Embed Size (px)
Citation preview

Running head: Displacement of Lumbar Intervertebral Disc Without Myelopathy 1
Geriatric Patient Nursing Process Paper
Megan Lynn Riedy
Kent State University College of Nursing
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 2
Introduction
C.C., an eighty two year old female with an admitting diagnosis of displacement of
lumbar intervertebral disk without myelopathy, was assigned to me for care on October 4th
, 2011.
In addition to the displaced lumbar disk, C.C. had a history of diabetes, osteoarthritis and
hypertension. The clinical shift included regular vital signs, head to toe assessments, medication
administration, and all appropriate charting in regard to the care given. Also, various teaching
opportunities were utilized where applicable, and helpful to C.C.’s wellness.
Patient Profile
C.C. was admitted to Altercare of Noble’s Pond, for treatment of a displaced lumbar disc.
C.C. was one of two patients I cared for during the clinical day. Prior to the clinical shift I was
given C.C’s medical cardex including her scheduled and as need medication, and her treatment
flow sheet. From this I was able to gain a basic understanding of what C.C.’s needs may be
throughout the day. After gathering the necessary background data and listening to report I
entered C.C.’s room to meet her and preform a complete assessment.
C.C.’s assessment showed her vital signs to be as followed: Temperature 99.3 F, pulse
72, respiration 14, blood pressure 144/74, and oxygen saturation of 97% o room air. C.C. denied
any pain so long as she wasn’t moving. She was alert and oriented to the person place time and
situation. Her attitude was pleasant and positive. Her skin felt warm and dry and was intact.
C.C.’s speech was clear, pupils were round equal and reactive to light. C.C. showed good range
of motion with strong and equal hand grasps and leg strength. C.C.’s respiratory rate and rhythm
was regular with clear inspiration and expirations in all lobes. Bowel sounds were present in all
four quadrants. Abdomen was soft round and non-distended. C.C. presented with no edema, and
was able to ambulate independently with the use of a walker to use the bathroom.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 3
Next, I preformed a fall risk assessment on C.C.. The “Hendrich II Fall Risk Modle”
assesses the patient’s factors which contribute to falls. In the first half of the test C.C. scored a
zero, as she did not meet any of the criteria which would increase her score. For the second half
of the test C.C. was assessed in her ability to get out of bed. This portion of the test is referred to
as the “Get Up and Go Test”. C.C. was able to rise in one single movement with no assistance.
This indicates a score of 1. The zero from the first portion of the test is added to the 1 from the
second portion of the test. C.C.’s total score is a 1. A score of a five or above indicates a fall
risk according to the test. However, given C.C.’s pain during movement and orders for analgesic
narcotics my care for her still included careful monitoring and fall risk precautions
(Talboski,2009).
Then, a Braden skin assessment was performed on C.C. in order to assess her risk of
developing skin breakdown. C.C.’s sensory perception was not impaired. She was occasionally
moist. C.C. walks occasionally for short distances. She has slightly limited mobility. Her
nutrition is probably inadequate as she eats only about one half of her meals. There appears to
be no problem with friction and shear, as she is able to move in bed and in chair independently.
These aspects of the Braden scale add up to a 20 out of a possible 23. A score of a 16 or less is
an indication of a pressure sore risk and thus needs prevention plan to be implemented.
(Tabloski, 2009)
Lastly a mini mental exam was performed on C.C. This exam required her demonstrate a
knowledge of her orientation, location, and the current time. She was also asked to demonstrate
the ability to name simple ordinary objects such as a pencil and to repeat a series of words. Then
C.C. was asked to draw a simple picture. The test is comprised of several categories which are
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 4
scored independently. The total possible points is 30. C.C. scored 30 points on her mini mental
exam. (Tabloski, 2009)
Admitting Medical Diagnosis
C.C. was admitted to Altercare of Noble’s pond due to a displacement of a lumbar
intervertebral disk without myelopathy. C.C.’s chief complaint was of a severe pain in the
lumbar region of her spine when she ambulated. C.C. stated that the pain had been ongoing for
several weeks and had become worse as time progressed.
Pathophysiology of Displaced lumbar Intervertebral Disk
Vertebrae are separated and cushioned by pads of cartilage call intervertebral discs. The
Intervertebral discs have a tough outer layers are called the annulus fibrous. The collagen fiber
of this layer, attach the disc to the adjacent vertebrae. Inside the annulus fibrous is the nucleus
pulpous. This is a soft cushion like area which is able to absorb shock and allow for movement
of the vertebral column. However, when too much pressure compresses the nucleus pulpous, it
can be displaced. (Black & Hawks, 2009)
As patients age the water content of the nucleus pulpous in each sick decreased. They
then become less cushion-like and the chances of a vertebral injury are increased. Also with
advanced age the ligament holding the vertebrae in place become weakened. The compressed
nucleus pulpous may distort resulting in the displacement of the lumbar intervertebral disk. This
often compresses on nerved which are passing thought the adjacent area. The compressed nerve
can produce pain or even myelopathy for the patient. C.C. did no experience any myelopathy.
However she did complain of pain when she was ambulating (Tabloski, 2009).
Clinical Manifestations
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 5
Common symptoms include pain while sitting standing walking or bending. The patient
may present a less then normal curvature of the lumbar area of the hip known as Lordosis.
Spinal strength and flexibility is often decreased. Diagnosis can be made by imaging such as a
magnetic resonance image (MRI).
Other Medical Diagnosis
C.C.’s additional medical history included hypertension, constipation, and diabetes. For
C.C., the hypertension was still being controlled with pharmaceutical interventions.
Constipation was controlled with diet, ambulation, and laxatives as needed. C.C.’s Anxiety was
controlled with The diabetes was controlled with diet and an oral antidiabetic medication.
Pathophysiology of Hypertension
Hypertension or high blood pressure, is a common condition in which the force of the
blood against the artery walls is higher than the defined normal. This can cause health problems,
such as heart disease. Hypertension often develops over time. Thus eventually, uncontrolled
and or undiagnosed hypertension will increase a patient’s risk of myocardial infarctions (MIs ) or
stroke (Black & Hawks, 2009).
Clinical manifestations of Hypertension
Many patients will not experience any signs or symptoms of elevated blood pressure.
