Embed Size (px)
Citation preview

The LaryngoscopeLippincott Williams & Wilkins, Inc.© 2006 The American Laryngological,Rhinological and Otological Society, Inc.
Frontal Sinus Cranialization Using thePericranial Flap: An Added Layerof Protection
Alexander Donath, MD; Raj Sindwani, MD, FACS, FRCS
Objectives: Extensive fractures involving the an-terior and posterior tables of the frontal sinus aretreated by frontal sinus cranialization. During thisprocedure, the disrupted posterior wall of the frontalsinus is removed, the sinus mucosa is drilled away,and the brain and dura are permitted to rest againstthe repaired anterior wall and sinus floor. Conven-tionally, the area originally occupied by the frontalsinus is left as dead space or filled with free adiposetissue. We describe a method of cranialization using apericranial flap and report our experience with thistechnique. Study Design: Retrospective study. Meth-ods: The medical records of patients who underwentfrontal sinus cranialization using the pericranial flapat our institution were reviewed. Demographics, in-dications for cranialization, complications, and peri-operative outcomes were examined. Results: A total of19 patients underwent (bilateral) frontal sinus crani-alization with the pericranial flap between 2000 and2005. Indications included extensive frontal sinusfractures involving the posterior table (78.9%), muco-cele (10.5%), arteriovenous malformation (5.3%), andfrontal bone osteomyelitis (5.3%). There were no intra-operative complications. A postoperative cerebrospinalfluid leak occurred in one patient with extensive skullbase injuries. This was repaired endoscopically. Follow-up ranged from 9 to 55 months. Conclusions: The peri-cranial flap is easily harvested and versatile. Usingthis vascularized tissue during cranialization affordsadded protection by providing an extra barrier be-tween the intracranial cavity and the frontal boneand sinonasal tract. This technique is inexpensive,safe, and effective and should be considered whencranialization of the frontal sinus is performed.
Key Words: Pericranial flap, frontal sinus cranial-ization, frontal sinus fractures.
Laryngoscope, 116:1585–1588, 2006
INTRODUCTIONManagement of extensive fractures of the frontal si-
nus remains controversial.1–4 These generally occur incases of head trauma resulting from extensive force, andpatients routinely present with multisystem injuries thatare often life-threatening. In the patient with extensivedisruption of the posterior table of the frontal sinus whohas a reasonable prognosis for recovery, ablation of thefrontal sinus(es) by cranialization has been recommended.
Cranialization of the frontal sinus was first describedin 1978 by Donald and Bernstein.5 The original descrip-tion consisted of removing the posterior wall of the frontalsinus, meticulous removal of the frontal sinus mucosa,and allowing the frontal lobe dura mater to come to restagainst the anterior table and floor of the frontal sinus.Goals of this procedure are the extirpation of all sinusmucosa and the complete separation of the intracranialcavity from the sinonasal tract below. Conventionally, thearea originally occupied by the frontal sinus is left as deadspace or filled with free adipose tissue.5–7
Pericranial (PC) flaps based on the supraorbital andsupratrochlear vasculature have previously been usedwith significant success for separation of intracranial andextracranial spaces after major reconstructive efforts inthe head, neck, and anterior skull base.8,9 More recently,reports advocating the use of the PC flap for advancedfrontal sinus operations have surfaced, although thesedescriptions have focused almost exclusively on the use ofthe PC flap in obliteration of the frontal sinus.10–13 Al-though frontal sinus obliteration also requires the re-moval of sinus mucosa and separation from the nasalvault, protection of the exposed intracranial contents is acritical issue encountered only during cranialization.
We hypothesized that the use of the PC flap in frontalsinus cranialization would enhance the safety and efficacyof this procedure. The purpose of this study was to de-scribe our experience with the PC flap in cranialization ofthe frontal sinus.
From the Department of Otolaryngology–Head and Neck Surgery,St. Louis University School of Medicine, St. Louis, Missouri, U.S.A.
Editor’s Note: This Manuscript was accepted for publicationMay 31, 2006.
Presented at the Middle and Western Section Meeting of the Trio-logical Society, San Diego, California, U.S.A., February 2006.
Send correspondence to Dr. Raj Sindwani, Department of Otolaryn-gology–Head and Neck Surgery, St. Louis University Hospital, 3635 VistaAve, 6th Floor, FDT, St. Louis, MO 63110. E-mail: [email protected].
DOI: 10.1097/01.mlg.0000232514.31101.39
Laryngoscope 116: September 2006 Donath and Sindwani: Frontal Sinus Cranialization Using Pericranial Flap
1585

MATERIALS AND METHODSPatients who underwent bilateral cranialization of the fron-
tal sinus using the PC flap technique at our institution wereidentified through a search of the institutional database by Cur-rent Procedural Terminology code for the years 2000 to 2005.Patient charts were retrospectively reviewed for demographics,indications for cranialization, details of the surgical procedure,intraoperative and postoperative complications, and surgicaloutcomes.
