Embed Size (px)
Citation preview

Ri Long Jin

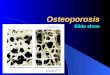
Osteoporosis

Osteoporosis Prevalence Affects 200 million women worldwide
1/3 of women aged 60 to 70 2/3 of women aged 80 or older
Approximately 30% of women over the age of 50 have one or more vertebral fractures
Approximately one in five men over the age of 50 will have an osteoporosis-related fracture in their remaining lifetime
IOF, 2005 (www.osteofound.org)

Osteoporosis
Loss of bone massIncrease bone fragilityIncrease risk of fractures
Osteoporosis, or porous bone, is a devastating disease that robs its victims of bone mass.

5
Normal Bone Osteoporotic Bone
Osteoporosis

6

Wrist Fractures:200,000+
Hip Fractures:300,000+
Vertebral Fractures:700,000+
Other Fractures:300,000+
Source: National Osteoporosis Foundation, 2000
1.5 Million Fractures Annually1.5 Million Fractures Annually

Normal Spine
Osteoporotic Spine
Source: National Osteoporosis Foundation, 2000


BoneBoneMineralisedMineralised
BoneBone
Osteoid
Osteoid
Osteoid
Osteoid
Osteoblasts
Osteoblasts
OsteoclastsOsteoclasts
Courtesy of Michael AmlingCourtesy of Michael Amling

Unbalanced Remodeling: Unbalanced Remodeling: Bone LossBone Loss
Unbalanced Remodeling: Unbalanced Remodeling: Bone LossBone Loss
ResorptionResorption
ReversalReversal
FormationFormation
QuiescenceQuiescence
Insufficientformation - aging
Insufficientformation - aging
ExcessResorption - menopause - hyperPTH
ExcessResorption - menopause - hyperPTH
Bone Loss Bone Loss


I. Primary osteoporosis Idiopathic osteoporosis Type I osteoporosis – postmenopausal ; affecting
trabeculae; compression Fx of spine Type II osteoporosis – senile ; affecting both cortex &
trabeculae; hip Fx, Colles’ Fx
II. Secondary osteoporosis 1.Endocrine disease Hypogonadism; Cushing syndrome Cretinsm; Hyperparathyroidism Diabetes Calcium deficiency
3. Marrow disorders Multiple myeloma
4. Collagen disease Osteogenesis imperfecta; Ehlers-Danlos syndrome Marfan syndrome
2.GI disease Gastrectomy Malabsorption syndrome Chronic obstructive jaundice Severe nutritional deficiency
5. Others COPDLack of exerciseChronic alcoholism RA Smoking

Postmenopausal osteoporosis (type I) Caused by lack of estrogen Causes PTH to overstimulate osteoclasts Excessive loss of trabecular bone
Age-associated osteoporosis (type II) Bone loss due to increased bone turnover Malabsorption Mineral and vitamin deficiency
Secondary osteoporosis
(ex, steroid, heparin, hyperthyroidism,
hyperparathyroidism, Cushing’s syndrome, etc)

Type I Type II Type I Type II
Age(yr)Age(yr)
Sex ratio(F:M)Sex ratio(F:M)
Type of bone lossType of bone loss
Rate of bone lossRate of bone loss
Bone markerBone marker
Fracture sitesFracture sites
Parathyroid functionParathyroid function
Calcium absorptionCalcium absorption
Metabolism of 25OH-D Metabolism of 25OH-D to 1,25(OH)2Dto 1,25(OH)2D
Main causesMain causes
Age(yr)Age(yr)
Sex ratio(F:M)Sex ratio(F:M)
Type of bone lossType of bone loss
Rate of bone lossRate of bone loss
Bone markerBone marker
Fracture sitesFracture sites
Parathyroid functionParathyroid function
Calcium absorptionCalcium absorption
Metabolism of 25OH-D Metabolism of 25OH-D to 1,25(OH)2Dto 1,25(OH)2D
Main causesMain causes
51 - 70
6 : 1
Mainly trabecular
Accelerated
Increased
Vertebrae & distal radius
Decreased
Decreased
Secondary decrease
Related to menopause
51 - 70
6 : 1
Mainly trabecular
Accelerated
Increased
Vertebrae & distal radius
Decreased
Decreased
Secondary decrease
Related to menopause
> 70> 70
2 : 12 : 1
Trabecular & corticalTrabecular & cortical
Not acceleratedNot accelerated
Not increasedNot increased
Vertebrae & hipVertebrae & hip
IncreasedIncreased
Markedly decreasedMarkedly decreased
Primary decreasePrimary decrease
Related to agingRelated to aging
> 70> 70
2 : 12 : 1
Trabecular & corticalTrabecular & cortical
Not acceleratedNot accelerated
Not increasedNot increased
Vertebrae & hipVertebrae & hip
IncreasedIncreased
Markedly decreasedMarkedly decreased
Primary decreasePrimary decrease
Related to agingRelated to aging

