Embed Size (px)
Citation preview
ORIGINAL RESEARCH ARTICLE Open Access
Risk factors for chronic liver disease inpopulation of Central India: a case-controlstudy from rural IndiaShashank Banait1, Shailesh Mohan Badole2, Jyoti Jain3* and Abasaheb Thorat3
Abstract
Background: Chronic liver disease (CLD) is one of the leading causes of morbidity and mortality in today’s world.Common risk factors for CLD are alcohol, chronic hepatitis B, chronic hepatitis C, non-alcoholic steatohepatitis(NASH), malnutrition, toxins, and some tropical infections. This case-control study was carried out to determine therisk factors of domestic CLD in a resource-constrained setting in central rural India. A hospital-based matched case-control study was carried out among eligible CLD cases from November 2015 to October 2017. A total of 200 casesand 200 age- and gender-matched community controls were selected using consecutive sampling from tertiarycare hospitals from central rural India. Information on socio-demographic, etiological was collected through using apretested structured questionnaire after obtaining informed written consent. Univariate and multivariate analyseswere carried out to find the risk factors associated with CLD.
Results: The median age of study participant was 58.5 years among the cases. There were 75% male and remaining 25%were female in each case and control group. On multivariate analysis, we found less education, poor socioeconomic status,diabetes mellitus, increased body mass index (BMI), alcohol consumption, and tobacco chewing were significant risk factorsfor CLD in comparison to controls. However, amount of alcohol, smoking, and occupation were not found to be statisticallysignificant association with CLD.
Conclusions: The findings showed that in patients with CLD when compared to controls, high alcohol intake, diabetesmellitus, tobacco chewing, central obesity, low education, and low-income group are significant risk factors in our ruralpopulation. An initiative needs to be taken to reduce alcohol, and tobacco chewing habits at various levels throughawareness campaigns, strict control, and legislation to limit further abuse. Control of blood glucose and reduction of obesitymay be important in preventing CLD in our rural community.
Keywords: Alcohol, Chronic liver disease, Cirrhosis of liver, Non-alcoholic steatohepatitis, Risk factors
BackgroundChronic liver disease (CLD) is one of the leading causesof morbidity and mortality in today’s world [1]. It is in-creasingly becoming more prevalent, and part of this risecan be attributed to improved detection and opportunis-tic screening. Medical researchers are trying continu-ously to analyze this problem and searching for factors
that aid in its prevention. Although overall mortalityfrom CLD has shown a gradual decline over the lastthree to four decades, death rates within certain sub-groups have increased over time [2].The risk factors for CLD may vary in different popula-
tions. In developed countries, common risk factors are al-cohol, chronic hepatitis B, chronic hepatitis C, and NASH,while in developing countries, predominant causes of cir-rhosis are alcoholic, hepatitis B, hepatitis C, malnutrition,toxins, and some tropical infections are common. More-over, certain risk factors are likely to be region-specific
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
* Correspondence: [email protected] of Medicine, Mahatma Gandhi Institute of Medical Sciences,Sevagram, Wardha, Maharashtra, IndiaFull list of author information is available at the end of the article
Egyptian Liver JournalBanait et al. Egyptian Liver Journal (2021) 11:10 https://doi.org/10.1186/s43066-021-00077-9

such as sickle cell disease in population subgroups wherethis disease is prevalent. It is important to know risk fac-tors for CLD, so that there is a potential to prevent suchexposures. It is also important to know the risk factors inthe early stage of CLD, a period which is largelyasymptomatic.Many of the studies had been conducted among west-
ern population and very scanty knowledge is availablefrom Indian perspective and especially from rural area.Moreover, it has been observed that many individualsland up in the early stages of CLD with exposure to dif-ferent risk factors and their progression to the advancestages along with complications of the disease requiringmanagement at high cost and also increased risk of mor-tality. Thus, the present case-control study was carriedout to determine if patients of more than 18 years of agewith CLD have a higher exposure of risk factors as com-pared to age- and gender-matched community controlsin a resource-constrained setting in central rural India.
MethodsThis study was conducted in the Department of Medicineat Kasturba Hospital and Mahatma Gandhi Institute ofMedical Sciences (MGIMS), Sevagram, India. KasturbaHospital is a 920-bed rural teaching hospital of centralIndia affiliated to MGIMS. Every year this hospital pro-vides care to about 900,000 outpatients and 50,000 inpa-tients. We enrolled patients from inpatient settings in thisstudy. Department of Medicine also has an outreach pro-gram where trained social workers screen individuals inthe community for chronic diseases. Currently, this pro-gram runs in a total of 25 villages around our college. Thiscase-control study was conducted from 1 November 2015to 31 October 2017, after taking approval from the institu-tional ethics committee of MGIMS (IRB00003623). Weobtained a written informed consent from all study partic-ipants before enrolling them in the study.All patients aged 18 years and above admitted to the
Medicine wards in Kasturba Hospital, were screened andwith incident CLD were identified through a Hospital in-formation system.The diagnosis of CLD was based on the clinical profile,
ultrasonography (USG) abdomen, and biochemical pa-rameters. The cases were defined as those who have oneor more of the following evidence suggestive of CLD ir-respective of its etiology, i.e., hypoalbuminemia (serumalbumin level < 3.5 mg/dl) along with any clinical evi-dence of portal hypertension (variceal bleed, ascites withor without spontaneous bacterial peritonitis, or recov-ered from hepatic encephalopathy) and/or a diagnosticimaging of abdomen showing raised, altered echo-texture suggestive of fatty liver, chronic hepatitis, or cir-rhosis or biopsy result consistent with chronic hepatitisor cirrhosis [3].
