Embed Size (px)
Citation preview

RV
DVMa
b
c
d
a
KLDEHR
1
te5cdib
uP
Pc
Rb
Ho
0d
Vaccine 27S (2009) F85–F88
Contents lists available at ScienceDirect
Vaccine
journa l homepage: www.e lsev ier .com/ locate /vacc ine
otavirus diarrhoea among children aged less than 5 years at Mahosot Hospital,ientiane, Lao PDR�,��
ouangdao Souk Alouna, Batmunkh Nyambatd,∗, Rattanaphone Phetsouvanhb,annida Douangbouphaa, Phonesavanh Keonakhonea, Bandit Xoumphonhphakdya,anivanh Vongsouvathb, Carl Kirkwoodc, Nada Bogdanovic-Sakranc, Paul E. Kilgored
Department of Paediatrics, Mahosot Hospital, Vientiane, Lao People’s Democratic RepublicMicrobiology Section, Mahosot Hospital, Vientiane, Lao People’s Democratic RepublicMurdoch Childrens Research Institute, Parkville, Victoria, AustraliaDivision of Translational Research, International Vaccine Institute, Seoul, South Korea
r t i c l e i n f o
eywords:ao PDRiarrhoea
a b s t r a c t
Rotavirus is one of the most common causes of severe life-threatening diarrhoea in children leading tohospitalization especially in developing countries. At Mahosot Hospital in Vientiane, Lao PDR, children
pidemiologyospitalizationotavirus
with diarrhoea underwent standard clinical evaluation and faecal specimen collection to estimate theburden of rotavirus hospitalizations and to determine rotavirus strain patterns among children aged lessthan 5 years old. From March 2005 to February 2007, a total of 1158 stool specimens were collected fromchildren aged less than 5 years old hospitalized with acute diarrhoea. Rotavirus was identified in 624(54%) of these patients. The G1P[8] strain was the most common genotype (35%), followed by G9P[8](25%). These surveillance data suggest that improved prevention and control programs for rotavirus as
arrho
well as other causes of di. Introduction
Globally, rotavirus is the most common cause of severe life-hreatening diarrhoea in children and it is responsible for anstimated 527,000 deaths each year among children aged less thanyears old [1,2]. Rotavirus is also one of the main causes of all
hildhood hospitalizations and is the leading cause of childhoodiarrhoeal hospitalizations [3,4]. In developing countries with lim-
ted access to health care, infants are particularly at risk for rapid
ody fluid losses associated with rotavirus infection [5].The Lao People’s Democratic Republic (Lao PDR) has a total pop-lation of 5,609,997 living within an area of 236,800 km2 [6]. In LaoDR, the national life expectancy is 61 years and the infant mor-
Abbreviations: IMR, infant mortality rate; IVI, International Vaccine Institute; LaoDR, Lao People’s Democratic Republic; RT-PCR, reverse transcriptase-polymerasehain reaction; U5MR, mortality rate of children aged less than 5 years.� Results reported in this manuscript were presented in part at the 6th Asianotavirus Surveillance Network Investigators’ Meeting, Bangkok, Thailand, Decem-er 3–4, 2007.�� Human experimentation guidelines of the U.S. Department of Health anduman Services and those of the authors’ institution(s) were followed in the conductf clinical research.∗ Corresponding author. Tel.: +82 2 881 1138; fax: +82 2 872 2803.
E-mail address: [email protected] (B. Nyambat).
264-410X/$ – see front matter © 2009 Elsevier Ltd. All rights reserved.oi:10.1016/j.vaccine.2009.08.100
ea are needed in Lao PDR.© 2009 Elsevier Ltd. All rights reserved.
tality rate (IMR) is 59 per 1000 live births while mortality rate ofchildren aged less than 5 years old (U5MR) is as high as 75 per1000 live births [7]. In Laotian children aged less than 5 years old,malaria accounts for 24% of major hospitalizations while diarrhoea,pneumonia and neonatal tetanus are responsible for 17%, 16% and9%, respectively [8]. Despite the fact that diarrhoea is one of lead-ing cause of admission to paediatric departments, there is littleinformation available on causes of diarrhoea in the Lao PDR [9,10].Currently, there are no systematic data available on rotavirus diar-rhoea in Lao PDR and such data are critical to help guide healthpolicy decisions regarding the use of new rotavirus vaccines inLaotian infants.
