Embed Size (px)
Citation preview

R
WO
FA
DC
ApntspdtnntbcssbipvcsabiPftinbar
Ka
PINTT
*8EAtac
Neuroscience 147 (2007) 260–271
0d
EVIEW
HEN WORDS ARE PAINFUL: UNRAVELING THE MECHANISMS
F THE NOCEBO EFFECTOCAR
Tris(2tosspcmwletasa1
ocirf2tanottt
Tata
. BENEDETTI,* M. LANOTTE, L. LOPIANOND L. COLLOCA
epartment of Neuroscience, University of Turin Medical School,orso Raffaello 30, 10125 Turin, Italy
bstract—The nocebo effect is a phenomenon that is op-osite to the placebo effect, whereby expectation of aegative outcome may lead to the worsening of a symp-
om. Thus far, its study has been limited by ethical con-traints, particularly in patients, as a nocebo procedure iser se stressful and anxiogenic. It basically consists inelivering verbal suggestions of negative outcomes so
hat the subject expects clinical worsening. Although someatural nocebo situations do exist, such as the impact ofegative diagnoses upon the patient and the patient’s dis-
rust in a therapy, the neurobiological mechanisms haveeen understood in the experimental setting under strictlyontrolled conditions. As for the placebo counterpart, thetudy of pain has been fruitful in recent years to under-tand both the neuroanatomical and the neurochemicalases of the nocebo effect. Recent experimental evidence
ndicates that negative verbal suggestions induce antici-atory anxiety about the impending pain increase, and thiserbally-induced anxiety triggers the activation of chole-ystokinin (CCK) which, in turn, facilitates pain transmis-ion. CCK-antagonists have been found to block thisnxiety-induced hyperalgesia, thus opening up the possi-ility of new therapeutic strategies whenever pain has an
mportant anxiety component. Other conditions, such asarkinson’s disease, although less studied, have been
ound to be affected by nocebo suggestions as well. Allhese findings underscore the important role of cognitionn the therapeutic outcome, and suggest that nocebo andocebo-related effects might represent a point of vulnera-ility both in the course of a disease and in the response totherapy. © 2007 IBRO. Published by Elsevier Ltd. All
ights reserved.
ey words: placebo, cholecystokinin, endogenous opioids,nxiety, pain, Parkinson’s disease.
Contentslacebo and nocebo effects 260
maging the brain when expecting negative outcomes 261ocebo hyperalgesia and its biochemistry 263he role of CCK in pain, cognition and emotion 263he nocebo effect in Parkinson’s disease 266
Corresponding author. Tel: �39-011-670-7709; fax: �39-011-670-174.-mail address: [email protected] (F. Benedetti).bbreviations: ACC, anterior cingulate cortex; ACTH, adrenocortico-
ropic hormone; CCK, cholecystokinin; HPA, hypothalamic–pituitary–
tdrenal; PFC, prefrontal cortex; PI, posterior insula; PO, parietal oper-ulum.
306-4522/07$30.00�0.00 © 2007 IBRO. Published by Elsevier Ltd. All rights reseroi:10.1016/j.neuroscience.2007.02.020
260
pen versus hidden interruption of treatments 266onclusions 268cknowledgments 269eferences 269
op-down control of sensory input plays a fundamentalole in shaping global perceptual experience. Whereas thiss well recognized and studied in many sensory modalities,uch as the visual, somatosensory and auditory systemsFrith and Dolan, 1997; Mesulam, 1998; Pessoa et al.,003), new lines of experimental evidence suggest thathis top-down cognitive and emotional modulation alsoccurs in the clinical setting, whereby the intensity andeverity of symptoms can be shaped by the psychologicaltate of the patient. Early studies showed that complexsychological factors can modulate both the patient’s per-eption of pain and his/her response to an analgesic treat-ent. For example, it was shown that pretreating patientsith placebos, i.e. inert substances that the patient be-
ieves to be effective, lowered the effectiveness of painkill-rs, while pretreatment with active painkillers enhancedhe analgesic effect of placebos (Kantor et al., 1966; Laskand Sunshine, 1973). Likewise, it was found that verbaluggestions can change the direction of nitrous oxide’sction from analgesia to hyperalgesia (Dworkin et al.,983).
Most research of this kind has been pursued in the fieldf pain and analgesia, and the study of placebo and no-ebo effects has been crucial to unravel the neurobiolog-
cal mechanisms of this top-down modulation. Since manyeviews have been written on the placebo effect in the pastew years (Benedetti et al., 2005; Colloca and Benedetti,005; Hoffman et al., 2005; Pacheco-Lopez et al., 2006),he present review describes only what we know todaybout the mechanisms of the nocebo effect, a phenome-on whereby anticipation and expectation of a negativeutcome may induce the worsening of a symptom. Ashese effects occur in the clinical setting, they have impor-ant implications for both therapy and patient–provider in-eraction.
PLACEBO AND NOCEBO EFFECTS
he placebo effect has been studied extensively from bothpsychological and biological perspective, but in recent
imes placebo research has focused on the neural mech-nisms, both from the neurochemical and the neuroana-
omical viewpoint. Placebos are known to powerfully affectved.
tmatHbaaP2wl2
auab1B22gd2ssldB
ntmccdn2
mwe2sbtnsh
cse1tee
eaiapaawawa
Mteiubtplsb
sftapofirt(saTtsr
pDAb(1Laeiiss
F. Benedetti et al. / Neuroscience 147 (2007) 260–271 261
he brain in different pathological conditions, like pain,otor disorders and depression, and in different systemsnd apparatuses, such as the immune and endocrine sys-em (Benedetti et al., 2005; Colloca and Benedetti, 2005;offman et al., 2005; Pacheco-Lopez et al., 2006). It haseen shown that this may occur through both expectationnd conditioning mechanisms, but expectation of the ther-peutic benefit seems to play a crucial role, at least in pain,arkinson’s disease and depression (Benedetti et al.,003b; Finniss and Benedetti, 2005; Hoffman et al., 2005),hereas immune and hormonal placebo responses are
ikely to involve conditioning mechanisms (Benedetti et al.,003b; Pacheco-Lopez et al., 2006).
Recently, placebo-induced expectations have beennalyzed with sophisticated neurobiological tools that havencovered specific mechanisms at both the biochemical,natomical and cellular level. In fact, expectations haveeen found to activate endogenous opioids (Levine et al.,978; Grevert et al., 1983; Benedetti, 1996; Amanzio andenedetti, 1999; Benedetti et al., 1999; Zubieta et al.,005) and pain modulating networks (Petrovic et al.,002), to decrease the transmission in pain pathways (Wa-er et al., 2004: Price et al., 2006), to induce a release ofopamine in the striatum (de la Fuente-Fernandez et al.,001), and to affect the activity of single neurons in theubthalamic nucleus (Benedetti et al., 2004). There is alsoome experimental evidence that different serotonin-re-ated brain regions are involved in the placebo response inepression (Leuchter et al., 2002; Mayberg et al., 2002;enedetti et al., 2005).
Overall, the search for the neurobiological mecha-isms of the placebo effect has given us information about
he intricate interaction that exists between a complexental activity, such as expectation and anticipation of
linical benefit, and different neuronal systems which areapable of modifying the course of a symptom and/or aisease. It has also given us important information aboutew ways of running clinical trials (Colloca and Benedetti,005; Finniss and Benedetti, 2005).
On the other hand, mainly due to ethical constraints,uch less is known about the nocebo counterpart. In fact,hereas the induction of placebo responses is certainlythical in many circumstances (Benedetti and Colloca,004; Colloca et al., 2004), the induction of nocebo re-ponses represents a stressful and anxiogenic procedure,ecause verbally-induced negative expectations of symp-om worsening may lead to a real worsening. Of course, aocebo procedure is unethical in patients, but some recenttudies in healthy volunteers and some others in animalsave shed new light on this phenomenon.