Criteria for exclusion were non-cirrhotic portal fibro-sis, obvious focal liver disease (hydatid cysts, liver ab-scess, cholangiocarcinoma, hepatocellular carcinoma,and multiple metastasis. Cases not consenting to thestudy and not a resident of Wardha district were also ex-cluded. We enrolled consecutive inpatients with diagno-sis of CLD according to our inclusion and exclusioncriteria.We recruited 200 cases of CLD as per case definition
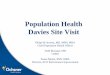
using consecutive sampling from our tertiary care hos-pital. Apparently, healthy controls with normal serum al-bumin levels, who are willing for participation in thestudy, were selected from the outreach service area andwere identified only after the case-selection was com-pleted. One healthy community-based control, frequencymatched with the case and was within 5 years of age,and of same gender as the case selected. The exclusioncriteria for controls were documented history of liverdisease in the past (Fig. 1).
Data collectionBaseline characteristics and clinical data were recordedfor all patients. All patients received the standard line ofmanagement for CLD. Patients with suspected CLDwere undergone hemogram, liver function test (LFT)[alanine transaminase (ALT), aspartate aminotransferase(AST), alkaline phosphatase, serum albumin, and globu-lin] in the central clinical laboratory. USG of the abdo-men to observe liver architecture, liver size, and featuresof portal hypertension (splenomegaly, ascites, and portalvein diameter) were done by using a Logic GE machineultrasound system, equipped with a 7.5 Megahertz(MHz) real-time, linear-array transducer B-mode scan-ner in patients of CLD by an experienced radiologist.Liver echo-texture was recorded as normal or coarse [4].
Measurement of risk factorsAll cases and controls were enquired about the potentialrisk factors of CLD through a semi-structured pre-codedand pre-tested questionnaire by the research investigator.The interviews were conducted in their local language(Marathi) from all cases and controls in the same manner.The risk factors we enquired into were classified and pre-sented into the following categories: demographic, socio-economic, anthropometric risk factors, occupational riskfactors, past-morbidity related risk factors, and recre-ational substance use and laboratory measures.BMI was calculated in all cases and control by the standard
method. It was considered as normal from 18.5 to 24.49,underweight < 18.49, obese ≥ 25-29.99, and overweight ≥ 30respectively. Blood pressure (BP) was measured in all casesand controls by Omron digital sphygmomanometer. Subjectswere assigned as hypertensive if systolic BP was ≥ 140mmHgor diastolic BP was ≥ 90mmHg [5].
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 2 of 9
History of occupations like automobile or paint indus-try (lead, solvents, and engine fumes), mining (silica andsand blasting), construction (cement, asbestos), chemicalindustry (solvents, chlorine, nitrous gasses), and farming(insecticides, grain dust) were enquired. History of vari-ous known and documented diseases was also obtainedfrom all cases and controls: diabetes mellitus, hyperten-sion (HT), or on antihypertensive drugs, history suggest-ive of rapid weight loss (loss of > 10% of body weightwithin 6 months period), intestinal bypass surgery, biliaryobstruction in past, polycystic liver disease, sickle celldisease and trait, known HIV infection.History of chronic recreational substance use [alco-
hol, smoking tobacco (cigarettes or bidis), tobacco orbeetle-nut chewing, intravenous or oral intake of a drugor abuse] with quantification was inquired among casesand controls [6, 7]. We also quantified alcohol intakeby asking type of alcohol, frequency, and averageamount of alcohol consumption and classified them asnever, current, and past (those who had given up drink-ing for 6 months or more) users. Patients were definedas having non-alcoholic fatty liver disease (NAFLD) ifthey have a history of consumption of alcohol < 20grams/day (g/day) [8–13]. Cases and controls were clas-sified as never smoker (not smoked cigarette or bidi forat least three months in a lifetime), current smoker(smoked at least one cigarette or bidi in the last threemonths), and former smoker (one who does not meetboth criteria).
Chronic consumption (˃ 3months) of medications suchas corticosteroids, methotrexate, amiodarone, methyldopaor herbal or folk remedies, or alternative medicine wasalso asked from all study participants.In addition, venous blood samples after a 12-h overnight
fast from all enrolled patients were collected for estima-tion of biochemical test. The collected sera were immedi-ately refrigerated till they were tested by a serologist whowas unaware of the clinical data of the patients. HepatitisB surface antigen (HbsAg) and anti-hepatitis C antibodiesqualitative detection (HCV) was done by rapid immuno-chromatographic assay. Venous blood samples trans-ported within 6 h to central laboratory of hospital for lipidpanel [total cholesterol, high-density lipoprotein choles-terol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG)] measurement by standard enzym-atic tests. Levels were considered abnormal if total choles-terol > 200mg/dl, LDL-C > 130mg/dl, TG > 150mg/dl,and HDL-C < 40mg/dl respectively. Random glucose andserum creatinine were also obtained on day 1 in all en-rolled participants.
