Embed Size (px)
Citation preview

Rising PSA after Radical Prostatectomy.Rising PSA after Radical Prostatectomy.My Approach.My Approach.
Dr Manish PatelDr Manish Patel Urological Cancer Surgeon Urological Cancer Surgeon
Westmead HospitalWestmead HospitalUniversity of SydneyUniversity of Sydney

Definition of BCRDefinition of BCR• No data evaluating super sensitive PSA assay (ie. Threshold
<0.1ng/ml)
• PSA t ½ is 3.1 days. Measure PSA at least 4 weeks after surgery
• No consensus on BCR definition. (0.2ng/ml to 0.6ng/ml)
– EAU: 0.2ng/ml with 2 subsequent rises.
– Amling et.al. PSA 0.2-0.29ng/ml, 50% stable in this range.
• CP rate increased as threshold increased.
– PSA >0.4ng/ml, 79% demonstrate CP.
• PSA Working Group Definition:
>0.4ng/ml with one subsequent rise.
• This definition is the best predictor for later CP.

Low PSA after RRPLow PSA after RRP• PSA <0.29ng/ml has a low incidence of CP
• Possible:
– Recurrence of low-volume or indolent CaP.
– Benign PSA production.
• 61% of men with Benign positive margins will have detectable PSA(Djavan et.al.)

Natural History of BCRNatural History of BCR
No. BCRDefn
% BCR Yrs toBCR
% CP Yrs toCP
% PCSM Yrs toPCSM
Pound 1997 1X >0.2 15 (15yr) 3.5 34 (15yr) 8 18 (15yr) 13
D’Amico 1095 2X >0.2 33 (5yr)
Roehl 3478 2X >0.2 18 (10yr) 3.2 36 (10yr)
Jhaveri 1132 1X >0.2 19 (10yr) 1.9 26 (10yr)
Hull 1000 2X >0.4 15 (10yr) 23 (10yr)
Bianco 1746 1X >0.2 23 (10yr) 2.8 (10yr)
•Only 20-30% with BCR suffer CPOnly 20-30% with BCR suffer CP•<1/2 of these men with CP die of PC <1/2 of these men with CP die of PC

Natural History of BCRNatural History of BCR•1997 RRP at John Hopkins Hospital•304 had BCR•Development of CP depended on GS, time to recurrence and PSADT
•Equal risk of PCSM and other causes mortality.
•For Every 100 men treated with RRP•15-30 will develop BCR•2-6 will die from CaP

BCR and Risk PredictionBCR and Risk Prediction• Need to know
– 1. Severity of the disease.
– 2. Location of the disease.
Severity- Predicted by GS and Time to RecurrenceSeverity- Predicted by GS and Time to Recurrence
Gleason Score Time to RecurrenceGleason Score Time to RecurrenceFreedland et.al

PSA DT- Strong Predictor of PC DeathPSA DT- Strong Predictor of PC Death
• PSADT <3m associated with high death rate.
• There is however a chance of mortality at all doubling times.
Freedland et.al

AlgorithmsAlgorithms• Nomograms assist in evaluating multiple variables.
• Assess risk for developing CP and PCSM
Cancer Specific Survival BCR After RRP.Cancer Specific Survival BCR After RRP.
Pound et.al.

AlgorithmsAlgorithms
Cancer Specific Survival BCR After RRP. Cancer Specific Survival BCR After RRP.
Freedland et.al.

Localised or Systemic?Localised or Systemic?Options for Investigation:• Prostate Fossa Biopsy
– Poor sensitivity.• MRI
– High sensitivty for pelvic mass but not correlated with pathology.– Endorectal probe 95% sensitivity but at median PSA 2.18ng/ml
• CT scan • Bone Scan
– Median PSA (positive=158ng/ml), (negative= 11.3ng/ml)• Prostascint
– No difference in RT response to + and - scans• PET
– High false positive and image resolution problems

Localised or Systemic?Localised or Systemic?NomogramNomogram
Stephenson et.al

Estimating Life ExpectancyEstimating Life Expectancy• Important as patient may not be at risk of CP or PCSM
• Many ways of calculating, which incorporate age and co-morbidity.
• Nomogram by Cowen et.al.- 70% accuracy.