The term nocebo (“I shall harm”) was introduced inontraposition to the term placebo (“I shall please”) byome authors to distinguish the pleasing from the noxiousffects of placebo (Kennedy, 1961; Kissel and Barrucand,964; Hahn, 1985, 1997). If the positive psychosocial con-ext (i.e. the verbal context), which is typical of the placeboffect, is reversed in the opposite direction, the nocebo
ffect can be studied. fIt is important to point out that the study of the noceboffect is the study of the negative psychosocial contextround the patient and the treatment, and its neurobiolog-
cal investigation is the analysis of the effects of this neg-tive context on the patient’s brain and body. As for thelacebo effect, the nocebo effect, or response, follows thedministration of and inert substance (the nocebo, or neg-tive placebo) along with the suggestion that the subjectill get worse. However, the term nocebo-related effect willlso be used throughout this review to indicate symptomorsening following negative expectations but without thedministration of any inert substance.
IMAGING THE BRAIN WHEN EXPECTINGNEGATIVE OUTCOMES
odern brain imaging techniques have been fundamen-al in the understanding of the neurobiology of negativexpectations. It should be noted that no inert substance
s given in these studies, and the experimenter typicallyses verbal suggestions. Therefore, in this case it woulde better to talk about nocebo-related effects. Typically,
he experimenter tells the subject about the forthcomingain so as to make the subject expect a painful stimu-
ation, and both the anticipatory phase and the post-timulus phase are analyzed. Most of this research haseen carried out in the field of pain.
By using this experimental approach, it has beenhown that the perceived intensity of a painful stimulusollowing negative expectation of pain increase is higherhan in the absence of negative expectations. For ex-mple, Sawamoto et al. (2000) found that expectation ofainful stimulation amplifies perceived unpleasantnessf innocuous thermal stimulation. These psychophysicalndings were correlated to enhanced transient brainesponses to the nonpainful thermal stimulus in the an-erior cingulate cortex (ACC), the parietal operculumPO) and posterior insula (PI). This enhancement con-isted in both a higher intensity signal change (in ACC)nd a larger volume of activated voxels (in PO and PI).herefore, expecting a painful stimulus enhances both
he subjective unpleasant experience of an innocuoustimulus and the objective responses in some brainegions.
Overall, negative expectations may result in the am-lification of pain (Koyama et al., 1998; Price 2000;annecker et al., 2003), and several brain regions, likeCC, the prefrontal cortex (PFC), and the insula, haveeen found to be activated during the anticipation of painChua et al., 1999; Hsieh et al., 1999; Ploghaus et al.,999; Porro et al., 2002, 2003; Koyama et al., 2005;orenz et al., 2005; Keltner et al., 2006). These effectsre in the opposite direction of those elicited by positivexpectations, whereby expectation of reduced pain is
nvestigated. In fact, in some studies in which both pos-tive and negative outcomes have been studied with theame experimental approach, the modulation of bothubjective experience and brain activation has been
ound. For example, in the study by Koyama et al.
(aAdpAiLdcmiw
oatt
tuccil(iic
psnesb
Few cleus cun 6).
F. Benedetti et al. / Neuroscience 147 (2007) 260–271262
2005), as the magnitude of expected pain increased,ctivation increased in the thalamus, insula, PFC, andCC. By contrast, expectations of decreased pain re-uced activation of pain-related brain regions, like therimary somatosensory cortex, the insular cortex andCC. In a different electroencephalogram (EEG) study
n which source localization analysis was performed,orenz et al. (2005) found a modulation of the electricalipole in the secondary somatosensory cortex by no-ebo-like and placebo-like suggestions. The dipole wasodulated in the same direction of expectations, shrink-
ng when pain decrease was expected and expandinghen pain increase was anticipated.
More recently, Keltner et al. (2006) found that the levelf expected pain intensity alters perceived pain intensitylong with the activation of different brain regions. By usingwo visual cues, each conditioned to one of two noxious
ig. 1. Brain fMRI responses to a high-temperature stimulus when thexpectation of a high-intensity noxious stimulus activates different brainell as the orbitofrontal cortex, amygdala, ventral striatum, and the nuoxious stimulus induces less fMRI activation (from Keltner et al., 200
hermal stimuli (high and low), Keltner et al. (2006) showed s
hat subjects reported higher pain when the noxious stim-lus was preceded by the high-intensity visual cue. Byomparing the brain activations produced by the two visualues, these authors found significant differences in the
psilateral caudal ACC, the head of the caudate, cerebel-um, and the contralateral nucleus cuneiformis (nCF)Fig. 1). Interestingly, the imaging results of this studyndicate that expectation and noxious stimulus intensity actn an additive manner on afferent pathways activated byutaneous noxious thermal stimulation.
By taking all these imaging studies together, it ap-ears clear that expectation of either low or high painfultimuli has a strong influence on the perceived pain. Asoted above, although these studies deal with negativexpectations, neither placebos nor nocebos (inert sub-tances) were administered, thus these effects can beetter called nocebo-related effects, in which only verbal
xpects a high (above) or a low (below) intensity stimulation. Note that, such as the thalamus, insular cortex, somatosensory cortex, ACC asneiformis in the brainstem. By contrast, expectation of a low-intensity
subject eregions
uggestions were given.

Lsn(iiw
cBslrtpItoktwwpcta
p(Cettpntt00iagpoee
ipavsasha
mnbbjtbomcabpttahabsa
wemCaiauaCl
BcbsIcibmnfHttnai
gCI
F. Benedetti et al. / Neuroscience 147 (2007) 260–271 263
NOCEBO HYPERALGESIA AND ITSBIOCHEMISTRY
ike placebo analgesia, nocebo hyperalgesia has repre-ented the best model to study the mechanism of theocebo effect. To obtain placebo analgesia, a placeboinert treatment) is given along with verbal suggestions ofmprovement. Likewise, to obtain nocebo hyperalgesia, annert treatment is given along with verbal suggestions oforsening.
A modulation of pain perception by placebo and no-ebo that is dependent on expectation has been shown byenedetti et al. (2003b). In this study, in one group ofubjects a pharmacological pre-conditioning with ketoro-ac, a nonopioid analgesic, was performed for 2 days in aow and then ketorolac was replaced with a placebo on thehird day along with verbal suggestions of analgesia. Thisrocedure induced a strong placebo analgesic response.n order to see whether this placebo response was due tohe pharmacological pre-conditioning, in a second groupf subjects the same pre-conditioning procedure withetorolac was carried out but the placebo was given onhe third day along with verbal suggestions that the drugas a hyperalgesic agent. These verbal instructionsere enough not only to block placebo analgesia com-letely, but also to produce hyperalgesia. These findingslearly show that nocebo hyperalgesia depends on expec-ation of pain increase, even though a pre-conditioningnalgesic procedure is done.
In 1997, Benedetti et al. (1997) ran a trial in postoperativeatients with proglumide, a nonspecific cholecystokininCCK) antagonist for both CCK-A and CCK-B receptors, orCK-1 and CCK-2 according to the new classification (Noblet al., 1999). The situation was a post-surgical manipulation
hat induces expectations of pain increase, so that the pa-ients were given an inert treatment that they expected to beainful. In that study, proglumide was found to preventocebo hyperalgesia in a dose-dependent manner, evenhough it is not a specific painkiller, thus suggesting thathis effect is mediated by CCK. In fact, a dose as low as.05 mg was totally ineffective whereas a dose increase to.5 and 5 mg proved to be effective. As CCK is also
nvolved in anxiety mechanisms, Benedetti et al. (1997)nd Benedetti and Amanzio (1997) hypothesized that pro-lumide affected anticipatory anxiety of the impendingain. Importantly, this effect was not antagonized by nal-xone, thus indicating that it is not opioid-mediated. How-ver, due to ethical constraints in these patients, theseffects were not investigated further.