Operative TechniqueAll procedures were performed using a two-team approach
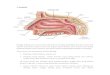
by otolaryngology and neurosurgery. With use of a standardbicoronal incision, a conventional skin flap is dissected anteriorlyin the subgaleal plane to the level of the supraorbital orbital rimsto adequately expose the frontal bone. Once the anteriorly basedPC flap is designed, its borders are incised sharply using thesuperior temporal lines as lateral limits of dissection. The poste-rior edge of the flap is incised in the region of the vertex to provideadequate flap length. As displayed in Figure 1, the flap is thengently elevated from the underlying calvarium using a periostealelevator from posterior to anterior. A frontal craniotomy extend-ing into the superior portion of the frontal sinus is then per-formed, which permits exposure of the posterior table of thefrontal sinus as well as the sinus interior. The dura, intracranialcontents, and posterior frontal sinus table are closely examinedfor injury. Necrotic tissue and foreign material are debrided. Withuse of a drill or rongeur, the disrupted posterior wall of the frontalsinus is then completely taken down, flush with to the floor of theanterior cranial fossa. Bony septations within the sinus are alsoremoved. Next, the mucosa of the frontal sinus is meticulouslyremoved, and the interior of the sinus is carefully drilled (Fig. 2).The mucosa at the frontal sinus ostium is inverted and pushedinferiorly into the nasal cavity, and the superior region of thefrontal sinus outflow tract (previously referred to as the nasofron-tal duct) is plugged with temporoparietal fascia or muscle andsecured with fibrin glue. Any defects of the anterior table of thefrontal bone and the frontal lobe dura are repaired.
After the mucosa is entirely removed and the communica-tion with the sinonasal cavity has been abolished, the PC flap isdraped over the denuded frontal sinus anterior wall and floor aswell as over the exposed anterior cranial fossa floor to cover anybony defects. Once the flap is tucked posteriorly under the infe-rior aspect of the retracted frontal lobes, we then reflect it supe-
riorly so that it rests on the anterior frontal lobe dura mater (Fig.3.). This folding of the flap on itself provides an additional layerof flap coverage between the frontal lobe dura and the damagedanterior frontal bone. The flap is secured into place using duraltacking sutures and fibrin glue. As the frontal bone is placed backto its native position, the anterior region of the craniotomy isdrilled down (approximately 3 mm) to ensure that its edges aresmooth and there is no impingement on the PC flap, which entersthe intracranial cavity at this site (Fig. 4). Finally, the skinwound is closed in a multilayered fashion over a closed-suctiondrain if desired.
RESULTSNineteen patients underwent frontal sinus cranial-
ization using the PC flap technique at our institution
Fig. 1. After anterior dissection of scalp in subgaleal plane througha standard bicoronal incision, pericranial flap (*) is gently elevatedfrom underlying calvarium (arrows) to expose frontal bone.
Fig. 2. Seen through frontal craniotomy, posterior wall of frontalsinus (*) has been taken down, and sinus mucosa has been metic-ulously removed. An anteriorly based pericranial flap (arrows) isshown before inset.
Fig. 3. Pericranial flap is inset so it drapes over interior aspect ofanterior frontal sinus table and covers floor of cranialized cavity.Flap is tucked posteriorly under inferior aspect of retracted frontallobes and then reflected superiorly (arrows) so that it rests onanterior frontal lobe dura mater, providing an additional layer ofcoverage.
Laryngoscope 116: September 2006 Donath and Sindwani: Frontal Sinus Cranialization Using Pericranial Flap
1586

during the past 5 years. Patients ranged in age from 19 to65 years, with an average 36.4 years. Mean follow-up wasover 15 (range, 9–55) months. The large majority of pa-tients were men (84%). Cranialization was performed inthe setting of significant disruption of the posterior tableof the frontal sinus, which was largely caused by extensivefacial trauma in our population (15 of 19 patients, 79%).The mechanism of injury was usually motor vehiclecrashes (53% of trauma cases), followed by blunt forcefrom a variety of objects (40%). In addition to posteriorfrontal sinus wall injuries, 13 of 15 (87%) trauma patientsalso had significant disruption of their anterior frontalsinus tables, which required operative management, usu-ally in the form of reduction and internal fixation of frac-tures. Other indications for cranialization, shown in TableI, included large frontal sinus mucoceles (10.5%), frontalsinusitis causing osteomyelitis with posterior table ero-sion (5.3%), and frontal sinus involvement by a duralarteriovenous malformation (5.3%).
