Embed Size (px)
Citation preview

Rotational and AngularDeformities in Children
February 9th 2012
Lauren Cochran MD
Knock Knees & Pigeon Toes
To-Do
• Search PREP for more questions?
• Email Myra to ensure no Mac-to-PC glitches?
• Summary slide / reasons to refer
• Clean up references slide

Objectives
• To review the common causes of intoeing & outtoeing in children
• To describe the progression of normal physiologic alignment over time & how to evaluate a child with genu varum or genu valgum
• To describe the physical examination techniques used in assessing rotational and angular deformities
• To review indications for imaging and/or Orthopedics referral
4 Categoriesof Lower Extremity Problems
• Rotational Deformities• Intoeing (“Pigeon Toes”)• Outtoeing
• Angular Deformities• Genu Varum (“Bow legs”)• Genu Valgum (“Knock knees”)
• Foot Deformities (e.g., clubfoot & pes planus)• Hip Disorders (e.g., DDH & SCFE)

Intoeing
Intoeing
• Often raised as concern by parents
• Sometimes associated with tripping/falling
• Possible origin:• Foot = metatarsus adductus
• Between knee & ankle = internal tibial torsion
• Between hip & knee = medial femoral torsion
Metatarsus Adductus

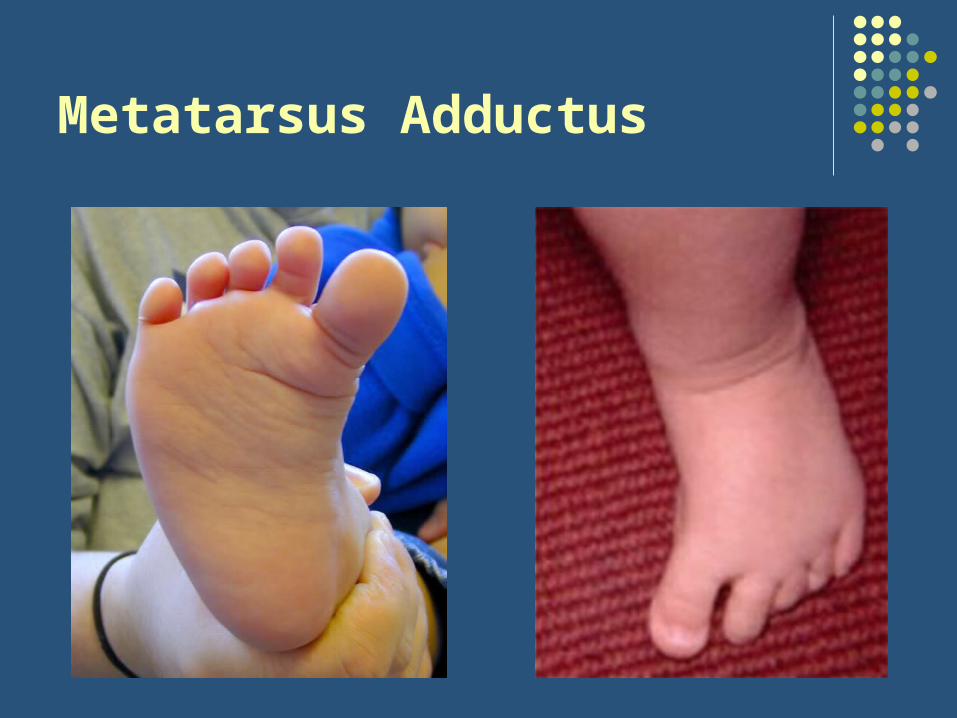
Metatarsus Adductus (MTA)
• “Packaging Defect” (1st born children at higher risk)
• Tarsal & phalangeal bones angled toward midline
• + convex lateral curvature of foot
• + medial instep crease
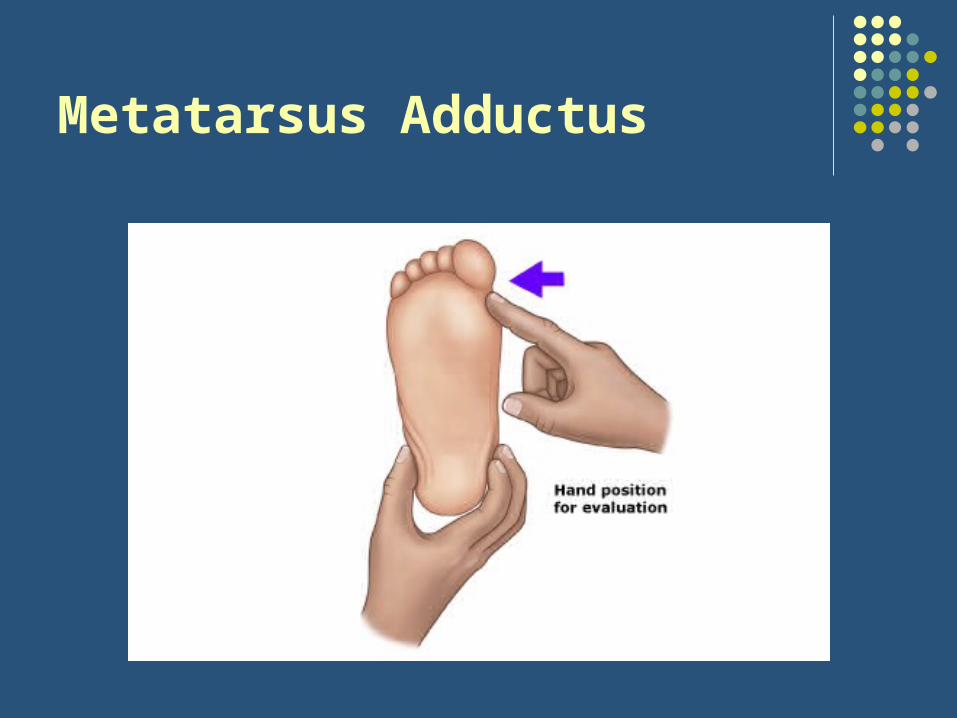
• Evaluation includes:
• Degree of adduction (heel bisector)
• Degree of flexibility

Metatarsus Adductus

Heel Bisectors
Heel Bisectors

Metatarsus Adductus
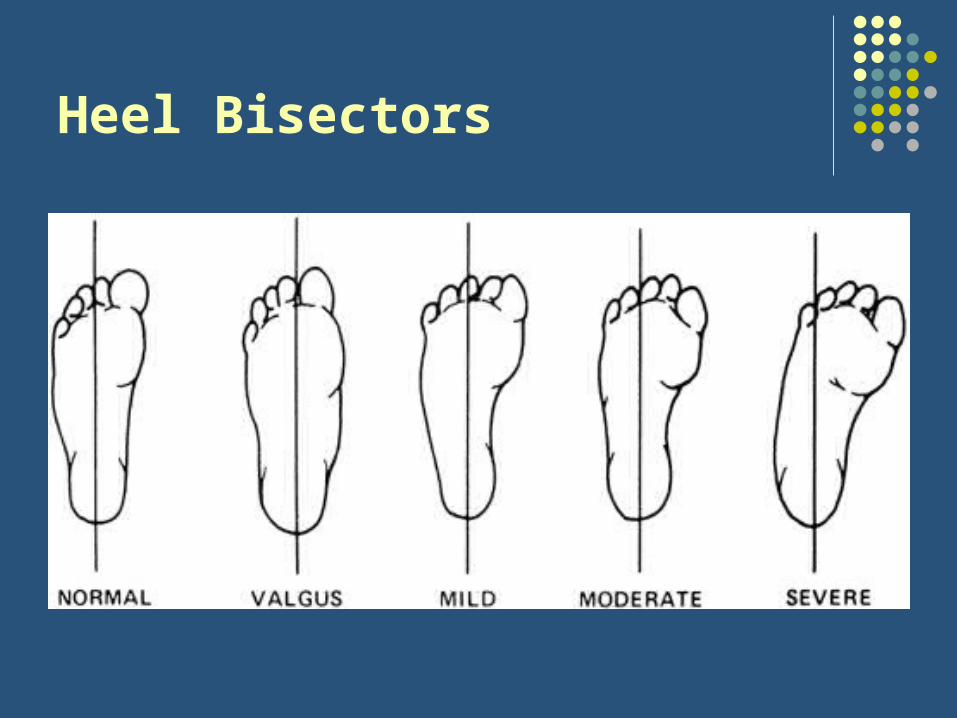
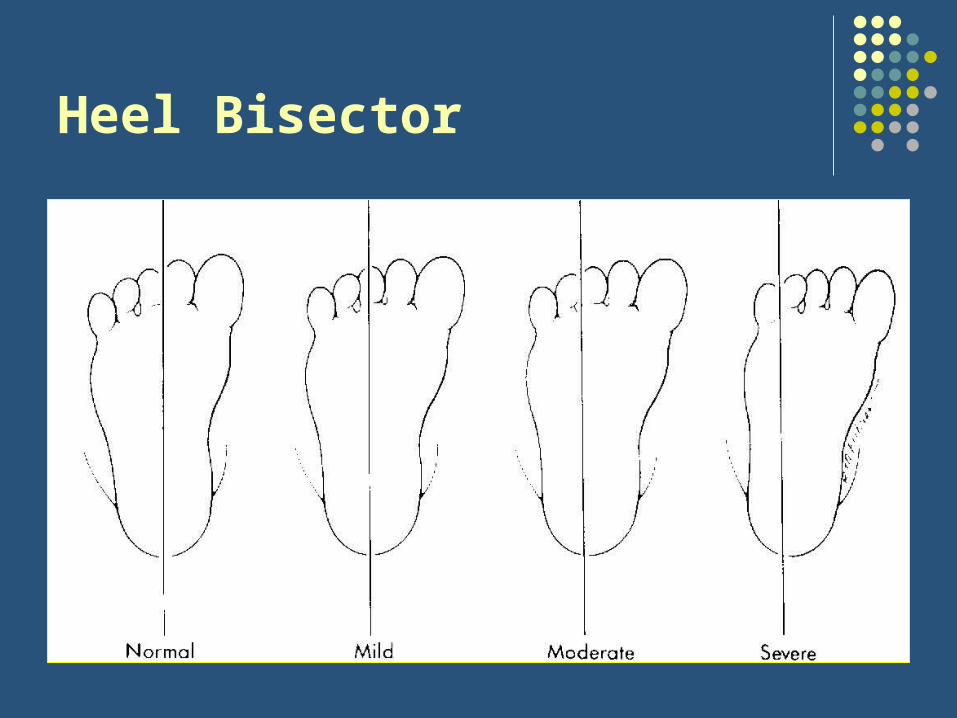
• Heel bisector (quantifies degree of adduction):
• Normal: between 2nd/3rd toes
• Mild MTA: 3rd toe
• Moderate MTA: 3rd/4th toe
• Severe MTA: 4th/5th toe

