Embed Size (px)
Citation preview

A STUDY TO ASSESS THE EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE OF STAFF NURSES REGARDING
SELECTED ALTERNATIVE AND CONTEMPORARY MODALITIES OF PAIN RELIEF DURING
FIRST STAGE OF LABOUR IN SELECTED MATERNITY
HOSPITALS, BANGALORE
By
SHANTI SONU SAM
Dissertation Submitted to
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, BANGALORE, KARNATAKA
IN PARTIAL FULFILLMENTOF THE REQUIREMENTS FOR THE DEGREE OF
MASTER OF SCIENCEIN
OBSTETRICS AND GYNAECOLOGICAL NURSING
Under the guidance ofMrs. Gowri Sayee
Associate Professor & HODDepartment of Obstetrics and Gynaecological Nursing
FORTIS INSTITUTE OF NURSING20/5, Yelachenahalli, Kanakapura road, Bangalore-560078
YEAR2010-2012
1

Rajiv Gandhi University Of Health Sciences, Bangalore, Karnataka.
DECLARATION BY THE CANDIDATE
I hereby declare that this thesis entitled “A STUDY TO
ASSESS THE EFFECTIVENESS OF STRUCTURED TEACHING
PROGRAMME ON KNOWLEDGE OF STAFF NURSES
REGARDING SELECTED ALTERNATIVE AND CONTEMPORARY
MODALITIES OF PAIN RELIEF DURING FIRST STAGE OF
LABOUR IN SELECTED MATERNITY HOSPITALS,
BANGALORE.” is a bonafide and genuine research work carried out by me
under the guidance of Mrs. Gowri Sayee, Associate professor and HOD,
Department of obstetrics and gynaecology, Fortis institute of nursing,
Bangalore.
Signature of Candidate
SHANTI SONU SAM
Date:
Bangalore:
2
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation titled “A STUDY TO
ASSESS THE EFFECTIVENESS OF STRUCTURED TEACHING
PROGRAMME ON KNOWLEDGE OF STAFF NURSES
REGARDING SELECTED ALTERNATIVE AND CONTEMPORARY
MODALITIES OF PAIN RELIEF DURING FIRST STAGE OF
LABOUR IN SELECTED MATERNITY HOSPITALS,
BANGALORE.” is a bonafide research work done by Ms. Shanti Sonu
Sam in partial fulfilment of the requirement for the degree of Masters of
Science in Nursing (Obstetrics and Gynaecology).
Signature of Guide:
Mrs. Gowri SayeeAssociate professor& HODObstetrics and gynaecological nursingFortis institute of nursingBangalore- 560078
Date:
Bangalore
3
ENDORSEMENT BY THE
HOD, PRINCIPAL/ HOD OF THE INSTITUTION .
This is to certify that the dissertation entitled “A STUDY TO
ASSESS THE EFFECTIVENESS OF STRUCTURED TEACHING
PROGRAMME ON KNOWLEDGE OF STAFF NURSES
REGARDING SELECTED ALTERNATIVE AND CONTEMPORARY
MODALITIES OF PAIN RELIEF DURING FIRST STAGE OF
LABOUR IN SELECTED MATERNITY HOSPITALS,
BANGALORE.” is a bonafide research work done by Ms. Shanti Sonu
Sam under the guidance of Mrs. Gowri Sayee, Department of Obstetrics
and Gynaecological Nursing, Fortis institute of nursing, Bangalore.
Signature of the HOD Signature of the Principal
Mrs. GOWRI SAYEE Prof. SRIDHAR K.V
Associate Professor
Date: Date:
Bangalore Bangalore
4

COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall have the right to preserve, use and disseminate this
dissertation thesis in print or electronic format for academic or research
purposes.
Signature of the candidate:
Shanti Sonu Sam
Date:
Bangalore
© Rajiv Gandhi University of Health Sciences, Karnataka
5
ACKNOWLEDGEMENTS
“Every good thing given and every perfect gift is from above, coming down
from the Father of lights, with whom there is no variation or shifting
shadow”.
(James 1: 17)
First and foremost I would like to thank the supreme teacher of all:
God. I know that I am here and that I am able to write all of this for a
reason. I will do my best in never forgetting what a great fortune I have had
in just being here, and that it comes with a lesson and a responsibility. I
hope I am doing the work you have planned me to do.
I extend my heartfelt thanks to my respected
teacher and guide Mrs. Gowri Sayee Associate professor,
HOD, Department of Obstetrics and gynecological nursing,
Fortis Institute of Nursing, Bangalore. Her appropriate
guidance, even support, encouragement, priceless
suggestions and co-operation has continually motivated me
for the successful achievement of this dissertation.
I express my profound and sincere thanks to our
beloved principal Prof. Shridhar K.V, Principal, HOD,
Department of Medical Surgical Nursing, Fortis Institute of
6

Nursing, Bangalore. His encouragement, guidance, valuable
suggestions and untiring effort which has motivated me
throughout the study. His personal interest, endless
patience, love and blessing have been the foundation of this
study.
I owe my earnest gratitude and sincere thanks
to my teacher and co-guide Mrs. Sabitha Sibbala
Associate professor, Department of Obstetrics and
gynecological nursing, Fortis Institute of Nursing, Bangalore.
I am thankful for her valued guidance, kind support and
judicious help which enabled me to complete my study
successfully.
My heartfelt gratitude to our class coordinator,
Dr. Mrs. Thressiamma P.M, vice principal HOD,
Department of Community health Nursing, Fortis Institute of
Nursing, Bangalore. I am thankful for her venerated
guidance and constant support which enabled me to
complete my study successfully.
A word of thanks to Mr. Prabhuswamy A C,
associate professor, Department of medical surgical nursing,
7
Fortis Institute of Nursing, Bangalore, for his help in
completing my study.
With great proud and privilege, I express my
profound sense of
gratitude and heart full thanks to all my P.G. Faculty,
Fortis Institute of
Nursing, Bangalore for the fathomless guidance, constant
availability,
intuitive suggestions, motivation and support rendered
throughout my
study.
I am deeply indebted to all the experts who
contributed the time and effort towards validating and
refining the tools used in the present study.
I owe my gratitude to all the subjects who
enthusiastically participated in carrying out the research
project.
I express my sincere thanks to the Nursing
Superintendent, Fortis hospitals, Bangalore Mrs.
Kavitha Biswas for giving me the authorization to conduct
8

the study among staff nurses in their revered institution. I
thank the nursing in-charges of LDRP ward and 6th level of
Fortis hospital for their help in arranging the classes.
A word of acclamation is to Mr. Arun, Asst.
Professor, Manjunath college of arts and science, a
prominent statistician who has helped me in the analysis of
data of my research study.
I pay my obliged salutations to my parents Rev. Fr
K. P. Sam and Mrs. Anitha Sam for their prayers and
blessings. I extend my love to my siblings Ms. Shalin
mary sam and Mr. Alwin sam for their support and best
wishes that helped me to carry out my study successfully.
There are many more people who have worked behind
the screen in their own loving way to help me accomplish
this task. Special word of thanks to my classmate and
dear friend Mrs. Reena stephen for her sensible help and
suggestions. I thank all my friends especially my friends
Ms. Navreet Virk and Mrs. Bincy Thomas for their
support and prayers.
9

There are many to whom I am yet to show gratitude
because all those who have helped in time have become
priceless charms.
Signature of the
candidate
(Ms.
Shanti Sonu Sam)
Date:Bangalore.
10

LIST OF ABBREVIATIONS USED
GNM GENERAL NURSING AND MIDWIFERY
B.Sc BACHELOR OF SCIENCE
STP STRUCTURED TEACHING PROGRAMME
SD STANDARD DEVIATION
S SIGNIFICANT
NS NON-SIGNIFICANT
df DEGREES OF FREEDOM
PPT POWER POINT PRESENTATION
11

ABSTRACT
“It is refreshing to know that for all the billions of times it has occurred,
the birth of a child, like the wonder inspired by a sunset, can never be
tarnished by repetition”
Background
Motherhood is one of life’s greatest blessings. It is a lifelong event
that forever changes woman into a mother. But the mother also has to go
through enormous pain during this process of transition from a woman to a
mother. As an expectant mother reaches her due date, a concern that looms
large in her mind is the pain that she will experience during labour.
Childbirth is a significant, though stressful event. A woman who is able to
cope with the stress of the labour tends to feel more satisfied with her
experience; an experience that is positive and has satisfying perceptions of
childbirth.
An ideal labour pain relief method should meet the following criteria:
having the least possible side effects for mother and fetus, having permanent
effect, could be administered easily, having appropriate sedative effect
without intervening the uterine contractures. Alternative and contemporary
12

modalities during delivery would lead to relaxation and consequently, a
rapid and easy delivery.
Midwives are the primary care takers who are with the labouring
woman throughout the process of labour. Hence they should be educated
about these alternative modalities and it should be applied in our hospitals.
A teaching programme on selected alternative modalities can promote the
use of these modalities during first stage of labour.
Statement of the problem
“A STUDY TO ASSESS THE EFFECTIVENESS OF
STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE OF
STAFF NURSES REGARDING SELECTED ALTERNATIVE AND
CONTEMPORARY MODALITIES OF PAIN RELIEF DURING FIRST
STAGE OF LABOUR IN SELECTED MATERNITY HOSPITALS,
BANGALORE”
Objectives of the study
1. To assess the pre-test knowledge scores of staff nurses regarding
alternative and contemporary modalities of pain relief during first
stage of labour.
13

2. To find out the effectiveness of structured teaching programme regarding
alternative and contemporary modalities of pain relief during first
stage of labour by assessing post-test knowledge scores of staff
nurses.
3. To find out the association between pre-test knowledge scores and
selected demographic variables.
Methods
Conceptual framework of the study is based on Von Ludwig
Bertalanaffy’s general system’s theory. Based on the problem selected and
objective of the study quasi-experimental one group pre-test post-test design
without control group was selected.
A sample of 60 staff nurses working in OBG department of Fortis
hospital, Bangalore were selected by non-probability sampling technique.
Data was collected by administering structured questionnaire before and
after the implementation of structured teaching programme. Data were
analysed using descriptive and inferential statistics and represented in graphs
and tables.
14

Results
In the present study 86.7% of the respondents had inadequate
knowledge regarding alternative and contemporary modalities before the
implementation of structured teaching programme. But after the
implementation of structured teaching programme 15% of them had
moderately adequate knowledge and 85% of them had adequate knowledge
The mean pre-test scores of 40.42% was higher than the mean post-
test scores of 80.50% which was significant at P-value of 0.001 level which
showed significant increase in knowledge and thus it proves the
effectiveness of the structured teaching programme.
In the preset study the knowledge scores of staff nurses were found to
be non-significant with the demographic variables i.e. age, qualification,
experience, religion. Hence it indicates that there is no association between
the knowledge scores of nurses and the selected demographic variables.
Interpretation and conclusion
The study showed that there was a significant improvement in the
knowledge scores after the administration of structured teaching programme.
Hence it can be concluded that the structured teaching programme was
15

effective in improving the knowledge of staff nurses on alternative and
contemporary modalities of pain relief during first stage of labour.
KEY WORDS: Structured teaching programme, effectiveness,
knowledge, alternative and contemporary modalities
16
TABLE OF CONTENTS
NO. CHAPTER PAGE
1. INTRODUCTION 1-9
2. OBJECTIVES 10-15
3. REVIEW OF LITERATURE 16-24
4. METHODOLOGY 25-40
5. RESULTS 41-64
6. DISCUSSION 65-68
7. CONCLUSION 69-72
8. SUMMARY 73-77
9. BIBLIOGRAPHIC REFERENCES 78-81
10. ANNEXURES 82-137
LIST OF TABLES
17

TABLE NUMBE
RTITLE OF TABLE PAGE
NUMBER
1. Design chosen for the study. 26
2. Distribution of respondents according to age. 43
3. Distribution of respondents according to qualification. 45
4. Distribution of respondents according to experience. 47
5. Distribution of respondents according to religion. 49
6. Distribution of respondents according to pre-test and post-test knowledge scores 51
7.Area wise distribution of mean, mean percentage and standard deviation of pre-test knowledge scores of the respondents.
54
8.Area wise distribution of mean, mean percentage and standard deviation of post-test knowledge scores of the respondents.
57
9.Paired ‘t’ test showing the significant difference between mean pre-test and mean post-test knowledge scores of the respondents
60
10.Association between pre-test knowledge scores of the respondents with selected demographic variables.
63
LIST OF FIGURES
18

FIGURE NUMBER
TITLE OF FIGURE PAGE NUMBER
1. Conceptual framework of the study 15
2. Schematic representation of research methodology 28
3. Cylindrical diagram showing distribution of respondents according to age. 44
4. Pie chart showing distribution of respondents according to qualification 46
5. Pyramid diagram showing distribution of respondents according to experience 48
6. Pie chart showing distribution of respondents according to religion 50
7.Cylindrical diagram showing distribution of staff nurse according to pre-test and post-test knowledge scores
53
8.
Bar diagram showing area wise distribution of mean, mean percentage and standard deviation of pre-test knowledge scores of staff nurses.
56
9.
Bar diagram showing area wise distribution of mean, mean percentage and standard deviation of post-test knowledge scores of staff nurses.
59
10.Cylindrical diagram showing the significant difference between mean pre-test and mean post-test knowledge scores of staff nurses
62
19

LIST OF ANNEXURES
ANNEXURE NO. TITLE OF ANNEXURE PAGE
NO.
A Ethical clearance certificate 82
B Letter seeking permission to conduct the study 83
C Letter requesting consent to validate the tool 84
D Acceptance form for tool validation 86
E Content validation certificate 87
F Letter to the participants requesting consent to participate in the study 88
G List of experts for tool validation 90
H Blue print of distribution of items 92
I Tool for data collection 93
J
Structured teaching programme on alternative and contemporary modalities of pain relief during first stage of labour.
109
20

