Embed Size (px)
Citation preview

MUSCULOSKELETAL CAREMusculoskelet. Care 4(2): 88–100 (2006)Published online in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/msc.81
Main article
Rheumatology nurse practitioners’ perceptions of their roleLeslie Goh MRCP(UK)1, Jo Samanta BA(Hons) RGN2, and Ash Samanta MD FRCP2
1Department of Rheumatology, Royal Cornwall Hospital, Truro, UK; 2Department of Rheumatology, University Hospitals of Leicester NHS Trust, Leicester Royal Infirmary, Leicester, UK
Abstract
Objectives: To identify the current practices of rheumatology nurse practitioners and ascertain their perceptions of how their role could be enhanced.Method: A cross-sectional questionnaire study of currently employed nurse practitioners in rheumatology in the United Kingdom (UK) was undertaken.Results: 200 questionnaires were distributed and 118 nurses responded. Ninety-five respondents met the inclusion criteria for undertaking an advanced nursing role. Typical conditions dealt with included: rheumatoid arthritis (96.8%); psoriatic arthritis (95.8%); osteoarthritis (63.2%); ankylosing spondylitis (62.8%); systemic lupus erythematosus (51.6%); and scleroderma (34.7%). Drug monitoring, education, counselling of patients and arranging basic investigations were routinely performed by more than 80% of respondents. A smaller proportion performed an extended role that included dealing with referrals, research and audit, the administration of intra-articular injections, and admis-sion of patients.
Specific attributes identified as being necessary for competence were: knowledge and understanding of rheumatic diseases (48.4%); drug therapy (33.7%); good commu-nication skills (35.8%); understanding of the roles of the team (27.4%); working effec-tively (23.2%) as part of a multidisciplinary team; assessment of patients by physical examination (28.4%); teaching (26.3%), research (17.9%); organizational skills (14.7%); and the interpretation of investigations (9.5%). Factors that could enhance their role included: attendance at postgraduate courses (30.5%); obtaining further qualifications (13.7%); active participation in the delivery of medical education (41.1%); training in practical procedures (31.6%); protected time and resources for audit and research (11.6%); formal training in counselling (11.6%); and implementation of nurse prescribing (10.5%).
88
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M

Rheumatology nurse practitioners’ role 89
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Conclusion: Nurse practitioners already have a wide remit and play an invaluable part in the delivery of modern rheumatology services. An extended role could improve patient care and enhance nursing career pathways in rheumatology. Copyright © 2006 John Wiley & Sons, Ltd.
Key words: Rheumatology, nurse practitioner, perceptions of role, extended role
Introduction
The role of the rheumatology nurse practitioner (‘nurse practitioner’) first emerged within the National Health Service environment almost 30 years ago. At that time nurse practitioners were employed as trained metrologists who performed clinical assessments of joint swelling, mobility and function and provided assistance with the completion of patient questionnaires (Bird, 1981). Gradually the role evolved, and current evidence suggests that typical aspects of the role include monitoring of side effects for disease-modifying anti-rheumatic drugs and patient education (Bird, 1981; Hill, 1985, 1992). Research by Hill et al. (1994) indicates that within defined areas of practice the quality and safety of care provided by nurse practitio-ners is equivalent to that of physicians, and patient surveys have revealed a high level of satisfaction with the care they provide.
Recent years have seen an increase in the number of nursing posts with a specialist focus in rheumatology (Cohen, 1994). These developments are due to a combination of factors such as patient need, local service requirements (Mounce and Ryan, 2001) and the drive for greater cost-effectiveness (Van den Hout et al., 2003). Changes in the working patterns of junior doctors due to the implementa-tion of the European Working Time Directive (93/104/EC 23 November 1993) and Modernizing Medical Careers (Department of Health, 2004) will further impact upon this trend. Under the Code of Professional Conduct (NMC, 2002) registered nurses are accountable for their conduct, the care they provide and any omissions on their part. The Code also provides the framework for nurse practitioners to develop their practice and take on responsibilities often perceived as beyond the traditional boundaries of nursing care.