Salvage RadiotherapySalvage Radiotherapy• Response depends on likihood of local disease.
• Stephensen et.al. Nomogram (also flowchart)
• Katz et.al.
– Also found absence of SM+, absence of ECE and SVI+ as poor pronostic factors.
• Pazona- 5 yr PFS was 40%.
• Salvage RT dose range from 60Gy to 70Gy.
• 50% loss of potency
• No change in continence
• Higher BNC rate.

Hormonal TherapyHormonal Therapy• HT with CP (metastases) is well established.
• HT earlier is controversial (PSA only).
• No randomised trials (TOAD is on going in Australia)
• Moul et.al.: Early(MO) vs Late HT (M1) for BCR after RRP
– CP was delayed in men with GS>8 or PSADT <12m only.
– No difference in survival
Trial No. Defn Tx Stage Early Late Benefit
ECOG (Messing) 98 RP N1, MO 85% (OS) 63% (OS) Yes
MRC 934 None M0 30% (OS) 23% (OS) Yes
4 Other clinical trials show no benefit of early HT in MO diseaseEPC Trial showed higher risk of death with Casodex in Clinically Localised CaP
Do Not Use HT when Not NeededDo Not Use HT when Not Needed
• Hyperlipidaemia• Insulin Resistence• Decreased libido• Cognitive impairment• Osteoporosis
Acute Cardiovascular Events
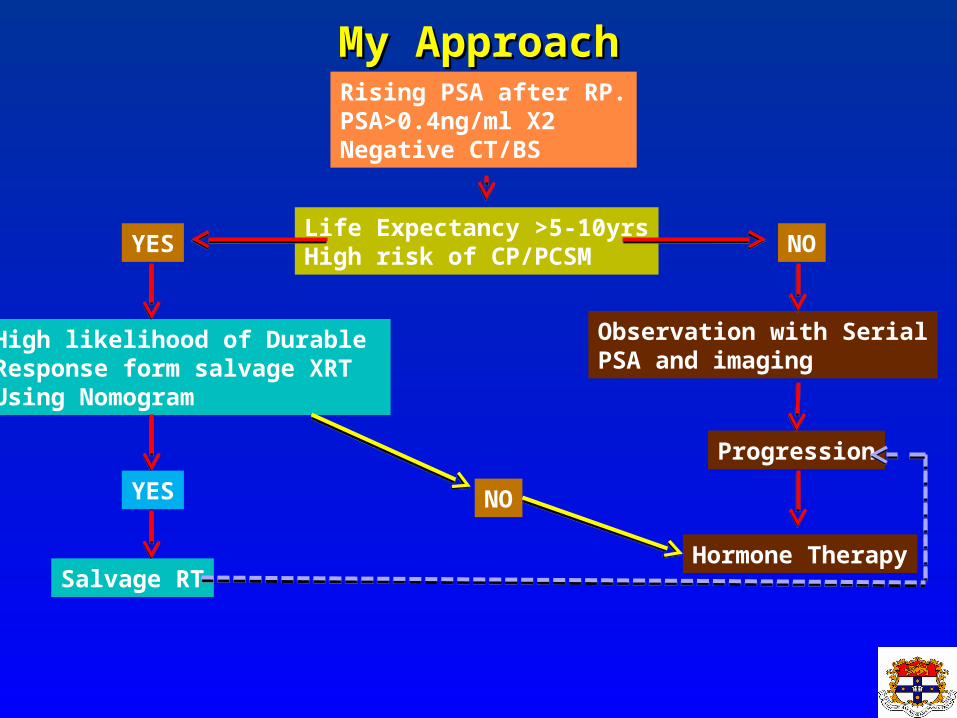
My ApproachMy ApproachRising PSA after RP.PSA>0.4ng/ml X2Negative CT/BS
Life Expectancy >5-10yrsHigh risk of CP/PCSMYES NO
High likelihood of Durable Response form salvage XRTUsing Nomogram
YES NO
Observation with SerialPSA and imaging
Progression
Hormone TherapySalvage RT