Embed Size (px)
Citation preview

CURRENT CONCEPTS IN ENDOCRINE SURGERY
Riedel’s thyroiditis: impact and strategyof a challenging surgery
Kerstin Lorenz & Oliver Gimm &
Hans Jürgen Holzhausen & Stephan Kittel &Jörg Ukkat & Phuong Nguyen Thanh &
Michael Brauckhoff & Henning Dralle
Received: 23 June 2006 /Accepted: 2 January 2007 / Published online: 3 April 2007# Springer-Verlag 2007
AbstractBackground No surgical standard for Riedel’s thyroiditis(RT) is established. Salvage surgery follows severe cervicaland compressive airway symptoms or strong suspicion ofmalignancy. Obscured planes and multi-infiltrative exten-sion prevent sufficient surgery with considerate complica-tions. No alternative definitive treatment is available. Infailing conservative treatment, the role of surgery in RTremains unclear.Materials and methods Clinical manifestation, treatment,outcome and follow-up in a unique series of eightconsecutive patients with RT are presented.Results Seven female patients and one male patient withcervical tumor growth or thyroiditis underwent four totaland three sub-total thyroidectomies, respectively, onepatient declined remedial surgery. Complications were onebilateral laryngeal nerve palsy and one transient hypopara-thyroidism. Histology confirmed RT with perithyroidal
extension and excluded malignancy in all. Symptomaticrelief of cervical and airway obstruction was achieved inall. Follow-up revealed two extensive mediastinal RTrecurrences 1 and 6 years after surgery.Conclusion Favourable symptomatic outcome and allevia-tion of steroids in the majority render surgery for RTvaluable when conservative treatment fails. However, moreradical procedures show no advantages and recurrences arenot prevented. The demanding technique in RT requiresspecial surgical expertise and highly recommends intra-operative neuromonitoring.
Keywords Riedel’s thyroiditis . Surgery . Outcome .
Neuromonitoring
Introduction
Riedel’s thyroiditis (RT) or invasive fibrous thyroiditis isthe rarest of all forms of thyroiditis with a continuouslyuncertain aetiology. The operative incidence is 0.06%,the female to male ratio is 3.1:1 and the median age ofonset is 51 years (range 23 to 67) [1, 2]. Since theprimary clinical description and denomination by Riedel in1896, the disease’s pathophysiology remains unclear [3].In the literature, there are only a few historical patientgroups clinically described, the largest with 37 cases of RT[1] and the remaining are mostly case reports. Until today,there are about 200 reported cases in total [4]. Mainimportant differential diagnosis are the fibrous variant ofHashimoto’s thyroiditis, granulomotous thyroiditis, solitaryfibrous tumor, cancer or lymphoma of the thyroid. Initially,patients with RT present with a recent rapid enlargement ofa pre-existing goiter. Characteristically, patients complain
Langenbecks Arch Surg (2007) 392:405–412DOI 10.1007/s00423-007-0147-8
Presented at the 2nd Biennial ESES Congress, 18–20 May 2006,Krakow, Poland.
K. Lorenz (*) :O. Gimm : S. Kittel : J. Ukkat : P. N. Thanh :M. Brauckhoff :H. DralleDepartment of General, Visceral and Vascular Surgery,Martin-Luther University of Halle-Wittenberg,Ernst-Grube-Straße 40,06120 Halle/Saale, Germanye-mail: [email protected]
H. J. HolzhausenDepartment of Pathology,Martin-Luther University of Halle-Wittenberg,Ernst-Grube-Straße 40,06120 Halle/Saale, Germany

Tab
le1
Patient
demog
raph
ics,diseasespecific
symptom
s,thyroidparameter
anddiagno
stics
Patient,gend
er,
age(inyears)
Durationof
symptom
s(w
eeks)
Thy
roid
labo
ratory
Sym
ptom
sUltrasou
ndScintigraph
yFNA
15
fT33.8pg
/ml[2.2–5
.1]a
Painful
node
righ
tthyroid
lobe
localcompression
+dy
sphagiaon
righ
tneck,
nody
spno
ea
Hyp
oechoiclesion
,poo
rly
definedrigh
tthy
roid
lobe,
leftun
regu
larmargin;
vol.