There is currently no clear consensus regarding the role or the remit of the nurse practitioner (Newbold, 1996). The term ‘nurse practitioner’ is not indicative of any particular level of professional responsibility, expertise, job description or salary and wide variations exist between individuals and geographical regions (Newbold, 1996). Moreover, other nursing titles such as clinical nurse specialist, advanced nurse practitioner and higher level practitioner are being adopted with no clear consensus to the nature or differences between such roles (Daly and Carnwell, 2003). In addition, there is limited recent data on the role and type of

Goh, Samanta and Samanta90
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
work undertaken by rheumatology nurse practitioners (Carr, 2001). In order to explore this area further we have conducted a questionnaire survey to ascertain current practice, elicit views on the necessary knowledge and skills required to undertake the role, and respondents’ perceptions of how the role might be enhanced.
Aim
The aim of this study was to identify current practice of nurse practitioners employed in NHS rheumatology departments, to elicit their views on the necessary knowl-edge and skills required to undertake the role effectively and to ascertain their perceptions of how the role might be enhanced.
Methods
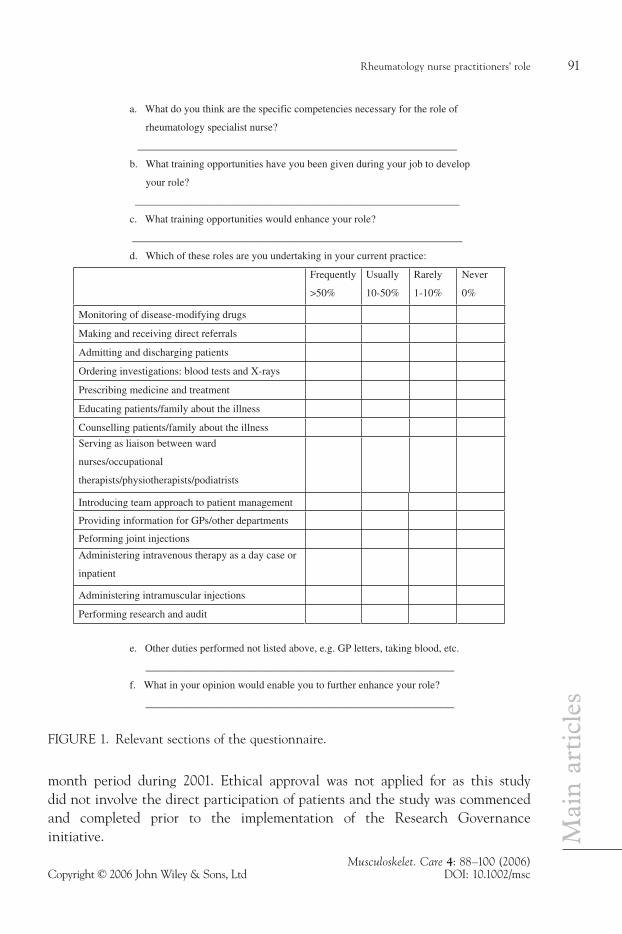
A questionnaire was designed to assess the current role and type of work that nurse practitioners undertake. Its content was based upon the present literature (Phelan et al., 1992, Carr, 2001) and a consensus on proposed questions by a focus group of local nurse practitioners and medical staff with an interest in this area. An introductory letter outlining the aims and objectives of the study was devised and a pilot study was carried out among a small group of nurse practitioners. These steps were undertaken to ensure that the covering letter and questionnaire comple-tion instructions were clear and to ascertain that each of the questions would be interpreted similarly by all participants. The feedback received was used by the researchers (LG and AS) to refine and develop the final version of the question-naire. The sections of the questionnaire that pertain to the current role of the nurse practitioner and respondents’ perceptions of how the role might be enhanced are shown in Figure 1.
Potential participants were identified through the British Health Professionals in Rheumatology (BHPR) handbook (2001). Details were obtained of all nurses currently employed in rheumatology units throughout the UK. Nurses with the title of ‘rheumatology nurse practitioner’, ‘rheumatology specialist nurse’, ‘clinical nurse specialist’ and ‘advanced nurse practitioner’ were included in the study in order to obtain a wide cross-section of participants who might satisfy our selection criteria. Participants’ views were ascertained about their clinical and non-clinical commitments, the knowledge and skills that they considered as essential to their role, and their perception of how their role could be enhanced in terms of patient care and personal professional development. At the end of each section participants were invited to contribute free-text comments to qualify or amplify their responses. Non-responders received a second distribution. This study took place over a six
Rheumatology nurse practitioners’ role 91
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
a. What do you think are the specific competencies necessary for the role of
rheumatology specialist nurse?