However, some will experience a dull headache, or dizziness. The most significant/reliable
finding is a regularly elevated blood pressure assessment (Black & Hawks, 2009)
Pathophysiology of Constipation
Constipation is defined s an infrequent defecation, a hardened stool and or a sensation of
incomplete evacuation of bowel movements. Many factors can contribute to constipation such as
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 6
dehydration, side effects of medications, and immobility. C.C. likely suffered from constipation
s a result of each of the aforementioned contributing factors (Tabloski, 2009).
Clinical manifestations of Constipation
Constipation results in hard stool. Hard stool is more difficult to pass. Thus, a
complication of constipation can be a fecal impaction which may result in other gastro intestinal
problems. Additionally, excessive straining to pass stool result in hemorrhoids, anal fissures, or
rector prolapse (Tabloski, 2009).
Pathophysiology of Diabetes
The hormone insulin is responsible for maintaining glucose levels in the blood. Insulin
allows the body tissue to use glucose as an energy source. However, in a diabetic patient,
glucose metabolism is compromised as a result in abnormal insulin metabolism. The result is an
increase in circulating blood glucose which can lead to severe complications including
cardiovascular disease kidney damage, nerve problems, and tissue and vision disorders (Black &
Hawks, 2009).
Clinical Manifestations of Diabetes
As a result of increased blood glucose levels, polyuria, polyphagia, glycosuria,
hyperglycemia, and an increase of specific gravity of urine are often clinical manifestation
leading to a diabetes diagnosis. Treatment includes a consistent carb diet and often use of insulin
analog replacement therapy. Hypoglycemia can result from ingesting too little carbohydrates or
taking too much insulin therapy. These symptoms include diaphoresis, confusion, and headache.
Both hyper and hypoglycemic episodes are to be monitored and assessed (Black & Hawks,
2009).
Surgical History
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 7
C.C. has currently had one surgery in her lifetime. At 20 years old she described being
sick for a few weeks. C.C. stated that her doctors at the time worried she had tuberculosis, but
later discovered that she did not. As a result of the prolonged illness she eventually had her
tonsils removed later that year.
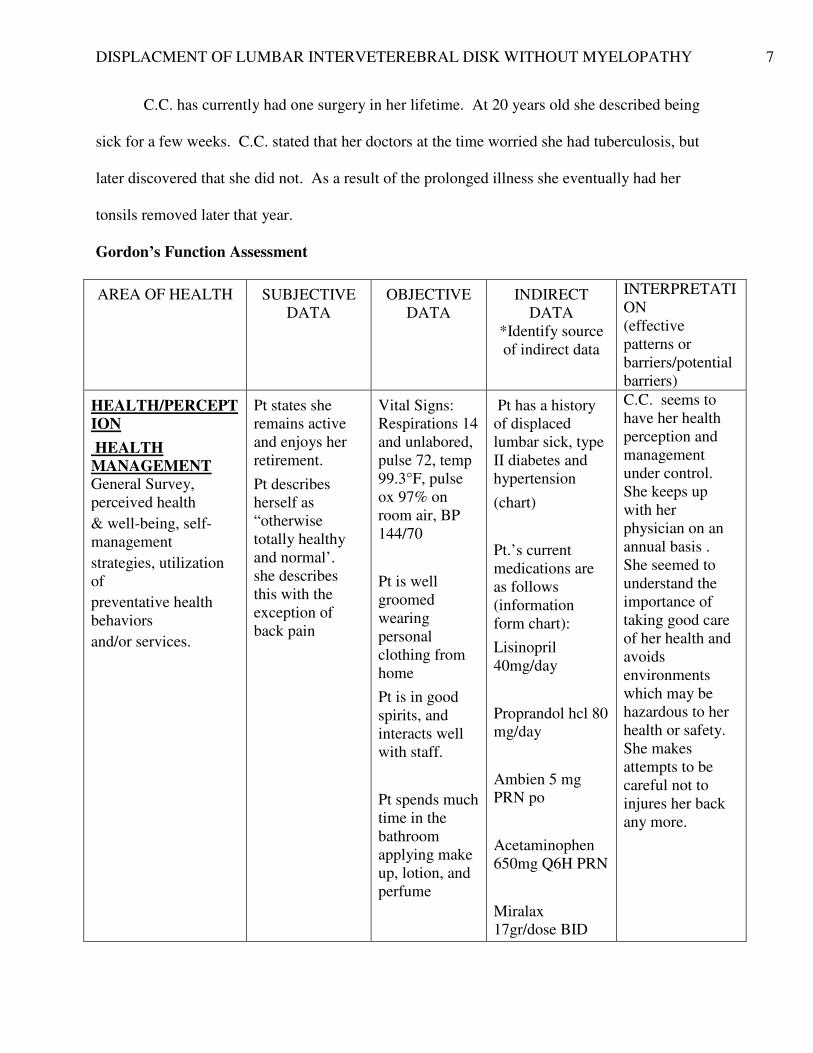
Gordon’s Function Assessment
AREA OF HEALTH SUBJECTIVE
DATA
OBJECTIVE
DATA
INDIRECT
DATA
*Identify source
of indirect data
INTERPRETATI
ON
(effective
patterns or
barriers/potential
barriers)
HEALTH/PERCEPT
ION
HEALTH
MANAGEMENT General Survey,
perceived health
& well-being, self-
management
strategies, utilization
of
preventative health
behaviors
and/or services.
Pt states she
remains active
and enjoys her
retirement.
Pt describes
herself as
“otherwise
totally healthy
and normal’.
she describes
this with the
exception of
back pain
Vital Signs:
Respirations 14
and unlabored,
pulse 72, temp
99.3°F, pulse
ox 97% on
room air, BP
144/70
Pt is well
groomed
wearing
personal
clothing from
home
Pt is in good
spirits, and
interacts well
with staff.
Pt spends much
time in the
bathroom
applying make
up, lotion, and
perfume
Pt has a history
of displaced
lumbar sick, type
II diabetes and
hypertension
(chart)
Pt.’s current
medications are
as follows
(information
form chart):
Lisinopril
40mg/day
Proprandol hcl 80
mg/day
Ambien 5 mg
PRN po
Acetaminophen
650mg Q6H PRN
Miralax
17gr/dose BID
C.C. seems to
have her health
perception and
management
under control.