12mlrigh
tTL,v
ol.8
ml
leftTL
Und
efined
orthotop
ic(TC99mmscintig
raph
y)multifocal
autono
my
Few
cells,sparse
histol.,
noatyp
iafT412
.8ng
/ml[7.8–19.4]
TSH
0.9mU/l[0.3–4
.0]
Anti-TPO
14.7
U/m
l[40–50
]TSH-Rec.AB0U/l[U
/l]“borderlinehy
perthy
roid”
248
fT31.9pg
/ml[2–5
]bRem
arkablestrido
r,dy
spno
ea,local
compression
pressure,
dysplasia
Highly-degenerated
hypoechogenic,loose
pattern;v
ol.2
8mlrightT
L,
vol.25
mlleftTL
n.a.
u.d.
fT41.8ng
/ml[0.7–2
]TSH
3.18
mU/l[0.25–3.5]
Anti-TPO
568mg/dl
[−10
0/50
0]TA
K14
7.6ng
/ml[−10
0/50
0]Tg0.1ng
/ml[−35
]CRP18
.5mg/dl
[<5]
ES11/22
“borderlinehy
pothyroid”
312
fT3<0.1pm
ol/l[4.4–9.3]a
Dyspn
oea,
dysphagia+
odyn
ophagia,
cervical
pressure+compression
,ho
arseness
Inho
mog
eneous–
hypo
echo
icmultin
odular;
vol.58
mlrigh
tTL,vo
l.39
mlleftTL
Mandibu
lary
lesion
,redu
cedup
take
(−0.12
%)
(49Mbq
Tc9
9mm)
“Lym
phocitic
thyroiditis”
fT4<2pm
ol/l[10–27
]TSH
>50
nU/m
l[0.4–3
.5]
Anti-TPO
15,200
U/m
l[−10
0/50
0]Tg<0.5ng
/ml[2–7
0]TRAK
<0.9U/l[<1.0]
Calcitonin2.5pg
/ml[<10
]“hyp
othy
roid”
44
fT31.22
mmol/l[0.69–2.11]b
Rapidly
prog
ressivegrow
thleftTL,dy
sphagia,
dyspno
ea,cervical
pressure,radiatingpain
towards
mandibu
la
Inho
mog
enou
s,hy
poecho
ic;vo
l.37
mlleft
TL,vo
l.16
mlrigh
tTL
Scinti,40
Mbq
TC99mm
uptake
1.6%
LTno
UPT,
RTno
rmal
“Dou
btful”
suspicious
ofmalignancy
fT412
9mmol/l[570
–154
]TSH
1.91
mU/l[0.49–4.67
]CRP42
.2mg/dl
[<8]
Calcitonin14
.9pg
/ml[<4.6]
“euthy
roid”
552
fT31.25
mmol/l[1.23–2.93
]aAsphy
gtic
attacks,thyroid
enlargem
ent,dy
spno
ea,
dysphagia,
dyspho
nia,
coug
h
Major
cervical
portion,
totalthyroid;
vol.57
ml
–Openbiop
sy:RT
fT44.92
mmol/l[66–18
1]TSH
2.53
mU/l[0.4–4.2]
Tg1.3ng
/l[0–40]
Calcitonin<1.5
ES36
/56
“euthy
roid”
672
fT33.1a
Severedy
spno
ea,
dysphagia,
prog
ressive
thyroidgrow
th
Inho
mog
eneous
hypo
echo
ic,blurred
margins;vo
l.50
mlRTL,
–Lym
phocytic
thyroiditis
fT411.6
TSH
19.8
406 Langenbecks Arch Surg (2007) 392:405–412

of cervical pressure, dysphagia or dyspnoea. The thyroidappears unusually hard and fixed, thus easily resemblingmalignancy. Most often there is bilobar involvement;however unilobar or even regional involvements aredescribed [4]. The progressive fibrous replacement ofthyroid tissue results in early hypothyroidism of theprimarily often euthyroid patients. Diagnostically, thetypically prevailing findings are a pronounced hypoechoicgland on ultrasound with the absence of vascular flow, adiminished uptake with a cold appearance on TC99-scintigraphy, hypointensity in T1 and T2-weighted MRIand fibrous tissue fragments and moderate cellularity withinflammatory cells on fine needle aspiration [5, 6].Laboratory findings may reveal