Metatarsus Adductus
• Degree of Flexibility determines need for treatment!
• Actively correctable: tickle foot on lateral border no treatment required
• Passively correctable: gentle lateral pressure to 1st metatarsal head “stretching” 10sec per foot x5 with each diaper change REFER if not corrected by 4-6mo
• Rigid: REFER for possible casting/bracing
Metatarsus Adductus
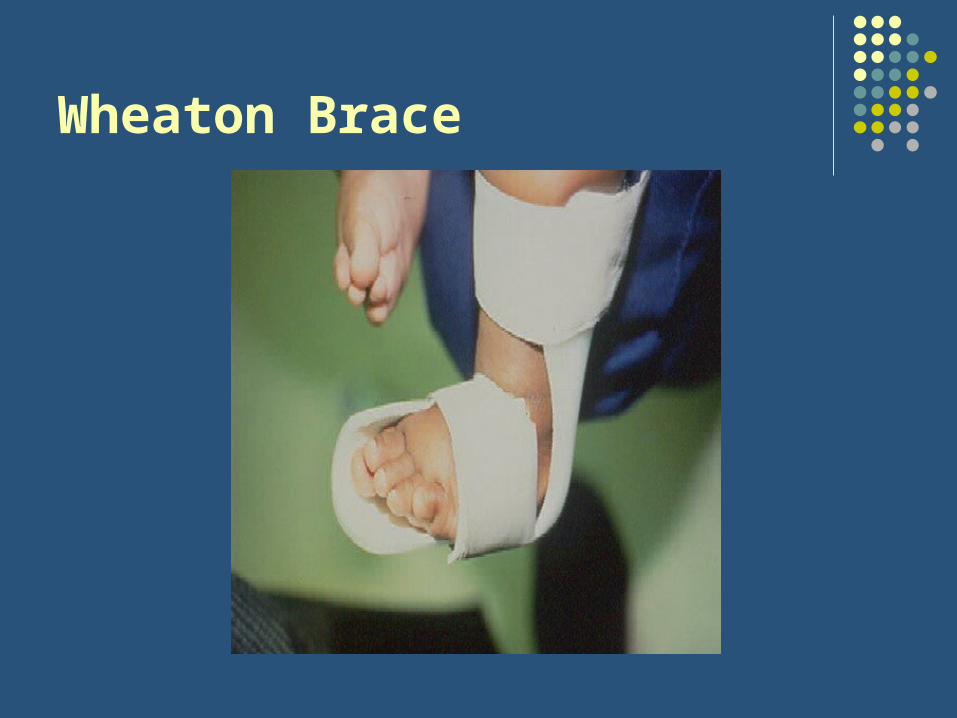
Wheaton Brace

Metatarsus Adductus & DDH?
• Previously reported association between MTA & DDH now disputed
• Still warrants careful hip exam
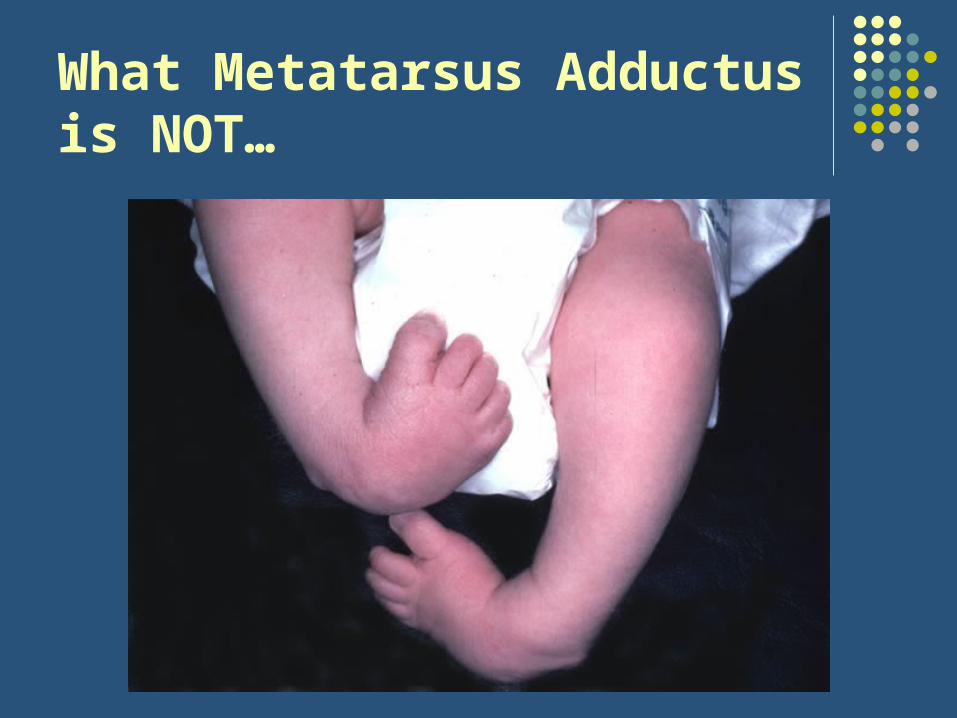
What Metatarsus Adductusis NOT…
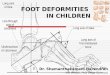
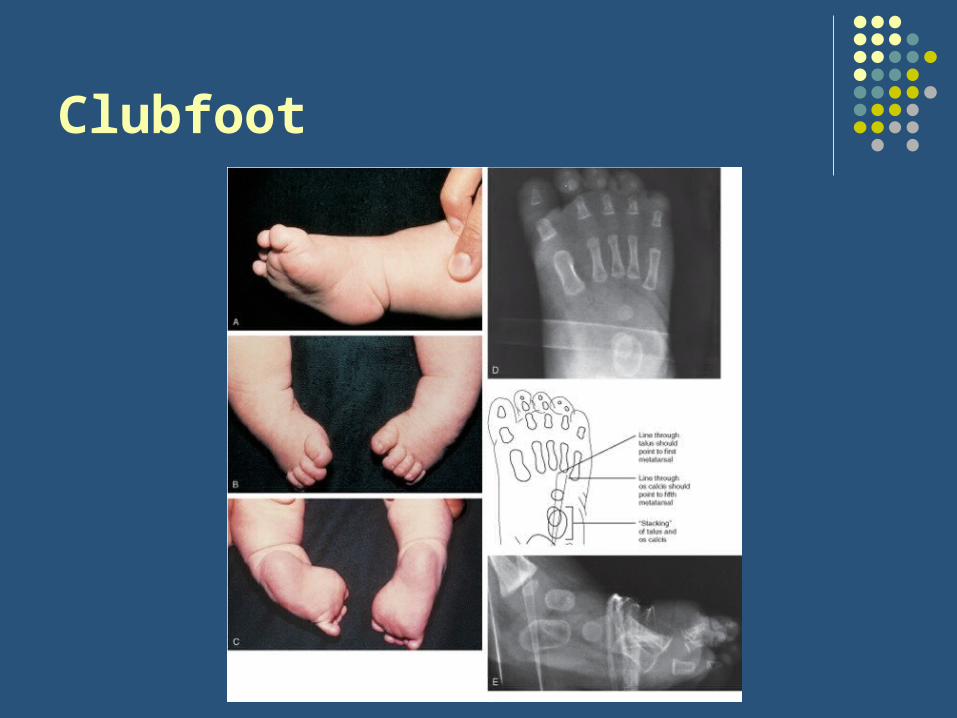
Clubfoot
• aka talipes equinovarus
• Constellation of metatarsus adductus PLUS:• Equinus positioning = inability to dorsiflex foot
(shortening of gastroc/soleus & tendon)
• Hindfoot varus (supination)
• Inversion of the forefoot
• Warrants early referral to Orthopedist
• Famous athletes with clubfoot: Troy Aikman, Kristi Yamaguchi, Mia Hamm
Clubfoot

