II inhibitors are epipodophyllotoxins (etoposide, tenoposide) and anthracyclines (adriamycin, mitoxantrone). In this case the patient received treatment for OS with anthracycline based chemotherapy. No abnormality regarding the MLL gene was discovered. The reported minimum time to develop sAML was generally more than 1 year. However, Escudero et al,[9] reported that one of their case developed sAML after 7 months while our case developed sAML after 2 years. A majority of the reported cases of sAML after topoisomerase II inhibitors are due to etoposide.[10] The incidence of sAML in patients who received anthracyclins for the treatment of their primary tumours is not well known. In the series from Bacci et al.,[5] of the 35 patients who received only anthracyclines, none developed sAML. The common drugs used for chemotherapy in OS are adriamycin, cisplatin and high-dose methotrexate, but ifosfamide, vincristine, bleomycin and carboplatin are also used. These chemotherapeutic drugs are not attributed to sAML commonly. Cisplatin has been reported for sAML
Fig.1. Cytogenetics revealing abnormal cariotype – 91, XXY
XIX, Vol.19, Number 4/2015 151
after germ cell tumours in young patients,[11] but not after OS treatment. It has been postulated that sAML in OS patients could be a synergistic effect of anthracyclins and cisplatin, which could be the likely cause in our case.[11] Our patient received chemotherapy containing both anthracycline and cisplatin.
Pyatt et al,[7] found no consistent relation between age at which chemotherapy was administered and development of sAML, and concluded that younger age was not a risk factor for the development of sAML. The time interval between completion of chemotherapy for the primary tumor and development of sAML depends on the type of chemotherapy used. Escudero et al,[3] reported a case of sAML after treatment for OS, who developed myelodysplastic syndrome 9 months after completion of chemotherapy for OS and evolved into sAML after 14 months. He also had deletion of long arm of chromosome 7. Because that patient had a short latency period and had only one dose of ifosphamide, the authors could not confirm the offending drug as alkylating agent.
Kawai et al.,[12] while presenting two cases of sAML after OS treatment, compiled a series of 16 cases of acute leukaemia following treatment for primary OS. In that series, there were only 10 confirmed cases of sAML. Three had prior myelodysplastic syndrome, of which two developed sAML. The most consistent cytogenetic abnormality was t(8q;21q), which was seen in five patients. Our patient had a complex cariotype, 91, XXY. The prognosis of the patients with sAML is generally considered poor compared to de novo AML.[13] Review of SEER data showed 5-year survival in sAML as 23.7%.[14] However, some authors have refuted this and reported that survival could be equal to de novo AML, depending on the karyotyping abnormality.[15] Despite the poor prognostic factor given by abnormal cytogenetics our patient achieved complete remission after the first induction phase, sustained remission throughout the treatment and is currently in complete remission after the allogeneic stem cell transplant.
ConclusionsConsidering the prior treatment for osteosarcoma
consisting in radiotherapy and chemotherapy we identified a secondary Acute Myeloid Leukaemia, this representing a major negative prognostic factor, along with the cytogenetic abnormalities found (hyperploidy). These factors strongly indicate that the first complete remission should be consolidated by an allogeneic stem cell transplant.
The particularities of this case are the association of two malignancies in a young patient, the presence of an abnormal karyotype (hyperploid), and also a good response to the induction therapy, this leading to complete remission after the first induction course, and of course, sustaining that response.
Acknowledgements: This paper is partly supported by the Sectorial Operational Programme Human Resources Development (SOPHRD), financed by the European Social Fund and Romanian Government under the contract number POSDRU 141531.
References1. Bielorai B, Meyer C, Trakhtenbrot L, et al.
Therapy-related acute myeloid leukemia with t(2;11)
(q37;q23) after treatment for osteosarcoma. Cancer Genet Cytogenet. 2010 Dec;203(2):288-91.
2. Pratt CB, Meyer WH, Luo X, et al. Second malignant neoplasms occuring in survivors of osteosarcoma. Cancer. 1997;80:960–5.
3. Escudero MC, Lassaletta A, Sevilla J, et al. Chemotherapy-related secondary acute myeloid leukemia in patients diagnosed with osteosarcoma. J Pediatr Hematol Oncol. 2004;26:454–6.
4. Mittal R, Ramaswamy NV, Pandita R, Al Bahar S, Khalifa N, Omar S. Secondary acute myeloid leukemia after successful treatment for osteosarcoma. Indian J Med Paediatr Oncol. 2010 Jan;31(1):33-5.
5. Bacci G, Ferrari C, Longhi A, Ferrari S, Forni C, Bacchini P, et al. Second malignant neoplasm in patients with osteosarcoma of the extremities treated with adjuvant and neoadjuvant chemotherapy. J Pediatr Hematol Oncol. 2006;28:774–80.
6. Draper GJ, Sanders BM, Kingston JE. Second primary neoplasms in patients with retinoblastoma. Br J Cancer. 1986;53:661–71.
7. Pratt CB, Meyer WH, Luo X, Cain AM, Kaste SC, Pappo AS, et al. Second malignant neoplasms occuring in survivors of osteosarcoma. Cancer. 1997;80:960–5.
8. Panizo C, Patiño A, Calasanz MJ, Rifón J, Sierrasesumaga L, Rocha E. Emergence of secondary acute leukemia in a patient treated for osteosarcoma: Implications of germline TP53 mutations. Med Pediatr Oncol. 1998;30:165–9.
9. Escudero MC, Lassaletta A, Sevilla J, Fernandez-Plaza S, Pérez A, Diaz MA, et al. Chemotherapy-related secondary acute myeloid leukemia in patients diagnosed with osteosarcoma. J Pediatr Hematol Oncol. 2004;26:454–6.
10. Felix CA. Secondary leukemias induced by topoisomerase-targeted drugs. Biochim Biophys Acta. 1998;1400:233–55.
11. Schneider DT, Hilgenfeld E, Schwabe D, Behnisch W, Zoubek A, Wessalowski R, et al. Acute myelogenous leukemia after treatment for malignant germ cell tumors in children. J Clin Oncol. 1999;17:3226–33.
12. Kawai A, Sugihara S, Naito N, Ozaki T, Isu K, Hatae Y, et al. Development of acute myeloid leukemia after chemotherapy for osteosarcoma. Clin Orthop Relat Res. 2001;391:239–46.
13. Rakesh Mittal, N. V. Ramaswamy,1 R. Pandita,1 S. Al Bahar,1 N. Khalifa, and S. Omar, Secondary acute myeloid leukemia after successful treatment for osteosarcoma Indian J Med Paediatr Oncol. 2010 Jan-Mar; 31(1): 33–35.
14. Hijiya N, Ness KK, Ribeiro RC, Hudson MM. Acute leukemia as a secondary malignancy in children and adolescents: Current findings and issues. Cancer. 2009;115:23–35.
15. Schoch C, Kern W, Schnittger S, Hiddemann W, Haferlach T. Karyotype is an independent prognostic parameter in therapy-related acute myeloid leukemia (t-AML): An analysis of 93 patients with t-AML in comparison to 1091 patients with de novo AML. Leukemia, 2004;18:120–5.

Therapeutics, Pharmacology and Clinical Toxicology152
Genica Caragea8 Calea Floreasca, 014461 Bucharest, Romaniae-mail: [email protected]
Abstract. Acute poisoning with organophosphoric compounds (OP) still remains an issue for the doctors, due to its’ high prevalence and sternness, many cases evolving to death. This occurs because the organophosphoric compounds are frequently used as insecticides in agriculture and in the household. They are extremely toxic and one of the most frequent types of contamination is through the lung, by inhalation of substances. More often the organophosphoric compound is not so poisonous for humans thant a metabolite of the compound. The diagnosis of poisoning is established based on two components: the clinical and analytical diagnostic. Clinical diagnostic refers to the clinical symptoms; it is called the cholinergic toxidrome. The analytical diagnostic concerns, on one hand, the level of pseudo cholinesterase and, on the anther hand, the identification of the organophosphoric compound. In the last years, great progress has been achieved in order to identify these compounds and their metabolites. The biological monitoring of pesticides is performed using Gas Chromatography coupled with Mass Spectrometry (GC-MS).
Key words: OP compounds, GC-MS, cholinesterase
1 Clinical Emergency Hospital Bucharest2 Scientific Research Center for Military Health 3 University of Medicine and Pharmacy “Carol Davila” Bucharest4 University “Politehnica” Bucharest
Dumitraşcu Monica1, Macovei R.A.1,3, Caragea Genica1,2, Avram Ruxandra1, Ionică M.2,4
INTOXICATION WITH DIAZINON
CASE REPORTTherapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 152 - 155© Copyright reserved 2015
Introduction
Organophosphorus compounds (OP) are a group of chemical substances widely used
in industrial and domestic surroundings. They exert their main toxicological effects trough irreversible inactivation of esterases in the central nervous system. As a result, Ach accumulates in the synaptic cleft, causing overstimulation of the cholinergic receptors and consequently impending neurotransmission (Bouchard M., 2006). Human exposure to OP occurs through multiple routes: dermal, oral or by inhalation.
To obtain an indication of the exposure, we can measure the compounds or their metabolites in blood or urine (Gil F. & Pla A., 2001).
The first synthesized products had increased potency, being extremely toxic to both humans and animals. That is why researchers sought to synthesize less toxic compounds. Hence new compounds were integrated, but their efficiency decreased in time due to the fact that insects developed resistance to them (Tudosie M.S., et all, 2014). However, these insecticides have remained extremely toxic to humans. Sometimes, not the mere compound but its metabolites prove to
be more toxic (Voicu V., et al. 1998). For example, tiono pesticides do not have an important effect on cholinesterase, but, through metabolism, under the action of P450 cytochrome, they become phosphate compounds, which are strong cholinesterase inhibitors. In the case of accidental exposure to pesticides, it is useful to identify the compound and its metabolites as well as to correctly assess the degree of toxicity.
A lot of research has been done to determine whether there is a link between exposure to pesticides and various diseases. One of the methods to determine an exposure to pesticides is to measure the plasmacholin-esterase and the erythrocyte acetylcholinesterase, reflecting the capacity of absorbed organophosphoric compound to inhibit these blood enzymes. However, it is well recognized that this is a relatively insensitive indicator of an absorbed dose of OP compound, (Rei S.J. & Watts R.R., 1981; Nutley B.P. & Cocker J., 1993; Hardt J. & Angerer J. 2000 , Cocker J., et all, 2002 ). Blood cholinesterase activity needs at least 15% depression from an individual’s normal level of plasma or erythrocyte enzyme activity to be considered indicative of pesticide over-exposure. In addition, the collection of blood samples is sometimes considered as invasive (Cocker J., et al 2002).
The measurement of urinary biomarkers of organophosphoric exposure is of special interest, being non-invasive and highly sensitive. Experimental studies

XIX, Vol.19, Number 4/2015 153
in volunteers, indicate that within a few hours following exposure to organophosphoric compound, whatever the route-of-entry, organophosphoric metabolites became easily measurable in urine, even at absorbed doses well below those necessary to induce any sign of toxic effects (Morgan D.P., et all, 1977; Richter E.D., et all, 1992; Carrier G. & Burnet R.C., 1999, Bouchard M., et all, 2003, 2006). The laboratory methods used to assess OP compounds are based on gas chromatography (GC), coupled with mass spectrometry (MS), (GC-MS). Biological monitoring through these methods is a useful tool in establishing the presence and magnitude of exposures.