elevation of leucocytesand erythrocyte sedimentation rate. Thyroid antibodiesmay be present in about 45–64% [1, 4]. In some instances,the primary clinical symptom may be hypoparathyroidismdue to the extension of the inflammatory fibrous process tothe parathyroids [2, 7]. Association with retroperitonealfibrosis in some patients and rare associations with otherdiseases, e.g. multiple sclerosis are described [8–13]. Insome instances, the disease is self-limiting for no obviousreasons; however symptomatic treatment is necessary.Conservative treatment with thyroid hormones, steroidsand tamoxifen is the first-line therapeutical option; how-ever, most often surgery in these patients is warrantedbecause of the high suspicion of malignancy [14–19].There is conflicting evidence of the role of surgery for RTas the nature of the disease is benign, however localinvasion mimics a semi-malignant nature, frequentlyrequiring extensive and multi-visceral resection whenconservative treatment fails and surgery becomes neces-sary. Moreover, the multi-infiltrative inflammation in RTclassifies surgery in these patients as technically mostchallenging even when compared to surgery for thyroidmalignancy. Thus, no surgical concept for RT is estab-lished so far. In this study, we report a unique series ofeight consecutive patients with RT and arrive at a surgicalalgorithm for this most challenging group of patients.
Materials and methods
From January 1995 to 2006, a consecutive series of eightpatients (seven women, one man) with histopathologicallyproven RT presented in the surgical department forevaluation of thyroid surgery. Except for one patient, allunderwent primary or remedial surgery in our institution.There was a symptom-oriented assessment of pre-operativeand post-operative complaints, and surgical outcomeevaluations and clinical follow-up of all patients wereperformed.
vol.63
mlLT
LMAK
>1,00
0“euthy
roid”
712
fT31.3mmol/lb
Dyspn
oea,
dysphagia,
cervical
compression
Echocom
plex,hy
poecho
iclesion
s51
Mbq
,up
take+0.2%
“euthy
roid”,
cold
nod.
LTOpenbiop
sy:RT
fT488
mmol/l
TSH
1.47
mU/m
l[0.55–
4.5]
Anti-T/O
18.9
JU/m
l[<35
]Anti-Tg26
.0JU
/ml[<4]
TRAK
<1.0U/l[<9]
“euthy
roid”
848
fT34.10
pmol/l[3.84–6]
aProgressive
thyroidgrow
th,
cervical
compression
Diffusely
hypercalcemic;
vol.56
mlLT
L,
vol.52
mlRTL
–Openbiop
sy:RT
fT419
.3pm
ol/l[7.7–14.2]
TSH
0.11
mU/l[0.3–3.5]
“hyp
erthyroid”
n.a.:no
tavailable,MD:miscellaneou
sdata(kids,ri...,fam
.hist.thyroiddis.),d.n.:un
diagno
sticdu
eto
sparse
material,w:weeks,m
:mon
ths,#:
follo
wtreatm
ent,previous
clinically
hypo
thyroid.
aWith
thyroidho
rmon
esubstitution.
bWith
outthyroidho
rmon
esubstitution.
