Embed Size (px)
Citation preview

2
tptf
N
f
1h
Original article
Risk of renal cell carcinoma and polymorphism in phase I xenobioticmetabolizing CYP1A1 and CYP2D6 enzymes�
Shiekh Tanveer Ahmad, M.Sc.a, Wani Arjumand, M.Sc.a,Amlesh Seth, M.B.B.S., D.N.B., M.Ch.b, Sana Nafees, M.Sc.a, Summya Rashid, M.Sc.a,Nemat Ali, M.Sc.a, Oday O. Hamiza, B.V.Sc., M.Sc.a, Sarwat Sultana, M.Sc., Ph.D.a,*
a Section of Molecular Carcinogenesis and Chemoprevention, Department of Medical Elementology and Toxicology, Faculty of Science, Jamia Hamdard(Hamdard University), New Delhi, India
b Department of Urology, All India Institute of Medical Sciences, New Delhi, India
Received 17 October 2011; received in revised form 8 December 2011; accepted 9 December 2011
Abstract
The progressive increase in sporadic renal cell carcinoma (RCC) observed in industrialized countries supports the opinion that certaincarcinogens present in the environment (tobacco smoke, drugs, pollutants, and dietary constituents) may affect the occurrence andprogression of this disease in developing countries like India. The polymorphism of the enzymes involved in metabolism of suchenvironmental factors may, therefore, confer variable propensity to RCC. The possible association between RCC and a polymorphism ofthe CYP1A1 and CYP2D6 genes specific to the Indian population was examined using peripheral blood DNA from 196 RCC cases and 250population controls with detailed data of clinicopathologic characteristics for the disease. The CYP1A1 (val) “variant” genotype, whichcontains at least 1 copy of the CYP1A1 variant alleles, was found to be associated with a 2.03-fold [GG ver. AA/AG, unadjusted OR �.03; 95%CI � 1.233–3.342; P � 0.005] increase in the risk of RCC. There was also a significant association (ptrend � 0.034) between
higher frequency of RCC subjects containing at least of copy of the CYP1A1 (val) “variant” genotype with III or IV Fuhrman’s grade.Whereas, the CYP2D6 polymorphism did not show any association with RCC risk [TT ver. CT/CC, unadjusted OR � 95%CI �1.233–3.342; P � 0.005]. There was a significant association (ptrend � 0.001) between the poor metabolizer CYP2D6 (TT) and progressionowards higher pathological stage of RCC. Our data demonstrate for the first time a significant association between pharmacogeneticolymorphisms of CYP1A1 and risk of RCC development in the Indian population. The findings suggest that inter-individual variation inhe phase I metabolic enzymes involved in the fictionalization and detoxification of specific xenobiotics is an important susceptibility factoror development and progression of RCC in Indians. © 2013 Elsevier Inc. All rights reserved.
Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
Keywords: CYP1A1; CYP2D6; Xenobiotic metabolizing enzyme; Renal cell carcinoma; AJCC cancer stage; Fuhrman’s grade
acrrvaemRbam
1. Introduction
Kidney cancer is among the ten most frequently occur-ring cancers in Western communities. Globally, about270,000 cases of kidney cancer are diagnosed yearly and116,000 people die from the disease [1]. In India in the year2010, there were an estimated 9,333 incidences and 6,049mortalities due to kidney cancer [2]. Approximately 90% of
� S.S. is thankful to the Indian Council of Medical Research (ICMR),ew Delhi, India for providing the funds to carry out this research work.
* Corresponding author. Tel.: �0091-11-26054685 ext: 5565/5566;ax: �0091-11-26059663.
aE-mail address: [email protected] (S. Sultana).
078-1439/$ – see front matter © 2013 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.urolonc.2011.12.009
all kidney cancers are renal cell carcinomas (RCC) [1]. Therere a number of evidences that indicate the development of theancers is the result of both cumulative effect of environmentalisk factors and genetic makeup of the individual. The envi-onment–gene interaction in carcinogenesis is also well re-ealed by metabolic enzymes involved in the inactivationnd/or detoxification of environmental carcinogens. Variouspidemiologic studies have shown that dietary and environ-ental factors may be involved in the development of sporadicCC [3]. Most of the carcinogens are metabolically inactivatedy detoxification enzymes [4]. Therefore, inherited set of vari-tions in genes encoding the carcinogen metabolizing enzymesay alter enzymatic activity and subsequently the carcinogen
ctivation and/or deactivation.

1351S.T. Ahmad et al. / Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
In the present study we have studied the genetic varia-tions within 2 important cytochrome P450 1A1 (CYP1A1)and cytochrome P450 2D6 (CYP2D6) biotransformationenzymes and their association with the development andprogression of RCC. These enzymes, involved in the me-tabolism of substances that are thought to be carcinogenic,are believed to participate in a variety of tumor formationprocesses [3]. Cytochrome P450s (CYP450) are phase-Ibiotransformation enzymes, and these enzymes play a keyrole in the metabolism of drugs, environmental chemicalsincluding food contaminants, as well as endogenous sub-stances. CYP450s metabolically activate procarcinogenssuch as polycyclic aromatic hydrocarbons (PAHs) and N-nitrosamines to reactive and genotoxic intermediates [5,6].These intermediates are capable of binding covalently toDNA to form DNA adducts, thereby potentially initiatingthe carcinogenic process.