Data management and analysisWe entered the data electronically by Microsoft Exceland analyzed by STATA software (Version 16, StataCorporation, TX, USA). We analyzed normally distrib-uted continuous variables by Student’s t test, proportionsby a chi-square test and continuous variables withskewed distribution by a Mann-Whitney test. We
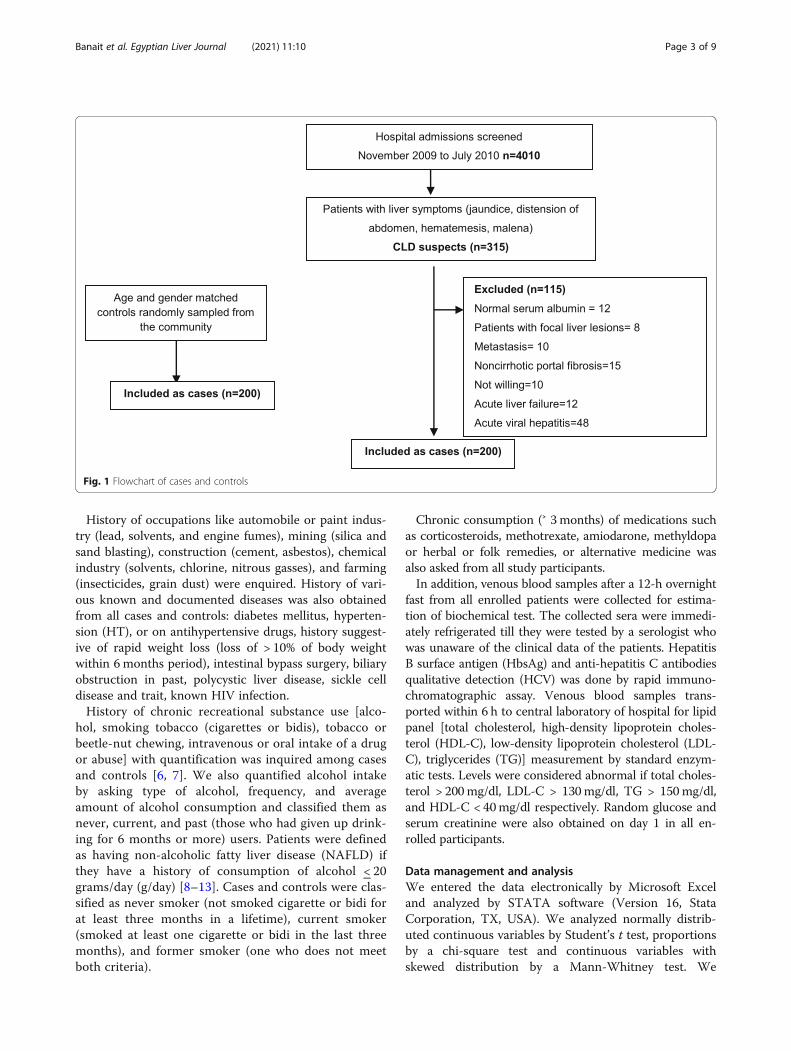
Fig. 1 Flowchart of cases and controls
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 3 of 9
considered a p value of less than 0.05 as significant.Exposure-related variables were included in the logisticregression analysis used in the multivariate model if theydisplayed a p value< 0.02 in the bivariate analysis. Wecalculated the odds ratios (ORs) as a measure of risk and95% confidence interval (CI) associated with the inde-pendent variables.
ResultsDuring the study, we screened 4010 consecutive patientswith symptoms of liver disease and found 315 clinicallysuspected CLD. Finally, 200 patients who had fulfilledone or more of the inclusion criteria suggestive of CLDwere included to the study, and 115 patients were ex-cluded (Fig. 1).The demographic and socioeconomic profile of the
study population is shown in Table 1. Matching couldachieve similar age and gender distribution among casesand controls. Among 200 cases and 200 controls, 150(75%) were males; with median age 58.5 ± 11.8 and 57 ±11.7 among cases and controls respectively. Majority ofthe study participants were in the age group of 41-65years contributing 72.5% among cases and 70% amongcontrols. Socioeconomic indicators and educational sta-tus were different statistically significant in patients withCLD when compared to controls with p value of 0.00001and 0.000004 respectively. Among cases and controlscommonest occupation was farming (60.8%); BMI was in
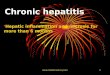
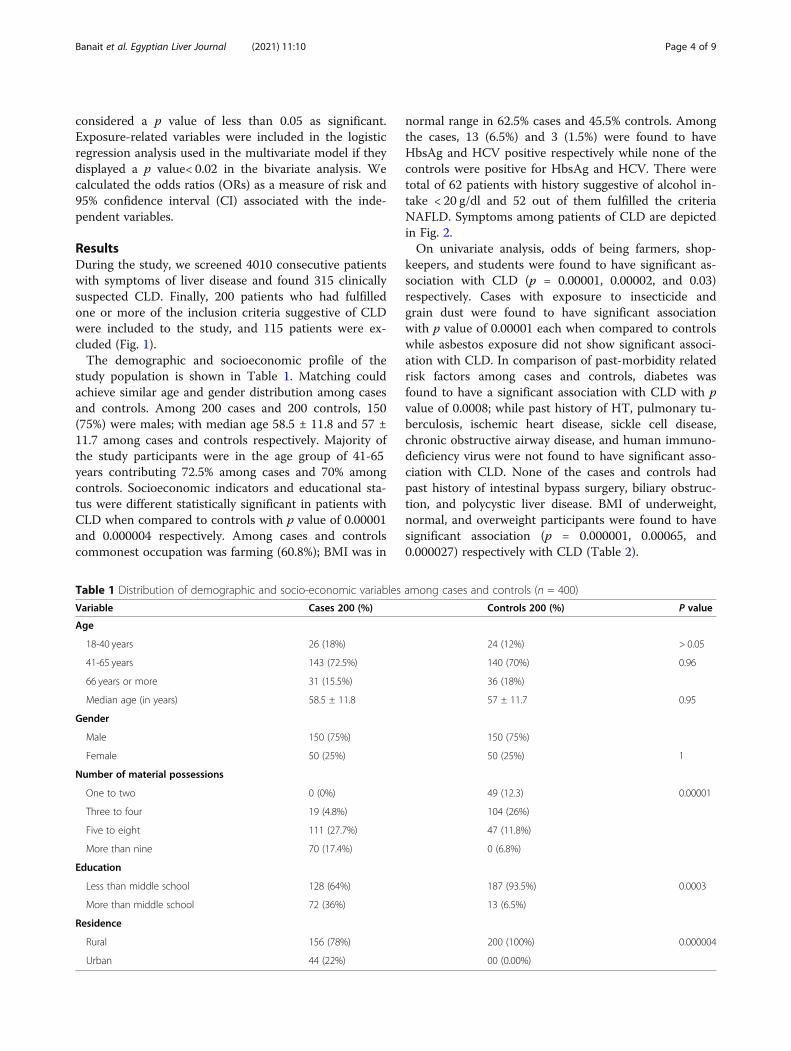
normal range in 62.5% cases and 45.5% controls. Amongthe cases, 13 (6.5%) and 3 (1.5%) were found to haveHbsAg and HCV positive respectively while none of thecontrols were positive for HbsAg and HCV. There weretotal of 62 patients with history suggestive of alcohol in-take < 20 g/dl and 52 out of them fulfilled the criteriaNAFLD. Symptoms among patients of CLD are depictedin Fig. 2.On univariate analysis, odds of being farmers, shop-
keepers, and students were found to have significant as-sociation with CLD (p = 0.00001, 0.00002, and 0.03)respectively. Cases with exposure to insecticide andgrain dust were found to have significant associationwith p value of 0.00001 each when compared to controlswhile asbestos exposure did not show significant associ-ation with CLD. In comparison of past-morbidity relatedrisk factors among cases and controls, diabetes wasfound to have a significant association with CLD with pvalue of 0.0008; while past history of HT, pulmonary tu-berculosis, ischemic heart disease, sickle cell disease,chronic obstructive airway disease, and human immuno-deficiency virus were not found to have significant asso-ciation with CLD. None of the cases and controls hadpast history of intestinal bypass surgery, biliary obstruc-tion, and polycystic liver disease. BMI of underweight,normal, and overweight participants were found to havesignificant association (p = 0.000001, 0.00065, and0.000027) respectively with CLD (Table 2).