This study describes the prevalence of acute diarrhoea causedby rotavirus as well as the distribution of G and P genotypes ofrotavirus strains among children aged less than 5 years old whowere admitted to Mahosot Hospital, Vientiane, Lao PDR. This studyalso describes demographic, seasonal and clinical characteristics ofrotavirus diarrhoea in these hospitalized patients.
2. Materials and methods
Mahosot Hospital is a major teaching and referral hospitallocated in Vientiane, Lao PDR. The majority (75%) of paediatric inpa-tient admissions (1824 of 2432 inpatients) to Mahosot Hospital in2005 were children aged less than 5 years old [11]. This study was

F cine 2
ccdA2otECwI
Msccidts
drOm(swtcpF
TC2
Fa2
Of 1172 children aged less than 5 years old admitted for acutediarrhoea from March 2005 to February 2007, 1158 (99%) had astool specimen available for rotavirus testing and of these 624 (54%)
86 D.S. Aloun et al. / Vac
onducted from March 1, 2005 through February 28, 2007 amonghildren aged less than 5 years old who were admitted for acuteiarrhoea to the Department of Paediatrics in Mahosot Hospital.cute diarrhoea was defined as three or more watery stools in a4-h period with onset less than 7 days before presentation. More-ver, a symptom-free interval of not less than 5 days was observedo distinguish between successive episodes of diarrhoea [12,13].thical clearance for this study was granted by the Ethical Reviewommittee of the Council of Medical Sciences and Technology asell as the Institutional Review Board of the International Vaccine
nstitute, Seoul, South Korea.Children were screened in all paediatric inpatient units of
ahosot Hospital and physicians interviewed parents to recordigns and symptoms of diarrhoea and relevant demographic andlinical information. Parents were provided with faecal specimenollection containers with plastic bags to collect diarrhoeal spec-mens. These containers were labelled by medical staff with theate of collection and a unique surveillance identification numbero permit reporting of test results to clinical paediatric departmenttaff.
Study investigators were provided with standardized forms foremographic and clinical data collection and data forms wereeviewed for completeness and accuracy to ensure data quality.n a weekly basis, data were entered into surveillance databaseanagement software created by IVI staff using MS Visual FoxPro®
Microsoft Corp., Redmond, USA). We performed descriptive analy-is of rotavirus diarrhoea epidemiologic patterns by age and sex asell as the seasonal distribution of diarrhoeal and rotavirus hospi-
alizations. Clinical characteristics, the severity of illness and familyharacteristics were compared between children with rotavirus-ositive and rotavirus-negative diarrhoea using chi-square test orisher’s exact test when the expected cell sizes were less than five.
able 1hildren with diarrhoea by age group, Vientiane, Lao PDR, March 2005–February007.
Age group,months
Total enrolled,n (%)a
Specimens tested,n (%)b
RV-positive,n (%)
<6 136 (12) 135 (99) 56 (42)6–11 380 (32) 376 (99) 207 (55)12–23 439 (38) 435 (99) 250 (58)24–35 122 (10) 121 (99) 79 (65)36–59 95 (8) 91 (96) 32 (35)
Total 1172 (100) 1158 (99) 624 (54)
a Column percentage.b Percentage of specimens tested among the total number of patients enrolled.
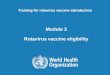
ig. 1. Age distribution and cumulative percentage of rotavirus-positive diarrhoeadmissions (n = 624), Mahosot Hospital, Vientiane, Lao PDR, March 2005–February007.