At present, there are is a significant number of OP compounds, for which exposures need to be assessed. Moreover, the contamination of small children, in whose case biological samples are more difficult to collect, is becoming increasingly problematic nowadays. Hence the need to develop new methods that may enable the collection of maximum amount of information from a limited amount of urine, this being the main biological product used for the biological monitoring of chemical substances such as pesticides (Barr D.B., et all, 2006).
Many currently used methods, described by scientific literature focus on the determination of certain pesticides and their metabolites. Over the past few years, GC methods which identify a higher number of markers belonging to more classes of compounds and requiring smaller amounts of urine, have been developed. These methods are of interest to epidemiological studies because they could help identify an increasing number of pesticides people are exposed to, and provide a statistical interpretation of the exposure effects on the population’s health.
New methods for pesticide detection, using HPLC-MS or GC-MS, with quantification using isotope dilution like the multiclass method, the dialkilphosphat method and the phenols method are currently being developed (Barr D.B., et all, 2006).
Recent studies concluded that the development of multi residue methodologies, which may screen simultaneously an increased number of different classes of pesticides is of great value for monitoring the population’s exposure to pesticides. Moreover, a trend in the development of such methodologies during the last couple of years can be observed.GC-MS methodOperational parameters for GC
• Injector temperature - 300°C• Interface GC-MS temperature - 260°C• Carriere gaz - He• Column flow - 1.2 ml/min • GC Column - DB5 MS (30m X 0.25 mm X 0.254
μm)The GC oven temperature program is shown in Table I.
• Manifold temperature - 80°C• Ion trap temperature - 170°C• Ionisation current – 10 μA• Acceleration voltage – 70 eV• Mass range 50 – 450 amuț
Analytical determinations Confirmation of the compounds’ identity of the is based on comparing the mass spectrum and the abundance of reference ions of each identified analyte in the sample, with those of standards, using a library of spectra. For spectroscopic identification the mass spectra library Pfleger Maurer was used Weber (PMW), a library specialized for the toxicological compounds and their metabolites. Also, other libraries were used: NIST2000 and Wiley6, both for confirmation of obtained mass spectra using PMW library, and for identification of some compounds that had no spectrum in the PMW library.
The organophosphorus compounds are extracted from urine using liquid-liquid method, with a synergist mixture of dichlormethane: dichlorethane: chlorophorm 1:1:1 v/v and a phosphate buffer.
The quality control of this method is performed by adding an internal standard, midazolam
The extract purification is carried out by centrifugation 1o min. to 2500rot/min. and is followed by sample concentration to 1000C. The residue is taken up in the mixture of three solvents 500ul
In the GC-MS system, it is inject 1μ from the analyte.
Case report Male patient, 51 years, presenting: nausea, vomiting,
salivation, headache, abdominal cramps, after accidental ingestion of a small amount of an unknown substance, two hours earlier. The patient is admitted in ATI II Toxicology Department
His breathing and cardiac functions were normal, SpO2 = 97%, without O2 supplement, PA = 125/75 mmHg, HR = 66 - 76/min. He had mitotic pupils. Upon investigating about the ingestion, he told the medical team , that three days earlier his wife had made a pest control of the house and she asked the company responsible for this to hand her the small bottle of insecticide. We had the suspicion that insecticide could probably be an organophosphoric compound. We determined the pseudo cholinesterase which turned out with a light decreased value, at 3000 u/l. The reference level for male at this laboratory is between 4000 and 12600 u/l. We collected 50 ml urine sample for GC-MS method.
Figure 2. presents the ion chromatography, the mass spectra of diazinon and its metabolite, hidroxidiazinone, obtained from a urine sample taken from the pacient N.G.
Diazinon is a thiophosphoric type of insecticide. It was synthesized to replace another compound – DDT. Diazinon metabolism is accomplished by oxidation dixozon, much more aggressive than initial insecticides. Because it is a fat-soluble compound, his toxicity manifests over 24 hours from exposure (depending on the amount of poison), by mobilization of fat tissue.
In the first 24 hours, the therapy required gastric
Temperature (°C) Rate (°C/min)
Waiting time (min)
140 0.00 1250 5.00 17.00
Table I. The GC oven temperature program
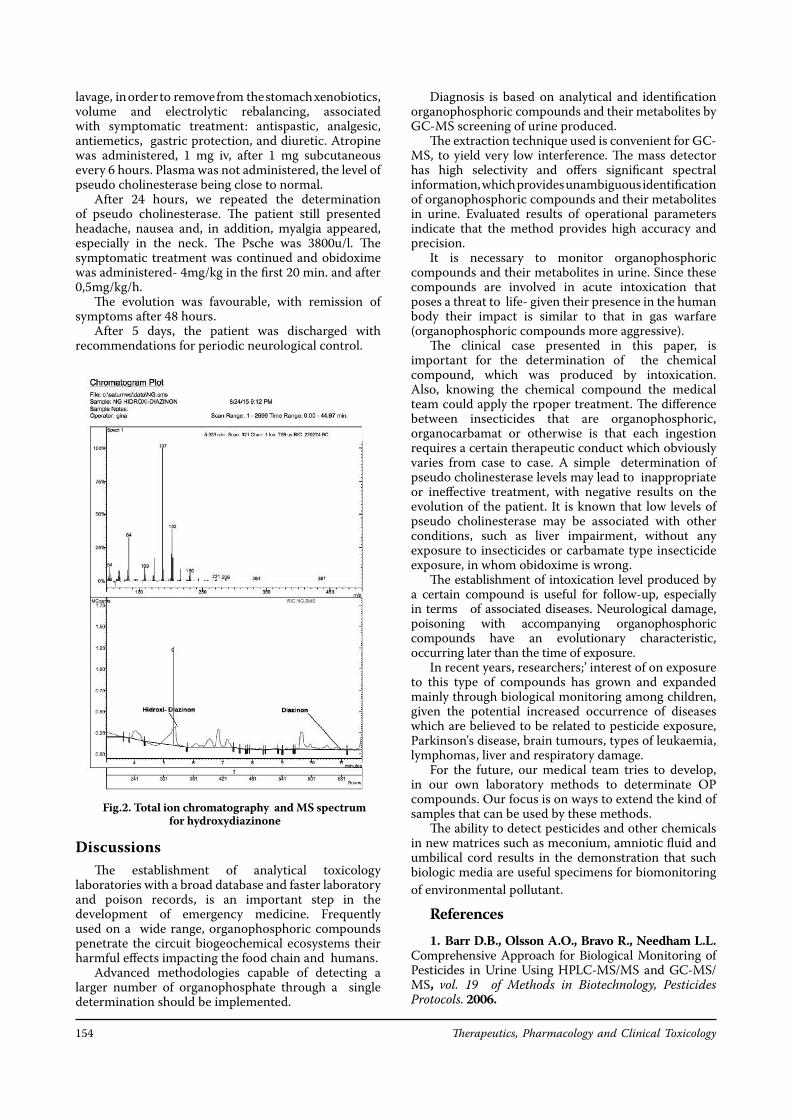
Therapeutics, Pharmacology and Clinical Toxicology154
lavage, in order to remove from the stomach xenobiotics, volume and electrolytic rebalancing, associated with symptomatic treatment: antispastic, analgesic, antiemetics, gastric protection, and diuretic. Atropine was administered, 1 mg iv, after 1 mg subcutaneous every 6 hours. Plasma was not administered, the level of pseudo cholinesterase being close to normal.
After 24 hours, we repeated the determination of pseudo cholinesterase. The patient still presented headache, nausea and, in addition, myalgia appeared, especially in the neck. The Psche was 3800u/l. The symptomatic treatment was continued and obidoxime was administered- 4mg/kg in the first 20 min. and after 0,5mg/kg/h.
The evolution was favourable, with remission of symptoms after 48 hours.
After 5 days, the patient was discharged with recommendations for periodic neurological control.
DiscussionsThe establishment of analytical toxicology
laboratories with a broad database and faster laboratory and poison records, is an important step in the development of emergency medicine. Frequently used on a wide range, organophosphoric compounds penetrate the circuit biogeochemical ecosystems their harmful effects impacting the food chain and humans.
Advanced methodologies capable of detecting a larger number of organophosphate through a single determination should be implemented.
Diagnosis is based on analytical and identification organophosphoric compounds and their metabolites by GC-MS screening of urine produced.
The extraction technique used is convenient for GC-MS, to yield very low interference. The mass detector has high selectivity and offers significant spectral information, which provides unambiguous identification of organophosphoric compounds and their metabolites in urine. Evaluated results of operational parameters indicate that the method provides high accuracy and precision.
It is necessary to monitor organophosphoric compounds and their metabolites in urine. Since these compounds are involved in acute intoxication that poses a threat to life- given their presence in the human body their impact is similar to that in gas warfare (organophosphoric compounds more aggressive).
The clinical case presented in this paper, is important for the determination of the chemical compound, which was produced by intoxication. Also, knowing the chemical compound the medical team could apply the rpoper treatment. The difference between insecticides that are organophosphoric, organocarbamat or otherwise is that each ingestion requires a certain therapeutic conduct which obviously varies from case to case. A simple determination of pseudo cholinesterase levels may lead to inappropriate or ineffective treatment, with negative results on the evolution of the patient. It is known that low levels of pseudo cholinesterase may be associated with other conditions, such as liver impairment, without any exposure to insecticides or carbamate type insecticide exposure, in whom obidoxime is wrong.
The establishment of intoxication level produced by a certain compound is useful for follow-up, especially in terms of associated diseases. Neurological damage, poisoning with accompanying organophosphoric compounds have an evolutionary characteristic, occurring later than the time of exposure.
In recent years, researchers;’ interest of on exposure to this type of compounds has grown and expanded mainly through biological monitoring among children, given the potential increased occurrence of diseases which are believed to be related to pesticide exposure, Parkinson's disease, brain tumours, types of leukaemia, lymphomas, liver and respiratory damage.
For the future, our medical team tries to develop, in our own laboratory methods to determinate OP compounds. Our focus is on ways to extend the kind of samples that can be used by these methods.
The ability to detect pesticides and other chemicals in new matrices such as meconium, amniotic fluid and umbilical cord results in the demonstration that such biologic media are useful specimens for biomonitoring of environmental pollutant.
References1. Barr D.B., Olsson A.O., Bravo R., Needham L.L.
Comprehensive Approach for Biological Monitoring of Pesticides in Urine Using HPLC-MS/MS and GC-MS/MS, vol. 19 of Methods in Biotechnology, Pesticides Protocols. 2006.
Fig.2. Total ion chromatography and MS spectrum for hydroxydiazinone

XIX, Vol.19, Number 4/2015 155
2. Bouchard M., Carrier G., Brunet R.C. Determination of biological reference values for chlorpyrifos metabolites in human urine using a toxicokinetic model. J Occup Environ Health, 2005, 2.
3. Bouchard M., Carrier G., Brunet R.C., Dumas P., Noisel N. Biological monitoring of exposure to organophosphoric insecticides in a group of horticultural greenhouse workers, Public Health Journal, march, 2006.