Table 1 Distribution of demographic and socio-economic variables among cases and controls (n = 400)
Variable Cases 200 (%) Controls 200 (%) P value
Age
18-40 years 26 (18%) 24 (12%) > 0.05
41-65 years 143 (72.5%) 140 (70%) 0.96
66 years or more 31 (15.5%) 36 (18%)
Median age (in years) 58.5 ± 11.8 57 ± 11.7 0.95
Gender
Male 150 (75%) 150 (75%)
Female 50 (25%) 50 (25%) 1
Number of material possessions
One to two 0 (0%) 49 (12.3) 0.00001
Three to four 19 (4.8%) 104 (26%)
Five to eight 111 (27.7%) 47 (11.8%)
More than nine 70 (17.4%) 0 (6.8%)
Education
Less than middle school 128 (64%) 187 (93.5%) 0.0003
More than middle school 72 (36%) 13 (6.5%)
Residence
Rural 156 (78%) 200 (100%) 0.000004
Urban 44 (22%) 00 (0.00%)
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 4 of 9
On recreational substance abuse history ever use of al-cohol, smoking, and tobacco were found to have statisti-cally significant association with CLD with p value of(0.0000001, 0.0001, and 0.000027) respectively. Alcoholconsumption rate in g/day when compared betweengroups of 0 to 19 g/dl vs ˃ 20 g/day also showed significant(p = 0.00001) association with CLD. Hepatitis B was foundto have a significant association with CLD (p = 0.00025).On analysis of lipid profile, there was a significant associ-ation between having low total cholesterol and LDL withCLD, but with hypertriglyceridemia and low HDL, therewas no increased risk of CLD was found.Final model derived by multivariate logistic regression
suggested that the significant risk factors for CLD wereless education, poor socioeconomic status, diabetes mel-litus, increased BMI, alcohol consumption, and tobaccochewing. Significant risk factors for CLD derived by uni-variate and multivariate logistic regression by finalmodel are shown in Table 3.
DiscussionOur case-control study showed that less education, poorsocioeconomic status, diabetes mellitus, increased BMI,alcohol consumption, and tobacco chewing were risksignificant factors for CLD in comparison to controls.Some factors such as occupation, smoking, and hepatitisB were significant on univariate analysis, but when ad-justed for other risk factors were not found to be signifi-cant. Other known risk factors such as hepatitis C,hyperlipidemia, and HT were not found to be significantin our age and gender-matched case-control study.The median age of study participants in our study was
58.5 years among cases and 57 years in controls were
similar to various studies done on CLD patients; how-ever, male-female ratio was not similar as more maleswere found to have CLD in our study [14–16]. Thesedifferences might be due to predominance of alcohol in-take and health-seeking behavior among males in ourcommunity. Most of the study participants had educa-tion less than middle school which was 64% and 93.5%among cases and controls respectively, which was morethan the study done by Frieden et al., 52% cases and 54%controls with education less than middle school [17].This difference of education might be because of the se-lection of 78% cases and all controls from rural area withpoor socioeconomic status and underprivileged re-sources for higher education.Farmers, shopkeepers, and students were found to
have significant association with CLD while Zhang et al.reported farmers, laborers, and small businessmen asrisk factors for CLD [18].The results of our study showed diabetes as a signifi-
cant risk factor for CLD with 10% and 1% among casesand controls respectively while in retrospective study,diabetes was found in 23%, which was more than ourstudy [14].Among recreational substance abuse ever use of alco-
