Embed Size (px)
Citation preview
Rheumatic FeverLicks the joints, bites the heart
Clare O’Donnell – Paediatric Cardiologist with thanks to Marion Hamer Nurse Practitioner - Paediatric Cardiology Paediatric and congenital cardiac servicesStarship Hospital
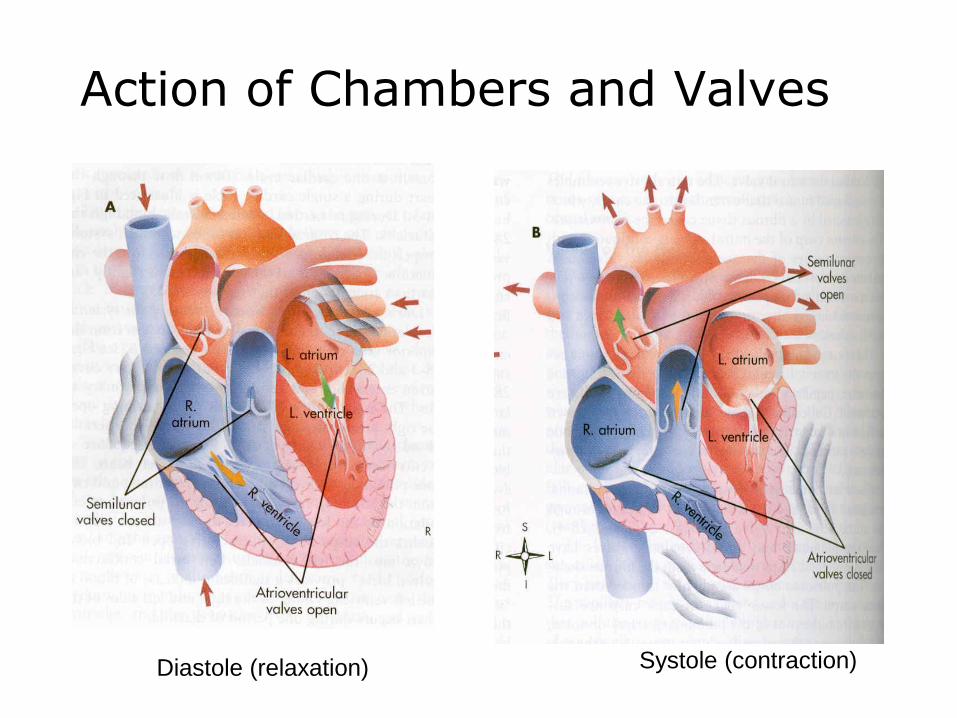
Action of Chambers and Valves
Diastole (relaxation) Systole (contraction)
Rheumatic fever - Epidemiology• Acute rheumatic fever (ARF) remains the most common
cause of acquired heart disease in children around the world
• The highest documented rates in the world have been in in Maori and Pacific people in NZ, Aboriginal Australians and those in the Pacific nations.
• ARF incidence is a sensitive marker of childhood disadvantage
• ARF tends to run in families and is more common in females
• Incidence peaks in the 5 – 14 year age group
Acute Rheumatic Fever
• Acute rheumatic fever starts after an illness with the Group A streptococcal bacteria (GAS infection)
• Usually from a sore throat - streptococcus pyogenes