7S (2009) F85–F88
For each child, a faecal specimen was collected at the time ofadmission and frozen at −20 ◦C. Those stools samples were testedusing a rotavirus antigen detection enzyme immunoassay (OxoidLtd, United Kingdom). A randomly selected group of 211 rotavirus-positive faecal specimens underwent further characterization todetermine strain genotype by reverse transcriptase-polymerasechain reaction (RT-PCR) at Murdoch Childrens Research Institute,Melbourne, Australia [14,15].
3. Results
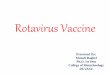
Fig. 2. Seasonal distribution of diarrhoea admissions (n = 1158) and rotavirus-positive diarrhoea (n = 624), Mahosot Hospital, Vientiane, Lao PDR, March2005–February 2007.
Table 2Clinical characteristics of children with diarrhoea, Vientiane, Lao PDR, March2005–February 2007.
Characteristics Rotavirus-positive,n (%)
Rotavirus-negative,n (%)
P-value
Temperature (◦C)≤37.5 341 (55) 286 (54)37.6–38.6 184 (30) 143 (26) 0.20≥38.7 99 (16) 105 (20)
DehydrationNone 22 (3.5) 70 (13)Some 587 (94) 455 (85) <0.0001Severe 15 (2.4) 9 (1.7)
Length of stay (days)≤2 473 (76) 368 (69)3–6 146 (23) 143 (27) <0.0001>6 5 (0.8) 23 (4.3)
Diarrhoea duration (days)≤2 28 (4.5) 31 (5.8)3–5 226 (36) 166 (31) 0.15>5 370 (59) 337 (63)
Vomiting duration (days)No vomiting 40 (6.4) 151 (28)<3 428 (69) 320 (60) <0.0001≥3 156 (25) 63 (12)
TreatmentORS + IVF 554 (89) 427 (80)ORS + IVF + ABX 19 (3.0) 48 (9) <0.0001Others 51 (8.2) 59 (11)
Note. ORS, oral rehydration solution; IVF, intravenous fluid; ABX, antibiotics.

D.S. Aloun et al. / Vaccine 27S (2009) F85–F88 F87
Table 3Distribution of rotavirus strains in children aged less than 5 years old hospitalized with diarrhoea, Vientiane, Lao PDR, March 2005–February 2007 (n = 211).
P genotype G genotype, n (%) Total
G1 G2 G3 G4 G9 G mixed NT
P4 – 2 (1) – – – – – 2 (1)P6 – – – – – – 3 (1) 3 (1)P8 73 (35) – 11 (5) – 53 (25) 2 (1) 1 (0.5) 140 (67)P9 – – – – – – – –P Mixed 12 (6) – – – – 1 (0.5) – 13 (6)
N
wp82plaa
tpdidcr
top(fcvwava
s32is
4
rriomsdafftpwt
NT 17 (8) – 3 (1) –
Total 102 (48) 2 (1) 14 (7) –
ote. NT, non-typeable.
ere positive for rotavirus. Among the total of 1172 diarrhoealatients, there were 136 (12%) children aged less than 6 months old,19 (70%) children aged 6–23 months and 217 (19%) children agedyears or older (Table 1 and Fig. 1). From a total of 624 rotavirus-ositive specimens, 56 (9.0%) were collected from young infants
ess than 6 months old, 457 (73%) from children aged 6–23 monthsnd remaining 111 (18%) specimens were collected from childrenged 2 or older.
We found a distinct peak for rotavirus diarrhoea from Januaryhrough April in Lao PDR (Fig. 2). The percentage of rotavirus-ositive specimens ranged from 60–90% during peak months whileuring non-peak months the percentage of rotavirus-positive spec-
mens ranged from 0% to 25%. There was a slight increase ofiarrhoeal hospitalizations in October but the study investigatorsould not describe aetiology of this outbreak due to limited localesources.
