Embed Size (px)
Citation preview
6/14/2013
1
Rheumatoid ArthritisRheumatoid ArthritisTreatment Past, Present and Treatment Past, Present and
FutureFuture
Jonathan S. Coblyn, M.D.Jonathan S. Coblyn, M.D.Brigham and Women’s HospitalBrigham and Women’s Hospital
DisclosuresDisclosures
CVSCVS
ConclusionConclusionA new era in the treatment of rheumatoid arthritisA new era in the treatment of rheumatoid arthritis
•• Proof of principle has been established that Proof of principle has been established that selective targeting of pathogenic elements is selective targeting of pathogenic elements is therapeutically effective. therapeutically effective.
•• Early therapyEarly therapy--especially combination therapy tied especially combination therapy tied to improved outcomes.to improved outcomes.
•• The future is now! Less joint replacements and The future is now! Less joint replacements and improved morbidity and mortality now evident.improved morbidity and mortality now evident.
•• Biologics decrease joint replacements and Biologics decrease joint replacements and hospitalizationshospitalizations
•• A plea. Refer to confirm diagnosis and initiate A plea. Refer to confirm diagnosis and initiate treatmenttreatment
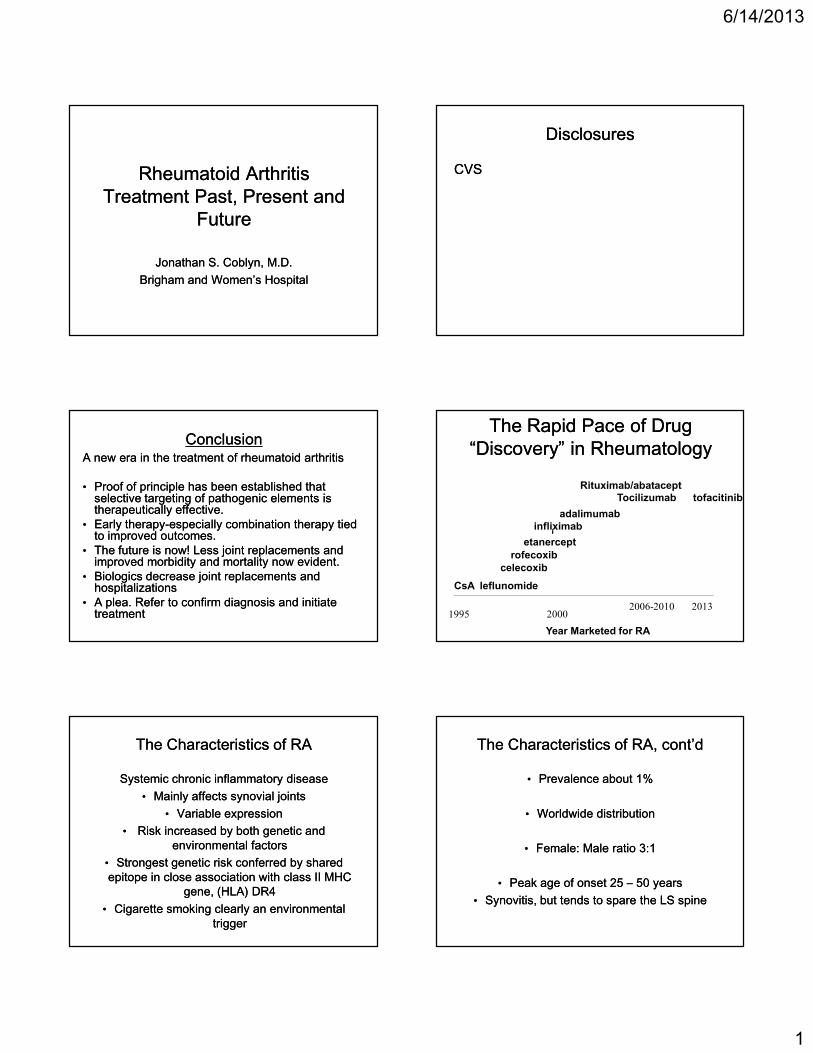
The Rapid Pace of Drug The Rapid Pace of Drug “Discovery” in Rheumatology“Discovery” in Rheumatology
1995 20002006-2010 2013
CsA leflunomide
celecoxib
rofecoxib
etanercept
infliximabadalimumab
Rituximab/abatacept Tocilizumab tofacitinib
Year Marketed for RA
iiii
The Characteristics of RAThe Characteristics of RA
Systemic chronic inflammatory diseaseSystemic chronic inflammatory disease•• Mainly affects synovial jointsMainly affects synovial joints
•• Variable expressionVariable expression•• Risk increased by both genetic and Risk increased by both genetic and
environmental factorsenvironmental factors•• Strongest genetic risk conferred by shared Strongest genetic risk conferred by shared epitope in close association with class II MHC epitope in close association with class II MHC
gene, (HLA) DR4gene, (HLA) DR4•• Cigarette smoking clearly an environmental Cigarette smoking clearly an environmental
triggertrigger
The Characteristics of RA, cont’dThe Characteristics of RA, cont’d
•• Prevalence about 1%Prevalence about 1%
•• Worldwide distributionWorldwide distribution
•• Female: Male ratio 3:1Female: Male ratio 3:1
•• Peak age of onset 25 Peak age of onset 25 –– 50 years50 years•• Synovitis, but tends to spare the LS spineSynovitis, but tends to spare the LS spine
6/14/2013
2
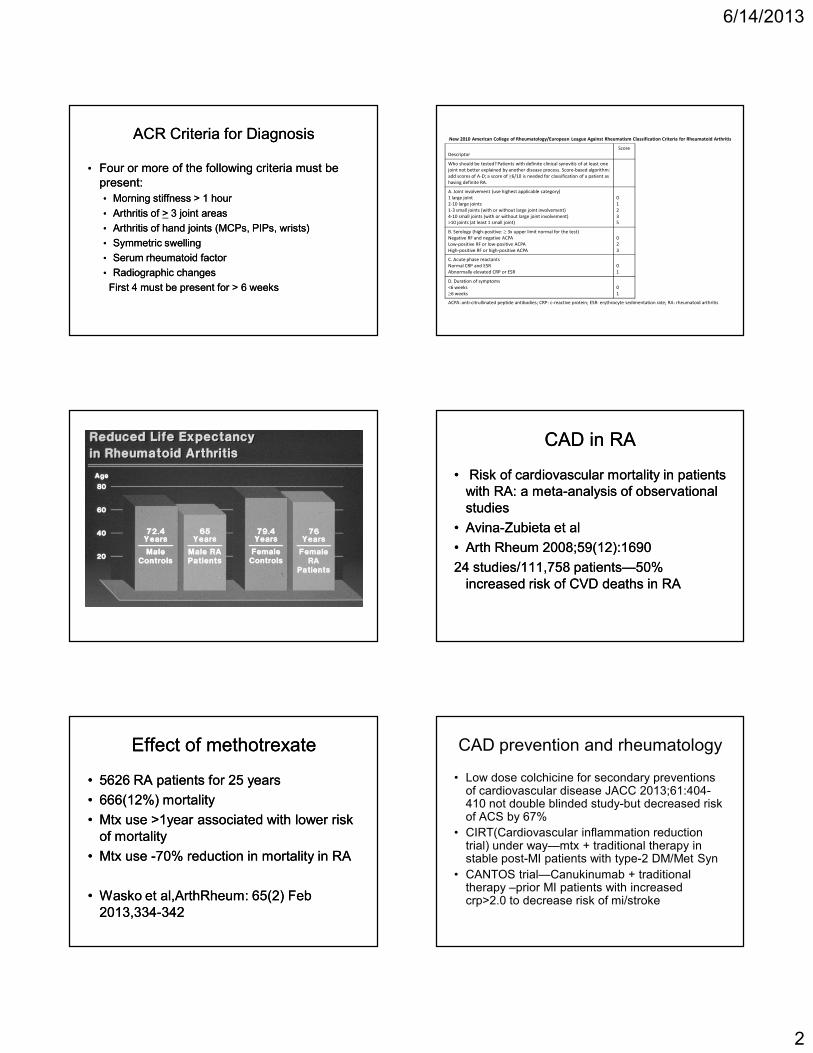
ACR Criteria for DiagnosisACR Criteria for Diagnosis
•• Four or more of the following criteria must be Four or more of the following criteria must be present:present:•• Morning stiffness > 1 hourMorning stiffness > 1 hour•• Arthritis of Arthritis of >> 3 joint areas3 joint areas•• Arthritis of hand joints (MCPs, PIPs, wrists)Arthritis of hand joints (MCPs, PIPs, wrists)•• Symmetric swellingSymmetric swelling•• Serum rheumatoid factorSerum rheumatoid factor•• Radiographic changesRadiographic changesFirst 4 must be present for > 6 weeksFirst 4 must be present for > 6 weeks
New 2010 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Rheumatoid Arthritis
Descriptor
Score
Who should be tested? Patients with definite clinical synovitis of at least one
joint not better explained by another disease process. Score-based algorithm:
add scores of A-D; a score of ≥6/10 is needed for classification of a patient as
having definite RA.
A. Joint involvement (use highest applicable category)
1 large joint
2-10 large joints
1-3 small joints (with or without large joint involvement)
4-10 small joints (with or without large joint involvement)
>10 joints (at least 1 small joint)
0
1
2
3
5
B. Serology (high-positive: ≥ 3x upper limit normal for the test)
Negative RF and negative ACPA
Low-positive RF or low-positive ACPA
High-positive RF or high-positive ACPA
0
2
3
C. Acute phase reactants
Normal CRP and ESR
Abnormally elevated CRP or ESR
0
1
D. Duration of symptoms
<6 weeks
≥6 weeks
0
1
ACPA: anti-citrullinated peptide antibodies; CRP: c-reactive protein; ESR: erythrocyte sedimentation rate; RA: rheumatoid arthritis
CAD in RACAD in RA
•• Risk of cardiovascular mortality in patients Risk of cardiovascular mortality in patients with RA: a metawith RA: a meta--analysis of observational analysis of observational studiesstudies
•• AvinaAvina--Zubieta et alZubieta et al
•• Arth Rheum 2008;59(12):1690Arth Rheum 2008;59(12):1690
24 studies/111,758 patients24 studies/111,758 patients——50% 50% increased risk of CVD deaths in RAincreased risk of CVD deaths in RA
Effect of methotrexateEffect of methotrexate
•• 5626 RA patients for 25 years5626 RA patients for 25 years
•• 666(12%) mortality666(12%) mortality
•• Mtx use >1year associated with lower risk Mtx use >1year associated with lower risk of mortalityof mortality
•• Mtx use Mtx use --70% reduction in mortality in RA70% reduction in mortality in RA
•• Wasko et al,ArthRheum: 65(2) Feb Wasko et al,ArthRheum: 65(2) Feb 2013,3342013,334--342 342
CAD prevention and rheumatology
• Low dose colchicine for secondary preventions of cardiovascular disease JACC 2013;61:404-410 not double blinded study-but decreased risk of ACS by 67%
• CIRT(Cardiovascular inflammation reduction trial) under way—mtx + traditional therapy in stable post-MI patients with type-2 DM/Met Syn
• CANTOS trial—Canukinumab + traditional therapy –prior MI patients with increased crp>2.0 to decrease risk of mi/stroke
6/14/2013
3
The Importance of Early Diagnosis and The Importance of Early Diagnosis and TreatmentTreatment
•• RA is progressive, not benignRA is progressive, not benign•• Structural damage/disability occurs within first 2 Structural damage/disability occurs within first 2
to 3 years of diseaseto 3 years of disease•• Slower progression of disease linked to early Slower progression of disease linked to early
and aggressive treatmentand aggressive treatment•• Less NSAIDS and steroidsLess NSAIDS and steroids•• Less Orthopedic surgery and hospitalizationsLess Orthopedic surgery and hospitalizations
Advantages of DMARDsAdvantages of DMARDs
•• Slow disease progressionSlow disease progression•• Improve functional disabilityImprove functional disability•• Decrease painDecrease pain•• Interfere with inflammatory processInterfere with inflammatory process•• Retard development of joint erosionsRetard development of joint erosions•• Remissions are now achievedRemissions are now achieved•• Most studies correlate favorable Most studies correlate favorable
outcomes with combination Rx or early outcomes with combination Rx or early and aggressive therapyand aggressive therapy
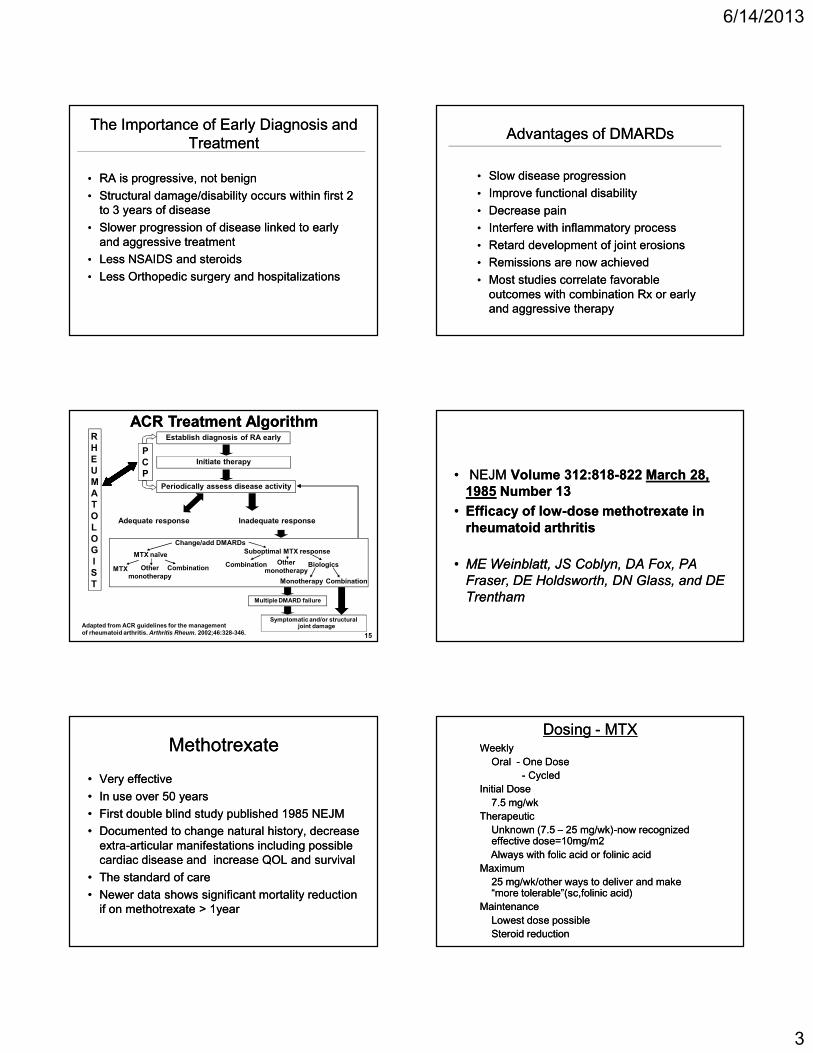
Establish diagnosis of RA early
Initiate therapy
PCP
Periodically assess disease activity