• In some children this causes an autoimmune response (body attacks own tissue)
• Affects mainly the heart, joints, brain and skin
• Damage to the heart: mitral and /or aortic valve
• Reoccurrences common if no preventative measures and may cause further cardiac valve damage.
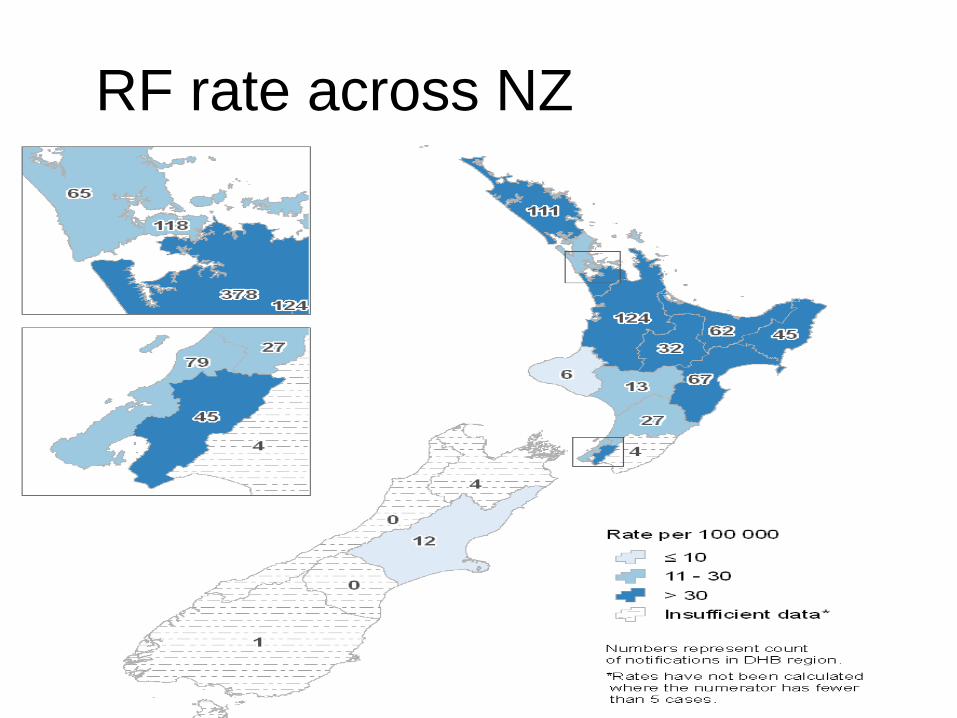
RF rate across NZ
Government response
• Rheumatic fever target as part of the
Better Public Services initiative
• Stop it: Prevent transmission of Strep A
sore throats
• Treat it: Treat Strep A throats quickly and
effectively
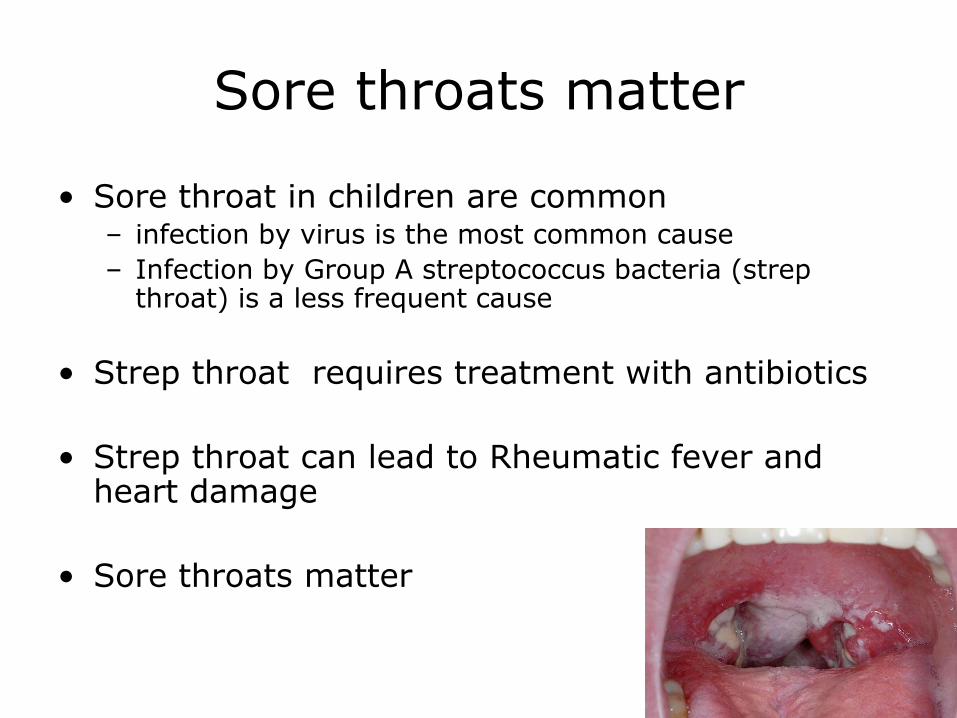
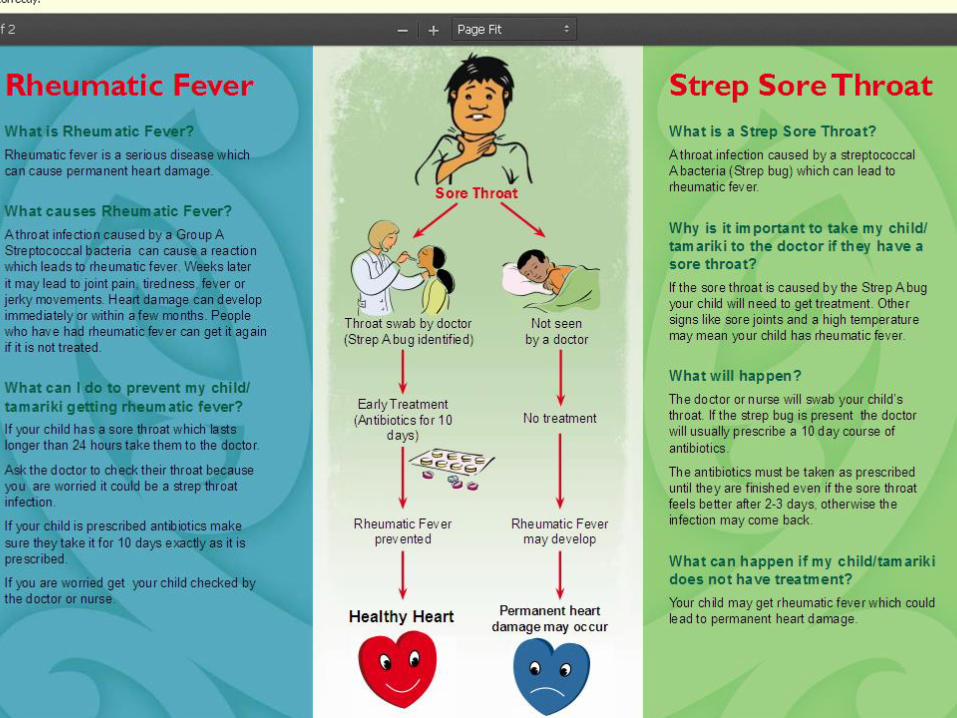
Sore throats matter
• Sore throat in children are common– infection by virus is the most common cause
– Infection by Group A streptococcus bacteria (strep throat) is a less frequent cause
• Strep throat requires treatment with antibiotics
• Strep throat can lead to Rheumatic fever and heart damage
• Sore throats matter
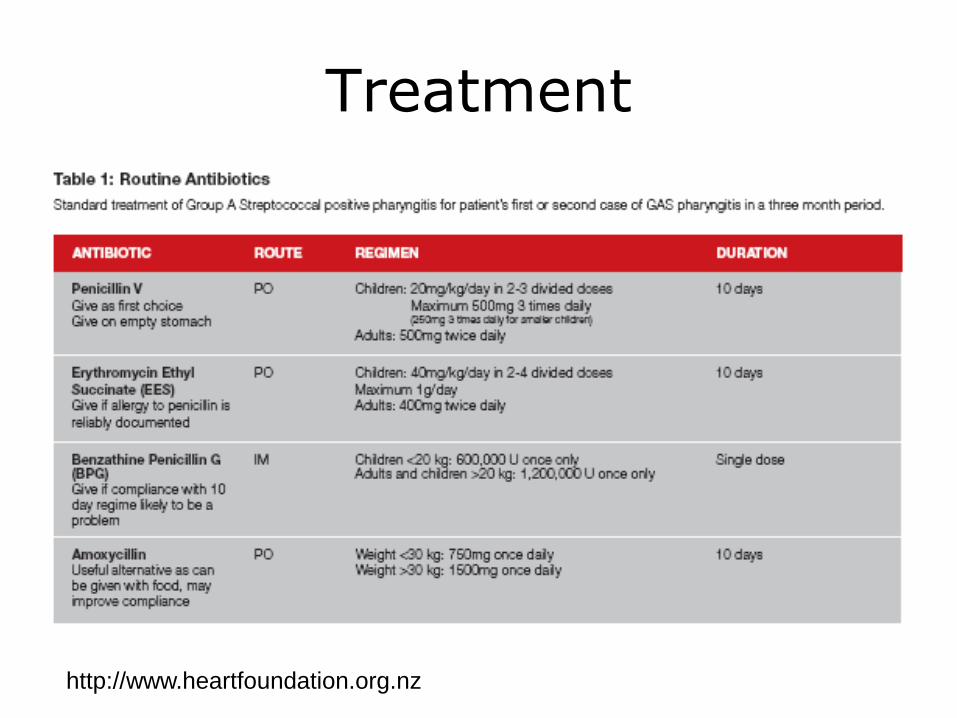
Treatment
http://www.heartfoundation.org.nz