Langenbecks Arch Surg (2007) 392:405–412 407

Results
In this series, there were 7 female patients and 1 malepatient with the mean age of 41 years (range 20–60).History of thyroid disease including goiter, cervicalpressure, pain or dyspnoea lasted a mean of 30 weeks(range 4–72) (Table 1). The presented patients all com-plained of severe subjective symptoms in projection of thecervical region with predominantly terrifying attacks ofdyspnoea, progressive dysphagia and cervical compression.All patients had previously received conservative medicaltreatment involving thyroid hormones, oral steroids andtamoxifen (Table 2). There was a temporary good symp-tomatic response to steroids in five out of eight patients,however the effect was lost whenever a dose-reduction wasattempted or the disease recurred early after or steroid sideeffects were not well-tolerated (two out of five). None ofthe patients showed any alleviation of progressive thyroid
enlargement with thyroid hormone supplementation and/orsteroids. Tamoxifen treatment was tried in one patient butdid not show any beneficial effect. There were threepatients who underwent previous outward thyroid surgeryfor the underlying RT. Previous surgical procedurescomprised: One transsternal–transthoracic probatory resec-tion of the dominating mediastinal tumor, however resec-tion was esteemed impossible and a pulmonary aneurysm indirect contact to the extending RT tumor was enforced witha Gore–Tex-patch (patient no. 5). Two patients underwentsurgery intended for thyroidectomy, however intra-opera-tive findings of the severe inflammatory hard tumor wasjudged as an inoperable situation with a high suspicion ofmalignancy and thus open biopsy and wedge excision wereperformed (patient no. 7) and a wedge resection of theisthmus was performed (patient no. 8). Indication forsurgical evaluation was suspicion of malignancy in 3 (38%)patients, failure of or recurrence under medical treatment
Table 2 Pre-treatment, CT/MRI—findings, local findings and conservative course
Patient Thyroidhormones
Medicaltreatment (days)
Steroids Tamoxifen CT/MRI Local findings Conservativecourse
1 – – – – – Firm, hard RTL,no LN
Rapid growth,suspectedmalignancy;inflammatorycomponent
2 Thyroxine125 mg/dMethizol (2a)
– 50 mgPrednisone/day(1a)
+ (2 mon) Trachea enwrapped,compressed,deviated
Very firm,nodular, fixed,slightly painful noLN
Radioiodinetreatmenthypothyroidismcons. progression,with ↓ steroids
3 Thyroxine150 mg/day
– – – – Very nodular,extremely hard,impaired moveno LN
Early onsethypothyroidismrapid enormousthyroid growthhoarseness
4 Thyroxine100 mg/day
Diclofenac100 mg/day
100 mgPrednisone/day
– Inhom. largenodular goiter,Invitation trachea,hypodense mal.anopel. RTL
Iron hard, fixed,indolent, largeLN erl.
Rapidlyprogressivegrowth LTL
5 Thyroxine100 mg/day
– 20 mgPrednisone/day
– Trachea deviation,compression(9 mm)
Firm, Fixed,nodular thyroidleft suprasternal
Remnant rapidprogression, shortalleviation withsteroids
6 Thyroxine125 mg/day
– 40 mgPrednisone/day
– – Very firm, tender Rapid progression,empor. alleviationwith steroids
7 Thyroxine125 mg/day
Diclofenac100 mg/day
10 mgPrednisone
– – Firm, nodularresistenceventral LTL
Slowly, progressivegrowth
8 Thyroxine150 mg/day
– – – – Very firm,enormous goiter,inoperative/indolent
Rapid progressive
408 Langenbecks Arch Surg (2007) 392:405–412

in 6 (75%) patients. Pre-operative work-up included thyroidhormones, thyroid scintigraphy, ultrasound and CT or MRIin all (Figs. 1, 2, 3). Pre-operatively, 2 (25%) patients wereeuthyroid without supplement of thyroid hormones, 2patients showed clinical and/or laboratory hypothyroidismwith and without thyroid hormones, respectively and theremaining 2 patients were hyperthyroid with and withoutthyroid hormones, respectively (Table 1). Fine needleaspiration biopsy was performed in 5 (63%) patients andwas suspective in 2 (25%) and inconclusive in 2 (25%)patients. In 1 (13%) patient, no sufficient material could beretrieved in FNA (Table 2). In 4 (50%) patients, operativediagnosis was Riedel’s thyroiditis due to clinical work-upor primary outward surgery. Indication for surgery waspossibly suspicion of malignancy or intractable symptom-atic disease. There were 4 (50%) total thyroidectomies, 2(25%) bilateral sub-total resections, 1 (13%) hemithyroid-ectomy with contralateral sub-total resection and 1 (13%)hemithyroidectomy with contralateral near-total resectionperformed, respectively (Table 3). In 2 (25%) patients,lymph node dissection was performed because intra-operatively, malignancy could not be ruled out even usingfrozen section. On two occasions, unilateral resection of therecurrent laryngeal nerve (RLN) became technically inevi-table for adequate resection. Surgical specimen werecharacterised and definitive histopathological diagnosisshowed RT in all (Fig. 4). The characteristic criteria ofextrathyroidal extension of the inflammatory fibrosingprocess were found at different degrees in all patients,whereas prevalence of perivasculitis and thrombosis was63%. Intra-operative neuromonitoring (IONM) becameavailable at our institution in 1998 and has since been usedroutinely. In this series, IONM was applied in all patientsoperated on. Complications were 1 (13%) transient bilateralRLN-palsy (RLNP) in a patient with unilateral RLNresection and intra-operative loss of the contralateral IONM
signal with intact nerve anatomy. After anti-phlogisticmedical and logopaedic treatment, the transient RLNPresolved within 3 months post-operatively. There wastransient hypocalcemia in 2 (25%) patients, however inter-mittent oral calcium substitution was only necessary in 1patient. Mean follow-up is 52 months (range: 3–78 months).There are two patients with severe symptomatic RT, one per-sistent and another with an impressively large recurrenceextending into the substernal region and circumferently en-trapping the trachea and esophageus. All patients are underthyroid hormone substitution and the above mentioned two
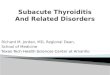
Fig. 3 Sagittal CT image of RT (patient no. 8)
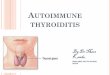
Fig. 2 Transversal CT image of RT (patient no. 8)
Fig. 1 Pre-operative ultrasound: typical hypoechoic appearance, rightthyroid lobe (patient no. 8)
Langenbecks Arch Surg (2007) 392:405–412 409

patients still require considerate steroids between 20 and50 mg prednisone per day. No patient underwent furtheroperative or adjunctive treatment so far.
Discussion
RT remains a rare form of thyroiditis with unknownaetiology. Formerly, RT was discussed to be a late form ofHashimoto or de Quervain’s thyroiditis, however mostauthors agree on distinct histopathological features and itsunique gross appearance [20–23]. Due to the low incidenceof RT, the majority of published data is derived from casereports. Only a few authors investigated larger historicalseries with histopathological features and retrospectivelyevaluated clinical findings and treatment outcome [1]. It is
Table 3 Surgery, histology and complications
Patient Surgery Histology Complications Post-operative findings Course/follow-up
1 Total thyroidectomy IONM RT (perithyroidal fibrousextension into strap muscles)
– Ca 2.1 mmol/la UCUEVL ++
2 Near total thyroidectomybilateral LA IONM
RT chronic sclerosing thyroiditisseverely extrathyroidal extensionperivasculitis
– Ca 2.20 mmol/la Impressivesympomaticrecurrence after5 years
UEVL ++
3 Bilateral subtotal thyroidresection IONM
Severely sclerosing thyroiditis,extension into soft tissue andstrap muscles
– Ca 1.4 mmol/la UCPTH 10.7 pg/mlb
4 Total thyroidectomyresection NLR leftsystematic LA K1a+bselective LA K2 IONM
Inflammatory-sclerosingthyroiditis pleomorphic fibrosis,perithyroidal infiltration,perivalsculitis LN v/o tumor
Transient bilateralRLNP stridor
Ca 1.99 mmol/la
PTH 4.1 pg/mlb
5 Bilateral subtotal resection,exploration sternotomy, leftanterior thoracotomy, PTFEvascular prothesis for coverof pulmonary arteryaneurismc
RTc – Ca 2.10 mmol/la Persist. exterivesSymptom.(envico.../thor...tumor)
Open biopsyd Pasrouled vascular fibrosisd –6 Total thyroidectomy IONM Invasive sclerosing RT – Ca 2.3 mmol/la UC7 Wedge excisionc RT continuing in adherent soft
tissuec– Ca 2.43 mmol/la UC
Hemithyroidectomy left,enuclation right IONMd
Fibros. NT+perithyroiditis totalthyroidal and partialextrathyroidal extensiond
8 Near total right,hemithyroidectomy leftresection RLN Lexploration...d IONM
RTd – Ca 2.20 mmol/la UC
Wedge resection isthmusc RTc
UE: uneventful, UC: unchanged.a 2.25–2.75 mmol/l.b 12–72 pg/ml.c Primary outward surgery.d No remedial surgery.