____________________________________________________________
b. What training opportunities have you been given during your job to develop
your role?
_____________________________________________________________
c. What training opportunities would enhance your role?
______________________________________________________________
d. Which of these roles are you undertaking in your current practice:
Frequently
>50%
Usually
10-50%
Rarely
1-10%
Never
0%
Monitoring of disease-modifying drugs
Making and receiving direct referrals
Admitting and discharging patients
Ordering investigations: blood tests and X-rays
Prescribing medicine and treatment
Educating patients/family about the illness
Counselling patients/family about the illness
Serving as liaison between ward
nurses/occupational
therapists/physiotherapists/podiatrists
Introducing team approach to patient management
Providing information for GPs/other departments
Peforming joint injections
Administering intravenous therapy as a day case or
inpatient
Administering intramuscular injections
Performing research and audit
e. Other duties performed not listed above, e.g. GP letters, taking blood, etc.
__________________________________________________________
f. What in your opinion would enable you to further enhance your role?
__________________________________________________________
FIGURE 1. Relevant sections of the questionnaire.
month period during 2001. Ethical approval was not applied for as this study did not involve the direct participation of patients and the study was commenced and completed prior to the implementation of the Research Governance initiative.
Goh, Samanta and Samanta92
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Statistical analysis
The complete data set (questionnaire responses) was entered directly onto Microsoft Excel 2000. These data were then transferred to SPSS (version 10). Percentages were calculated for all sets of data. The answers to open-ended questions were grouped into a number of common themes initially by a single researcher (LG) and subsequently corroborated by a second researcher (AS) to maximize validity and reliability.
Results
A target group of 200 nurses was identified using the BHPR handbook as holding a suitable specialist title. A questionnaire, covering letter and pre-paid envelope was sent to each. Specialist titles included those that indicated advanced status such as rheumatology specialist nurse, clinical nurse specialist, rheumatology nurse practitioner and advanced nurse practitioner. A total of 118 members initially responded of which 95 met our inclusion criteria as being nurse practitioners (23 questionnaires were returned from sisters/ward managers and staff and research nurses working within rheumatology units). None of the non-responders replied following the reminder. For the remainder of this paper the term nurse practitioner will include those respondents with the above specialist titles and who met our inclusion criteria.
Of the respondents, 66.3% (n = 63) held full-time positions and 33.7% (n = 32) held part-time posts. All respondents undertook at least two nurse-led clinics per week. About 24.7% (n = 23) and 34.4% (n = 32) did three and four clinics per week, respectively. Conditions commonly managed were: rheumatoid arthritis (96.8 %); psoriatic arthritis (95.8%); osteoarthritis (63.2%); ankylosing spondylitis (62.8%); systemic lupus erythematosus (51.6%) and scleroderma (34.7%).
Current practices
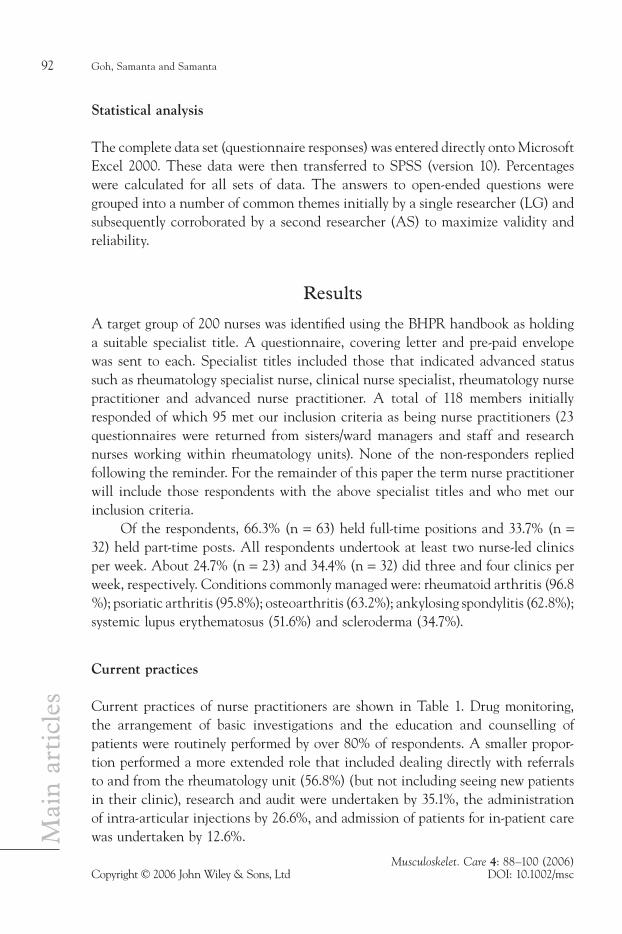
Current practices of nurse practitioners are shown in Table 1. Drug monitoring, the arrangement of basic investigations and the education and counselling of patients were routinely performed by over 80% of respondents. A smaller propor-tion performed a more extended role that included dealing directly with referrals to and from the rheumatology unit (56.8%) (but not including seeing new patients in their clinic), research and audit were undertaken by 35.1%, the administration of intra-articular injections by 26.6%, and admission of patients for in-patient care was undertaken by 12.6%.