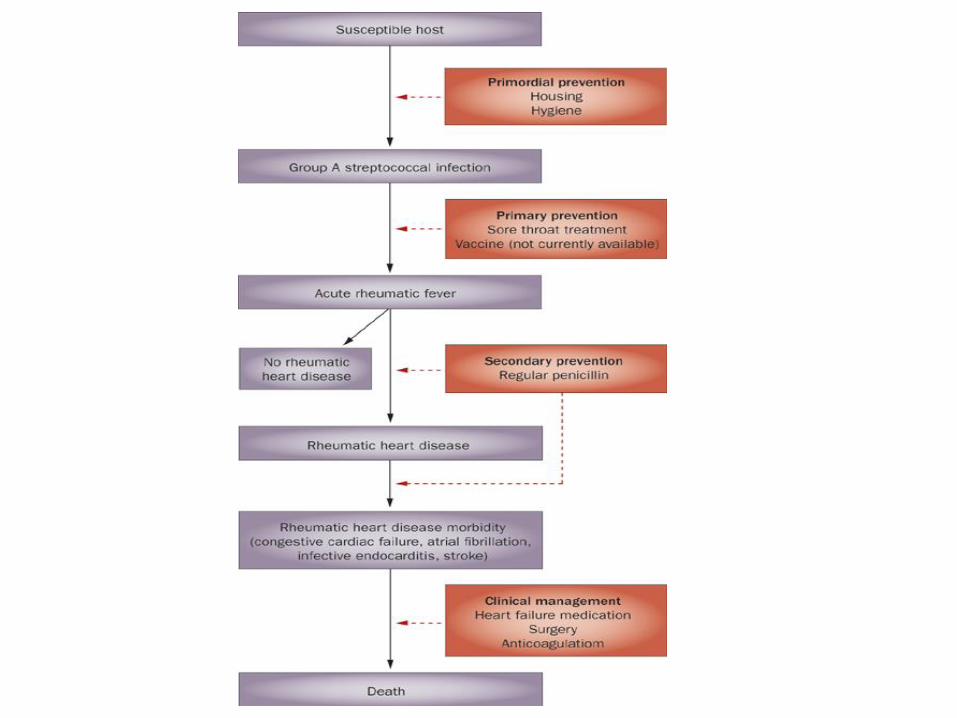
Primary prevention
• Alleviating child poverty
• Education
–Sore throats matter – get seen and get treatment
–Hand hygiene
–Safe sneezing / coughing into the elbow

Faith - 6 years
old Symptoms
• Chest pain – left side
• short of breath while lying flat and on exertion
• Cough
• Vomiting
• Fevers
• Achy and tired
• Murmur
• Sore left knee, swollen / hot
History
Previously well and active
• No regular medicines,
• immunised
• occasional sore throat,
• About 4-6 weeks ago had sore throat, mild cold / sniffles and a bit sore and achy and got better .
• Unwell about 2 weeks ago – left sided chest pain. Also had a sore ankle and couldn’t walk
• One week ago - breathless, chest pain, fever, nausea, vomiting lethargy. Had a sore ankle.
On arrival in hospital:
• cough, left upper quadrant pain and chest pain, breathless, can’t lie flat , fevers, feel miserable and achy
• no sore throat, no diarrhoea, no rash
• Mum says sore knee came on that morning
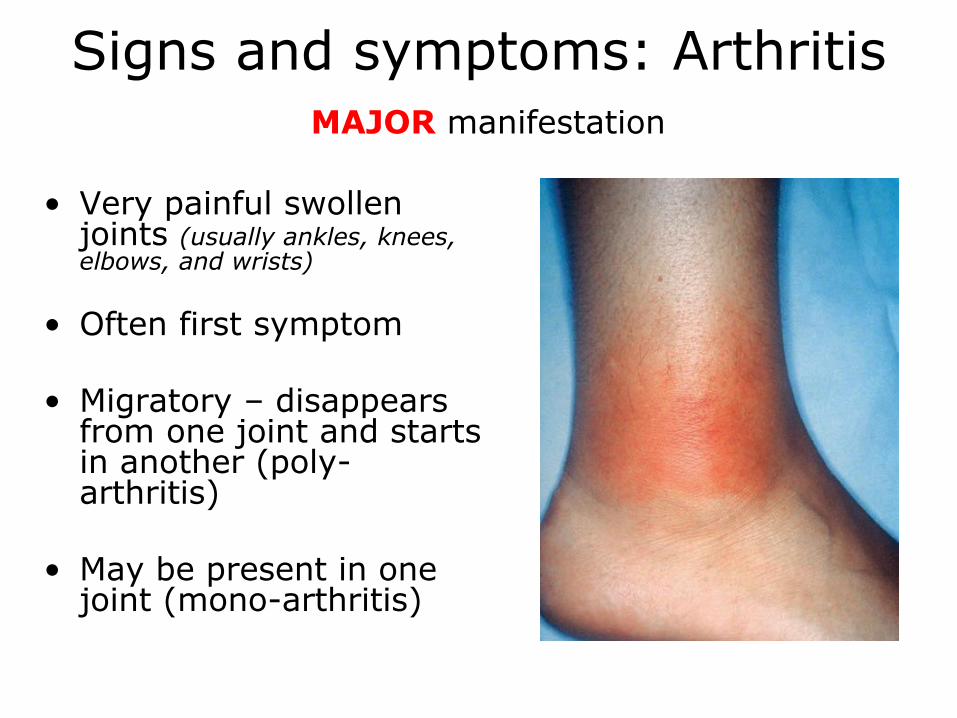