She keeps up
with her
physician on an
annual basis .
She seemed to
understand the
importance of
taking good care
of her health and
avoids
environments
which may be
hazardous to her
health or safety.
She makes
attempts to be
careful not to
injures her back
any more.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 8
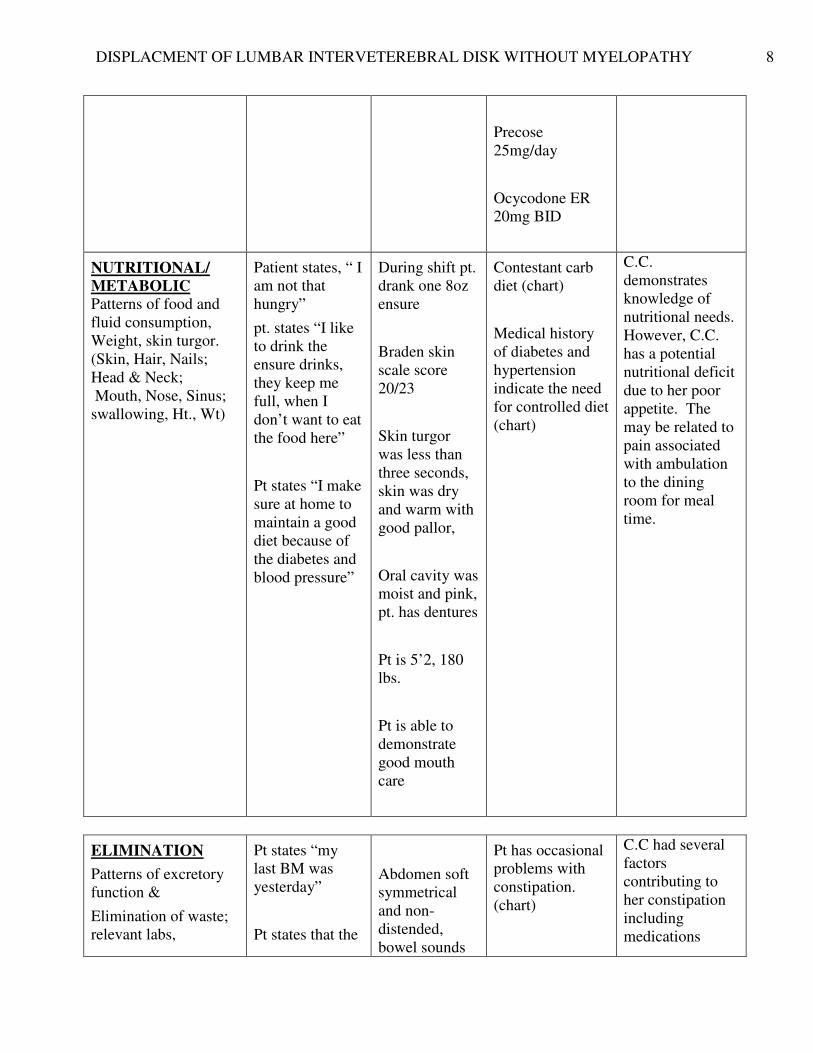
Precose
25mg/day
Ocycodone ER
20mg BID
NUTRITIONAL/
METABOLIC
Patterns of food and
fluid consumption,
Weight, skin turgor.
(Skin, Hair, Nails;
Head & Neck;
Mouth, Nose, Sinus;
swallowing, Ht., Wt)
Patient states, “ I
am not that
hungry”
pt. states “I like
to drink the
ensure drinks,
they keep me
full, when I
don’t want to eat
the food here”
Pt states “I make
sure at home to
maintain a good
diet because of
the diabetes and
blood pressure”
During shift pt.
drank one 8oz
ensure
Braden skin
scale score
20/23
Skin turgor
was less than
three seconds,
skin was dry
and warm with
good pallor,
Oral cavity was
moist and pink,
pt. has dentures
Pt is 5’2, 180
lbs.
Pt is able to
demonstrate
good mouth
care
Contestant carb
diet (chart)
Medical history
of diabetes and
hypertension
indicate the need
for controlled diet
(chart)
C.C.
demonstrates
knowledge of
nutritional needs.
However, C.C.
has a potential
nutritional deficit
due to her poor
appetite. The
may be related to
pain associated
with ambulation
to the dining
room for meal
time.
ELIMINATION
Patterns of excretory
function &
Elimination of waste;
relevant labs,
Pt states “my
last BM was
yesterday”
Pt states that the
Abdomen soft
symmetrical
and non-
distended,
bowel sounds
Pt has occasional
problems with
constipation.
(chart)
C.C had several
factors
contributing to
her constipation
including
medications
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 9
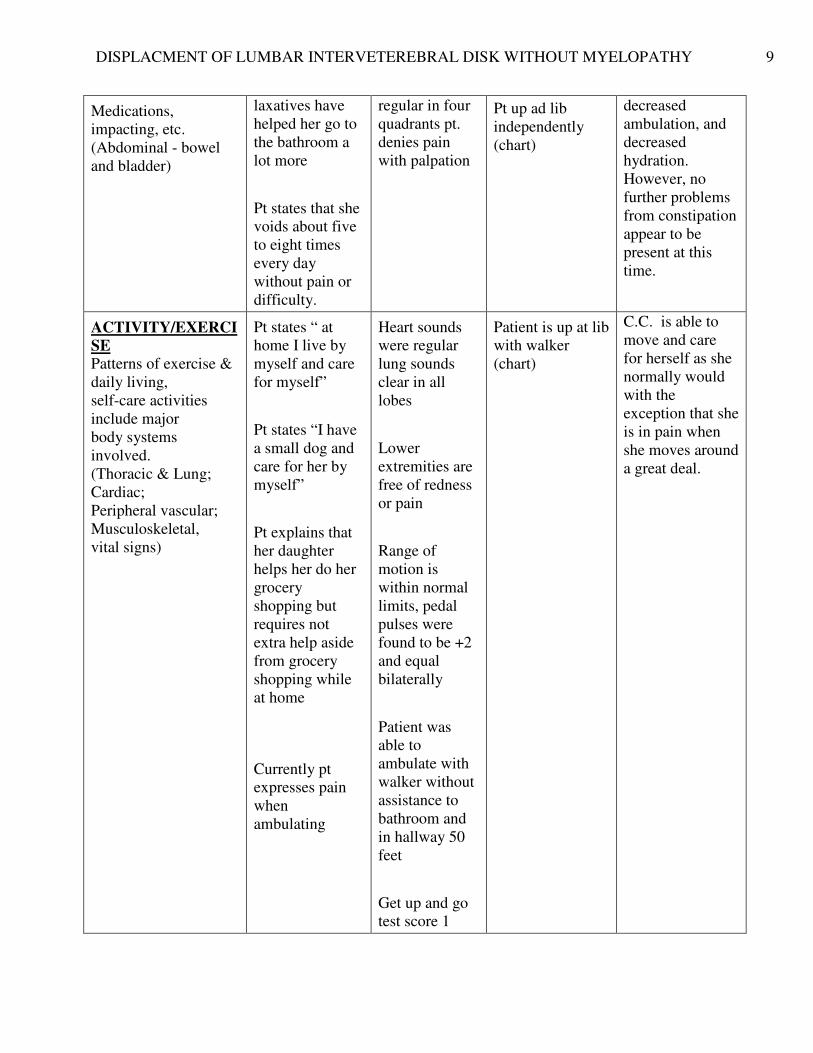
Medications,
impacting, etc.