CYP1A1 activates polycyclic aromatic hydrocarbons,such as those found in cigarette smoke [3]. In CYP1A1, abase substitution of adenine to guanine at position 2455 inthe heme-binding region of exon 7 results in an isoleucine tovaline amino acid substitution at codon 462 (Ile462Val).The valine allele, designated CYP1A1*2C following theinitial trivial designation of CYP1A1 m2, correlates withincreased enzymatic activity [7], thought to lead to greatercarcinogen susceptibility and consequently higher risk ofdeveloping cancer. CYP2D6 metabolizes many clinicallyimportant drugs and procarcinogens, such as a tobacco-specific nitrosamine, 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone [3]. CYP2D6 is one of the best studied cyto-chrome P450 enzymes with regard to its association withcancer risk. Ethnicity is an important contributing factor inthe occurrence of CYP2D6 variability. Among the differentvariants, the detrimental mutation of the CYP2D6 gene isC188T, causing a Pro34Ser amino acid substitution in thehighly conserved region. This substitution results in lowerCYP2D6 stability and, thus, decreased enzymatic activity[8]. There are large numbers of epidemiologic studies per-formed in different ethnic populations regarding the asso-ciation of CYP1A1 (Ile462Val) and CYP2D6 (Pro34Ser)polymorphism with cancer risk, but their results are contra-dicting.
In the case of RCC, there are a very limited number ofstudies available in the literature, which have investigatedthe role of above mentioned genetic variants of CYP 450s inthe risk of cancer development and progression. The rapidlygrowing population and economic development is causing anumber of environmental issues in India because of the un-controlled growth of urbanization and industrialization, expan-sion, and massive intensification of agriculture and the defor-estation. Indian cities, particularly in the capital city of Delhi,are full of environmental toxicants of anthropogenic nature;therefore, people living there and the adjacent states are likelyto get exposed to variety of environmental toxicants, includingvarious potential procarcinogens. Thus, the fate of these pro-
carcinogens may depend upon gene–environment interactionamong the Indian population residing in Delhi and nearbyareas and may ultimately may serve as a vital determinant ofsusceptibly to renal carcinogenesis. To best of our knowledge,the association between the polymorphism of CYP1A1 andCYP2D6 gene and RCC risk has not been studied in the Indianpopulation to date. This study investigated the association ofgenetic variants of phase I xenobiotic metabolizing with risk ofRCC development and progression.
2. Materials and methods
2.1. Subjects
The present case-control study was carried out fromDecember 2008 to February 2011. In this study, a total of196 (138 males and 58 females) newly diagnosed RCCpatients from the North Indian population (from the states ofDelhi and bordering states) registered in the Department ofUrology, All India Institute of Medical Sciences (AIIMS),New Delhi, India were recruited. Patients were recruitedafter radiologic and histologic diagnosis of renal cell carci-noma. Histologic subtyping revealed that there were 176(89.8%) clear cell RCC, 14 (7.1%) papillary RCC, 4 (2%)chromophobe RCC, and 2 (1%) transitional cell RCC cases.The control group included 250 healthy volunteers (172men and 78 women), chosen at the same time, who werefree of any chronic diseases, having no history of anycancer, and living in the same geographic area. They werematched with cases in age and gender. Smoking, hyperten-sion, and body mass index (BMI) were also evaluated dur-ing the recruitment of cases and controls by means of apatient case record form and a questionnaire, respectively.Histopathologic staging and grading were done after ne-phrectomy and followed the tumor-node-metastasis (TNM)classification of the American Joint Committee on Cancer(AJCC), 6th edition [9]. All patients received a patientinformation sheet and signed a consent form, approved bythe Institutional Committee on Human Ethics (ICHE pro-posal no. P-18/1.09.08). Likewise, controls received a vol-unteer information sheet and signed consent. About 5 ml ofperipheral blood was collected from both the patients andhealthy volunteers for DNA extraction and then processedfor genotyping. To validate the findings of PCR-RFLP, theanalysis of all the mutant homozygous samples and 20% ofheterozygotes were duplicated and confirmed by direct se-quencing with 100% concordance.
2.2. DNA isolation
Genomic DNA samples were obtained from blood lym-phocytes using a genomic DNA extraction kit (BioserveBiotechnologies Pvt. Ltd., Hyderabad, Andhra Pradesh, In-dia). Isolated DNA was resuspended in Tris EDTA buffer
(pH 8.0) and stored at �20°C until use.