RHEUMATOLOGIST
Adequate response Inadequate response
Change/add DMARDs
MTX naïve Suboptimal MTX response
MTX Othermonotherapy
Combination Combination Othermonotherapy
Biologics
Monotherapy Combination
Multiple DMARD failure
Symptomatic and/or structural joint damage
ACR Treatment AlgorithmACR Treatment Algorithm
Adapted from ACR guidelines for the management of rheumatoid arthritis. Arthritis Rheum. 2002;46:328-346. 15
•• NEJM NEJM Volume 312:818Volume 312:818--822822 March 28, March 28, 19851985 Number 13Number 13
•• Efficacy of lowEfficacy of low--dose methotrexate in dose methotrexate in rheumatoid arthritisrheumatoid arthritis
•• ME Weinblatt, JS Coblyn, DA Fox, PA ME Weinblatt, JS Coblyn, DA Fox, PA
Fraser, DE Holdsworth, DN Glass, and DE Fraser, DE Holdsworth, DN Glass, and DE
TrenthamTrentham
Methotrexate Methotrexate
•• Very effectiveVery effective
•• In use over 50 yearsIn use over 50 years
•• First double blind study published 1985 NEJMFirst double blind study published 1985 NEJM
•• Documented to change natural history, decrease Documented to change natural history, decrease extraextra--articular manifestations including possible articular manifestations including possible cardiac disease and increase QOL and survivalcardiac disease and increase QOL and survival
•• The standard of careThe standard of care
•• Newer data shows significant mortality reduction Newer data shows significant mortality reduction if on methotrexate > 1yearif on methotrexate > 1year
Dosing Dosing -- MTXMTXWeeklyWeekly
Oral Oral -- One DoseOne Dose-- Cycled Cycled
Initial DoseInitial Dose7.5 mg/wk 7.5 mg/wk
TherapeuticTherapeuticUnknown (7.5 Unknown (7.5 –– 25 mg/wk)25 mg/wk)--now recognized now recognized effective dose=10mg/m2effective dose=10mg/m2Always with folic acid or folinic acidAlways with folic acid or folinic acid
MaximumMaximum25 mg/wk/other ways to deliver and make 25 mg/wk/other ways to deliver and make “more tolerable”(sc,folinic acid)“more tolerable”(sc,folinic acid)
MaintenanceMaintenanceLowest dose possibleLowest dose possibleSteroid reductionSteroid reduction
6/14/2013
4
Methotrexate Methotrexate
•• EfficacyEfficacy——Now established DMARDNow established DMARD
•• patients with RApatients with RA——treated with mtx treated with mtx decreased mortality and c/v riskdecreased mortality and c/v risk——Other Other studies confirmed these observationsstudies confirmed these observations
•• Established Gold StandardEstablished Gold Standard
Next therapy after Methotrexate:Next therapy after Methotrexate:How to decide when and whatHow to decide when and what
•• Disease activityDisease activity——Use objective Use objective measurementsmeasurements——DAS, CDAIDAS, CDAI
•• Radiographic progressionRadiographic progression
•• Patient’s appetite for riskPatient’s appetite for risk
•• Prior medical issues which may make some Prior medical issues which may make some therapies contraindicatedtherapies contraindicated
•• Economic review of systems!Economic review of systems!
•• Triple small molecule therapy/leflunomide +/Triple small molecule therapy/leflunomide +/--MTXMTX
•• And how to decide next drug?And how to decide next drug?
Biologic TherapiesBiologic Therapies
•• Changed the face of RAChanged the face of RA
•• Induce remissionInduce remission
•• Change the natural history even without a Change the natural history even without a clinical improvement!clinical improvement!