Where’s the Intoeing Origin?
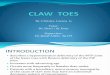
Internal Tibial Torsion
• Origin of intoeing between knee & ankle
• Most common intoeing etiology for children less than 3yrs
• “Packaging defect” present from birth but often noticed only when child begins to stand/walk
• Almost never requires treatment:
• Most cases gradually resolve by age 2-3yrs
• REFER if persists beyond age 6
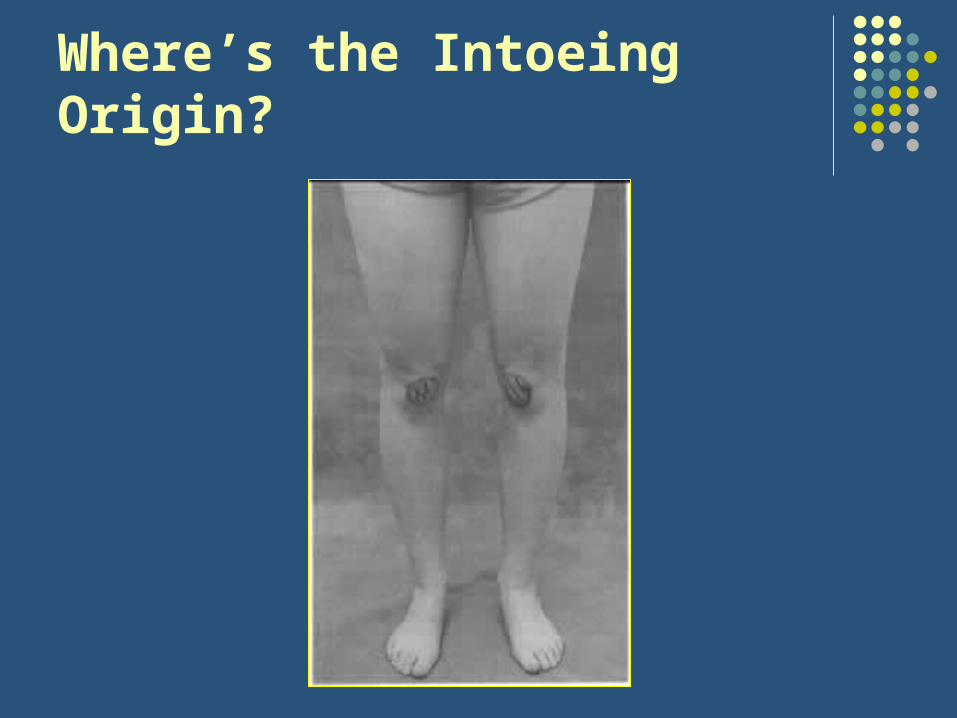
Where’s the Intoeing Origin?

Medial Femoral Torsion
• Origin of intoeing between hip & knee
• aka “femoral anteversion” but to a pathologic degree (> 60-65)
• Most common intoeing etiology for children older than 3yrs
• Associated with “W sitting position” (unclear effect on progression/outcome)
• “Egg beater” or “windmill” running pattern
• Almost always corrects gradually by age 10

Medial Femoral Torsion

W Sitting Position

“Kissing Patellae”
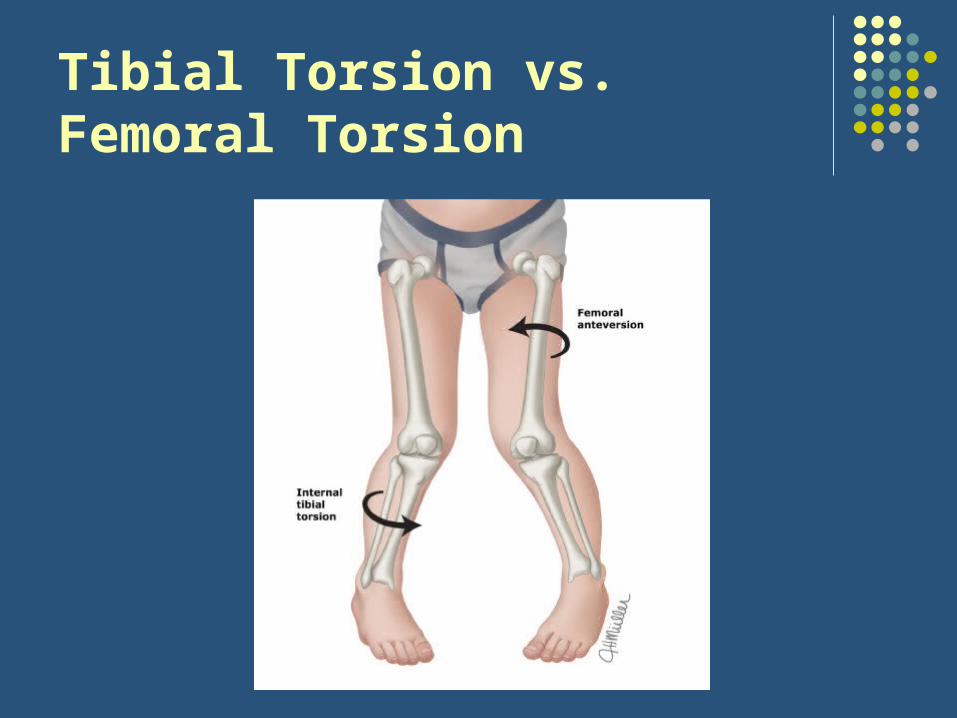
Tibial Torsion vs.Femoral Torsion
Intoeing: H&P
• HPI: onset, progression, pain, disability, previous evaluation/treatment
• Development: particularly gross motor milestones including walking
• General screening exam:• Growth parameters• Evaluation for DDH (Ortolani/Barlow, Galeazzi, skin fold
asymmetry)• Basic neurological exam (UE+LE reflexes, ankle clonus,
heel/toe walking)
Intoeing: “Rotational Profile”
1. Foot progression angle
2. Heel bisector
3. Thigh foot angle
4. Hip rotation
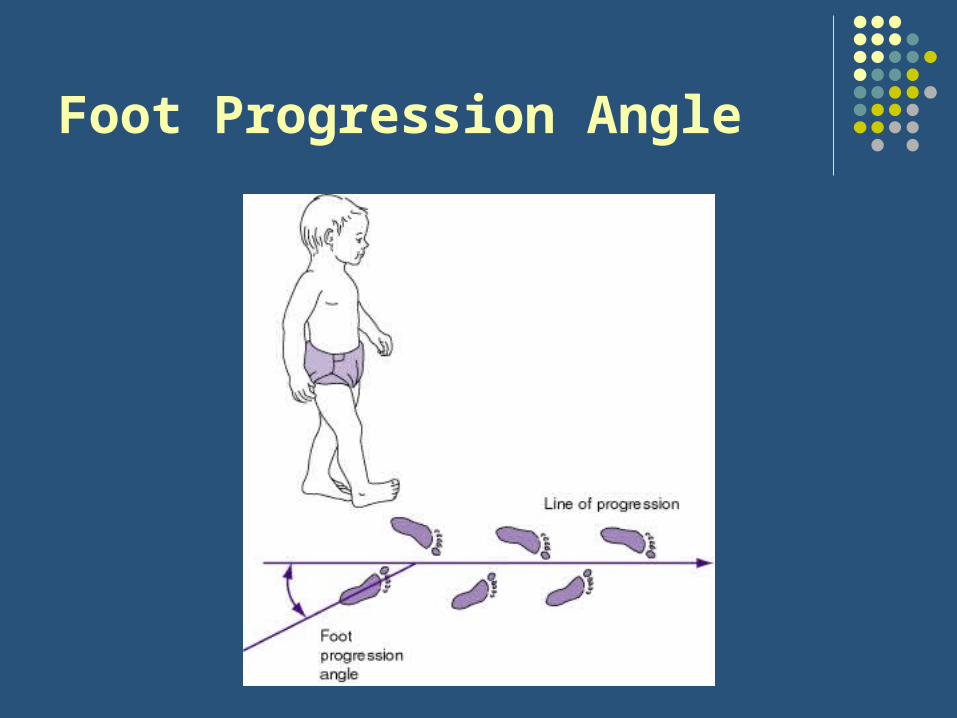
Foot Progression Angle
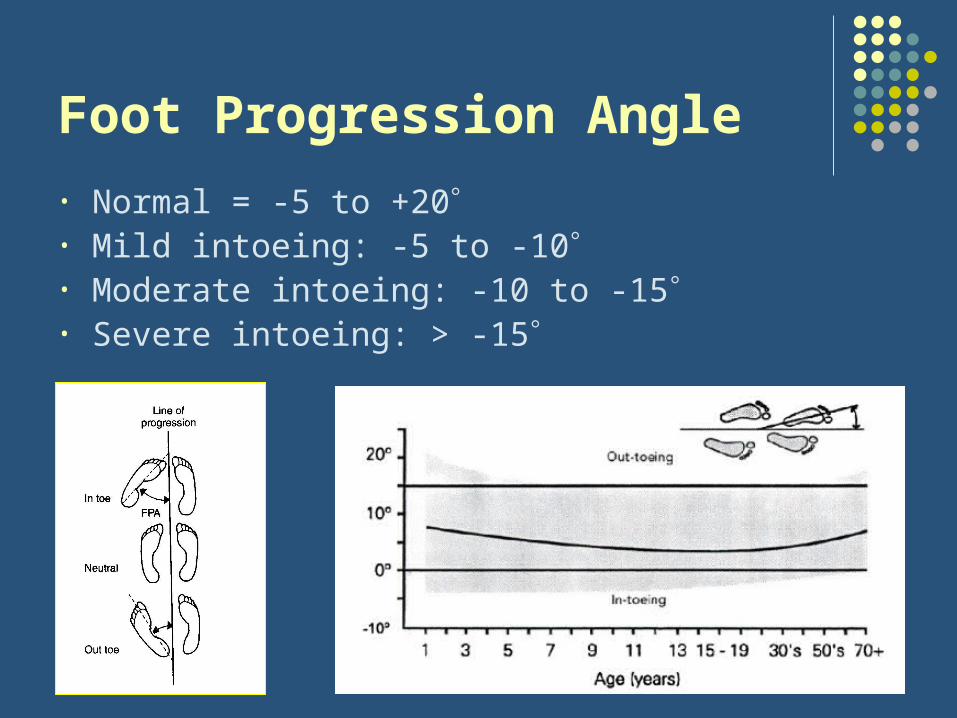
Foot Progression Angle
• Normal = -5 to +20• Mild intoeing: -5 to -10• Moderate intoeing: -10 to -15• Severe intoeing: > -15
Heel Bisector

