Embed Size (px)
Citation preview
RITA-3RITA-3
Is this a benign lesion Is this a benign lesion in a benign condition?in a benign condition?
Who Needs Angioplasty in 2008?Who Needs Angioplasty in 2008?• Stable AnginaStable Angina
Keith A A FoxProfessor of CardiologyUniversity & Royal InfirmaryEdinburgh

Conflicts of interest slide
Advanced angioplasty 2008
Device industry: None
Grant Funding: British Heart Foundation, Wellcome Trust, Medical Research Council, ESC, Sanofi-Aventis, BMS, GSK
Travel & honoraria: Sanofi-Aventis, BMS, GSK
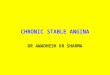
Event Rates: “Primary Prevention”; Stable Angina ; Event Rates: “Primary Prevention”; Stable Angina ; non-ST Elevation ACS. Death / MI after 12 monthsnon-ST Elevation ACS. Death / MI after 12 months
Wallentin L et al. Lancet 2000;356:9–16Juul-Moller S et al. Lancet 1992;340:1421–1425Shepherd J et al. N Engl J Med 1995;333:1301–1307
Poole-Wilson et al ACTION Lancet 2004;364:849-57.
Dea
th/ M
I (%
)
Months of follow up
Unstable angina/non Q wave MI (FRISC II)
16
12
8
4
0
0 2 4 6 8 10 12
Stable angina (SAPAT)
Primary Prevention (WOSCOPS)
ACTION trial (stable CAD)
Approx 1.5%Stable CAD

salvage of ischaemic myocardiumsalvage of ischaemic myocardium
Stable anginaStable angina Non-ST elevation ACSNon-ST elevation ACS ST Elevation MIST Elevation MI
Concepts: Extent of salvage (infarction) proportional to clinical benefit: death or MIExtent of reversible ischaemia proportional to benefit on relief of angina

Conservative
Intervention
0
5
10
15
20
25C
umul
ativ
e pe
rcen
tage
0 1 2 3 4 5Follow-up time (years)
RITA 3, 5 yr outcome:RITA 3, 5 yr outcome:
p = 0.054odds ratio: 0.76 95% CI 0.58 - 1.00
15.1%
12.1%
Cardiovascular Deaths:p = 0.026
odds ratio: 0.68 95% CI 0.49 – 0.95
Lancet 2005: 366; 914-20
Death or MI: odds ratio 0.78, Death or MI: odds ratio 0.78,
95%CI 0.61-0.99, p= 0.0495%CI 0.61-0.99, p= 0.04
All deaths
BHF BHF RITA-3RITA-3
PCI vs. Conservative Therapy: Stable CAD PCI vs. Conservative Therapy: Stable CAD Meta-analysis Meta-analysis (pre-COURAGE)(pre-COURAGE)
PCI vs. Conservative Therapy: Stable CAD PCI vs. Conservative Therapy: Stable CAD Meta-analysis Meta-analysis (pre-COURAGE)(pre-COURAGE)
Primary Endpoint: Death, or nonfatal MI, CABG, and PCI during follow-Primary Endpoint: Death, or nonfatal MI, CABG, and PCI during follow-up (in the target vessel or other vessel/segment). up (in the target vessel or other vessel/segment).
Primary Endpoint: Death, or nonfatal MI, CABG, and PCI during follow-Primary Endpoint: Death, or nonfatal MI, CABG, and PCI during follow-up (in the target vessel or other vessel/segment). up (in the target vessel or other vessel/segment).
PCIPCIn=1476n=1476
PCIPCIn=1476n=1476
Conservative TherapyConservative Therapyn=1474n=1474
Conservative TherapyConservative Therapyn=1474n=1474
Stable CAD & >1 stenosis: 2950 patients from randomized Stable CAD & >1 stenosis: 2950 patients from randomized trials (PCI versus conservative medical therapy)trials (PCI versus conservative medical therapy)
Stable CAD & >1 stenosis: 2950 patients from randomized Stable CAD & >1 stenosis: 2950 patients from randomized trials (PCI versus conservative medical therapy)trials (PCI versus conservative medical therapy)
Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912