•• Adverse events but no “new signals”Adverse events but no “new signals”
•• Early use in methotrexate “inadequate Early use in methotrexate “inadequate responders”responders”
•• But methotrexate is great in 20But methotrexate is great in 20--30% if 30% if used correctlyused correctly
Biologic Therapies as of 2013Biologic Therapies as of 2013
•• Five antiFive anti--tnf agentstnf agents--etanercept, etanercept, adalimumab, infliximab, golimumab and adalimumab, infliximab, golimumab and certolizumab pegolcertolizumab pegol
•• IL1IL1--receptor antagonistreceptor antagonist——anakinraanakinra
•• CoCo--stimulatory blocker abataceptstimulatory blocker abatacept
•• B cell depletion rituximabB cell depletion rituximab
•• IL6 receptor antagonist tocilizumabIL6 receptor antagonist tocilizumab
AntiAnti--Tnf TherapyTnf Therapy
•• All have similar effectsAll have similar effects——with roughly a with roughly a response rate of 60response rate of 60--70%70%
•• Work in early disease and late diseaseWork in early disease and late disease——clinical outcomes better in early diseaseclinical outcomes better in early disease
•• Stabilize radiographic progressionStabilize radiographic progression
•• Decreased NSAIDS, steroids and mtx Decreased NSAIDS, steroids and mtx dosesdoses
•• Remission in some studies upon Remission in some studies upon withdrawalwithdrawal
6/14/2013
5
Absolute contraindications to Absolute contraindications to TNFTNF--BlockersBlockers
•• CHF III/IVCHF III/IV•• Active/latent TbActive/latent Tb•• Active infectionActive infection•• Active or recent h/o malignancy (solid tumors)Active or recent h/o malignancy (solid tumors)•• MS/optic neuritisMS/optic neuritis•• h/o lymphomah/o lymphoma•• Live vaccinesLive vaccines•• AnaphylaxisAnaphylaxis
Adapted Semin A&R 2005;34Adapted Semin A&R 2005;34
Newer Biologics in RANewer Biologics in RA
•• AbataceptAbatacept
•• RituximabRituximab
•• TocilizumabTocilizumab
How many antiHow many anti--TNFs should we try?TNFs should we try?
Which one to select??? Use these first?Which one to select??? Use these first?
?Difference in side effects?Difference in side effects
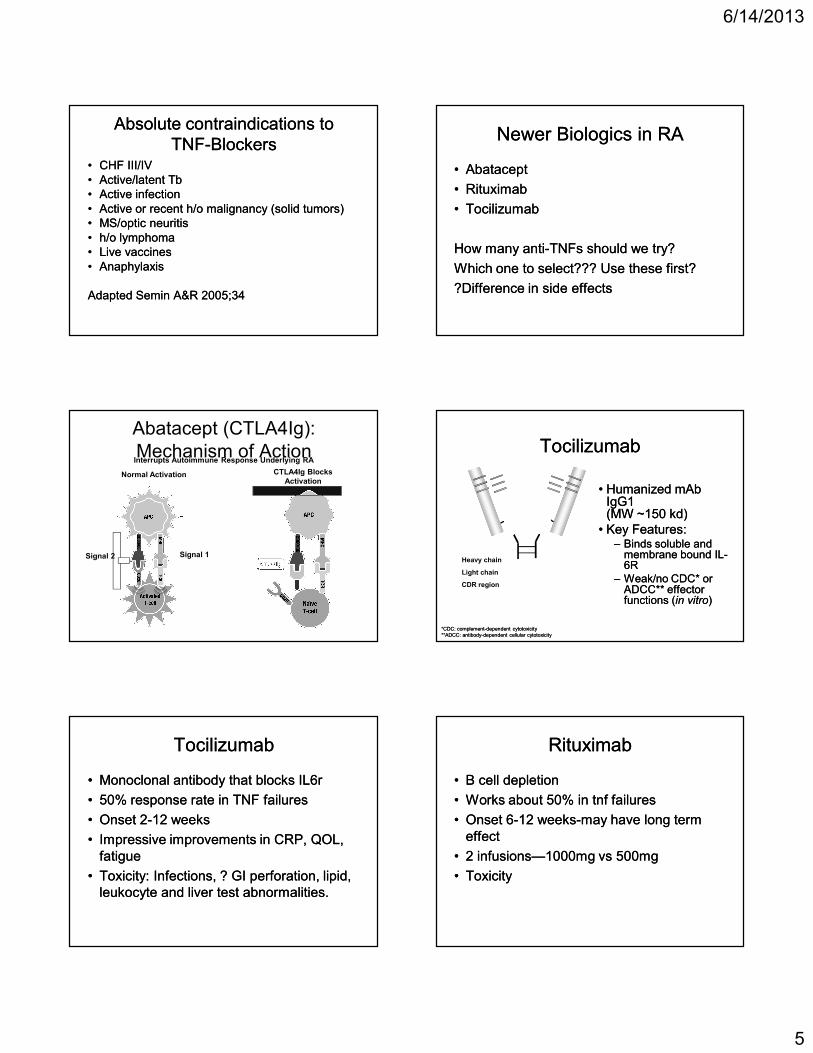
Interrupts Autoimmune Response Underlying RA
Abatacept (CTLA4Ig): Mechanism of Action
CTLA4Ig BlocksActivation
Normal Activation
Signal 1Signal 2
TocilizumabTocilizumab
•• Humanized mAb Humanized mAb IgG1 IgG1 (MW ~150 kd)(MW ~150 kd)
•• Key Features:Key Features:–– Binds soluble and Binds soluble and
membrane bound ILmembrane bound IL--6R 6R
–– Weak/no CDC* or Weak/no CDC* or ADCC** effector ADCC** effector functions (functions (in vitroin vitro))
Heavy chain
Light chain
CDR region
*CDC: complement*CDC: complement--dependent cytotoxicitydependent cytotoxicity**ADCC: antibody**ADCC: antibody--dependent cellular cytotoxicitydependent cellular cytotoxicity
TocilizumabTocilizumab
•• Monoclonal antibody that blocks IL6rMonoclonal antibody that blocks IL6r
•• 50% response rate in TNF failures50% response rate in TNF failures
•• Onset 2Onset 2--12 weeks12 weeks
•• Impressive improvements in CRP, QOL, Impressive improvements in CRP, QOL, fatiguefatigue
•• Toxicity: Infections, ? GI perforation, lipid, Toxicity: Infections, ? GI perforation, lipid, leukocyte and liver test abnormalities.leukocyte and liver test abnormalities.
RituximabRituximab
•• B cell depletionB cell depletion
•• Works about 50% in tnf failuresWorks about 50% in tnf failures
•• Onset 6Onset 6--12 weeks12 weeks--may have long term may have long term effecteffect
•• 2 infusions2 infusions——1000mg vs 500mg1000mg vs 500mg
•• ToxicityToxicity
6/14/2013
6
Concerns regarding rituximabConcerns regarding rituximab
•• What studies should be done before?What studies should be done before?