Fig. 4 Surgical specimen of RTwith tracheal entrapment (patient no. 8)
410 Langenbecks Arch Surg (2007) 392:405–412

stressed that medical anti-inflammatory treatment is thefirst-line treatment of choice, however in failing conserva-tive treatment, progressive airway compression or ulti-mately an acute airway emergency surgery may becomenecessary [24]. The unique series of patients presented heredemonstrate the full spectrum of the typical symptoms ofRT with rapid thyroid enlargement airway compression anddysphagia. However, there seems to be stronger pro-nounced degree of complaints and none had a history oflonger known goiter [2]. Conservative treatment ultimatelyfailed in all patients presented and surgery becamenecessary. In the literature it is well-pronounced thatsurgery in RT is extremely challenging due to thecompletely undiscriminable planes, the inflammatorycomponent with a tendency to bleed and obscured iden-tification of structures and fixedness. It is thereforesurprising that only a few authors mention complicationrates at all. It may be assumed that the expectedly elevatedcomplication rate, especially regarding RLNP and hypo-parathyroidism is well-underestimated. On the other hand,the extreme difficult dissection may be responsible for thepredominantly restricted resection with isthmusectomy oranterior wedge resections, although recurrences followingrestrictive resection are also described. Also, in someinstances, the nature of the thyroidal disease intra-opera-tively cannot be differentiated between benign and malig-nant as was true for two cases in our series. Therefore, nosurgical strategy is so far established. Herein, we aimed atradical surgery whenever possible. Even though the natureof the disease is benign, there are no reliable criteria topredict recurrences that may be surgically intractable due tothe involved structures comparable to malignancy. With theaid of IONM, a valuable adjunct for nerve identification inthe obscured planes of the fibrous process, a more radicalyet safe resection becomes possible. However, even usingIONM, in one case a transient bilateral RLNP afterresection of one RLN could not be prevented. There wasno necessity for tracheostomy, however transient stridorwas severe in the early post-operative period. In 50% of thepatients herein, total thyroidectomy was accomplished andtwice unilateral resection of RLN was technically neces-sary. After sub-total resection, there were two cases ofseverely symptomatic RT, one persistent after outwardsurgery and one recurrence 5 years after surgery in ourinstitution. In the remaining three patients with sub-totalresection, follow-up revealed no recurrences and nosymptoms. With regard to the results, we arrive at thefollowing algorithm for patients with known or suspectedRT who require surgery: Pre-operative work-up shouldinclude ultrasound and CT or MRI or sometimes PET toevaluate extension of the disease, especially possiblemediastinal affection [25, 26]. At the same time, involve-ment of the adjacent structures is assessed and the
possibility of soft tissue resection and prospective necessityof RLN resection must be discussed with the patient indetail. This evaluation should consider the individualpatient’s response to steroid treatment and subjectivesymptoms and his acceptance and compliance in case ofpossible RLN resection. Whenever possible, resectionshould be performed with anatomical and functionalpreservation of the RLN. It does not seem reasonable toenforce most radical surgery at cost of a higher complica-tion rate; however in some cases, unilateral RLN resectionmay be discussed to arrive at adequate resection for thealleviation of symptoms, especially dyspnoea and dyspha-gia. In our experience, IONM is highly recommendable forthe most challenging surgery in this type of thyroid disease.