The V-Finger Test
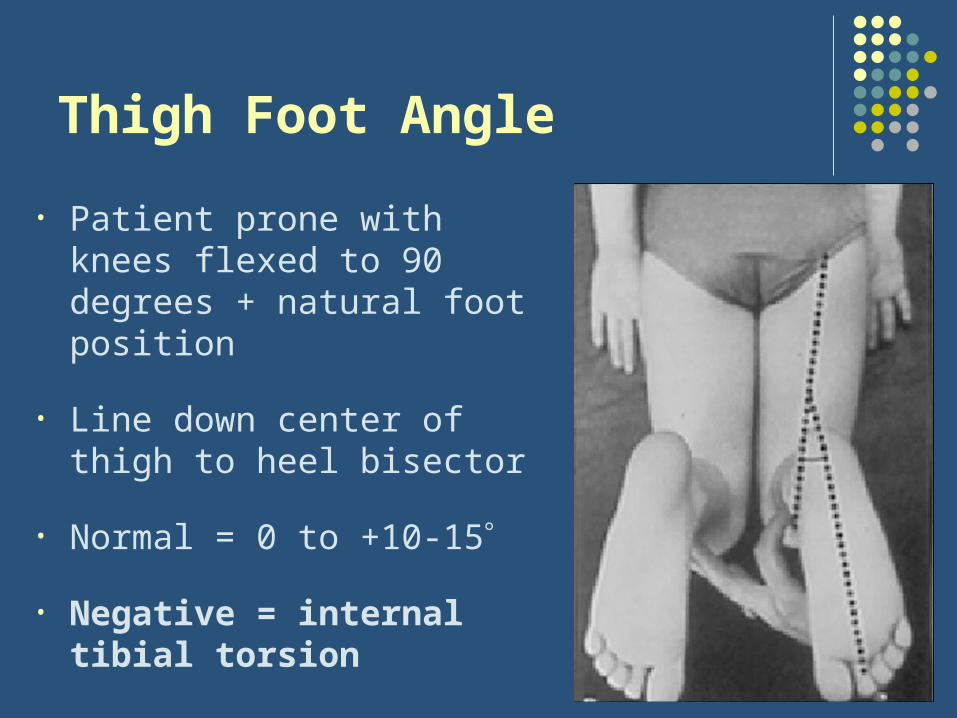
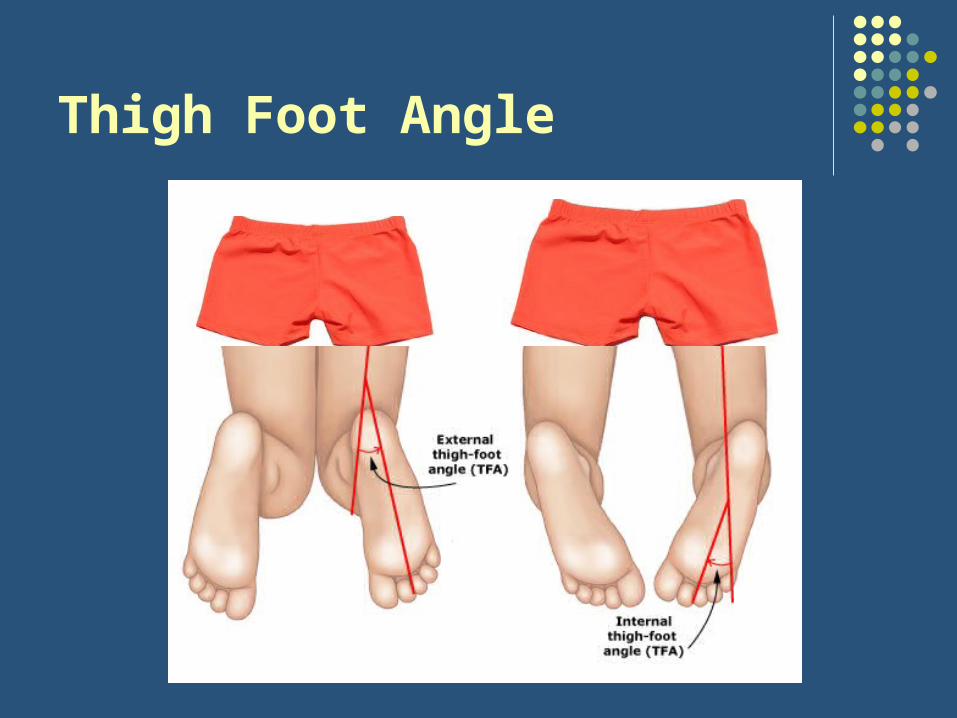
Thigh Foot Angle
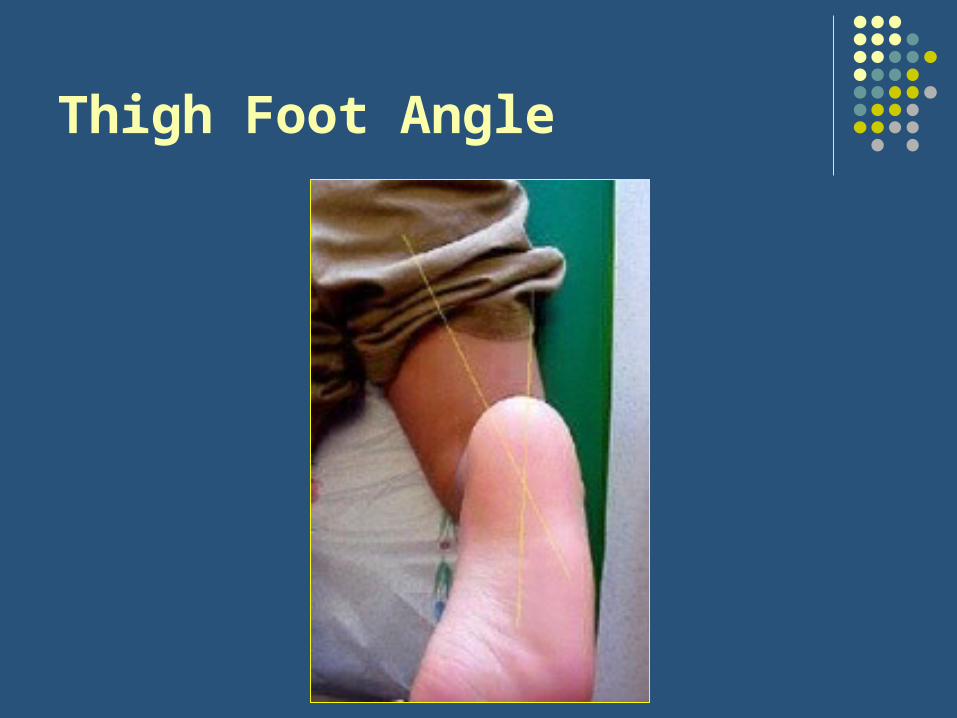
• Patient prone with knees flexed to 90 degrees + natural foot position
• Line down center of thigh to heel bisector
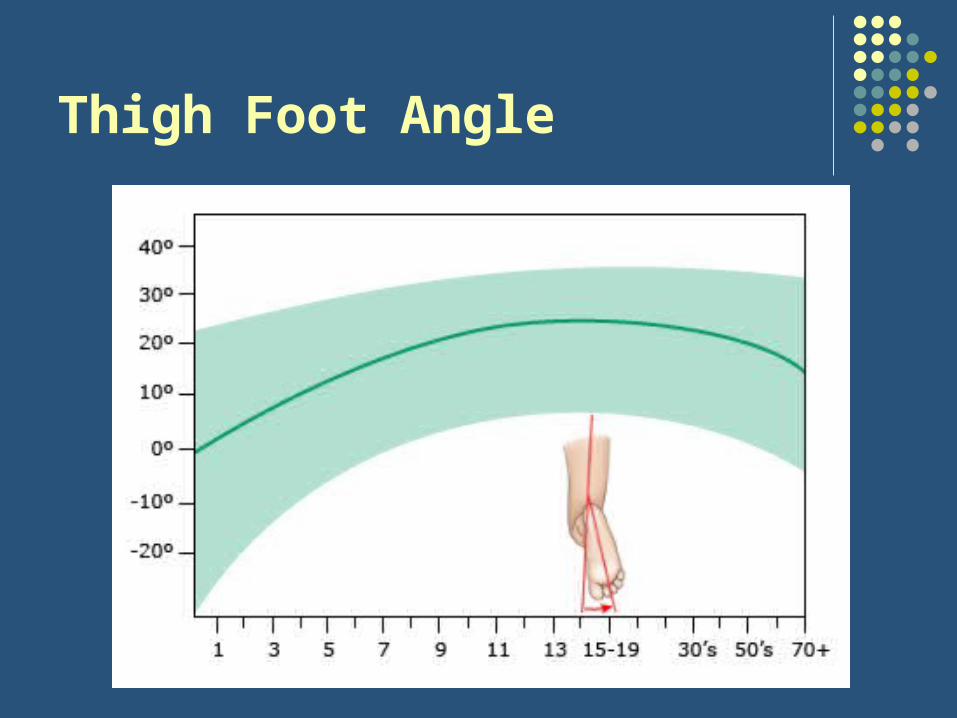
• Normal = 0 to +10-15
• Negative = internal tibial torsion
Thigh Foot Angle
Thigh Foot Angle
Thigh Foot Angle

