Embed Size (px)
DESCRIPTION
Saket Jain, Setu Satani, Sanyukta Khandelwal, Sakshi Dandona, Akshay Gursale. Right sided congenital diaphragmatic defect with liver hernia: A case report. IAIM, 2014; 1(4): 75-79.
Citation preview
Right sided congenital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Case Report
Right sided congenital diaphragmatic defect
with liver hernia: A case report
Saket Jain1, Setu Satani
1Resident, Department of Radio diagnosis, MGM Hospital
2Resident, Department of Pediatrics, MGM Hospital
*Corresponding author email:
How to cite this article: Saket Jain, Setu Satani, Sanyukta Khandelwal, Sakshi Dandona, Akshay
Gursale. Right sided congenital diaphragmatic defect with liver hernia: A case report
1(4): 75-79.
Available online at
Received on: 01-12-2014
Abstract
Congenital diaphragmatic hernia is a rare entity occurring in 1 in 2000
for 8% of all major congenital anomalies. Congenital diaphragmatic hernia (CDH) is a major surgical
emergency in new-borns because the key to survival depends on the prompt diagnosis and
treatments. We reported here
hernia in a 7 month old baby, who came to seek medical care at a tertiary care centre in Navi
Mumbai for on and off cold and cough with breathlessness after feeds. The baby was tachypneic
examination. Immediately chest X
symptomatically and clinically suspected case of congenital diaphragmatic hernia. It was a case of
right sided congenital diaphragmatic hernia.
Key words
Congenital diaphragmatic hernia,
Introduction
Congenital diaphragmatic hernia is definitely a
matter of concern due to its high incidence of
morbidity and mortality. There
predominance with the ratio of 3:2
are three types and these are posterolateral
genital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
Right sided congenital diaphragmatic defect
with liver hernia: A case report
, Setu Satani1*
, Sanyukta Khandelwal2, Sakshi Dandona
Akshay Gursale1
, Department of Radio diagnosis, MGM Hospital, Navi Mumbai
, Department of Pediatrics, MGM Hospital, Navi Mumbai
*Corresponding author email: [email protected]
Saket Jain, Setu Satani, Sanyukta Khandelwal, Sakshi Dandona, Akshay
congenital diaphragmatic defect with liver hernia: A case report
Available online at www.iaimjournal.com
2014 Accepted on:
Congenital diaphragmatic hernia is a rare entity occurring in 1 in 2000-4000 live
for 8% of all major congenital anomalies. Congenital diaphragmatic hernia (CDH) is a major surgical
borns because the key to survival depends on the prompt diagnosis and
ed here a case of right sided congenital diaphragmatic
, who came to seek medical care at a tertiary care centre in Navi
off cold and cough with breathlessness after feeds. The baby was tachypneic
examination. Immediately chest X-ray and CT scan of thorax and abdomen was done to assess
symptomatically and clinically suspected case of congenital diaphragmatic hernia. It was a case of
right sided congenital diaphragmatic hernia.
Congenital diaphragmatic hernia, Right side, Rare, Liver herniation, 7 month female.
Congenital diaphragmatic hernia is definitely a
matter of concern due to its high incidence of
morbidity and mortality. There is a male
predominance with the ratio of 3:2 [1]. There
are three types and these are posterolateral
Bockdalek hernia (usually occurring at
approximately 6 weeks of gestation), the
anterior Morgagni hernia and the hiatal hernia.
Most common type of CDH is
Bockdalek hernia (85%) through posterolateral
defect in diaphragm (Foramen of Bockdalek). In
left sided hernia the large and the small bowel
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 75
Right sided congenital diaphragmatic defect
with liver hernia: A case report
, Sakshi Dandona1,
, Navi Mumbai, India
, Navi Mumbai, India
Saket Jain, Setu Satani, Sanyukta Khandelwal, Sakshi Dandona, Akshay
congenital diaphragmatic defect with liver hernia: A case report. IAIM, 2014;
Accepted on: 11-12-2014
4000 live births and accounts
for 8% of all major congenital anomalies. Congenital diaphragmatic hernia (CDH) is a major surgical
borns because the key to survival depends on the prompt diagnosis and
iaphragmatic defect with liver
, who came to seek medical care at a tertiary care centre in Navi
off cold and cough with breathlessness after feeds. The baby was tachypneic on
ray and CT scan of thorax and abdomen was done to assess
symptomatically and clinically suspected case of congenital diaphragmatic hernia. It was a case of
iver herniation, 7 month female.