4. Bravo R., Caltabiano L.M., Weerasekera G., Whitehead R.D., Fernandez C., Needham L.L., Bradman A., Barr D.B. Measurement of dialkyl phosphate metabolites of organophosphoric pesticides in human urine using lyophilization with gas chromatography- tandem mass spectrometry and isotope dilution quantification. J of Exposure and Environmental Epidemilogy, 2004, 14, 249-259.
5. Bravo R., Driskell W.J., Whitehead R.D., Needham L.L., Barr D.B.. Quantification of dialkyl phosphate metabolites of organophosphate pesticides in human urine using GC-MS/MS with isotope dilution method. J Anal Toxicol 2002; 26: 245-252.
6. Carrier G., Burnet R.C. A toxicokinetic model to assess the risk of azimphosmethyl exposure in humans through measures of urinary elimination of alkylphosphates. Toxicol Sci, 1999, 47.
7. Cocker J., Mason H.J., Garfitt S.J., Jones K., Biological monitoring of exposure to organophosphate pesticides, Article published in Toxicology Letters, September 2002.
8. Gil F., Pla A., Biomarkers as biological indicators of xenobiotic exposure. J Appl Toxicol, 2001, 21.
9. Hardt J., Angerer J. Determination of dialkyl phosphates in human urine using gas chromatography-mass spectrometry. J Anal Toxicol. 2000; 24: 678-684.
10. Jaga K., Dharmani C. Sources of exposure to and public health implications of organophosphate pesticides, Rev. Panam. Salud Publica, vol. 14, n. 3, Washington, Sep. 2003.
11. Koureas M., Tsakalof A., Tsatsakis A., Hadjichristodoulou G. Systematic review of biomonitoring studies to determine the association between exposure to organophosphoric and pyrethroid insecticides and human health outcomes. Toxicology Letters, 2012.
12. Margariti M.G., Tsakalof A.K., Tsatsakis A.M. Analytical Methods of Biological Monitoring for Exposure to Pesticides: Recent Update, The Drug Monit. Vol 29, april 2007.
13. Morgan D.P., Hetzler H.L., Slach E.F. Urinary excretion of paranitrophenol and alkyl phosphates following ingestion of methyl and ethyl parathion by human subjects. Arch Environ Contam Toxico, 1977, l; 6.
14. Nutley B.P, Cocker J. Biological monitoring of workers occupationally exposed to organophosphoric pesticides. Pesticide Science, 1993, 38, 315-322.
15. Rei S.J., Watts R.R. A method for determination of dialkyl phosphate residues in urine. J Anal Toxicol 1981; 15: 126-132.
16. Richter E.D., Chuwers P., Levy Y. Health effects from exposure to organophosphate pesticides in workers and residents in Israel. Isr J Med Sci, 1992. 28.
17. Tudosie M.S., Macovei R.A., Ionică M. Intoxicaţia acută cu compuşi organofosforici, corelaţii toxicocinetice şi toxicodinamice, Ed Univ “Carol Davila” Bucureşti, 2014.
18. Voicu V., Macovei R., Miclea L. Ghid de toxicologie clinic, Editura Amaltea, Bucureşti 1998.
19. Wessels D., Barr D.B., Mendola P. Use of Biomarkers to Indicate Exposure of Children to Organophosphate pesticides: Implications of a Longitudinal Study of Children s Environmental Health. Environmental Health Perspectives, vol111, number 16, dec. 2003.
***. From the Centers for Diseas Control and Prevention. Illnesses associated with occupational use of fleacontrol products, Califosnia, Texas and Washington, 1989-1997, JAMA 1999, 282.
Therapeutics, Pharmacology and Clinical Toxicology156
Felicia Galoș20 Constantin Brâncoveanu Blvd, 4th District, Bucharest, Romaniae-mail: [email protected]
Abstract. The correct diagnosis and effective treatment of Helicobacter pylori (H pylori) gastric infection are essential in controlling this condition. The methods available have both advantages and limitations related to factors such as the level of technical difficulty, costs and extensive accessibility in hospitals. Bacterial culture from the gastric biopsy is the gold standard technique and recommended for antibiotic susceptibility tests. Many patients investigated for H. Pylori infection have been taking antibiotics or following a non steroidal anti-inflammatory treatment beforehand. These factors influenced the culture. We present the case of a 15-year -old girl with continuous pain in the upper abdomen that woke her in the early hours of the morning for several months, and nausea. She also has a psychiatric condition, having attempted suicide repeatedly. This case report presents some of the most relevant diagnostic methods for H pylori infection, as well as the influences from previously followed treatments, environmental factors (i.e. smoking) and conditions which influenced the grows colonies. In the case of a negative culture and in the absence of response to the empirical therapy based on current antibiotics (amoxicillin, clarithromycin, metronidazole), we consider it is useful to use other methods when it comes to detecting the primary antibiotic resistance.
Keywords: Helicobacter pylori culture, antibiotic resistance
1 Marie Curie Children’s Emergency Hospital Bucharest2 University of Medicine and Pharmacy Carol Davila Bucharest
Năstase Gabriela1, Anghel Mălina1, Galoș Felicia1,2, Stoicescu M.1,2, Munteanu M.1, Bălgrădean Mihaela1,2
CORRELATION OF HISTOLOGICAL FINDINGS WITH BACTERIAL CULTURE IN CHILDREN WITH HELICOBACTER PYLORI GASTRITIS
Therapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 156 - 158© Copyright reserved 2015
Introduction
The correct diagnosis and effective treatment of H pylori gastric infection are essential in
controlling this entity, characterized by a high rate of prevalence worldwide and linked with chronic gastritis, gastric atrophy and cancer.[1] The methods available have both advantages and limitations related to factors such as the level of technical difficulty, costs and extensive accessibility in hospitals. The bacterial culture from the gastric biopsy is the gold standard technique and recommended for antibiotic susceptibility tests. The sensitivity of bacteria isolation has been reported to vary greatly among laboratories because it is very fastidious in nature. Even the experienced laboratories recover the organism from only 50 to 70% of infected biopsies.[2]
AimThe purpose of this case report is to underline the
difficulties in the realization of the H pylori culture, the factors that influenced the culture and to present some of the most relevant diagnostic methods of H pylori infection.
Case reportWe aim to analyze the case of a 15-year- old girl
with nagging pain in the upper abdomen that often woke her in the early hours of the morning, for one month. Nausea is also mentioned, on average of 2-3 episodes/week. The patient suffered from chronic gastritis and was H pylori positive 6 months previous to this hospitalization. She was treated before with sequential therapy: an esomeprazole plus amoxicillin 1g, both given twice daily for the first 5 days, followed by triple therapy- esomeprazole, clarithromycin 500mg and metronidazole, all given twice daily, for another 5 days. No other check-up followed after the previous hospital discharge. For a few months the patient was asymptomatic. In terms of family history, no sign of gastric suffering was reported. She also presented with
CASE REPORT

XIX, Vol.19, Number 4/2015 157
psychiatric condition, with repeated suicide attempts. She denies taking any drugs that could explain the occurrence of symptoms and does not remember of any recent imfection.
The clinical exam shows an adolescent with a normal condition, no fever, good nutritional status: weight 46 kg (10-25ºP), height 157 cm (10-25ºP). Scars post-cuts on her forearms. Stethacoustic pulmonary physiologic vesicular murmur, without rales. Cardiac normal relations. Clear pharynx. Lean abdomen, sensitivity on palpation in the upper abdomen. Normal stool. Spontaneous urination, normal macroscopic aspect of urine. Clear sensor, tonus, normal reactions.
H pylori antigen in stool specimen was positive as well serology. On endoscopy, antral nodularity was found. Rapid urease test was positive and H pylori culture of gastric biopsy (antrum) was negative. The organism was found in the histological section beside the mononuclear infiltration.
We prescribed her a rescue eradication regimen for H pylori with IPP, Tinidazole and Levofloxacin, as antibiotic resistance in our geographic area continues to be a rather challenging issue Several recommendations were made as to the hygienic and dietetic treatment (avoiding smoking). Treatment compliance plays a major role in predicting therapeutic outcome. A follow-up was scheduled at two months after her demission
Discussions
The Maastricht Consensus Report[3] recommends H pylori culture for performing antibiotic susceptibility testing if primary resistance to Clarithromycin is higher than 20% or after failure of second line – therapy. As the prevalence of antibiotic resistance increases globally, there is a strong argument for performing culture and sensitivity testing after the first treatment failure (to prevent emergence of double resistance to Clarithromycin and Metronidazole) and certainly after the second; indeed, some would argue that it should be performed at the initial diagnosis in areas of high resistance prevalence.[4] Despite its long use, culture remains a challenge because of the fastidious nature of the bacterium, with particular growth requirements regarding environment and atmosphere[5]. Altering the pH, the proton pump inhibitors (PPIs) indirectly interfere with H pylori distribution in the stomach. The antral part has been found to be the most affected part of the stomach by PPIs as H pylori almost disappears from this niche. To avoid false negative results, it is recommended not to consume these drugs 2 weeks prior to endoscopy.[6] Smoking has been identified by several studies to be an important factor associated with treatment failure.[7] In our case, the adolescent denied the use of IPPs and antibiotics before being accepted to the hospital. She also denied smoking, but the information which she offered us may not be true. It has been established that H pylori has patchy distribution in the stomach. It has also been discocvered that the corpus may be the only site which remains positive despite the consumption of antisecretory drugs. In our case we took two biopsies from the antrum for H pylori culture (Figure 1). This could be adjusted by taking another one/two samples from the gastric body as well,
in an attempt to improve the culture success rate.We prescribed pr patient a rescue eradication
regimen with IPP, Tinidazole and Levofloxacin, because we had scarce information on antibiotic resistance in our geographical area. In particular, primary Clarithromycin resistance is regarded as the main factor that affects the treatment’s efficacy, reducing the success rate of standard triple therapies to mean values of 18-44%.[8] However considering the difficulty of H pylori culture development, this technique could be completed by molecular methods (as FISH or PCR from biopsies) which do not require strict conditions of biopsy specimen transport and can be used to detect the point mutation associated with the Clarithromycin resistance, the main antibiotic responsible for decreasing the eradication rate.[9]
Conclusions
Several factors have been found to affect the efficacy of therapies: bacterial resistance to antibiotics, compliance to therapy, bacterial load in the stomach, smoking. In the case of a negative culture and in the absence of response to the empirical therapy based on current antibiotics (Amoxicillin, Clarithromycin, Metronidazole), we consider it useful to use other methods when it comes to detecting the primary resistance of antibiotics(genotypic analysis).
References1. Arismendi-Morillo G, Hernandez I, Mengual E
et al. Comparison of three methods based on endoscopic gastric biopsies for diagnosis of Helicobacter pylori active infection in a clinical setting. Arq Gastroenterol 2011;48(3):190-194.
2. Saurabh KP, Chandra BP, Ashok KJ et al. Diagnosis of Helicobacter pylori: What should be the gold standard? Word J Gastroenterol 2014;20(36):12847-12859.
3. Malfertheiner P, Megraud F, O’Morain CA et all. Management of Helicobacter pylori infection – The Maastricht IV/ Florence Consensus Report. Gut 2012;61:646-664.
4. Holton J, Figura N, Vaira B. Helicobacter pylori. An atlas of investigation and management. Clinical Publishing Oxford 2012.
5. Lopes AI, Vale FF, Oleastro M. Helicobacter pylori infection – recent developments in diagnosis. Word J Gastroenterol 2014:20(28):9299-9313.