Signs and symptoms: ArthritisMAJOR manifestation
• Very painful swollen joints (usually ankles, knees, elbows, and wrists)
• Often first symptom
• Migratory – disappears from one joint and starts in another (poly-arthritis)
• May be present in one joint (mono-arthritis)
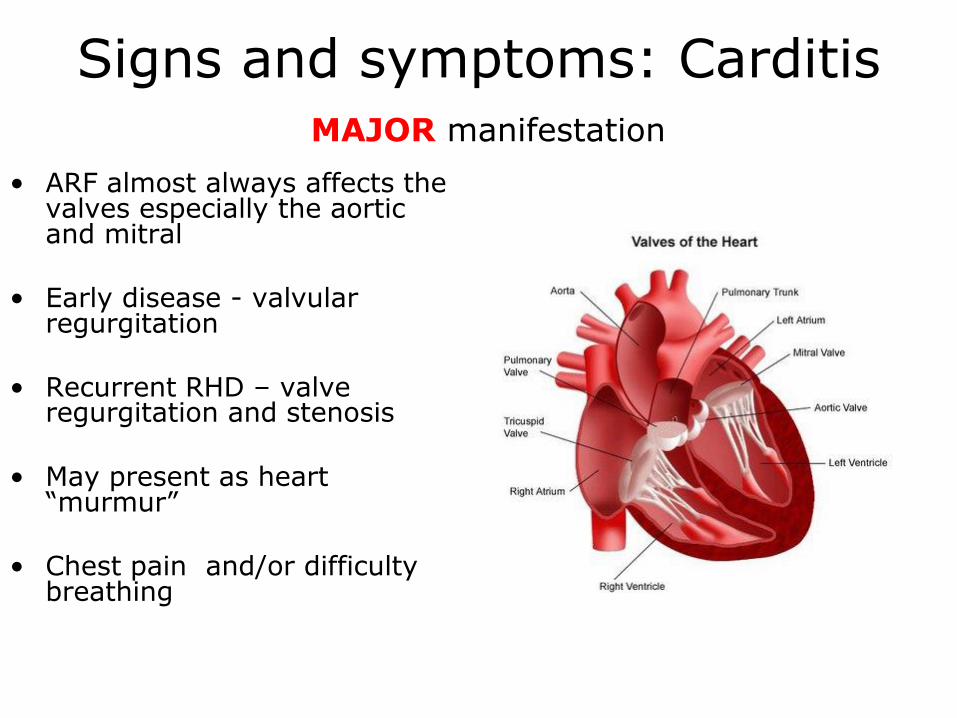
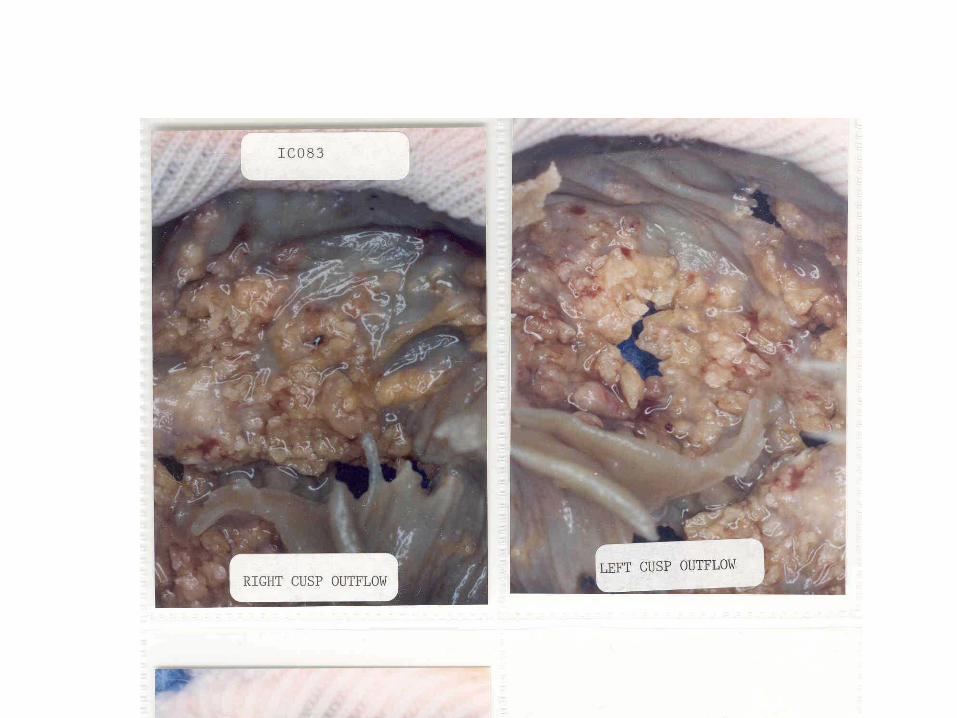
Signs and symptoms: Carditis MAJOR manifestation
• ARF almost always affects the valves especially the aortic and mitral
• Early disease - valvular regurgitation
• Recurrent RHD – valve regurgitation and stenosis
• May present as heart “murmur”
• Chest pain and/or difficulty breathing
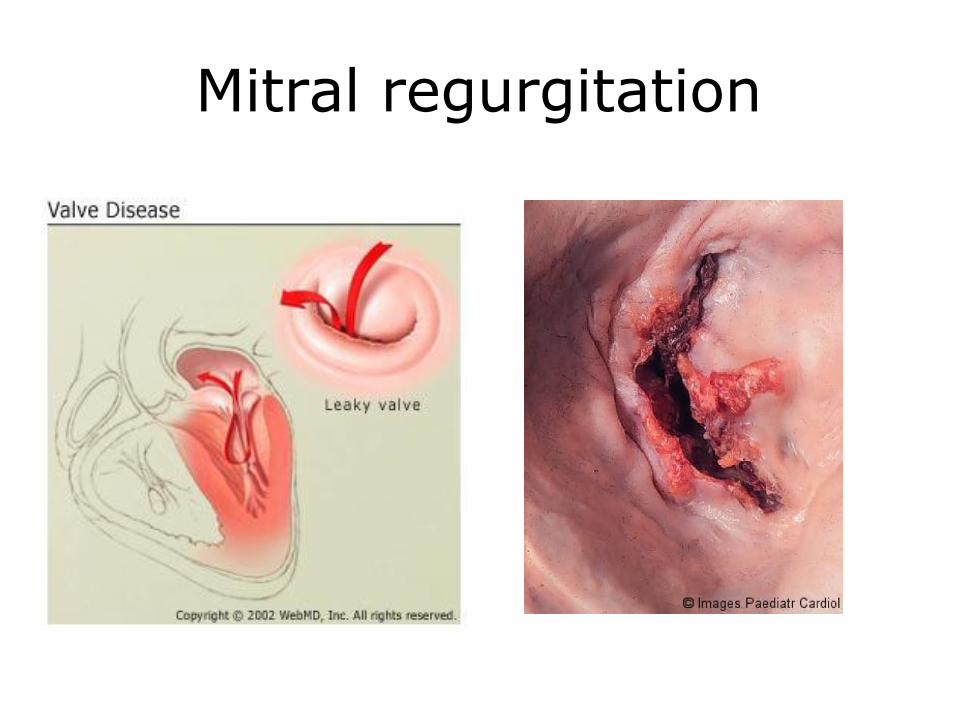
Mitral regurgitation
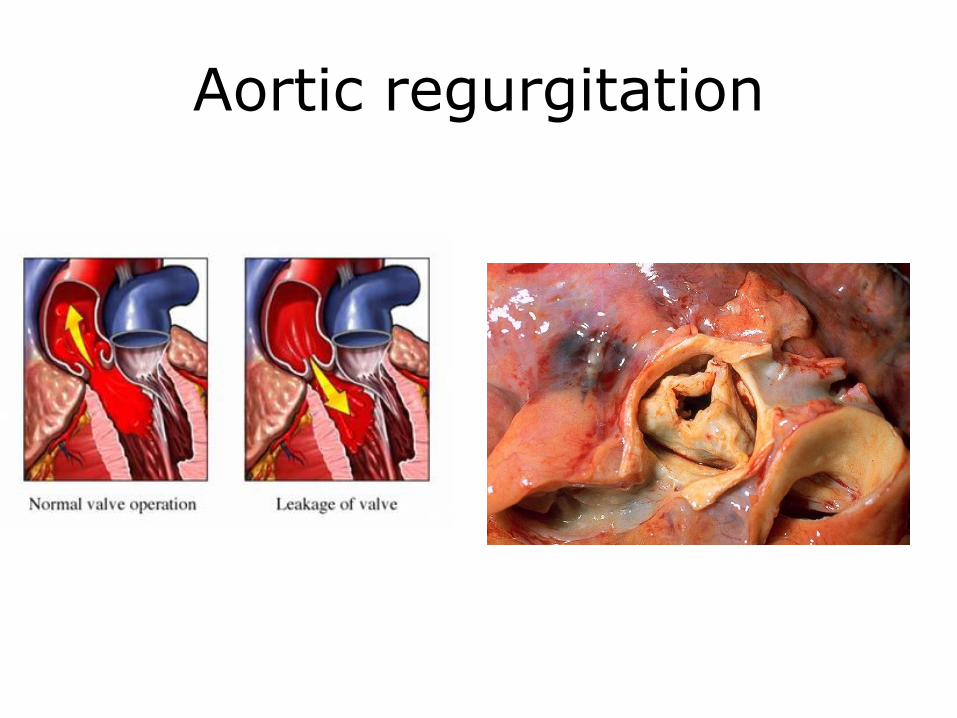
Aortic regurgitation
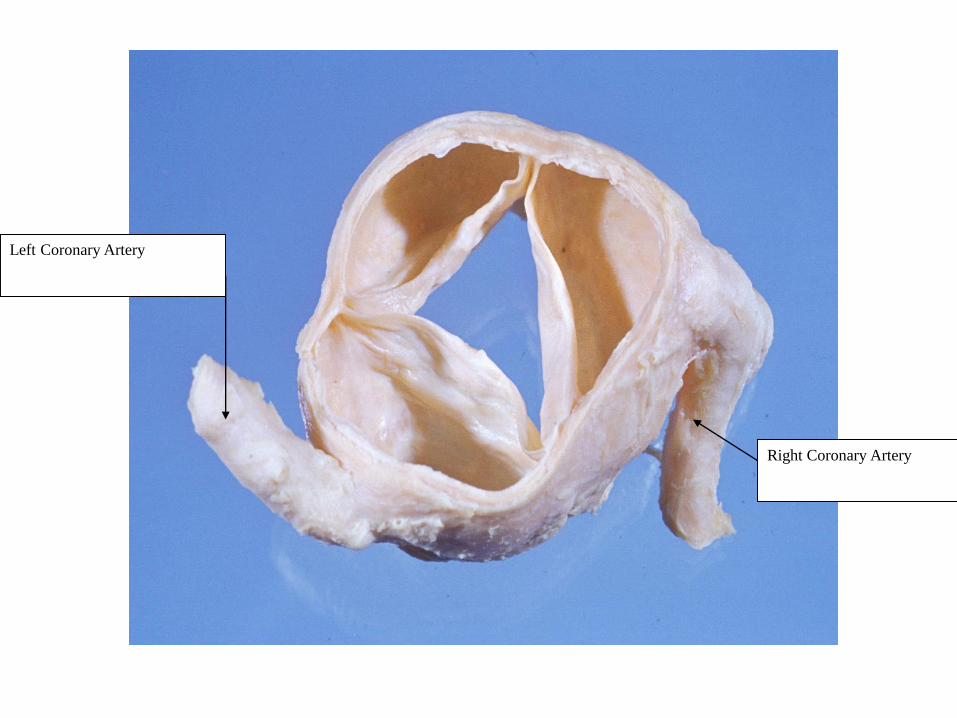
Left Coronary Artery
Right Coronary Artery
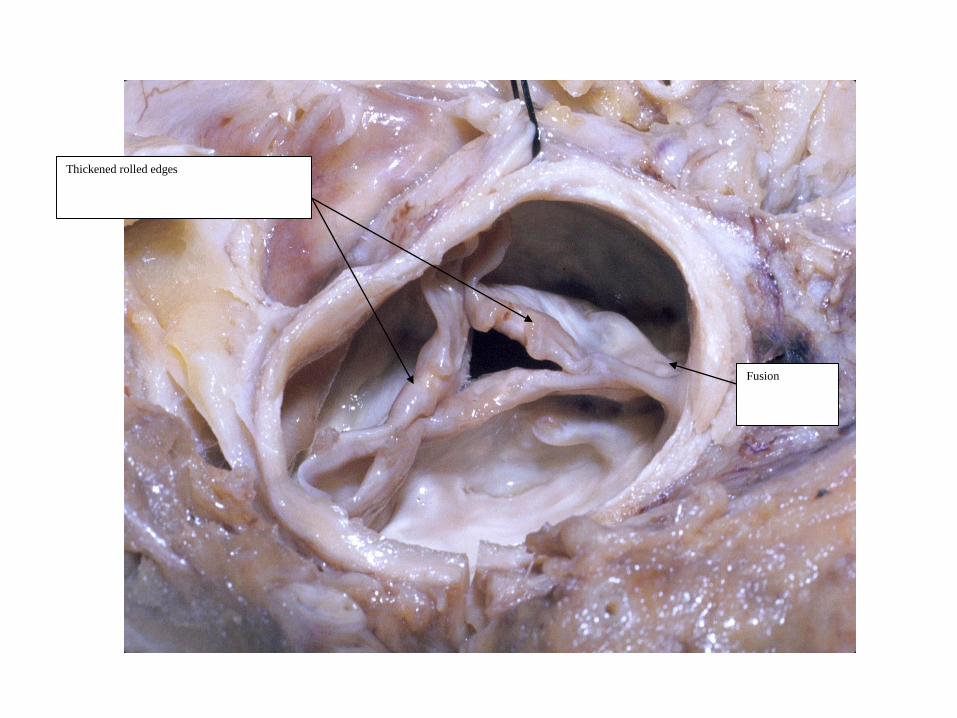
Fusion
Thickened rolled edges
S & S: Sydenham's choreaMAJOR manifestation