1. INTRODUCTION
“To her who loves us before she meets.”
-An inscription in Mexico City.
The foundation for the whole humankind is the art of motherhood. Mother is the
greatest gift to the world.1 Every woman is a mother and she should be respected.
Childbirth is an intense event and strong emotions both positive and negative can be
brought to the surface. Childbirth is a divine process and women should be supported
during labor.2
Genesis 3:16 says, “I will greatly multiply your sorrows and your conception, in
pain you shall bring forth children” as said to eve the first woman created. This was the
background of labor pain in biblical terms.
Childbirth is a magnificent event with meaning far beyond the actual physiologic
process. Normal labour can be defined as a series of events that take place in the genital
organs in an effort to expel the viable products of conception out of the womb through
the vagina into the outer world. Normal labour occurs between 37 and 42 weeks of
gestation.3
Conventionally, the events of labour are divided into four stages. First stage starts
from the onset of true labour pain and ends with full dilatation of cervix. It is in other
words, the “cervical stage” of labour. Second stage of labour starts with full dilatation of
cervix and ends with the expulsion of fetus. Third stage begins after the expulsion of
21

fetus and ends with the expulsion of placenta and membranes. Fourth stage is the stage of
observation of at least one hour after the expulsion of placenta and membranes.3
The first symptom to appear in first stage of labour is intermittent painful uterine
contractions followed by expulsion of bloody mucous per vagina. The first stage of
labour is characterized by noticeable cervical changes as a result of uterine contractions.
The cervix softens, thins, shortens and opens to a diameter of 10 cm. These changes are
referred to as effacement and dilatation. The first stage is characterized by several
physical and psychological changes of which the most important one to be managed is
the pain due to intermittent uterine contractions.4
During the process of giving birth to new life, the mother has to undergo
enormous pain. Labor pain is an unpleasant, complex, highly individualized phenomenon
with both sensory and emotional components. Childbirth while primarily a joyful event
predisposes the mother to one of the most severe form of pain ever reported.5
The causes of labor pain can be either physical or psychological. Physical factors
include uterine contractions, cervical dilatations, cervical effacements etc. Psychological
factors include fear and anxiety, previous experiences, inadequate support, inadequate
knowledge. Pain perceived during labor may be different for each woman.4
Pain relief is the way in which women feel that they have coped with pain during
labor. It is an essential part in good obstetric care. This involves the use of
pharmacological and non-pharmacological or alternative methods of pain relief. Some of
them are sedatives and analgesics, inhalation agents, general anesthesia, epidural
analgesia, alternative and contemporary modalities. Due to its widespread popularity and
22

proved effectiveness alternative and contemporary modalities should be made available
to every mother.
Alternative and contemporary modalities are simple, safe and inexpensive. It
considers the human body as the sum total of its physical, mental, social and spiritual
dimensions. It has no side effects. Remedies are based on natural ingredients thereby
advocating a drugless cure. Alternative modalities are simple to practice and easily
affordable. Preventive and promotive aspects are accorded equal emphasis in alternative
modalities.6
Midwifery, a field where the mother is viewed as a whole being requires the
practice of alternative and contemporary modalities in reducing labor pain. The
effectiveness of alternative modalities is proved by various studies. Alternative
modalities help the woman to maintain a sense of personal control over birth process.7
Alternative and contemporary modalities include a wide variety of techniques to
address not only the physical sensations of pain but also to prevent suffering by
enhancing psycho-emotional and spiritual components of care.8 Rather than making the
pain disappear, these modalities build self confidence and maintain a sense of well being
in the mother. The mother can attain mastery over pain management with these
modalities.9 The woman is supported and guided in using these modalities to minimize
pain and enhance the progress of labor.
Alternative and contemporary modalities offer lots of possibilities for relieving
pain and can be combined with each other. These modalities do not actively interfere
with labor progress but in some cases can enhance progress or effectiveness of pushing.
23

These modalities promote a sense of accomplishment and capability, which can be more
critical to a satisfying childbirth experience than pain relief. Unlike pain medications they
can be discontinued immediately if they don’t help or in the unlikely event that they
cause a problem.9
Different alternative and contemporary modalities used are: continuous labor
support, hydrotherapy, intra-dermal water blocks, positioning and movement, touch and
massage, acupressure, acupuncture, hypnosis, trans-cutaneous electric nerve stimulation,
aromatherapy, hot and cold application, breathing and relaxation, music, audio analgesia,
birth balls.10
A women experiences great pain during labor and she needs physical and
emotional support to pass over this plateau. A midwife is the ideal person to assist the
woman in this crucial period, combining her skills and knowledge with abundant
humanity.2 The topic of labor pain management occupies a unique place in the evaluation
of effectiveness of maternity care.8
The mother should also be provided with evidence based information on all
these alternative modalities during antenatal period itself. Alternative modalities reduce
suffering by empowering the women to utilize her coping strategies.9
Alternative modalities should be adopted according to the women’s need and
expanding options available should be a primary focus of maternity care. The main goal
should be to provide a safe and acceptable alternative to women.
24
In present study five main modalities namely aromatherapy, touch and massages,
breathing exercises, intra-dermal water block, and hydrotherapy are selected and a
structured teaching programme is given to nurses working in the maternity department.
Aromatherapy is the science of using highly concentrated essential oils or
essences distilled from plants in order to utilize their therapeutic properties. Massaging is
a simple technique of rubbing and kneading painful body muscles. Massages relieve
contraction discomfort as well as aches and pains from tension and long hours of labor.
Hydrotherapy is the method of using water to minimize labour pain and ease birth.7
Breathing exercises use learned breathing patterns to aid the woman’s relaxation
efforts and also helps her to distract from the painful response. Breathing exercises allows
her uterus to do its work without any added effort or waste of energy. Intra-dermal water
block is a new technique for non-narcotic pain relief in which four tiny (0.1ml) injections
of sterile water are administered intra-dermally around the sacrum or lower back.7
These modalities are very effective in minimizing pain during first stage of
labour. Midwives are with the mother during the entire process of labour and hence they
are at a position to provide relief to the woman from labour pain. Hence the investigator
wishes to select them to provide an educational programme on the selected alternative
modalities of pain relief with a view of stressing the importance of understanding and
applying these modalities in order to accelerate the standards of midwifery services
provided.
25
Need for the study
Childbirth has a deep significance not only to mother and her partner but also to
the whole family. It is a profound physiological, psychosocial and spiritual event. It is
this joy and expectation from the entire family that drives the mother to face the pain and
all the suffering associated with it.5
The management of labor pain is one of the main goals of maternity care.
Although pain and suffering occur together, one may suffer without pain or have pain
without suffering. The goal of eliminating labor pain not only requires pain medication
but also require other techniques/modalities to preserve health and maintain coping
strategies. This requires highly skilled personnel to control any undesirable side effects.
The effectiveness of most widely used alternative modalities is discussed with a view to
educate the primary care providers, the midwives.8
A systematic review on non-pharmacological approaches to relieve labor pain and
sufferings was conducted in university of Mexico. A systematic review on randomized
trials was conducted and thirteen methods were found to be effective. Systematic review
of randomized controlled trial of methods like continuous labor support, hydrotherapy,
intra-dermal water blocks, movement and positioning, touch and massage, acupuncture,
hypnosis, transcutaneous electric nerve stimulation, aromatherapy, heat and cold,
childbirth education, self-help techniques such as breathing and relaxation, music and
audio analgesia were taken.8
A study to assess the effectiveness of non-pharmacological aspects in relieving labor
pain was conducted in a public maternity centre in Brazil. Clinical trials were taken
26

before and after therapeutic interventions like hydrotherapy, massages, hot and cold
applications, accupressure, trans-cutaneous electric nerve stimulation, aromatherapy etc.
It was conducted among parturients (n=100). A significant difference was observed in
pain relief showing reduced pain with the help of visual analogue scale.11
Alternative modalities have fewer or no side effects and require very few safety
precautions. They can be combined or used sequentially to enhance their total effect.
Surveys suggest that women prefer alternative modalities for pain relief during labor.9
Women tend to rate alternative modalities of pain relief highly in terms of satisfaction
and desire to repeat them in future labor, even though their pain relieving capability is
short lived. It can be practiced in any setting as it is easy and affordable.
Alternative modalities focus on preventing suffering rather than completely
eliminating pain. It helps the mother in building up self confidence, improving her coping
abilities and perceptions of child birth8. In fact the element that best predicts a woman’s
experience of labor pain is her level of confidence and the ability to cope with the pain.
Satisfaction, fulfillment and a sense of accomplishment are often high when woman
copes well, even when the pain she is experiencing is great.8A single modality can’t meet
the needs of every woman.
A study on knowledge and competence of nurses in pain management was
conducted across United States of America. A 74 item questionnaire was developed by
the investigators. The result was that on an average only 56% of items were answered
correctly. This demonstrated stronger knowledge in pain assessment and less knowledge
in pain management.12
27

In rural India, alternative modalities were used in some or other forms by the
dais who conducted deliveries in villages. Measures like aromatherapy, massages, hot
and cold applications are used in traditional settings.13 All these should be revived to
bring out a change in maternity services. The main requirement for this is the training of
nurses regarding these modalities which can bring out a change in viewing labor and its
pain in the society.
A midwife is the ideal person to help the women understand and select these
modalities. Suffering which is different from pain is not an outcome to be measured after
childbirth. Suffering is unlikely if indicators of satisfaction were positive during child
birth.8 Alternative modalities boost this positive satisfaction. It is the duty of the midwife
to bring about this positive satisfaction.
Although effectiveness of alternative modalities is proved by various studies it is
not practiced in many of our hospitals and maternity centers. There is a need to increase
awareness among midwives about women’s preferences for alternative modalities to
relieve pain during labor. The midwives should consider alternative modalities a valid
form of pain relief and coping. However possible women should be provided with
alternative modalities through a skilled person. The midwives should be stressed the need
for practicing these modalities as women are highly satisfied with these alternative
modalities of pain relief.
As of the investigator’s previous clinical experience alternative modalities are not
used to relieve pain during labor in many of our hospitals due to limited resources
available and various other factors. With the effectiveness of various alternative
28

modalities proved by different studies the need to stress the importance of these
modalities among nurses working in maternity department was felt. Hence a structured
teaching programme on alternative and contemporary modalities regarding pain relief
during first stage of labor can be effective in improving the standards of maternal
services.
29

2- OBJECTIVES
Statement of the problem
“A STUDY TO ASSESS THE EFFECTIVENESS OF STRUCTURED
TEACHING PROGRAMME ON KNOWLEDGE OF STAFF NURSES REGARDING
SELECTED ALTERNATIVE AND CONTEMPORARY MODALITIES OF PAIN
RELIEF DURING FIRST STAGE OF LABOR IN SELECTED MATERNITY
HOSPITALS, BANGALORE.”
Objectives of the study
1. To assess the knowledge of staff nurses regarding alternative and contemporary
modalities of pain relief during first stage of labor by conducting pre-test.
2. To assess the effectiveness of structured teaching programme regarding alternative
and contemporary modalities of pain relief during first stage of labor by using
post-test scores.
3. To find out the association between pre-test knowledge scores and selected
demographic variable.
Operational definitions:
Effectiveness It refers to the significant improvement in knowledge regarding alternative
and contemporary modalities among staff nurses after the implementation of structured
teaching programme.
30
Structured teaching programme
It refers to systematically developed instruction designed for a group of staff
nurses to provide information regarding alternative and contemporary modalities of pain
relief during first stage of labor.
Knowledge
It refers to specific information regarding alternative and contemporary
modalities of pain relief among staff nurses.
Alternative and contemporary modalities
It refers to safe, simple, effective, inexpensive therapies other than the
conventional methods that help in reducing pain during first stage of labor. In the present
study it refers to selected five modalities namely hydrotherapy, intra-dermal water
blocks, aromatherapy, breathing exercises, touch & massage.
First stage of labour
It refers to the period from the onset of true uterine contractions till the complete
dilatation of the cervix.
Pain relief It refers to a feeling of relaxation and reassurance along with the alleviation of
pain and its symptoms by the use of alternative modalities during the first stage of labor.
31

Staff nurse
In this study staff nurses refers to those who have completed basic training in
nursing and registered in respective nursing council available for the study and working
in the maternity department.
Hypothesis
H0 - There is no significant difference between mean pre-test and post-test knowledge
scores regarding alternative and contemporary modalities of pain relief.
H1 - The mean post test knowledge scores of staff nurses exposed to structured
teaching programme regarding alternative and contemporary modalities of pain
relief will be higher than the mean pre-test knowledge scores as measured by
knowledge questionnaire at 0.05 level of significance
H0.1 - There is no significant association between pre-test knowledge scores and
selected demographical variables
H1.1 - There is a significant association between pre-test knowledge scores and selected
demographical variables
Conceptual framework
A theoretical framework serves as a guide or map to systematically identify
a logical precisely defined relationship between variables. (Wood and Hamber, 1994)34
Theoretical framework provides ways and methods to conduct the study and
guiding the interpretation, evaluation and integration of significant findings. (Kothari,
2000)35
32
Theoretical framework selected for this study was based on general systems
theory as postulated by Von Bertalanffy (1998). This is regarded as a universal grand
theory because of its unique relevancy and applicability (Johnson and Webber, 2005). It
is one type of exchange theory. In general systems theory, systems are composed of both
structural and functional components that interact within the boundary that filters the type
and rate of exchange with the environment. Here all the living systems are open systems
because there is an ongoing exchange of matter, energy and information.
The following elements are common to the system:
The system is a unit that is greater than the sum of its parts and it has got various
subsystems which has boundaries. Communication and feedback mechanism is essential
for system to function in a system goal or end can be reached in various ways and any
change in one part causes change in the whole system.
According to Von Bertalanffy “INPUT” which is matter, energy and
information is received from the environment and in this study input is considered as the
various socio-demographic variables which have influenced the respondents.
According to Von Ludwig Bertalanffy, “THROUGHPUT” refers to matter,
energy and information that is modified or transformed within the system. The process by
which the system processes the input and releases an output. In this study throughput
includes 3 stages, first is the pre-assessment of knowledge by pre-test, second is the
administration of structured teaching programme on alternative modalities and third is the
post-assessment through post-test. This will process the information about alternative and
contemporary modalities of pain relief during first stage of labour.
33

According to systems theory, “OUTPUT” refers to energy, matter and
information that leave a system into the environment. In the present study it is the change
in knowledge that is obtained by structured teaching programme on alternative and
contemporary modalities. This can be assessed by means of post-test knowledge scores
which can be adequate, moderately adequate and inadequate which proves the
effectiveness of structured teaching programme.
According to the theory, “FEEDBACK” refers to the information regarding
responses used by the system (may be positive, negative or neutral). In the present study
it is the backflow of information regarding the adequate, moderately adequate and
inadequate changes in the level of knowledge in staff nurses which is measured through a
structured questionnaire in the post-test.
34
1
INPUT
TARGET GROUPSTAFF NURSES
DEMOGRAPHIC VARIABLES;
AGE, QUALIFICATION
EXPERIENCE RELIGION
THROUGHPUT
ASSESSMENT OF PRE-TEST KNOWLEDGE OF STAFF NURSES
DEVELOPMENT AND ADMINISTRATION OF STP ON ALTERNATIVE MODALITIES
ASSESSMENT OF POST-TEST KNOWLEDGE OF STAFF NURSES
OUTPUT
ADEQUATE KNOWLEDGE
MODERATELY ADEQUATE KNOWLEDGE
INADEQUATE KNOWLEDGE
STP EFFECTIVE
RE-ASSESSMENT
STP NOT EFFECTIVE
FIG 1: CONCEPTUAL FRAMEWORK BASED ON BERTALANFFY’S GENERAL SYSTEM’S MODEL
FEEDBACK

3. REVIEW OF LITERATURE
A review of literature refers to activities involved in identifying and
searching for information on atopic and also developing and understanding the state
of knowledge on the topic. A review of literature was undertaken to gain in depth
knowledge of the various aspects of the problem under study.14
The investigator carried out an extensive review of literature on the research
topic in order to gain an insight into the selected problem under study as well as to
collect maximum relevant information for building up the study. It helped to develop
the instruments and select the demographic variables in the study.
Review of literature for the present study has been organized under the
following headings.
1. Studies related to review of alternative and contemporary modalities
2. Studies related to effectiveness of aromatherapy in relieving pain during first
stage of labor
3. Studies related to effectiveness of massages in relieving pain during first
stage of labor
4. Studies related to effectiveness of breathing exercises in relieving pain during
first stage of labor
5. Studies related to effectiveness of intra-dermal water blocks in relieving pain
during first stage of labor
6. Studies related to effectiveness of hydrotherapy in relieving pain during first
stage of labor
7. Studies related to knowledge of staff nurses regarding alternative and
contemporary modalities of pain relief during first stage of labor
41