Fig.1. Gastric Biopsy - Giemsa stain

Therapeutics, Pharmacology and Clinical Toxicology158
6. Patel SK, Pratap CB, Jain AK et al. Diagnosis of Helicobacter pylori: What should be the gold standard? Word J Gastroenterol 2014:20(36):12847-12859.
7. Janssen MRJ, Laheij RJF, Janse JBMJ. The influence of pretreatment on cure rates of Helicobacter pylori eradication. The Journal of Medicine 2004;62(4):192-196.
8. Saracino IM, Zullo A, Holton J et al. High Prevalence of Primary Antibiotic Resistance in Helicobacter pylori Isolates in Italy. J Gastrointestin Liver Dis December 2012;21(4):363-365.
9. Manfredi M, Gismondi P, Maffini V et al. Primary antimicrobial susceptibility changes in children with Helicobacter pylori infection over 13 years in northern Italy. Gastroenterology Research and Practice 2015.

XIX, Vol.19, Number 4/2015 159
Luminita Stanciulescu8 Calea Floreasca, 014461 Bucharest, Romaniae-mail: [email protected]
Abstract. Even if, ileal carcinoid tumours have a low incidence (0.2-0.8/100000), the diagnosis must be considered in the presence of hepatic metastasis of unknown origin. We report a case of 55 years old female that presents persistent nausea, for one year prior to admission. She was suspected of gallbladder stones and an abdominal ultrasound was performed. The result was normal and the patient presented to our clinic for a routine check-up. At the repeated ultrasound we found multiple focal hyperechoic liver lesions of maximum 10 mm. She was referred immediately for a CT-scan with intravenous contrast but the result was surprisingly normal. We insisted in our investigation and the patient was sent for a total abdominal MRI. The result revealed ileal tumour of 2 cm with liver metastases. Palliative surgery with resection of ileal tumour and liver metastasis biopsy is performed. The pathology result was compatible with neuroendocrine tumor G1(Ki 67 index 1-2%) with liver metastasis.
Keywords: neuroendocrine tumor, liver metastasis, nausea, Ki 67 index
1 UMF Carol Davila, Bucharest2 Bucharest Emergency Hospital
* all authors equally contributed to this work
Ilie Mădălina1,2*, Turculeţ C.1,2*, Diaconu Camelia1,2*, Tincu R.1,2*, Constantinescu G.1,2*, Stănciulescu Luminiţa1,2*, Macovei R.1,2*, Enache V.1,2*, Popa B.1,2*, Ene D.1,2*
AN ATYPICAL CAUSE OF NAUSEA
Therapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 159 - 162© Copyright reserved 2015
Introduction
The term carcinoid was introduced by Oberndorfer in 1907 in his description of a class
of malignant tumours that behaved less aggressively than the more common adenocarcinomas of the gastrointestinal tract [1]. An early diagnosis is often delayed by a few years because most small intestinal carcinoids are small, initially asymptomatic, or misdiagnosed as irritable bowel syndrome. The most frequent presentations are abdominal pain (16% to 41%) and episodic small bowel obstruction (24% to 41%), which are usually of long duration. A classic carcinoid syndrome is relatively uncommon (10% to 15%), typically consisting of diarrhoea, coetaneous flushing, bronchoconstriction and right-sided heart failure. The article emphasises the case of a patient with a single symptom at presentation - nausea subsequently was discovered with liver metastasis after an MRI, misdiagnosed even after a CT scan.
Patient, methods and result A 55 years old female presented at the emergency
room with persistent nausea, for one year prior to admission. She denied vomiting, weight loss, modifications in the stool pattern, fever or headache. She was non-smoker and didn’t consume alcohol. The usual
blood tests were normal (no anaemia, no inflammatory syndrome). She was suspected of gallbladder stones hence an abdominal ultrasound was performed. The result was normal hence shewas sent home. Due to the persistence and discomfort of symptoms, the patient presented to our clinic for an accurate diagnosis.
At the repeated ultrasound multiple focal hyperechoic liver lesions of maximum 10 mm were detected. A CT-scan with intravenous contrast is performed but the result is surprisingly normal. We mistrusted the CT result and sent the patient for a total abdominal MRI.
The result revealed: ileal tumour of 2 cm with liver metastases.
CASE REPORT
Fig.1. Resected specimen

Therapeutics, Pharmacology and Clinical Toxicology160
A total colonoscopy with also viewing of the last 50 cm of terminal ileum was done but no lesions were found. Upper GI endoscopy was also normal. Cardiac ultrasound excluded valve disease or right heart failure.
Biochemical markers showed highly elevated values of serotonin 1200 ng/ml, with normal 5 HIAA and Chromogranin A.
An intraoperative white-yellow tumour of 2 cm on
Fig.2.CDX2-20x positive diffuse in diffuse in tumoral cells
Fig.3. Chromogranin 20x-positive and in rare neuroendocrine cells
Fig.4. Ki67-positive nuclear in 1-2% of the tumoral cells
Fig.5. Hepatic metastasis of NET
Fig.6. Synaptophysin 4x-positive diffuse in tumoral cells cytoplasm
Fig.7. NET grade 2-intestinal wall with proliferation of tumoral cells
Fig.8.NET grade 2-mucosa without neoplasia, submucosa with proliferation
Fig.9. NET with low mitotic rate
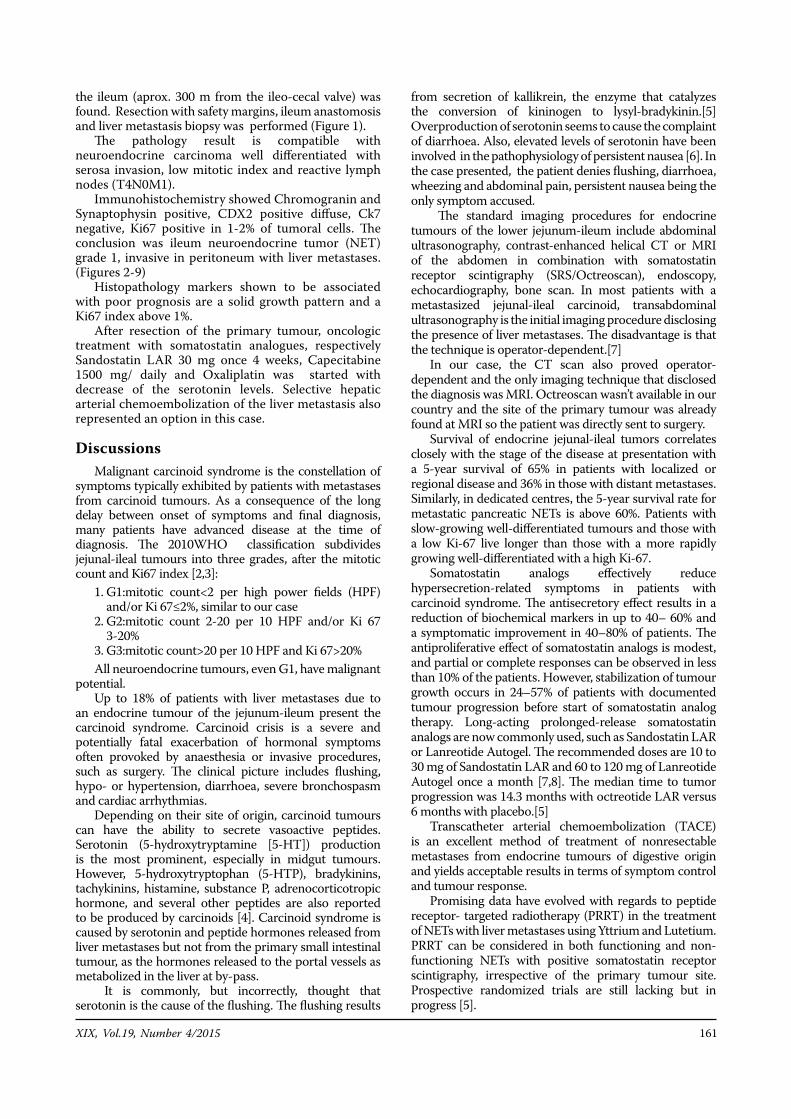
XIX, Vol.19, Number 4/2015 161
the ileum (aprox. 300 m from the ileo-cecal valve) was found. Resection with safety margins, ileum anastomosis and liver metastasis biopsy was performed (Figure 1).
The pathology result is compatible with neuroendocrine carcinoma well differentiated with serosa invasion, low mitotic index and reactive lymph nodes (T4N0M1).
Immunohistochemistry showed Chromogranin and Synaptophysin positive, CDX2 positive diffuse, Ck7 negative, Ki67 positive in 1-2% of tumoral cells. The conclusion was ileum neuroendocrine tumor (NET) grade 1, invasive in peritoneum with liver metastases.(Figures 2-9)
Histopathology markers shown to be associated with poor prognosis are a solid growth pattern and a Ki67 index above 1%.
After resection of the primary tumour, oncologic treatment with somatostatin analogues, respectively Sandostatin LAR 30 mg once 4 weeks, Capecitabine 1500 mg/ daily and Oxaliplatin was started with decrease of the serotonin levels. Selective hepatic arterial chemoembolization of the liver metastasis also represented an option in this case.
DiscussionsMalignant carcinoid syndrome is the constellation of
symptoms typically exhibited by patients with metastases from carcinoid tumours. As a consequence of the long delay between onset of symptoms and final diagnosis, many patients have advanced disease at the time of diagnosis. The 2010WHO classification subdivides jejunal-ileal tumours into three grades, after the mitotic count and Ki67 index [2,3]:
1. G1:mitotic count<2 per high power fields (HPF) and/or Ki 67≤2%, similar to our case
2. G2:mitotic count 2-20 per 10 HPF and/or Ki 67 3-20%
3. G3:mitotic count>20 per 10 HPF and Ki 67>20%All neuroendocrine tumours, even G1, have malignant
potential.Up to 18% of patients with liver metastases due to
an endocrine tumour of the jejunum-ileum present the carcinoid syndrome. Carcinoid crisis is a severe and potentially fatal exacerbation of hormonal symptoms often provoked by anaesthesia or invasive procedures, such as surgery. The clinical picture includes flushing, hypo- or hypertension, diarrhoea, severe bronchospasm and cardiac arrhythmias.
Depending on their site of origin, carcinoid tumours can have the ability to secrete vasoactive peptides. Serotonin (5-hydroxytryptamine [5-HT]) production is the most prominent, especially in midgut tumours. However, 5-hydroxytryptophan (5-HTP), bradykinins, tachykinins, histamine, substance P, adrenocorticotropic hormone, and several other peptides are also reported to be produced by carcinoids [4]. Carcinoid syndrome is caused by serotonin and peptide hormones released from liver metastases but not from the primary small intestinal tumour, as the hormones released to the portal vessels as metabolized in the liver at by-pass.
It is commonly, but incorrectly, thought that serotonin is the cause of the flushing. The flushing results
from secretion of kallikrein, the enzyme that catalyzes the conversion of kininogen to lysyl-bradykinin.[5]Overproduction of serotonin seems to cause the complaint of diarrhoea. Also, elevated levels of serotonin have been involved in the pathophysiology of persistent nausea [6]. In the case presented, the patient denies flushing, diarrhoea, wheezing and abdominal pain, persistent nausea being the only symptom accused.