•• What order should we add these medicines?What order should we add these medicines?
•• Can (should) we treat seronegative patients?Can (should) we treat seronegative patients?
•• What dosing and intervals and how often?What dosing and intervals and how often?
•• How much steroids to use?How much steroids to use?
•• Can we use without methotrexate or with other Can we use without methotrexate or with other small molecules?small molecules?
•• When can we add another therapy?When can we add another therapy?
•• Will there be more surprising side effects? (PML)Will there be more surprising side effects? (PML)
Newer drugs in developmentNewer drugs in development
•• Newer B cell and anti TNF agentsNewer B cell and anti TNF agents
•• p38MAP kinase inhibitorsp38MAP kinase inhibitors
•• Janus Kinase 3 inhibitorsJanus Kinase 3 inhibitors--tofacitinibtofacitinib--FDA advisory board approvalFDA advisory board approval
•• Spleen tyrosine kinase inhibitorsSpleen tyrosine kinase inhibitors
•• CCR1 antagonistsCCR1 antagonists
•• Gene therapyGene therapy
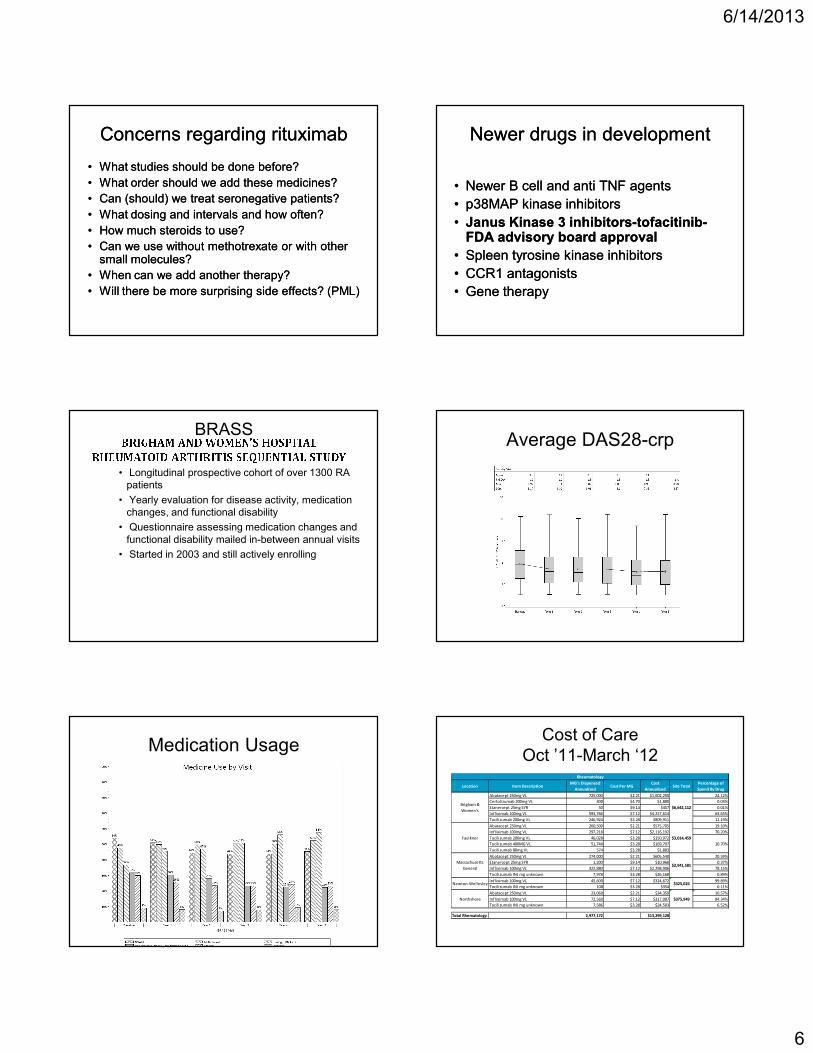
BRASS
• Longitudinal prospective cohort of over 1300 RA patients
• Yearly evaluation for disease activity, medication changes, and functional disability
• Questionnaire assessing medication changes and functional disability mailed in-between annual visits
• Started in 2003 and still actively enrolling
Average DAS28-crp
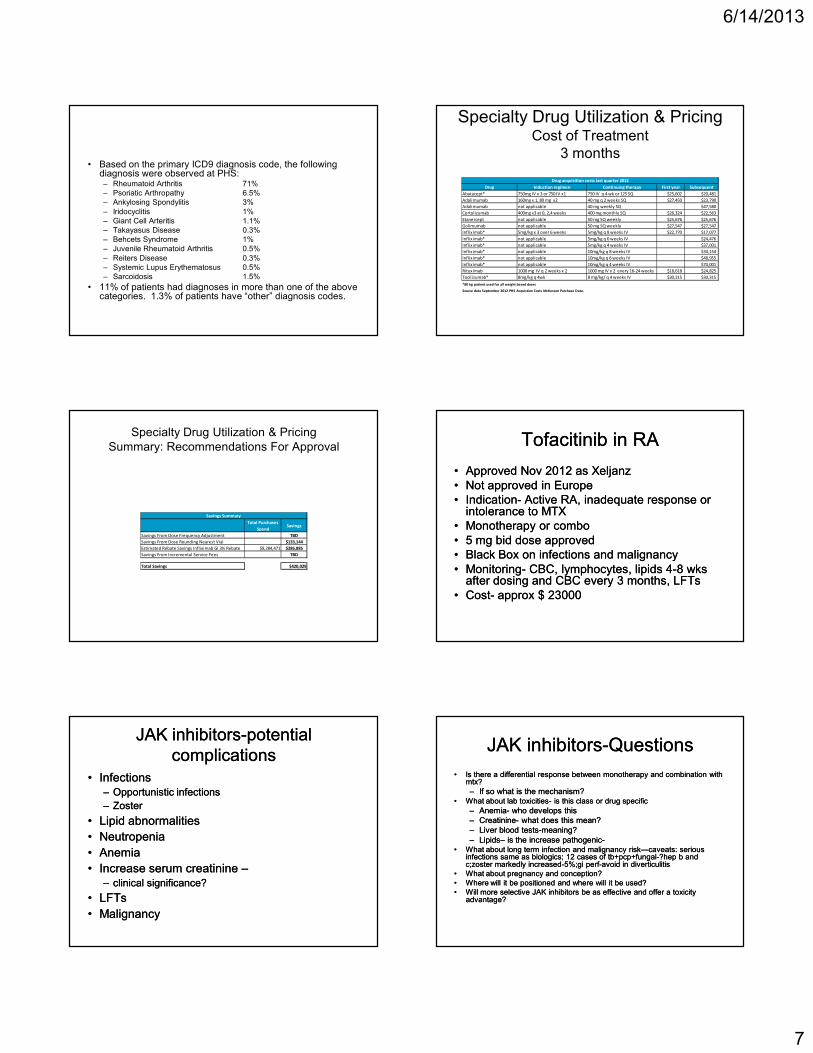
Medication UsageCost of Care
Oct ’11-March ‘12
Location Item Description MG's Dispensed
AnnualizedCost Per MG
Cost
AnnualizedSite Total
Percentage of
Spend By Drug
Abatacept 250mg VL 725,000 $2.21 $1,602,250 24.12%
Certolizumab 200mg VL 400 $4.70 $1,880 0.03%
Etanercept 25mg SYR 50 $9.14 $457 0.01%
Infliximab 100mg VL 593,766 $7.12 $4,227,614 63.65%
Tocilizumab 200mg VL 246,924 $3.28 $809,911 12.19%
Abatacept 250mg VL 260,500 $2.21 $575,705 19.10%
Infliximab 100mg VL 297,218 $7.12 $2,116,192 70.20%
Tocilizumab 200mg VL 46,028 $3.28 $150,972
Tocilizumab 400MG VL 51,740 $3.28 $169,707
Tocilizumab 80mg VL 574 $3.28 $1,883
Abatacept 250mg VL 274,000 $2.21 $605,540 20.59%
Etanercept 25mg SYR 1,200 $9.14 $10,968 0.37%
Infliximab 100mg VL 322,880 $7.12 $2,298,906 78.15%
Tocilizumab INJ mg unknown 7,978 $3.28 $26,168 0.89%
Infliximab 100mg VL 45,600 $7.12 $324,672 99.89%
Tocilizumab INJ mg unknown 108 $3.28 $354 0.11%
Abatacept 250mg VL 23,060 $2.21 $34,359 10.57%
Infliximab 100mg VL 72,560 $7.12 $317,087 84.34%
Tocilizumab INJ mg unknown 7,586 $3.28 $24,503 6.52%
Total Rhematology 2,977,172 $13,299,128
Newton-Wellesley
Northshore
$325,026
$375,949
Rheumatology
$6,642,112
$3,014,459
$2,941,581
10.70%
Brigham &
Women's
Faulkner
Massachusetts
General
6/14/2013
7