Operative time averaged 5.6 (range, 3–10.5) hours.Although most operative procedures were limited to cra-nialization of the frontal sinus and repair of anterior tablefractures, several patients underwent a variety of associ-ated procedures at the same operative setting includingorbital exenteration (for ruptured globe), ethmoidectomy,reduction and fixation of additional facial fractures, andresection of a dural arteriovenous malformation (Table I).Rents in the dura mater were identified and repaired in 10of 15 (67%) trauma patients. Postoperative length of hos-pital stay varied widely from 3 to 70 days, with 13.1 daysas the average.
There were no intraoperative complications, and noperioperative infections were noted. Postoperative cere-brospinal fluid (CSF) rhinorrhea was encountered in onepatient (representing 6.7% of trauma patients and 5.2% ofthe total study population), who had extensive skull basefractures. This young male patient sustained severe inju-
ries when he was involved in a high-speed collision whileriding a motorcycle without a helmet. At the time of hisfrontal sinus cranialization surgery, numerous anteriorskull base defects were noted and covered with the PCflap. However, postoperatively, the patient developed aCSF leak that did not respond to conservative therapy,including a lumbar drain, and the patient was thereforetaken back to the operating room 3 weeks later for endo-scopic repair. At the second procedure, two areas suspi-cious for CSF leak and bony dehiscence within the lateralwall of the right sphenoid sinus were identified and suc-cessfully repaired endoscopically.
DISCUSSIONThis series, the largest in the North American liter-
ature, supports the PC flap technique as a safe and effec-tive method for cranialization of the frontal sinus. The PCflap is a pedicled myofascial flap that consists of scalpperiosteum and the overlying loose connective (areolar)tissue. The flap is well vascularized, receiving contribu-tions from the supraorbital, supratrochlear, and superfi-cial temporal vessels.14 This rich vascularity allows forversatility in design: the flap may be unilateral or bilat-eral, and it can be based either anteriorly or laterally. ThePC flap can be harvested easily and quickly, and its use infrontal sinus surgery obviates the morbidity of anotherdonor site because it is already within the surgical field.
Most reports describe flap elevation after a tradi-tional bicoronal incision, although other routes of accessmay include pretrichial, trichophytic, through preexistinglacerations, and even the midforehead approach forshorter flaps.10,13,15 The method of harvesting the flap alsovaries by report6,7,10,13–15 because the initial elevation maybe subperiosteal, after which the pericranium is dissectedfrom the scalp skin, or elevation may begin in the sub-galeal plane, to be followed by elevation of the pericra-nium from the cranial bone. We prefer to elevate the flapin the subgaleal plane through a bicoronal incision be-cause the flap is more easily designed and dissected from
Fig. 4. Before replacing frontal bone (*),anterior region of craniotomyis carefully drilled down to ensure that its edges are smooth andthere is no impingement on pericranial flap as it enters intracranialcavity (arrows). Bone is then secured, and skin is closed.
TABLE I.Indications for Cranialization and Modes of Injury.
Associated Procedures
Trauma
MVC 8 (42.1%) Orbital exenteration (1 of 8 pts),ORIF nonfrontal facialfractures (2 of 8)
Blunt trauma 6 (31.6%) ORIF nonfrontal facial fractures(2 of 6)
Penetrating trauma(GSW)
1 (5.3%)
Other
Frontal sinusmucocele
2 (10.5%) Drainage epidural abscess andethmoidectomy (1 of 2)
Frontal boneosteomyelitis
1 (5.3%) Drainage of subdural abscess
AVM 1 (5.3%) Resection of dural AVM
Total 19 8 of 19
MVC � motor vehicle collision; ORIF � open reduction, internal fixa-tion; GSW � gunshot wound; AVM � arteriovenous malformations.
Laryngoscope 116: September 2006 Donath and Sindwani: Frontal Sinus Cranialization Using Pericranial Flap
1587

the stable platform of the calvarium as opposed to dissec-tion from a mobile, previously elevated scalp.
A key element in advocating this flap for the crani-alization procedure is that it provides an additional layerof protection for the intracranial contents by using vascu-larized tissue. We believe that in this particular patientpopulation, the importance of this cannot be overstated.As demonstrated by our study and others,6,7,10,12,15 thelarge majority of individuals requiring this procedurehave suffered extensive frontal trauma, which routinelyresults in significant injury to the anterior frontal sinuswall and forehead skin as well as to the posterior sinuswall. As a function of the cranialization procedure, thealready damaged (and often contaminated) anterior tableis then drilled from the inside, potentially resulting infurther devitalization. In addition to providing coverage ofthe frontal lobes and separating the intracranial cavityfrom the sinonasal tract below, the PC flap also impor-tantly reinforces these damaged anterior structures andfurther separates them from the intracranial contents.The recruitment of healthy vascularized tissue into thisheavily traumatized area may also enhance healing. Byfolding the flap on itself using the technique described, a“double layer” of protection of vital neurologic structurescan easily be achieved. The presence of a PC flap appliedto the dura and floor of the cranialized cavity may alsoconfer an advantage over the longer term, during whichmucocele formation may occur. Believed to arise becauseof the incomplete exenteration of sinus mucosa, the devel-opment of a mucocele is a significant complication thatmay occur 10 years or more after frontal sinus cranializa-tion.16 Theoretically, an extra barrier of tissue may pro-vide the brain and neurologic structures some element ofprotection from an expanding mucocele.