The standard imaging procedures for endocrine tumours of the lower jejunum-ileum include abdominal ultrasonography, contrast-enhanced helical CT or MRI of the abdomen in combination with somatostatin receptor scintigraphy (SRS/Octreoscan), endoscopy, echocardiography, bone scan. In most patients with a metastasized jejunal-ileal carcinoid, transabdominal ultrasonography is the initial imaging procedure disclosing the presence of liver metastases. The disadvantage is that the technique is operator-dependent.[7]
In our case, the CT scan also proved operator-dependent and the only imaging technique that disclosed the diagnosis was MRI. Octreoscan wasn’t available in our country and the site of the primary tumour was already found at MRI so the patient was directly sent to surgery.
Survival of endocrine jejunal-ileal tumors correlates closely with the stage of the disease at presentation with a 5-year survival of 65% in patients with localized or regional disease and 36% in those with distant metastases. Similarly, in dedicated centres, the 5-year survival rate for metastatic pancreatic NETs is above 60%. Patients with slow-growing well-differentiated tumours and those with a low Ki-67 live longer than those with a more rapidly growing well-differentiated with a high Ki-67.
Somatostatin analogs effectively reduce hypersecretion-related symptoms in patients with carcinoid syndrome. The antisecretory effect results in a reduction of biochemical markers in up to 40– 60% and a symptomatic improvement in 40–80% of patients. The antiproliferative effect of somatostatin analogs is modest, and partial or complete responses can be observed in less than 10% of the patients. However, stabilization of tumour growth occurs in 24–57% of patients with documented tumour progression before start of somatostatin analog therapy. Long-acting prolonged-release somatostatin analogs are now commonly used, such as Sandostatin LAR or Lanreotide Autogel. The recommended doses are 10 to 30 mg of Sandostatin LAR and 60 to 120 mg of Lanreotide Autogel once a month [7,8]. The median time to tumor progression was 14.3 months with octreotide LAR versus 6 months with placebo.[5]
Transcatheter arterial chemoembolization (TACE) is an excellent method of treatment of nonresectable metastases from endocrine tumours of digestive origin and yields acceptable results in terms of symptom control and tumour response.
Promising data have evolved with regards to peptide receptor- targeted radiotherapy (PRRT) in the treatment of NETs with liver metastases using Yttrium and Lutetium. PRRT can be considered in both functioning and non-functioning NETs with positive somatostatin receptor scintigraphy, irrespective of the primary tumour site. Prospective randomized trials are still lacking but in progress [5].

Therapeutics, Pharmacology and Clinical Toxicology162
ConclusionsSmall bowel neuroendocrine tumors are difficult to
diagnose especially if the patient has atypical symptoms. Imaging plays a crucial role in the diagnosis but is operator dependent even after a CT scan. After surgery of the primary tumour, correct immunohistochemistry confirms the neuroendocrine nature of the tumour and establishes the grade. Even a well differentiated, G 1 neuroendocrine tumour has a malignant behaviour leading to liver metastasis, as is the case with our patient. The increasing number of therapeutic options and diagnostic procedures requires a multidisciplinary approach with a team consisting of an oncologist, a surgeon, a pathologist, a gastroenterologist, a radiologist, and a nuclear medicine specialist. Decisions should be made in multidisciplinary meetings based on patients’ specific conditions.
References1. Kjell Oberg, Gastrointestinal Neuroendocrine
Tumors and the Carcinoid Syndrome, Chapter 31 in Sleisenger and Fordtrans’2 Gastrointestinal and Liver Diseases, 9th Edition.
2. David S. Klimstra, Irvin R. Modlin, Domenico Coppola, The Pathologic Classification of Neuroendocrine Tumors, NANET Guidelines, Pancreas 2010;39: 707-712.
3. Rindi G, Arnold R, Bosman FT, et al.
Nomenclature and classification of neuroendocrine neoplasms of the digestive system. In: WHO Classification of Tumours of the Digestive System, 4th ed, Bosman TF, Carneiro F, Hruban RH, Theise ND (Eds), International Agency for Research on cancer (IARC), Lyon 2010. p.13.
4. Johanna Zuetenhosrt and Babs G. Taal, Metastatic Carcinoid Tumors: A Clinical Review, The Oncologist, 2005,2, 123-131.
5. K. Öberg, U. Knigge, D. Kwekkeboom & A. Perren on behalf of the ESMO Guidelines Working Group, Neuroendocrine gastro-entero-pancreatic tumors: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up, Annals of Oncology 23 (Supplement 7) 2012: 124-130.
6. Izchak Kohen, MD and Sascha Arbouet, Neuroendocrine Carcinoid Cancer Associated with Psychosis, Psychiatry (Edgmont). Jun 2008; 5(6): 29–30.
7. Barbro Eriksson, Günter Klöppel and al. Frascati Consensus Conference participants, Consensus Guidelines for the Management of Patients with Digestive Neuroendocrine Tumors – Well-Differentiated Jejunal-Ileal Tumor/Carcinoma, Neuroendocrinology 2008;87:8–19;DOI: 10.1159/000111034.
8. Toumpanakis C, Caplin ME. Update on the role of somatostatin analogs for the treatment of patients with gastroenteropancreatic neuroendocrine tumors. Semin Oncol 2013; 40:56.

XIX, Vol.19, Number 4/2015 163
Toader Miorița30-32 Iancu de Hunedoara Blvd., Bucharest, Romaniae-mail: [email protected]
Abstract. Neck masses always require an extensive differential diagnosis, including both benign and malignant etiologies. Therefore an accurate diagnosis is of paramount importance and three broad categories should be taken into account: congenital, inflammatory and neoplastic. In particular, congenital lesions are usually midline, nontender, mobile, submental neck masses. For example dermoid cysts are due to entrapment of epithelium in deeper tissue, occurring either developmentally or post trauma. They are treated by surgical excision. The authors report a clinical case presentation of dermoid cyst in the midlevel lateral cervical area which, beside the usual symptoms, adds cardiovascular and respiratory symptomatology by compression.
Keywords: dermoid cyst, breathing difficulties, syncope
1 University of Medicine and Pharmacy “Grigore T. Popa” Iasi2 Emergency Clinical Hospital for Children “Grigore Alexandrescu”, Bucharest3 National Institute of Cerebrovascular Disease, Bucharest
Palade O.D.1, Rebega Cătălina1, Cobzeanu M.D.1, Oprea Alina2, Toader Mioriţa2, Toader C3
COMPRESSING DERMOID CYST OF THE NECK
Therapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 163 - 164© Copyright reserved 2015
Introduction
A new neck mass is a relatively common head and neck problem in patients presenting
to the primary care clinician. Often there are no associated symptoms, other than the recognition of a "new lump" noted incidentally on palpation while grooming, or noticed by another individual.[1,2]
Evaluation of the neck mass must be approached in a thorough and disciplined manner. The mass may be the only manifestation of a serious and potentially malignant pathology, especially in the adult population.[3]
The differential diagnosis in a patient presenting with a neck mass is often extensive and will vary with the age of the patient at presentation. A thorough history and physical examination are essential steps in the evaluation. This will narrow the diagnostic possibilities and help determine the appropriate next diagnostic steps.[4]
Congenital neck masses are usually present at birth, but may present at any age. They are the most common noninflammatory neck mass in children. For masses presenting in adulthood, the patient should be approached with a presumption of malignancy until proven otherwise. Although cystic lesions such as branchial cleft cysts can present in adulthood, these lesions should be approached with a keen diagnostic eye to ensure malignancy is not present. Carcinomas of
the tonsil, tongue base, and thyroid may all present as cystic neck masses.[2]
Material and methodsWe are presenting a male patient T.C., age 42, which
has been hospitalized in the ENT Department with the following symptoms: swelling of the right midlevel lateral cervical area, accompanied by light upper dysphagia, obstructive inspiratory dyspnea and fatigue. Symptoms appeared about 6 months before, but they worsened in the last month. Within this interval the patient presented two episodes of faintness with an unknown etiology (no neurological or cardiovascular causes).
Clinical examination showed the swelling of the right midlevel lateral cervical area reaching up to the right submandibular area by a 30/30 millimetres, firm-elastic fluctuating consistency, mobile, not painful mass.
The indirect laryngoscopy revealed a small lump in the right lateral wall of the oropharynx along with mild stasis of saliva in the right pyriform recess.
During the ENT examination no other pathological signs were identified. The patient had a 32 BMI (Body Mass Index) with an excess of adipose tissue, making the dissection difficult. Cardiologic examination concluded that the patient had normal heart beat, 75 beats/min, blood pressure was 120/75 mmHg. Echocardiographic and electrocardiogram tests were normal.
Blood tests for syphilis, Epstein Barr and Cytomegalic viruses and toxoplasmosis were negative, while a mild biological inflammatory syndrome and hypercholesterolemia were present. The thoracic and cervical X-rays were also normal.
The neck ultrasound described a mass with cystic aspect, sized 35/36 mm, with thin walls, unilocular,
CASE REPORT
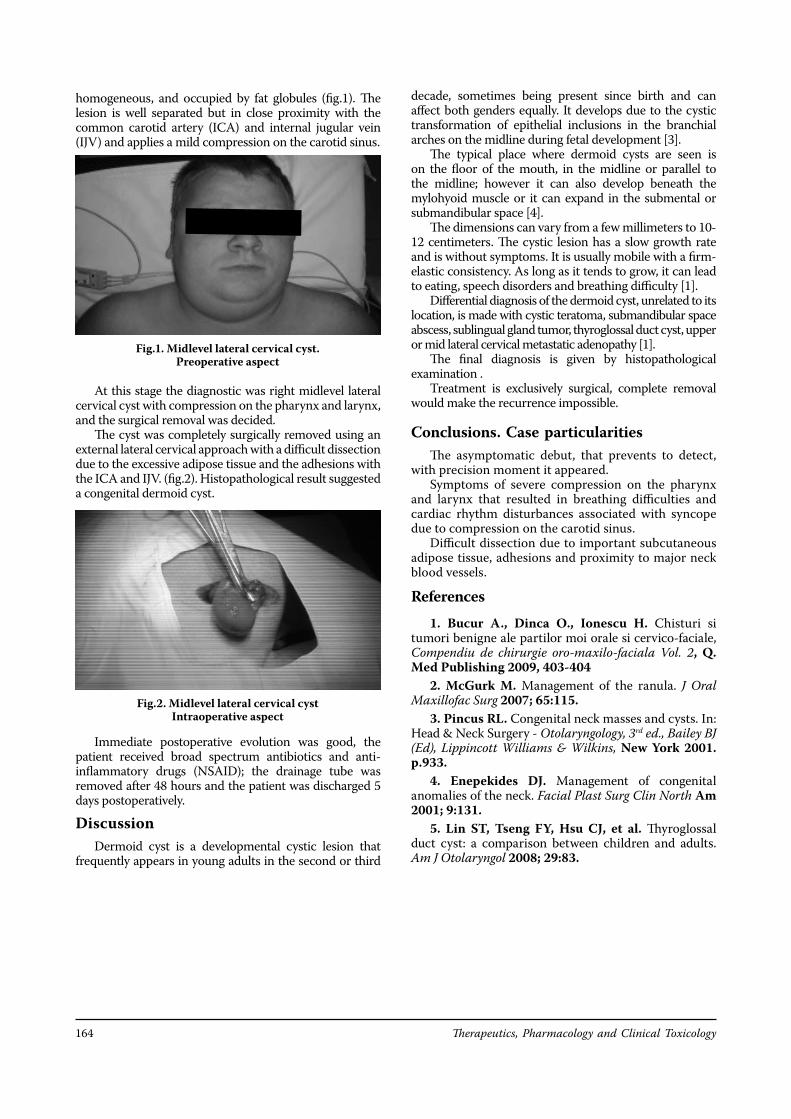
Therapeutics, Pharmacology and Clinical Toxicology164
homogeneous, and occupied by fat globules (fig.1). The lesion is well separated but in close proximity with the common carotid artery (ICA) and internal jugular vein (IJV) and applies a mild compression on the carotid sinus.