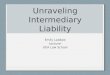
In order to overcome the ethical limitations that arenherent to any clinical study, a similar experimental ap-roach was used in healthy volunteers. In fact, Benedetti etl. (2006), by studying experimental ischemic arm pain inolunteers, performed a detailed neuropharmacologicaltudy of nocebo hyperalgesia. It was found that the oraldministration of an inert substance, along with verbaluggestions of hyperalgesia, induced hyperalgesia andyperactivity of the hypothalamic–pituitary–adrenal (HPA)
xis, as assessed by means of adrenocorticotropic hor- cone (ACTH) and cortisol plasma concentrations. Bothocebo-induced hyperalgesia and HPA hyperactivity werelocked by diazepam, one of the most used anti-anxietyenzodiazepines, which suggests that anxiety plays a ma-
or role in these effects. By contrast, the administration ofhe mixed CCK type-A/B receptor antagonist, proglumide,locked nocebo hyperalgesia completely, but had no effectn HPA hyperactivity, thus suggesting a specific involve-ent of CCK in the hyperalgesic but not in the anxiety
omponent of the nocebo effect. Most important, diazepamnd proglumide did not show analgesic properties onaseline pain, as they acted only on the nocebo-inducedain increase. Therefore, these data indicate a close rela-ionship between anxiety and nocebo hyperalgesia, buthey also indicate that proglumide does not act by blockingnticipatory anxiety of the impending pain, as previouslyypothesized by Benedetti et al. (1997) and by (Benedettind Amanzio 1997), but rather it interrupts a CCKergic linketween anxiety and pain. In other words, these datauggest that CCK turns anxiety into pain and that CCK-ntagonists may prevent this effect (Fig. 2).
A support to this view comes from animal studies, inhich CCK antagonists have been found to prevent anxi-ty-induced hyperalgesia. In particular, in a social-defeatodel of anxiety in rats, it has recently been shown thatI-988, a selective CCK-B receptor antagonist, preventednxiety-induced hyperalgesia, with an effect that was sim-
lar to that produced by the established anxiolytic chlordi-zepoxide (Andre et al., 2005). Similarly, other studies thatsed selective CCK-A and CCK-B receptor antagonists innimals and humans have shown the important role ofCKergic systems in the modulation of anxiety and in the
ink between anxiety and hyperalgesia (Hebb et al., 2005).
THE ROLE OF CCK IN PAIN, COGNITIONAND EMOTION
esides the understanding of the mechanisms of the no-ebo effect, these studies on nocebo hyperalgesia haveeen useful to understand the role of CCK in both pain andome complex functions, such as cognition and emotion.n fact, in recent years CCK has been found to play arucial role in many complex physiological and psycholog-
cal functions (Hebb et al., 2005). For example, there haseen accumulating evidence that CCK acts as a neuro-odulator of pain and anxiety, although the exact mecha-isms are still unclear (Vanderhaeghen et al., 1975; Bein-eld, 1983; Baber et al., 1989; Crawley and Corwin, 1994;ebb et al., 2005). CCK is found in the brain as an oc-
apeptide (CCK-8) and its distribution in the brain matcheshat of the opioid peptides at both the spinal and supraspi-al level (Stengaard-Pedersen and Larsson, 1981; Gall etl., 1987; Gibbins et al., 1987; Benedetti, 1997), suggest-
ng a close interaction between the two neuropeptides.Thus far, the involvement of CCK in nocebo hyperal-
esia is based only on the pharmacological action of theCK-antagonist proglumide (Benedetti et al., 1997, 2006).
t should be noted that, although proglumide is a nonspe-
ific CCK-A/B receptor antagonist with a weak preference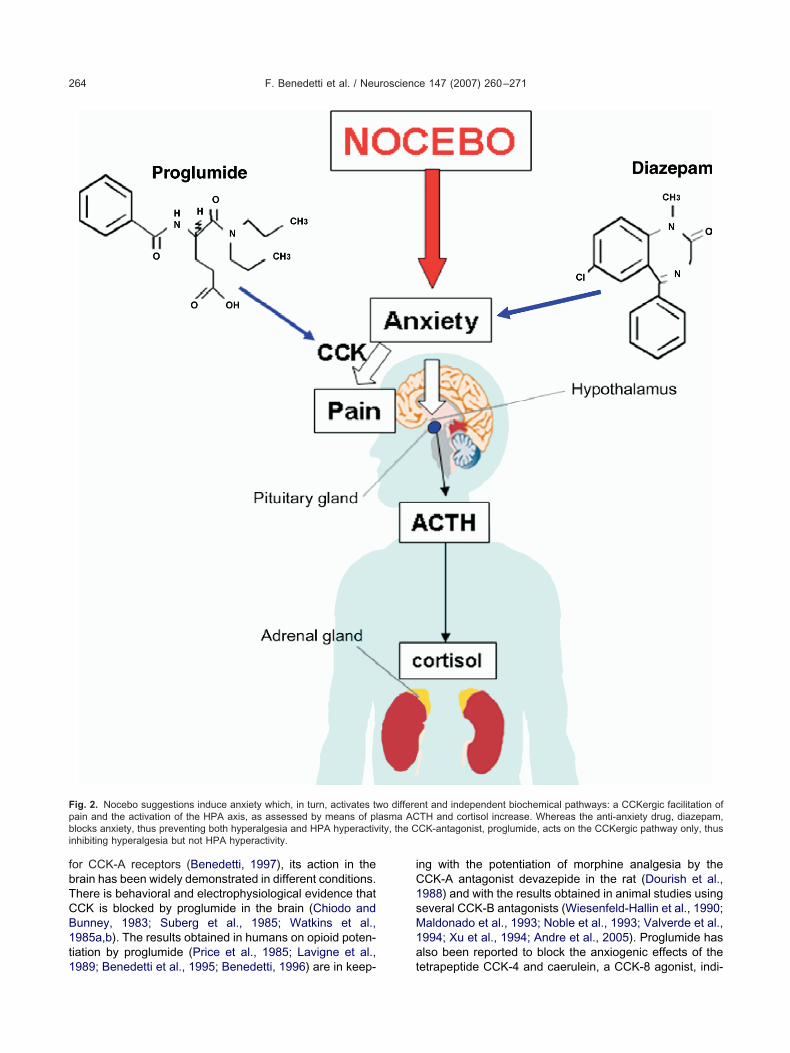
fbTCB1t1
iC1sM1a
Fpbi
F. Benedetti et al. / Neuroscience 147 (2007) 260–271264
or CCK-A receptors (Benedetti, 1997), its action in therain has been widely demonstrated in different conditions.here is behavioral and electrophysiological evidence thatCK is blocked by proglumide in the brain (Chiodo andunney, 1983; Suberg et al., 1985; Watkins et al.,985a,b). The results obtained in humans on opioid poten-iation by proglumide (Price et al., 1985; Lavigne et al.,
ig. 2. Nocebo suggestions induce anxiety which, in turn, activates twain and the activation of the HPA axis, as assessed by means of pllocks anxiety, thus preventing both hyperalgesia and HPA hyperactiv
nhibiting hyperalgesia but not HPA hyperactivity.
989; Benedetti et al., 1995; Benedetti, 1996) are in keep- t
ng with the potentiation of morphine analgesia by theCK-A antagonist devazepide in the rat (Dourish et al.,988) and with the results obtained in animal studies usingeveral CCK-B antagonists (Wiesenfeld-Hallin et al., 1990;aldonado et al., 1993; Noble et al., 1993; Valverde et al.,994; Xu et al., 1994; Andre et al., 2005). Proglumide haslso been reported to block the anxiogenic effects of the
nt and independent biochemical pathways: a CCKergic facilitation ofTH and cortisol increase. Whereas the anti-anxiety drug, diazepam,CK-antagonist, proglumide, acts on the CCKergic pathway only, thus
o differeasma ACity, the C
etrapeptide CCK-4 and caerulein, a CCK-8 agonist, indi-
ct1
(otdrs2itessvsCospC
awLts
assco
vampbauham(bwNtoami
apa
Fs
F. Benedetti et al. / Neuroscience 147 (2007) 260–271 265
ating an anti-CCK action in the CNS at the level of affec-ive mechanisms (Harro et al., 1990; Harro and Vasar,991; van Megen et al., 1994).
The antagonist action of CCK on endogenous opioidsBenedetti, 1997) is particularly interesting in light of thepposing effects of placebos and nocebos. In fact, todayhere is general agreement that placebo analgesia is me-iated by endogenous opioids, specifically the mu-opioideceptors (Zubieta et al., 2005), at least in some circum-tances (Benedetti et al., 2005; Colloca and Benedetti,005). Therefore, the findings on the involvement of CCK
n nocebo hyperalgesia suggest that the opioidergic andhe CCKergic systems may be activated by oppositexpectations of either analgesia or hyperalgesia, re-pectively. In other words, as shown in Fig. 3, verbaluggestions of a positive outcome (pain decrease) acti-ate endogenous mu-opioid neurotransmission, whileuggestions of a negative outcome (pain increase) activateCK-A and/or CCK-B receptors. This neurochemical viewf the placebo–nocebo phenomenon, in which two oppo-ite systems are activated by opposite expectations aboutain, is in keeping with the opposite action of opioids andCK in other studies (Benedetti, 1997; Hebb et al., 2005).