(ari5AC1S5w6ere
2
bc[i
N
tme
sf
1352 S.T. Ahmad et al. / Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
2.3. CYP1A1 genotyping
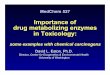
The CYP1A1 (A2455G or rs1048943) genotyping wasassayed using an allele-specific PCR method previouslydescribed by Chan et al. [10]. Two oligonucleotide primers1A and 2G), complementary at the 3=end for the A and Glleles, respectively, were used as reverse primers in sepa-ate PCR reactions. A common forward primer (3) was usedn each reaction. The sequences of the primers were: (1A)-AAG ACC TCC CAG CGG GCA AT-3; (2G) 5-AAGCC TCC CAG CGG GCA AC; (3) 5-GAA CTG CCATT CAG CTG TCT-3. Each reaction (25 �l) contained.25 mM MgCl2, 240 �M dNTPs and 1U Taq polymerase.amples were subjected to an initial denaturation period ofminutes at 94°C before the addition of polymerase. Thisas followed by 35 thermal cycles of 94°C for 45 seconds,4 °C for 45 seconds, and 72°C for 35 seconds. A finalxtension period of 5 minutes at 72°C completed the PCReaction. PCR products were detected using 2% agarose gellectrophoresis (Fig. 1).
.4. CYP2D6 genotyping
The CYP2D6 (C188T) polymorphisms were determinedy PCR and restriction fragment length polymorphism ac-ording to the method of Luo et al. with some modifications4]. The PCR amplification was carried out with 50 ng DNAn 10 mM Tris-HCl, pH 8.3, 50 mM KCl, 1.5 mM MgCl2,
0.3 mM deoxyribonucleotide triphosphates (Fermentas LifeSciences, Inc.), 200 ng of each primer, and 1.0 U of Taqpolymerase (Fermentas Life Sciences, Inc.) in a total vol-ume of 25 �l. Amplification was performed with an initialdenaturation step at 95°C for 12 minutes, followed by 35cycles at 94°C for 30 seconds, 62°C for 30 seconds, 72°Cfor 45 seconds, and a final extension at 72°C for 10 minutes.
The amplification product (20 �l) was digested with 5Uof KpnI (New England Biolabs, Beverly, MA) in 50 mM
aCl, 10 mM Tris-HCl, 10 mM MgCl2, and 1 mM dithio-
Fig. 1. Representative photomicrograph of agarose gel electrophoresis ofASO-PCR of CYP1A1 (A2455G). P1, P2, P3, P4, P5, and P6 representsthe patients, whereas, (A) represents A allele; (G) represents G allele of the
Icorresponding patients.
hreitol, and then incubated at 37°C for 4 hours. The frag-ent lengths were analyzed on a 3.5% agarose gel with
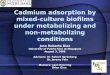
thidium bromide (0.5 �g/ml). When KpnI restriction sitewas present, the fragment of 210 bp was digested into 2lengths of 180 and 30 bp. Electrophoresis of the digestedPCR products (Fig. 2) showed individuals homozygousmutant (TT or Ser/Ser) for the CYP2D6 KpnI polymor-phism as 1 band of 210 bp. Heterozygous mutant (Pro/Ser)for the polymorphism showed 3 bands of 210, 180, and 30.Homozygous wild (Pro/Pro) showed 2 bands of 180 and 30bp. Previously sequenced samples were used as negativeand positive controls to rule out possible genotyping errors.
2.5. Statistical analysis
Differences in genotypic frequencies of CYP1A1 andCYP2D6 variants between the RCC cases and the controlsubjects were studied. The �2 test was performed to verifywhether control genotypic distribution was following Har-dy-Weinberg law of equilibrium. The associations betweenthe genotypes and the clinicopathologic characteristics atthe time of diagnosis of the RCC patients were also assessedfor statistical significance using the �2 test (Fisher’s exacttest when expected frequencies were small) and �2 test fortrend. Odds ratio at 95% confidence intervals (95% CI) andP values were computed by binary logistic regression, andall results were adjusted for age, gender, hypertension,smoking, and BMI. The independent sample Student’s t-testwas applied to check association between cases and con-trols. The P values � 0.05 were considered to indicatetatistical significance in these tests. All analyses were per-ormed using the statistical package SPSS ver. 16 (SPSS
Fig. 2. Representative photomicrograph of agarose gel electrophoresis ofPCR-RFLP of CYP2D6 (C188T). Individuals with homozygous mutant(TT or Ser/Ser) for the CYP2D6 KpnI polymorphism show one band of210 bp, heterozygous mutant (Pro/Ser) show 3 bands of 210, 180, and 30,and homozygous wild (Pro/Pro) show 2 bands of 180 and 30 bp.
nc., Chicago, IL).