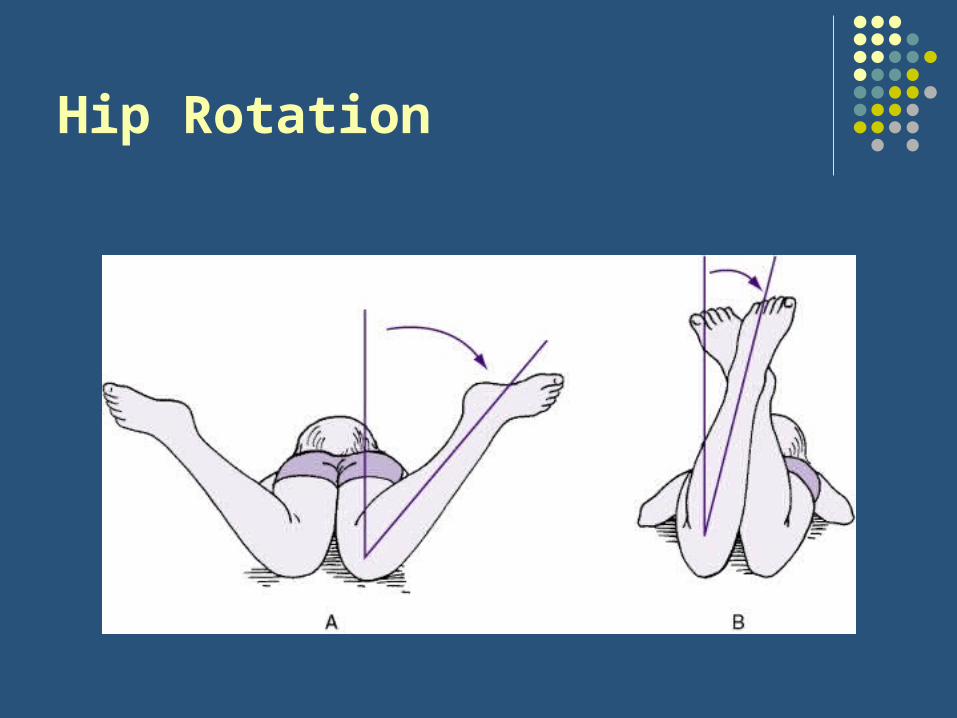
Hip Rotation
• Child is prone with knees flexed to 90• Assess both sides simultaneously• Normal (varies by age): ~-45 to +45
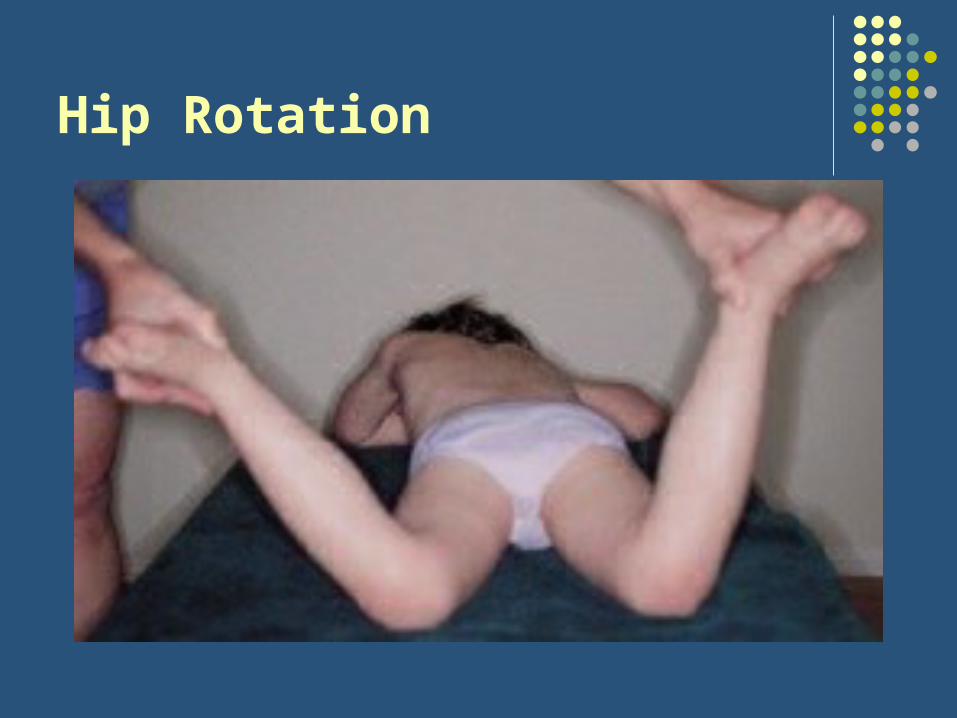
Hip Rotation

Hip Rotation
• If asymmetric get XR (AP pelvis AP) to evaluate for DDH or other hip problem
• Increased internal rotation > 60-65 = femoral anteversion• > 80 = moderate• > 90 = severe
Hip Rotation
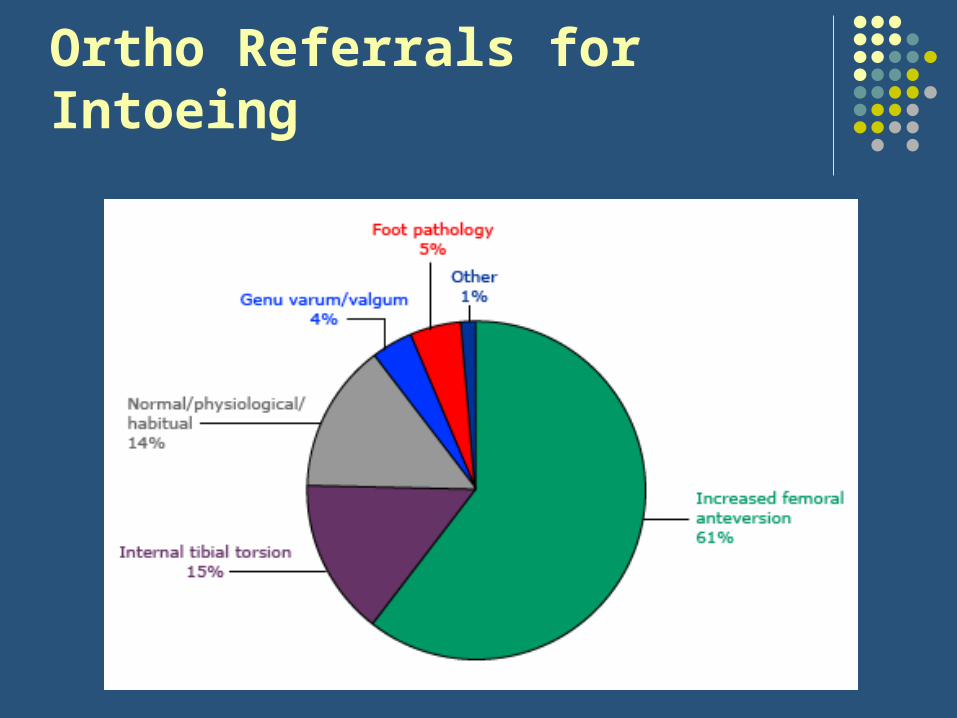
Ortho Referrals for Intoeing