The involvement of CCK in both pain modulation andnxiety is particularly relevant to the nocebo effect. It isorth noting that some CCK-B receptor antagonists, like-365,260, have a benzodiazepine-based chemical struc-
ure that is similar to the anxiolytic drug diazepam, whichuggests a similarity of action of CCK-antagonists and
ig. 3. Placebo and nocebo modulation of pain. Whereas placebo suggestionuggestions induce anxiety which activates CCK-A and/or CCK-B receptors th
nti-anxiety drugs. However, it should be stressed that thetudy by Benedetti et al. (2006) suggests that nocebouggestions activate two different and independent bio-hemical pathways, one blocked by proglumide and thether by diazepam (Fig. 2).
On the basis of all these considerations and the in-olvement of CCKergic systems in pain and anxiety mech-nisms, nocebo hyperalgesia represents an interestingodel to better understand when and how the endogenousro-nociceptive systems are activated. In the case of CCK,esides the studies described above, the pro-nociceptivend anti-opioid action of this neuropeptide has been doc-mented more recently in the brainstem. For example, itas been shown that CCK is capable of reversing opioidnalgesia by acting at the level of the rostral ventromedialedulla, a region that plays a key role in pain modulation
Mitchell et al., 1998; Heinricher et al., 2001). It has alsoeen shown that CCK activates pain facilitating neuronsithin the rostral ventromedial medulla (Heinricher andeubert, 2004). The similarity of the pain facilitating ac-
ion of CCK on brainstem neurons on the one hand andn nocebo mechanisms on the other hand, can stimulatend guide further research into the neurochemicalechanisms underlying nocebo-induced and/or anxiety-
nduced hyperalgesia.It is also worth noting that CCK has been found to play
role in placebo analgesia. In fact, the CCK-antagonistroglumide has been found to potentiate placebo-inducednalgesia, an effect that is probably due to the blockade of
s activate mu-opioid neurotransmission which inhibits pain, noceboat, in turn, enhance pain.

tBrpa
Wabocca(meopanb
midtnsmbssemfepoi
ivdtwsbvtwaptpss
Ebtpstpcoetp(come
Meafe(sCi2i
niprsmuc
Otns2ptprpeoucse
F. Benedetti et al. / Neuroscience 147 (2007) 260–271266
he anti-opioid action of CCK (Benedetti et al., 1995;enedetti, 1996). Therefore, CCK appears to play a pivotal
ole in the psychological modulation of pain, antagonizinglacebo-induced opioid release on the one hand and medi-ting nocebo-induced facilitation of pain on the other hand.
THE NOCEBO EFFECT INPARKINSON’S DISEASE
hereas nocebo hyperalgesia and, more in general, neg-tive expectations of pain increase have been studied fromoth a behavioral, neuroanatomical and biochemical pointf view, the neural mechanisms of the nocebo effect inonditions other than pain are poorly understood. Re-ently, Parkinson’s disease, a disorder of movement char-cterized by tremor, muscle rigidity and bradykinesiamovements slow down), has represented an interestingodel to investigate both the placebo and the noceboffect. However, whereas in the first case some neurobi-logical mechanisms have been uncovered, such as do-amine release in the striatum (de la Fuente-Fernandez etl., 2001) and altered firing pattern in subthalamic nucleuseurons (Benedetti et al., 2004), in the second case onlyehavioral/clinical studies have been done.
In a study by Pollo et al. (2002), the velocity of move-ents was analyzed in Parkinson patients who had been
mplanted with electrodes in the subthalamic nuclei foreep brain stimulation, a highly effective anti-Parkinsonreatment that is capable of relieving the motor parkinso-ian symptoms. These patients were tested in two oppo-ite conditions. In the first condition, they expected a goodotor performance whereas in the second they expected aad motor performance. It was found that these two oppo-ite expectations modulate the therapeutic effect of theubthalamic nucleus stimulation. In fact, by analyzing theffect of subthalamic stimulation on the velocity of move-ent of the right hand with a movement analyzer, it was
ound the hand movement was faster when the patientsxpected a good motor performance than when they ex-ected bad performance. Interestingly, all these effectsccurred within minutes, which indicates that expectations
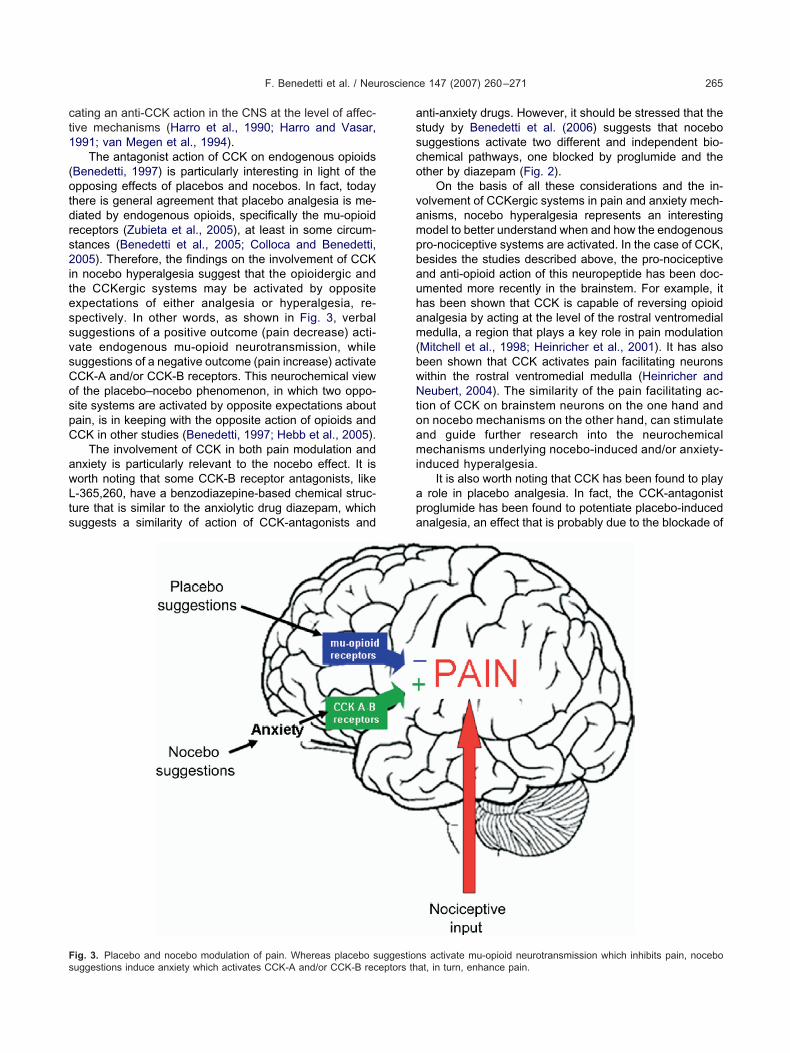
nduce neural changes very quickly.In another study by Benedetti et al. (2003b), patients
mplanted for deep brain stimulation were tested for theelocity of movement of their right hand according to aouble-blind experimental design in which neither the pa-ient nor the experimenter knew whether the stimulatoras turned off. The velocity of hand movement was as-essed by means of a movement analyzer, characterizedy a rectangular surface where the patients performed aisual directional-choice task (Fig. 4, above). To do this,he right index finger was positioned on a central sensorith a green light. After a random interval of a few seconds,red light turned on randomly in one of three sensors
laced 10 cm away from the green-light sensor. The pa-ients were instructed to move their hand as quickly asossible in order to reach the target red-light sensor. Ashown in Fig. 4 (below), the stimulator was turned off
everal times (at 4 and 2 weeks) before the test session. tach time the velocity of movement was measured justefore the stimulator was turned off and 30 min later. Thushe measurement at 30 min reflects the worsening of motorerformance. On the day of the experimental session, thetimulator was maintained on but the patients were toldhat it had been turned off, so as to induce negative ex-ectations of motor performance worsening (nocebo pro-edure). It can be seen that, although the stimulator wasn, motor performance worsened and mimicked the wors-ning of the previous days. In Fig. 4, it can also be seenhat this nocebo bradykinesia could be prevented com-letely by verbal suggestions of good motor performanceplacebo procedure). Therefore, as occurs for pain, in thisase also, motor performance can be modulated in twopposite directions by placebos and nocebos, and thisodulation occurs on the basis of positive and negativexpectations about motor performance.
