Embed Size (px)
Citation preview

E U R O P E A N U R O L O G Y 6 1 ( 2 0 1 2 ) 2 2 5 – 2 3 1 229
[8] Wauben OSGL, van Veelen MA, Gossor D, Goossens RHM. Application
of ergonomic guidelines during minimally invasive surgery: a ques-
tionnaire survey of 284 surgeons. Surg Endosc 2006;20:1268–74.
[9] Bagrodia A, Raman JD. Ergonomics considerations of radical prosta-
tectomy: physician perspective of open, laparoscopic, and robot-
assisted techniques. J Endourol 2009;23:627–33.
Jens J. Rassweilera,*
Ali S. Goezena
Akbar Ali Jalala
Michael Schulzea
Vito Pansadorob
Giovannalberto Pinia
Fernando Kimc
Craig Turnerd
aDepartment of Urology, SLK Kliniken Heilbronn,
University of Heidelberg, Germany
bLaparoscopy and Robotic Section, Vincenzo Pansadoro Foundation,
Rome, ItalycDepartment of Urology, Denver Health Medical Center,
Denver, CO, USAdSt. Vincent Hospital, Portland, OR, USA
*Corresponding author. Department of Urology, Am Gesundbrunnen 20,
D-74078 Heilbronn, Germany.
Tel. +49 7131 492400; Fax: +49 7131 492429
E-mail address: [email protected]
URL: http://www.urologie-heilbronn.de
(J.J. Rassweiler)
September 16, 2011
Published online ahead of print on September 28, 2011
doi:10.1016/j.eururo.2011.09.018
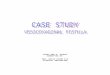
[(Fig._1)TD$FIG]
Fig. 1 – The peritoneal flap is harvested from the right iliac fossa and fixedabove the vaginal suture. The bladder closure follows next.
Robot-Assisted Laparoscopic Repair of High Vesicovagi-
nal Fistulae With Peritoneal Flap Inlay
We would like to present the technique and our experience
in the management of vesicovaginal fistulae with peritoneal
flap inlay using the da Vinci system. So far, only a few
reports can be found about robot-assisted fistula repair
[1–5]. The first one was described in 2005 by Melamud et al
at the University of California [1].
We operated on three females aged 40–64 yr who were
diagnosed with a supratrigonal fistula as a complication
after abdominal hysterectomy with no malignancy. Indica-
tions for the operation were high vaginal fistulae difficult to
achieve by vaginal approach. We chose the laparoscopic
access to get the best exposure to the fistula and to avoid
laparotomy, thereby causing less morbidity to the patients
and giving a superior view for fistula dissection. The fistulae
were diagnosed and localized by cystoscopy and conven-
tional cystography.
The operation was performed under general anesthesia.
We started with the vaginoscopy in lithotomy position. First
we inserted a 5F Fogarty catheter from the vagina through
the fistula into the bladder and verified the position
cystoscopically. Ureteral stents were inserted bilaterally.
A sponge stick was inserted into the vagina to ease
subsequent intraoperative identification. After establishing
the pneumoperitoneum via the camera port, two additional
8-mm robotic trocars and two assistant trocars (5 mm and
10 mm) were placed.
After initial adhesiolysis, we performed sharp and blunt
dissection using the PK bipolar forceps and monopolar
curved scissors to expose the abdominal surface of the
bladder and the vaginal stump, entering into the vesicovagi-
nal space. After getting good exposition, we opened the
fistula between the bladder and the vagina. The fistula was
finally resected completely including perifistular scar
tissue. Sharp dissection is used to protect the ureteric
orifices and to prevent wide excisions.
The next step was to mobilize the bladder dorsally to get
a tension-free suture. The closure of the vagina was
performed using 2-0 Vicryl. Before the closure of the
bladder, we mobilized the adjacent peritoneum to use it as a
vital layer between the vaginal and bladder sutures. This
peritoneal inlay flap prevents time-consuming mobilization
of the greater omentum as an alternative (Fig. 1). The
bladder was finally closed using 4-0 Biosyn. After a leakage
test of the bladder, we removed all the ports.
The most demanding steps are the preparation of
the fistula and the closing of the vagina and the bladder
as well as harvesting the peritoneal flap. The peritoneal flap
was mobilized from the iliac fossa or from the pararectal
space.
Postoperatively, the wound drain could be removed after
24–48 h. The patients were discharged after 5 d with the
indwelling Foley catheter. After 14 d, cystography was
performed prior to the catheter removal.