Benefits of Intoeing?
Some evidence that persistent intoeing is actually beneficial for some sports that require quick directional shifts:
Tennis
Basketball
Soccer
Etc.
Outtoeing
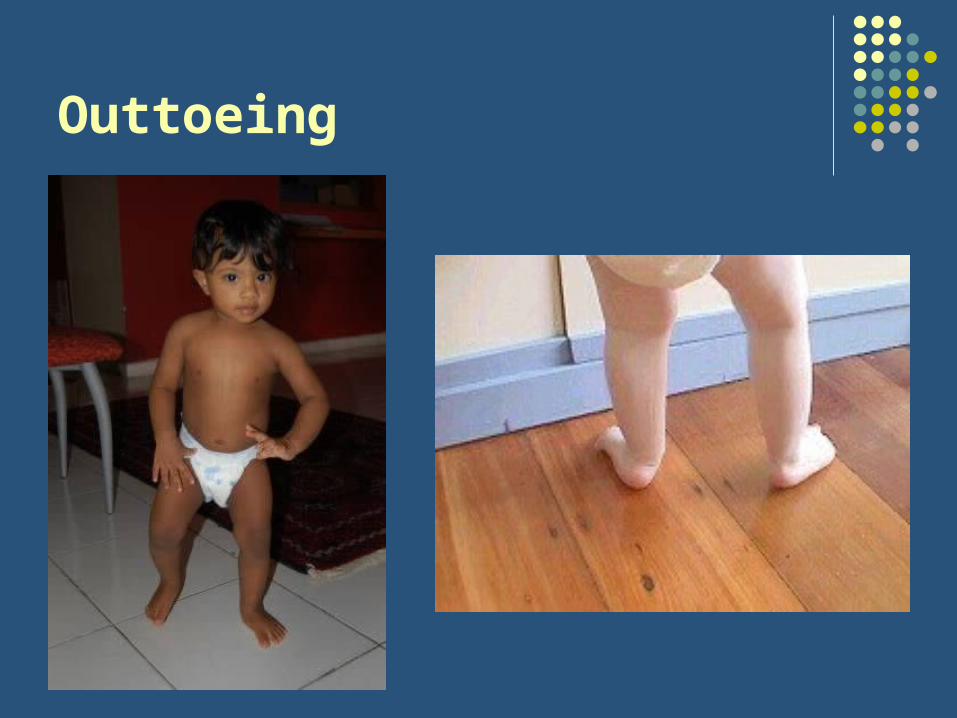
Outtoeing
• Much less common than intoeing
• Origin:• Foot: Calcaneovalgus deformity
• Between knee & ankle: External tibial torsion
• Between hip & knee: Femoral retroversion
• Hip: External rotation contracture
• Most cases resolve within first 1-2yrs of ambulation
Calcaneovalgus Foot
• Hyperdorsiflexion of foot
• Abduction of forefoot
• Forefoot often rests on anterior surface of leg
• REFER for casting if foot cannot be plantar-flexed below neutral

Calcaneovalgus Foot

Calcaneovalgus Foot
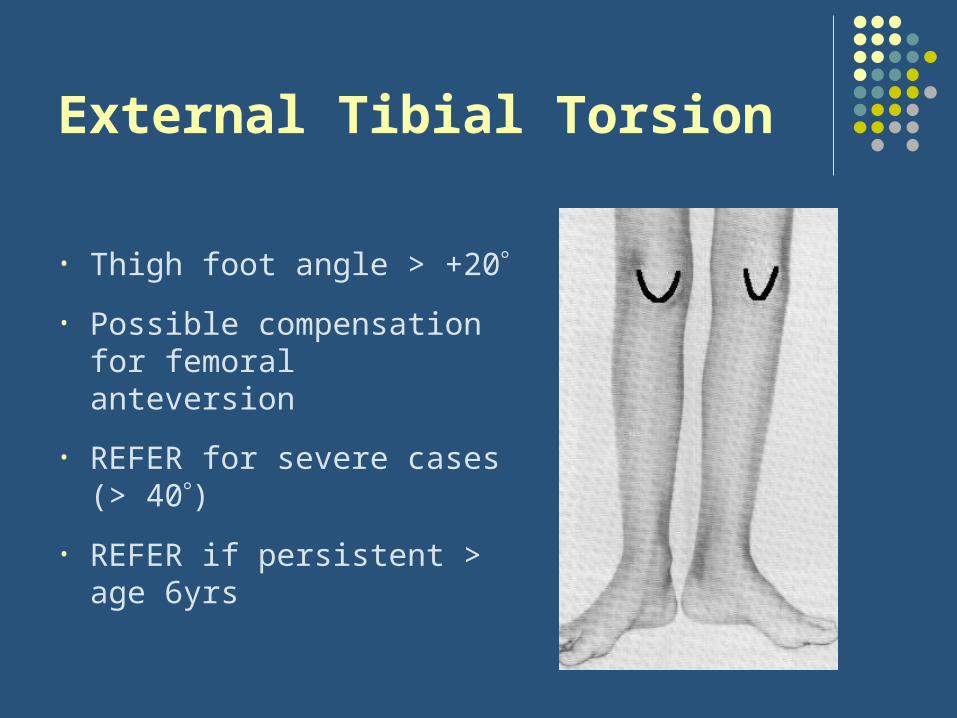
External Tibial Torsion
• Thigh foot angle > +20
• Possible compensation for femoral anteversion
• REFER for severe cases (> 40)
• REFER if persistent > age 6yrs

External Tibial Torsion
Femoral Retroversion
• Rare cause of outtoeing
• Characterized by increased external rotation (and decreased internal rotation) at the hip
• Associated with obesity
• Possibly associated with osteoarthritis, stress fractures, and SCFE
External Rotation Contracture
• Normal intrauterine position = flexed and externally rotated hips
• May result in external rotation contracture
• Usually resolves spontaneously by 12 months of age (or when child begins to walk)

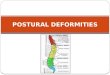
Angular Deformities
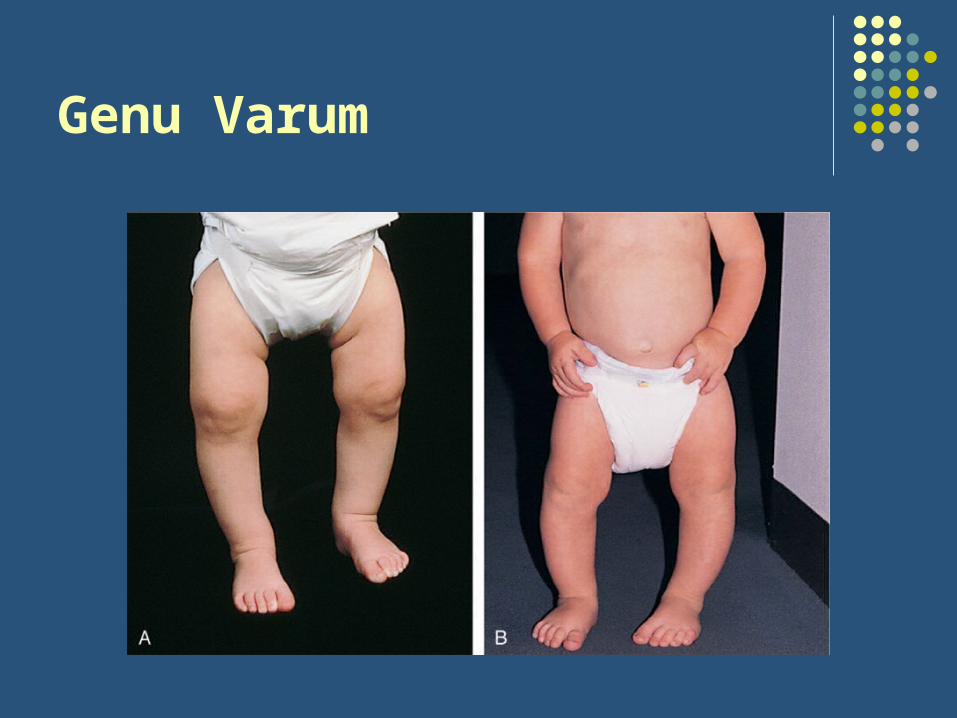
Genu Varum
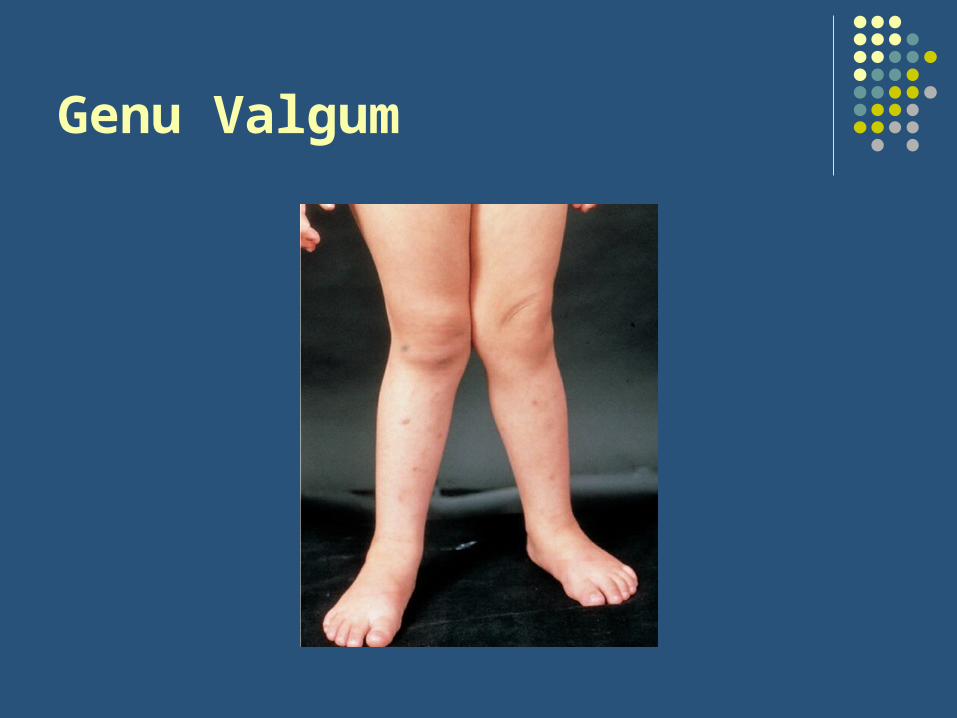
Genu Valgum
Mnemonics
• Varus = “vAIRus” (more air between the legs)
• Valgus Gum (knees stick together)