hol, smoking and tobacco were found to have statisti-cally significant association with CLD. Similar resultswere found by Lin et al. in their study [19]; however,Steffensen et al. found statistically significant associationof smoking only with CLD [20]. Our study showed thatthe amount of alcohol consumed and CLD are closelyassociated and results of our study were similar to thevarious studies [21, 22]. Coates et al. also concluded thatas the amount of alcohol per day increases, the risk of
Fig. 2 Symptoms and signs among the cases of chronic liver disease
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 5 of 9
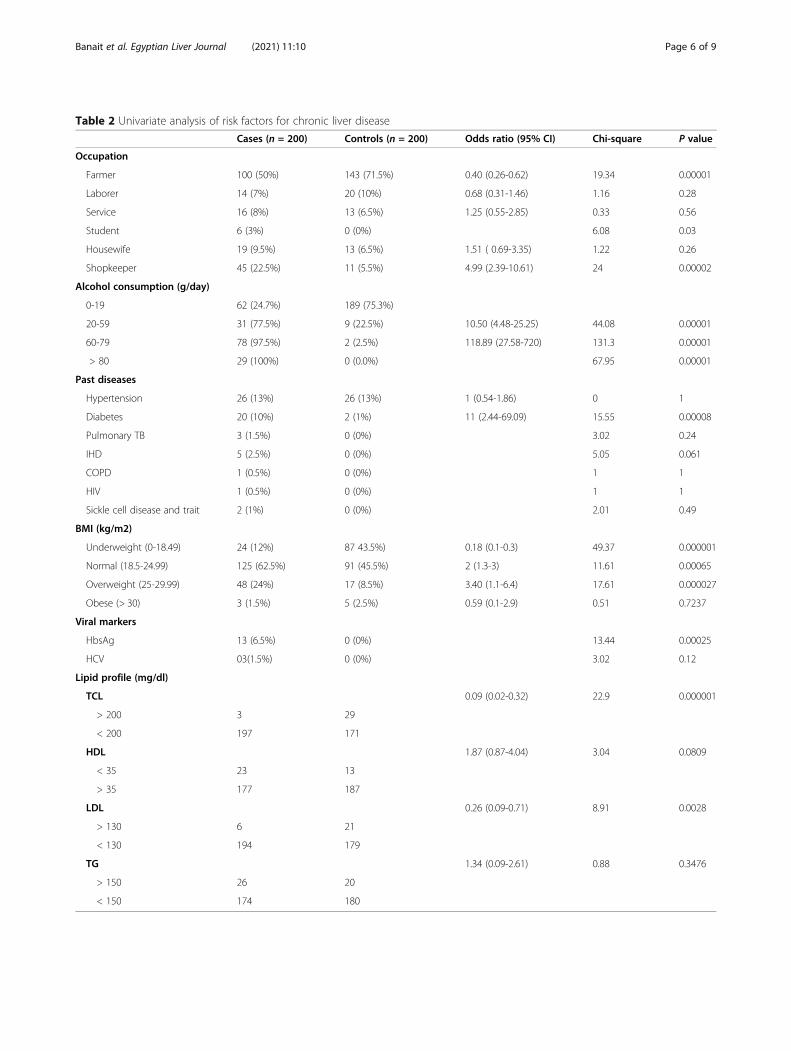
Table 2 Univariate analysis of risk factors for chronic liver disease
Cases (n = 200) Controls (n = 200) Odds ratio (95% CI) Chi-square P value
Occupation
Farmer 100 (50%) 143 (71.5%) 0.40 (0.26-0.62) 19.34 0.00001
Laborer 14 (7%) 20 (10%) 0.68 (0.31-1.46) 1.16 0.28
Service 16 (8%) 13 (6.5%) 1.25 (0.55-2.85) 0.33 0.56
Student 6 (3%) 0 (0%) 6.08 0.03
Housewife 19 (9.5%) 13 (6.5%) 1.51 ( 0.69-3.35) 1.22 0.26
Shopkeeper 45 (22.5%) 11 (5.5%) 4.99 (2.39-10.61) 24 0.00002
Alcohol consumption (g/day)
0-19 62 (24.7%) 189 (75.3%)
20-59 31 (77.5%) 9 (22.5%) 10.50 (4.48-25.25) 44.08 0.00001
60-79 78 (97.5%) 2 (2.5%) 118.89 (27.58-720) 131.3 0.00001
> 80 29 (100%) 0 (0.0%) 67.95 0.00001
Past diseases
Hypertension 26 (13%) 26 (13%) 1 (0.54-1.86) 0 1
Diabetes 20 (10%) 2 (1%) 11 (2.44-69.09) 15.55 0.00008
Pulmonary TB 3 (1.5%) 0 (0%) 3.02 0.24
IHD 5 (2.5%) 0 (0%) 5.05 0.061
COPD 1 (0.5%) 0 (0%) 1 1
HIV 1 (0.5%) 0 (0%) 1 1
Sickle cell disease and trait 2 (1%) 0 (0%) 2.01 0.49
BMI (kg/m2)
Underweight (0-18.49) 24 (12%) 87 43.5%) 0.18 (0.1-0.3) 49.37 0.000001
Normal (18.5-24.99) 125 (62.5%) 91 (45.5%) 2 (1.3-3) 11.61 0.00065
Overweight (25-29.99) 48 (24%) 17 (8.5%) 3.40 (1.1-6.4) 17.61 0.000027
Obese (> 30) 3 (1.5%) 5 (2.5%) 0.59 (0.1-2.9) 0.51 0.7237
Viral markers
HbsAg 13 (6.5%) 0 (0%) 13.44 0.00025
HCV 03(1.5%) 0 (0%) 3.02 0.12
Lipid profile (mg/dl)
TCL 0.09 (0.02-0.32) 22.9 0.000001
> 200 3 29
< 200 197 171
HDL 1.87 (0.87-4.04) 3.04 0.0809
< 35 23 13
> 35 177 187
LDL 0.26 (0.09-0.71) 8.91 0.0028
> 130 6 21
< 130 194 179
TG 1.34 (0.09-2.61) 0.88 0.3476
> 150 26 20
< 150 174 180
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 6 of 9

development of cirrhosis increases (at 40 to 59 g/day—relative risk 1.37, at 60 to 79 g/day—relative risk 4, at >80 g/day it was 50) [23].In our study on univariate analysis, hepatitis B was
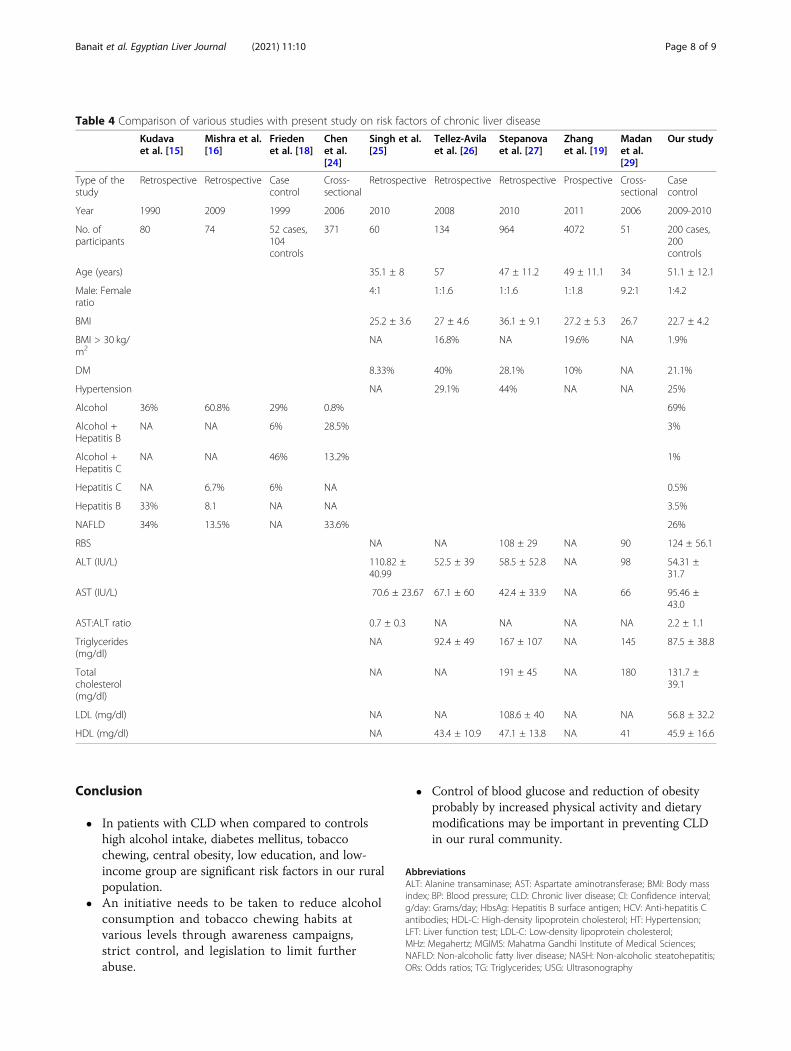
found statistically significant (p value 0.00025) withCLD, while hepatitis C was not found to be statisticallysignificant. In our study, the commonest probable reasonfor development of CLD was alcohol in 69% of the par-ticipants, while NAFLD and hepatitis B were found in26% and 7.5% respectively. Alcohol had been reported asthe most common probable reason for development ofCLD by various studies conducted in past [14, 15]. How-ever, Frieden et al. reported combination of alcohol andhepatitis C as the commonest probable reason for devel-opment of CLD followed by alcohol alone [17] (Table 4).Another study reported NAFLD as the commonestprobable reason for development of CLD followed bycombination of alcohol and hepatitis B [28]. These dif-ferences in our study with respect to other studies mightbe due to consumption of large amount, locally made al-cohol and nutritional deficient diet along with lowprevalent incidence of hepatitis B and C in our studysuggests that these sexually transmitted and blood-bornedisease were less among the cases either due to safe sexpractices or practice of universal safety precautions. Sig-nificant relationship between lipid level and developmentof NAFLD is found in various studies, but our study didnot revealed statistical significance between lipid levelsand NAFLD [18, 24–26, 29].In our study, BMI of participants was found to have signifi-
