Embed Size (px)
Citation preview

Riyaz ShahKent Oncology Centre Maidstone, UK
ErbB family blockade in squamous cell carcinoma (SCC):Latest clinical understanding

Background
• SCC of the lung remains a disease with high unmet medical need
• ErbB pathway dysregulation is frequently observed in SCC1-3
• Erlotinib, a reversible EGFR TKI, is an approved second-line therapy for these patients
Although no direct head-to-head trials, erlotinib has improved tolerability over docetaxel4 yet similar survival in second-line unselected and EGFR WT NSCLC5
• Afatinib could confer additional benefit over erlotinib Irreversible inhibition of signaling from ErbB1(EGFR), HER2 to
HER46
*Afatinib is approved in a number of markets, including the EU, Japan, Taiwan and Canada under the brand name GIOTRIF® and in the USA under the brand name GILOTRIF® for use in patients with distinct types of EGFR mutation-positive NSCLC. Registration conditions differ internationally, please refer to locally approved prescribing information. Afatinib is under regulatory review by health authorities in other countries worldwide. Afatinib is not approved in other indications.
1. Heinmöller P, et al. Clin Cancer Res 2003;9:5238–43; 2. Ugocsai K, et al. Anticancer Res 2005;25:3061–6. 3. Cancer Genome Atlas Research Network. Nature 2012;489:519–25; 4. Lee C, et al. J Natl Cancer Inst 2013;105:595–605; 5. Li N, et al. PLoS One 2014;9:e102777; 6. Solca F, et al.
J Pharmacol Exp Ther 2012;343:342–50

Question: What is your current standard-of-care in treatment of second-line SCC?
1. Erlotinib
2. Chemotherapy (e.g. docetaxel)
3. Nivolumab
4. Other TKIs
5. Other

Question: In what SCC patients do you typically prescribe erlotinib?
1. All patients
2. Older patients
3. Younger, more active patients
4. PS>2
5. PS≤2
6. As ≥third-line treatment only

Question: In what SCC patients do you typically prescribe docetaxel?
1. All patients
2. Older patients
3. Younger, more active patients
4. PS>2
5. PS≤2

Question: In what setting do you prescribe a TKI to SCC patients?
1. Second-line only
2. Second- or third-line in patients unfit for chemotherapy (BR.21)
3. Combination of 2 and 3
4. As maintenance in patients with stable disease post-first-line
5. I don’t prescribe TKIs to squamous cell cancer patients

0 5 10 15 20 25 300.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
Is erlotinib the right TKI comparator?BR.21 trial in patients not eligible for further chemotherapy
Shepherd F, et al. N Engl J Med 2005;352:123–32; Clark G, et al. Clin Lung Cancer 2006;7:389–94; Bezjak A, et al. J Clin Oncol 2006;24:3831–7
Patient characteristics
Erlotinib (n=488)
Placebo (n=243)
Squamous-cell carcinoma
29.5% 32.1%
PS2 25.8% 23%
PS3 8.6% 8.6%
≥2 lines prior therapy
49.4% 49.8%
Survival time (months)
Erlotinib (n=488)
Placebo (n=243)
Patie
nts HR 0.70 (95% CI 0.58–0.85)
p<0.001 by stratified log-rank test
Survival by histology HR (95% CI)
Squamous-cell carcinoma 0.67 (0.50–0.90)
Adenocarcinoma 0.71 (0.56–0.92)
• TTD of symptoms better regardless of histology
• QoL better regardless of histology