• Jerky , twitchy uncoordinated, involuntary and random movements, muscle weakness (most obvious in the face, hands and feet)
• Emotional instability. – irritability & anger, depression & sadness
• Clinical features – May begin 3-4 months after strep throat infection
and often without other symptoms– Usually resolves in 6 months – More common in teenagers ( rare after 20 years)– Affects females more than males– May recur during pregnancy
• Chorea has a strong association with carditis
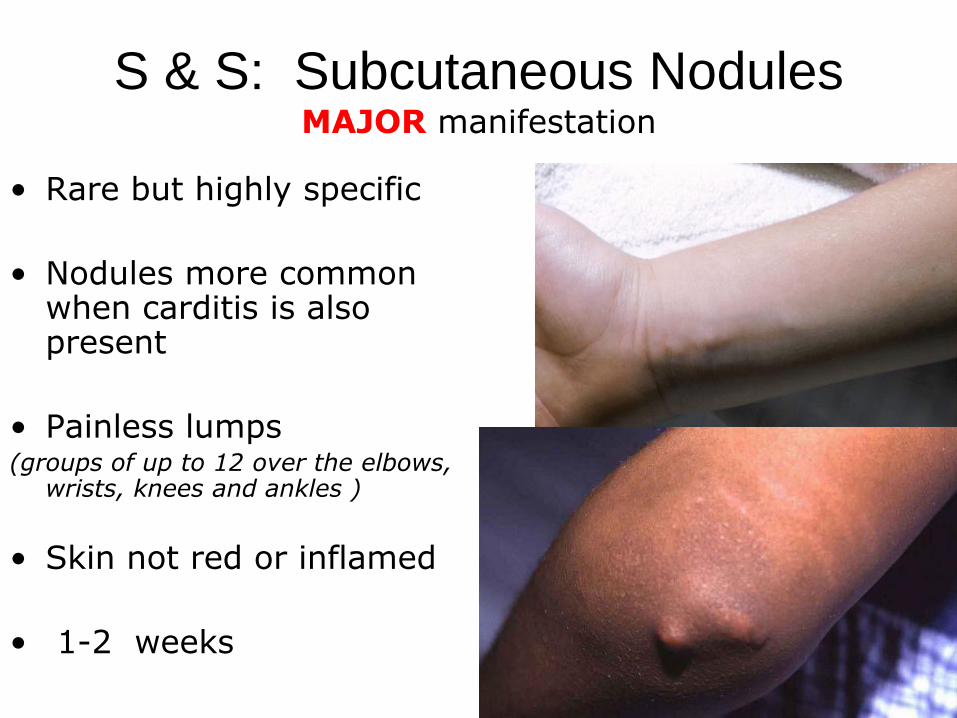
S & S: Subcutaneous Nodules MAJOR manifestation
• Rare but highly specific
• Nodules more common when carditis is also present
• Painless lumps (groups of up to 12 over the elbows,
wrists, knees and ankles )
• Skin not red or inflamed
• 1-2 weeks
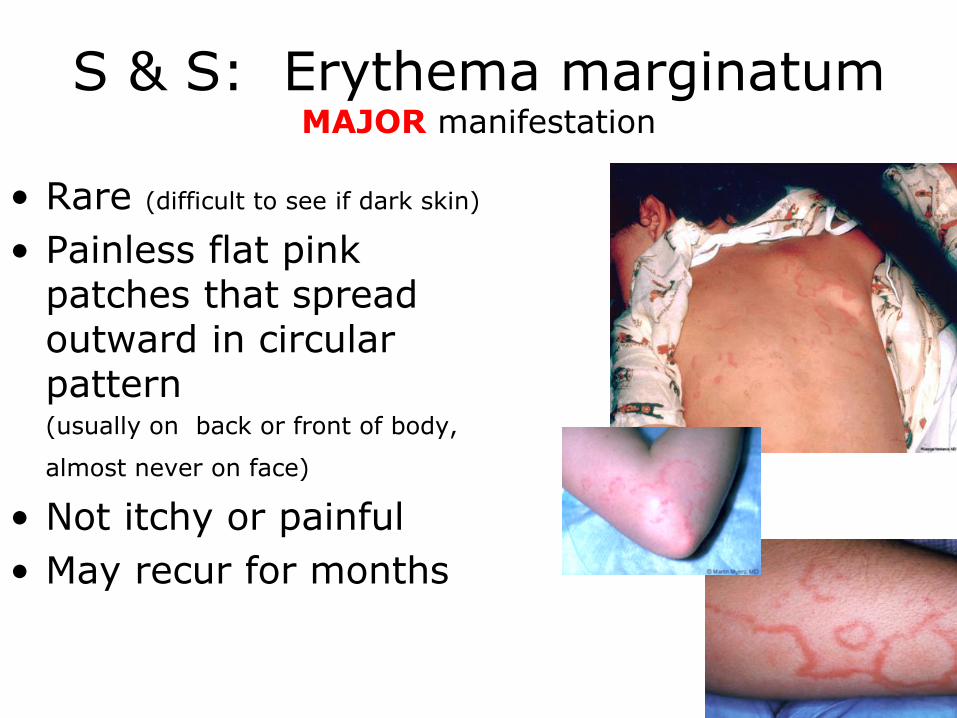
S & S: Erythema marginatum MAJOR manifestation
• Rare (difficult to see if dark skin)
• Painless flat pink patches that spread outward in circular pattern (usually on back or front of body,
almost never on face)
• Not itchy or painful
• May recur for months