8. Studies related to effectiveness of structured teaching programme.
Studies related to review of alternative and contemporary modalities
A study was conducted in North America to assess the effectiveness of non-
pharmacological approaches to relieve labor pain and prevent suffering. 13 methods
were updated. Randomized controlled trials included 60 women, 30 of whom received
the alternative modalities and other 30 women in the control group with usual care.
Experimental group had statistically significant lower pain intensity scores (0.73 vs.
1.30). The results of these studies indicate that with appropriate skill and attention
alternative modalities are effective in reducing pain during labor. A systematic review
of 9 trials (n=2259) was conducted to compare outcomes of continuous labor support
versus usual care. Hence the effectiveness of alternative modalities in relieving pain
during labor was proved by this study.8
A study was conducted in Children's Hospital, Australia on the effectiveness of
alternative modalities in labor pain relief. Meta-analysis was performed using relative
risks for dichotomous outcomes and weighed mean differences for continuous
outcomes. Seven trials involving 366 women and using different modalities of pain
management were included in this review. The trials included one involving
acupuncture (n = 100), one involving audio-analgesia (n = 25), one involving
aromatherapy (n = 22), three trials of hypnosis (n = 189) and one trial of music (n =
30). These trials decreased the need for pain relief (relative risk (RR) 0.56, 95%
confidence interval (CI) 0.39 to 0.81). Women receiving alternative modalities were
more satisfied with their pain management in labor compared with controls (RR 2.33,
42

95% CI 1.55 to 4.71). Hence alternative modalities are effective in reducing labor
pain.15
Studies related to effectiveness of aromatherapy in relieving pain during first
stage of labor
A study was conducted at Oxford Brookes university to explore the effects
that essential oils can have on helping a mother mentally cope with labor. During the
eight-year study involving 8,000 mothers, they found that aromatherapy was effective
in managing labour pains. They found that using essential oils lessened maternal
anxiety and fear while inducing a sense of well-being. Fear and anxiety are two things
which can slow labour and make the mother to be unable to cope with the pain of
labour. The study showed a drop in the use of opiate pain relief by those mothers who
used aromatherapy during labour. The normal uptake of opiate pain relief would have
been expected to be 30% in the Oxford study this dropped to 0.4%.16
One large, uncontrolled prospective study reported on the use and
effectiveness of aromatherapy in a large referral maternity unit in the United
Kingdom. During this time, 8058 women received aromatherapy during labor under
the supervision of midwives trained in aromatherapy. Sixty-one percent of the women
received aromatherapy (lavender, rose, or frankincense) to relieve anxiety and fear.
Rose oil was rated helpful by most (71%), followed by lavender (50%). Lavender and
frankincense were used for pain by 537 women, of whom 54% found lavender helpful
and 64% found frankincense helpful. In conclusion, aromatherapy is inexpensive and
popular with laboring women and midwives.17
43

Studies related to effectiveness of massages in relieving pain during first stage of
labour
A retrospective descriptive survey design study was conducted on “10 Non
Pharmacological pain relief techniques” for 46 women who were at least 18 years old
in North California. Of the 10 Non Pharmacological strategies rated by the sample,
breathing techniques relaxation, acupressure and massage found to be most effective.
Results found that a greater use of techniques were safe and effective and enhance
patient satisfaction during birth experience.18
An experimental study was conducted in a public maternity centre of Brazil.
A randomized trial consisting of 60 women were selected to receive massage or usual
care was selected to explore the effectiveness of massages in relieving pain during
labor. Massage was performed three times, once during each phase of the first stage of
labor and lasted for 30 minutes in each phase. Pain and anxiety was measured using
present behavioral intensity (PBI) scale and visual analog scale for anxiety (VASA).
Although pain intensity increased steadily through progressing phases of labor, the
massage group had significantly lower pain intensity scores at each phase of labor
(0.73 versus 1.30 in latent, 1.73 versus 2.17 in active, and 2.17 versus 2.87 in
transition phases). 87 % of the women in the massage group reported that the massage
was helpful in providing pain relief.19
A study was conducted to assess the effect of massage therapy on severity of
pain and outcome of labour at selected hospitals of Tehran. The results demonstrated
that the mean of pain severity at the first stage of labour was significantly different
among the experiment group and the control group. Massage therapy could be
44
introduced as a new useful method during delivery; regarding its supportive role to
reduce the labour pain.20
Studies related to effectiveness of breathing and relaxation in relieving pain
during first stage of labor
A study conducted by Oregon Health Sciences University School of Nursing,
Nigeria in 1998 involving 4,171 women who used different methods for managing
first stage of labour has showed that the majority that is 84% of women used non-
drug methods, while about half 49% used drugs for relieving pain. Among 84% of
women who used non-pharmacologic methods, 55.2% of women found that paced
breathing is effective.21
A study conducted in a maternity centre in Coobee, USA has listed pain
relief options during childbirth and labour. Among those options breathing exercises
is one, and has shown that slow and regular breathing can promote relaxation,
reducing pain and increasing comfort. Research has shown that none of these
techniques adversely affect the baby in any way or produce after-effects in the
mother.22
Studies related to effectiveness of intra-dermal water blocks in relieving pain
during first stage of labor
An experimental study was conducted in the University of Mexico. A
randomized trial compared the effect of intra-dermal water blocks to a "placebo"
blank (using saline). It was found that intra-dermal water blocks significantly
decreased severe low back pain in laboring women. Pain relief lasted 45 to 120
45
minutes and most women stated they would want to use intra-dermal water blocks
again during a subsequent birth.23
One of the trials compared the efficacy of three different treatments to decrease
low back pain: intradermal water blocks, TENS, and usual care (massage, water
immersion, movement as needed. Even though the water blocks were effective in
decreasing low back pain, women in the usual care group had the lowest requests for
pain medication.24
Studies related to effectiveness of hydrotherapy in relieving pain during first
stage of labor
An experimental study was conducted in Columbia to determine the
effectiveness of hydrotherapy on labour. Using a randomized, pre-test –post test
control group design with repeated measures, 18 term parturient’s were assigned to a
control and an experimental group. Experimental subjects were placed in a tub of 37 0
C water for 1 hour during early labour. At 15 minutes bathers’ pain scores were
decreased compared to non bathers. After 15 minutes of immersion, bathers had a
significantly greater increase in plasma volume than non bathers. The findings offer
preliminary support for therapeutic effects of bathing in labour for acute, short term
anxiety and pain reduction. Findings from the study support the therapeutic effects of
water immersion as an alternative or supplemental intervention for clients who need
fast short acting anxiety and pain relief.25
A recent systematic review analyzed findings of 2 prospective cohort studies
and 7 RCTs of bathing published between 1987 and 2001. A total of 3496 women
participated in these trials. Sample sizes in the individual trials ranged from 18
to1237. The trials varied widely in study designs and quality, timing of entry into the
46

water, water temperature, and in baseline rates of epidural analgesia and other
interventions, as reflected by the rates in the control ("usual care") groups. Of the 3
best designed RCTs, 2 found a reduction in pain indicators in the bath groups1 one
did not. Maternal satisfaction was high in the bath group, with 89% stating they would
like to use the bath in a future labor.26
Studies related to knowledge of staff nurses regarding alternative modalities of
pain relief during first stage of labor.
A study was conducted on “Midwife’s utilization of non-pharmacological pain
management methods during the first of stage labor”. The data was obtained by means
of a structured questionnaire which was given to midwives working in the Maternity
wards of the Christian Hospital Association of Lesotho. According to the results, the
midwives indicated that they were taught non-pharmacologic methods of pain
management, however they expressed that they inadequately use these methods
during the first stage of labor due to shortage of staff, lack of privacy and space, a
high midwife-mother ratio, culture and hospital policies. In the light of these findings,
recommendations were made of maximizing the use of non-pharmacologic methods
during the first stage of labor.27
A descriptive survey was conducted in a large Canadian hospital on 97
registered staff nurses regarding nurse’s attitude towards providing continuous labor
support. Scores measuring nurses' attitudes, subjective norms, and intentions
regarding continuous labor support for women with epidural analgesia were
significantly lower than those for women without epidural analgesia (p<.0001).Top
perceived organizational barriers to continuous labor support included unit acuity and
method of patient assignment. Nurses view organizational barriers as important
factors influencing their ability to provide continuous labor support.28
47

A study was conducted across United States on nursing students and faculty
member’s knowledge of experience with and attitudes towards complementary or
alternative therapies. The study was designed to describe and compare the knowledge,
experience and attitude of nursing faculty and student’s .The results revealed that 85%
of the participants desired more education about complementary and alternative
medicine. Faculty and nursing students expressed positive attitude towards generating
complementary therapy into undergraduate nursing curriculum and nursing practice.29
Studies related to effectiveness of structured teaching programme.
A quasi experimental study was carried out at rural health centre at South
Pitchavaram in Tamil Nadu on effectiveness of structured teaching programme on
knowledge, Attitude and practices regarding tobacco consumption in rural
health setting. Sixty subjects who were attending the rural health centre were
selected by systematic random sampling technique. The data was collected by
questionnaire. Out of 19 smokers about 6 (31.6%) had the highest level of readiness to
quit smoking. Out of 28 tobacco chewers 15 (53.6%) had highest level of readiness to
quit their behavior of chewing tobacco. A structured teaching programme was found
to be effective in changing these behaviours.30
A study was conducted to assess the effectiveness of
structured teaching programme on knowledge and practice of
breast feeding among primi-postnatal mothers of maternity wards in
C.M.C Vellore hospital, research design employed descriptive survey
method, simple random sampling used, sample size were 100 primi-
postnatal mothers, tools used were observation checklist and
interview guide. The study’s results shows that mother who had
48
teaching programme showed highly significant knowledge gain and
good practice of breast feeding(P<0.01).31
A study was conducted to assess the effectiveness of
structured teaching programme on knowledge and practice of
breast feeding and its problems among lactating mothers in Vani
Villas Hospital, Bangalore. The descriptive evaluation study was
conducted on 20 lactating mothers of hospitalized children, data
collection done using a structured interview schedule and
observational checklist, analysis of data revealed that 50% of
mothers had satisfactory level of knowledge about the advantages
of colostrums. The desirable mothers and child relationship before
was 15% and after instruction was 50%, significant at P<0.01
level.32
An evaluative study was conducted on the effectiveness of
structured teaching programme on breast feeding among ante natal
mothers at Mangalore among 30 mothers selected by purposive
sampling technique. Data was collected using a structured closed
ended questionnaire, following which a planned teaching
programme was administered. The study findings revealed that the
mean post-test knowledge score was significantly higher than the
mean pre-test knowledge score (t=52.65, P < 0.001), showing
effectiveness of the structured teaching programme in improving
the knowledge on breast feeding benefits and practices.33
49

4. METHODOLOGY
The research methodology indicates the general pattern to gather valid and
reliable data for the problem under investigation.34
Research methodology is a way to systematically solve the research problem. It
involves systematic procedure by which the researcher starts from initial identification
of research problem to its final conclusion.14
This chapter deals with description of various steps adopted to collect and
organize data for the study. It includes the research approach, research design, setting
of the study variables under study, population, sample and sample size, sampling
technique, development of the tool, development of structured teaching programme,
method of data collection and plan for data analysis.
Research approach
Research approach indicates the basic procedure for conducting the research
study. Research approach helps the researcher to determine what data to be collected
and how to analyze it. It also suggests possible conclusions to be drawn from the data.
The selection of approach depends upon the purpose of the study.35
50

In view of the nature of the problem selected for the study, an evaluative
approach was found appropriate.
Evaluation research is an applied form of research that involves finding out
how well a programme, procedure or policy is working. Its goal is to assess or
evaluate the success of a programme.34
Research design
The research design is the plan, structure and strategy of investigation for
answering the research question. It is the overall plan or blue print, the researcher
select to carry out their study.35
The term research design refers to the plan or organization of a scientific
investigation. Research design helps the researcher in selection of subjects,
manipulation of experimental variables, control of extraneous variables, procedure of
data collection and the type of statistical analysis to be used to interpret the data.14
Quasi-experimental one group pre-test post-test design without control group
was selected as the research design for the present study. The primary objective of
study was to find the effectiveness of structured teaching programme.
The design chosen for the study is presented in the table-1 as follows
Group Pre-Test(Day 1)
Intervention(Day 2)
Post-Test(Day 7)
Experimental 01 X 07
51

Key:
01: Assessment of knowledge by pre-test.
X: Structured teaching programme on Alternative and contemporary modalities
of pain relief during first stage of labour.
02: Assessment of knowledge by post-test.
A structured questionnaire was administered to staff nurses working in
maternity department in Fortis hospitals on day 1, following that a structured teaching
programme on alternative and contemporary modalities was delivered. Post-test was
conducted on day 7 to assess the effectiveness of structured teaching programme.
52

53
RESEARCH DESIGNQUASI-EXPERIMENTAL ONE GROUP
PRE-TEST POST-TEST DESIGN WITHOUT CONTROL GROUP
POPULATIONSTAFF NURSES WORKING IN MATERNITY DEPARTMENTS
SAMPLE60 STAFF NURSES OF MATERNITY DEPARTMENT, FORTIS HOSPITAL
PRE-TEST
STRUCTURED QUESTIONNAIRE REGARDING ALTERNATIVE AND CONTEMPORARY MODALITIES
STRUCTURED TEACHING PROGRAMME REGARDING ALTERNATIVE AND CONTEMPORARY MODALITIES
POST TEST
STRUCTURED QUESTIONNAIRE REGARDING ALTERNATIVE AND CONTEMPORARY MODALITIES
ANALYSIS
DESCRIPTIVE & INFERENTIAL STATISTICS
DAY 7
DAY 1
SAMPLING TECHNIQUE
NON-PROBABILITY PURPOSIVE SAMPLING

Setting
The setting is the physical location and conditions in which data collection
takes place. This study was conducted in Fortis hospital, Bannerghatta road,
Bangalore. Fortis hospital was selected for the study on the basis of feasibility of
conducting study and the availability of the sample.
Variables under investigation
A variable is a phenomena or characteristic or attribute under a study.
Variables are the measurable characteristics of a concept and consist of a logical
group of attributes.35
Three types of attributes were identified in the study. They are independent
variable, dependent and extraneous variable.
Independent variable:
According to Treece and Treece (1988) the independent variable is the one
variable that stands alone and not dependent on any other. It is the cause of the
action.34
In present study it refers to the structured teaching programme regarding
alternative and contemporary modalities of pain relief.
Dependent variable:
54

Dependent variables are the effect of the independent variable and cannot exist
by itself (Treece and Treece 1988).34
In the present study it refers to the knowledge of staff nurses regarding
alternative and contemporary modalities.
Demographic variables:
An uncontrolled variable that greatly influences the results of the study is called
as the demographic variables (Treece and Treece 1988).
Demographic variables selected for this study are age in years, qualification,
experience and religion.
Population
Population refers to the complete set of observations or measurements about
which the investigator would like to draw conclusions. Population is a group whose
members possess specific attributes that the researcher is interested in studying. In the
present study the population consists of all staff nurses working in maternity
departments of various hospitals.35
Sample and sampling technique
Sample:
A sample is a subset or portion of the population that has been selected to
represent the population of interest.14
The present study was conducted among 60 staff nurses working in maternity
department of Fortis hospital, Bannerghatta road, Bangalore.
55