These findings have been confirmed very recently byercado et al. (2006) who also found a dissociation of theffects in tremor, rigidity and bradykinesia. In fact, theseuthors found significant effects for bradykinesia, but notor tremor and rigidity. On the basis of the studies by Pollot al. (2002), Benedetti et al. (2003b) and Mercado et al.2006), bradykinesia appears to be a symptom that is moreensitive to verbal suggestions than tremor and rigidity.ertainly, more studies are needed to clarify this point, as
n at least two studies (Pollo et al., 2002; Benedetti et al.,003b) only bradykinesia was tested, thus no detailed
nformation is available for the other symptoms.Due to ethical limitations, no neurobiological mecha-
ism is known for this nocebo bradykinesia. Unfortunately,t will not be easy to devise experimental protocols in theseatients to search for its neural mechanisms, as this wouldequire some unnecessary worsening of the parkinsonianymptoms. It is important to point out that in the experi-ents described above the procedure of turning the stim-lator off for a short period of time represents routinelinical practice to test several parameters of stimulation.
OPEN VERSUS HIDDEN INTERRUPTIONOF TREATMENTS
ne of the most interesting experimental approacheshat emphasizes both the importance of positive andegative expectations and their clinical impact is repre-ented by the open– hidden paradigm (Colloca et al.,004; Colloca and Benedetti, 2005). The open (ex-ected) administration of a medical treatment consists of
he administration of a therapy by a doctor who tells theatient that his/her symptoms will improve, according tooutine clinical practice. Therefore, in this condition, theatient expects a benefit. By contrast, the hidden (un-xpected) administration consists in the administrationf a therapy by a computer with the subject completelynaware that a treatment is being carried out. In thisase, the patient does not expect anything. Severaltudies have shown that an open treatment is moreffective than a hidden one, thus indicating that expec-
ation plays a crucial role in the therapeutic outcome
(affitTbtP
ucbd
dcra
Cvcarhtit
Fbmao Benede
F. Benedetti et al. / Neuroscience 147 (2007) 260–271 267
Levine et al., 1981; Amanzio et al., 2001; Benedetti etl., 2003a; Colloca et al., 2004). Whereas the outcome
ollowing a hidden treatment represents the real specific ef-ect of the treatment itself, free of any psychological contam-nation, the outcome following an open treatment representshe sum of the specific effect plus the psychological effect.he difference between the open and hidden treatment haseen considered to represent the placebo component, evenhough no placebo has been given (Amanzio et al., 2001;rice, 2001; Benedetti et al., 2003a; Colloca et al., 2004).
The open–hidden approach has also proven to beseful to understand nocebo-related phenomena. In thisase, open and hidden interruptions of treatments haveeen studied. An open interruption is preformed by the
ig. 4. Assessment of movement velocity in Parkinson patients by meeen turned off at 4 and 2 weeks before the experimental session,aintained on. Each time the velocity of movement was measured just 30 min reflects the worsening of motor performance. Note that, despif improvement antagonized this nocebo effect completely (data from
octor who tells the patient that the treatment has been p
iscontinued. A hidden interruption is carried out by aomputer and the patient does not know about the inter-uption: he believes that the therapy is still beingdministered.
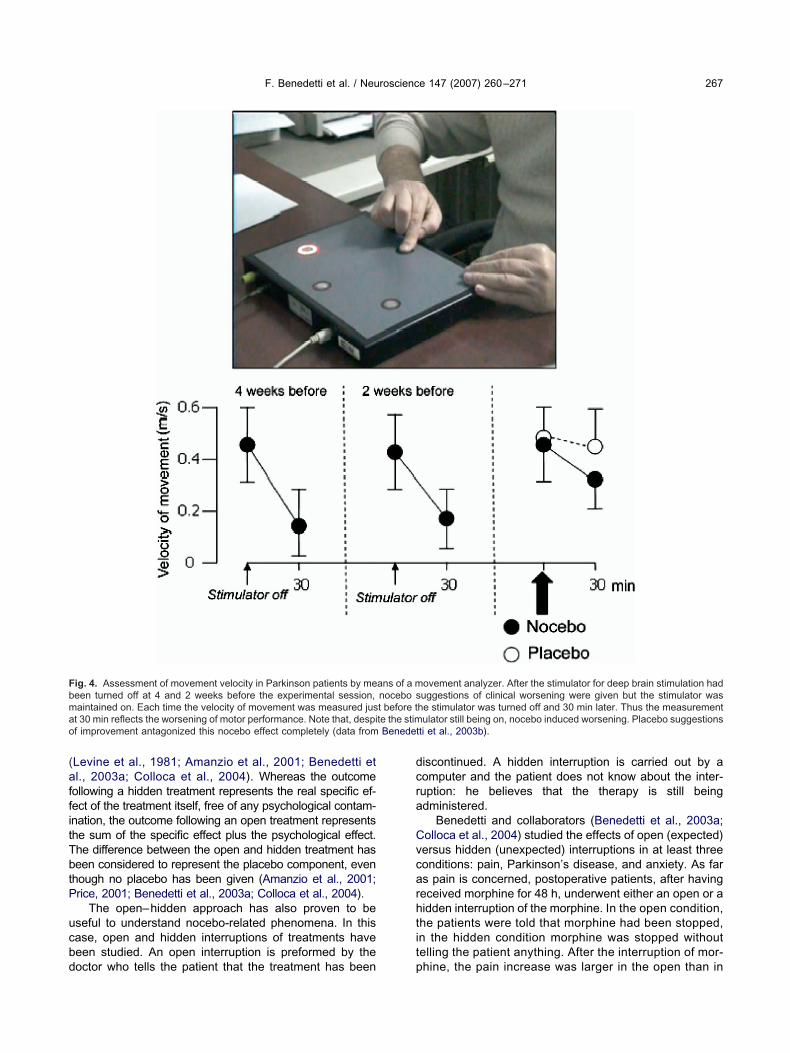
Benedetti and collaborators (Benedetti et al., 2003a;olloca et al., 2004) studied the effects of open (expected)ersus hidden (unexpected) interruptions in at least threeonditions: pain, Parkinson’s disease, and anxiety. As fars pain is concerned, postoperative patients, after havingeceived morphine for 48 h, underwent either an open or aidden interruption of the morphine. In the open condition,he patients were told that morphine had been stopped,n the hidden condition morphine was stopped withoutelling the patient anything. After the interruption of mor-
ovement analyzer. After the stimulator for deep brain stimulation haduggestions of clinical worsening were given but the stimulator was
he stimulator was turned off and 30 min later. Thus the measurementulator still being on, nocebo induced worsening. Placebo suggestions
tti et al., 2003b).
ans of a mnocebo st before tte the stim
hine, the pain increase was larger in the open than in

tifTlnac
wathdwlasiit
etcwaebpctv
aic
Aktarpbwimmep
Ttnshaawfippa
Fp e relapses
F. Benedetti et al. / Neuroscience 147 (2007) 260–271268
he hidden condition (Fig. 5). At 10 h from morphinenterruption, more patients of the open group requestedurther painkillers than the patients of the hidden group.herefore, the hidden interruption of morphine pro-
onged the post-interruption analgesia. The best expla-ation of this difference is that in the open condition, fearnd negative expectations of pain relapse played a cru-ial role.