Signs and symptoms: MINOR manifestation
• Arthralgia:– Joint pain ( non inflammatory), Usually large joints, mild or severe
• Fever:– Occurs in majority of cases, usually with onset of symptoms– Quick response to NSAID / salicylates
• Prolonged PR Interval:– Extreme 1st degree heart block can sometimes lead to 2nd degree HB
• Elevated acute phase reactants:– CRP ≥ 30 & ESR ≥ 50
• Evidence of Group A streptococcal infection:– Group A betahaemolytic strep might be seen on throat swab since the infection
may have finished by time of onset of the ARF symptoms– ASOT – serum reaches peak at around 3-6 weeks after infection and starts to fall
around 6-8 weeks– Anti BNase B reaches peak level at 6-8 weeks after infection and starts to fall
around 3 months
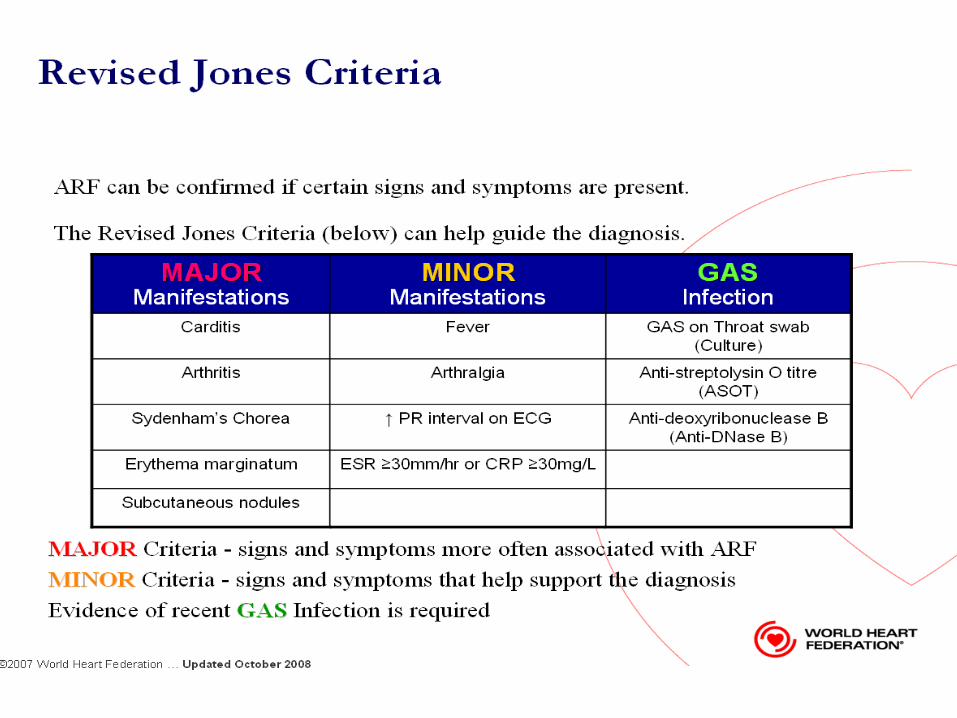
Jones Criteria - summary
Major Criteria
J Joints (polyarthritis)
♥ Carditis (pancarditis and mid diastolic murmur)
N Nodules
E Erythema marginatum
S Sydenham's chorea
Minor criteria Fever, ESR, Arthralgia, Long PR interval
Difficulties with ARF diagnosis
• Child and family don’t always come to hospital or health clinic with their symptoms because;– Symptoms don’t seem serious enough– Access to health clinic is difficult
• Health staff don’t recognise the signs and symptoms of ARF– A sore throat can seem just like any other cold and sore throat– Lots of children get colds and sore throats
• ARF can look like other illnesses– Sore joints may get confused with a sports injury or “growing pains”– Septic arthritis etc
Treatment of Acute RF
Treat the acute illness – All cases of ARF should receive; – A single injection of Benzathine penicillin G, or– Oral Penicillin for 10 days (Erythromycin if penicillin
allergy)
Relieve symptoms– Pain relief for arthritis (paracetamol or aspirin)– Bed rest if cardiac failure– Anti-failure medication (Diuretics, ACEi, +/- Digoxin) – Treat chorea (Carbamazepine or Valporic acid if severe)
Secondary prophylaxis Key element in management of RHD
• Prevents further Group A streptococcal infection (stop
strep throat !!!!)