Sampling Technique:
Sampling is a process of selecting a group of people, events or position of the
population to represent the entire population.34
Non-probability purposive sampling technique was used to select 60 staff
nurses working in maternity department of Fortis hospital as the sample for the
present study.
Criteria for selecting the sample
Inclusion Criteria:
1. Staff nurses who are willing to participate in this study.
2. Staff nurses who are available during the period of data collection.
Exclusion Criteria:
1. Staff nurses working in departments other than the maternity department.
Selection and development of tool
Tools are the procedures or instruments used by the researcher to collect the
data. It acts as a best instrument to assess and collect the data from the samples of the
study.35
The instruments selected in a research must be the best vehicle for drawing
conclusion for the study. It is a device used to measure the concept of interest in a
research project.14
The present study was aimed to evaluate the effectiveness of structured
teaching programme on knowledge of staff nurses regarding alternative and
contemporary modalities of pain relief during first stage of labour. Structured teaching
programme followed by administration of structured knowledge questionnaire was
56
used as an appropriate and effective method to evaluate the knowledge of the staff
nurses.
The main strengths behind development of the tool were:
Review of research and non-research materials in the areas relevant to
alternative and contemporary modalities of pain relief
Experts’ opinion and suggestions were taken from the field of nursing and
medicine in determining the important areas to be included.
Discussion with colleagues and personal experience in clinical settings.
Books.
Preparation of the blueprint
A blueprint on knowledge questionnaire regarding alternative and
contemporary modalities was prepared consisting of Eight sub-areas that include,
general information about labour, general information about labour pain, alternative
and contemporary modalities, aromatherapy, massages, breathing exercises, intra-
dermal water block, hydrotherapy. It depicted the distribution of items according to
the content areas based on three domains: knowledge, comprehension and application.
Development of criteria checklist for the tool
Criteria checklist was developed to validate the tool regarding accuracy,
relevance and appropriateness of the content.
Description of tool
Data collection tool contain items on the following aspects;
Part I: includes items related to demographic variables - Age (in years), qualification,
experience, religion
57

Part II: Includes 40 knowledge questions of which Nine items were related to
General information about labour, Three items regarding labour pain, Two items
regarding alternative modalities, Six items regarding aromatherapy, Five items
regarding massages, Five items regarding breathing exercises, Five items regarding
intra-dermal water blocks, Five items regarding hydrotherapy.
The knowledge regarding alternative and contemporary modalities was
measured in terms of knowledge score. Each correct answer was given a score of one
mark and wrong answer or unanswered was given a score of zero. The maximum
score was 40. To interpret level of knowledge the scores were distributed as follows;
Inadequate knowledge ≤ 50 %
Moderately adequate knowledge 51 – 75 %
Adequate knowledge > 75 %
Content validity of the tool
Content validity represents the universe of content which provides the
framework and basis for formulating the items that will adequately represent the
content.
The constructed tool along with objectives, blue print and criterion checklist
was submitted to seven experts in the field of obstetric nursing and medicine for
content validity. The selection of experts was done based on their experience and
clinical expertise. The experts were requested to give their opinions regarding
relevancy, accuracy and appropriateness of the items for further modifications.
Pre-testing of tool
58

Pre-testing of the structured questionnaire was done to check the clarity of
items, their feasibility and practicability. The prepared questionnaire was
administered to ten staff nurses. The sample chosen were similar in characteristics to
those of the population under study.
The investigator found that the language of tool was simple and practicable; the
average time taken to complete the questionnaire for each sample was 30 –
45minutes. The tool consisted of 40 items. Based on the pre-testing suggestions given
by the experts, modification and rearrangement of few items were done.
Reliability
Reliability of research instrument is defined as the extent to which the
instrument yields the same results on repeated measures. The reliability of a
measuring tool can be assessed in the aspects of stability, internal consistency, and
equivalence depending on the nature of the instrument and aspects of the reliability
concept.14
The method adopted for the present study was split-half method to measure the
homogeneity of the tool. The questionnaire was first divided into two equivalent
halves and correlation for the half test was found using Karl Pearson’s correlation
coefficient formula. The tool was found to be statistically reliable for the main study.
Ethical consideration
The researcher had taken permission from the parent institution to conduct the
research study. Permission was obtained from the nursing superintendent of Fortis
hospital, Bangalore. Consent was taken from the subjects before data collection. The
subjects were informed that the confidentiality of data will be maintained.
59

Development of structured teaching programme
Teaching plan is a guide for the teacher because it helps to cover the topic
comprehensively with proper sequence of points and without missing anything.
The steps to prepare teaching plan were:
Review of literature
Framing the outline of the content.
Preparation and organization of content.
Deciding the method of instruction and AV aids.
Preparation of the final draft.
Editing the teaching plan evaluating the teaching plan.
1. Review of literature:
An extensive literature review was undertaken from research and non research
materials, internet sources, journals etc., regarding alternative and contemporary
modalities.
2. Framing the outline of the content:
The outline of the teaching plan was framed which included setting of the
general and specific objectives regarding alternative and contemporary modalities,
specifying the date, time, place and size of the group, number of sessions and duration
of sessions.
3. Preparation and organization of the content:
Content of the structured teaching programme on alternative and contemporary
modalities was prepared and organized under various headings according to the
60
specific objectives. Structured teaching programme was organized under various
headings such as, general
information about labour and labour pain, alternative and contemporary modalities,
aromatherapy, massages, breathing exercises, intra-dermal water block, hydrotherapy.
4. Deciding the method of instruction and AV aids:
The method of instruction adopted was lecture method with power point
presentation.
5. Preparation of the final draft of structured teaching programme:
General and specific objectives of the teaching plan were given in the
beginning of the structured teaching programme. Final draft of structured teaching
programme was organized under various headings such as general information about
labour and labour pain, alternative and contemporary modalities, aromatherapy,
massages, breathing exercises, intra-dermal water block and hydrotherapy.
6. Editing the teaching plan.
The prepared structured teaching programme was edited by professional
editors.
Description of structured teaching programme
Structured teaching programme was prepared to enhance the knowledge of staff
nurses regarding alternative and contemporary modalities which consist of the
following content.
Introduction
General information about labour and labour pain
Alternative and contemporary modalities
Aromatherapy
61

Massages
Breathing exercises
Intra-dermal water blocks
Hydrotherapy
Content validity of the structured teaching programme:
Content validation of the structured teaching programme was ascertained in
consultation with the experts in the field of nursing such as obstetrics and
gynaecological nursing. Suggestions and recommendations of the experts were
considered to modify the content of structured teaching programme.
Pre-testing of the structured teaching programme:
Pre-testing of the validated structured teaching programme was done at Fortis
Hospital, Bangalore to determine the feasibility, clarity and ambiguity, and time taken
to complete the teaching. The time taken by the researcher to complete the teaching
programme was 30-40 minutes. The researcher did not face any problems during the
administration of the structured teaching programme. Structured teaching programme
found to be feasible with regard to time, simplicity and clarity.
Pilot study
Pilot study is a small scale version of the proposed study conducted to
refine the methodology. It is conducted similar to the proposed study, using similar
subjects, the similar setting, the same treatment, the same data collection and the same
analysis technique.
The Purpose of the Pilot Study:
To find out the feasibility of conducting the final study
To evaluate the tool constructed.
To finalize the plan for analysis.
62

The pilot study was conducted in Fortis Hospital, Bangalore from 1.3.2012 to
10.3.2012 to find the feasibility of the study. Ten staff nurses were selected using
purposive random sampling technique. The subjects for the pilot study possessed the
same characteristics as that of the sample for the final study, but were not included in
the main study. Prior to the study permission was obtained from the concerned
authority. The selected subjects were informed of the purpose of the study and
consent was obtained. Assessment of knowledge was done by using structured
questionnaire. Post-test was conducted using the same structured questionnaire on the
seventh day of pre-test and after the administration of structured teaching programme.
The time taken to complete one questionnaire was 30-40 minutes. The collected data
were analyzed using descriptive and inferential statistics.
After conducting the pilot study, it was found that the study was feasible.
The concerned authority and the sample were found to be cooperative, the
questionnaire and structured teaching programme were relevant and the time and cost
of the study was within the limit.
Problems faced during pilot study:
Some of the subjects have to be reminded personally to come for the post-test.
Number of subjects showed great reluctance to participate in study as they
complained of tiredness due to their tiring duty shifts.
Procedure for data collection of main study
Before collecting the data, permission was obtained from the concerned
authority. Keeping in mind the ethical aspect of research, the data was collected after
obtaining the informed consent of the sample. The samples were assured anonymity
and confidentiality of information provided by them. The researcher collected the data
63

from the subjects. Pre-test was conducted from 15th March 2012 to 15th April 2012
followed by administration of structured teaching programme using A V aids. The
duration of the session was 30 minutes. Post-test was conducted from 21st March
2012 to 21st April 2012 to evaluate the effectiveness of structured teaching
programme.
Plan for data analysis
The data obtained will be analyzed on the basis of the objectives of the study
using descriptive and inferential statistics. Inferential statistics which are based on
laws of probability provide a means of drawing conclusion about the population from
which data was obtained for the study. Plan for data analysis includes:
The data was entered in a master sheet.
Data was analyzed using descriptive and inferential statistics.
Description of the subjects with respect to demographic variables was presented
in terms of frequency and percentage.
Mean, Standard Deviation, and Mean Percentage was used to evaluate the
knowledge level of staff nurses on alternative and contemporary modalities.
Statistical significance of the effectiveness of structured teaching programme
was analyzed using Paired ‘t’ test.
Chi-square test was used to find out the relationship between demographic
variables and knowledge level of staff nurses on alternative and
contemporary modalities.
Results would be represented in tables and graphs.
Summary
64

A quasi-experimental design with evaluative approach was adopted in order
to evaluate the effectiveness of structured teaching programme regarding alternative
and contemporary modalities of pain relief during first stage of labour among staff
nurses working in maternity department in Fortis hospital, Bangalore. Pilot study was
conducted to find out the feasibility of the study. Validity and reliability of the
questionnaire and structured teaching programme was tested. Closed ended questions
were used to assess the knowledge regarding alternative and contemporary modalities.
Data was collected from the sample after obtaining permission from the concerned
authority. Collected data was analysed using descriptive and inferential statistics and
was presented in the form of tables, graphs and diagrams.
65

5. RESULTS The chapter deals with the analysis and interpretation of data collected
from staff nurses regarding alternative and contemporary modalities. The analysis and
interpretation was based on the data collected by using structured questionnaire. The
data collected were organized, tabulated, analyzed and interpreted by using
descriptive and inferential statistics. Statistical analysis is a method of rendering
quantitative information and elicits meaningful form of research data. It is the process
of organizing and synthesizing data so as to answer research questions and to test the
hypothesis.
Objectives of the study
1. To assess the pre-test knowledge scores of staff nurses regarding alternative and
contemporary modalities of pain relief during first stage of labor.
2. To assess the effectiveness of structured teaching programme regarding
alternative and contemporary modalities of pain relief during first stage of
labor by using post-test scores.
3. To find out the association between pre-test knowledge scores and selected
demographic variable.
66

Hypothesis
H0-There is no significant difference between mean pre-test and post-test knowledge
scores regarding alternative and contemporary modalities of pain relief.
H1-The mean post test knowledge scores of staff nurses exposed to structured
teaching programme regarding alternative and contemporary modalities of
pain relief will be higher than the mean pre-test knowledge scores as
measured by knowledge questionnaire at 0.05 level of significance
H0.1-There is no significant association between pre-test knowledge scores and
selected demographical variables
H1.1-There is a significant association between pre-test knowledge scores and
selected demographical variables
Organisation of findings
The collected data were edited, tabulated, analyzed, interpreted and
findings obtained were presented in the form of tables and diagrams which were
represented under the following sections.
Section 1:
Demographic profile of staff nurses.
Section 2:
Knowledge of staff nurses regarding alternative and contemporary
modalities of pain relief during first stage of labour in pre-test and post-test
Section 3:
Findings related to effectiveness of the structured teaching programme by
comparing the mean pre-test & mean post-test knowledge scores
67

Section 4:
Association of pre-test knowledge scores of staff nurses with the selected
demographic variables
Section – 1
Demographic profile of staff nurses
Table – 2: Distribution of respondents according to their age
n=60Age
(in years) Frequency Percentage
20-25 26 43.3
26-30 30 50.0
31-35 2 3.3
36-40 2 3.3
Total 60 100
Table - 2 shows the distribution of respondents according to their age. It can
be seen from the table that majority of the respondents i.e. 30 (50%) are in the age
group of 26-30 yrs and 26 (43.3%) are in the age group of 20-25 yrs. Only 4 (6.6%)
are in the age group of 31-40 yrs. The above data is represented in cylindrical diagram
in the Fig 3
68

69

20-25 years 26-30 years 31-35 years 36-40 years0.0%5.0%
10.0%15.0%20.0%25.0%30.0%35.0%40.0%45.0%50.0%
Fig - 3: Cylindrical diagram showing percentage dis-tribution of respondents by age
Age in years
Fre
quen
cy in
per
cent
age
70

Table – 3: Distribution of respondents according to Qualification
n=60
Qualification Frequency Percentage
GNM 47 78.3
B.Sc. Nursing 13 21.7
Total 60 100
In Table 3 the distribution of respondents according to their qualification is
shown. It is evident that majority of them 47(78.3%) have GNM qualification and 13
(21.7%) of them have completed B.Sc. nursing. The above distribution is given in pie
diagram in Fig 4
71

78.30%
21.70%
Fig- 4: Pie diagram showing percentage distribution of respondents by their qualification
GNM
B.Sc. Nursing
72

Table – 4: Distribution of respondents according to years of experience
n=60
Experience Frequency Percentage
Below one year 3 5.0
1-3 years 25 41.7
4-6 years 27 45.0
7 years and above 5 8.3
Total 60 100
In Table - 4 the distribution of respondents according to experience is given. It
was observed that out of 60 staff nurses majority of them 27(45%) have 4-6 years of
experience and 25(41.7%) of them have1-3 years of experience. 5 (8.3%) of them
have experience of 7 years and above and only 3(5%) of them have less than one year
experience. The above distribution is given in pyramid diagram in the Fig 5
73

Below one year1-3 years
4-6 years7 years and above
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
Fig - 5: Pyramid diagram showing frequency distribution of re-spondents according to their experience
Experience in yearsFreq
uenc
y in
per
cent
age
74

Table – 5: Distribution of respondents according to religion.
n=60
Religion Frequency Percentage
Hindu 23 38.3
Christian 37 61.7
Total 60 100
In Table 5 the distribution of respondents according to religion is given. It was
found that out of 60 staff nurses majority of them 37(61.7%) were Christians and
23(38.3%) were Hindus. This distribution is shown in pie diagram in fig 6
75

38.3%
61.7%
Fig - 6: Pie diagram showing percentage distribution of respondents by religion
HinduChristian
76

SECTION II
KNOWLEDGE OF STAFF NURSES REGARDING ALTERNATIVE AND
CONTEMPORARY MODALITIES OF PAIN RELIEF DURING FIRST
STAGE OF LABOUR IN PRE TEST
TABLE – 6: Distribution of respondents according to pre-test and post-test
knowledge scores.
n=60
Knowledge levelPre test Post test
Frequency Percent Frequency Percent
Inadequate knowledge52 86.7 0 0.0
Moderately adequate knowledge 8 13.3 9 15.0
Adequate knowledge0 0.0 51 85.0
Total 60 100 60 100
In the Table 6 distribution of respondents according to pre-test and post-test
knowledge scores is given. The pre-test was conducted by administering a structured
questionnaire to the staff nurses. In which majority of nurses 52(86.7%) of them have
inadequate knowledge, 8(13.3%) of them have moderate knowledge and none of the
staff nurses (0%) have adequate knowledge. The above data clearly indicates the need
for a planned teaching programme on imparting the knowledge to the staff nurses.
The post-test was administered after the structured teaching programme. The post-test
knowledge scores show a significant difference ie, none (0%) them are having
inadequate knowledge, 9(15%) are having moderate knowledge and majority of them
51(85%) have acquired adequate knowledge from the structured teaching programme
77

on alternative and contemporary modalities of pain relief during first stage of labour.
This distribution is given in the diagram below in Fig 7
78