1353S.T. Ahmad et al. / Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
3. Results
3.1. Association of clinicopathologic parameters withRCC risk
Exposures associated with increased RCC risk includedsmoking, high BMI, and hypertension as mentioned inTable 1. Demographic characteristics and exposure historiesof cases and controls were similar. We examined 196 casesand 250 controls for GSTP1, GSTT1, and GSTM1 geno-typing. We performed Pearson’s �2 test of our control pop-ulation for CYP1A1 and CYP2D6 genotypic distribution.CYP2D6 genotypic distribution was according to Hardy-Weinberg equilibrium, with P value of 0.51 whereas, CYP1A1genotypic distribution did not follow Hardy-Weinberg law(P � 0.038).
The association of various clinicopathologic parameterswith RCC risk has been depicted in Table 1. The mean agewas 54.21 � 0.967 years in cases and 54.01 � 0.916 yearsin controls, thus, was matched with P value � 0.883. Thegender ratio also did not differ significantly between casesand controls (males vs. females, OR � 1.079; CI � 0.718–1.621; P � 0.714). Hypertension was present in 66 (33.9%)and 130 (16.0%) of cases and control, respectively, anddiffered significantly (present vs. absent, OR � 2.665; 95%CI � 1.700–4.178; P � 0.001). Smoking was associatedstrongly with cases 54 (27.6%) than controls 142 (12.8%)(smokers vs. non-smokers, OR � 2.591; 95% CI � 1.594–4.210; P � 0.001). Table 1 shows significant difference(P � 0.008) in the mean BMI (body mass index) of cases(23.67 � 0.164) and controls (22.76 � 0.126). The highertertile BMI group had a higher risk to RCC developmentthan lower BMI group (higher vs. lower, OR � 2.075; 95%CI � 1.298–3.316; P � 0.003).
Table 1Associations between cigarette smoking, BMI, and hypertension in RCC
Parameter Cases (n � 196) Control
Age (years) (Mean � SE) 54.21 � 0.967 54.01 �Sex
Male 138 (70.4%) 172 (68.Female 58 (29.6%) 78 (31.
HypertensionPresent 66 (33.7%) 130 (16.Absent 40 (66.1%) 210 (84.
SmokingPresent 54 (27.6%) 32 (12.Absent 142 (72.4%) 218 (87.
BMI (Mean � S.E) 23.67 � 0.164 22.76 �Low 69 (35.2%) 115 (46.Middle 61 (31.1%) 82 (32.High 66 (33.7%) 53 (21.
a P value of t-test for independent samples.b P value (two sided) Pearson �2 test.OR � crude odds ratio calculated at 95% confidence interval (95% CI)
Low BMI tertile � 22; middle BMI tertile � 23–24; higher BMI tertile �25.3.2. Association of CYP1A1 genotypes with RCC risk
Association of CYP1A1 genotypes with RCC has beenshown in Table 2. The frequency of CYP1A1 AA, AG, andGG genotype in RCC cases was 27%, 50%, and 23%;compared with 44.8%, 42.4%, and 12.8% in healthy con-trols, respectively. The CYP1A1 AG genotype had signifi-cantly higher risk of developing RCC than CYP1A1 AAgenotype (AG vs. AA, OR � 1.953; CI � 1.274–2.994;P � 0.002). Similarly, CYP1A1 GG genotype had evensignificantly greater risk of developing RCC than CYP1A1AA genotype (GG vs. AA, OR � 2.971; CI � 1.699–5.196;P � 0.0001). Multivariate analysis after adjusting for gen-der, age, BMI, smoking, and hypertension, also revealedhigher risk of RCC in CYP1A1 AG genotype than CYP1A1AA genotype (AG vs. AA, OR � 1.403; CI � 0.942–2.088;P � 0.095) but statistically insignificant. Similarly,CYP1A1 GG genotype had even significantly greater risk ofdeveloping RCC than CYP1A1 AA genotype (GG vs.AAOR � 1.693; CI � 0.997–2.875; P � 0.051). WhenCYP1A1 AA and AG genotype were combined, univariateanalysis found a higher risk of RCC in individuals withCYP1A1 GG genotype compared to AA/AG genotype (GGvs. AA/AG, OR � 2.030; CI � 1.233–3.342; P � 0.005).Multivariate analysis after adjusting for age, gender, smok-ing, BMI, and hypertension also revealed higher risk ofRCC among the individuals with CYP1A1 GG genotype(GG vs. AA/AG, OR � 1.693; CI � 0.997–2.875; P �0.05).
When we compared allelic frequency of CYP1A1 Gallele and A allele between RCC cases and controls, wefound there was significantly higher frequency of CYP1A1G allele in RCC cases compared with controls (cases vs.controls, OR � 1.788; CI � 1.364–2.346; P � 0.00002).
0) OR 95% (CI) P valueb
— — 0.883a
1.079 0.718–1.621 0.7141.0 (Reference)
2.665 1.700–4.178 01.0 (Reference)
2.591 1.594–4.210 01.0 (Reference)— — �0.000a
1.0 (Reference)1.2398 0.793–1.936 0.0082.0755 1.298–3.316
(n � 25
0.916
8%)2%)
0%)0%)
8%)2%)0.126
0%)8%)2%)
.