• Based on the primary ICD9 diagnosis code, the following diagnosis were observed at PHS: – Rheumatoid Arthritis 71%– Psoriatic Arthropathy 6.5%– Ankylosing Spondylitis 3%– Iridocyclitis 1%– Giant Cell Arteritis 1.1%– Takayasus Disease 0.3%– Behcets Syndrome 1%– Juvenile Rheumatoid Arthritis 0.5%– Reiters Disease 0.3%– Systemic Lupus Erythematosus 0.5%– Sarcoidosis 1.5%
• 11% of patients had diagnoses in more than one of the above categories. 1.3% of patients have “other” diagnosis codes.
Specialty Drug Utilization & PricingCost of Treatment
3 months
Drug Induction regimen Continuing therapy First year Subsequent
Abatacept* 750mg IV x 3 or 750 IV x1 750 IV q 4 wk or 125 SQ $25,602 $20,481
Adalimumab 160mg x 1, 80 mg x2 40 mg q 2 weeks SQ $27,450 $23,790
Adalimumab not applicable 40 mg weekly SQ $47,580
Certolizumab 400mg x3 at 0, 2,4 weeks 400 mg monthly SQ $26,324 $22,563
Etanercept not applicable 50 mg SQ weekly $25,676 $25,676
Golimumab not applicable 50 mg SQ weekly $27,547 $27,547
Infliximab* 5mg/kg x 3 over 6 weeks 5mg/kg q 8 weeks IV $22,770 $17,077
Infliximab* not applicable 5mg/kg q 6 weeks IV $24,476
Infliximab* not applicable 5mg/kg q 4 weeks IV $37,001
Infliximab* not applicable 10mg/kg q 8 weeks IV $34,154
Infliximab* not applicable 10mg/kg q 6 weeks IV $48,955
Infliximab* not applicable 10mg/kg q 4 weeks IV $74,001
Rituximab 1000 mg IV q 2 weeks x 2 1000 mg IV x 2 every 16-24 weeks $18,618 $24,825
Tocilizumab* 8mg/kg q 4wk 8 mg/kg/ q 4 weeks IV $30,315 $30,315
*80 kg patient used for all weight based doses
Source data September 2012 PHS Acquistion Costs McKesson Purchase Data.
Drug acquisition costs last quarter 2012
Specialty Drug Utilization & PricingSummary: Recommendations For Approval
Total Purchases
SpendSavings
Savings From Dose Frequency Adjustment TBD
Savings From Dose Rounding Nearest Vial $133,144
Estimated Rebate Savings Infliximab GI 3% Rebate $9,284,471 $286,885
Savings From Incremental Service Fees TBD
Total Savings $420,029
Savings Summary
Tofacitinib in RATofacitinib in RA
•• Approved Nov 2012 as XeljanzApproved Nov 2012 as Xeljanz•• Not approved in EuropeNot approved in Europe•• IndicationIndication-- Active RA, inadequate response or Active RA, inadequate response or
intolerance to MTXintolerance to MTX•• Monotherapy or comboMonotherapy or combo•• 5 mg bid dose approved5 mg bid dose approved•• Black Box on infections and malignancyBlack Box on infections and malignancy•• MonitoringMonitoring-- CBC, lymphocytes, lipids 4CBC, lymphocytes, lipids 4--8 wks 8 wks
after dosing and CBC every 3 months, LFTsafter dosing and CBC every 3 months, LFTs•• CostCost-- approx $ 23000approx $ 23000
JAK inhibitorsJAK inhibitors--potential potential complicationscomplications
•• InfectionsInfections–– Opportunistic infectionsOpportunistic infections
–– ZosterZoster
•• Lipid abnormalities Lipid abnormalities
•• Neutropenia Neutropenia
•• Anemia Anemia
•• Increase serum creatinine Increase serum creatinine –––– clinical significance?clinical significance?