Inadequate knowledge Moderate knowledge Adequate knowledge0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Fig - 7: Pre-test and post-test knowledge level of respondents
Pre testPost test
Knowledge level
Freq
uenc
y in
per
cent
age
79
TABLE – 7: Mean, Mean percentage and standard deviation for the pre test knowledge of staff nurses
n=60Sl.
No.
Knowledge
aspects
No. of
Items
Max
ScoreMean
Mean
%Median SD
1 General
information about
labour
9 9 5.53 61.44 6 1.478
2 General
information
regarding labour
pain
3 3 1.57 52.33 2 0.927
3 Alternative and
contemporary
modalities
2 2 0.38 19 0 0.666
4 Aromatherapy 6 6 1.97 32.83 2 0.901
5 Massages 5 5 1.13 22.6 1 1.033
6 Breathing
exercises5 5 1.85 37 2 0.954
7 Intra-dermal
water blocks5 5 2.05 41 2 1.080
8 Hydrotherapy 5 5 2.48 49.6 2.5 1.142
Overall 40 40 16.97 40.42 18 3.773
The above table 6 shows the mean, mean percentage and standard deviation of pre test
knowledge scores in various aspects. The mean, mean percentage and SD in the area
of general information about labour is 5.53, 61.44% and 1.478 respectively. The
scores in the area of general information regarding labour pain are 1.57, 52.33 and
0.927, in the areas of alternative and contemporary modalities are 0.38, 19 and 0.666,
80

in the area of aromatherapy are 1.97, 32.83 and 0.901, in the area of massages the
scores are 1.13,22.6 and 1.033, in the area of breathing exercises the score are 1.85,37
and 0.954, in the area of intra-dermal water blocks 2.05, 41 and 1.080 and the scores
of hydrotherapy are 2.48, 49.6 and 1.142. The overall pre test mean, mean percentage
and SD are 16.97, 40.42 and 3.773 respectively.
81

Genera
l infor
mation about la
bour
Labour pain
Altern
ative m
odalities
Aromathera
py
Massa
ges
Breathing ex
ercise
s
Intra
-dermal w
ater block
s
Hydrothera
py
Over all
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Fig - 8: Mean percentage of pre-test knowledge scores of the re-spondents
Knowledge aspects
Mea
n pe
rcen
tage
82

TABLE – 8: Mean, Mean percentage and standard deviation for the post test knowledge of staff nurses
n=60Sl.
No.
Knowledge
aspects
No. of
Items
Max
ScoreMean
Mean
%Median SD
1 General
information
about labour9 9 8.12 90.22 8 0.922
2 General
information
regarding
labour pain
3 3 2.52 84 3 0.624
3 Alternative and
contemporary
modalities
2 2 1.13 56.5 1 0.596
4 Aromatherapy 6 6 4.27 71.16 4 1.148
5 Massages 5 5 3.40 68 3.5 1.265
6 Breathing
exercises5 5 3.93 78.6 4 0.918
7 Intra-dermal
water blocks5 5 4.32 86.4 4 0.701
8 Hydrotherapy 5 5 4.52 90.4 5 0.770
Overall 40 40 32.20 80.5 32.5 2.773
The above table 7 shows the mean, mean percentage and standard deviation of post
test knowledge scores in various aspects. The mean, mean percentage and SD in the
area of general information about labour is 8.12, 90.22% and 0.922 respectively. The
scores in the area of general information regarding labour pain are 2.52, 84 and 0.624,
in the areas of alternative and contemporary modalities are 1.13, 56.5and 0.596, in the
area of aromatherapy are 4.27, 71.16and 1.148, in the area of massages the scores are
3.40, 68and 1.265, in the area of breathing exercises the score are 3.93, 78.6and
83

0.918, in the area of intra-dermal water blocks 4.32, 86.4 and 0.701and the scores of
hydrotherapy are 4.52, 90.4and 0.770.
84

Gener
al inform
ation abou
t labour
Gener
al inform
ation re
garding la
bour pain
Altern
ative a
nd contem
porary
modaliti
es
Aromather
apy
Massa
ges
Breathing ex
ercis
es
Intra
-dermal w
ater b
locks
Hydrother
apy
Overall
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
100.00%
Fig - 9: Mean percentage distribution of post-test knowledge scores of respondents
Knowledge aspects
Mea
n pe
rcen
tage
Fig 9: Mean percentage distribution of post test knowledge scores of staff nurses.
85

SECTION III
FINDINGS RELATED TO EFFECTIVENESS OF STRUCTURED
TEACHING PROGRAMME
TABLE 9: Comparison of pretest and post test knowledge scores
n= 60
The above table shows the comparison between the pretest and post test
knowledge score of staff nurses regarding alternative and contemporary modalities of
pain relief during first stage of labor in various aspects. The ‘t’ test values shows
significance (at the level of α=0.05) in all the areas.
86
Sl. No.
Knowledge aspects
Pre test Post testMean
differencet Value Df
Inference
Mean S D Mean S D
1General information about labour
5.53 1.478 8.12 0.922 2.58 12.205 49 S
2
General information regarding labour pain
1.57 0.927 2.52 0.624 0.95 6.913 49 S
3Alternative and contemporary modalities
0.38 0.666 1.13 0.596 0.75 7.123 49 S
4 Aromatherapy 1.97 0.901 4.27 1.148 2.30 15.057 49 S
5 Massages 1.13 1.033 3.40 1.265 2.26 12.124 49 S
6 Breathing exercises 1.85 0.954 3.93 0.918 2.08 13.17 49 S
7Intra-dermal water blocks
2.05 1.080 4.32 0.701 2.26 14.738 49 S
8 Hydrotherapy 2.48 1.142 4.52 0.770 2.03 10.613 49 S
Overall 16.97 3.773 32.20 2.773 15.23 31.91 49 S

It is evident that compared to pre-test knowledge scores there is significant
increase in the post-rest knowledge scores in all the areas. Hence the null hypothesis
(H0) related to no difference between pre-test and post-test overall mean scores is
rejected and research hypothesis (H1) is accepted. Therefore it can be interpreted that
the structured teaching programme was effective in improving the knowledge of staff
nurses regarding alternative and contemporary modalities.
6. DISCUSSION
87

This chapter presents the discussion of findings based on
sample characteristics, knowledge of staff nurses working in
maternity department on alternative modalities of pain relief during
first stage of labour, effectiveness of structured teaching
programme and association between pre-test knowledge score of
staff nurses and selected demographic variables.
The aim of this study was to develop and implement
structured teaching programme to improve the knowledge of staff
nurse on alternative modalities of pain relief during first stage of
labour. The effectiveness of structured teaching programme was
evaluated by assessing the knowledge of staff nurses on alternative
modalities.
Objectives of the study
The objectives of the study are:
1. To assess the knowledge of staff nurses regarding alternative and contemporary
modalities of pain relief during first stage of labour by conducting pre-test.
2. To assess the effectiveness of structured teaching programme regarding
alternative and contemporary modalities of pain relief during first stage of
labour by using post-test scores.
3. To find out the association between pre-test knowledge scores and selected
demographic variables
Hypothesis
The hypothesis will be tested at 0.05 level of significance
88

H0-There is no significant difference between mean pre-test and post-test knowledge
scores regarding alternative and contemporary modalities of pain relief.
H1-The mean post test knowledge scores of staff nurses exposed to structured
teaching programme regarding alternative and contemporary modalities of pain
relief will be higher than the mean pre-test knowledge scores as measured by
knowledge questionnaire at 0.05 level of significance
H0.1-There is no significant association between pre-test knowledge scores and
selected demographical variables
H1.1-There is a significant association between pre-test knowledge scores and
selected demographic variables
Major findings of the study
Majority of the respondents i.e. 30 (50%) are in the age group of 26-30 yrs
It was found that based on qualification majority of the respondents 47(78.3%)
have GNM qualification and 13 (21.7%) of them have completed B.Sc.
nursing.
It was observed that out of 60 staff nurses majority of them 27(45%) have 4-6
years of experience
Out of 60 staff nurses majority of them 37(61.7%) were Christians and
23(38.3%) were Hindus.
Section 2: Pre-interventional knowledge score
In the present study the pre-interventional score shows that majority of the
samples 52 (86.7%) had inadequate knowledge regarding alternative modalities of
pain relief before the administration of structured teaching programme. 8 (13.3%) of
them had moderately adequate knowledge and none of them had adequate knowledge.
89

The findings of this study are consistent with an evaluative
study done to assess the knowledge of staff nurses in selected
hospitals, Bangalore on alternative and contemporary modalities of
pain relief during first stage of labour. The samples were selected by
random sampling and the data were collected using structured
questionnaire. The result showed that the mean post-test
knowledge scores (36.18%) was found to be significantly higher
than their mean pre-test knowledge score (23.14%) as evident from
‘t’ value.
Section 3: Evaluation of effectiveness of STP
The analysis result of the present study shows that the mean post-test
knowledge score obtained by the staff nurses is improved to 80.5% from a mean pre-
test knowledge score of 40.42%. With the structured teaching, 15% of staff nurses
were found to have moderately adequate knowledge and remaining 85% were found
to have adequate knowledge and none among the staff nurses had inadequate
knowledge regarding alternative and contemporary modalities of pain relief during
first stage of labour. This gives an inference that the structured teaching programme
was effective in improving the knowledge level of staff nurses regarding alternative
modalities.
The findings of the study was consistent with an evaluative study done to assess
the knowledge of adolescent girls (16-18yrs) in a selected college, Bangalore
regarding reproductive health and sexual issues before and after administration of
structured teaching programme. A sample of 60 adolescent girls was selected by
purposive sampling technique. A pre-test was conducted and STP was administered to
90

the subjects. The post-test was conducted after seven days. The findings revealed
higher post-test mean score. Thus the study showed that the STP was effective in
improving the knowledge level of adolescent girls.
Section 3: Association between the pre-test level of knowledge and selected
demographic variables.
The study findings revealed that there is no association between the
demographic variables such as age, qualification, experience and religion among the
pre-test level of knowledge among staff nurses working in maternity department.
Summary
The findings of the study and other studies have shown that knowledge
regarding alternative and contemporary modalities of pain relief during first stage of
labour was very less among staff nurses. It considerably increased after the
administration of a structured teaching programme.
91

7. CONCLUSION
The main aim of the study was to assess the effectiveness of structured
teaching programme on knowledge regarding alternative and contemporary modalities
among staff nurses. Information was given to the staff nurses through a structured
teaching programme which includes various aspects like, general information about
labour and labour pain, aromatherapy, massages, breathing exercises, intra-dermal
water blocks and hydrotherapy.
The following conclusions were drawn on the basis of findings of the study:
The pre-test findings showed that knowledge of staff nurses regarding alternative
and contemporary modalities was inadequate.
The administration of structured teaching programme helped the nurses to
understand more about alternative and contemporary modalities.
Most of the nurses were having adequate level of knowledge after the teaching
programme.
The structured teaching programme is proved to be very effective method of
transforming information.
Nursing implications
The findings of the study have implications on the field of nursing education,
nursing practice, nursing administration and nursing research.
Nursing education
92

Education is the key component to update and improve the knowledge of an
individual. In the present scenario, knowledge on alternative and contemporary
modalities of pain relief in first stage of labour is much deficient among the nursing
students as well as the nursing staffs as this body of knowledge is not fully developed
and is still on the path of expansion and discoveries. Hence, there is a dire need to
include these components into present curriculum prescribed by INC. It is the duty of
maternity nurses to educate their clients. Hence, to excel in this strategy nurses need
to be well equipped with enormous amount of knowledge that will convince clients
approaching them. In-service education regarding this topic should be conducted to
improve the knowledge of the staff nurses who are working in the obstetric
departments.
Nursing administration
Nurse administrators are the key persons to plan, organize and conduct in-
service education programmes. Nurse administrator’s support should be necessary to
conduct and evaluate health education programmes. They can help to improve the
knowledge of the staff nurses working in maternity departments by providing various
teaching programmes with the help of various AV aids. They are in a key position to
organize, implement and evaluate educative programmes which will in turn helps to
improve the knowledge as well as to meet the future needs and accelerate the
standards of maternity services.
Nursing practice
Nursing is an art and a science. As a science, nursing is based upon a body of
knowledge that is always changing with new discoveries and innovations. When
nurses integrate the science and art of nursing into their practice, the quality of care
provided to clients is at a level of excellence that benefits clients in numerous ways.
93
They are the key persons of the health team, who plays a vital role in the promotion
and maintenance of health. They can provide adequate teaching to both parents and
family members so that they will come to know about the advantages of the vast
developing field of pain relief during labour through alternative modalities. Hence the
nurses should have adequate knowledge about these modalities to improve the
standards of maternity care.
The major role and responsibilities can be summarized as:
Identifying the problems of the woman in labour
Providing appropriate information regarding the topic alternative modalities of
pain relief during labour
Helps the women to ventilate all their doubts by interpersonal interactions.
Helps the women in labour to select the appropriate modality for effective pain
relief.
Effective application of alternative modalities of pain relief during first stage
of labour and thereby managing labour pain effectively.
Nursing research
The main goal of the nursing research is to improve the knowledge of staff
nurses through the implementation of evidence based practice. The study provides a
baseline data for conducting other research studies. The study will be a motivation for
the budding researchers to conduct similar studies in large scale. The study will be a
reference for the research scholars. Further research works can be conducted with
every medical condition to identify most effective knowledge imparting strategies.
Limitations
The following points were beyond the control of the investigator:
Study is limited only those who are willing to participate in the study
94

Study samples were small
There were limitations due to the duty schedule of the nurses
The study was limited to the experience of the researcher
The relevant study was scanty as very few nursing studies were conducted on
alternative and contemporary modalities of pain relief during first stage of labour.
The study was confirmed to only on selected hospital, which obviously imposed
limits to larger generalizations.
Recommendations
On the basis of the findings of the study, the following recommendations have been
made:
a. A similar study can be replicated on a large scale to generalize the findings.
b. A similar study can be conducted to find the differences in the knowledge level of
the staff nurses on the basis of various institutional settings such as government
and private institutions.
c. A similar study can be conducted to find differences the knowledge level of the
nursing students as well as the nursing staffs.
95