(Abdominal - bowel
and bladder)
laxatives have
helped her go to
the bathroom a
lot more
Pt states that she
voids about five
to eight times
every day
without pain or
difficulty.
regular in four
quadrants pt.
denies pain
with palpation
Pt up ad lib
independently
(chart)
decreased
ambulation, and
decreased
hydration.
However, no
further problems
from constipation
appear to be
present at this
time.
ACTIVITY/EXERCI
SE Patterns of exercise &
daily living,
self-care activities
include major
body systems
involved.
(Thoracic & Lung;
Cardiac;
Peripheral vascular;
Musculoskeletal,
vital signs)
Pt states “ at
home I live by
myself and care
for myself”
Pt states “I have
a small dog and
care for her by
myself”
Pt explains that
her daughter
helps her do her
grocery
shopping but
requires not
extra help aside
from grocery
shopping while
at home
Currently pt
expresses pain
when
ambulating
Heart sounds
were regular
lung sounds
clear in all
lobes
Lower
extremities are
free of redness
or pain
Range of
motion is
within normal
limits, pedal
pulses were
found to be +2
and equal
bilaterally
Patient was
able to
ambulate with
walker without
assistance to
bathroom and
in hallway 50
feet
Get up and go
test score 1
Patient is up at lib
with walker
(chart)
C.C. is able to
move and care
for herself as she
normally would
with the
exception that she
is in pain when
she moves around
a great deal.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 10
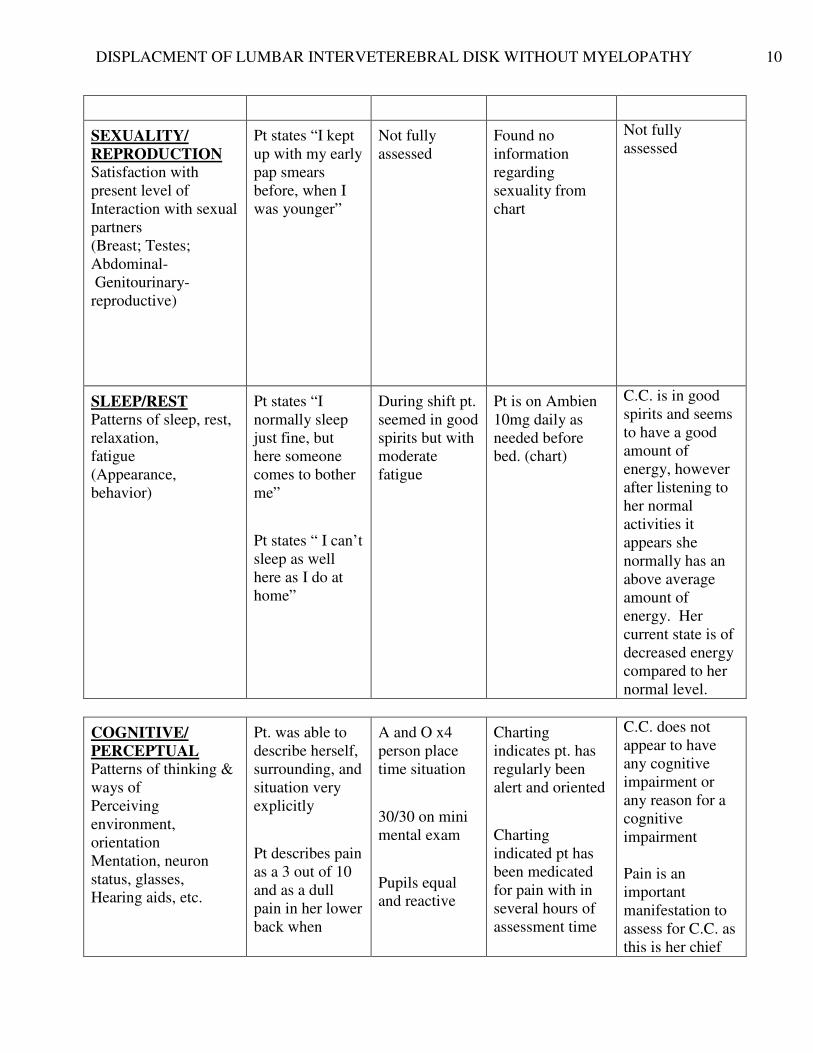
SEXUALITY/
REPRODUCTION Satisfaction with
present level of
Interaction with sexual
partners
(Breast; Testes;
Abdominal-
Genitourinary-
reproductive)
Pt states “I kept
up with my early
pap smears
before, when I
was younger”
Not fully
assessed
Found no
information
regarding
sexuality from
chart
Not fully
assessed
SLEEP/REST Patterns of sleep, rest,
relaxation,
fatigue
(Appearance,
behavior)
Pt states “I
normally sleep
just fine, but
here someone
comes to bother
me”
Pt states “ I can’t
sleep as well
here as I do at
home”
During shift pt.
seemed in good
spirits but with
moderate
fatigue
Pt is on Ambien
10mg daily as
needed before
bed. (chart)
C.C. is in good
spirits and seems
to have a good
amount of
energy, however
after listening to
her normal
activities it
appears she
normally has an
above average
amount of
energy. Her
current state is of
decreased energy
compared to her
normal level.