•• LFTs LFTs
•• MalignancyMalignancy
JAK inhibitorsJAK inhibitors--QuestionsQuestions
•• Is there a differential response between monotherapy and combination with Is there a differential response between monotherapy and combination with mtx?mtx?
–– If so what is the mechanism?If so what is the mechanism?•• What about lab toxicitiesWhat about lab toxicities-- is this class or drug specificis this class or drug specific
–– AnemiaAnemia-- who develops thiswho develops this–– CreatinineCreatinine-- what does this mean? what does this mean? –– Liver blood testsLiver blood tests--meaning?meaning?–– LipidsLipids–– is the increase pathogenicis the increase pathogenic--
•• What about long term infection and malignancy riskWhat about long term infection and malignancy risk——caveats: serious caveats: serious infections same as biologics; 12 cases of tb+pcp+fungalinfections same as biologics; 12 cases of tb+pcp+fungal--?hep b and ?hep b and c;zoster markedly increasedc;zoster markedly increased--5%;gi perf5%;gi perf--avoid in diverticulitisavoid in diverticulitis
•• What about pregnancy and conception?What about pregnancy and conception?•• Where will it be positioned and where will it be used?Where will it be positioned and where will it be used?•• Will more selective JAK inhibitors be as effective and offer a toxicity Will more selective JAK inhibitors be as effective and offer a toxicity
advantage?advantage?
6/14/2013
8
Syk inhibitorsSyk inhibitors
An inhibitor of the spleen tyrosine kinase pathway An inhibitor of the spleen tyrosine kinase pathway has demonstrated efficacy in Phase 2 studieshas demonstrated efficacy in Phase 2 studies
The drug worked quickly achieving response as The drug worked quickly achieving response as early as one week in combination with MTXearly as one week in combination with MTX
One phase 2 study in pts who failed prior biologics One phase 2 study in pts who failed prior biologics was not positivewas not positive-- this may have been due to this may have been due to study design and patient selectionstudy design and patient selection
Toxicity included diarrhea and hypertension these Toxicity included diarrhea and hypertension these AEs were responsive to dose reduction and/or AEs were responsive to dose reduction and/or antianti--BP medsBP meds
Phase 3 studies are in progressPhase 3 studies are in progress
Questions re Syk inhibitorsQuestions re Syk inhibitors
••Does Does Fostamatinib work as Fostamatinib work as monotherapy?monotherapy?
••Does Fostamatinib work in TNF failures?Does Fostamatinib work in TNF failures?
••Can you lower dose and maintain responseCan you lower dose and maintain response
••What about toxicities?What about toxicities?What about long term infection, HBP and malignancy risk?What about long term infection, HBP and malignancy risk?
––What is the etiology of the HBPWhat is the etiology of the HBP——VEGF VEGF inhibition?inhibition?
–– Is the mechanism of action due to Syk inhibition Is the mechanism of action due to Syk inhibition or other kinase inhibitionor other kinase inhibition
••Where will it be positioned and where will it be used?Where will it be positioned and where will it be used?
••Will more selective Syk inhibitors be as effective and offer Will more selective Syk inhibitors be as effective and offer a toxicity advantagea toxicity advantage
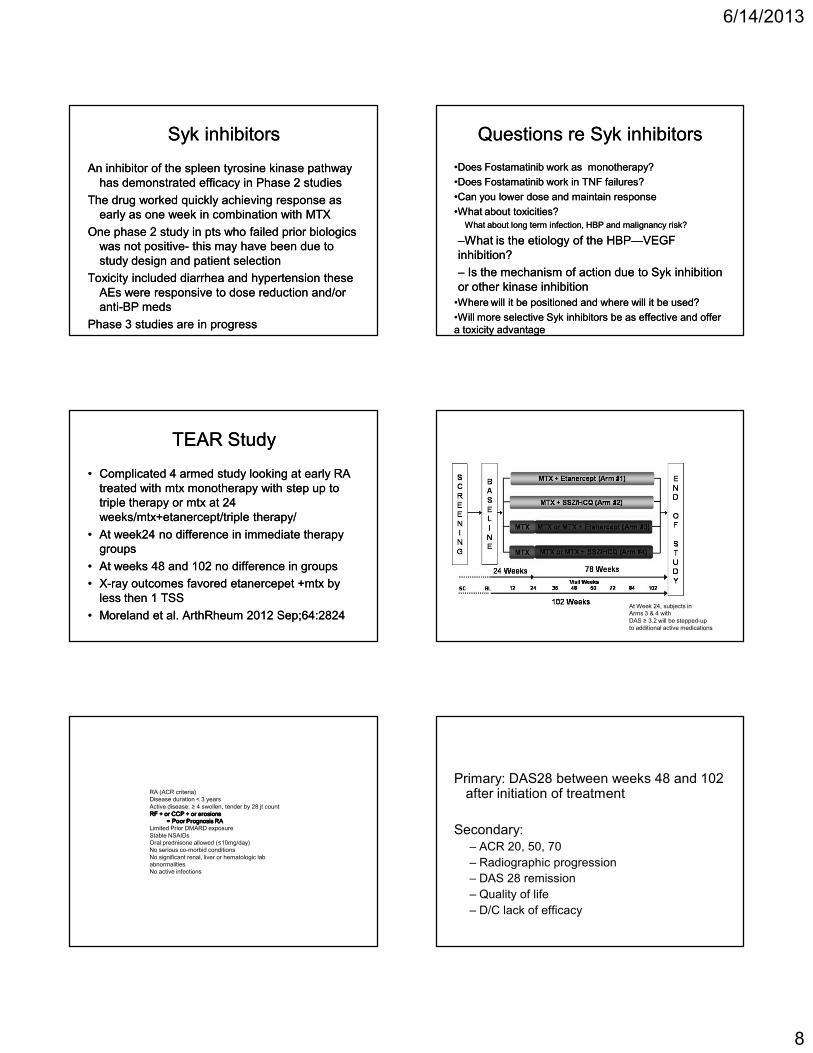
TEAR StudyTEAR Study
•• Complicated 4 armed study looking at early RA Complicated 4 armed study looking at early RA treated with mtx monotherapy with step up to treated with mtx monotherapy with step up to triple therapy or mtx at 24 triple therapy or mtx at 24 weeks/mtx+etanercept/triple therapy/weeks/mtx+etanercept/triple therapy/