8. SUMMARY
Statement of the problem
“A STUDY TO ASSESS THE EFFECTIVENESS OF STRUCTURED
TEACHING PROGRAMME ON KNOWLEDGE OF STAFF NURSES
REGARDING SELECTED ALTERNATIVE AND CONTEMPORARY
MODALITIES OF PAIN RELIEF DURING FIRST STAGE OF LABOR IN
SELECTED MATERNITY HOSPITALS, BANGALORE.”
Objectives of the study
1. To assess the knowledge of staff nurses regarding alternative and contemporary
modalities of pain relief during first stage of labor by conducting pre-test.
2. To assess the effectiveness of structured teaching programme regarding alternative
and contemporary modalities of pain relief during first stage of labor by using
post-test scores.
3. To find out the association between pre-test knowledge scores and selected
demographic variables
Hypothesis
H0-There is no significant difference between mean pre-test and post-test knowledge
scores regarding alternative and contemporary modalities of pain relief.
H1-The mean post test knowledge scores of staff nurses exposed to structured
teaching programme regarding alternative and contemporary modalities of
96

pain relief will be higher than the mean pre-test knowledge scores as measured
by knowledge questionnaire at 0.05 level of significance
H0.1-There is no significant association between pre-test knowledge scores and
selected demographical variables
H1.1-There is a significant association between pre-test knowledge scores and
selected demographical variables
Conceptual frame work and methodology
The conceptual framework of the present study was based on Von Ludwig
Bertalanffy’s General Systems Theory.
This study adopted quasi-experimental one group pre-test post-test research
design. In the present study, a total of 60 staff nurses working in maternity
department were selected from Fortis Hospital, Bangalore. Samples were
selected by using non probability purposive sampling technique.
The tool used for data collection consisted of Performa for socio-demographic
data and structured questionnaire.
Three types of variables were identified in the present study. Independent refers
to the structured teaching programme regarding alternative and contemporary
modalities of pain relief during first stage of labour and dependent variables
refer to the knowledge of staff nurses regarding alternative and contemporary
modalities. Demographic variables selected for this study were age (yrs),
qualification, experience and religion.
The instrument used for data collection was self administered knowledge
questionnaire on alternative and contemporary modalities. Data collection tool
contain items on the following aspects;
97

Part I: It includes items of demographic variables – age (yrs), qualification,
experience and religion.
Part II: Includes 40 knowledge questions regarding alternative and contemporary
modalities. A structured teaching programme was developed on alternative and
contemporary modalities of pain relief during first stage of labour.
The pilot study was conducted in Fortis Hospital, Bangalore from 1.3.2012 to
10.3.2012to find the feasibility of the study. Ten staff nurses working in
maternity department were selected using purposive random sampling
technique.
The main study was conducted from 15-3- 2012 to 21-4-2012 in Fortis
Hospital, Bangalore. Samples were selected by non probability purposive
sampling technique. Pre-test was administered before structured teaching
programme and post-test was administered after six days.
Data gathered were analyzed using descriptive and inferential statistics and was
presented in tables and graphs.
Major findings of the study
Findings related to demographic variables
It was observed that majority of the respondents i.e. 30 (50%) are in the age
group of 26-30 yrs and 26 (43.3%) are in the age group of 20-25 yrs. Only 4
(6.6%) are in the age group of 31-40 yrs.
It was noted that with regard to the qualification of the staff nurses majority of
them 47(78.3%) have GNM qualification and 13 (21.7%) of them have
completed B.Sc. nursing
It was observed that out of 60 staff nurses majority of them 27(45%) have 4-6
years of experience and 25(41.7%) of them have1-3 years of experience. 5
98

(8.3%) of them have experience of 7 years and above and only 3(5%) of them
have less than one year experience.
Among the 60 staff nurses, 37(61.7%) were Christians and 23(38.3%) were
Hindus.
Findings related to pre-test and post-test scores
In pre-test knowledge score, highest mean percentage of 61.44% was obtained in
the area of General information about normal labour and the lowest mean
percentage of 19% was in the area of alternative and contemporary modalities.
In post-test knowledge scores, the maximum mean percentage of 90.4% was in
the area of hydrotherapy and the lowest mean percentage of 56.5% was in the
area of alternative modalities.
Findings related to effectiveness of structured teaching programme
Overall mean percentage in post-test knowledge was found to be 80.5% and in
pre-test knowledge was (40.42%), revealing a significant difference in the knowledge
level with their P-value in all areas were 0.001 which was greater than the table value
at 0.05 level of significance. Therefore the null hypothesis (H0) was rejected and
research hypothesis (H1) was accepted, which depicts the effectiveness of structured
teaching programme.
Findings related to association of knowledge scores with selected demographic
variables
In the present study, it is apparent that the pre-test knowledge scores of staff
nurses are found to be statistically not significant with the demographic variables i.e.
age (yrs), qualification, experience and religion. Hence it is proved that there is no
99

significant association between knowledge scores with selected demographic
variables.
As expected in the hypothesis of the study, the investigator found that there
is a significant improvement in the knowledge of staff nurses regarding alternative
and contemporary modalities of pain relief during first stage of labour after the
structured teaching programme. Hence it is concluded that the structured teaching
programme was very effective on alternative and contemporary modalities of pain
relief during first stage of labour staff nurses working in maternity department.
100

BIBLIOGRAPHY
1. Meaning of motherhood. Available from URL:www.articlebase.com
2. Tsweleng Lowsa Mmakwena. A study on experiences of women regarding
pain management during first stage of labor.
3. Dutta DC. Textbook of obstetrics. 7th edition. New central book agency.
4. Susan Orshan. Maternity, newborn and women’s health nursing:
comprehensive care across the life span. Lippincott publishers.
5. Sr. Barthalomea Joseph. A study to assess the effectiveness of acupressure on
labor in full term gravid women in selected hospitals, Mangalore. Unpublished
thesis submitted to RGUHS.
6. Learner’s guide to alternative medicine. Institute of alternative medicine and
research, Kolkata. Available at URL:
www.instituteofalternativemedicine.com
7. Comfort measures during labour. Child birth connections. Available from:
URL: http://www.childbirthconnection.org/
8. April Bolding, Penny Simkin. Update on non-pharmacological approaches to
relieve pain and prevent suffering. British journal of obstetrics and
gynaecology. 2004;49(6):pg 489-504.
9. A leaflet on non-epidural strategies for pain relief during labour. MIDIRS,
Royal College of midwives & national childbirth trust. May 2003. Available at
URL: www.infochoice.org
101

10. Expectant mothers guide. Nativiti women’s health and birth centre Houston.
Available at: www.expectantmothersguide.com
11. Rejane Marie, Gilson Torres, Janmilli Da Costa. Available at URL:
www.pdfcast.org
12. Myra Glajchen, Maulyn Bookbinder. Journal of pain and symptom
management. 2001 april;21(4):307-16.
13. Janet Chawla. Understanding narak rethinking pollution, learning from the
experience and knowledge of midwives. This paper was presented at the
Conference on Religions and Cultures in the Indian Civilisation organised by
CSDS and MANUSHI in December, 2005.
14. Polit DF, Hungler BP. Essentials of nursing research: methods, appraisal and
utilisation. 2nd edition. Lippincott publishers; 1995.
15. Smith CA, Collins CT, Cyna AM, Crowther C. Complementary and
alternative therapies for pain management in labor. Cochrane database syst.
Review, 2006(4) CD003521. Available at URL:
www.ncbi.nlm.nih.gov/pubmed
16. Burns E, Zobbi V, Panzeri D, Oskorochi R. Aromatherapy in childbirth: a
pilot randomized controlled trial. School of health and social care. Journal of
oxford university 2007;114(7):838-844.
17. Effectiveness of aromatherapy in relieving pain during labour. Available at
URL: www.medscape.com
18. Jayalakshmi S, Venkatesan L, Jamuna N. Effectiveness of olive oil massage
upon low back pain of parturient mothers in the first stage of labour.
Nightingale nursing times 2008:October (7);48
102

19. Brown ST, Douglas C, Flood PLA. Women’s evaluation of intra-partum non-
pharmacological pain relief methods used during labour. Journal on perinatal
education 2001;10(3): 1-3
20. Karami NK, Safarzadeh A, Fathizadeh N. Effects of massage therapy on
severity of pain and labour of primi-parous women. Iranian journal of nursing
and midwifery research 2009; 12(1): 6-9
21. Arinolao O, Sanya H, Adermada MA. Effect of controlled breathing on pain
tolerance. Department of physiotherapy, Nigeria.
22. Crandom AJ. Maternal anxiety and obstetric complication. Psychosomatic
research institute, USA 1979; 23(6): 109.
23. Labrecque M, Nouween A, Bergeron M, Rancourt JF. A randomized
controlled trial of non-pharmacological approaches for relief of low back pain
during labour. Journal of family practice 1999; 48: 259.
24. Martensson L, Willin G. Labour pain treated with cutaneous injections of
sterile water: a randomized controlled trial. British journal of obstetrics and
gynaecology 1999; 106:633.
25. Benfield RD, Herman J, Kate VL, Wilson SP, Davis JM. Hydrotherapy in
labour. Research in nursing and health 2001; 24: 57-67.
26. Penny Simkin, Michael CK. Non-pharmacological approaches to management
of labour pain 2007. Available at URL:www.uptodate.com.
27. Roets L, Moru MM, Nel M. Lesotho’s midwife’s utilization of non
pharmacological pain management methods during first stage of labour.
Cochrane database library PMID 1624548.
103

28. Payant L, Davis B, Graham ID, Peterson WE, Clinch J. Nurse’s intentions to
provide continous labour support to women. Journal of obstetrics and neonatal
nursing. July 2008; 37(4):405-414.
29. Kim SS, Exlen JA, Kim KB. Nursing students and faculty member’s
knowledge of experience with an attitude toward complementary and
alternative therapies. Journal of nursing education 2006 September; 45(a):375-
378.
30. Gowri N. Effectiveness of STP on knowledge and practices regarding tobacco
consumption in rural health setting. The nursing journal of India. Feb 2010;
vol(2).
31. Yanichin. Study to assess the effectiveness of organized instruction on
knowledge , skill and attitude of practice of breast feeding in CMC, Vellore
2002.
32. Sarojamma. Study on the knowledge and practice of breast feeding in mothers
of hospitalized infants in Vanivilas hospital, Bangalore 2000
33. Shailaja KG. A study to assess the knowledge and confidence of the primi-
para mothers regarding exclusive breast feeding. Nightingale nursing times.
March 2008 Vol 3(12).
34. Denise F Polit, Cherry Tatano Beck. Nursing research: generating and
assessing evidence for nursing practice. Lippincott publications. 8th edition.
Pg: 105, 139, 337-341, 367, 712.
35. Basavanthappa BT. Nursing research. Jaypee publishers. First edition 2003.
Pg: 49, 66, 93, 215, 219.
104
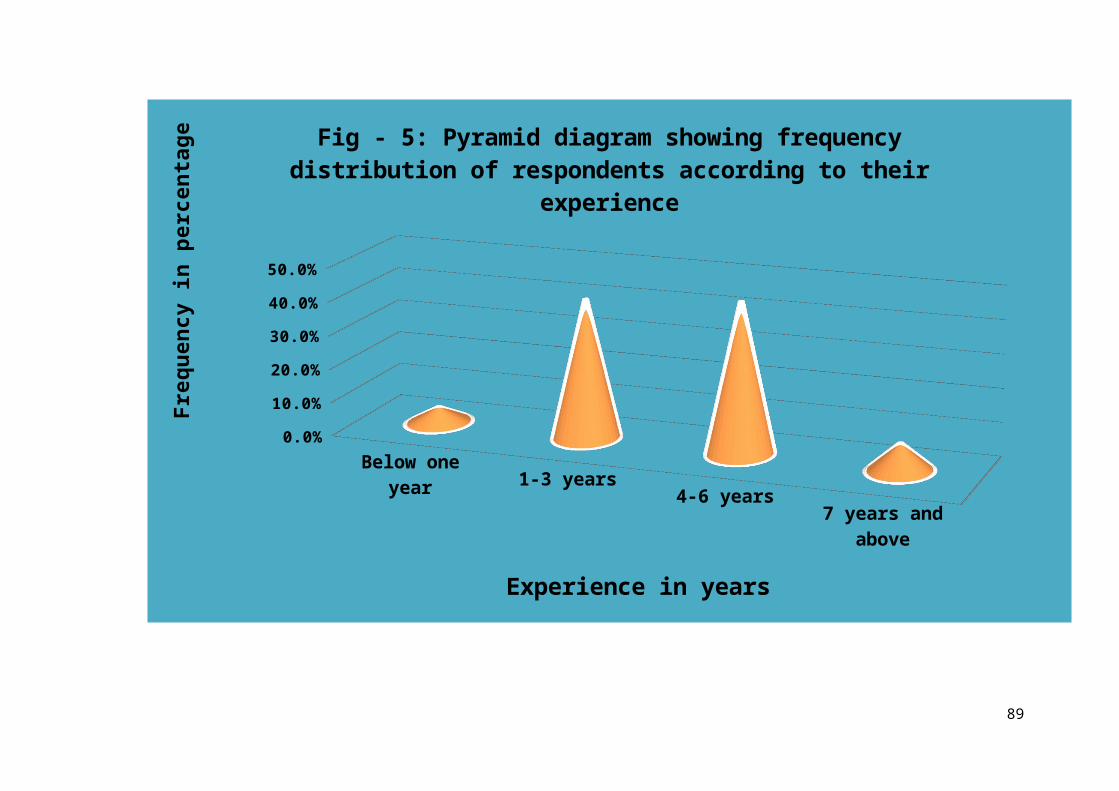
ANNEXURE A
ETHICAL CLEARANCE CERTIFICATE
105

ANNEXURE B
LETTER SEEKING PERMISSION TO CONDUCT THE STUDY
106

ANNEXURE C
LETTER REQUESTING CONSENT TO VALIDATE THE TOOL
107

Date:
FROM,
MS. SHANTI SONU SAM 2nd year M.Sc NursingFortis Institute of NursingBangalore-560078To,
………………………………..........
……………………………...............
Forwarded through:
THE PRINCIPAL,Fortis Institute of Nursing,Bangalore.
Sub: - Requisition for expert opinion on content validity of the research tool.Respected Sir/Madam,
I, Ms. Shanti Sonu Sam, 2nd year M.Sc nursing student of Fortis
Institute of Nursing Bangalore, have selected the topic “a study to assess the
effectiveness of structured teaching programme on knowledge of staff
nurses regarding selected alternative and contemporary modalities of
pain relief during first stage of labour in selected maternity hospitals,
Bangalore” for dissertation to be submitted to Rajiv Gandhi University of
Health Sciences, Bangalore as a partial fulfillment of university requirement
of awarding M.Sc Nursing degree.
Here with I am enclosing a copy of
a) Acceptance form
b) Letter requesting opinions and suggestions from experts
c) Statement of problem, objectives and hypothesis
d) Tool
e) Answer keys
108