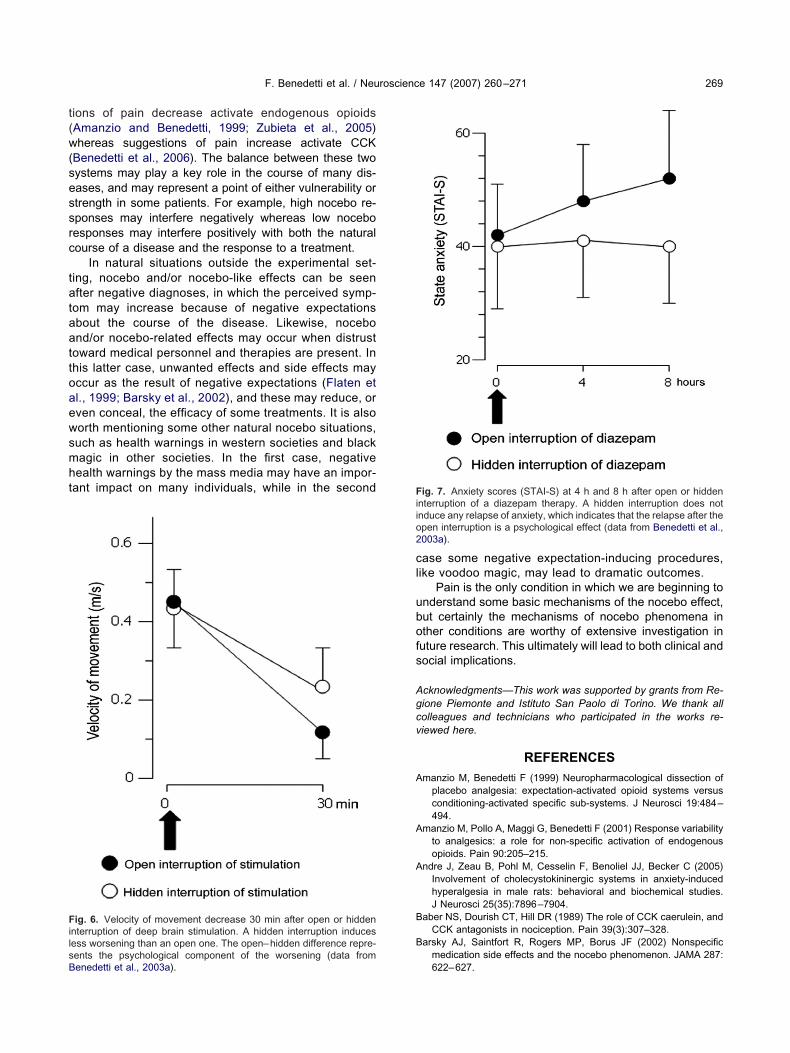
A similar effect was found in Parkinson patients whoere undergoing deep brain stimulation (Benedetti etl., 2003a; Colloca et al., 2004). The stimulator wasurned off either overtly or covertly and the velocity ofand movement assessed. The open interruption in-uced a decrease of movement velocity at 30 min whichas larger than the hidden interruption (Fig. 6). Simi-
arly, in postoperative patients who had undergone di-zepam administration for 48 h, the infusion wastopped either overtly or covertly and their level of anx-ety tested every 4 h. In the open condition, anxietyncreased after 4 and 8 h whereas in the hidden condi-ion it changed neither at 4 nor at 8 h (Fig. 7).
Although no biological mechanism is known for theseffects, these clinical observations are extremely important
o understand how expectations affect the therapeutic out-ome. Furthermore, these clinical data may be integratedith those described above, in which the neuroanatomynd biochemistry of negative expectations and noceboffects are better known. In fact, a hidden interruption isasically an unexpected interruption whereby negative ex-ectations of symptom relapse are absent. In these cir-umstances, patients believe that the treatment is still on,hus their expectation of clinical benefit is still active. Con-
ig. 5. Open versus hidden interruption of a morphine treatment. Theain in the open group but not in the hidden one, thus indicating that thcale (data from Benedetti et al., 2003a and Colloca et al., 2004).
ersely, the open interruption basically tells the patient that n
symptom relapse may be occurring shortly, so that anx-ety about the impending relapse may be critical in thisase.
The clinical impact of these findings is important.lthough doctors should strive to enhance the patient’snowledge about a therapy, it is interesting to note thathis is advantageous only when the therapy is beingdministered. By contrast, if the therapy has to be inter-upted, such awareness might be deleterious for theatient. In fact, the open interruption of morphine, deeprain stimulation and diazepam produces a greaterorsening of the symptoms compared with a hidden
nterruption. Therefore, if the patient is told that a treat-ent is going to be stopped, a nocebo-like phenomenonay occur or, in other words, the expectation of wors-ning may counteract the beneficial effects which areresent after the treatment interruption.
CONCLUSIONS
he concept of nocebo and nocebo-like effects is relatedo that of negative expectation of an outcome. Unfortu-ately, little is known about its neurobiology, althoughome neuroanatomical and neurochemical mechanismsave been unraveled for pain. In particular, anticipatorynxiety about the impending pain has been found to playn important role and to activate the CCKergic systemshich, in turn, facilitate pain transmission. By taking thendings on nocebo and those on placebo together, thelacebo–nocebo phenomenon represents a nice exam-le of how positive and negative expectations about painffect different neurochemical systems, that is, endoge-
ine shows the time of morphine interruption. Note the early relapse ofin the open condition is a psychological effect. NRS�numerical rating
broken l
ous opioids and CCK. More specifically, verbal sugges-
t(w(sessrc
tataattoaewsmht
cl
ubofs
Agcv
A
A
A
B
B
FilsB
Fiio2
F. Benedetti et al. / Neuroscience 147 (2007) 260–271 269
ions of pain decrease activate endogenous opioidsAmanzio and Benedetti, 1999; Zubieta et al., 2005)hereas suggestions of pain increase activate CCK
Benedetti et al., 2006). The balance between these twoystems may play a key role in the course of many dis-ases, and may represent a point of either vulnerability ortrength in some patients. For example, high nocebo re-ponses may interfere negatively whereas low noceboesponses may interfere positively with both the naturalourse of a disease and the response to a treatment.
In natural situations outside the experimental set-ing, nocebo and/or nocebo-like effects can be seenfter negative diagnoses, in which the perceived symp-
om may increase because of negative expectationsbout the course of the disease. Likewise, nocebond/or nocebo-related effects may occur when distrust
oward medical personnel and therapies are present. Inhis latter case, unwanted effects and side effects mayccur as the result of negative expectations (Flaten etl., 1999; Barsky et al., 2002), and these may reduce, orven conceal, the efficacy of some treatments. It is alsoorth mentioning some other natural nocebo situations,uch as health warnings in western societies and blackagic in other societies. In the first case, negativeealth warnings by the mass media may have an impor-ant impact on many individuals, while in the second
ig. 6. Velocity of movement decrease 30 min after open or hiddennterruption of deep brain stimulation. A hidden interruption inducesess worsening than an open one. The open–hidden difference repre-
ents the psychological component of the worsening (data fromenedetti et al., 2003a).ase some negative expectation-inducing procedures,ike voodoo magic, may lead to dramatic outcomes.
Pain is the only condition in which we are beginning tonderstand some basic mechanisms of the nocebo effect,ut certainly the mechanisms of nocebo phenomena inther conditions are worthy of extensive investigation inuture research. This ultimately will lead to both clinical andocial implications.
cknowledgments—This work was supported by grants from Re-ione Piemonte and Istituto San Paolo di Torino. We thank allolleagues and technicians who participated in the works re-iewed here.
REFERENCES
manzio M, Benedetti F (1999) Neuropharmacological dissection ofplacebo analgesia: expectation-activated opioid systems versusconditioning-activated specific sub-systems. J Neurosci 19:484–494.
manzio M, Pollo A, Maggi G, Benedetti F (2001) Response variabilityto analgesics: a role for non-specific activation of endogenousopioids. Pain 90:205–215.
ndre J, Zeau B, Pohl M, Cesselin F, Benoliel JJ, Becker C (2005)Involvement of cholecystokininergic systems in anxiety-inducedhyperalgesia in male rats: behavioral and biochemical studies.J Neurosci 25(35):7896–7904.
aber NS, Dourish CT, Hill DR (1989) The role of CCK caerulein, andCCK antagonists in nociception. Pain 39(3):307–328.
arsky AJ, Saintfort R, Rogers MP, Borus JF (2002) Nonspecificmedication side effects and the nocebo phenomenon. JAMA 287:
ig. 7. Anxiety scores (STAI-S) at 4 h and 8 h after open or hiddennterruption of a diazepam therapy. A hidden interruption does notnduce any relapse of anxiety, which indicates that the relapse after thepen interruption is a psychological effect (data from Benedetti et al.,003a).