Clinically, episodes of rotavirus diarrhoea were more severehan episodes of non-rotavirus diarrhoea (Table 2). Vomitingccurred in 584 (94%) children with rotavirus diarrhoea com-ared with 383 (72%) children without rotavirus diarrhoeaP-value < 0.0001). Children with diarrhoea who tested positiveor rotavirus were more likely to have dehydration compared tohildren who did not test positive for rotavirus (97% vs. 87%, P-alue < 0.0001). Intravenous fluids with oral rehydration solutionere administered to 573 (92%) children with rotavirus diarrhoea
nd to 475 (89%) children with diarrhoea due to other causes (P-alue < 0.0001). The proportion of children with fever was similarmong those with and without rotavirus diarrhoea.
A total of 211 rotavirus-positive specimens obtained duringurveillance in Lao PDR were genotyped (Table 3). G1P[8] (n = 73;5%) was the most common strain followed by G9P[8] (n = 53;5%). A substantial number of strains were non-typeable includ-
ng 53 (25%) P non-typeable strains and 35 (17%) G non-typeabletrains.
. Discussion
This is the first systematic prospective study of rotavirus diar-hoea among children of Lao PDR and the results showed thatotavirus was associated with more than half of diarrhoeal hospital-zations in children. A total of 1172 children aged less than 5 yearsld with acute diarrhoea were admitted to the Paediatric Depart-ent of Mahosot Hospital in Vientiane, Lao PDR over the 24-month
urveillance period. In our study, rotavirus accounted for 54% ofiarrhoeal episodes and the greatest burden of rotavirus was foundmong young children aged 6–23 months. Interestingly, this studyound that rotavirus-related diarrhoeal hospitalizations peaked
rom January through April each year while rotavirus diarrhoea pat-erns in neighbouring Cambodia showed no clear seasonality (dataublished separately in Supplement). These findings are consistentith data presented by Levy et al. that suggest rotavirus respondso changes in climate in the tropics, with the highest number of
2 (1) – 31 (15) 53 (25)
55 (26) 3 (1) 35 (17) 211 (100)
cases of rotavirus diarrhoea found at the colder and drier timesof the year [16]. In this study, children with rotavirus diarrhoeaexperienced more severe diarrhoea with prolonged vomiting anddehydration compared with children having diarrhoea from othercauses. These results were also consistent with previous epidemi-ological studies in the US and Asian countries [17–19]. The G1P[8]strain was the most common genotype in Lao PDR (35%) followedby G9P[8] (25%). A substantial number of strains was non-typeablein Lao PDR and highlights the value of further strain typing usinggenetic sequencing.
In Lao PDR, the proportion of diarrhoea associated with rotavirusin this hospital-based surveillance study was within the rangefound from previous studies of rotavirus conducted in Asia[13,20–22]. Our findings including the age distribution and clini-cal characteristics of rotavirus diarrhoea are also consistent withthe findings of previous hospital-based studies in the Asian region[3,12,13,22].
Our study found no significant difference in the proportion ofchildren with fever among children with rotavirus-positive versusrotavirus-negative diarrhoea. This observation may be due to thefact that the majority of patients studied had received antipyretictherapy prior to admission. Additionally, the length of hospitalstay at Mahosot Hospital was similar between the groups of chil-dren with rotavirus-positive and rotavirus-negative diarrhoea. Thismay be explained by the fact that most of these patients’ fami-lies requested to go home early even though they are not yet fullyrecovered.
Data in this study were collected from one hospital and, thus, it ispossible that patterns of rotavirus may be different in other regionsof Lao PDR. Therefore, enhanced surveillance for rotavirus in otherareas of Lao PDR will be beneficial to more accurately estimate thenational burden of disease. Continued surveillance for rotavirus inLao PDR should also include additional laboratory rotavirus straincharacterization to understand changes in circulating strains overtime. These data will enable local decision makers to estimate thenational rotavirus disease burden of hospitalizations in Lao PDR.The results of the study are critical for accelerated rotavirus vaccineintroduction with GAVI support.