f) Blue print
g) Evaluation criteria check list
h) Lesson plan
i) Certificate of content validity
I kindly request you to examine the structured teaching programme and
tool and give your valuable opinion and suggestions for further improvements.
I would be highly obliged and remain thankful for your great help if
you could kindly return this structured teaching programme and tool, after
signing the “ContentValidity Certificate” attached here with, as early as
possible.
Thanking you
Yours sincerely,
Shanti Sonu Sam
Forwarded for expert validation
and approval through, Principal.
109
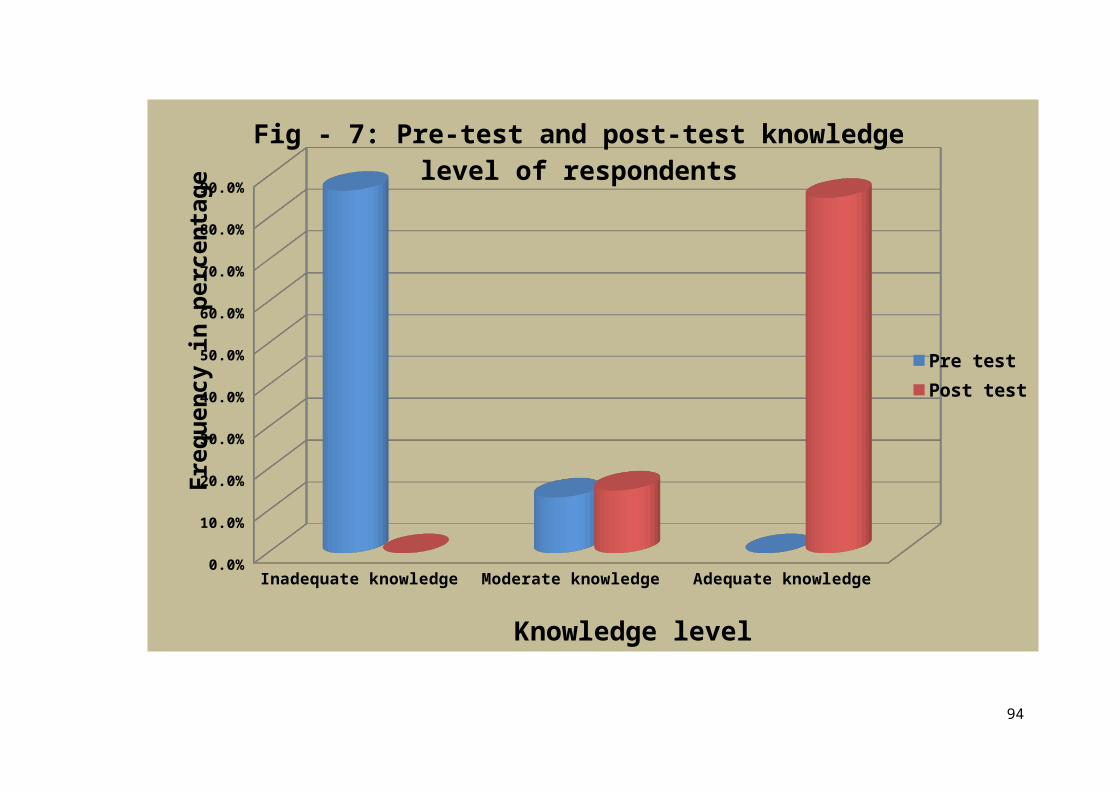
ANNEXURE D
ACCEPTANCE FORM FOR TOOL VALIDATION
Problem statement:
“A STUDY TO ASSESS THE EFFECTIVENESS OF STRUCTURED
TEACHING PROGRAMME ON KNOWLEDGE OF STAFF NURSES
REGARDING SELECTED ALTERNATIVE AND CONTEMPORARY
MODALITIES OF PAIN RELIEF DURING FIRST STAGE OF LABOUR IN
SELECTED MATERNITY HOSPITALS, BANGALORE.”
I……………………………………………….....would/ would not agree upon in
validating the tool.
Name:
Designation:
Address:
Signature:
Date…………….
Place……………
110

ANNEXURE E
CONTENT VALIDATION CERTIFICATE
I hereby certify that, I have validated the tool of Shanti Sonu Sam, IInd year
M.Sc.Nursing student, Fortis Institute of Nursing, Bangalore who is under taking this
study: “A study to assess the effectiveness of structured teaching programme on
knowledge of staff nurses regarding selected alternative and contemporary
modalities of pain relief during first stage of labour in selected maternity
hospitals, bangalore.”
Place:Signature of the Expert.
Date:
Designation and Address.
111

ANNEXURE F
LETTER TO THE PARTICIPANTS REQUESTING CONSENT TO PARTICIPATE IN THE STUDY
Dear participants,
I, Miss. Shanti Sonu Sam, IInd year M.Sc. nursing student of Fortis
institute of nursing, Bangalore, am planning to conduct a research project on “A
study to assess the effectiveness of structured teaching programme on knowledge
of staff nurses regarding selected alternative and contemporary modalities of
pain relief during first stage of labour in selected maternity hospitals,
Bangalore”. I request you to participate in the study.
The information provided will be kept confidential and anonymity will be
maintained throughout and after the study.
Thank you for participating in the study
Yours faithfully
Miss. Shanti Sonu Sam
Date:Place:
112

ANNEXURE G
LIST OF EXPERTS FOR TOOL VALIDATION
1. Mrs. P. Swarnalatha
Principal
BMS Hospital Nursing College
N.R. Colony, Bangalore-560019.
2. Mrs. Reddamma
Professor
Government College Of Nursing, Fort
Banglore-2
3. Mrs. saraswathi
Principal
VenkateshwaraCollege of nursing
Bangalore.
4. Mrs. Balalakshmamma,
Lecturer
The Oxford College of nursing
Bangalore.
113
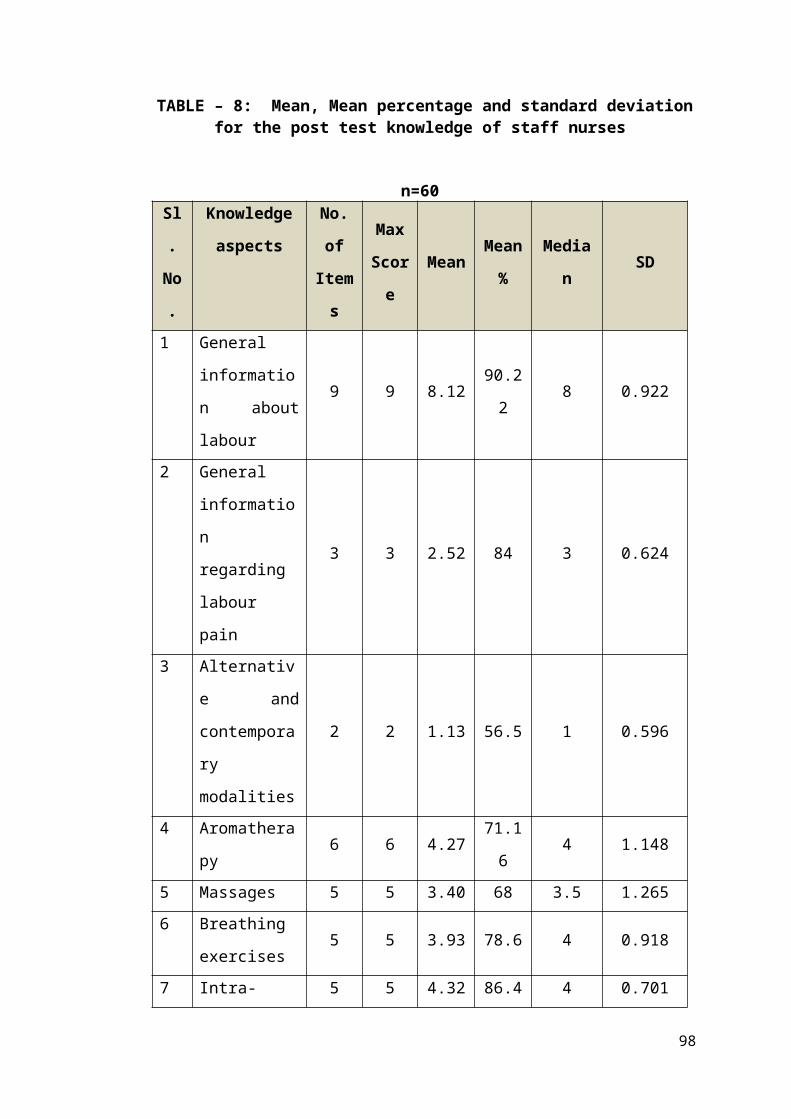
5. Mrs. D. Kanitha
Lecturer
NIMHANS College of nursing
Bangalore.
6. Mrs. Kamala J
Associate Professor
Kempegowda College of nursing
Bangalore.
7.Dr. GayathriKamath
Dept. of Obstetrics and Gynaecology
Fortis Hospitals
Bangalore.
114

ANNEXURE H
BLUE PRINT FOR DISTRIBUTION OF ITEMS
The blue print of the structured questionnaire for assessing knowledge
regarding alternative and contemporary modalities is given below:
AREAS
KNOWLEDGE ASSESSMENT QUESTIONNAIRE
Knowledge Comprehension Application Total items
Percentage
Item no.
No. of items
Item no.
No. of items
Item no.
No. of items
Normal labour 1,2,4,7,8 5 3,5 2 7,9 2 9 22.5
Labour pain 10,11,12 3 - - - - 3 7.5
Alternative modalities 17,18 2 - - - - 2 5
Aromatherapy 15,16,17,19,20 5 18 1 - - 6 15
Massages 21,22,24,25 4 23 1 - - 5 12.5
Breathing exercises 26,29,30 3 27,28 2 - - 5 12.5
Intra-dermal water blocks
31,32,33,34 4 35 1 - - 5 12.5
Hydrotherapy 36,38,39 3 37,40 2 - - 5 12.5
Total no 29 9 2 40
Percentage 72.5% 22.5% 5% 100%
115

ANNEXURE I
TOOL FOR DATA COLLECTION
INSTRUCTIONS
Read the questions carefully
Answer all the questions to the best of your ability
Please tick for the appropriate answer.
Part 1-Details with demographic data.
Part2-Details with structured questionnaire to assess the knowledge
regardingalternative and contemporary modalities of pain relief.
Part 1: Demographic profile
Participant No: _________________________
Date: _________________________
1. Age:______________________
2. Qualification: _____________________
3. Working experience: _____________________
3. Religion: ____________________
116

Part II Structured Questionnaire
Section A: General information regarding labour
1) What is normal labour?
a. It is the expulsion of viable products of conception through
vagina.
b. It is the expulsion of viable products of conception through
womb.
c. It is the removal of viable products of conception through
abdomen.
d. It is the expulsion of products of conception before 28 wks.
2) What is the other name for normal labour?
a Dystocia
b Eutocia
c Delivery
d Caesarean
3) Who is a parturient?
a Postnatal mother
b Person supporting woman in labour
c Person conducting labour
d Woman in labour
4) How many stages are there in normal labour?
117

a One
b Two
c Three
d Four
5) The first stage of labour starts with the onset of:
a Cervical effacement
b True uterine contractions
c Rupture of membranes
d Show
6) What is the duration of first stage of labour in primi
mothers?
a 8-12 hours
b 4-8 hours
c 14-16 hours
d 6-8 hours
7) What is second stage of labour?
118

a It is the stage of full dilatation of cervix
b It is the stage of rupture of membrane
c It is the stage of foetal descend
d It is the stage of foetal expulsion
8) Which stage is characterized by the expulsion of placenta?
a First stage
b Third stage
c Fourth stage
d Second stage
9) Which is the most important aspect of management during
first stage of labour?
a Aseptic precautions
b Psychologicsupport
c Minimizing labour pain
d Maintaining body temperature.
Section B: General information on labour pain
10) Who brought out the concept of gate control theory?
a RonaldMelzack and P D Wall
119

b Penny Simkin and Ronald Melzack
c P D Wall and PennySimkin
d Penny Simkin and April Bolding
11) Where is the pain modulation gate situated?
a Cerebrum
b Cerebellum
c Spinal cord
d Medulla oblongata
12) What are the characteristics of true labour pain?
a Pain is from abdomen, back and then thigh.
b Pain is from back, abdomen and then thigh.
c Pain is felt over lower abdomen and then thigh.
d Pain is felt from lower back to thigh.
Section C: Alternative and contemporary modalities
13) What do you mean by alternative and contemporary
modalities?
a Modalities using medical interventions
120

b Modalities used along with medical interventions
c Modalities other than medical interventions
d Modalities providing permanent relief
14) How do alternative modalities help in minimizing labour
pain?
a By blocking pain receptors
b By blocking pain modulation gate
c By blocking nerve impulses
d By using medical interventions.
Section D: Aromatherapy
15) What is aromatherapy?
a Use of essential oils
b Use of drugs
121

c Use of perfumes
d Use of flowers
16) How does aromatherapy works?
a Stimulates chemo-receptors in oro-pharynx
b Stimulates chemo-receptors in naso-pharynx
c Stimulates pain receptors in naso-pharynx
d Stimulates receptors in naso-pharynx
17) How are essential oils extracted?
a Steam distillation
b Churning leaves
c Blending flowers
d Mixing oils
18) What is usually mixed with essential oils to dilute them?
a Water
b Rose water
c Vegetable oil
122

d Perfumes
19) Which oil can be used in latent phase of first stage of
labour?
a Lavender, rosemary
b Rosemary, jasmine
c Jasmine, lavender
d Lavender, neroli
20) Which oils can be used in active phase?
a Lavender, jasmine, rosemary
b Lavender, neroli, rose
c Jasmine, lavender, sage
d Peppermint, lavender, neroli
Section E: Massage
21) Define massage
a Rubbing muscles
b Pressing the body muscles
c Rubbing and kneading muscles
123

d Stroking body parts
22) How does massage help in minimizing labour pain
a By stimulating the release of endorphin
b By blocking the production of adrenaline
c By promoting uterine contractions
d By promoting muscle relaxation
23) Which massage can be used to warm up women in labour?
a Back massage
b Foot massage
c Shoulder massage
d Sacral massage
24) What is effleurage?
a Making small circles in palm
b Simple stroking of hand, abdomen and back
c Stroking feet and hands firmly
d Light, circular stroking of abdomen, lower back
124

25) What are meissner’s corpuscles?
a Nerve endings
b Sensory receptors
c Nerve fibres
d Pain receptors
Section F: Breathing Exercises
26) How does breathing exercises help in minimizing labour
pain?
a Relieves anxiety and pain
b Relaxes the mother
c Redirects from the painful response
d Reduces pain
125

27) How are breathing exercises beneficial to the baby?
a Provides more oxygen
b Promotes well being
c Promotes health
d Promotes breathing
28) What is the ideal time for breathing exercises?
a During and at the end of contractions
b At the beginning and at the end of contractions
c At the beginning of each contractions
d In between contractions
29) What is slide breathing?
a Four, short, light puffing breaths
b Deep breaths and exhale slowly
c Deep abdominal breaths
d Inhale and exhale with relaxed lips
30) When is light accelerated breathing done?
126

a Latent phase
b Transitional phase
c Active phase
d Expulsive phase
Section G: Intra-dermal water blocks
31) What are intra-dermal water blocks?
a Injecting sterile water
b Sterile water injections intra-dermally
c Sterile injections
d Water injections
32) What is the site for intra-dermal water block?
127

a Posterior inferior iliac spine
b Anterior superior iliac spine
c Posterior superior iliac spine
d Anterior inferior iliac spine
33) How many points are used for intra-dermal water blocks?
a Two
b Three
c One
d Four
34) How does intra-dermal water block minimizing labour
pain?
a By blocking pain transmission
b By stimulating endorphin release
c By reducing anxiety and stress
d By blocking pain receptors
35) What is the precaution to be taken after water blocks?
128
a Avoid wiping
b Avoid massaging
c Avoid repeat injections
d None of the above
Section H: Hydrotherapy
36) What is hydrotherapy?
a Therapy that uses medicines
b Therapy that uses drugs
c Therapy that uses water
d Therapy using massages
37) What is the ideal time to start water immersions?
129

a Cervical dilatation greater than 5 cm
b Cervical dilatation greater than 3 cm
c Cervical dilatation less than 5 cm
d Cervical dilatation less than 3cm
38) What kind of water is used for water immersions?
a Lukewarm water
b Cold water
c Clean water
d Warm water
39) How long should mother stay in water tub during
immersion?
a 2 hours
b 3hours
c 20 min
d 4 hours
40) How does buoyancy help in minimizing labour pain?
a Relieves pressure on joints and muscles
130

b Reduces pain on muscles
c Increases circulation
d Decreases fluid retention.
131