COGNITIVE/
PERCEPTUAL Patterns of thinking &
ways of
Perceiving
environment,
orientation
Mentation, neuron
status, glasses,
Hearing aids, etc.
Pt. was able to
describe herself,
surrounding, and
situation very
explicitly
Pt describes pain
as a 3 out of 10
and as a dull
pain in her lower
back when
A and O x4
person place
time situation
30/30 on mini
mental exam
Pupils equal
and reactive
Charting
indicates pt. has
regularly been
alert and oriented
Charting
indicated pt has
been medicated
for pain with in
several hours of
assessment time
C.C. does not
appear to have
any cognitive
impairment or
any reason for a
cognitive
impairment
Pain is an
important
manifestation to
assess for C.C. as
this is her chief
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 11
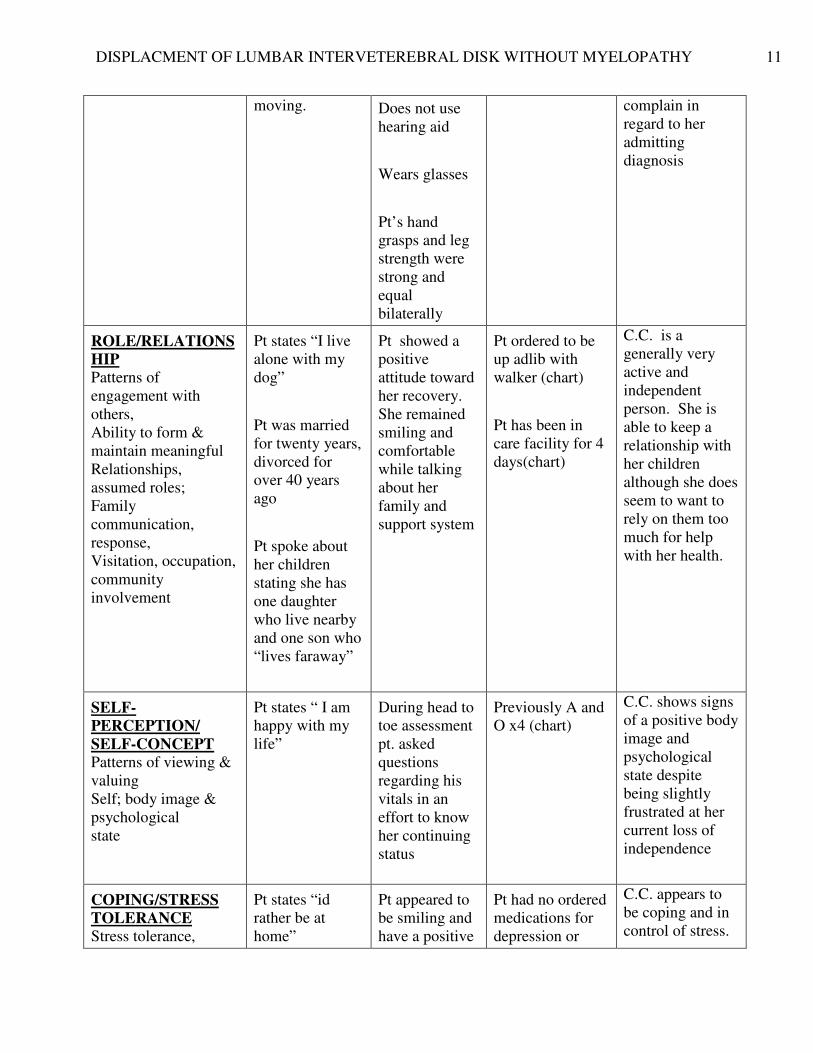
moving. Does not use
hearing aid
Wears glasses
Pt’s hand
grasps and leg
strength were
strong and
equal
bilaterally
complain in
regard to her
admitting
diagnosis
ROLE/RELATIONS
HIP Patterns of
engagement with
others,
Ability to form &
maintain meaningful
Relationships,
assumed roles;
Family
communication,
response,
Visitation, occupation,
community
involvement
Pt states “I live
alone with my
dog”
Pt was married
for twenty years,
divorced for
over 40 years
ago
Pt spoke about
her children
stating she has
one daughter
who live nearby
and one son who
“lives faraway”
Pt showed a
positive
attitude toward
her recovery.
She remained
smiling and
comfortable
while talking
about her
family and
support system
Pt ordered to be
up adlib with
walker (chart)
Pt has been in
care facility for 4
days(chart)
C.C. is a
generally very
active and
independent
person. She is
able to keep a
relationship with
her children
although she does
seem to want to
rely on them too
much for help
with her health.