g
af0wsh
3F
wCgtc
1354 S.T. Ahmad et al. / Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
3.3. Association of CYP2D6 genotypes with RCC risk
Association of CYP2D6 genotypes with RCC is shownin Table 2. The frequency of CYP2D6 CC, CT, and TTgenotype in RCC cases was 18.9%, 48.5%, and 32.7%,compared with 16.8%, 50.8%, and 32.4% in healthy con-trols, respectively. The CYP2D6 CT genotype did not differfrom CYP2D6 CC genotype towards risk of developingRCC (CT vs. CC, OR � 0.849; CI � 0.507–1.422; P �0.597). Similarly, CYP2D6 TT genotype did not differtowards risk of developing RCC than CYP2D6 CC geno-type (TT vs. CC, OR � 0.896; CI � 0.517–1.554; P �0.778). Multivariate analysis after adjusting for gender, age,BMI, smoking, and hypertension also revealed that therewas no significant difference in risk to RCC betweenCYP2D6 CT genotype and CYP1A1 CC genotype (CT vs.CC, OR � 0.884; CI � 0.595–1.314; P � 0.543). Similarly,multivariate analysis showed that CYP2D6 TT genotypealso did not differ in risk towards the development of RCCthan CYP2D6 CC genotype (TT vs. CC, OR � 0.979; CI �0.640–1.498; P � 0.923). When CYP2D6 CC and CTgenotype were combined, univariate analysis did not findany significant difference of risk to RCC development inindividuals with CYP2D6 TT genotype compared to CC/CTgenotype (TT vs. CC/CT, OR � 1.012; CI � 0.679–1.508;P � 1.00). Multivariate analysis after adjusting for age,gender, smoking, BMI, and hypertension also revealed thatthere was no significant difference of risk to RCC develop-ment between CYP2D6 TT and CYP2D6 CC/CT genotype(TT vs. CC/CT, OR � 0.979; CI � 0.640–1.498; P �0.923).
When we compared allelic frequency of CYP2D6 T allele
Table 2Multivariate logistic regression model for association of CYP1A1 and CY
Genotype Cases (%) Control (%) ORa C
CYP1A1AA 53 (27.0%) 112 (44.8%) 1.0 (Ref)AG 98 (50.0%) 106 (42.4%) 1.953 (1GG 45 (23.0%) 32 (12.8%) 2.971 (1
AA/AG 151 (77.0%) 218 (87.2%) 1.0 (Ref)GG 45 (23.0%) 32 (12.8%) 2.03 (1A allele 204 (52.04%) 330 (66.0%) 1.0 (Ref)G allele 188 (47.95%) 170 (34.0%) 1.788 (1CYP2D6
CC 37 (18.9%) 42 (16.8%) 1.0 (Ref)CT 95 (48.5%) 127 (50.8%) 0.849 (0TT 64 (32.7%) 81 (32.4%) 0.896 (0
CC/CT 132 (67.3%) 169 (67.6%) 1.0 (Ref)TT 64 (32.7%) 81 (32.4%) 1.012 (0
C allele 169 (43.11%) 211 (42.2%) 1.0 (Ref)T allele 223 (56.88%) 289 (57.8%) 0.963 (0
a P value (two sided) Fisher’s exact test.ORa � crude odds ratio calculated at 95% confidence interval (95% CIb P value (two sided) Fisher’s exact test.ORb � crude odds ratio calculated at 95% confidence interval (95% C(categorical), and BMI (continuous).
and C allele between RCC cases and controls, we found there s
was no significant association between CYP2D6 T allele andRCC risk (cases vs. controls, OR � 0.963; CI � 0.737–1.258;P � 0.785).
3.4. Association of CYP1A1 and CYP2D6 genotypes withAJCC stage
The association of CYP1A1 and CYP2D6 genotypeswith AJCC stage is shown in Table 3. When CYP1A1genotypic distribution among different AJCC cancer stageswas studied, we found that there was no significant trend inthe frequency of genotypes (ptrend � 0.117). After combin-ing CYP1A1 AA and AG genotypes, we still did not findany significant trend (ptrend � 0.267) in the distribution ofenotypes among different histological RCC stages.
When we studied the distribution of CYP2D6 genotypesmong different AJCC cancer stages, we found a higherrequency of CYP2D6 TT genotype significantly (ptrend �.001) associated with higher RCC stages. Similarly, whene combined CYP2D6 CC and CT genotypes, there was
trong association (ptrend � 0.001) of TT genotype withigher cancer stage.