Bockdalek hernia (usually occurring at
approximately 6 weeks of gestation), the
anterior Morgagni hernia and the hiatal hernia.
Most common type of CDH is left-sided
Bockdalek hernia (85%) through posterolateral
defect in diaphragm (Foramen of Bockdalek). In
left sided hernia the large and the small bowel

Right sided congenital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
with or without intra abdominal solid organ may
be herniated into the thorax. In right
hernia (incidence 13%) only the liver and portion
of small bowel tend to be herniated into the
thorax [2]. Chest x-ray and CT are considered as
best diagnostic methods [3].
Case report
A 7 month old female, full term, normal vaginal
delivery with no previous antenatal
ultrasonography done presented to MGM
Hospital, Kamothe, Navi Mumbai with chief
complaints of on and off episodes of cough and
cold, breathlessness especially after feeds s
two months. Usually child presents with
malnutrition after 1 month of birth. This is unlike
the classic presentation of CDH as this patient
was well developed and presented late i.e. 5
months of age. There were no gastrointestinal
symptoms in this case. On examination, the child
was found to be tachypneic with a respiratory
rate of 60 breaths per min with mild intercostal
retractions and decreased air entry on the right
side. The most severely affected events develop
respiratory distress at birth where
majority present respiratory symptoms within
24 hours. Of birth, only 2.6-10% of the cases
may present after this period. It has been seen
that the proportion of right sided CDH in late
presenting cases is higher. In retrospective view
of patients with right CDH, the mean age for
diagnosis to be six months. Usually right sided
CDH presents with gastrointestinal problems
and left sided CDH presents with respiratory
symptoms. Immediately chest x
ill defined non- homogenous soft tissue
occupying lower half of the right hemi
with shift of mediastinum and heart towards the
left side. The right hemi-diaphragm silhouette is
obscured with this opacity (Photo
the left hemi-diaphragm appears at its normal
level without any diaphragmatic defect.
genital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
abdominal solid organ may
be herniated into the thorax. In right-sided
cidence 13%) only the liver and portion
of small bowel tend to be herniated into the
ray and CT are considered as
A 7 month old female, full term, normal vaginal
delivery with no previous antenatal
ultrasonography done presented to MGM
Hospital, Kamothe, Navi Mumbai with chief
complaints of on and off episodes of cough and
cold, breathlessness especially after feeds since
two months. Usually child presents with
malnutrition after 1 month of birth. This is unlike
the classic presentation of CDH as this patient
was well developed and presented late i.e. 5
no gastrointestinal
e. On examination, the child
was found to be tachypneic with a respiratory
rate of 60 breaths per min with mild intercostal
retractions and decreased air entry on the right
side. The most severely affected events develop
respiratory distress at birth whereas large
majority present respiratory symptoms within
10% of the cases
may present after this period. It has been seen
the proportion of right sided CDH in late
presenting cases is higher. In retrospective view
with right CDH, the mean age for
diagnosis to be six months. Usually right sided
CDH presents with gastrointestinal problems
and left sided CDH presents with respiratory
Immediately chest x -ray showed an
homogenous soft tissue opacity
occupying lower half of the right hemi-thorax
with shift of mediastinum and heart towards the
diaphragm silhouette is
(Photo - 1) whereas
diaphragm appears at its normal
ut any diaphragmatic defect.
Photo - 1: Frontal chest radiograph: R
diaphragm is obscured with the well
opacity in right lower zone.
Tomogram showed soft tissue attenuation
occupying lower half of right hemi thorax with
non-visualization of right hemi diaphragm. There
is evidence of mediastinal and cardiac shif
towards the left side. (Photo
showed soft tissue attenuation oc
lower hemi thorax part of the right lobe of liver.