Normal Progression
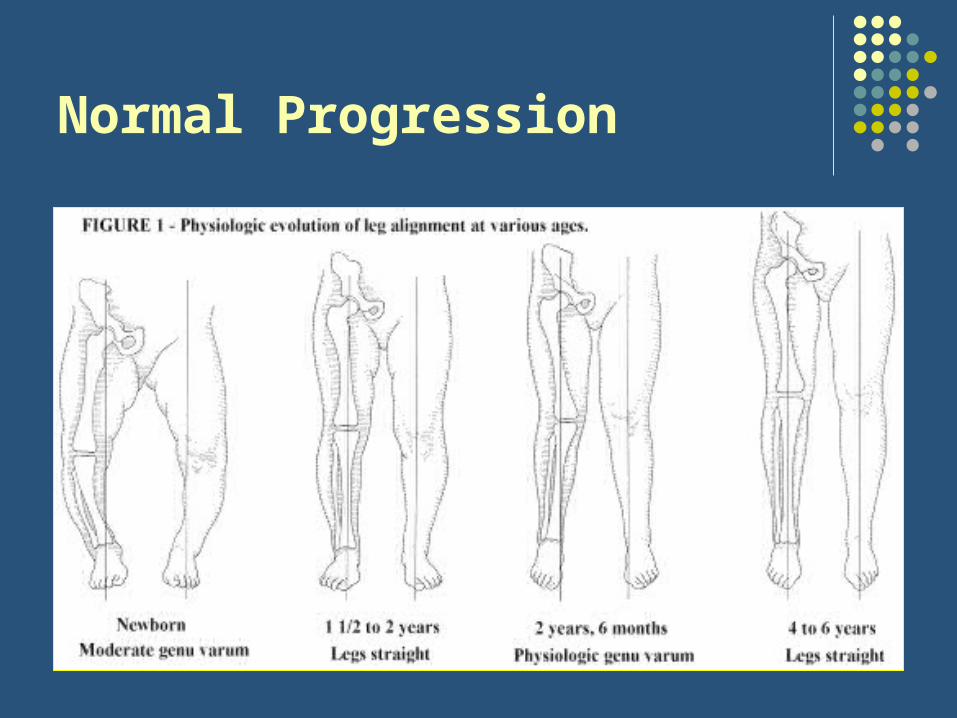
Normal Progression
Normal Progression
• Birth: genu varum improves by age 2
• Age 3: genu valgum improves by age 6-7
• Can monitor over time with distance between• knees w/ ankles together (genu varum)• ankles w/ knees together (genu valgum)
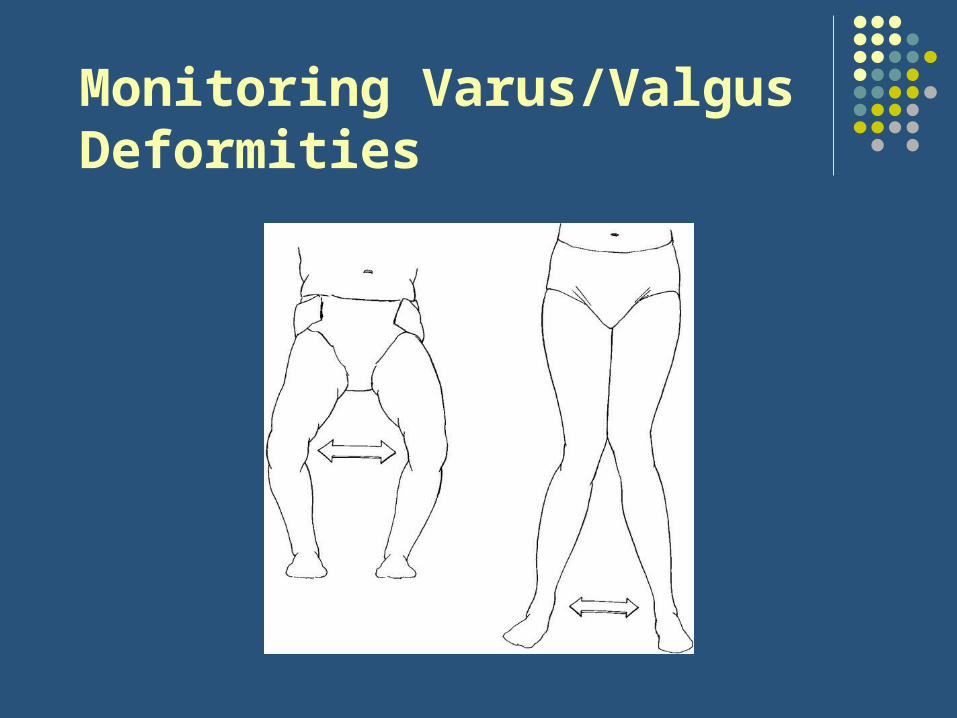
Monitoring Varus/Valgus Deformities

Measurement: Genu _____
When to Work Upand/or Refer?
• Asymmetry (or Unilateral)
• Associated with pain
• Associated with short stature
• Associated with poor nutrition
• Progression defers from expected
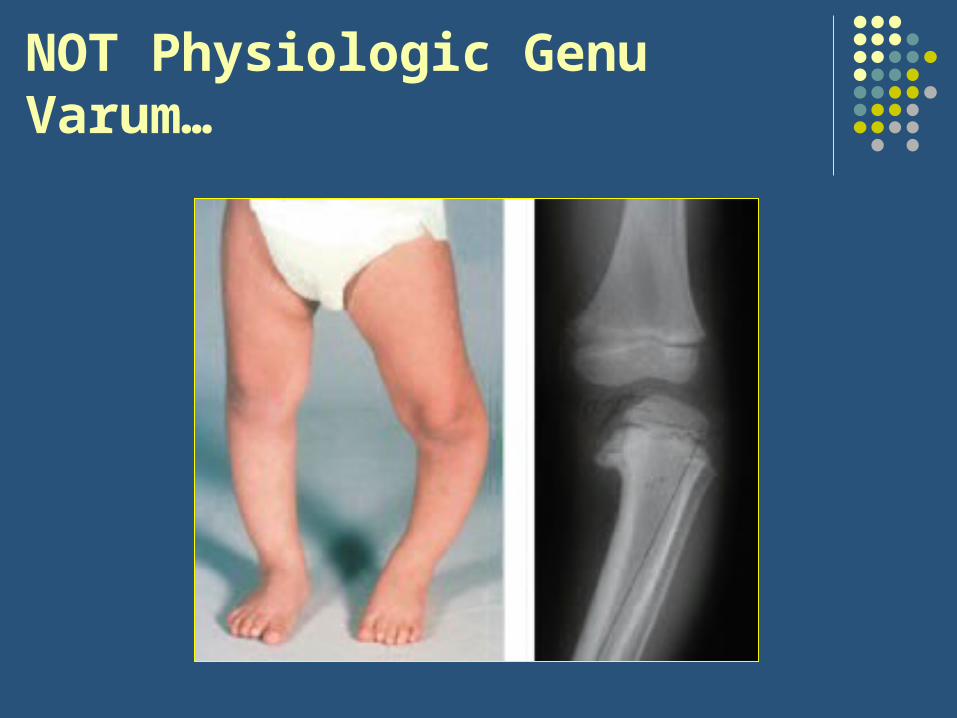
NOT Physiologic Genu Varum…
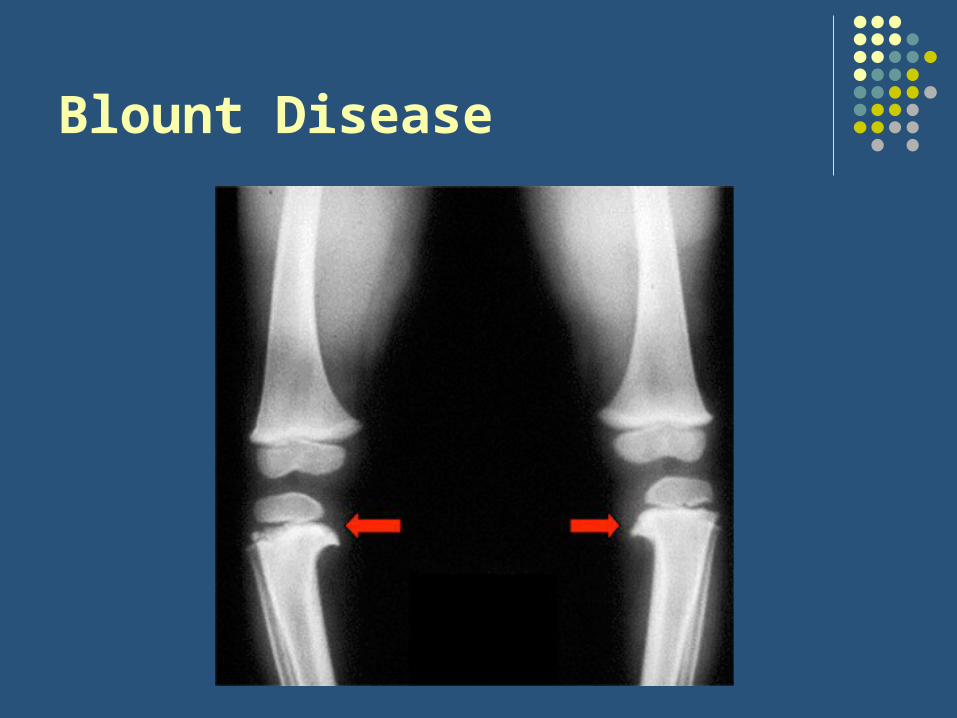
Blount Disease• Pathologic varus deformity due to disruption of normal
cartilage at the proximal tibial physis (medial aspect)
• Infantile & adolescent types
• Differentiate from physiologic genu varum based on:• Atypical age/progression
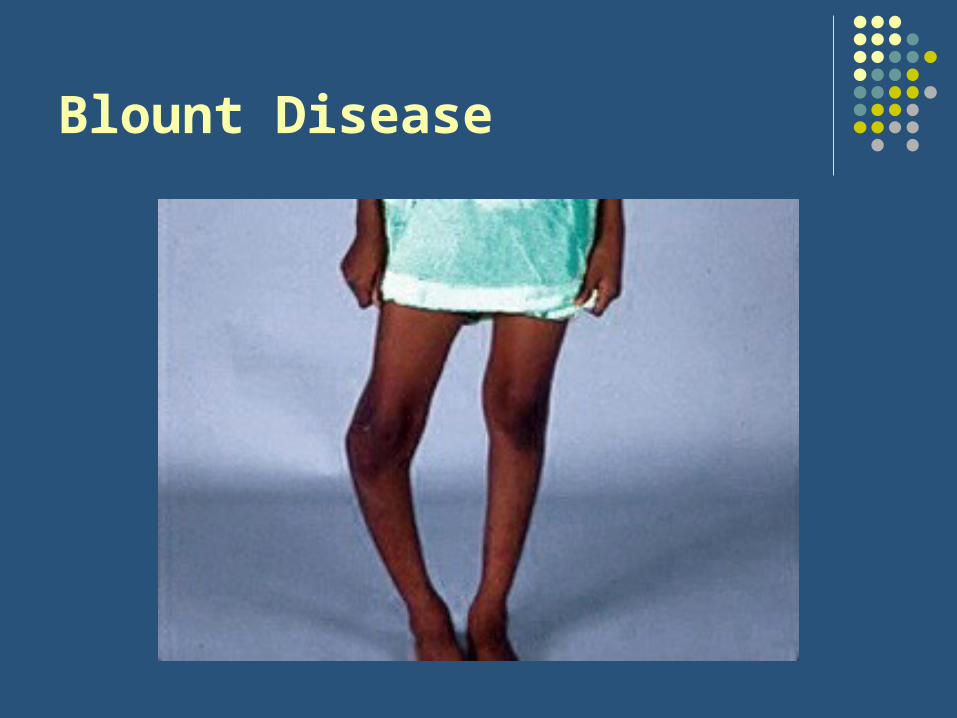
• Asymmetry
• “Lateral thrust” with ambulation
• Focal angulation at proximal tibia
• Risk factors: early walking, obesity, African American heritage, + family history
• If any doubt get an x-ray!
Blount Disease
Blount Disease