cant association with CLD, however, there was no significantassociation of BMI among NAFLD and non-NAFLD group.In a few studies, BMI > 25 was found to be significant in theNAFLD group [18, 27] (Table 4). These differences may bedue to involvement of rural population among our studywith poor socioeconomic status.On multivariate analysis, our study showed that less
education, poor socioeconomic status, diabetes mellitus,increased BMI, alcohol consumption, and tobacco chew-ing were significant risk factors for CLD in comparisonto controls.
This case-control study for risk factors of CLD is oneof the few from rural India, which has a different riskfactor profile as compared to urban areas, as well asfrom other developed countries. We used standard def-initions for classification of CLD and we performed anextensive literature search and have presented an up-dated review of CLD risk factor literature. The samplesize of the study population (200 cases and 200 con-trols) was adequate. Another strength of our study wasthat we have taken controls from the community ra-ther than from the hospital. Our study has certain limi-tations also. First, is selection bias. Although thecontrol sampling was from community, numerically ahigher proportion of controls per case would have im-proved the risk factor profile among controls. Second,is information bias. History aims to capture presenceof risk factors prior to onset of CLD. When the onsetof disease is uncertain, it remains difficult to ascertainif risk factors were really present prior to onset of dis-ease. Further, information bias could also result due tointerviewer bias, as the interviewer is unblinded to thecase and control status of individuals. Third, case-control study design has some inherent limitations,such as inability to prove a temporal association be-tween presence of a risk factor and outcome. Furthercontrol selection depends on some assumptions suchas the prevalence of risk factors in controls represent-ing the community as a whole, which might not havebeen adequately addressed in the study design. Lastly,we did not study risk factors such as history of bloodtransfusion and unsafe sex in our study. Our patientsbeing from rural background do not disclose theirsex-related issues clearly, so we thought not to in-clude this variable as a risk factor; however, we havetested all the study participants for hepatitis B andhepatitis C.Despite these limitations, the current study clearly de-
lineates what may be the priorities in terms of risk re-duction for CLD as alcohol, hepatitis, and NAFLD areclear-cut risk factors which may be associated with de-velopment for CLD.
Table 3 Multivariate conditional logistic regression of risk factors for chronic liver disease
Odds ratio 95% C.I. Coefficient S. E. Z statistic P value
Alcohol consumption rate (g/day) 27.41 5.6-133.16 3.3109 0.8065 4.1054 0.0001
BMI (kg/m2) 3.61 1.5-8.71 1.2848 0.4489 2.8623 0.0042
Diabetes mellitus (RBS < 200 or > 200mg/dl) 24.11 1.2-472.48 3.1827 1.5181 2.0965 0.0360
Education (< middle school or > middle school) 12.35 2.4-63.31 2.5140 0.8338 3.0152 0.0026
Smoking (ever use) 0.43 0.09-2.084 −0.8372 0.8020 −1.0439 0.2965
Tobacco (ever use) 7.48 1.46-38.4075 2.0127 0.8345 2.4120 0.0159
Material possession 0.11 0.01-0.8209 2.2363 1.0403 2.1497 0.0316
Occupation 0.96 0.63-1.4695 0.0401 0.2168 0.1850 0.8532
Final-2*Log-Likelihood: 46.9463
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 7 of 9
Conclusion
� In patients with CLD when compared to controlshigh alcohol intake, diabetes mellitus, tobaccochewing, central obesity, low education, and low-income group are significant risk factors in our ruralpopulation.