At this stage the diagnostic was right midlevel lateral cervical cyst with compression on the pharynx and larynx, and the surgical removal was decided.
The cyst was completely surgically removed using an external lateral cervical approach with a difficult dissection due to the excessive adipose tissue and the adhesions with the ICA and IJV. (fig.2). Histopathological result suggested a congenital dermoid cyst.
Immediate postoperative evolution was good, the patient received broad spectrum antibiotics and anti-inflammatory drugs (NSAID); the drainage tube was removed after 48 hours and the patient was discharged 5 days postoperatively.
DiscussionDermoid cyst is a developmental cystic lesion that
frequently appears in young adults in the second or third
decade, sometimes being present since birth and can affect both genders equally. It develops due to the cystic transformation of epithelial inclusions in the branchial arches on the midline during fetal development [3].
The typical place where dermoid cysts are seen is on the floor of the mouth, in the midline or parallel to the midline; however it can also develop beneath the mylohyoid muscle or it can expand in the submental or submandibular space [4].
The dimensions can vary from a few millimeters to 10-12 centimeters. The cystic lesion has a slow growth rate and is without symptoms. It is usually mobile with a firm-elastic consistency. As long as it tends to grow, it can lead to eating, speech disorders and breathing difficulty [1].
Differential diagnosis of the dermoid cyst, unrelated to its location, is made with cystic teratoma, submandibular space abscess, sublingual gland tumor, thyroglossal duct cyst, upper or mid lateral cervical metastatic adenopathy [1].
The final diagnosis is given by histopathological examination .
Treatment is exclusively surgical, complete removal would make the recurrence impossible.
Conclusions. Case particularitiesThe asymptomatic debut, that prevents to detect,
with precision moment it appeared.Symptoms of severe compression on the pharynx
and larynx that resulted in breathing difficulties and cardiac rhythm disturbances associated with syncope due to compression on the carotid sinus.
Difficult dissection due to important subcutaneous adipose tissue, adhesions and proximity to major neck blood vessels.
References1. Bucur A., Dinca O., Ionescu H. Chisturi si
tumori benigne ale partilor moi orale si cervico-faciale, Compendiu de chirurgie oro-maxilo-faciala Vol. 2, Q. Med Publishing 2009, 403-404
2. McGurk M. Management of the ranula. J Oral Maxillofac Surg 2007; 65:115.
3. Pincus RL. Congenital neck masses and cysts. In: Head & Neck Surgery - Otolaryngology, 3rd ed., Bailey BJ (Ed), Lippincott Williams & Wilkins, New York 2001. p.933.
4. Enepekides DJ. Management of congenital anomalies of the neck. Facial Plast Surg Clin North Am 2001; 9:131.
5. Lin ST, Tseng FY, Hsu CJ, et al. Thyroglossal duct cyst: a comparison between children and adults. Am J Otolaryngol 2008; 29:83.
Fig.1. Midlevel lateral cervical cyst. Preoperative aspect
Fig.2. Midlevel lateral cervical cyst Intraoperative aspect

XIX, Vol.19, Number 4/2015 165
Therapeutics, Pharmacology and Clinical ToxicologyVol XIX, Number 4, December 2015Pages: 165 - 167© Copyright reserved 2015
CASE REPORT
Luminița Stănciulescu 8 Calea Floreasca, 014461 Bucharest, Romaniae-mail: [email protected]
Abstract. Crohn's disease (CD) may affect any segment of the gastrointestinal tract. Although rare, its oesophageal manifestation may be seen as the first sign of this disease. We present the case of a 27 years old female who is admitted with heartburn and dysphagia for 4 years, being misdiagnosed as reflux esophagitis. Endoscopy performed in our unit pointed out erythema, segmental ulcers separated by normal mucosa, “cobble stone’’ aspect. The histological findings were ulcers and a chronic inflammatory mucosal infiltrate. The patient was unresponsive to PPI(Proton Pump Inhibitor), but a rapid improvement was seen after corticosteroid administration. Differential diagnosis and treatment opportunities are presented below.
Keywords: esophageal Crohn’s disease, esophageal ulcers, corticosteroids
A RARE CASE OF ISOLATED OESOPHAGEAL CROHN’S DISEASE
Introduction
Crohn’s disease is a chronic inflammatory disease of unknown aetiology characterized by a chronic,
granulomatous, segmental transmural inflammation that may affect any part of the gastrointestinal tract. The ileum, the colon, the rectum, and the perianal region are the most frequent locations of disease involvement. Esophageal Crohn’s disease is rare, with an adult prevalence of 0.2% to 3% in patients with coexisting ileocolonic disease. Very few cases of isolated esophageal involvement are reported.[1,2] An accurate diagnosis and treatment is often made rather late in its course, due to the unusual presentation of isolated esophageal CD. Here, we report a case of isolated esophageal CD, misdiagnosed as reflux esophagitis, unresponsive to PPI, with a favorable clinical outcome after oral corticosteroids.
Patient, methods and result A 27 years old patient presents with dysphagia and
heartburn for 4 years persistent despite PPI treatment. She didn’t manifest any modification in the stool pattern. She was non smoker and denied alcohol consumption.
She was examined in the past by three upper endoscopy exams which were interpreted as reflux esophagitis. Blood tests revealed slight inflammatory syndrome (CRP-10 mg/dl) and no other modification. We repeated an upper gastro-intestinal endoscopy
which showed throughout the entire length of the oesophagus, oedema, erythema, segmental ulcers with a cobble stone aspect. Biopsies were sampled (Figure 1). Colonoscopy was normal on the entire colon, also terminal ileum was without lesions. Abdominal CT scan was also normal (for suspected lesions of small bowel).
Fig.1. (a, b, c)-endoscopy imagest
1 UMF Carol Davila, Bucharest2 Bucharest Emergency Hospital
* all authors equally contributed to this work
Ilie Mădălina1,2*, Constantinescu G.1,2*, Diaconu Camelia1,2*, Stănciulescu Elena-Luminiţa1,2*, Enache V.1,2*, Macovei R.1,2*, Popa B.1,2*, Țincu R.1,2*
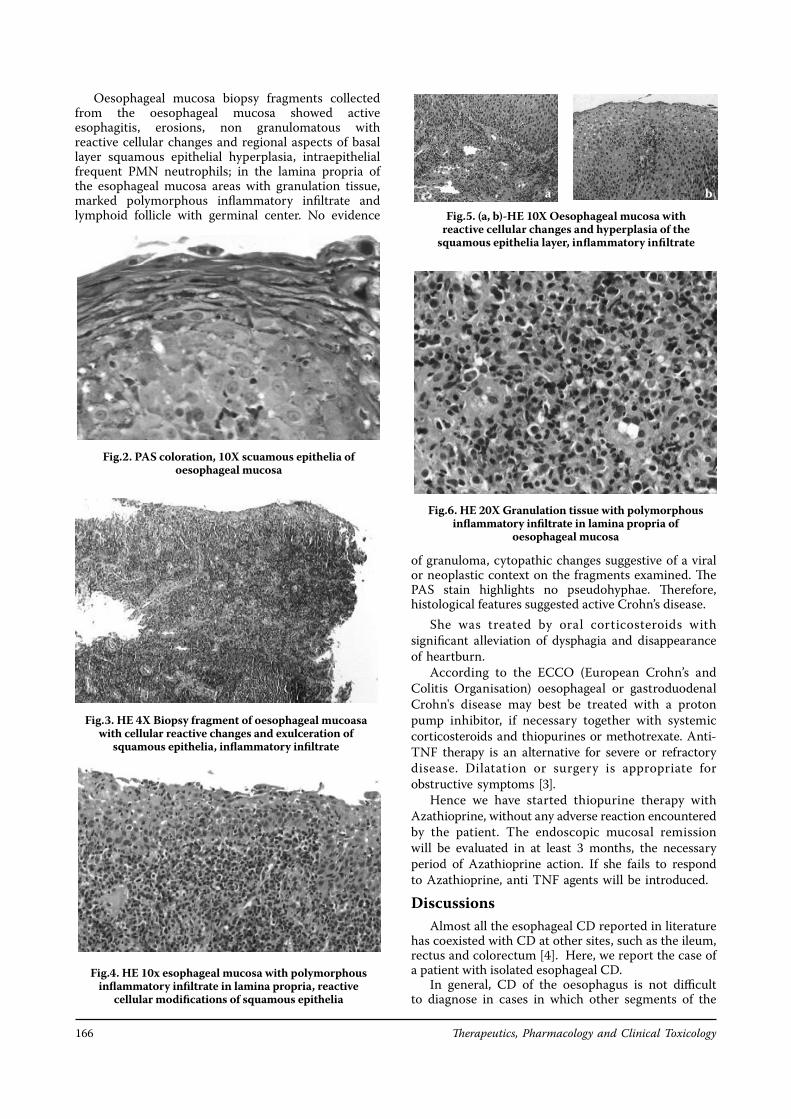
Therapeutics, Pharmacology and Clinical Toxicology166
Oesophageal mucosa biopsy fragments collected from the oesophageal mucosa showed active esophagitis, erosions, non granulomatous with reactive cellular changes and regional aspects of basal layer squamous epithelial hyperplasia, intraepithelial frequent PMN neutrophils; in the lamina propria of the esophageal mucosa areas with granulation tissue, marked polymorphous inflammatory infiltrate and lymphoid follicle with germinal center. No evidence
Fig.2. PAS coloration, 10X scuamous epithelia of oesophageal mucosa
Fig.3. HE 4X Biopsy fragment of oesophageal mucoasa with cellular reactive changes and exulceration of
squamous epithelia, inflammatory infiltrate
of granuloma, cytopathic changes suggestive of a viral or neoplastic context on the fragments examined. The PAS stain highlights no pseudohyphae. Therefore, histological features suggested active Crohn’s disease.
She was treated by oral corticosteroids with significant alleviation of dysphagia and disappearance of heartburn.
According to the ECCO (European Crohn’s and Colitis Organisation) oesophageal or gastroduodenal Crohn's disease may best be treated with a proton pump inhibitor, if necessary together with systemic corticosteroids and thiopurines or methotrexate. Anti-TNF therapy is an alternative for severe or refractory disease. Dilatation or surgery is appropriate for obstructive symptoms [3].
Hence we have started thiopurine therapy with Azathioprine, without any adverse reaction encountered by the patient. The endoscopic mucosal remission will be evaluated in at least 3 months, the necessary period of Azathioprine action. If she fails to respond to Azathioprine, anti TNF agents will be introduced.