Is erlotinib the right TKI comparator?
1. Shepherd F, et al, J Clin Oncol 2000;18:2095–103; 2. Thatcher N, et al. Lancet 2005;366:1527–37; 3. Kim E, et al. Lancet 2008;372:1809–18;4. Shepherd N, et al. N Engl J Med 2005;352:123–32; 5. Cappuzzo F, et al. Lancet Oncol 2010;11:521–9
StudyTreatment
lineOutcome
TAX-3171 ≥2nd Docetaxel > BSC
ISEL2 2nd/3rd Gefitinib = BSC
INTEREST3 ≥2nd Docetaxel = Gefitinib
BR-214 2nd/3rd Erlotinib > Placebo
SATURN5 Maintenance (SD)
Erlotinib > Placebo
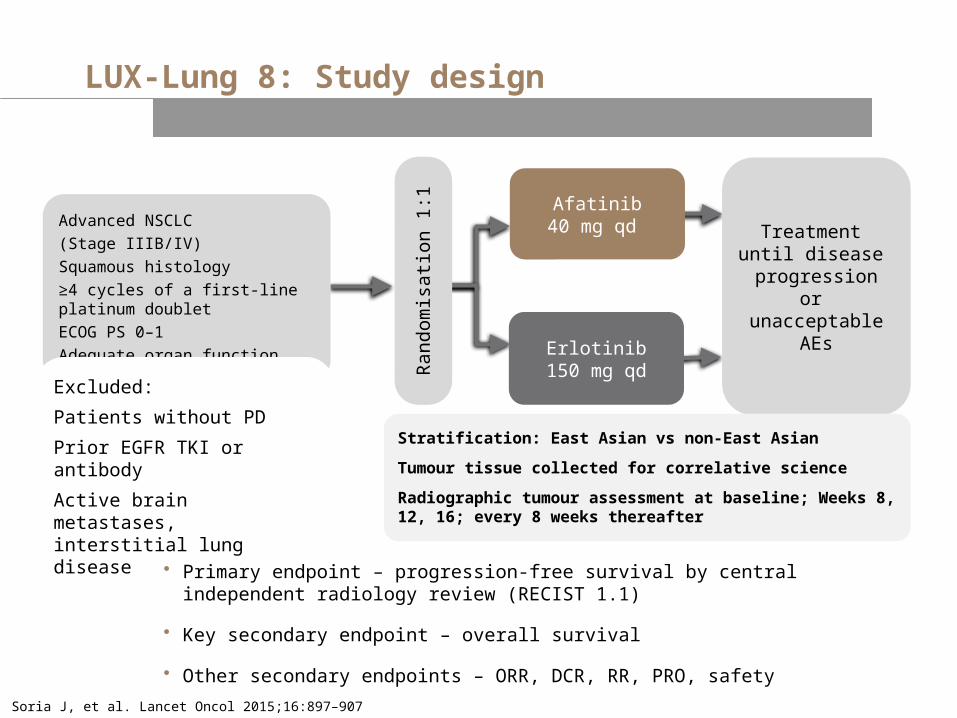
LUX-Lung 8: Study design
Soria J, et al. Lancet Oncol 2015;16:897–907
Advanced NSCLC
(Stage IIIB/IV)
Squamous histology
≥4 cycles of a first-line platinum doublet
ECOG PS 0–1
Adequate organ function
Afatinib40 mg qd
Erlotinib150 mg qd
Treatment until disease progression
or unacceptable
AEsRan
dom
isat
ion
1:1
Excluded:
Patients without PD
Prior EGFR TKI or antibody
Active brain metastases, interstitial lung disease
Stratification: East Asian vs non-East Asian
Tumour tissue collected for correlative science
Radiographic tumour assessment at baseline; Weeks 8, 12, 16; every 8 weeks thereafter
• Primary endpoint – progression-free survival by central independent radiology review (RECIST 1.1)
• Key secondary endpoint – overall survival
• Other secondary endpoints – ORR, DCR, RR, PRO, safety

Afatinib***(n=398)
Erlotinib***(n=397)
Median age, years 65 64
Male, % 84 83Ethnic origin Non-eastern Asian 78 78
East Asian 22 22Smoking history, % Never smoker 7 5
Light ex-smoker§§ 3 3
Current and other ex-smoker¶¶ 91 92ECOG,* % 0/1 32/68 34/66Clinical stage,§ % IIIB/IV 12/88 12/87Median time since diagnosis, years (range) 0.8 (0.2–9.3) 0.7 (0.2–13.5)Histology,¶ % Squamous 96 96
Mixed 4 4Best response to first-line chemotherapy, %
CR/PR 47 47
SD 40 42
Unknown 12 11
Demographics and baseline characteristics
*<1% were ECOG PS 2; §≤1% were stage IIIA; ¶<1% were undifferentiated (considered to be of squamous histology); §§Fifteen pack-years and stopped >1 year before diagnosis; ¶¶71 (17.8%) and 85 (21.4%) patients were current smokers, respectively; ***Percentages may not total 100 due to rounding.Soria J, et al. Lancet Oncol 2015;16:897–907

Progression-free survival (primary endpoint independent review)
CI, confidence interval; HR, hazard ratio. Soria J, et al. Lancet Oncol 2015;16:897–907
No. of patients
Afatinib 335 266 127 96 54 45 28 25 16 15 8 8 4 2 2 1Erlotinib 334 256 112 72 43 34 15 12 6 5 0 0 0 0 0 0
0
0.4
0.8
1.0
0.6
0.2
01 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Afatinib (n=335)
Erlotinib (n=334)
Patients progressed or died, n (%)
202 (60) 212 (64)
Median PFS (months) 2.4 1.9
HR 0.82 (95% CI 0.676–0.998); p=0.0427
Pro
bab
ilit
y o
f P
FS
(%
)
Time (months)