5. Conclusion
In this prospective surveillance study, diarrhoea was a com-mon cause of hospitalization in children in Lao PDR and rotavirusaccounted for more than half of diarrhoeal hospitalizations amongchildren less than 5 years of age. With the high morbidity associatedwith rotavirus diarrhoea in Laotian children, it is likely that intro-duction of routine rotavirus immunization will reduce the burden
of diarrhoea among young children and diarrhoea that occurs dur-ing the cool, dry season [23,24]. Because of limited access to healthcare in many areas of Lao PDR, routine rotavirus immunization isthe best option to reduce total morbidity and mortality rates amongchildren aged less than 5 years old in Lao PDR. Maintenance of a
F cine 2
rnv
A
DPHTsPLdawn
C
F
tfb
R
[
[[
[
[
[
[
[
[
[
[
[
[
[
88 D.S. Aloun et al. / Vac
otavirus diarrhoeal surveillance system following introduction ofew vaccines will be essential to enable measurement of rotavirusaccine impact in Lao PDR.
cknowledgements
We would like to acknowledge Prof. Chanhpheng Thammavong,irector, Mahosot Hospital, Prof. Boungnong Boupha, Director,ublic Health Institute, Prof. Sithat Insixiangmay, Director ofygiene Department, Ministry of Health, for their kind support.hanks go to Dr. Khonesavanh Luangxay, Dr. Inpanh Phouang-ouvanh, Ms. Nody Xayasane and all doctors and nurses at theaediatrics Department and to all the staff of the Bacteriologicaboratory for their kind cooperation. Ms. Deok Ryun Kim at IVIeveloped and supported the rotavirus surveillance database man-gement system. Finally, this surveillance would not be successfulithout the kind support from the staff of ARSN/CDC and the Inter-ational Vaccine Institute.
onflict of interest statement
None of the authors have a conflict of interest.
unding sources
This work was performed under a collaborative agreement withhe Program for Appropriate Technology in Health (PATH) and wasunded in full or in part by the GAVI Alliance, and was supportedy the Governments of Kuwait, Sweden and the Republic of Korea.
eferences
[1] Glass RI, Parashar UD, Bresee JS, Turcios R, Fischer TK, Widdowson MA,et al. Rotavirus vaccines: current prospects and future challenges. Lancet2006;368(July (9532)):323–32.
[2] Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI. Global illness anddeaths caused by rotavirus disease in children. Emerg Infect Dis 2003;9(May(5)):565–72.
[3] Bresee J, Fang ZY, Wang B, Nelson EA, Tam J, Soenarto Y, et al. First reportfrom the Asian Rotavirus Surveillance Network. Emerg Infect Dis 2004;10(June
(6)):988–95.[4] Nelson EA, Bresee JS, Parashar UD, Widdowson MA, Glass RI. Rotavirus epi-demiology: the Asian Rotavirus Surveillance Network. Vaccine 2008;26(June(26)):3192–6.
[5] Grimwood K, Lambert SB. Rotavirus vaccines: opportunities and challenges.Hum Vac 2009;5(January (1)).
[
7S (2009) F85–F88
[6] Population and Household Survey 2005. Vientiane: State Planning Committee,National Statistics Centre; 2005.
[7] WHO Statistical Information System (WHOSIS). WHO; 2008.[8] Morbidity and Mortality in Lao PDR in 2005. Vientiane: Statistics Department,
Ministry of Health; 2005.[9] Wahlstrom R, Kounnavong S, Sisounthone B, Phanyanouvong A, Southam-
mavong T, Eriksson B, et al. Effectiveness of feedback for improving casemanagement of malaria, diarrhoea and pneumonia—a randomized controlledtrial at provincial hospitals in Lao PDR. Trop Med Int Health 2003;8(October(10)):901–9.