.5. Association of CYP1A1 and CYP2D6 genotypes withuhrman’s nuclear grade
The association of CYP1A1 and CYP2D6 genotypesith Fuhrman’s nuclear grade is shown in Table 3. WhenYP1A1 genotypic distribution among different cancerrades was studied, we found that there was no significantrend in the frequency of genotypes (ptrend � 0.085). Afterombining CYP1A1 AA and AG genotypes, there was a
polymorphism and RCC risk
)a P valuea ORb CI (95%)b P valueb
1.0 (Ref).994) 0.002 1.403 (0.942–2.088) 0.095.196) 0.0001 1.693 (0.997–2.875) 0.051
1.0 (Ref).342) 0.005 1.693 (0.997–2.875) 0.05
.346) 0.00002
.422) 0.597 0.884 (0.595–1.314) 0.543
.554) 0.778 0.979 (0.640–1.498) 0.9231.0 (Ref)
.508) 1 0.979 (0.640–1.498) 0.923
.258) 0.785
adjusted multivariate model.
djusted model for sex (categorical), hypertension (categorical), smoking
P2D6
I (95%
.274–2
.699–5
.233–3
.364–2
.507–1
.517–1
.679–1
.737–1
) of un
I) for a
ignificant trend (ptrend � 0.034) in the distribution of ge-

1355S.T. Ahmad et al. / Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
notypes among different nuclear grades, with highest fre-quency of GG genotype in the III�IV nuclear grade.
When we studied the distribution of CYP2D6 genotypesamong different nuclear grade of RCC, we did not find anysignificant trend (ptrend � 0.178) in the distribution ofCYP2D6 genotypes among different Fuhrman’s nucleargrade. Similarly, when we combined CYP2D6 CC and CTgenotypes, still we did not find any significant trend (ptrend �0.188) in the distribution of combined CYP2D6 CC/CT geno-types among different nuclear grades.
4. Discussion
Epidemiologic and human genetic studies have recog-nized different types of population “at risk,” first populationwith heavy exposure to carcinogens, such as smokers andexposed workers, and the other consisting of carriers ofcancer predetermining germ-line mutations in genes which,because of high penetrance, confer a very high risk forcancer per se [11]. There is an additional group of predis-posing polymorphic, low-penetrance genes, which are in-volved in carcinogen metabolism and DNA repair and, thus,modestly increase the risk for cancer in exposed population,perhaps at low doses of carcinogens [12,13]. Drug metab-
Table 3Association of genotypes with different AJCC cancer stages and Fuhrman
AJCC staging Stage I S
CYP1A1AA 18 (40.5%) 22AG 40 (32.6%) 24GG 12 (26.7%) 14AA/AG 58 (38.4%) 46GG 12 (26.7%) 14
CYP2D6CC 15 (24.1%) 16CT 31 (40.1%) 35TT 24 (37.5%) 09CC/CT 46 (34.8%) 51TT 24 (37.5%) 09
Fuhrman’sgrade
Grade I G
CYP1A1AA 16 (30.2%) 30AG 22 (22.4%) 58GG 04 (8.9%) 34AA/AG 38 (25.2%) 88GG 04 (8.9%) 34
CYP2D6CC 12 (32.4%) 20CT 18 (18.9%) 65TT 12 (18.8%) 37CC/CT 30 (22.7%) 85TT 12 (18.8%) 37
a �2 Test for trend.
olizing enzymes, which often display genetic polymor-
phism, metabolize many tobacco carcinogens into DNAadducts in target cells and ultimately may increase the riskfor cancer.
Cytochrome P450s are enzymes that catalyze phase-Imetabolism reactions, such as C-, N- and S-oxidation anddealkylation. CYP1A1 is a member of the CYP1 family andparticipates in the metabolism of a vast number of xenobi-otics as well as endogenous substrates, and is found mainlyin extrahepatic tissues [14]. Hayashi et al. [15] first de-scribed a base substitution of adenine to guanine at position2455 in the heme-binding region of exon 7, which results inan isoleucine to valine amino acid substitution at codon 462(Ile462Val). The valine allele correlates with increased en-zymatic activity [7], thought to lead to greater carcinogensusceptibility. Therefore, we hypothesized that the overrep-resentation of valine allele in our studied population willconfer increased risk to the development of renal cell car-cinoma. In all ethnic groups, the valine variant occurs lessfrequently than the isoleucine variant. CYP1A1 Valine vari-ant occurs most frequently in Asians, where 1%–8% areVal/Val and 15%–46% are Ile/Val. In Europeans and USWhites, at most 3% are Val/Val and as many as 15% areIle/Val. The Val variant is less common among AfricanAmericans than Whites. In the present study, we found thatthe genotypic distribution of the control population was
ear grade
Stage III � IV P valuea
0.117) 13 (16.2%)) 34 (30.5%)) 19 (42.2%)) 47 (31.1%) 0.267) 19 (42.2%)
0.001) 06 (38.9%)) 29 (31.7%)) 31 (48.4%)) 35 (26.5%) �0.001) 31 (48.4%)
Grade III � IV P valuea
) 07 (13.2%) 0.085) 18 (18.4%)) 07 (15.6%)) 25 (16.6%) 0.034) 07 (15.6%)
0.178) 05 (13.5%)) 12 (12.6%)) 15 (23.4%)) 17 (12.9%) 0.188) 15 (23.4%)
’s nucl
tage II
(43.2%(36.8%(31.1%(30.5%(31.1%
(37.0%(28.2%(14.1%(38.6%(14.1%
rade II
(56.6%(59.2%(75.6%(58.3%(75.6%
(54.1%(68.4%(57.8%(64.4%(57.8%
quite comparable to controls in previous study conducted in

fcvdplvetiwaposTCCofbasm(cCip
i
iddmpaCsCTlsRaRCosFbvpg
[
[
[
[