Rheumatology nurse practitioners’ role 93
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Knowledge and skills
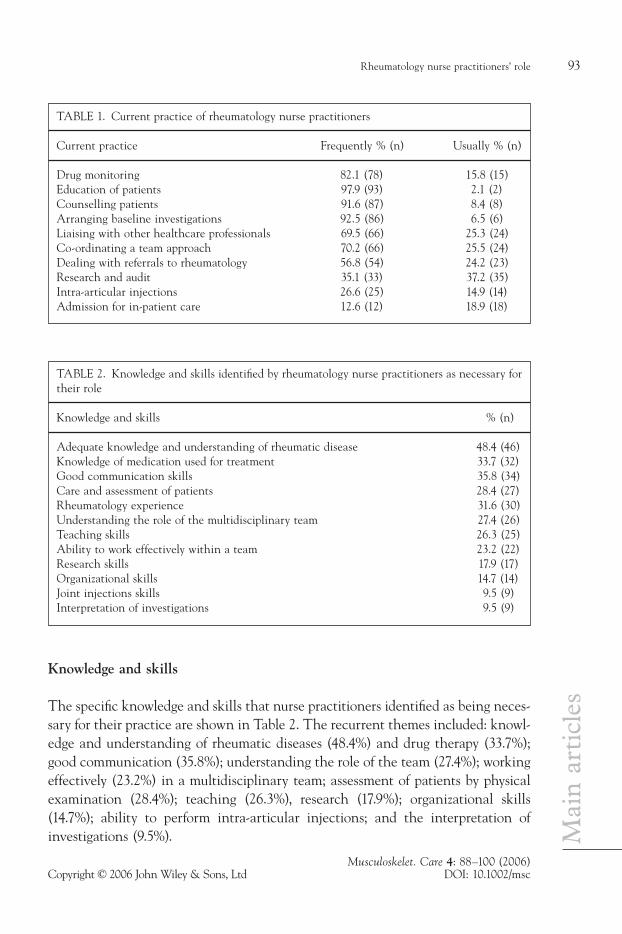
The specific knowledge and skills that nurse practitioners identified as being neces-sary for their practice are shown in Table 2. The recurrent themes included: knowl-edge and understanding of rheumatic diseases (48.4%) and drug therapy (33.7%); good communication (35.8%); understanding the role of the team (27.4%); working effectively (23.2%) in a multidisciplinary team; assessment of patients by physical examination (28.4%); teaching (26.3%), research (17.9%); organizational skills (14.7%); ability to perform intra-articular injections; and the interpretation of investigations (9.5%).