Conclusions
The primary choice of treatment in RT is prednisone ortamoxifen. However, in failing conservative treatment, theclinical symptoms of RT may individually be disabilitatingto a degree that surgery becomes inevitable. Surgicalprocedures should be as radical as safely possible to pre-vent recurrences. The pre-operative investigational standardshould always include CT or MRI in addition to the usuallaboratory, ultrasound and scintigraphy findings to evaluatethe perithyroidal extension and plan resection adequately.This also enables detailed discussion with the individualpatient with regard to possible extended surgical proce-dures. Although benign in nature, RT is a severe surgicalchallenge and should only be treated in very experiencedcenters with access to IONM and an experienced patholo-gist for frozen section. The rarity of the disease makes ithighly desirable to collect and unite international data onthe actual incidence, treatment, outcome and course of RT.
References
1. Woolner LB, Mc Conahey WM, Bears OB (1957) Invasivefibrous thyroiditis (Riedel’s struma). JCEM 17:201–220
2. Hay ID (1985) Thyroiditis: a clinical update. Mayo Clin Proc60:836–843
3. Riedel BM (1896) Die chronische, zur BIldung eisenharterTumoren führende Entzündung der Schilddrüse. Verh Dtsch GesChir 25:101–105
4. Martin Schwaegerle S, Bauer TW, Esselstyn (1988) Single casereports. Riedel’s thyroiditis. Am J Clin Pathol 90:715–722
5. Harigopal M, Sahoo S, Recant WM, DeMay RM (2004) Fineneedle aspiration of Riedel’s disease: report of a case and reviewof the literature. Diagn Cytopathol 30:193–197
6. Papi G, Corrado S, Carapezzi C, De Gaetani C, Carani C (2003)Riedel’s thyroiditis and fibrous variant of Hashimoto’s thyroiditis: aclinicopathological and immunohistochemical study. J EndocrinolInvest 26:444–449
Langenbecks Arch Surg (2007) 392:405–412 411

7. Nazal EM, Belmatoug N, De Roquancourt A, Lefort A, Fantin B(2003) Hypoparathyroidism preceding Riedel’s thyroiditis. Eur JIntern Med 14:202–204
8. Emch TM, Miller MA (2005) Case report. Retroperitoneal fibrosisinvolving the left kidney in a patient with a remote history ofRiedel’s thyroiditis. AJR Am J Roentgenol 184:97–98
9. Kotilainen P, Airas L, Kojo T, Kurki T, Kataja K, Minn H, NuutilaP (2005) Riedel’s thyroiditis in a patient with multiple sclerosis.Neuroendocrinol Lett 26:67–68
10. Armiagliato M, Paolini R, Bianchini E, Monesi G, Zamboni S,D’Andrea E (2002) Hashimoto’s thyroiditis and Grave’s diseaseassociated with retroperitoneal fibrosis. Thyroid 12:829–831
11. Drieskens O, Blockmans D, Van den Bruel A, Mortelmans L(2002) Riedel’s thyroiditis and retroperitoeneal fibrosis in multi-focal fibrosclerosis. Positron emission tomographic findings. ClinNucl Med 27:413–415
12. Fontaine S, Gaches F, Lamant L, Uzan M, Bennet A, Caron Ph(2005) An unusual form of Riedel’s thyroiditis: a case report andreview of the literature. Thyroid 15:85–88