• Prevent repeated episodes of ARF ( where heart,
joints, brain and skin become inflamed and swollen →
repeated damage to valves in heart )
• Prevent development of RHD
• Reduces the severity of RHD
• Helps to reduce the risk of death form severe RHD
Secondary prophylaxis
The standard dose
• 1,200,000 units of Benzathine Penicillin G IM for ALL people ≥30kg
• 600,000 units IM for children <30kg
• Monthly depot IM BPG (every 28 days)
• 3 weekly (21-days) BPG for those with recurrent ARF despite full adherence to 28-day BPG.
Summary
• Acute rheumatic fever starts after an illness with the Group A streptococcal bacteria (GAS infection)
• Usually from a sore throat - streptococcus pyogenes
• Rheumatic fever is serious it can cause permanent damage to the heart
• Sore throats matter – Primary prevention – education families and health workers to take sore throats seriously – Treat with antibiotics
• Jones Criteria is used to guide diagnosis of ARF and RHD
• Need good long-term secondary prophylaxis to prevent further development of RHD
Education
• Early evaluation and treatment of pharyngitis in children to help prevent RF – Sore throats matter !!!
– Hand hygiene / sneeze into elbow
• Emphasize measures that minimize further damage to the valves of the heart.– Secondary prophylaxis of patients with previous RF and valve
involvement with penicillin injections every 3-4 weeks decrease the recurrence of RHD.
• Additional prophylactic antibiotics prior to dental and surgical procedures decrease the likelihood of bacterial endocarditis.
Rheumatic fever resources
• New Zealand www.heartfoundation.org.nz
• For NZ Guidelines for Rheumatic fever http://www.heartfoundation.org.nz/uploads/Rheumatic%20fever%20guideline%201(5).pdf
• World Heart federation – Resources for Health Professionals www.worldheart.org/rhd
• For training resources and data base development resources http://www.world-heart-federation.org/what-we-do/rheumatic-heart-disease-network/for-health-professionals/world-heart-federation-rheumatic-heart-disease-resources/
• RHD Australiawww.rhdaustralia.org.au
• http://www.youtube.com/watch?v=tWMGNG61SRA
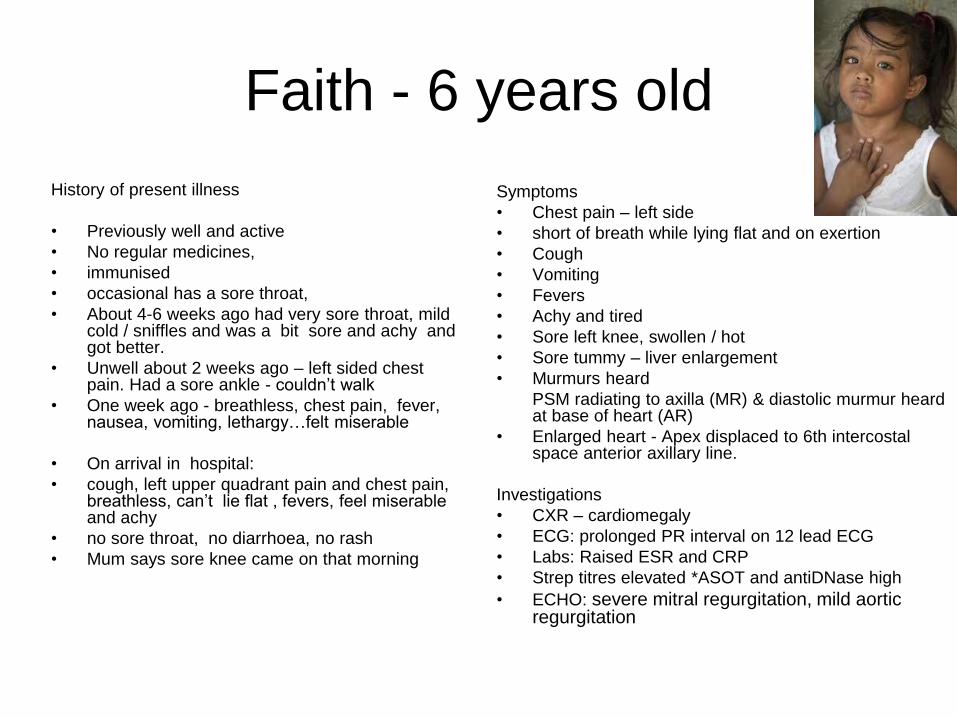
Faith - 6 years old
History of present illness
• Previously well and active
• No regular medicines,
• immunised
• occasional has a sore throat,
• About 4-6 weeks ago had very sore throat, mild cold / sniffles and was a bit sore and achy and got better.
• Unwell about 2 weeks ago – left sided chest pain. Had a sore ankle - couldn’t walk
• One week ago - breathless, chest pain, fever, nausea, vomiting, lethargy…felt miserable
• On arrival in hospital:
• cough, left upper quadrant pain and chest pain, breathless, can’t lie flat , fevers, feel miserable and achy
• no sore throat, no diarrhoea, no rash
• Mum says sore knee came on that morning
Symptoms
• Chest pain – left side
• short of breath while lying flat and on exertion
• Cough
• Vomiting
• Fevers
• Achy and tired
• Sore left knee, swollen / hot
• Sore tummy – liver enlargement
• Murmurs heard
PSM radiating to axilla (MR) & diastolic murmur heard at base of heart (AR)
• Enlarged heart - Apex displaced to 6th intercostal space anterior axillary line.
Investigations
• CXR – cardiomegaly
• ECG: prolonged PR interval on 12 lead ECG
• Labs: Raised ESR and CRP
• Strep titres elevated *ASOT and antiDNase high
• ECHO: severe mitral regurgitation, mild aortic regurgitation





