PCI vs. Conservative Therapy: Meta-AnalysisPCI vs. Conservative Therapy: Meta-AnalysisPCI vs. Conservative Therapy: Meta-AnalysisPCI vs. Conservative Therapy: Meta-Analysis
• No significant difference: death, No significant difference: death, cardiac death or MI, nonfatal MI, and cardiac death or MI, nonfatal MI, and need for CABGneed for CABG
# pa
tient
s#
patie
nts
95126
87109101 109
66
106
0
50
100
150
200
250
Death Cardiacdeath/MI
nonfatal MI CABG
PCI Conservative
95126
87109101 109
66
106
0
50
100
150
200
250
Death Cardiacdeath/MI
nonfatal MI CABG
PCI Conservative
Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912
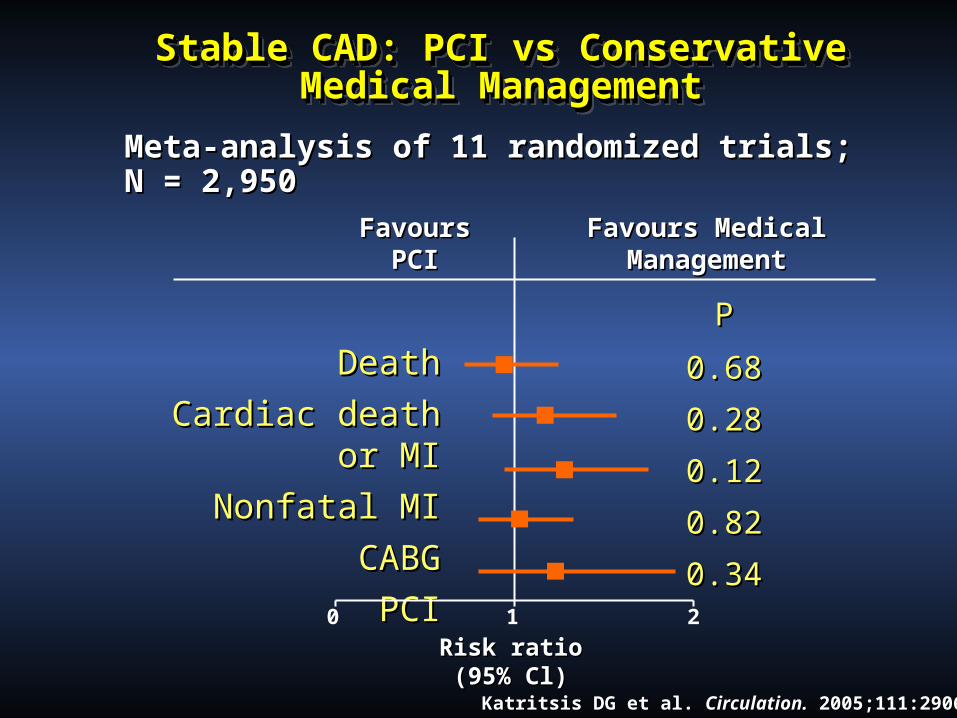
Stable CAD: PCI vs ConservativeStable CAD: PCI vs ConservativeMedical ManagementMedical Management
Stable CAD: PCI vs ConservativeStable CAD: PCI vs ConservativeMedical ManagementMedical Management
Meta-analysis of 11 randomized trials; N = 2,950Meta-analysis of 11 randomized trials; N = 2,950
DeathDeath
Cardiac death or MICardiac death or MI
Nonfatal MINonfatal MI
CABGCABG
PCIPCI
Katritsis DG et al. Katritsis DG et al. Circulation.Circulation. 2005;111:2906-12 2005;111:2906-12..
0 1 2
PP
0.680.68
0.280.28
0.120.12
0.820.82
0.340.34
Risk ratioRisk ratio(95% Cl)(95% Cl)
Favours Favours PCIPCI
Favours Medical Favours Medical ManagementManagement

RITA-2: PTCA vs Medical Therapy in RITA-2: PTCA vs Medical Therapy in Stable Angina(n=1000)Stable Angina(n=1000)
RITA-2: PTCA vs Medical Therapy in RITA-2: PTCA vs Medical Therapy in Stable Angina(n=1000)Stable Angina(n=1000)
PTCAPTCA MedicalMedical OROR PP
Death/MIDeath/MI 32 (6.3%)32 (6.3%) 17 (3.3%)17 (3.3%) 1.911.91 0.020.02
CABGCABG 40 (7.2%)40 (7.2%) 30 (5.8%)30 (5.8%) 1.241.24 --
Post-rand PTCAPost-rand PTCA 62 (12.3%)62 (12.3%) 101 (19.9%)101 (19.9%) 0.620.62 0.0010.001
Any PTCAAny PTCA 533 (>100.0%)533 (>100.0%) 101 (19.9%)101 (19.9%) 5.285.28 <<0.0001<<0.0001
Total proceduresTotal procedures 577577 131131 4.504.50 <<0.0001<<0.0001
Lancet 1997