� An initiative needs to be taken to reduce alcoholconsumption and tobacco chewing habits atvarious levels through awareness campaigns,strict control, and legislation to limit furtherabuse.
� Control of blood glucose and reduction of obesityprobably by increased physical activity and dietarymodifications may be important in preventing CLDin our rural community.
AbbreviationsALT: Alanine transaminase; AST: Aspartate aminotransferase; BMI: Body massindex; BP: Blood pressure; CLD: Chronic liver disease; CI: Confidence interval;g/day: Grams/day; HbsAg: Hepatitis B surface antigen; HCV: Anti-hepatitis Cantibodies; HDL-C: High-density lipoprotein cholesterol; HT: Hypertension;LFT: Liver function test; LDL-C: Low-density lipoprotein cholesterol;MHz: Megahertz; MGIMS: Mahatma Gandhi Institute of Medical Sciences;NAFLD: Non-alcoholic fatty liver disease; NASH: Non-alcoholic steatohepatitis;ORs: Odds ratios; TG: Triglycerides; USG: Ultrasonography
Table 4 Comparison of various studies with present study on risk factors of chronic liver disease
Kudavaet al. [15]
Mishra et al.[16]
Friedenet al. [18]
Chenet al.[24]
Singh et al.[25]
Tellez-Avilaet al. [26]
Stepanovaet al. [27]
Zhanget al. [19]
Madanet al.[29]
Our study
Type of thestudy
Retrospective Retrospective Casecontrol
Cross-sectional
Retrospective Retrospective Retrospective Prospective Cross-sectional
Casecontrol
Year 1990 2009 1999 2006 2010 2008 2010 2011 2006 2009-2010
No. ofparticipants
80 74 52 cases,104controls
371 60 134 964 4072 51 200 cases,200controls
Age (years) 35.1 ± 8 57 47 ± 11.2 49 ± 11.1 34 51.1 ± 12.1
Male: Femaleratio
4:1 1:1.6 1:1.6 1:1.8 9.2:1 1:4.2
BMI 25.2 ± 3.6 27 ± 4.6 36.1 ± 9.1 27.2 ± 5.3 26.7 22.7 ± 4.2
BMI > 30 kg/m2
NA 16.8% NA 19.6% NA 1.9%
DM 8.33% 40% 28.1% 10% NA 21.1%
Hypertension NA 29.1% 44% NA NA 25%
Alcohol 36% 60.8% 29% 0.8% 69%
Alcohol +Hepatitis B
NA NA 6% 28.5% 3%
Alcohol +Hepatitis C
NA NA 46% 13.2% 1%
Hepatitis C NA 6.7% 6% NA 0.5%
Hepatitis B 33% 8.1 NA NA 3.5%
NAFLD 34% 13.5% NA 33.6% 26%
RBS NA NA 108 ± 29 NA 90 124 ± 56.1
ALT (IU/L) 110.82 ±40.99
52.5 ± 39 58.5 ± 52.8 NA 98 54.31 ±31.7
AST (IU/L) 70.6 ± 23.67 67.1 ± 60 42.4 ± 33.9 NA 66 95.46 ±43.0
AST:ALT ratio 0.7 ± 0.3 NA NA NA NA 2.2 ± 1.1
Triglycerides(mg/dl)
NA 92.4 ± 49 167 ± 107 NA 145 87.5 ± 38.8
Totalcholesterol(mg/dl)
NA NA 191 ± 45 NA 180 131.7 ±39.1
LDL (mg/dl) NA NA 108.6 ± 40 NA NA 56.8 ± 32.2
HDL (mg/dl) NA 43.4 ± 10.9 47.1 ± 13.8 NA 41 45.9 ± 16.6
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 8 of 9

AcknowledgementsNot applicable.
Authors’ contributionsSB contributed to the design and implementation of the research,contributed to the revision of the work, and the acceptance of the final formof the manuscript. 2-SMB contributed to the design and implementation ofthe research, aided in choosing the patients and helped shape the research,supervised the findings of this work, and discussed the results. 3-JJ formu-lated the research idea, contributed to the design and implementation ofthe research, contributed in the collection of the data, and in performing thestatistical part of the work. 4-AST contributed to the design and implementa-tion of the research and performed the laboratory work. All authors providedcritical feedback and helped shape the research, analysis, and manuscript. Allauthors have read and approved the final manuscript.
FundingNot applicable.
Availability of data and materialsAll data used and/or analyzed during the current study are available fromthe corresponding author on reasonable request.
Ethics approval and consent to participateAll subjects involved in the study signed an informed written consent toparticipate. This study was performed in accordance with the standards ofthe ethical research committee of MGIMS, Sevagram (reference number:IRB00003623).
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1Department of Ophthalmology, JNMC Sawangi, Wardha, Maharashtra, India.2DNB Neurology, Russh Super Speciality Hospital, Hyderabad, Telangana,India. 3Department of Medicine, Mahatma Gandhi Institute of MedicalSciences, Sevagram, Wardha, Maharashtra, India.