SELF-
PERCEPTION/
SELF-CONCEPT Patterns of viewing &
valuing
Self; body image &
psychological
state
Pt states “ I am
happy with my
life”
During head to
toe assessment
pt. asked
questions
regarding his
vitals in an
effort to know
her continuing
status
Previously A and
O x4 (chart)
C.C. shows signs
of a positive body
image and
psychological
state despite
being slightly
frustrated at her
current loss of
independence
COPING/STRESS
TOLERANCE Stress tolerance,
Pt states “id
rather be at
home”
Pt appeared to
be smiling and
have a positive
Pt had no ordered
medications for
depression or
C.C. appears to
be coping and in
control of stress.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 12
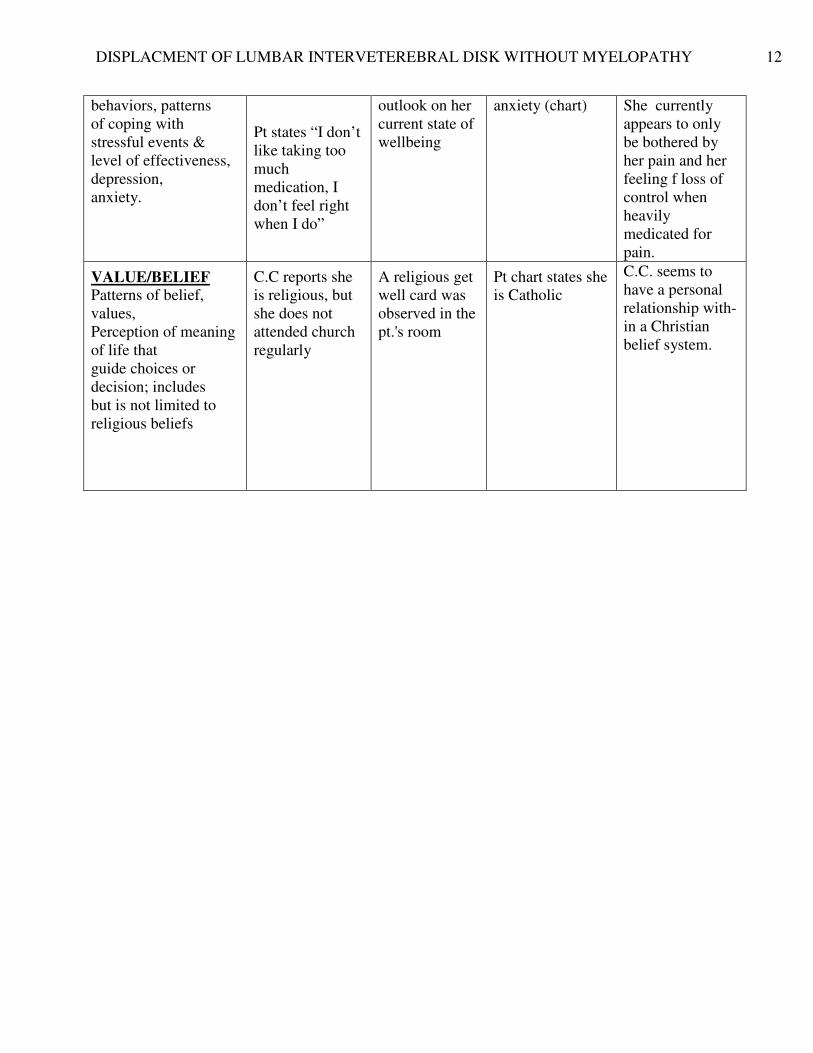
behaviors, patterns
of coping with
stressful events &
level of effectiveness,
depression,
anxiety.
Pt states “I don’t
like taking too
much
medication, I
don’t feel right
when I do”
outlook on her
current state of
wellbeing
anxiety (chart) She currently
appears to only
be bothered by
her pain and her
feeling f loss of
control when
heavily
medicated for
pain.
VALUE/BELIEF Patterns of belief,
values,
Perception of meaning
of life that
guide choices or
decision; includes
but is not limited to
religious beliefs
C.C reports she
is religious, but
she does not
attended church
regularly
A religious get
well card was
observed in the
pt.'s room
Pt chart states she
is Catholic
C.C. seems to
have a personal
relationship with-
in a Christian
belief system.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 13
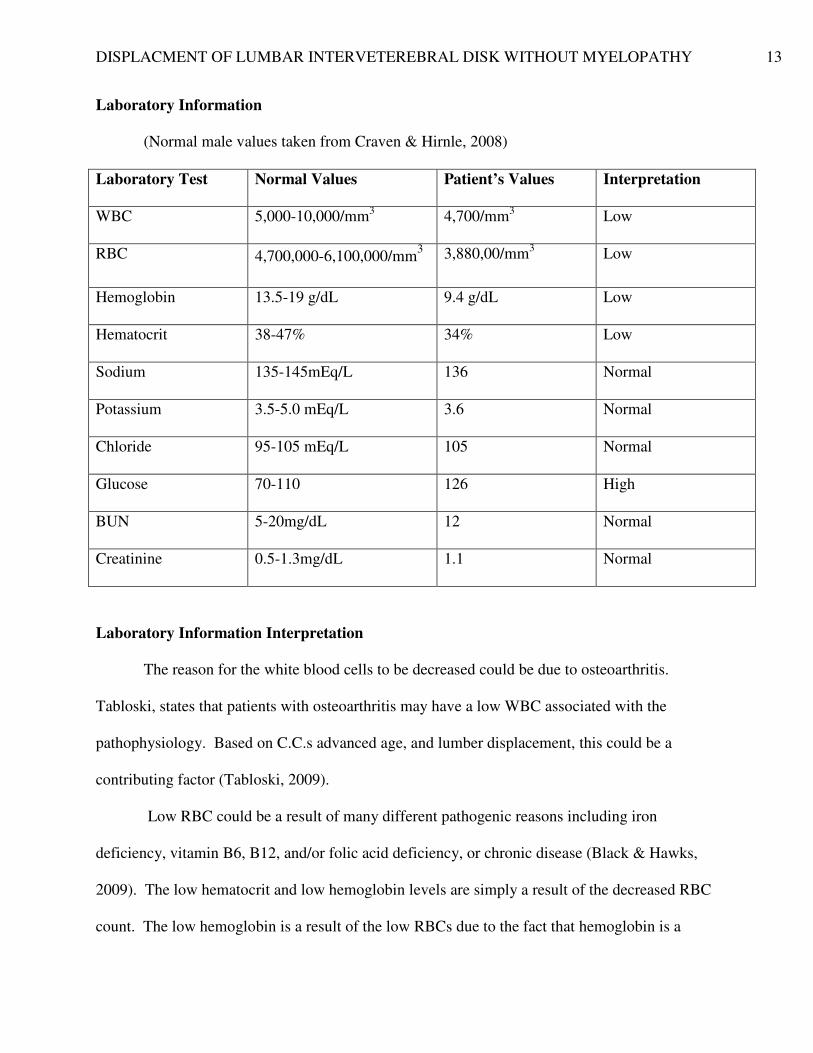
Laboratory Information
(Normal male values taken from Craven & Hirnle, 2008)
Laboratory Test Normal Values Patient’s Values Interpretation
WBC 5,000-10,000/mm3
4,700/mm3
Low
RBC 4,700,000-6,100,000/mm3 3,880,00/mm
3 Low
Hemoglobin 13.5-19 g/dL 9.4 g/dL Low
Hematocrit 38-47% 34% Low
Sodium 135-145mEq/L 136 Normal
Potassium 3.5-5.0 mEq/L 3.6 Normal
Chloride 95-105 mEq/L 105 Normal
Glucose 70-110 126 High
BUN 5-20mg/dL 12 Normal
Creatinine 0.5-1.3mg/dL 1.1 Normal
Laboratory Information Interpretation
The reason for the white blood cells to be decreased could be due to osteoarthritis.