Primary analysis of overall survival (n=795)
CI, confidence interval; HR, hazard ratio. Median follow-up time: 18.4 months.Soria J, et al. Lancet Oncol 2015;16:897–907
Afatinib (n=398)
Erlotinib (n=397)
Median OS (months) 7.9 6.8
HR 0.81 (95% CI 0.69–0.95); p=0.0077
Pro
bab
ilit
y o
f O
S (
%)
No. at risk
AfatinibErlotinib
398 316 249 170 124 82 47 28 10 4 0397 305 210 150 94 54 30 11 4 2 0
3 6 9 12 15 3018 21 24 27
0.2
0.4
0.6
0.8
1.0
00
36.4%
28.2%22.0%
14.4%
Time (months)

Factors No. of patients HR (95% CI)
Overall 795 0.81 (0.69–0.95)Age
<65 years 399 0.68 (0.55–0.85)≥65 years 396 0.95 (0.76–1.19)
GenderMale 666 0.82 (0.69–0.97)Female 129 0.77 (0.51–1.14)
RaceNon-East Asian 623 0.87 (0.73–1.03)East Asian 172 0.62 (0.44–0.88)
ECOG at baseline0 260 0.76 (0.58–1.01)1 531 0.80 (0.66–0.97)
Smoking historyNever smoker 44 0.77 (0.37–1.57)Light ex-smoker 23 0.43 (0.16–1.12)Current and other ex-smoker 728 0.81 (0.69–0.96)
HistologySquamous 763 0.82 (0.70–0.96)Mixed 32 0.55 (0.26–1.17)
Best response to first-line chemotherapyCR/PR 371 0.91 (0.72–1.15)SD 328 0.71 (0.56–0.90)Unknown 89 0.72 (0.44–1.17)
Overall survival subgroup analysis
Favours afatinib Favours erlotinib
1/16 10/16 6 4/16
CI, confidence interval; HR, hazard ratio.Soria J, et al. Lancet Oncol 2015;16:897–907

Objective response and tumour shrinkage
Soria J, et al. Lancet Oncol 2015;16:897–907
Afatinib
ErlotinibPatient index sorted by maximum decrease (%)
Max
imu
m d
ecre
ase
fr
om
bas
elin
e S
LD
(%
)
–100
–80
–60
–40
–20
0
20
40
60
80
100 ≥20% increase (n=62)0–<20% increase (n=90)>0–<30% decrease (n=81)≥30% decrease (n=22)
Patient index sorted by maximum decrease (%)–100
–80
–60
–40
–20
0
20
40
60
80
100 ≥20% increase (n=74)0–<20% increase (n=101)>0–<30% decrease (n=77)≥30% decrease (n=13)
Max
imu
m d
ecre
ase
fro
m
bas
elin
e S
LD
(%
)DCR ORR
0
10
20
30
40
50
60
50.5
5.5
39.5
2.8
Afatinib
Erlotinib
p=0.055
p=0.002
Pe
r c
en
t
• Duration of response was 7.3 months for afatinib and 3.7 months for erlotinib
Objective response Tumour shrinkage

No. of patients HR (95% Cl)
Coughing (Q1from QLQ-LC13) 793 0.89 (0.72–1.09)
Dyspnoea (Q3–Q5from QLQ-LC13) 793 0.79 (0.66–0.94)
Pain (Q9, Q19from QLQ-C30) 793 0.99 (0.82–1.18)
GHS/QoL (Q29–Q30from QLQ-C30) 793 0.93 (0.78–1.12)
Patient-reported outcomes
GHS, global health status.Gadgeel S, et al. ASCO 2015. Poster 425
1/4 1/2 1 2 4
Symptom improvement Time to deterioration
Patients with improvement in symptoms (%)
GHS/QoL (Q29–Q30from QLQ-C30)
Pain (Q9, Q19from QLQ-C30)
Dyspnea (Q3–Q5from QLQ-LC13)
Coughing (Q1from QLQ-LC13)
0 10 20 30 40 50 60
28.3
39.2
44.1
35.2
35.7
40.2
51.3
43.4
Afatinib Erlotinib
Dyspnoea (Q3–Q5from QLQ-LC13)
p=0.04
p=0.78
p=0.06
p=0.03
Favours afatinib Favours erlotinib
Adverse events as expected based on the mechanism of action

Summary and conclusion
• LUX-Lung 8 is the largest Phase III trial in the second-line treatment for SCC of the lung
• Afatinib significantly improved PFS when compared with erlotinib – Independent and investigator reviews were consistent
• In this head-to-head trial, afatinib showed a significant reduction in the risk of death and disease progression by 19% when compared with erlotinib
– ~8% more patients alive at 12 and 18 months with afatinib treatment
• Consistent advantage across most endpoints and subgroups
• Overall symptom relief and QoL measures favouring afatinib
• Afatinib should be the TKI of choice in patients with advanced SCC progressing after treatment with first-line chemotherapy

Questions and discussion