TABLE 1. Current practice of rheumatology nurse practitioners
Current practice Frequently % (n) Usually % (n)
Drug monitoring 82.1 (78) 15.8 (15)Education of patients 97.9 (93) 2.1 (2)Counselling patients 91.6 (87) 8.4 (8)Arranging baseline investigations 92.5 (86) 6.5 (6)Liaising with other healthcare professionals 69.5 (66) 25.3 (24)Co-ordinating a team approach 70.2 (66) 25.5 (24)Dealing with referrals to rheumatology 56.8 (54) 24.2 (23)Research and audit 35.1 (33) 37.2 (35)Intra-articular injections 26.6 (25) 14.9 (14)Admission for in-patient care 12.6 (12) 18.9 (18)
TABLE 2. Knowledge and skills identified by rheumatology nurse practitioners as necessary for their role
Knowledge and skills % (n)
Adequate knowledge and understanding of rheumatic disease 48.4 (46)Knowledge of medication used for treatment 33.7 (32)Good communication skills 35.8 (34)Care and assessment of patients 28.4 (27)Rheumatology experience 31.6 (30)Understanding the role of the multidisciplinary team 27.4 (26)Teaching skills 26.3 (25)Ability to work effectively within a team 23.2 (22)Research skills 17.9 (17)Organizational skills 14.7 (14)Joint injections skills 9.5 (9)Interpretation of investigations 9.5 (9)
Goh, Samanta and Samanta94
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Role enhancement
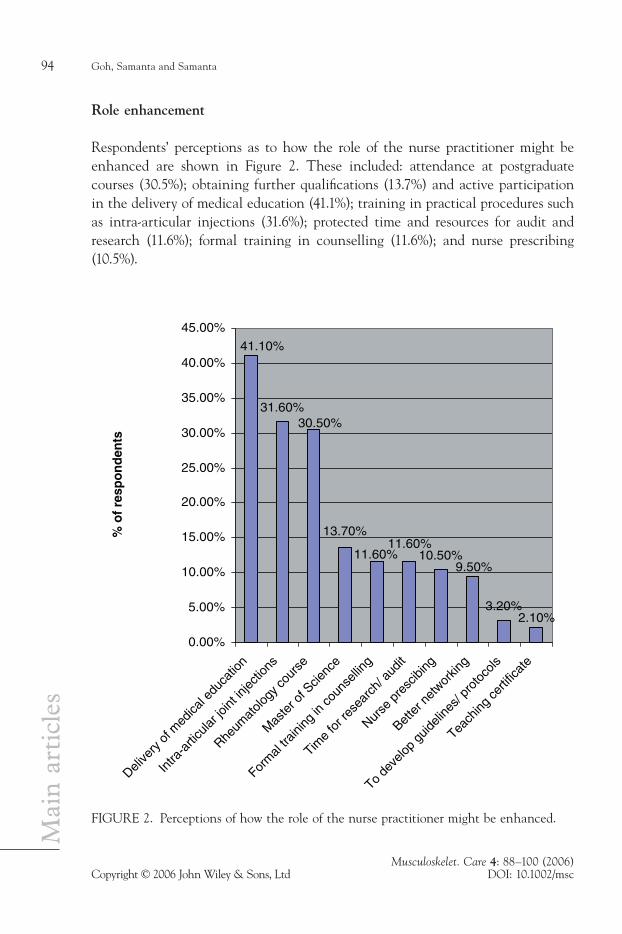
Respondents’ perceptions as to how the role of the nurse practitioner might be enhanced are shown in Figure 2. These included: attendance at postgraduate courses (30.5%); obtaining further qualifications (13.7%) and active participation in the delivery of medical education (41.1%); training in practical procedures such as intra-articular injections (31.6%); protected time and resources for audit and research (11.6%); formal training in counselling (11.6%); and nurse prescribing (10.5%).
31.60%
10.50%
3.20%
41.10%
2.10%
9.50%
11.60%11.60%
13.70%
30.50%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
Delive
ry o
f med
ical e
duca
tion
Intra
-arti
cular
joint
injec
tions
Rheum
atolo
gy co
urse
Mas
ter o
f Scie
nce
Form
al tra
ining
in co
unse
lling
Time
for r
esea
rch/
aud
it
Bette
r net
workin
g
Nurse
pre
scibi
ng
To de
velop
guid
eline
s/ pr
otoc
ols
Teach
ing ce
rtific
ate
% o
f re
spo
nd
ents
FIGURE 2. Perceptions of how the role of the nurse practitioner might be enhanced.

Rheumatology nurse practitioners’ role 95
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Discussion
The present study was designed to determine the current practice of nurse practi-tioners in NHS rheumatology units and to ascertain their views on the necessary knowledge and skills for the role and their perceptions as to how this role might be enhanced. Whilst a previous study has surveyed extended practice at entry and advanced level of nurses working within rheumatology departments (Carr, 2001), there is still a marked paucity of recent data on how the role of nurses has evolved over the past few years.