Tabloski, states that patients with osteoarthritis may have a low WBC associated with the
pathophysiology. Based on C.C.s advanced age, and lumber displacement, this could be a
contributing factor (Tabloski, 2009).
Low RBC could be a result of many different pathogenic reasons including iron
deficiency, vitamin B6, B12, and/or folic acid deficiency, or chronic disease (Black & Hawks,
2009). The low hematocrit and low hemoglobin levels are simply a result of the decreased RBC
count. The low hemoglobin is a result of the low RBCs due to the fact that hemoglobin is a
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 14
protein with in the RBCs. When the total number of circulating RBCs decrease, as in C.C.’s
case, the hemoglobin also decreases. Hematocrit percentage is also directly dependent on the
RBCs. Hematocrit is a measurement in percentage of the RBC’s concentration in blood. As the
RBC count decreases and the plasma remains constant the RBC percentage decreases which is
indicated by the low hematocrit percentage (Black and Hawks, 2009).
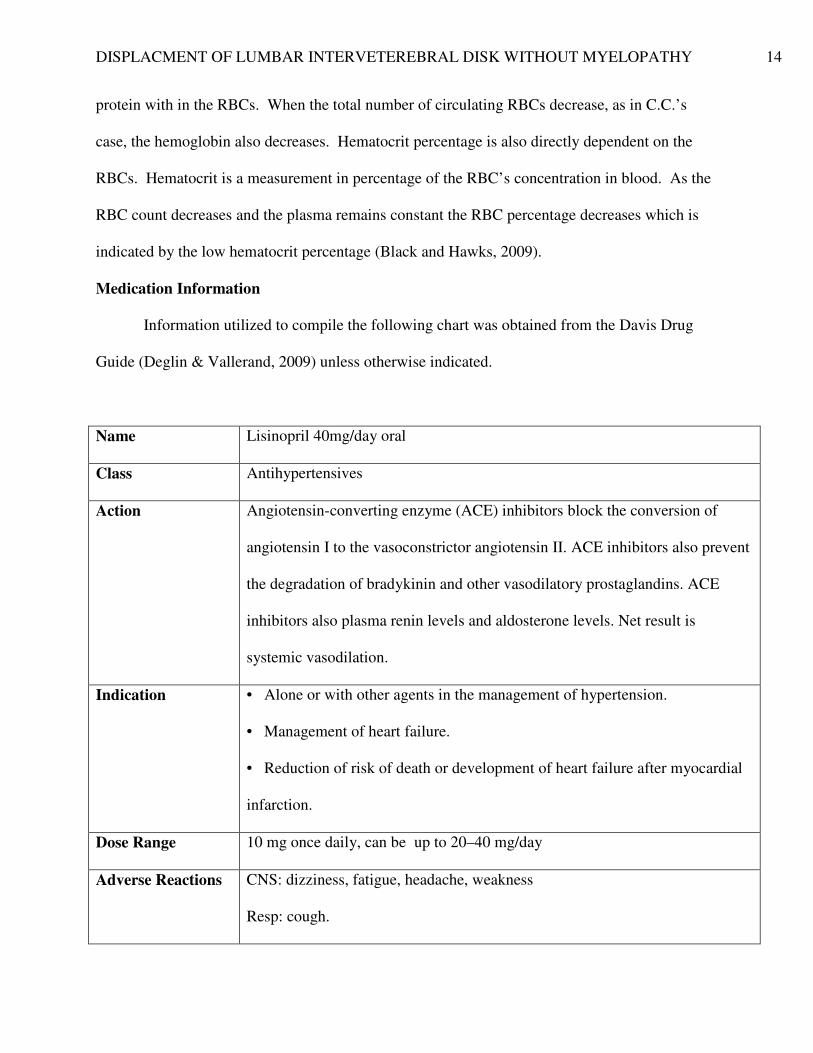
Medication Information
Information utilized to compile the following chart was obtained from the Davis Drug
Guide (Deglin & Vallerand, 2009) unless otherwise indicated.
Name Lisinopril 40mg/day oral
Class Antihypertensives
Action Angiotensin-converting enzyme (ACE) inhibitors block the conversion of
angiotensin I to the vasoconstrictor angiotensin II. ACE inhibitors also prevent
the degradation of bradykinin and other vasodilatory prostaglandins. ACE
inhibitors also plasma renin levels and aldosterone levels. Net result is
systemic vasodilation.
Indication • Alone or with other agents in the management of hypertension.
• Management of heart failure.
• Reduction of risk of death or development of heart failure after myocardial
infarction.
Dose Range 10 mg once daily, can be up to 20–40 mg/day
Adverse Reactions CNS: dizziness, fatigue, headache, weakness
Resp: cough.