It showed at the level of origin of left lower lobe
bronchus the liver can be seen, herniation of
part of right lobe of liver in the right hemi
with non-visualization of right dome of
diaphragm throughout its entire extent.
evidence of shift of mediastinum and heart in
left hemi thorax. (Photo -
contrast enhanced CT was not done on the view
of increased radiation exposure to the child.
Right diaphragmatic crura
discontinuous on its progression.
Kidney was found in normal position whereas
liver was herniating into right hemi thorax.
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 76
Frontal chest radiograph: Right hemi-
diaphragm is obscured with the well-defined
Tomogram showed soft tissue attenuation
occupying lower half of right hemi thorax with
ation of right hemi diaphragm. There
is evidence of mediastinal and cardiac shift
(Photo - 2) NECT of thorax
showed soft tissue attenuation occupying right
part of the right lobe of liver.
at the level of origin of left lower lobe
bronchus the liver can be seen, herniation of
part of right lobe of liver in the right hemi thorax
visualization of right dome of
diaphragm throughout its entire extent. There is
stinum and heart in
- 3, Photo - 4) The
contrast enhanced CT was not done on the view
of increased radiation exposure to the child.
Right diaphragmatic crura were found to be
uous on its progression. (Photo - 5)
found in normal position whereas
into right hemi thorax.
Right sided congenital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
(Photo - 6) Post-operatively X-ray showed repair
of the hernia with absence of the opacity in the
right lower zone, the right lun
expanded. (Photo - 7)
Photo - 2: Tomogram: Soft tissue attenuation
occupying lower half of right hemi thorax with
non-visualization of right hemi diaphragm.
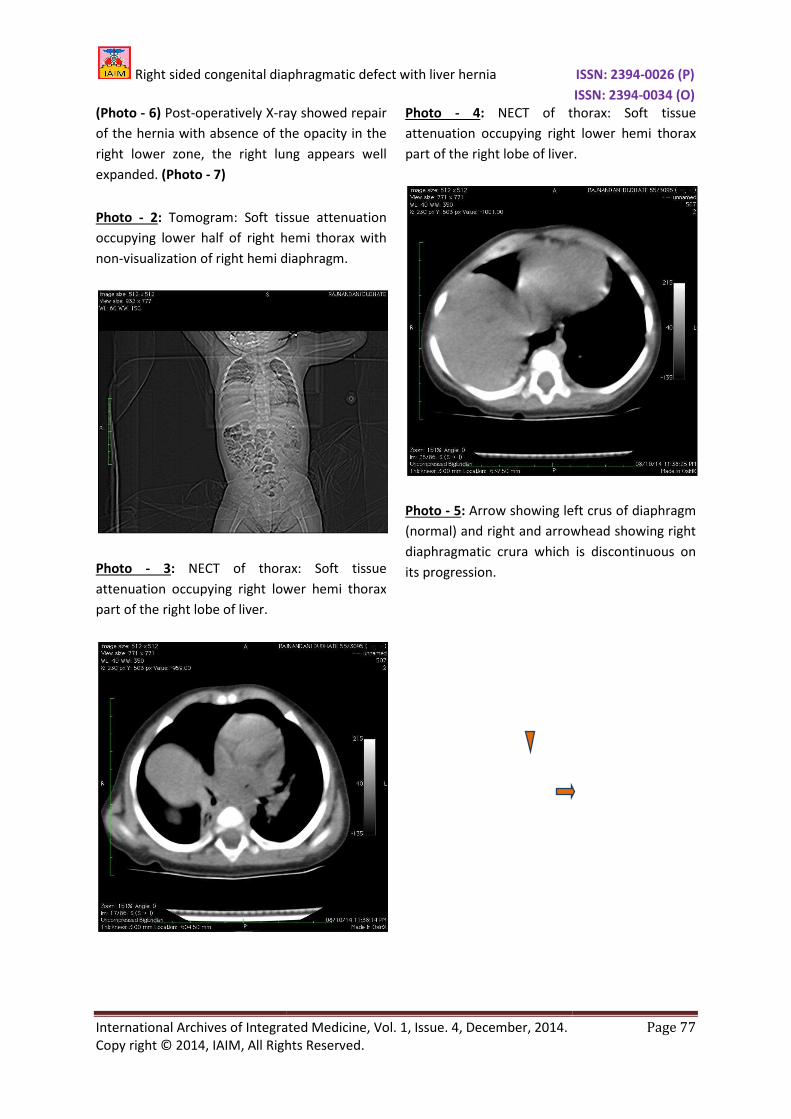
Photo - 3: NECT of thorax: S
attenuation occupying right lower hemi thorax
part of the right lobe of liver.