NOT Physiologic Genu Valgum…

Rickets
• Deficient growth plate mineralization associated with insufficient Ca/Phos
• Differentiate from physiologic genu valgum or genu varum based on:• Atypical age/progression
• Short stature (<10%ile for age)
• Poor nutrition
• Associated findings like frontal bossing, craniotabes, costochondral swelling (aka rachitic rosary), wrist widening
PREP Question #1
You are seeing a child born at home for the first time at his 2-week health supervision visit. The mother’s primary concern is the shape of her son’s foot. The best maneuver to differentiate metatarsus adductus from clubfoot is to:
a) Abduct the forefoot
b) Compare the appearance of the feet
c) Dorsiflex the ankle
d) Look for a transverse crease on the plantar surface
e) Tickle along the lateral aspect of the foot
PREP Question #1
You are seeing a child born at home for the first time at his 2-week health supervision visit. The mother’s primary concern is the shape of her son’s foot. The best maneuver to differentiate metatarsus adductus from clubfoot is to:
a) Abduct the forefoot
b) Compare the appearance of the feet
c) Dorsiflex the ankle
d) Look for a transverse crease on the plantar surface
e) Tickle along the lateral aspect of the foot

PREP Question #2
A 5-year-old girl continues to “intoe,” although this has no impact on her level of activity or function and she is otherwise healthy. The most likely cause for this condition is:
a) Femoral anteversionb) Malignant malalignment syndromec) Metatarsus adductusd) Talipes equinovaruse) Tibial torsion
PREP Question #2
A 5-year-old girl continues to “intoe,” although this has no impact on her level of activity or function and she is otherwise healthy. The most likely cause for this condition is:
a) Femoral anteversionb) Malignant malalignment syndromec) Metatarsus adductusd) Talipes equinovaruse) Tibial torsion
PREP Question #3
A 3-year old girl is “bowlegged,” and because her mother is certain that it is getting worse, she requests an immediate radiograph. The finding that would best support the parent’s request is:
a) A “bowlegged” appearance at birth
b) A normal sequence of achieving motor milestones
c) A symmetric appearance to the lower extremities
d) The absence of pain in the lower extremities
e) The natural history of angular deformities in the lower extremities

PREP Question #3
A 3-year old girl is “bowlegged,” and because her mother is certain that it is getting worse, she requests an immediate radiograph. The finding that would best support the parent’s request is:
a) A “bowlegged” appearance at birth
b) A normal sequence of achieving motor milestones
c) A symmetric appearance to the lower extremities
d) The absence of pain in the lower extremities
e) The natural history of angular deformities in the lower extremities
PREP Question #4
Which of the following is a characteristic of metatarsus adductus?
a) Hindfoot equinus deformityb) Hindfoot varus deformityc) Hindfoot valgus deformityd) Lateral deviation of the forefoote) Medial crease of the instep
PREP Question #4
Which of the following is a characteristic of metatarsus adductus?
a) Hindfoot equinus deformityb) Hindfoot varus deformityc) Hindfoot valgus deformityd) Lateral deviation of the forefoote) Medial crease of the instep
PREP Question #5 A 7-year-old girl is brought to your clinic for in-toeing that has
persisted since she was about 3 years of age. She frequently sits in a “W” pattern on the floor while watching television. Physical examination reveals markedly increased internal rotation of the hips while prone. Which of the following statements regarding his girl’s condition is true?
a) Computed tomography scan is indicated to confirm the diagnosis
b) She is at high risk of developing osteoarthritis of the hips later in life
c) She likely will be able to participate in spots without difficulty
d) She should begin wearing medial pads in her shoes to correct the in-toeing
e) The in-toeing likely is due to a dietary deficiency
PREP Question #5 A 7-year-old girl is brought to your clinic for intoeing that has
persisted since she was about 3 years of age. She frequently sits in a “W” pattern on the floor while watching television. Physical examination reveals markedly increased internal rotation of the hips while prone. Which of the following statements regarding his girl’s condition is true?
a) Computed tomography scan is indicated to confirm the diagnosis
b) She is at high risk of developing osteoarthritis of the hips later in life
c) She likely will be able to participate in spots without difficulty
d) She should begin wearing medial pads in her shoes to correct the in-toeing
e) The in-toeing likely is due to a dietary deficiency

PREP Question #6
You are evaluating an 18-month-old boy whose mother thinks he is “pigeon-toed”. He began walking at 12 months and walks well, but in-toeing is noted on examination. Range of motion at the hips, knees, and ankles is normal. Which of the following is the most likely cause of his gait disturbance?
a) Blount diseaseb) Femoral anteversionc) Internal tibial torsiond) Metatarsus adductuse) Pes planus

PREP Question #6
You are evaluating an 18-month-old boy whose mother thinks he is “pigeon-toed”. He began walking at 12 months and walks well, but in-toeing is noted on examination. Range of motion at the hips, knees, and ankles is normal. Which of the following is the most likely cause of his gait disturbance?
a) Blount diseaseb) Femoral anteversionc) Internal tibial torsiond) Metatarsus adductuse) Pes planus
Summary?
• Most intoeing, outtoeing, knock knees, and bow legs are NORMAL & require only reassurance and observation
• BUT… don’t want to miss clubfoot, DDH, CP, rickets, Blount disease
• Systemic approach to exam
Reasons to Refer• Rigid metatarsus adductus, which may require serial casting (refer to pediatric
orthopedic surgeon or an orthopedic surgeon with expertise in rotational problems)
• Unilateral or asymmetric in-toeing associated with clinical findings suggestive of neurologic disorder (refer to a pediatric orthopedic surgeon, pediatric neurologist, or physical medicine and rehabilitation specialist)
• Children ≥8 years with activity limiting or cosmetically unacceptable in-toeing due to internal tibial torsion (may be candidates for derotational osteotomy; refer to an orthopedic surgeon with expertise in rotational problems)
• Children ≥11 years with activity limiting or cosmetically unacceptable in-toeing due to increased femoral anteversion (may be candidates for derotational osteotomy; refer to an orthopedic surgeon with expertise in rotational problems)
• In-toeing that does not follow the expected course (eg, increased femoral anteversion that progresses after age five or six years) [16] (refer to pediatric orthopedic surgeon or an orthopedic surgeon with expertise in rotational
problems)

References
• Scherl SA. Common lower extremity problems in children. Pediatr Rev. 2004;25(2):52-62.
• Smith BG. Lower extremity disorders in children and adolescents. Pediatr Rev. 2009;30(8):287-301.
• Grottkau BE. Intoeing, outtoeing, and limping: making sense of common pediatric gait abnormalities.
• UpToDate: Lower extremity positional deformations; Approach to the child with in-toeing; Approach to the child with outtoeing; Approach to the child with bow legs

Thank You!