13. Tütüncü NB, Erbas T, Bayraktar M, Özgen A, Gedik O (2000)Multifocal idiopathic fibrosclerosis manifesting with Riedel’sthyroiditis. Endocr Pract 6:447–449
14. Hostalet F, Hellin D, Ruitz JA (2003) Tumefactive fibroinflam-matory lesion of the head and neck treated with steroids: a casereport. Eur Arch Otorhinolaryngol 260:229–231
15. Moore SE, Suvarna SK, Harrison BJ (2001) Management ofcomplicated intrathoracic Riedel’s thyroiditis. ANZ Journal ofSurgery 71:559–560
16. Pritchyk K, Newkirk K, Garlich P, Deeb Z (2004) Tamoxifentherapy for Riedel’s thyroiditis. Laryngoscope 114:1758–1760
17. Few J, Thompson NW, Angelos P, Simeone D, Giordano T, ReeveT (1996) Riedel’s thyroiditis: treatment with tamoxifen. Surgery120:993–999
18. Lo JC, Loh KC, Rubin AL, Cha I, Greenspan FS (1998) Riedel’sthyroiditis presenting with hypothyroidism and hypoparathyroid-ism: dramatic response to glucocorticoid and thyroxine therapy.Clin Endocrinol 48:815–818
19. Jung YJ, Schaub CR, Rhodes R, Rich FA, Muehlenbein SJ (2004)A case of Riedel’s thyroiditis treated with tamoxifen. Anothersuccessful outcome. Endocr Pract 10:483–486
20. Meijer S, Hausman R (1978) Occlusive phlebitis, a diagnosticfeature in Riedel’s thyroiditis. Virchow’s Arch A 337:339–349
21. KojimaM,Nakamura S, Yamane Y, Shimizu K, Sugihara S,MasaweN (2003) Riedel’s thyroiditis containing cytologically atypicallyappearing B-cells: a case report. Pathol Res Pract 199:497–501
22. Heufelder AE, Goellner JR, Bahn RS, Gleich GJ, Hay ID (1996)Tissue eosinophilis and eosinophil degranulation in Riedel’sinvasive fibrous thyroiditis. J Clin Endocrinol Metab 81:977–984
23. Rodriguez I, Ayala E, Caballero C, De Miguel C, Matia-Guiu X,Cubilla AL, Rosai J (2001) Solitary fibrous tumor of the thyroidgland. Am J Surg Pathol 25:1424–1428
24. Sato K, Hanazawa H, Watanabe J, Takahashi S (2005) Differentialdiagnosis and management of airway obstruction in Riedel’sthyroiditis: a case report. Auris Nasus Larynx 32:439–443
25. Kotilainen P, Airas L, Kojo T, Kurki T, Kataja K, Minn H, Nuutila P(2004) Positron emission tomography as an aid in the diagnosis andfollow-up of Riedel’s thyroiditis. Eur J Intern Med 15:186–189
26. Papi G, Corrado S, Cesinaro AM, Novelli L, Smerieri A,Carapezzi C (2002) Riedel’s thyroiditis: clinical, pathologicaland imaging features. Int J Clin Pract 56:65–67
412 Langenbecks Arch Surg (2007) 392:405–412



![Hashimoto’s Thyroiditis and Encephalopathy · Hashimoto’s Thyroiditis and Encephalopathy David S. Younger Department of Neurology, ... [36]. In humans, disease susceptibility](https://img.pdfslide.net/doc/110x75/5c814ac809d3f263728c0c55/hashimotos-thyroiditis-and-hashimotos-thyroiditis-and-encephalopathy-david.jpg)









![Riedel’s thyroiditis presenting as large retropharyngeal ... · in literature are multinodular goiters[2,8,9] with one large study failing to mention the pathology of the goiter.[3]](https://img.pdfslide.net/doc/110x75/5b6a1e7a7f8b9af6098bb781/riedels-thyroiditis-presenting-as-large-retropharyngeal-in-literature.jpg)