•• At week24 no difference in immediate therapy At week24 no difference in immediate therapy groupsgroups
•• At weeks 48 and 102 no difference in groupsAt weeks 48 and 102 no difference in groups
•• XX--ray outcomes favored etanercepet +mtx by ray outcomes favored etanercepet +mtx by less then 1 TSSless then 1 TSS
•• Moreland et al. ArthRheum 2012 Sep;64:2824Moreland et al. ArthRheum 2012 Sep;64:2824At Week 24, subjects in Arms 3 & 4 with DAS ≥ 3.2 will be stepped-up to additional active medications
RA (ACR criteria)Disease duration < 3 yearsActive disease: ≥ 4 swollen, tender by 28 jt countRF + or CCP + or erosionsRF + or CCP + or erosionsRF + or CCP + or erosionsRF + or CCP + or erosions
= Poor Prognosis RA= Poor Prognosis RA= Poor Prognosis RA= Poor Prognosis RALimited Prior DMARD exposure Stable NSAIDsOral prednisone allowed (≤10mg/day)No serious co-morbid conditionsNo significant renal, liver or hematologic lab abnormalitiesNo active infections
Primary: DAS28 between weeks 48 and 102 after initiation of treatment
Secondary:– ACR 20, 50, 70
– Radiographic progression
– DAS 28 remission
– Quality of life
– D/C lack of efficacy
6/14/2013
9
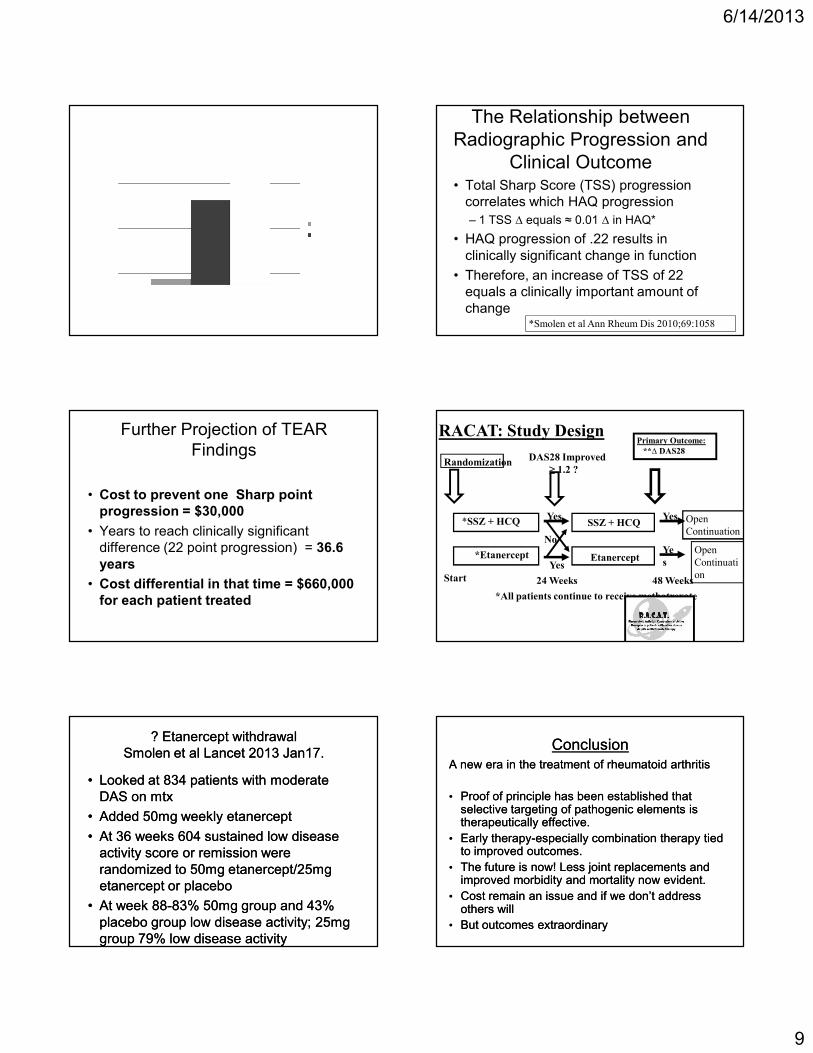
The Relationship between Radiographic Progression and
Clinical Outcome• Total Sharp Score (TSS) progression
correlates which HAQ progression
– 1 TSS ∆ equals ≈ 0.01 ∆ in HAQ*
• HAQ progression of .22 results in clinically significant change in function
• Therefore, an increase of TSS of 22 equals a clinically important amount of change
*Smolen et al Ann Rheum Dis 2010;69:1058
Further Projection of TEAR Findings
• Cost to prevent one Sharp point progression = $30,000
• Years to reach clinically significant difference (22 point progression) = 36.6 years
• Cost differential in that time = $660,000 for each patient treated
Randomization
Start 24 Weeks 48 Weeks
DAS28 Improved
≥ 1.2 ?
Yes
�o
Yes
Primary Outcome:
**& DAS28
Ye
s
*SSZ + HCQ SSZ + HCQ
*Etanercept Etanercept
Yes Open
Continuation
Open
Continuati
on
*All patients continue to receive methotrexate
RACAT: Study Design
? Etanercept withdrawal? Etanercept withdrawalSmolen et al Lancet 2013 Jan17.Smolen et al Lancet 2013 Jan17.
•• Looked at 834 patients with moderate Looked at 834 patients with moderate DAS on mtxDAS on mtx
•• Added 50mg weekly etanerceptAdded 50mg weekly etanercept
•• At 36 weeks 604 sustained low disease At 36 weeks 604 sustained low disease activity score or remission were activity score or remission were randomized to 50mg etanercept/25mg randomized to 50mg etanercept/25mg etanercept or placeboetanercept or placebo
•• At week 88At week 88--83% 50mg group and 43% 83% 50mg group and 43% placebo group low disease activity; 25mg placebo group low disease activity; 25mg group 79% low disease activitygroup 79% low disease activity
ConclusionConclusionA new era in the treatment of rheumatoid arthritisA new era in the treatment of rheumatoid arthritis
•• Proof of principle has been established that Proof of principle has been established that selective targeting of pathogenic elements is selective targeting of pathogenic elements is therapeutically effective. therapeutically effective.
•• Early therapyEarly therapy--especially combination therapy tied especially combination therapy tied to improved outcomes.to improved outcomes.
•• The future is now! Less joint replacements and The future is now! Less joint replacements and improved morbidity and mortality now evident.improved morbidity and mortality now evident.
•• Cost remain an issue and if we don’t address Cost remain an issue and if we don’t address others willothers will
•• But outcomes extraordinaryBut outcomes extraordinary