A limitation of our study concerns the potential for selection bias in the sampling technique used since our target population was identified using the BHPR handbook. It is clear that not all nurse practitioners who might have fulfilled our inclusion criteria would be members of the BHPR and for this reason the results may not be representative of the overall population. It could perhaps be further argued that nurse practitioners who are members of BHPR are likely to be more proactive and aware of the educational and development opportunities that exist. An alternative sampling technique would have been to enlist the co-operation of consultant rheumatologists, since a national database is available of all those cur-rently in practice. The consultants could have been asked to pass on the question-naire to nurse practitioners attached to their unit. However, the extent to which this approach might have biased the findings (through use of an intermediary) is indeterminate.
Current practice described by respondents includes dealing with the more common rheumatological conditions such as rheumatoid arthritis, psoriatic arthrop-athy, osteoarthritis and ankylosing spondylitis. The majority of nurse practitioners routinely undertake monitoring of drug therapy as well as education and counsel-ling of their patients. These findings broadly concur with those in the published literature (Phelan et al., 1992), and have been evaluated as being effective in terms of patient satisfaction and quality (Hill et al., 1994). A smaller number of nurse practitioners reported that they actively engage in extended role activities such as patient referrals, the administration of intra-articular medication, research, audit and in-patient care. As a proportion of the total respondents this is higher in our study when compared to that of Phelan et al. (1992). The authors are conscious that the variation in practice among nurse practitioners could partly be due to local differences in the number of allied health professionals performing similar roles, for example, physiotherapists who perform joint injections. In this study we did not survey or compare the role of other healthcare professionals allied to medicine. From free-text comments received it would appear that there is a sense of willing-ness among nurses for furthering their professional development. Assuming that

Goh, Samanta and Samanta96
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
nurse practitioners are actually prepared to extend their clinical role, there would then be a need to address the gap between ‘what is done’ and ‘what could be done’. It is likely that this gap will be bridged with the recent establishment of Skills for Health (2004), which focuses primarily on education and training of employees within the NHS, as this initiative is in the process of actively formulating compe-tencies for rheumatology.
Two principal themes have emerged from nurse practitioners’ own perceptions of how their role could be enhanced. These pertain to clinical care (intra-articular injections, formal counselling and nurse prescribing) and education (postgraduate training, research and audit). Our results indicate that only about one quarter of respondents regularly performs intra-articular injections, and a third of the remain-der would welcome the opportunity for training. None of the respondents was involved in the prescription of medication but we are aware that with the recent introduction of supplementary prescribing and further extension of this role, nurse practitioners are likely to engage in this activity in the near future. Although the majority (91.6%) (n = 87) frequently engage in counselling, 8% felt the need for specific training in this area in order to enhance their role and effectiveness. Of the remainder (8.4%) (n = 8) who usually engage in counselling, 37.5% (n = 3) stated that they would value the opportunity to obtain a recognized qualification.
Our study suggests an overall willingness among nurse practitioners to develop their role. This enthusiasm should be nurtured as there are several potential benefits for the clinical care of patients. Evidence suggests that nurse practitioners in rheumatology departments are able to offer a quality of care similar with that of a physician (Hill et al., 1994) and are able to detect early synovitis with a degree of accuracy that approaches that of an experienced rheumatologist (Gormley et al., 2003). Nurses with extended roles tend to provide more holistic care (Ryan, 1997) thereby helping to avoid fragmentation of services, and enhance job satisfaction (Rees, 1996). Given the resource constraints upon the existing system and the drive towards greater cost-effectiveness (Department of Health, 2000), the role of the nurse practitioner could perhaps be usefully employed in meeting waiting list targets. Furthermore, it is our opinion that developing their role within research, audit and medical education could have a beneficial effect for the training of junior doctors whose work patterns have had to change in line with the European Working Time Directive requirements and Modernizing Medical Careers (Department of Health 2004). In the context of medical education the potential for nurse practitioners in rheumatology to engage in the teaching and training of medical staff has largely remained untapped. It has been suggested that nurse practitioners may have an important educational role in delivering the undergradu-ate musculoskeletal medical curriculum (Goh et al., 2004).