1356 S.T. Ahmad et al. / Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
North India [16]. Moreover, the CYP1A1 val allele wasound to be more frequent in RCC population than in theontrol population. Thus, our finding also confirmed that thealine variant renders population to higher risk of RCCevelopment. These results were in accordance to our hy-othesis and supported the previous studies, which reportedower risk of cancers [17] associated with the CYPA1A1aline variant, possibly due to latter’s higher enzymaticfficiency ultimately leading to greater carcinogen activa-ion during phase I biotransformation step. When we strat-fied our study population on the basis of smoking habits, itas found that there was no difference between smokers
nd non-smokers in the extent of association between therevalence of CYP1A1 polymorphism and RCC risk. More-ver, compared with normal kidney, RCC tissue has beenhown to contain significantly higher CYP1A1 activity [18].he only study conducted so far on the association betweenYP1A1 polymorphism and RCC reported that theYP1A1 “variant” genotype, which contains at least 1 copyf the CYP1A1 valine alleles, was associated with a 2.1-old increased risk of RCC [3]. Similarly, there are a num-er of studies on the association of CYP1A1 polymorphismnd risk to different types of cancers. A meta-analysis oftudies carried out to find an association of CYP1A1 poly-orphism and breast cancer risk found that A2455G
Ile462Val) G allele polymorphism status was closely asso-iated with breast cancer risk in Caucasians but not inhinese subjects [17]. Similarly, results of previous studies
nvestigating the impact of CYP1A1 A2455G polymor-hism on colon cancer [19–21], lung cancer [5,22], and
head and neck cancer [23] are in accordance with the find-ngs of our study.
Cytochrome P450 2D6 (CYP2D6) metabolizes manymportant drugs. CYP2D6 activity ranges from completeeficiency to ultrafast metabolism, depending on at least 16ifferent known alleles [24]. CYP2D6 is involved in theetabolism of a number of therapeutic drugs and is a
ossible susceptibility factor for certain environmental re-gent-induced diseases [25]. A detrimental mutation of theYP2D6 gene at C188-T, causing a Pro34-Ser amino acid
ubstitution in the highly conserved region, results in lowerYP2D6 stability and, thus, decreased enzymatic activity.hus, we hypothesized that the variation at 188 nucleotide
eading to low efficiency of carcinogen metabolism mayerve beneficial to our population, decreasing the risk ofCC development. But, in the current study we did not findny significant correlation between this polymorphism andCC risk. There are only a few studies regarding the role of188T polymorphism and cancer risk. Thus, the findings ofur study, although it contradicted our generated hypothe-is, was in accordance with an earlier study carried out in arench population that did not discover any clear correlationetween CYP2D6 polymorphism and RCC risk [3]. A pre-ious study conducted in a Chinese lung cancer patientopulation found significant association between non-T188T
enotypes and lung cancer risk [26]. Therefore, although ap-parently it looks as if it contradicted our results, this study wascarried out in an altogether different ethnicity. When we ana-lyzed the distribution of CYP1A1 and CYP2D6 genotypesamong different cancer stages and grades, we found that therewas no significant association between the CYP1A1 with can-cer progression. But CYP2D6 TT genotype was found to bestrongly associated with RCC progression to higher cancerstage. There is no possible explanation available for this at thistime.
The inference that we can draw from the results of ourstudy is that our population may have been exposed todifferent environmental agents, which upon activation byactive CYP1A1 (val variant) biotransformation metabolism,may have yielded potential carcinogenic products that leadto the development of renal cell cancer, whereas CYP2D6polymorphism did not make an impact on risk of RCCdevelopment. It may be that the polymorphism of CYP2D6gene is not susceptible to renal cell carcinoma because ofsome specific genetic background or environmental influ-ences. Further investigations with large sample size arerequired to clarify the exact cause. Although the reasons forheterogeneity of our results remain incompletely under-stood, this study clearly suggests that the CYP1A1 deficientgenotype is protective for RCC.
References
[1] Ljungberg B, Campbell SC, Cho HY, et al. The epidemiology of renalcell carcinoma. Eur Urol 2011;60:615–21.
[2] Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA CancerJ Clin 2010;60:277–300.
[3] Longuemaux S, Deloménie C, Gallou C, et al. Candidate geneticmodifiers of individual susceptibility to renal cell carcinoma. CancerRes 1999;59:2903–8.