Patients surviving extensive head trauma often haveunique and devastating injuries, which makes comparisonof complication rates somewhat problematic. The majorcomplication rate of 5.2% in this series of 19 frontal sinuscranializations (6.7% for trauma patients, specifically) isconsistent with other published series.6,12,15 The one post-operative CSF leak we encountered, however, was subse-quently identified to be originating in the lateral sphenoidsinus and not the anterior skull base. This complication,therefore, does not represent a failure of the PC flaptechnique, which, even in this patient, did well to preventany CSF leakage from the heavily damaged anterior cra-nial fossa region that was actually covered by the flap. Itshould be further noted that, unlike other reports, we didnot encounter any perioperative infectious complications.Congruent with the findings of the study by Gerbino etal.,12 we suspect that the reduction in postoperative infec-tions may be attributed to the use of the PC flap duringthe cranialization procedure.
The ideal technique for cranialization of the frontalsinus and the role of the PC flap in this operation has yetto be established. Larger-scale efforts with long-term pa-tient follow-up are needed to further clarify the advan-tages of this method. The use of the PC flap, especially inthe setting of extensive frontal trauma, may reduce therisk of CSF leak and perioperative infections and augmentthe results of the cranialization procedure.
CONCLUSIONSThe PC flap is easily harvested and versatile. Using
this vascularized tissue during cranialization affordsadded protection by providing an extra barrier betweenthe intracranial cavity and the frontal bone and sinonasaltract. This technique is inexpensive, safe, and effectiveand should be considered when cranialization of the fron-tal sinus is performed.
BIBLIOGRAPHY1. Gonty AA, Marciani RD, Adornato DC. Management of fron-
tal sinus fractures: a review of 33 cases. J Oral MaxillofacSurg 1999;57:372–379.
2. Newman MH, Travis LW. Frontal sinus fractures. Laryngo-scope 1973;83:1281–1292.
3. Pollak K, Payne E. Fractures of the frontal sinus. OtolaryngolClin North Am 1976;9:517–522.
4. Donald PJ. Frontal sinus fractures. In: Cummings CW,Fredrickson JM, Harker LA, et al., eds. Otolaryngology. St.Louis, MO: Mosby, 1986:47.
5. Donald PJ, Bernstein L. Compound frontal sinus injurieswith intracranial penetration. Laryngoscope 1978;90:225–232.
6. Wallis A, Donald PJ. Frontal sinus fractures: a review of 72cases. Laryngoscope 1988;98:593–598.
7. Donald PJ. Frontal sinus ablation by cranialization. Report of21 cases. Arch Otolaryngol 1982;108:142–146.
8. Wolfe SA. The utility of pericranial flaps. Ann Plast Surg1978;1:146–153.
9. Johns ME, Winn HR, McLean WE, Cantrell WR. Pericranialflap for the closure of defects of craniofacial resections.Laryngoscope 1981;91:952–959.
10. Thaller SR, Donald P. The use of pericranial flaps in frontalsinus fractures. Ann Plast Surg 1994;32:284–287.
11. Ducic Y, Stone TL. Frontal sinus obliteration using a later-ally based pedicled pericranial flap. Laryngoscope 1999;109:541–545.
12. Gerbino G, Roccia F, Benech A, Caldarelli C. Analysis of 158frontal sinus fractures: current surgical management andcomplications. J Craniomaxillofac Surg 2000;28:133–139.
13. Parhiscar A, Har-El G. Frontal sinus obliteration with thepericranial flap. Otolaryngol Head Neck Surg 2001;124:304–307.
14. Potparic Z, Jackson IT, Colen LB, et al. The galeo-pericranialflaps in the forehead: a study of blood supply. Plast SurgForum 1994;17:292–294.
15. Day TA, Meehan R, Stucker FJ, Nanda A. Management offrontal sinus fractures with posterior table involvement: aretrospective study. J Cranio Maxillofac Trauma 1998;4:6–9.
16. Smoot EC, Bowen DG, Lappert P, Ruiz JA. Delayed develop-ment of an ectopic frontal sinus mucocele after pediatriccranial trauma. J Craniofac Surg 1995;4:327–331.
Laryngoscope 116: September 2006 Donath and Sindwani: Frontal Sinus Cranialization Using Pericranial Flap
1588