Persistent, unexplained back pain
Shorter than you used to be Spinal deformities

Recurrent fractures Fracture from minimal trauma
Experiencing chronic medical problems

1) Genetic or constitutional factors
a. white or Asia ethnicity b. maternal history of fractures c. small body frame d. long hip axis length e. premature menopause (<45 years) f. late menarche
1) Genetic or constitutional factors
a. white or Asia ethnicity b. maternal history of fractures c. small body frame d. long hip axis length e. premature menopause (<45 years) f. late menarche
European Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis Foundation


Factors contributing to osteoporosis II
Factors contributing to osteoporosis II
2) Lifestyle and nutritional factors
a. nulliparity
b. prolonged secondary amenorrhea
c. smoking
d. excessive alcohol intake
e. inactivity
f. prolonged immobilization
g. prolonged parenteral nutrition
h. low body weight
2) Lifestyle and nutritional factors
a. nulliparity
b. prolonged secondary amenorrhea
c. smoking
d. excessive alcohol intake
e. inactivity
f. prolonged immobilization
g. prolonged parenteral nutrition
h. low body weight
European Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis Foundation

“Women married to a smoker
have a 91% greater
risk of heart disease”

TOBACCO USE CAN TOBACCO USE CAN MAKE YOU IMPOTENTMAKE YOU IMPOTENT
Cigarettes may cause sexual impotence due to decreased blood flow to the penis. This can prevent you from having an erection.
Health Canada
WARNINGWARNING

a. anorexia nervosa
b. malabsorption due to gastrointestinal and hepatobiliary disease
c. primary hyperparathyroidism d. thyrotoxicosis
e. primary hypogonadism f. prolactinoma
g. hypercortisolism (Cushing's disease or syndrome)
h. Osteogenesis imperfecta i. rheumatoid arthritis
j. chronic obstructive pulmonary disease k. post transplantation
l. chronic neurological disorders m. chronic renal failure
n. mastocytosis o. type I diabetes
a. anorexia nervosa
b. malabsorption due to gastrointestinal and hepatobiliary disease
c. primary hyperparathyroidism d. thyrotoxicosis
e. primary hypogonadism f. prolactinoma
g. hypercortisolism (Cushing's disease or syndrome)
h. Osteogenesis imperfecta i. rheumatoid arthritis
j. chronic obstructive pulmonary disease k. post transplantation
l. chronic neurological disorders m. chronic renal failure
n. mastocytosis o. type I diabetes
3) medical disorders 3) medical disorders
Factors contributing to osteoporosis IIIFactors contributing to osteoporosis III
European Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis Foundation

4) Drugs
a. chronic corticosteroid therapy
b. excessive thyroid therapy
c. anticoagulants
d. chemotherapy
e. gonadotropin releasing hormone agonist or
antagonist
f. chronic phosphate-binding antacid use
g. anticonvulsant
4) Drugs
a. chronic corticosteroid therapy
b. excessive thyroid therapy
c. anticoagulants
d. chemotherapy
e. gonadotropin releasing hormone agonist or
antagonist
f. chronic phosphate-binding antacid use
g. anticonvulsant
Factors contributing to osteoporosis IVFactors contributing to osteoporosis IV
European Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis FoundationEuropean Osteoporosis Foundation

BMD test Biochemical markers - Blood - urine
BMD test Biochemical markers - Blood - urine

X-ray finding:
1.Mineral loss 30-40%2. Generalized decreased density of bone 3. Spine –manifested in early stage Loss trabeculae (transverse >longitudinal), thining of cortex, codfish spine; Wedging of vertebra caused by compression Fx > round back or kyphotic deformity4. Widening of medullary canal – loss of both cortical & trabecular bones 5. Bone densitometries a. Singh’s index b. Photon absorptiometry c. Dual energy X-ray absorptiometry DEXA d. Quantitative computed tomography, QCT


low energy and high energy X-ray
lumbar spine A-P & Lat., femoral
neck, whole body, ulnar & radius
good precision and accuracy
low dose X-ray (1/50 of chest X-
ray)
Most popular
low energy and high energy X-ray
lumbar spine A-P & Lat., femoral
neck, whole body, ulnar & radius
good precision and accuracy
low dose X-ray (1/50 of chest X-
ray)
Most popular