genital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
ray showed repair
of the hernia with absence of the opacity in the
right lower zone, the right lung appears well
oft tissue attenuation
occupying lower half of right hemi thorax with
visualization of right hemi diaphragm.
of thorax: Soft tissue
cupying right lower hemi thorax
Photo - 4: NECT of thorax
attenuation occupying right lower hemi thorax
part of the right lobe of liver.
Photo - 5: Arrow showing left crus of diaphragm
(normal) and right and arrowhead showing right
diaphragmatic crura which is discontinu
its progression.
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 77
NECT of thorax: Soft tissue
upying right lower hemi thorax
part of the right lobe of liver.
Arrow showing left crus of diaphragm
(normal) and right and arrowhead showing right
diaphragmatic crura which is discontinuous on
Right sided congenital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
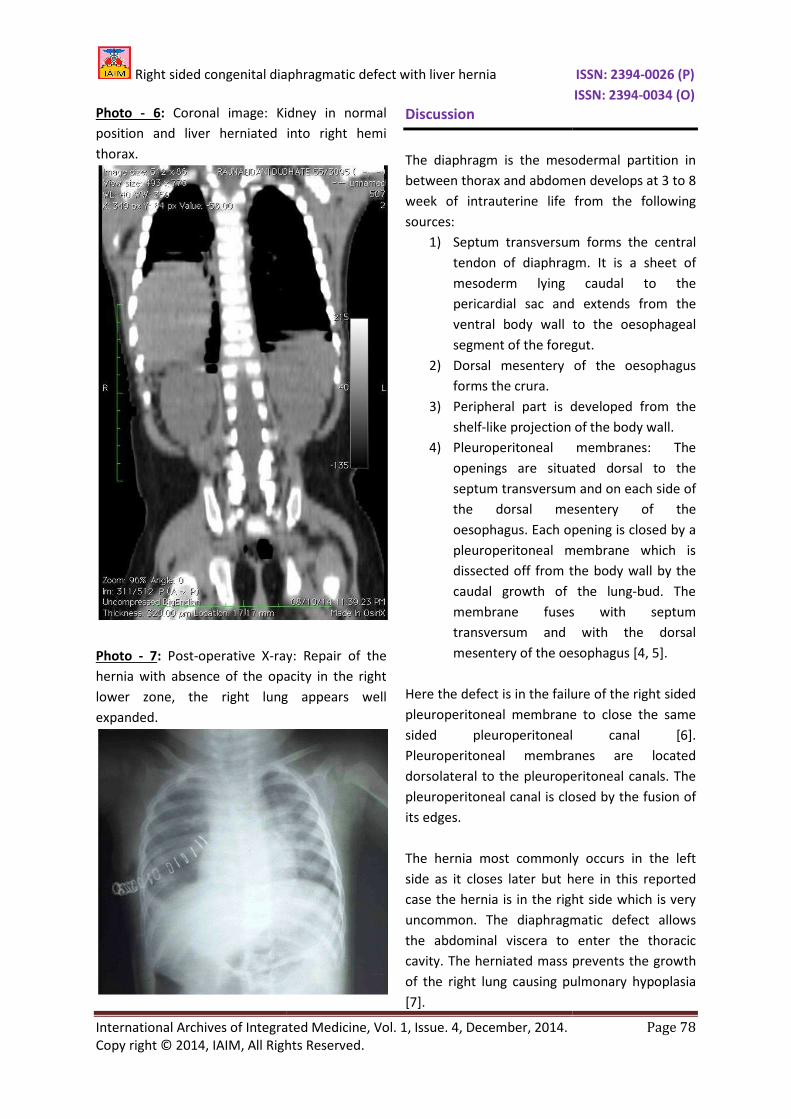
Photo - 6: Coronal image: Kidney in normal
position and liver herniated into right hemi
thorax.