Rheumatology nurse practitioners’ role 97
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Currently in the UK, there are no defined competencies for nurse practitioners (Ryan, 1996). The NHS Plan (Department of Health, 2001a) has identified 10 key components by which the role of nurses could be enhanced. These include perform-ing outpatient procedures, prescribing medicine and treatment, making and receiv-ing referrals, admitting and discharging patients, managing patient caseloads, running clinics, taking a lead in the organization of local health services, carrying out a range of resuscitation procedures and triaging patients using the latest infor-mation technology. This is helpful in as much as these factors may serve as a generic guide as to how to achieve an extended role in nursing, but is not specialty specific for rheumatology. To our knowledge this is the first study that has canvassed the views of nurses in rheumatology with respect to the attributes they consider as being essential to fulfil such a role. Reported attributes include: knowledge and understanding of the rheumatic diseases and the medication used; good commu-nication skills; the ability to work within a multidisciplinary team; skills in physical examination; teaching; organization; and research. Further studies of this kind are required in order to obtain information that could be used to inform criterion- referenced competences for grade selection and career progression.
About one-third of the respondents (31.5%) reported frequent involvement in audit and research. A further 11% stated they would welcome enhanced opportuni-ties for this. Audit should be encouraged and facilitated as part of quality improve-ment in healthcare under the aegis of clinical governance (Department of Health, 2001b). In the context of clinical governance, an acknowledged cause for concern is that of the potential liability of the nurse practitioner in a clinical negligence action (Dowling et al., 1996). Undoubtedly, professional accountability will remain with the nurse practitioner (Department of Health, 1989), and on this account he or she will be answerable to the Nursing and Midwifery Council. However, in a case of purported negligence, it is suggested that an act or omission will be judged according to the standard expected of a reasonably competent nurse practitioner exercising his or her special skill (Edwards and Hassell, 2000). However, as our results confirm, there are no clearly defined functions of this role, unlike that of the consultant nurse (Ryan, 2001). In reality, therefore, the identification of such a standard may not be simple. It is nevertheless vital that new incumbents are aware of their professional accountability and legal duties owed towards their patients. While all hospital employees (acting in the course of their duties) have the benefit of Crown indemnity as far as actions for negligence are concerned (provided that their organizations are aware and endorse their work), this will not protect employ-ees against criminal actions or sanctions by professional bodies. For the employer, negligence actions and settlements have increasingly severe resource implications and it is essential that employers are aware of the activities and professional remit of their staff. This can partly be achieved with effective systems of appraisal, job

Goh, Samanta and Samanta98
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
specification reviews and ensuring that clear, accurate and up-to-date job descrip-tions are available. In order to protect the NHS Trust and the nurse practitioner it is imperative that nurse practitioners are given adequate opportunities to main-tain their own professional and educational development.
Our study shows that some nurse practitioners in rheumatology already take on a wide range of clinical activities, and perceive that their role could be further enhanced. With the recent introduction of the Agenda for Change initiative, extended roles are recognized (Department of Health, 2005). As a consequence it is likely that more nurses will extend their role into areas traditionally perceived as being part of the ‘medical domain’. There are concerns among the nursing pro-fession that extension of their clinical role may convert nurses into an inferior and lowly paid ‘pseudo doctor’ with an accompanying loss of traditional nursing skills (Edwards, 1995). This may be unfounded within the modern NHS wherein allied health professionals take on a more extended role that has traditionally been regarded as ‘medically dominated’. However, provided that the extended role is performed with the intention of improving overall patient care and that this is clearly defined within their job description, then this could, in our opinion, promote job satisfaction and lead to enhanced career pathways within clinical nursing in rheumatology.
Acknowledgments
The authors would like to thank Dr S Ryan, Nurse Consultant in Rheumatology and two anonymous reviewers for their helpful comments on an earlier draft of this paper.
References
Bird HA (1981). Nurse practitioners in a hospital environment. World Medicine 16: 47.Bird HA, Leatham P, LeGallez P (1981). Clinical metrology. Nursing Times 77: 1926–7.British Health Professionals in Rheumatology (BHPR) Handbook (2001). London: British Society
for Rheumatology (BSR).Carr A (2001). Defining the Extended Clinical Role for Allied Health Professionals in
Rheumatology. Arthritis Research Campaign Conference Proceedings No: 12. ARC: Chesterfield.
Cohen P (1994). Joint efforts. Nursing Times 90: 2–18.Daly W, Carnwell R (2003). Nursing roles and levels of practice: A framework for differentiating
between elementary, specialist and advancing nursing practice. Journal of Clinical Nursing 12: 158–67.