Normal : T-score > -1.0Osteopenia : -2.5 < T-score < -1.0 Osteoporosis : T-score < -2.5Servere osteoporosis : T-score < -2.5 with presence of one or more fractures (established osteoporosis)
Normal : T-score > -1.0Osteopenia : -2.5 < T-score < -1.0 Osteoporosis : T-score < -2.5Servere osteoporosis : T-score < -2.5 with presence of one or more fractures (established osteoporosis)
WHO criteria of osteoporosisWHO criteria of osteoporosis
T-score ; adult peak bone density 와 비교한 score

Bone resorption
Pyridinoline & Deoxypyridinoline
Type I collagen telopeptide N-terminal C-terminal
Hydroxyproline
Tartrate resistant acid phosphatase
Galactosyl hydroxylysine
Bone resorption
Pyridinoline & Deoxypyridinoline
Type I collagen telopeptide N-terminal C-terminal
Hydroxyproline
Tartrate resistant acid phosphatase
Galactosyl hydroxylysine
Bone formationBone formation
Osteocalcin (bone gla protein)Osteocalcin (bone gla protein)
Bone-specific alkaline Bone-specific alkaline
phosphatasephosphatase
Procollagen type I propeptidesProcollagen type I propeptides C-terminal (PICP)C-terminal (PICP) N-terminal (PINP)N-terminal (PINP)
Bone formationBone formation
Osteocalcin (bone gla protein)Osteocalcin (bone gla protein)
Bone-specific alkaline Bone-specific alkaline
phosphatasephosphatase
Procollagen type I propeptidesProcollagen type I propeptides C-terminal (PICP)C-terminal (PICP) N-terminal (PINP)N-terminal (PINP)

Anyone with a fragility fracture All women age 65 and older Postmenopausal younger than 65
with risk factors Men over 50 with risk factors


Treatment of Osteoporosis
1. Treament for primary factor or disease & regular exercise
2. medication: - Enough dose of calcium + activated
Vitamin D (1(OH)D3 or 1.25(OH)2D3)
- Estrogen threapy for type I osteoporosis - Synthectic calcitonin3. Fracture : Avoid longterm bed rest Early ambulation after firm internal fixation

36
Bisphosphonates Fosamax Actonel Didronel Estrogen Replacement Therapy Medications made from natural hormones SERMs Raloxifene (Evista)
Calcitonin Sodium Flouride

37
Vitamin D metabolites
Parathyroid hormone
New bisphosphonates
New SERMs

Weight-Bearing Exercise


Inflammation of a joint usually accompanied by pain swelling and changes in structure
Etiology Degenerative Joint Disease
Osteoarthritis, Rheumatoid Metabolic disturbances
Gout Infection
Gonococcus, TB, Pneumonia

1. Classification:
major socio-ecomomic problem
I. Rheumatoid Arthritis (RA)
II. Degenerative arthritis ․Primary osteoarthritis ․Secondary osteoarthritis
III. Others :
Hemophilic Arthritis
Gouty Arthritis
Neuropathic or Charcot Joint
Chondrocalcinosis &Pseudogout

PainStiffnessRednessSwellingKnee effusions Crepitus


Chronic, Systemic Autoimmune Disease Inflammation of the connective tissue, Inflammation of the joint
Prevalence 0.5-1% 30-50 yrs F>M

unkonwn Infectious : hemolytic and nonhemolytic
types streptococci Endocrine: this is suggested by response
to adrenocortical steroids. Autoimmune: frequently exhibit various
allergic manifestations. = Eosinophilia is frequent.
Metabolic:

Diffuse proliferative synovitis Villous processes hypertrophy -> necrotic
&extruded into the joint .• Fibrinoid necrosis around with fibroblasts • ->fibrous tissue • Synovium making->pannus- cover the
articular surface with fibrous connective tissue• Vascular granulation tissue ->growing from
medullary->distruction articular cartilage