Photo - 7: Post-operative X-ray
hernia with absence of the opacity in the right
lower zone, the right lung
expanded.
genital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
idney in normal
position and liver herniated into right hemi
ray: Repair of the
hernia with absence of the opacity in the right
lower zone, the right lung appears well
Discussion
The diaphragm is the mesodermal partition in
between thorax and abdomen develops at 3 to 8
week of intrauterine life from the following
sources:
1) Septum transversum forms the central
tendon of diaphragm.
mesoderm lying caudal to the
pericardial sac and
ventral body wall to the oesophageal
segment of the foregut.
2) Dorsal mesentery of the oesophagus
forms the crura.
3) Peripheral part is developed from the
shelf-like projection of the body
4) Pleuroperitoneal membranes: The
openings are situated dorsal to the
septum transversum and on each side of
the dorsal mesentery of the
oesophagus. Each opening is closed
pleuroperitoneal membrane which is
dissected off from the body wall by the
caudal growth of the lung
membrane fuses with septum
transversum and with the dorsal
mesentery of the oesophagus
Here the defect is in the failure of the right sided
pleuroperitoneal membrane to close the same
sided pleuroperitoneal canal
Pleuroperitoneal membranes are located
dorsolateral to the pleuroperitoneal canals. The
pleuroperitoneal canal is closed by the fusion of
its edges.
The hernia most commonly occurs in the left
side as it closes later but here in this reported
case the hernia is in the right side which is very
uncommon. The diaphragmatic defect allows
the abdominal viscera to enter the thoracic
cavity. The herniated mass prevents the growth
of the right lung causing pulmonary hypoplasia
[7].
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 78
The diaphragm is the mesodermal partition in
between thorax and abdomen develops at 3 to 8
week of intrauterine life from the following
Septum transversum forms the central
tendon of diaphragm. It is a sheet of
mesoderm lying caudal to the
pericardial sac and extends from the
ventral body wall to the oesophageal
segment of the foregut.
sal mesentery of the oesophagus
Peripheral part is developed from the
like projection of the body wall.
peritoneal membranes: The
openings are situated dorsal to the
septum transversum and on each side of
dorsal mesentery of the
oesophagus. Each opening is closed by a
peritoneal membrane which is
dissected off from the body wall by the
of the lung-bud. The
membrane fuses with septum
transversum and with the dorsal
oesophagus [4, 5].
ilure of the right sided
peritoneal membrane to close the same
sided pleuroperitoneal canal [6].
Pleuroperitoneal membranes are located
dorsolateral to the pleuroperitoneal canals. The
pleuroperitoneal canal is closed by the fusion of
The hernia most commonly occurs in the left
side as it closes later but here in this reported
he hernia is in the right side which is very
uncommon. The diaphragmatic defect allows
the abdominal viscera to enter the thoracic
cavity. The herniated mass prevents the growth
of the right lung causing pulmonary hypoplasia

Right sided congenital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Even though majority of such cases occur as
isolated entity, it is important to look for other
congenital malformations like cardiac anomalies,
pulmonary agenesis or hypoplasia, renal
agenesis, hydronephrosis, spina bifida and
chromosomal anomalies such as Trisomy 21, 18
or 13 which can coexist along with CDH. Familial
inheritance is reported to occur in 2% of the
cases. The key to survival of these patients
depends on the prompt diagnosis, prenatal
management, delivery, stabilization and
treatment. The site, size, contents of the
and associated anomalies also greatly influence
the outcome of the disease.