Received: 14 October 2020 Accepted: 7 January 2021
References1. Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B (2009)
Deaths: final data for 2006. Natl Vital Stat Rep 57:1–1342. Vong S, Bell BP (2004) Chronic liver disease mortality in the United States,
1990-1998. Hepatology 39:476–4833. Harriman S.A (1999) New country liver study. State of Connecticut,
Department of Public Health 2–74. Bruneton JN. Diagnostic ultrasound, Carol M. Rumack, Stephanie R. Wilson,
JW Charbonneau, J-. AM Johnson (Eds.), Elsevier/Mosby, Philadelphia, PA(2005), Volume 1: chapter 4,pages 77
5. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, JonesDW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ (2003) Seventh report ofthe Joint National Committee on Prevention, Detection, Evaluation, andTreatment of High Blood Pressure. Hypertension 42:1206–1252
6. Reynolds K, Lewis B, Nolen JD, Kinney GL, Sathya B, He, J. (2003) Alcoholconsumption and risk of stroke: a meta-analysis. JAMA 289:579–588
7. DR ALA ALWAN, ASSISTANT DIRECTOR-GENERAL, NONCOMMUNICABLEDISEASES AND MENTAL HEALTH & WORLD HEALTH ORGANIZATION 2011.Global status report on alcohol and health, WHO Report 2011. In:NONCOMMUNICABLE DISEASES AND MENTAL HEALTH & ORGANIZATION,W. H. (eds.)
8. Adams LA, Angulo P, Lindor KD (2005) Nonalcoholic fatty liver disease.CMAJ 172:899–905
9. Sanyal AJ, Campbell-Sargent C, Mirshahi F, Rizzo WB, Contos MJ, Sterling RK,Luketic VA, Shiffman ML, Clore JN (2001) Nonalcoholic steatohepatitis:association of insulin resistance and mitochondrial abnormalities.Gastroenterology 120:1183–1192
10. CHOI SS, DIEHL AM (2008) Hepatic triglyceride synthesis and nonalcoholicfatty liver disease. Curr Opin Lipidol 19:295–300
11. Mccullough AJ (2002) Update on nonalcoholic fatty liver disease. J ClinGastroenterol 34:255–262
12. Das K, Kar P (2005) Non-alcoholic steatohepatitis. J Assoc Physicians India53:195–199
13. Wanless IR, Lentz JS (1990) Fatty liver hepatitis (steatohepatitis) and obesity:an autopsy study with analysis of risk factors. Hepatology 12:1106–1110
14. Kudva MV, Zawawi MM (1990) Chronic liver disease in Kuala Lumpur,Malaysia: a clinical study. Singapore Med J 31:368–373
15. Mishra AK, SP, Bista NR, Bhurtel P, Bhattarai S, Thakali K, Banthia P, Pathak SR(2009) Pattern of liver diseases. J Nepal Health Res Council 7:14–18
16. Corrao G, Arico S (1998) Independent and combined action of hepatitis Cvirus infection and alcohol consumption on the risk of symptomatic livercirrhosis. Hepatology 27:914–919
17. Frieden TR, Ozick L, Mccord C, Nainan OV, Workman S, Comer G, Lee TP,Byun KS, Patel D, Henning KJ (1999) Chronic liver disease in central Harlem:the role of alcohol and viral hepatitis. Hepatology 29:883–888
18. Zhang H, Jiang YF, He SM, Sun J, Gu Q, Feng XW, Du B, Wang W, Shi XD,Wang CY, Zhang SQ, Li WY, Niu JQ (2011) Etiology and prevalence ofabnormal serum alanine aminotransferase levels in a general population inNortheast China. Chin Med J (Engl) 124:2661–2668
19. Lin HH, Wang LY, Shaw CK, Cheng ML, Chung WK, Chiang HJ, Lin TY, ChenCJ (2002) Combined effects of chronic hepatitis virus infections andsubstance-use habits on chronic liver diseases in Taiwanese aborigines. JFormos Med Assoc 101:826–834
20. Steffensen FH, Sorensen HT, Brock A, Vilstrup H, Lauritzen T (1997) Alcoholconsumption and serum liver-derived enzymes in a Danish population aged30-50 years. Int J Epidemiol 26:92–99
21. Tuyns AJ, Pequignot G (1984) Greater risk of ascitic cirrhosis in females inrelation to alcohol consumption. Int J Epidemiol 13:53–57
22. Lau K, Freyer-Adam J, Coder B, RIEDEL J, Rumpf HJ, John U, Hapke U (2008)Dose-response relation between volume of drinking and alcohol-relateddiseases in male general hospital inpatients. Alcohol Alcohol 43:34–38
23. Coates RA, Halliday ML, Rankin JG, Feinman SV, Fisher MM (1986) Risk offatty infiltration or cirrhosis of the liver in relation to ethanol consumption: acase-control study. Clin Invest Med 9:26–32
24. Tellez-Avila FI, Sanchez-Avila F, Garcia-Saenz-de-Sicilia M, Chavez-Tapia NC,Franco-Guzman AM, Lopez-Arce G, Cerda-Contreras E, Uribe M (2008)Prevalence of metabolic syndrome, obesity and diabetes type 2 incryptogenic cirrhosis. World J Gastroenterol 14:4771–4775
25. Stepanova M, Aquino R, Alsheddi A, Gupta R, Fang Y, Younossi Z (2010)Clinical predictors of fibrosis in patients with chronic liver disease. AlimentPharmacol Ther 31:1085–1094
26. Singh DK, Rastogi A, Sakhuja P, Gondal R, Sarin SK (2010) Comparison ofclinical, biochemical and histological features of alcoholic steatohepatitisand non-alcoholic steatohepatitis in Asian Indian patients. Indian J PatholMicrobiol 53:408–413
27. Marchesini G, Bugianesi E, Forlani G, Cerrelli F, Lenzi M, Manini R, Natale S,Vanni E, Villanova N, Melchionda N, Rizzetto M (2003) Nonalcoholic fattyliver, steatohepatitis, and the metabolic syndrome. Hepatology 37:917–923
28. Chen CH, Huang MH, Yang JC, Nien CK, Yang CC, Yeh YH, Yueh SK (2007)Prevalence and etiology of elevated serum alanine aminotransferase level inan adult population in Taiwan. J Gastroenterol Hepatol 22:1482–1489
29. Madan K, Batra Y, Gupta SD, Chander B, Rajan KD, Tewatia MS, Panda SK,Acharya SK (2006) Non-alcoholic fatty liver disease may not be a severedisease at presentation among Asian Indians. World J Gastroenterol 12:3400–5
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Banait et al. Egyptian Liver Journal (2021) 11:10 Page 9 of 9