RITA-2: Impact on Grade 2 Angina RITA-2: Impact on Grade 2 Angina (Med v PTCA)(Med v PTCA)
RITA-2: Impact on Grade 2 Angina RITA-2: Impact on Grade 2 Angina (Med v PTCA)(Med v PTCA)
RITA-2 Lancet 1997

RITA 2: Quality of Life over 3 years of RITA 2: Quality of Life over 3 years of Follow-upFollow-up
RITA 2: Quality of Life over 3 years of RITA 2: Quality of Life over 3 years of Follow-upFollow-up
Pocock et al. JACC 2000
• Compared with conservative therapy, PCI does not Compared with conservative therapy, PCI does not decrease mortality or the risk of MI during follow-up in decrease mortality or the risk of MI during follow-up in patients with chronic CAD.patients with chronic CAD.
• A trend for increased risk of MI in patients undergoing A trend for increased risk of MI in patients undergoing PCI was observed. PCI was observed.
• Even when analyses were limited to studies that used Even when analyses were limited to studies that used stents, the meta-analysis found no evidence of stents, the meta-analysis found no evidence of superiority for the PCI strategy.superiority for the PCI strategy.
• Need for more randomized trials…Need for more randomized trials…
• Compared with conservative therapy, PCI does not Compared with conservative therapy, PCI does not decrease mortality or the risk of MI during follow-up in decrease mortality or the risk of MI during follow-up in patients with chronic CAD.patients with chronic CAD.
• A trend for increased risk of MI in patients undergoing A trend for increased risk of MI in patients undergoing PCI was observed. PCI was observed.
• Even when analyses were limited to studies that used Even when analyses were limited to studies that used stents, the meta-analysis found no evidence of stents, the meta-analysis found no evidence of superiority for the PCI strategy.superiority for the PCI strategy.
• Need for more randomized trials…Need for more randomized trials…
PCI vs. Conservative Therapy: SummaryPCI vs. Conservative Therapy: SummaryPCI vs. Conservative Therapy: SummaryPCI vs. Conservative Therapy: Summary
Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912Katritsis DG et al Circulation 2005; 111:2906-2912

• objective evidence of myocardial ischemiaobjective evidence of myocardial ischemia• stenosis > 70% in stenosis > 70% in > > one proximal coronary arteryone proximal coronary artery
Objective myocardial ischemia:ST-segment depression or T-wave inversion on the resting ECG or inducible ischemia (exercise or vasodilator stress) or at least one coronary stenosis > 80% plus classic angina
BMS not DES; all patients suitable for PCI; low event rate
2287 patients
“Optimal Medical Therapy“At 5 yrs: 70% had LDL <2.20 mmol per liter)65% and 94% had systolic and diastolic BP < 130/8545% of patients with diabetes had Hb A1c <7% High adherence to diet, exercise, and smoking cessation
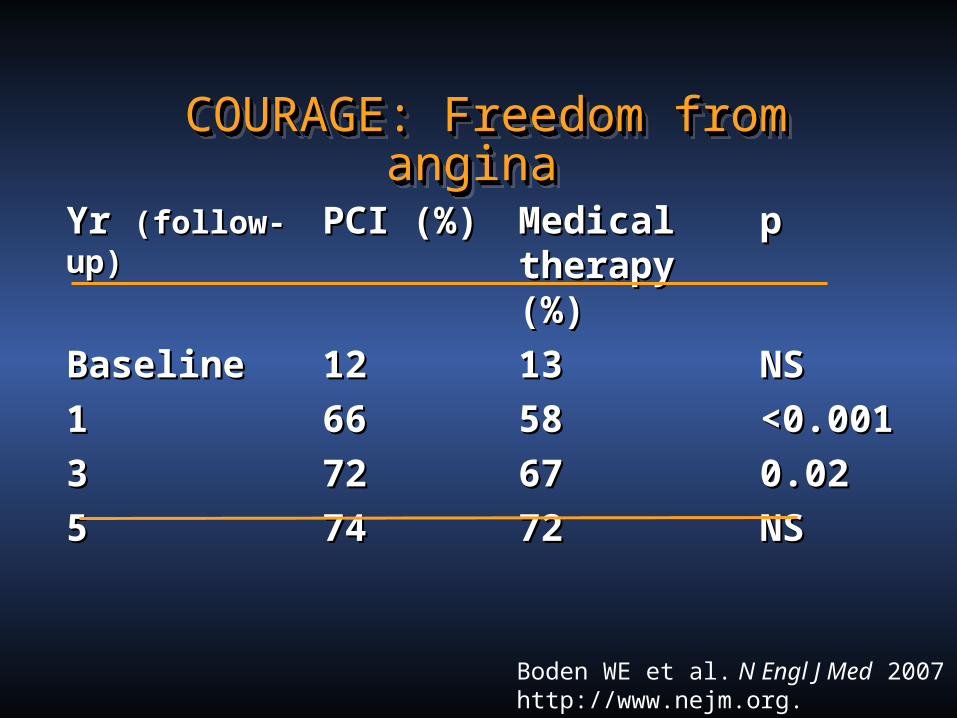
COURAGE: Freedom from angina COURAGE: Freedom from angina COURAGE: Freedom from angina COURAGE: Freedom from angina
Boden WE et al. N Engl J Med 2007 http://www.nejm.org.
Yr Yr (follow-up)(follow-up) PCI (%)PCI (%) Medical Medical therapy (%)therapy (%)
pp
BaselineBaseline 1212 1313 NSNS
1 1 6666 5858 <0.001<0.001
3 3 7272 6767 0.020.02
5 5 7474 7272 NSNS