Joint symptoms Pain, swelling, stiffness (↑in morning) Deformity and muscle atrophy Limited ROM
Other Symptoms Fatigue Anorexia Low-grade fever Inflammatory changes of heart and
lungs


3. Dx of RA: ACR classification criteria for RA
Morning stiffness at least 1 hour Swelling of 3 or more joint Swelling of hand joints (P.I.P M.C.P. or Wrist) Symmetric joint swelling Erosion or decalcification on radiograph of hand Rheumatoid nodule Presence of serum rheumatoid factor
1987 USA RA Association:
4 of more of sever criteria

History and physical exam Labs
Rheumatoid factors (RF) ESR (Erythrocyte Sedimentation Rate) Synovial fluid exam
X-rays Symmetric periarticular osteoporosis Narrowing joint space Bony trabeculation bridge, obliterate the
joint space: ankylosis

ESRî Slight Leukocytosis, ±eosinophlilia (immune reaction) usually normocytic,hypochromic anemia refractory to iron. Alpha2 fraction of gamma globulin(RF, IgM gamma globulin
against Fc portion of IgG) îSerum albumin Serum (because of the presence of abnormal macroglobulins called
rheumatoid factors) will agglutinate or flocculate suspended particles such as hemolytic streptococci, sheep erythrocytes, latex, and with bentonite sensitized with human gama globulin
Latex fixation test on serum; unknown serum +gamma globulin-latex suspension
Inhibition test : rheumatoid serum of known high agglutinating activity + unknown euglobulin +standard gamma glubulin-latex suspension

4. RA 的病因和预后
① Pathogenesis of RA.
unknown
Genetic predisposition
Chromic antoimmune responces
② Indications of poor prognosis in RA.
reduced functional states
early radigraphic changes
multiple involved joints
older age at onset
high titiers of rhematoid factor
prolonged elevation of ESR
lower educational level
genetics

NO CURE
Goals of Treatment Relieve pain Reduce inflammation Stop or slow joint damage and deformity Improve well-being and ability to function

5. RA medical treatment
․NSAID ․DMARD ․Steroid ․others

6. RA operative treatment ․Synovectomy ․Arthrodesis ․Arthroplasty


Metabolic disorder
Inflammation 2° deposits of uric acid crystals in joint
Body produces too much uric acid Or
Body excretes too little uric acid

Uric acid is a waste product formed from the breakdown of purines
High levels of purines are found in organ meats (liver, brains, kidney), anchovies, herring, mackerel. Alcohol and some drugs may affect
purine excretion.

Uric acid levels elevated to 9-10 range (normals ~ 3 – 6)
No symptoms
Client may not progress to symptomatic disease

Sudden onset, acute pain, redness, swelling
Usually hits the big toe, may affect another joint
Fever, chills Elevated WBC, sed rate “Attack” lasts hours to weeks 60% have recurrent attack in 1 yr

Hyperuricemia untreated
Tophi (urate crystals deposits) develop in cartilage, synovial membranes, tendons, soft tissues
Pain, ulceration, nerve damage
Uric acid crystals—>kidney stones

Symptom: hyperuricemia ( >7mg%). Several yrs
① acute : 1st metatarsophalangeal joint , sudden onset
* Intercritical Period: weeks -years
recurr factor: meat, high purine diet, drug, fatigue, trauma, surgery
② chronic: continuous slight pain, degenerative arthritis, fibrous ankylosing

Dx: ① family history ② Repeated attacks with intervals of freedom from pain ③ Renal disturbance as urate calculus ④ Hyperuricemia ⑤ Satisfactory response to adequate doses of colchicine ⑥ Sodium biurate crystals ( rod type, blunt ended, strong
negative birefringence under polarized microscope, uricase digested) at joint aspirate ensure.
* tophi : subcutaneous tissue -> urate salt deposit -> ear site -> chalky white material.

Pain Indocin NSAIDS, Narcotics Steroids (po/intra-articular)
Interrupt urate crystal formation Colchicine: Does NOT alter uric acid
levels Inhibit tubular reabsorption of uric
acid Probenecid (Benemid)
Reduce the production of uric acid Allopurinol (Zyloprim)

Dietary Management Drink 3-4 quarts of fluids daily Avoid alcohol Sometimes no diet is prescribed
Low purine diet Meats, seafood, yeast, beans, peas,
lentils, oatmeal, spinach, asparagus, cauliflower, mushrooms