10] Yamashiro T, Nakasone N, Higa N, Iwanaga M, Insisiengmay S, Phounane T, etal. Etiological study of diarrheal patients in Vientiane, Lao People’s DemocraticRepublic. J Clin Microbiol 1998;36(August (8)):2195–9.
11] Annual Report 2005. Vientiane: Mahosot Hospital; 2005.12] Fang ZY, Wang B, Kilgore PE, Bresee JS, Zhang LJ, Sun LW, et al. Sentinel hospital
surveillance for rotavirus diarrhea in the People’s Republic of China, August2001–July 2003. J Infect Dis 2005;192(September (Suppl. 1)):S94–9.
13] Kim JS, Kang JO, Cho SC, Jang YT, Min SA, Park TH, et al. Epidemiological profileof rotavirus infection in the Republic of Korea: results from prospective surveil-lance in the Jeongeub District, 1 July 2002 through 30 June 2004. J Infect Dis2005;192(September (Suppl. 1)):S49–56.
14] Gentsch JR, Glass RI, Woods P, Gouvea V, Gorziglia M, Flores J, et al. Identificationof group A rotavirus gene 4 types by polymerase chain reaction. J Clin Microbiol1992;30(June (6)):1365–73.
15] Gouvea V, Glass RI, Woods P, Taniguchi K, Clark HF, Forrester B, et al. Polymerasechain reaction amplification and typing of rotavirus nucleic acid from stoolspecimens. J Clin Microbiol 1990;28(February (2)):276–82.
16] Levy K, Hubbard AE, Eisenberg JN. Seasonality of rotavirus disease in the tropics:a systematic review and meta-analysis. Int J Epidemiol 2008;(December).
17] Dennehy PH, Cortese MM, Begue RE, Jaeger JL, Roberts NE, Zhang R, etal. A case-control study to determine risk factors for hospitalization forrotavirus gastroenteritis in U.S. children. Pediatr Infect Dis J 2006;25(December(12)):1123–31.
18] Nguyen TV, Le Van P, Le Huy C, Weintraub A. Diarrhea caused by rotavirusin children less than 5 years of age in Hanoi, Vietnam. J Clin Microbiol2004;42(December (12)):5745–50.
19] Payne DC, Staat MA, Edwards KM, Szilagyi PG, Gentsch JR, Stockman LJ, et al.Active, population-based surveillance for severe rotavirus gastroenteritis inchildren in the United States. Pediatrics 2008;122(December (6)):1235–43.
20] Bodhidatta L, Lan NT, Hien BT, Lai NV, Srijan A, Serichantalergs O, et al.Rotavirus disease in young children from Hanoi, Vietnam. Pediatr Infect DisJ 2007;26(April (4)):325–8.
21] Moe K, Hummelman EG, Oo WM, Lwin T, Htwe TT. Hospital-based surveil-lance for rotavirus diarrhea in children in Yangon, Myanmar. J Infect Dis2005;192(September (Suppl. 1)):S111–3.
22] Nguyen VM, Nguyen VT, Huynh PL, Dang DT, Nguyen TH, Phan VT, et al. Theepidemiology and disease burden of rotavirus in Vietnam: sentinel surveillanceat 6 hospitals. J Infect Dis 2001;183(June (12)):1707–12.
23] Clark HF, Burke CJ, Volkin DB, Offit P, Ward RL, Bresee JS, et al. Safety, immuno-
genicity and efficacy in healthy infants of G1 and G2 human reassortantrotavirus vaccine in a new stabilizer/buffer liquid formulation. Pediatr InfectDis J 2003;22(October (10)):914–20.24] Joensuu J, Koskenniemi E, Pang XL, Vesikari T. Randomised placebo-controlledtrial of rhesus–human reassortant rotavirus vaccine for prevention of severerotavirus gastroenteritis. Lancet 1997;350(October (9086)):1205–9.