Department of Health (1989). Working for Patients. London: HMSO.

Rheumatology nurse practitioners’ role 99
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Department of Health (2000). The NHS Plan: A Plan for Investment, a Plan for Reform. London: HMSO.
Department of Health (2001a). The NHS Plan: An Action Guide for Nurses, Midwives and Health Visitors. London: HMSO.
Department of Health (2001b). A Quest for Excellence. London: HMSO.Department of Health (2004). Modernising Medical Careers. London: HMSO.Department of Health (2005). Agenda for Change: NHS Terms and Conditions of Service
Handbook. London: HMSO.Dowling S, Martin R, Skidmore P, Doyal L, Cameron A, Lloyd S (1996). Nurses taking on junior
doctors’ work: A confusion of accountability. British Medical Journal 312: 1211–4.Edwards J, Hassell A (2000). Intra-articular and soft tissue injections by nurses: Preparation for
expanded practice. Nursing Standard 14(33): 43–6.Edwards K (1995). What are the nurses’ views on expanding practice? Nursing Standard 9(41):
38–40.Goh L, Samanta A, Cavendish S, Heney D (2004). Rheumatology curriculum: Passport to
the future successful handling of the musculoskeletal burden? Rheumatology 43: 1468–72.
Gormley GJ, Steele WK, Gilliland A, Leggett P, Wright GD, Bell AL, Matthews C, Meenagh G, Wylie E, Mulligan R, Stevenson M, O’Reilly D, Taggart AJ (2003). Can diagnostic triage by general practitioners or rheumatology nurses improve the positive predictive value of referrals to early arthritis clinics? Rheumatology 42: 763–8.
Hill J (1992). A nurse practitioner rheumatology clinic. Nursing Standard 7: 35–7.Hill J (1985). Nursing clinics for arthritis. Nursing Times 81: 33–4.Hill J, Bird HA, Harmer R, Wright V, Lawton C (1994). An evaluation of the effectiveness, safety
and acceptability of a nurse practitioner in a rheumatology outpatient clinic. British Journal of Rheumatology 33: 283–8.
Mounce K, Ryan S (2001). The historical development of extended clinical roles in rheumatology. In Carr A (ed.) Defining the Extended Clinical role for Allied Health Professionals in Rheumatology. Arthritis Research Campaign Conference Proceedings No: 12. ARC: Chesterfield.
NHSME (1991). Junior Doctors: The New Deal. London: NHSME.NMC (2002). Code of Professional Conduct. London: NMC.Newbold D (1996). An evaluation of the role of the nurse practitioner. Nursing Times 92(22):
45–6.Phelan MJ, Byrne J, Campell A, Lynch MP (1992). A profile of the rheumatology nurse specialist
in the United Kingdom. British Journal of Rheumatology 31: 858–9.Rees M, Kinnersley P (1996). Nurse-led management of minor illness in a GP surgery. Nursing
Times 92(6): 32–3.Ryan S (1996). Defining the role of the specialist nurse. Nursing Standard 10(17): 27–9.Ryan S (1997). Nurse-led drug monitoring in the rheumatology clinic. Nursing Standard 11(24):
45–7.Ryan S (2001). Consultant nurses in rheumatology: Releasing the potential! Rheumatology 40:
1325–7.Skills for Health (2004). The Sector Skills Council for Health. Available from
www.skillsforhealth.org.ukVan den Hout WB, Tijhuis GJ, Hazes JM, Breedveld FC, Vliet Vlieland TP (2003). Cost
effectiveness and cost utility analysis of multidisciplinary care in patients with Rheumatoid arthritis: A randomized comparison of clinical nurse specialist care, inpatient care and day patient team care. Annals of Rheumatic Diseases 62: 308–15.

Goh, Samanta and Samanta100
Musculoskelet. Care 4: 88–100 (2006)Copyright © 2006 John Wiley & Sons, Ltd DOI: 10.1002/msc
Mai
n a
rtic
les
M
Correspondence should be sent to A Samanta FRCP, MD, Department of Rheumatology, University Hospitals of Leicester NHS Trust, Leicester Royal Infirmary, Leicester LE1 5WW. Tel: 0116 258 5940, Fax: 0116258 5833. E-mail: [email protected]
Received July 2005 Accepted January 2006





