LESSON PLAN ON
ALTERNATIVE AND CONTEMPORARY MODALITIES OF PAIN RELIEF DURING FIRST
STAGE OF LABOUR
GUIDED BY, SUBMITTED BY,
MRS. GOWRI SAYEE MS. SHANTI SONU SAM
ASSOCIATE PROFESSOR 2ND YEAR M.Sc NURSING,
OBSTETRICS AND GYNAECOLOGICAL NURSING OBSTETRICS AND GYNAECOLOGICAL NURSING
FORTIS INSTITUTE OF NURSING FORTIS INSTITUTE OF NURSING
NAME OF THE INSTITUTION Fortis institute of nursing
132

COURSE M.Sc. nursing 2nd yearSUBJECT Obstetrics and Gynaecological NursingTOPIC Alternative and contemporary modalities
NAME OF THE RESEARCH GUIDE Mrs. Gowri Sayee Associate Professor
NAME OF THE CO-GUIDE Mrs. Sabitha Sibbala Associate Professor
NAME OF THE RESEARCHER Ms. Shanti Sonu SamPARTICIPANTS OF THE STUDY Staff nursesDURATION 1hourMETHOD OF TEACHING Lecture cum discussionMEDIA OF TEACHING Power point, Black board
133

GENERAL OBJECTIVES
At the end of the class the participants will be able to gain knowledge regarding alternative and contemporary
modalities of pain relief during first stage of labour and will be able to apply that knowledge in their practical life situation.
SPECIFIC OBJECTIVES
At the end of the class participants will be able to:
• Introduce the topic
• Define alternative and contemporary modalities
• Describe about aromatherapy
• Describe the process of massaging
• Explain the different types of massages
• Explain the different types of breathing exercises
• Explain about intra-dermal water blocks
• Describe about hydrotherapy
134

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
135

1 2 min To
introduce
the topic
INTRODUCTION:
Birth is a normal, healthy part of a woman’s
life. This unexplainable happiness is usually
accompanied by severe pain due to contractions.
The amount of pain a woman experiences is
influenced by many individual, physical,
emotional and environmental factors. There are
several measures used for relieving pain during
labour. Alternative and contemporary modalities
are one among them; it refers to all those
therapies not provided by the conventional
methods. These modalities boosts up the
confidence of the women, hence these modalities
should be made available.
Introducing
the topic
Listening
136

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
2 2 min To review
about
normal
labour.
PHYSIOLOGY OF NORMAL LABOUR
The precise mechanism of initiation of labour is
still obscure. Series of events that take place in the
genital organs to expel the viable products of
conception out of the womb through the vagina
into the outer world is called normal labour. It’s
otherwise called eutocia.
Stages of labour:
Normal labour is divided into 4 stages.
First stage of labour starts from the onset of
true labour pains and ends with full dilatation of
cervix. Its average duration is about 12 hrs in
primi-gravida and about 6 hrs in multi-gravida.
Reviews
about
normal
labour
Listens What is
normal
labour?
137

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
Second stage starts from full dilatation of
cervix till expulsion of fetus. Full cervical
dilatation is upto 10 cm.
Third stage begins after the expulsion of fetus
and ends with the expulsion of placenta and
membranes.
Fourth stage is the stage of observation for at least
one hour after the expulsion of placenta and
membranes.
138
SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
3 2 min To explain
about
labour pain
PHYSIOLOGY OF LABOUR PAIN
The first symptom to appear in first stage of labour
is painful intermittent contractions. This pain is felt
anteriorly with simultaneous hardening of the
uterus. Initially the pain is not strong enough and
come at various intervals of 15-30 min with
duration of about 30 sec. The pain starts from the
abdomen, back and then radiates to thigh.
Probable causes of labour pain are:
• Myometrial hypoxia.
• Stretching of perineum over the fundus.
• Stretching of cervix during dilatation.
• Compression of nerve ganglion.
Explaining
about
labour pain
Listening What are the
causes of
labour pain?
139

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
4 2 min To explain
about pain
relief
measures.
PAIN RELIEF MEASURES
Normal labour may be easy and trouble free
provided a rational approach is made with the
beginning of pregnancy. Pain can be relieved by
various measures:
Sedatives and analgesics.
Epidural analgesia.
Inhalation agents.
Alternative and contemporary modalities.
Due to various research evidences of their
effectiveness, popularity among patients, no side
effects, natural pain relief alternative and
contemporary modalities can be considered much
effective.
Explaining
about pain
relief
measures
Listening slide Name the
different
pain relief
measures?
140

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
141

5 2 min To introduce
about various
modalities
ALTERNATIVE & CONTEMPORARY
MODALITIES
Alternative and contemporary modalities are
those therapies given other than the usual
medical interventions. Some of the benefits:
It considers human body as a whole.
There are no side effects.
They are easily affordable.
Simple to prescribe and practice.
It does not interfere with the progress of
labour.
Promotes a sense of accomplishment.
They have no effect on state of
consciousness.
Introducing
about
alternative
modalities
Listening Board What are the
advantages?
142

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
GATE CONTROL THEORY
• It implies that a non-painful stimulus can
block transmission of a noxious stimulus.
• It is based on the premise that the gate
modulates the pain impulses.
• There are three types of nerve fibres: A-Delta
fibres(sharp pain), C fibres(dull pain), A-Beta
fibres(light touch).
• The substantia gelatinosa acts as the
modulating gate.
• A-Delta and C firbres open the gate and A-
Beta fibres close the gate.
• Alternative modalities activate the A-Beta
fibres and thus the gate is closed.
143

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
6 10
min
To explain
about
aromatherapy
AROMATHERAPY
Aromatherapy is the science of using highly
concentrated essential oils or essences distilled
from plants in order to utilize their therapeutic
properties. The use of aromatic substances
stimulates the chemoreceptor sites in the naso-
pharynx and directly affects the hypothalamic-
pituitary,adrenal axis. Administration includes
putting drops in a pillow, in a bath, or in
awoman’s brow. Essential oils are as potent as
drugs and equally open to misuse or abuse.
Explaining
about
aromathera
py
Listening PPT Explain about
aromatherapy
144
SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
Important essential oils
(1) Lavender Oil
Lavender oil is extracted from the flower
of lavender primarily through steam distillation.
The benefits of lavender oil are:
It’s balancing and calming.
It relieves tension and stress.
It induces sleep and reduces pain.
145

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
(2) Peppermint Oil:
Peppermint is a cross between the watermint
and spearmint and is native to Europe. Some of
the benefits are:
It’s cooling and refreshing.
It relieves nausea and headache.
It also reduces pain.
It improves immunity.
(3) Rosemary Oil:
Rosemary is very popular in the
Mediterranean region as an herb. Some of the
benefits are:
It relieves pain and strengthens the body.
It’s used for hair, mouth and skin care.
It boosts mental activity.
146

It can be used as room freshener too.SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
147

(4) Neroli Oil:
Neroli oil has been widely used across the world
for centuries. Derived from the blossoms of
bitter orange tree. It is extracted by steam
distillation. Some of the benefits are:
It has a soothing and relaxing effect.
It relieves headache and nausea.
It prevents the scarring of skin.
It also improves digestion.
(5) Rose Oil:
Rose oil is extracted from fresh Damascus rose
by steam distillation. Some of the benefits are:
It is an uterine tonic and supports labour.
It is an anti-depressant.
It reduces nausea and fatigue
SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
148
(6) Jasmine Oil:
Jasmine oil is extracted from the flowers of
jasmine, the very famous flower. Some of the
benefits are:
It is uplifting and balancing.
It eases birth and reduces pain.
It also acts as a sedative.
It relieves anxiety.
SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
149

Aromatherapy can be used according to
different phases of first stage:
Latent Phase:
During the early phase of labour when
contractions begin, the mother should relax and
take a nap if possible. In a 10ml bottle pour
4drops of lavender, 2 drops of neroli and add
vegetable oil. Massage temples, forehead and
chest and advice to take deep breaths.
Active Phase:
During this phase, contractions become intense
and frequent. In 10ml bottle pour 6 drops
lavender, 1drop neroli, 1drop rose oil and add
vegetable oil. Massage and advice to breathe
and relax.
150

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
7 5 min To explain
about various
massages.
TOUCH AND MASSAGES:
Touch and massages stimulates the body to
release endorphins which are natural pain killing
and mood lifting hormones. Some of the
massages are:
(1) Hand massages:
Simply stroke each hand in turn, first on the
back, then on the palm, sweeping firmly down
from wrists to fingertips. Make small circles all
over the palm.
Explaining
about
various
massaging
techniques
Listening PPT What are the
different
types of
massages?
151

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
(2) Foot massages:
Simply stroke feet firmly from ankle to toes or
make circles with thumb all over the soles of
feet. Feet become cold during labour and a foot
massage can help to warm up.
(3) Effleurage:
Light circular stroking of abdomen and lower
back. It stimulates nerve endings called
meissner’s corpuscles which travel faster than
signals of a pain thereby blocking pain
transmission. Use a flat hand stroke on the arms,
legs and broad flat surface of the back.
Effleurage with only fingertips gliding is called
feathering.
152

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
(4) Back massage:
Firm massage can be applied on lower back to
relieve contraction and discomfort from long
hours of labour.
(5) Shoulder massage:
This massage can be performed to facilitate
breathing and relaxation.
(6) Knee press:
Make the woman to sit on a firm chair with
feet touching the floor. Kneel on the floor and
extend hands out to her knee and cover her
knees. During a contraction lean on body weight
and apply pressure to her knees.
153

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
(7) Sacral massage:
Use the palm of hand over the sacral area and
massage firmly. The hand not being used is
supporting the woman either on hip or shoulder.
(8) Circular hip massage:
Either the woman kneels on the floor or against
the head of a bed and supported by pillows.
Two hands are placed on either side of the spine
in the sacral region with the hands pointing in
an upward direction.
154

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
8 5 min To explain
about
breathing
exercises.
BRETHING EXERCISES:
It simply means breathing at any number of
possible rates and depths. The theory behind
breathing patterns is that the thought process is
redirected from the painful response. Breathing
exercises should be done at the beginning and at
the end of each contraction. Some of the
breathing exercises are:
(1) Slow breathing:
Begin slow breathing when contractions
are intense enough.
Take an organizing breath.
Release all tension and breathe out.
Focus attention.
Explaining
about
breathing
exercises
Listening PPT What are
breathing
exercises?
155

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
(2) Light accelerated breathing:
Keep breathing shallow and light.
The inhalation should be quiet, but
exhalation clearly audible.
Take a deep breath, release all tension
and breathe out
Focus attention.
Exhale through mouth.
(3) Variable transition breathing:
Referred as pant-pant-blow breathing.
Take an organizing breath, release all
tension and breathe out.
Breathe out through mouth in light
shallow breaths.
156

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
After every second, third, fourth or fifth
breaths blow out a longer breath.
(4) Slow relaxed abdominal breathing:
Inhale slowly through nose, allowing
belly to expand first then chest.
Exhale slowly through mouth pursing
lips.
6-9 breaths to be taken.
(5) Slide Breathing:
Four, short, light puffing breaths.
157
SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
9 5 min To explain
about intra-
dermal water
blocks.
INTRA-DERMAL WATER BLOCKS
It is a new technique for non-narcotic pain relief
originally developed to relieve pain from kidney
stones. With slight modifications it can be used
in labour, especially for posterior positions.
Procedure:
• Fill a small tuberculin syringe with sterile
water
• Identify the posterior superior iliac spine
and mark them
• Approx. 3 to 4 cm down and 1 to 2 cm in
identify other two points and mark them.
• During a contraction inject a small
amount of sterile water into the skin
raising a bleb.
Explaining
about intra-
dermal
water
blocks
Listening PPT What is intra-
dermal water
blocks?
158

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
• Repeat at the other three sites as quickly
as possible.
• During the injection the woman will feel
a sharp stinging pain.
• The stinging will fade in 10 to 15 sec.
• Avoid back massage after the water
block as it could shorten the duration of
action.
• The small blebs block the pain
transmission as explained by gate control
theory.
159

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
10 5 min To explain
about
hydrotherapy
HYDROTHERAPY
One of the safest and most effective forms of
pain relief in labour is the immersion in deep
water or a warm shower. Hydrotherapy has been
used for relaxation, healing and pain relief for
centuries. It relieves the stretching sensations of
ligaments and areas associated with posterior
presentation.
Mode of action
The hydrostatic pressure of water relieves
some of the discomforts of contractions.
Warm water soothes tired and aching
muscles.
Explaining
the use of
hydrothera
py
Listening PPT Explain the
use of
hydrotherapy
in labour.
160

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
There are three factors that contribute to
the benefit of hydrotherapy: heat,
buoyancy and massage.
Immersion in water results in increased
circulation.
It lowers the blood pressure and decrease
any fluid retention or swelling.
The buoyancy of water creates a
weightless feeling and promotes
relaxation.
The mother should get into bath tub at around
4 to 5cm cervical dilatation. Time in tub should
be limited to 2 hours. Warm water should be
used.
161

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
11 2 min To conclude
the topic
CONCLUSION
Alternative and contemporary modalities are the
techniques which imparts a sense of well being
in an individual with the desired effect. The
main advantage is that it can be discontinued at
any time without any side effects. Midwives
should possess adequate knowledge about these
modalities.
Concluding
the topic,
asking
questions.
Asking
doubts.
162

SL
NO
TIME SPECIFIC
OBJECTIVE
CONTENT TEACHER’S
ACTIVITY
LEARNER’S
ACTIVITY
AV
AIDS
EVALUATION
12 BIBLIOGRAPHY
1. Dutta D.C. Textbook of obstetrics. 1st edition,
2004. Central agency, New Delhi.
2. Annamma Jacob. A comprehensive textbook
of midwifery. Jaypee publications, New Delhi
2005.
3. Trolle B, Moller M, Kronberg H, Thomson S.
The effect of sterile water blocks on low back
pain. British journal of obstetrics and
gynaecology. 1991; 164; pg 1277-81.
4. www.wikipedia.org
5. www.expectantmothersguide.com
6. www.aromalchemy.com
7. www.womenshealth.com
163

164

165

0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
61.44%
52.33%
19.00%
32.83%
22.60%
37.00%41.00%
49.60%
40.42%
90.22%84.00%
56.50%
71.16% 68.00%
78.60%86.40%
90.40%
80.50%
Fig -10: Comparison of pre and post test knowledge scores of the respondents
Pretest Scores
Post-test scores
166

167

SECTION IV: ASSOCIATION OF PRE TEST KNOWLEDGE SCORES WITH DEMOGRAPHIC VARIABLES
Table – 10: Association of pre test knowledge scores of staff nurses with selected demographic variables
n= 60
Variables Below Median
Median and above
Chi square Df P value
(0.05)Inferen
ce
Age in years
20-25 years 12 14
0.292 3 7.82 NS26-30 years 12 18
31-35 years 1 1
36-40 years 1 1
Qualification
GNM 18 292.240 1 3.84 NS
B.Sc. Nursing 8 5
Experience
Fresher 3 0 5.038 3 7.82 NS
1-3 years 10 15
4-6 years 10 17
16

7 years and above 3 2
Religion
Hindu 8 151.111 1 3.84 NS
Christian 18 19
The above table 9 shows that there is no significant association between age of staff nurses and total pre-test knowledge scores (chi square-
0.292, Df-3, P value -7.82). Similarly the other demographic variables viz; qualification (chi square – 2.240, Df – 1, P value – 3.84), experience
(chi square – 1.111, Df – 1, P value – 3.84) also have no association with the total knowledge scores of staff nurses as they are found to be non-
significant at 0.05 level of significance. Hence the null hypothesis (H0.1) is accepted and research hypothesis (H1.1) rejected.
17

18