622–627.

B
B
B
B
B
B
B
B
B
B
B
B
B
C
C
C
C
C
D
d
D
D
F
F
F
G
G
G
H
H
H
H
H
H
H
H
H
K
K
K
K
K
K
L
L
F. Benedetti et al. / Neuroscience 147 (2007) 260–271270
einfeld MC (1983) Cholecystokinin in the central nervous system: aminireview. Neuropeptides 3(6):411–427.
enedetti F, Amanzio M, Maggi G (1995) Potentiation of placeboanalgesia by proglumide. Lancet 346:1231.
enedetti F (1996) The opposite effects of the opiate antagonistnaloxone and the cholecystokinin antagonist proglumide on pla-cebo analgesia. Pain 64:535–543.
enedetti F (1997) Cholecystokinin type-A and type-B receptorsand their modulation of opioid analgesia. News Physiol Sci 12:263–268.
enedetti F, Amanzio M (1997) The neurobiology of placeboanalgesia: from endogenous opioids to cholecystokinin. ProgrNeurobiol 52:109–125.
enedetti F, Amanzio M, Vighetti S, Asteggiano G (2006) The bio-chemical and neuroendocrine bases of the hyperalgesic noceboeffect. J Neurosci 26(46):12014–12022.
enedetti F, Amanzio M, Casadio C, Oliaro A, Maggi G (1997) Block-ade of nocebo hyperalgesia by the cholecystokinin antagonistproglumide. Pain 71:135–140.
enedetti F, Arduino C, Amanzio M (1999) Somatotopic activation ofopioid systems by target-directed expectations of analgesia.J Neurosci 19:3639–3648.
enedetti F, Colloca L, Torre E, Lanotte M, Melcarne A, Pesare M,Bergamasco B, Lopiano L (2004) Placebo-responsive Parkinsonpatients show decreased activity in single neurons of subthalamicnucleus. Nat Neurosci 7:587–588.
enedetti F, Colloca L (2004) Placebo-induced analgesia: methodol-ogy, neurobiology, clinical use, and ethics. Rev Analg 7:129–143.
enedetti F, Maggi G, Lopiano L, Lanotte M, Rainero I, Vighetti S,Pollo A (2003a) Open versus hidden medical treatments: the pa-tient’s knowledge about a therapy affects the therapy outcome.Prevent Treat. Available online at: http://journals.apa.org/prevention/volume6/toc-jun-03.html.
enedetti F, Pollo A, Lopiano L, Lanotte M, Vighetti S, Rainero I(2003b) Conscious expectation and unconscious conditioning inanalgesic, motor and hormonal placebo/nocebo responses. J Neu-rosci 23:4315–4323.
enedetti F, Mayberg HS, Wager TD, Stohler CS, Zubieta JK (2005)Neurobiological mechanisms of the placebo effect. J Neurosci25(45):10390–10402.
hiodo LA, Bunney BS (1983) Proglumide: selective antagonism ofexcitatory effects of cholecystokinin in the central nervous system.Science 219(4591):1449–1451.
hua P, Krams M, Toni I, Passingham R, Dolan R (1999) A functionalanatomy of anticipatory anxiety. Neuroimage 9 (6 Pt 1):563–571.
olloca L, Lopiano L, Lanotte M, Benedetti F (2004) Overt versuscovert treatment for pain, anxiety, and Parkinson’s disease. LancetNeurol 3(11):679–684.
olloca L, Benedetti F (2005) Placebos and painkillers: is mind asreally as matter? Nat Rev Neurosci 6(7):545–552.
rawley JN, Corwin RL (1994) Biological actions of cholecystokinin.Peptides 15(4):731–755.
annecker EA, Price DD, Robinson ME (2003) An examination of therelationships among recalled, expected, and actual intensity andunpleasantness of delayed onset muscle pain. J Pain 4(2):74–81.
e la Fuente-Fernandez R, Ruth TJ, Sossi V, Schulzer M, Calne DB,Stoessl AJ (2001) Expectation and dopamine release: mechanismof the placebo effect in Parkinson’s disease. Science 293:1164–1166.
ourish CT, Hawley D, Iversen SD (1988) Enhancement of morphineanalgesia and prevention of morphine tolerance in the rat by thecholecystokinin antagonist L-364,718. Eur J Pharmacol 147:469–472.
workin SF, Chen AC, LeResche L, Clark DW (1983) Cognitive re-versal of expected nitrous oxide analgesia for acute pain. Anesth
Analg 62:1073–1077.inniss DG, Benedetti F (2005) Mechanisms of the placebo responseand their impact on clinical trials and clinical practice. Pain114:3–6.
laten MA, Simonsen T, Olsen H (1999) Drug-related informationgenerates placebo and nocebo responses that modify the drugresponse. Psychosom Med 61(2):250–255.
rith C, Dolan RJ (1997) Brain mechanisms associated with top-downprocesses in perception. Philos Trans R Soc Lond B Biol Sci352(1358):1221–1230.
all C, Lauterborn J, Burks D, Seroogy K (1987) Co-localization ofenkephalin and cholecystokinin in discrete areas of rat brain. BrainRes 403(2):403–408.
ibbins IL, Furness JB, Costa M (1987) Pathway-specific patterns ofthe co-existence of substance P, calcitonin gene-related peptide,cholecystokinin and dynorphin in neurons of the dorsal root gangliaof the guinea-pig. Cell Tissue Res 248(2):417–437.
revert P, Albert LH, Goldstein A (1983) Partial antagonism of placeboanalgesia by naloxone. Pain 16:129–143.
ahn RA (1985) A sociocultural model of illness and healing. In: L.White, Tursky, B., Schwartz, G.E. (eds.), Placebo: Theory, Re-search, and Mechanisms, Guilford, New York, pp. 332–350.
ahn RA (1997) The nocebo phenomenon: concept, evidence, andimplications for public health. Prev Med 26(5 Pt 1):607–611.
arro J, Pold M, Vasar E (1990) Anxiogenic-like action of caerulein, aCCK-8 receptor agonist, in the mouse: influence of acute andsubchronic diazepam treatment. Naunyn Schmiedebergs ArchPharmacol 341(1–2):62–67.
arro J, Vasar E (1991) Evidence that CCK-B receptors mediate theregulation of exploratory behaviour in the rat. Eur J Pharmacol193(3):379–381.
ebb ALO, Poulin J-F, Roach SP, Zacharko RM, Drolet G (2005)Cholecystokinin and endogenous opioid peptides: interactive influ-ence on pain, cognition, and emotion. Prog Neuropsychopharma-col Biol Psychiatry 29:1225–1238.
einricher MM, McGaraughty S, Tortorici V (2001) Circuitry underlyingantiopioid actions of cholecystokinin within the rostral ventromedialmedulla. J Neurophysiol 85:280–286.
einricher MM, Neubert MJ (2004) Neural basis for the hyperalgesicaction of cholecystokinin in the rostral ventromedial medulla.J Neurophysiol 92:1982–1989.
offman GA, Harrington A, Fields HL (2005) Pain and the placebo:what we have learned. Perspect Biol Med 48(2):248–265.
sieh JC, Stone-Elander S, Ingvar M (1999) Anticipatory coping ofpain expressed in the human anterior cingulated cortex: a positronemission tomography study. Neurosci Lett 26: 262(1):61–64.
antor TG, Sunshine A, Laska E, Meisner M, Hopper M (1966) Oralanalgesic studies: pentazocine hydrochloride, codeine, aspirin,and placebo and their influence on response to placebo. ClinPharmacol Ther 7(4):447–454.
eltner JR, Furst A, Fan C, Redfern R, Inglis B, Fields HL (2006)Isolating the modulatory effect of expectation on pain transmission:a functional magnetic resonance imaging study. J Neurosci26(16):4437–4443.
ennedy WP (1961) The nocebo reaction. Med Exp Int J Exp Med95:203–205.
issel P, Barrucand D (1964) Placebos et effect placebo en medicine.Paris: Masson.
oyama T, Tanaka YZ, Mikami A (1998) Nociceptive neurons in themacaque anterior cingulated activate during anticipation of pain.Neuroreport 9(11):2663–2667.
oyama T, McHaffie JG, Laurienti PJ, Coghill RC (2005) The subjec-tive experience of pain: where expectations become reality. ProcNatl Acad Sci U S A 102(36):12950–12955.
aska E, Sunshine A (1973) Anticipation of analgesia. A placeboeffect. Headache 13(1):1–11.
avigne GJ, Hargreaves KM, Schmidt EA, Dionne RA (1989) Proglu-mide potentiates morphine analgesia for acute postsurgical pain.