CDH is also reported to occur in babies of the
mothers who are exposed to quinine,
thalidomide and antiepileptic drugs during
pregnancy [8]. Liver herniation might be
associated with poorer prognosis detected by
radiological investigations in
diaphragmatic hernia. Plain radiography
sometimes may be helpful for presumptive
diagnosis and contrast CT may help to arrive at a
precise diagnosis.
References
1. Torfs CP, Curry CJR, Bateson TF, et al. A
population based study of congenital
diaphragmatic hernia. Teratology
46: 555-65.
Source of support: Nil
genital diaphragmatic defect with liver hernia
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
ch cases occur as
isolated entity, it is important to look for other
congenital malformations like cardiac anomalies,
pulmonary agenesis or hypoplasia, renal
agenesis, hydronephrosis, spina bifida and
chromosomal anomalies such as Trisomy 21, 18
h can coexist along with CDH. Familial
inheritance is reported to occur in 2% of the
cases. The key to survival of these patients
depends on the prompt diagnosis, prenatal
management, delivery, stabilization and
The site, size, contents of the hernia
and associated anomalies also greatly influence
CDH is also reported to occur in babies of the
mothers who are exposed to quinine,
thalidomide and antiepileptic drugs during
. Liver herniation might be
iated with poorer prognosis detected by
radiological investigations in fetal congenital
diaphragmatic hernia. Plain radiography
sometimes may be helpful for presumptive
help to arrive at a
CP, Curry CJR, Bateson TF, et al. A
population based study of congenital
diaphragmatic hernia. Teratology, 1992;
2. Snow RW, Armstrong JRM, Forster D,
Winstanley MT, Marsh VM, Newton CR
et al. Childhood deaths in Africa:
and limitations of
Lancet, 1992; 340: 351
3. Khawahur H, Kattan A, Al
Saidy K. Congenital diaphragmatic
hernia: A local experience. Annal Saudi
Med, 1999; 19(6): 501
4. Dutta A.K. Essential Human Embryology.
3rd
edition. Kolkata: Current Books
International; 1995, p
5. Saddler TW. Langman's Medical
Embryology in Body Cavities. 11
edition. New Delhi: Lippincott Williams
and Wilkins, Wolters Kluwer Health
India Pvt Ltd; 2006, p
6. Moore KL, Persaud TVN.
mesenteries and diaphragm, 7
USA: Elsevier Publishers; 2003, p
97.
7. Standring S, Collins P, Heely LC, Johnson
D, Shah P, Wigley C. Gray's Anatomy in
Development of trachea, lungs and
diaphragm. 39th
London, New York, Oxford, Philadelphia,
St. Louis, Sydney, Toronto: Elsevier
Churchill Livingstones Publication; 2005,
p. 1092-93.
8. Hoboth N. Drugs and congenital
anomalies. Lancet, 1962; 2: 1444.
Nil Conflict of interest:
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 79
Snow RW, Armstrong JRM, Forster D,
Winstanley MT, Marsh VM, Newton CR,
et al. Childhood deaths in Africa: Uses
and limitations of verbal autopsies.
351–5.
Khawahur H, Kattan A, Al-Alaiyan S,
Saidy K. Congenital diaphragmatic
hernia: A local experience. Annal Saudi
501-4.
Essential Human Embryology.
. Kolkata: Current Books
International; 1995, p. 157-59.
Saddler TW. Langman's Medical
Embryology in Body Cavities. 11th
. New Delhi: Lippincott Williams
and Wilkins, Wolters Kluwer Health
India Pvt Ltd; 2006, p. 159-162.
Persaud TVN. Body cavities,
nd diaphragm, 7th
edition.
USA: Elsevier Publishers; 2003, p. 192-
Standring S, Collins P, Heely LC, Johnson
D, Shah P, Wigley C. Gray's Anatomy in
Development of trachea, lungs and
edition. Edinburg,
London, New York, Oxford, Philadelphia,
St. Louis, Sydney, Toronto: Elsevier-
Churchill Livingstones Publication; 2005,
Hoboth N. Drugs and congenital
1962; 2: 1444.
Conflict of interest: None declared.