[4] Luo Y, Chen H, Khan MA, et al. Genetic polymorphisms of meta-bolic enzymes—CYP1A1, CYP2D6, GSTM1, GSTT1, and gastriccarcinoma susceptibility. Tumor Biol 2011;32:215–22.
[5] Larsen JE, Colosimo ML, Yang IA, et al. Risk of non-small-cell lungcancer and the cytochrome p4501a1 ile462val polymorphism. CancerCauses Control 2005;16:579–85.
[6] Agúndez JAG. Cytochrome p450 gene polymorphism and cancer.Current drug metabolism 2004;5:211–24.
[7] Crofts F, Taioll E, Trachman J, et al. Functional significance ofdifferent human cyplal genotypes. Carcinogenesis 1994;15:2961–3.
[8] Yokoi T, Kamataki T. Genetic polymorphism of drug metabolizingenzymes: New mutations in CYP2D6 and CYP2A6 genes in Japa-nese. Pharm Res 1998;15:517–24.
[9] Greene FL: AJCC cancer staging handbook: From the AJCC cancerstaging manual. New York: Springer Verlag, 2002.
10] Chan DKY, Mellick GD, Buchanan DD, et al. Lack of associationbetween CYP1A1 polymorphism and Parkinson’s disease in a Chi-nese population. J Neural Transmission 2002;109:35–9.
11] Caporaso N, Goldstein A. Cancer genes: Single and susceptibility—exposing the difference. Pharmacogenetics and Genomics 1995;5:59.
12] Vineis P, Bartsch H, Caporaso N, et al. Genetically based N-acetyl-transferase metabolic polymorphism and low-level environmentalexposure to carcinogens. Nature 1994;369:154–6.
13] Vineis P. Molecular epidemiology: Low dose carcinogens and genetic
susceptibility. Int J Cancer 1997;71:1–3.
[
[
[
[
[
[
[
[
1357S.T. Ahmad et al. / Urologic Oncology: Seminars and Original Investigations 31 (2013) 1350–1357
[14] Androutsopoulos V, Tsatsakis A, Spandidos D. Cytochrome p450CYP1A1: Wider roles in cancer progression and prevention. BMCCancer 2009;9:187.
[15] Hayashi S, Watanabe J, Nakachi K, et al. Genetic linkage of lungcancer-associated mspi polymorphisms with amino acid replacementin the heme binding region of the human cytochrome p450ia1 gene.J Biochem 1991;110:407–11.
[16] Yadav CS, Bajpai M, Kumar V, et al. Polymorphism in CYP1A1,GSTM1, GSTT1 genes and organochlorine pesticides in the etiologyof hypospadias. Hum Exp Toxicol 2011;78:902–7.
[17] Sergentanis TN, Economopoulos KP. Four polymorphisms in cyto-chrome p450 1a1 (CYP1A1) gene and breast cancer risk: A meta-analysis. Breast Cancer Res Treatment 2010;122:459–69.
[18] Rintala S, Tammela TLJ, Tuimala R. Cyp1A1 activity in renal cell carci-noma and in adjacent normal renal tissue. Urol Res 1998;26:117–21.
19] Kiss I, OrsÓS Z, Gombos K, et al. Association between allelicpolymorphisms of metabolizing enzymes (CY1A1, CYP1A2,CYP2E1, MEH) and occurrence of colorectal cancer in Hungary.Anticancer Res 2007;27:2931–7.
20] Sachse C, Smith G, Wilkie MJV, et al. A pharmacogenetic study toinvestigate the role of dietary carcinogens in the etiology of colorectal
cancer. Carcinogenesis 2002;23:1839–49.21] Pereira Serafim PV, Cotrim Guerreiro da Silva ID, Manoukias Fo-rones N. Relationship between genetic polymorphism of CYP1A1 atcodon 462 (ile462val) in colorectal cancer. Int J Biol Markers 2008;23:18–23.
22] Tefre T, Ryberg D, Haugen A, et al. Human CYP1A1 (cytochromep(1)450) gene: Lack of association between the msp i restrictionfragment length polymorphism and incidence of lung cancer in aNorwegian population. Pharmacogenetics 1991;1:20–5.
23] Ophuis MBO, Lieshout EMM, Roelofs HMJ, et al. Glutathione stransferase m1 and t1 and cytochrome p4501a1 polymorphisms inrelation to the risk for benign and malignant head and neck lesions.Cancer 1998;82:936–43.
24] Sachse C, Brockmöller J, Bauer S, et al. Cytochrome p450 2d6variants in a Caucasian population: Allele frequencies and phenotypicconsequences. Am J Human Genet 1997;60:284–95.
25] Thuerauf N, Lunkenheimer J. The impact of the CYP2D6-polymor-phism on dose recommendations for current antidepressants. EurArch Psychiatry Clin Neurosci 2006;256:287–93.
26] Yan Z, Wu YM, Wu YJ. [CYP2D6�10 Polymorphisms and lungcancer susceptibility]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao
2008;30:564–8.