Boden WE et al. N Engl J Med 2007 http://www.nejm.org.
COURAGE: Cumulative event rates (4.6 yrs)COURAGE: Cumulative event rates (4.6 yrs)COURAGE: Cumulative event rates (4.6 yrs)COURAGE: Cumulative event rates (4.6 yrs)
OutcomeOutcome PCI PCI (%)(%)
Medical Medical Rx (%)Rx (%)
Hazard Hazard ratio ratio
95% CI95% CI pp
Death, MIDeath, MI 1919 18.518.5 1.05 1.05 0.87–1.270.87–1.27 0.620.62

Boden WE et al. N Engl J Med 2007 http://www.nejm.org.
COURAGE: Cumulative event rates (4.6 yrs)COURAGE: Cumulative event rates (4.6 yrs)COURAGE: Cumulative event rates (4.6 yrs)COURAGE: Cumulative event rates (4.6 yrs)
OutcomeOutcome PCI PCI (%)(%)
Medical Medical Rx (%)Rx (%)
Hazard Hazard ratio ratio
95% CI95% CI pp
Death, MIDeath, MI 1919 18.518.5 1.05 1.05 0.87–1.270.87–1.27 0.620.62
Death, MI, strokeDeath, MI, stroke 2020 19.519.5 1.051.05 0.87–1.270.87–1.27 0.620.62
DeathDeath 7.67.6 8.38.3 0.870.87 0.65–1.160.65–1.16 0.380.38
Nonfatal MINonfatal MI 13.213.2 12.312.3 1.131.13 0.89–1.430.89–1.43 0.330.33
StrokeStroke 2.12.1 1.81.8 1.561.56 0.80–3.040.80–3.04 0.190.19
Hospitalization Hospitalization for ACSfor ACS
12.412.4 11.811.8 1.071.07 0.84–1.370.84–1.37 0.560.56
Revascularization Revascularization (PCI or CABG)(PCI or CABG)
21.121.1 32.632.6 0.600.60 0.51–0.710.51–0.71 <0.001<0.001


Rest
Mid
Base
Apex
StressRestStress
After optimal anti-ischemicmedical therapy
Before treatment
20032000COURAGEstudy
Patient randomizedto medical treatment only
Case presented at ACC 2003 by Dr. Robert O´Rourke
PCI in stable angina…
• Event rates of death & MI approx 1.5% per annum - on optimal medical therapy• Scope to improve rate of death or MI is very limited - even in patients with proximal stenosis & inducible ischaemia• PCI is superior to medical therapy (at least over 3 yrs) in relief of angina, but not longer term• Greater benefit in those with more extensive ischaemia (>5% LV)• Role of PCI in those with angina and LV dysfunction is unresolved
Conclusions: 2008