Sexual intercourse was prohibited for 4 wk. After a
follow-up period of 4–42 wk, all patients were still
continent and there were no signs of fistula recurrence.

E U R O P E A N U R O L O G Y 6 1 ( 2 0 1 2 ) 2 2 5 – 2 3 1230
Robot-assisted laparoscopic repair with peritoneal flap
inlay seems to be a very promising approach for high
vesicovaginal fistulae.
Conflicts of interest: The authors have nothing to disclose.
References
[1] Melamud O, Eichel L, Turbow B, Shanberg A. Laparoscopic vesicova-
ginal fistula repair with robotic reconstruction. Urology 2005;65:
163–6.
[2] Sundaram BM, Kalidasan G, Hemal AK. Robotic repair of vesico-
vaginal fistula: case series of five patients. Urology 2006;67:970–3.
[3] Hemal AK, Kolla SB, Wadhwa P. Robotic reconstruction for recurrent
supratrigonal vesicovaginal fistulas. J Urol 2008;180:981–5.
[4] Schimpf MO, Morgenstern JH, Tulikangas PK, Wagner JR. Vesico-
vaginal fistula repair without intentional cystotomy using the lapa-
roscopic robotic approach: a case report. JSLS 2007;11:378–80.
Table 1 – Outcomes on positive first and second biopsies
Parameter Positive initial biopsy
n = 3669
Age, median (IQR) 65.0 (9.0)
PSA, median (IQR) 6.54 (3.00)
Volume, median (IQR) 43.0 (26.0)
TRUS volume, n (%)
<30 607 (17.1)
30–49 1635 (46.2)
50–70 776 (21.9)
�70 523 (14.8)
Gleason grade, n (%)
6 1693 (46.1)
7 1479 (40.3)
�8 497 (13.5)
Low risk, n (%) 865 (23.6)
IQR = interquartile range; PSA = prostate-specific antigen; TRUS = transrectal ultra Wilcoxon rank-sum test.b Chi-square test.
[5] Engel N, John H. Laparoscopic robot assisted vesico-vaginal fistula
repair with peritoneal flap inlay [abstract]. J Urol 2008; 179(Suppl 4):
666.
Michael Kurz
Marcus Horstmann
Hubert John*
Kantonsspital Winterthur, Division of Urologic Surgery, Brauerstrasse 15,
Winterthur 8401, Switzerland
*Corresponding author
E-mail address: [email protected] (H. John)
September 25, 2011
Published online ahead of print October 3, 2011
doi:10.1016/j.eururo.2011.09.022
Does Low-Risk Prostate Cancer Detection Change With
Repeat Biopsies?
Many patients with a negative prostate biopsy (PBx) but
persistent clinical suspicion of prostate cancer (PCa)
undergo repeat PBx. On repeat PBx, there are higher rates
of low-grade and organ-confined PCa, which are associated
with lower risk of disease progression and cancer-specific
mortality [1,2]. Increasing emphasis is being placed on
treating only clinically significant disease [1]. We hypothe-
size that a considerable risk of clinically significant
PCa remains on repeat PBx. Therefore, we reviewed a
contemporary cohort of patients who underwent one or
more PBx.
We retrospectively reviewed the data from a cohort of
25 584 patients who underwent PBx at two institutions.
One dedicated uropathologist evaluated 90% of PBx speci-
mens; the remaining specimens were evaluated by two
other uropathologists. To ensure current pathologic grading
standards, the study was limited to patients biopsied from
2004 to 2010. Only patients with at least 10 cores taken
were included. Statistical analysis was performed using
SPSS v.17.0 (SPSS Inc., IBM Corp., Armonk, NY, USA).
Descriptive statistics are reported as medians with inter-
quartile ranges (IQRs). All tests were two-sided, and a
p value of 0.05 was considered statistically significant.
Of 25 584 patients, 6729 met the inclusion criteria, and
764 (11.3%) of those underwent a second PBx after negative
initial biopsy. The median age was 65 yr (IQR: 9.0), prostate-
specific antigen (PSA) was 6.20 ng/ml (IQR: 4.79), and
prostate volume was 47 ml (IQR: 30). Overall, 3671 (54.6%)
men were diagnosed with PCa on first PBx, whereas 199
Positive second biopsy p
n = 199
66.0 (9.25) >0.05a
7.26 (5.02) >0.05a
47.5 (30.0) <0.01a
<0.01b
21 (11.5)
71 (38.8)
50 (27.3)
41 (22.4)
<0.01b
121 (60.8)
60 (30.2)
18 (9.0)
72 (36.2) <0.01b
asound.