Discussions Almost all the esophageal CD reported in literature
has coexisted with CD at other sites, such as the ileum, rectus and colorectum [4]. Here, we report the case of a patient with isolated esophageal CD.
In general, CD of the oesophagus is not difficult to diagnose in cases in which other segments of the
Fig.6. HE 20X Granulation tissue with polymorphous inflammatory infiltrate in lamina propria of
oesophageal mucosa
Fig.4. HE 10x esophageal mucosa with polymorphous inflammatory infiltrate in lamina propria, reactive
cellular modifications of squamous epithelia
Fig.5. (a, b)-HE 10X Oesophageal mucosa with reactive cellular changes and hyperplasia of the
squamous epithelia layer, inflammatory infiltrate
a b
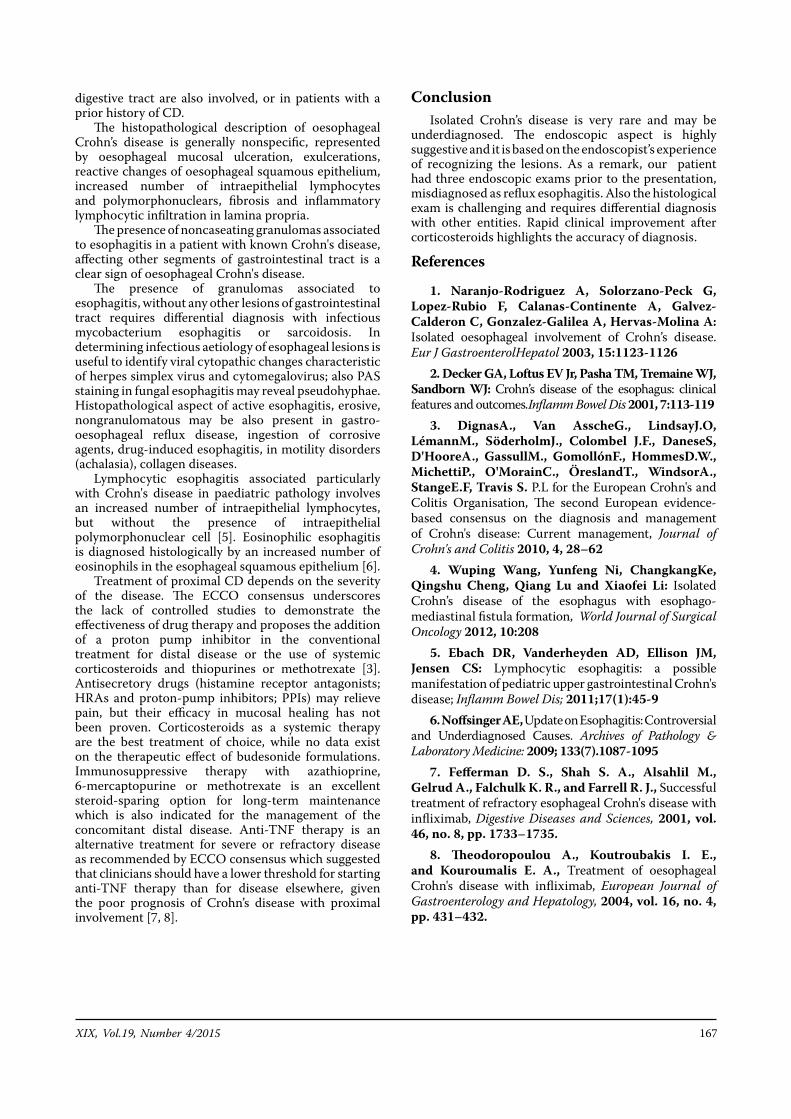
XIX, Vol.19, Number 4/2015 167
digestive tract are also involved, or in patients with a prior history of CD.
The histopathological description of oesophageal Crohn’s disease is generally nonspecific, represented by oesophageal mucosal ulceration, exulcerations, reactive changes of oesophageal squamous epithelium, increased number of intraepithelial lymphocytes and polymorphonuclears, fibrosis and inflammatory lymphocytic infiltration in lamina propria.
The presence of noncaseating granulomas associated to esophagitis in a patient with known Crohn's disease, affecting other segments of gastrointestinal tract is a clear sign of oesophageal Crohn's disease.
The presence of granulomas associated to esophagitis, without any other lesions of gastrointestinal tract requires differential diagnosis with infectious mycobacterium esophagitis or sarcoidosis. In determining infectious aetiology of esophageal lesions is useful to identify viral cytopathic changes characteristic of herpes simplex virus and cytomegalovirus; also PAS staining in fungal esophagitis may reveal pseudohyphae. Histopathological aspect of active esophagitis, erosive, nongranulomatous may be also present in gastro-oesophageal reflux disease, ingestion of corrosive agents, drug-induced esophagitis, in motility disorders (achalasia), collagen diseases.
Lymphocytic esophagitis associated particularly with Crohn's disease in paediatric pathology involves an increased number of intraepithelial lymphocytes, but without the presence of intraepithelial polymorphonuclear cell [5]. Eosinophilic esophagitis is diagnosed histologically by an increased number of eosinophils in the esophageal squamous epithelium [6].
Treatment of proximal CD depends on the severity of the disease. The ECCO consensus underscores the lack of controlled studies to demonstrate the effectiveness of drug therapy and proposes the addition of a proton pump inhibitor in the conventional treatment for distal disease or the use of systemic corticosteroids and thiopurines or methotrexate [3]. Antisecretory drugs (histamine receptor antagonists; HRAs and proton-pump inhibitors; PPIs) may relieve pain, but their efficacy in mucosal healing has not been proven. Corticosteroids as a systemic therapy are the best treatment of choice, while no data exist on the therapeutic effect of budesonide formulations. Immunosuppressive therapy with azathioprine, 6-mercaptopurine or methotrexate is an excellent steroid-sparing option for long-term maintenance which is also indicated for the management of the concomitant distal disease. Anti-TNF therapy is an alternative treatment for severe or refractory disease as recommended by ECCO consensus which suggested that clinicians should have a lower threshold for starting anti-TNF therapy than for disease elsewhere, given the poor prognosis of Crohn’s disease with proximal involvement [7, 8].
Conclusion Isolated Crohn’s disease is very rare and may be
underdiagnosed. The endoscopic aspect is highly suggestive and it is based on the endoscopist’s experience of recognizing the lesions. As a remark, our patient had three endoscopic exams prior to the presentation, misdiagnosed as reflux esophagitis. Also the histological exam is challenging and requires differential diagnosis with other entities. Rapid clinical improvement after corticosteroids highlights the accuracy of diagnosis.
References
1. Naranjo-Rodriguez A, Solorzano-Peck G, Lopez-Rubio F, Calanas-Continente A, Galvez-Calderon C, Gonzalez-Galilea A, Hervas-Molina A: Isolated oesophageal involvement of Crohn’s disease. Eur J GastroenterolHepatol 2003, 15:1123-1126
2. Decker GA, Loftus EV Jr, Pasha TM, Tremaine WJ, Sandborn WJ: Crohn’s disease of the esophagus: clinical features and outcomes.Inflamm Bowel Dis 2001, 7:113-119
3. DignasA., Van AsscheG., LindsayJ.O, LémannM., SöderholmJ., Colombel J.F., DaneseS, D'HooreA., GassullM., GomollónF., HommesD.W., MichettiP., O'MorainC., ÖreslandT., WindsorA., StangeE.F, Travis S. P.L for the European Crohn's and Colitis Organisation, The second European evidence-based consensus on the diagnosis and management of Crohn's disease: Current management, Journal of Crohn's and Colitis 2010, 4, 28–62
4. Wuping Wang, Yunfeng Ni, ChangkangKe, Qingshu Cheng, Qiang Lu and Xiaofei Li: Isolated Crohn’s disease of the esophagus with esophago-mediastinal fistula formation, World Journal of Surgical Oncology 2012, 10:208
5. Ebach DR, Vanderheyden AD, Ellison JM, Jensen CS: Lymphocytic esophagitis: a possible manifestation of pediatric upper gastrointestinal Crohn's disease; Inflamm Bowel Dis; 2011;17(1):45-9
6. Noffsinger AE, Update on Esophagitis: Controversial and Underdiagnosed Causes. Archives of Pathology & Laboratory Medicine: 2009; 133(7).1087-1095
7. Fefferman D. S., Shah S. A., Alsahlil M., Gelrud A., Falchulk K. R., and Farrell R. J., Successful treatment of refractory esophageal Crohn's disease with infliximab, Digestive Diseases and Sciences, 2001, vol. 46, no. 8, pp. 1733–1735.
8. Theodoropoulou A., Koutroubakis I. E., and Kouroumalis E. A., Treatment of oesophageal Crohn's disease with infliximab, European Journal of Gastroenterology and Hepatology, 2004, vol. 16, no. 4, pp. 431–432.
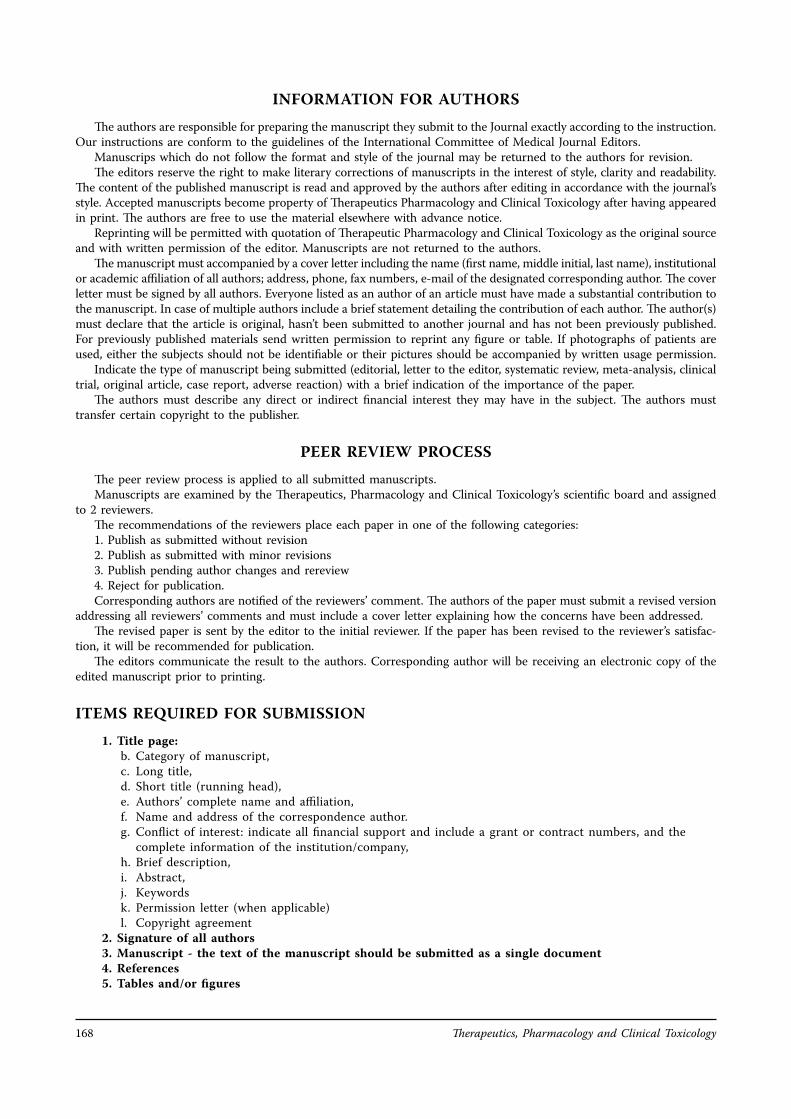
Therapeutics, Pharmacology and Clinical Toxicology168
INFORMATION FOR AUTHORS
The authors are responsible for preparing the manuscript they submit to the Journal exactly according to the instruction. Our instructions are conform to the guidelines of the International Committee of Medical Journal Editors.