Clin Pharmacol Ther 45(6):666–673.
L
L
L
L
M
M
M
M
M
N
N
P
P
P
P
P
P
P
P
P
P
P
S
S
S
V
V
v
W
W
W
W
X
Z
F. Benedetti et al. / Neuroscience 147 (2007) 260–271 271
euchter AF, Cook IA, Witte EA, Morgan M, Abrams M (2002)Changes in brain function of depressed subjects during treatmentwith placebo. Am J Psychiatry 159:122–129.
evine JD, Gordon NC, Fields HL (1978) The mechanism of placeboanalgesia. Lancet 2(8091):654–657.
evine JD, Gordon NC, Smith R, Fields HL (1981) Analgesic re-sponses to morphine and placebo in individuals with postoperativepain. Pain 10(3):379–389.
orenz J, Hauck M, Paur RC, Nakamura Y, Zimmermann R, Bromm B,Engel AK (2005) Cortical correlates of false expectations duringpain intensity judgments: a possible manifestation of placebo/no-cebo cognitions. Brain Behav Immun 19(4):283–295.
aldonado R, Derrien M, Noble F, Roques BP (1993) Association ofthe peptidase inhibitor RB 101 and CCK-B antagonist stronglyenhances antinociceptive responses. Neuroreport 4(7):947–950.
ayberg HS, Silva JA, Brannan SK, Tekell JL, Mahurin RK, McGinnisS, Jerabek PA (2002) The functional neuroanatomy of the placeboeffect. Am J Psychiatry 159(5):728–737.
ercado R, Constantoyannis C, Mandat T, Kumar A, Schulzer M,Stoessl AJ, Honey CR (2006) Expectation and the placebo effect inParkinson’s disease patients with subthalamic nucleus deep brainstimulation. Mov Disord 21(9):1457–1461.
esulam MM (1998) From sensation to cognition. Brain 121 (Pt6):1013–1052.
itchell JM, Lowe D, Fields HL (1998) The contribution of the rostralventromedial medulla to the antinociceptive effects of systemicmorphine in restrained and unrestrained rats. Neuroscience87:123–133.
oble F, Derrien M, Roques BP (1993) Modulation of opioid antinoci-ception by CCK at the supraspinal level: evidence of regulatorymechanisms between CCK and enkephalin systems in the controlpain. Br J Pharmacol 109(4):1064–1070.
oble F, Wank SA, Crawley JN, Bradwejn J, Seroogy KB, Hamon M,Roques BP (1999) International Union of Pharmacology. XXI.Structure, disribution, and functions of cholecystokinin receptors.Pharmacol Rev 51:745–781.
acheco-Lopez G, Engler H, Niemi MB, Schedlowski M (2006) Ex-pectations and associations that heal: immunomodulatory placeboeffects and its neurobiology. Brain Behav Immun 20(5):430–446.
essoa L, Kastner S, Ungerleider LG (2003) Neuroimaging studies ofattention: from modulation of sensory processing to top-down con-trol. J Neurosci 23(10):3990–3998.
etrovic P, Kalso E, Petersson KM, Ingvar M (2002) Placebo andopioid analgesia: imaging a shared neuronal network. Science295(5560):1737–1740.
loghaus A, Tracey I, Gati JS, Clare S, Menon RS, Matthews PM,Rawlins JN (1999) Dissociating pain from its anticipation in thehuman brain. Science 284(5422):1979–1981.
ollo A, Torre E, Lopiano L, Rizzone M, Lanotte M, Cavanna A,Bergamasco B, Benedetti F (2002) Expectation modulates theresponse to subthalamic nucleus stimulation in Parkinsonian pa-tients. Neuroreport 13(11):1383–1386.
orro CA, Baraldi P, Pagnoni G, Serafini M, Facchin P, Maieron M,Nichelli P (2002) Does anticipation of pain affect cortical nocicep-tive systems? J Neurosci 22(8):3206–3214.
orro CA, Cettolo V, Francescato MP, Baraldi P (2003) Functionalactivity mapping of the mesial hemispheric wall during anticipation
of pain. Neuroimage 19(4):1738–1747.rice DD, von der Gruen A, Miller J, Rafii A, Price C (1985) Potenti-ation of systemic morphine analgesia in humans by proglumide, acholecystokinin antagonist. Anesth Analg 64(8):801–806.
rice DD (2000) Psychological and neural mechanisms of the affectivedimension of pain. Science 288(5472):1769–1772.
rice DD (2001) Assessing placebo effects without placebo groups: anuntapped possibility? Pain 90(3):201–203.
rice DD, Craggs J, Nicholas Verne G, Perlstein WM, Robimson ME(2006) Placebo analgesia is accompanied by large reductions inpain-related brain activity in irritable bowel syndrome patients. Pain127(1–2):63–72.
awamoto N, Honda M, Okada T, Hanakawa T, Kanda M, FukuyamaH, Konishi J, Shibasaki H (2000) Expectation of pain enhancesresponses to nonpainful somatosensory stimulation in the anteriorcingulated cortex and parietal operculum/posterior insula: anevent-related functional magnetic resonance imaging study.J Neurosci 20(19):7438–7445.
tengaard-Pedersen K, Larsson LI (1981) Localization and opiatebinding of enkephalin, CCK and ACTH/beta-endorphin in the ratcentral nervous system. Peptides 2 (Suppl 1):3–19.
uberg SN, Culhane ES, Carstens E, Watkins LR (1985) Behavioraland electrophysiological investigations of opiate/cholecystokinininteractions. In: Advances in pain research and therapy, Vol 9(Fields HL, Dubner R, Cervero F, eds), pp 541–553. New York:Raven.
alverde O, Maldonado R, Fournie-Zaluski MC, Roques BP (1994)Cholecystokinin B antagonists strongly potentiate antinociceptionmediated by endogenous enkephalins. J Pharmacol Exp Ther270(1):77–88.
anderhaeghen JJ, Signeau JC, Gepts W (1975) New peptide in thevertebrate CNS reacting with antigastrin antibodies. Nature257(5527):604–605.
an Megen HJ, den Boer JA, Westenberg HG (1994) On the signifi-cance of cholecystokinin receptors in panic disorder. Prog Neuro-psychopharmacol Biol Psychiatry 18(8):1235–1246.
ager TD, Rilling JK, Smith EE, Sokolik A, Casey KL, Davidson RJ,Kosslyn SM, Rose RM, Cohen JD (2004) Placebo-inducedchanges in FMRI in the anticipation and experience of pain. Sci-ence 303(5661):1162–1167.
atkins LR, Kinscheck IB, Mayer DJ (1985a) Potentiation of morphineanalgesia by the cholecystokinin antagonist proglumide. Brain Res327(1–2):169–180.
atkins LR, Kinscheck IB, Kaufman EF, Miller J, Frenk H, Mayer DJ(1985b) Cholecystokinin antagonists selectively potentiate analge-sia induced by endogenous opiates. Brain Res 327(1–2):181–190.
iesenfeld-Hallin Z, Xu XJ, Hughes J, Horwell DC, Hokfelt T (1990)PD134308, a selective antagonist of cholecystokinin type B recep-tor, enhances the analgesic effect of morphine and synergisticallyinteracts with intrathecal galanin to depress spinal nociceptivereflexes. Proc Natl Acad Sci U S A 87(18):7105–7109.
u XJ, Hokfelt T, Hughes J, Wiesenfeld-Hallin Z (1994) The CCK-Bantagonist CI988 enhances the reflex-depressive effect of mor-phine in axotomized rats. Neuroreport 5(6):718–720.
ubieta JK, Bueller JA, Jackson LR, Scott DJ, Xu Y, Koeppe RA,Nichols TE, Stohler C (2005) Placebo effects mediated by endog-enous opioid activity on �-opioid receptors. J Neurosci 25(34):
7754–7762.(Accepted 13 February 2007)(Available online 26 March 2007)