Manuscrips which do not follow the format and style of the journal may be returned to the authors for revision. The editors reserve the right to make literary corrections of manuscripts in the interest of style, clarity and readability.
The content of the published manuscript is read and approved by the authors after editing in accordance with the journal’s style. Accepted manuscripts become property of Therapeutics Pharmacology and Clinical Toxicology after having appeared in print. The authors are free to use the material elsewhere with advance notice.
Reprinting will be permitted with quotation of Therapeutic Pharmacology and Clinical Toxicology as the original source and with written permission of the editor. Manuscripts are not returned to the authors.
The manuscript must accompanied by a cover letter including the name (first name, middle initial, last name), institutional or academic affiliation of all authors; address, phone, fax numbers, e-mail of the designated corresponding author. The cover letter must be signed by all authors. Everyone listed as an author of an article must have made a substantial contribution to the manuscript. In case of multiple authors include a brief statement detailing the contribution of each author. The author(s) must declare that the article is original, hasn’t been submitted to another journal and has not been previously published. For previously published materials send written permission to reprint any figure or table. If photographs of patients are used, either the subjects should not be identifiable or their pictures should be accompanied by written usage permission.
Indicate the type of manuscript being submitted (editorial, letter to the editor, systematic review, meta-analysis, clinical trial, original article, case report, adverse reaction) with a brief indication of the importance of the paper.
The authors must describe any direct or indirect financial interest they may have in the subject. The authors must transfer certain copyright to the publisher.
PEER REVIEW PROCESS
The peer review process is applied to all submitted manuscripts. Manuscripts are examined by the Therapeutics, Pharmacology and Clinical Toxicology’s scientific board and assigned
to 2 reviewers. The recommendations of the reviewers place each paper in one of the following categories: 1. Publish as submitted without revision 2. Publish as submitted with minor revisions 3. Publish pending author changes and rereview 4. Reject for publication. Corresponding authors are notified of the reviewers’ comment. The authors of the paper must submit a revised version
addressing all reviewers’ comments and must include a cover letter explaining how the concerns have been addressed. The revised paper is sent by the editor to the initial reviewer. If the paper has been revised to the reviewer’s satisfac-
tion, it will be recommended for publication. The editors communicate the result to the authors. Corresponding author will be receiving an electronic copy of the
edited manuscript prior to printing.
ITEMS REQUIRED FOR SUBMISSION
1. Title page:b. Category of manuscript,c. Long title,d. Short title (running head),e. Authors’ complete name and affiliation,f. Name and address of the correspondence author.g. Conflict of interest: indicate all financial support and include a grant or contract numbers, and the
complete information of the institution/company,h. Brief description,i. Abstract,j. Keywordsk. Permission letter (when applicable)l. Copyright agreement
2. Signature of all authors3. Manuscript - the text of the manuscript should be submitted as a single document4. References5. Tables and/or figures
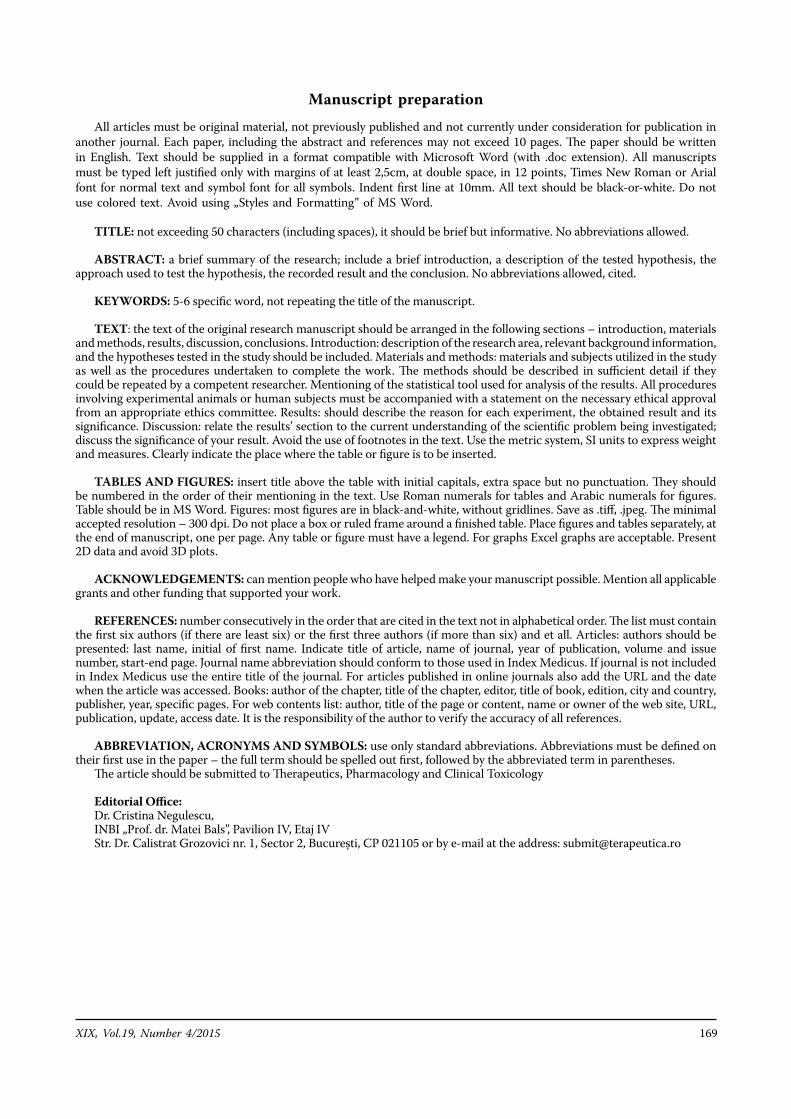
XIX, Vol.19, Number 4/2015 169
Manuscript preparation
All articles must be original material, not previously published and not currently under consideration for publication in another journal. Each paper, including the abstract and references may not exceed 10 pages. The paper should be written in English. Text should be supplied in a format compatible with Microsoft Word (with .doc extension). All manuscripts must be typed left justified only with margins of at least 2,5cm, at double space, in 12 points, Times New Roman or Arial font for normal text and symbol font for all symbols. Indent first line at 10mm. All text should be black-or-white. Do not use colored text. Avoid using „Styles and Formatting” of MS Word.
TITLE: not exceeding 50 characters (including spaces), it should be brief but informative. No abbreviations allowed.
ABSTRACT: a brief summary of the research; include a brief introduction, a description of the tested hypothesis, the approach used to test the hypothesis, the recorded result and the conclusion. No abbreviations allowed, cited.
KEYWORDS: 5-6 specific word, not repeating the title of the manuscript.
TEXT: the text of the original research manuscript should be arranged in the following sections – introduction, materials and methods, results, discussion, conclusions. Introduction: description of the research area, relevant background information, and the hypotheses tested in the study should be included. Materials and methods: materials and subjects utilized in the study as well as the procedures undertaken to complete the work. The methods should be described in sufficient detail if they could be repeated by a competent researcher. Mentioning of the statistical tool used for analysis of the results. All procedures involving experimental animals or human subjects must be accompanied with a statement on the necessary ethical approval from an appropriate ethics committee. Results: should describe the reason for each experiment, the obtained result and its significance. Discussion: relate the results’ section to the current understanding of the scientific problem being investigated; discuss the significance of your result. Avoid the use of footnotes in the text. Use the metric system, SI units to express weight and measures. Clearly indicate the place where the table or figure is to be inserted.
TABLES AND FIGURES: insert title above the table with initial capitals, extra space but no punctuation. They should be numbered in the order of their mentioning in the text. Use Roman numerals for tables and Arabic numerals for figures. Table should be in MS Word. Figures: most figures are in black-and-white, without gridlines. Save as .tiff, .jpeg. The minimal accepted resolution – 300 dpi. Do not place a box or ruled frame around a finished table. Place figures and tables separately, at the end of manuscript, one per page. Any table or figure must have a legend. For graphs Excel graphs are acceptable. Present 2D data and avoid 3D plots.
ACKNOWLEDGEMENTS: can mention people who have helped make your manuscript possible. Mention all applicable grants and other funding that supported your work.
REFERENCES: number consecutively in the order that are cited in the text not in alphabetical order. The list must contain the first six authors (if there are least six) or the first three authors (if more than six) and et all. Articles: authors should be presented: last name, initial of first name. Indicate title of article, name of journal, year of publication, volume and issue number, start-end page. Journal name abbreviation should conform to those used in Index Medicus. If journal is not included in Index Medicus use the entire title of the journal. For articles published in online journals also add the URL and the date when the article was accessed. Books: author of the chapter, title of the chapter, editor, title of book, edition, city and country, publisher, year, specific pages. For web contents list: author, title of the page or content, name or owner of the web site, URL, publication, update, access date. It is the responsibility of the author to verify the accuracy of all references.
ABBREVIATION, ACRONYMS AND SYMBOLS: use only standard abbreviations. Abbreviations must be defined on their first use in the paper – the full term should be spelled out first, followed by the abbreviated term in parentheses.
The article should be submitted to Therapeutics, Pharmacology and Clinical Toxicology
Editorial Office: Dr. Cristina Negulescu, INBI „Prof. dr. Matei Bals”, Pavilion IV, Etaj IVStr. Dr. Calistrat Grozovici nr. 1, Sector 2, București, CP 021105 or by e-mail at the address: [email protected]
Therapeutics, Pharmacology and Clinical Toxicology170
THERAPEUTICS PHARMACOLOGY AND CLINICAL TOXICOLOGY
Subscription 2015
Last name ................................................................................................................................... First name .................................................................................................................................. Identity card series.......... No .............................. Personal identi�cation code............................................................................ Specialties ................................................................................................................................. Organisation............................................................................................................................... Address: Street ............................................................no ......... building ......... sc .... ap ......
City/Country.............................................................................................................................. E-mail ............................................... Phone ................................................
Bank account: RO 80 BPOS 7060 2559 568 ROL 01 Banc Post Universitate For : Editura RP Annual subscription rates for 2016: 450 RON Frequency: 4 issues a year Orders should be sent to the Editorial o�ce by E-mail: [email protected]

![[Click here and type address] - forskning.ruc.dk · IULIU HAŢIEGANU UNIVERSITY OF MEDICINE AND PHARMACY, CLUJ-NAPOCA FOLLOW-UP EVALUATION REPORT May 2015 Team: Henrik Toft Jensen,](https://img.pdfslide.net/doc/110x75/5e085ed06457db30e50f5b6d/click-here-and-type-address-iuliu-haieganu-university-of-medicine-and-pharmacy.jpg)



