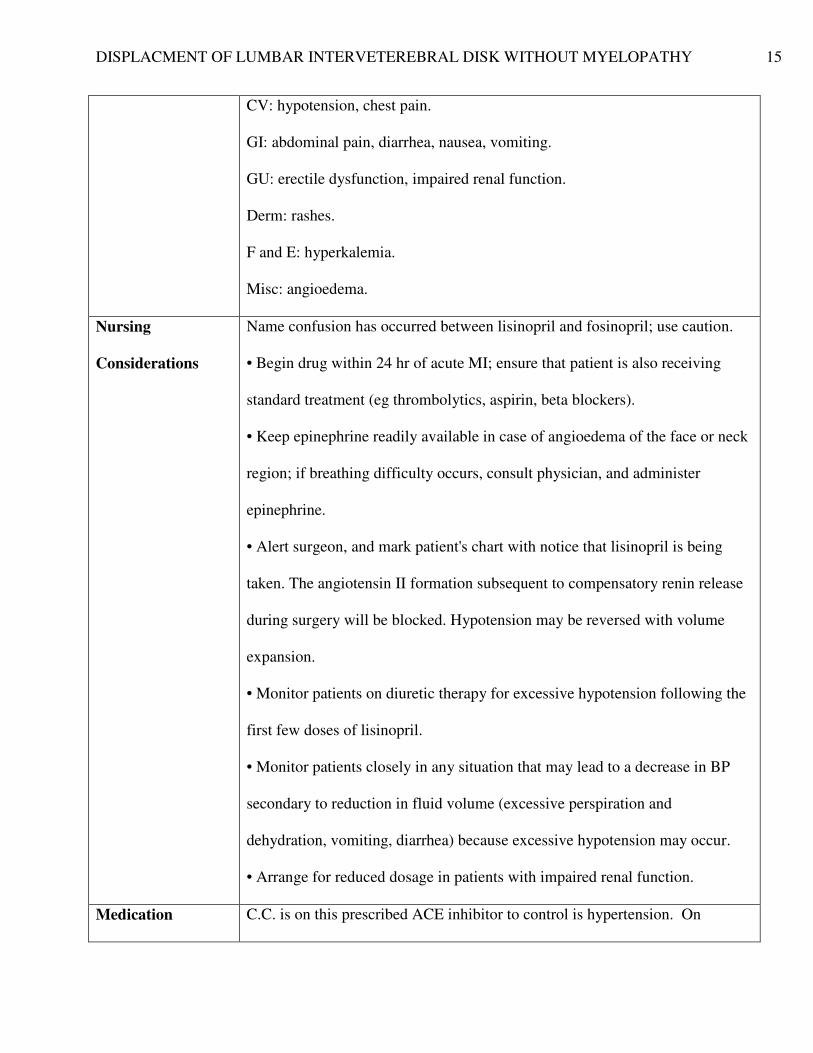
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 15
CV: hypotension, chest pain.
GI: abdominal pain, diarrhea, nausea, vomiting.
GU: erectile dysfunction, impaired renal function.
Derm: rashes.
F and E: hyperkalemia.
Misc: angioedema.
Nursing
Considerations
Name confusion has occurred between lisinopril and fosinopril; use caution.
• Begin drug within 24 hr of acute MI; ensure that patient is also receiving
standard treatment (eg thrombolytics, aspirin, beta blockers).
• Keep epinephrine readily available in case of angioedema of the face or neck
region; if breathing difficulty occurs, consult physician, and administer
epinephrine.
• Alert surgeon, and mark patient's chart with notice that lisinopril is being
taken. The angiotensin II formation subsequent to compensatory renin release
during surgery will be blocked. Hypotension may be reversed with volume
expansion.
• Monitor patients on diuretic therapy for excessive hypotension following the
first few doses of lisinopril.
• Monitor patients closely in any situation that may lead to a decrease in BP
secondary to reduction in fluid volume (excessive perspiration and
dehydration, vomiting, diarrhea) because excessive hypotension may occur.
• Arrange for reduced dosage in patients with impaired renal function.
Medication C.C. is on this prescribed ACE inhibitor to control is hypertension. On
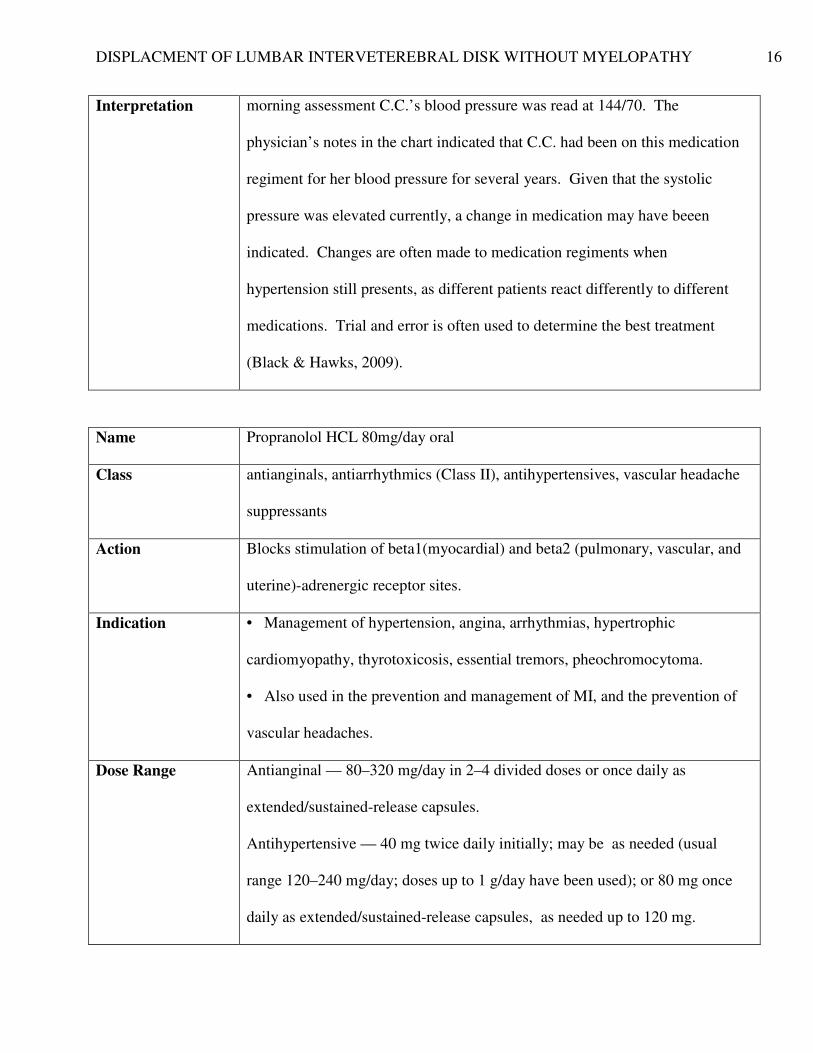
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 16
Interpretation morning assessment C.C.’s blood pressure was read at 144/70. The
physician’s notes in the chart indicated that C.C. had been on this medication
regiment for her blood pressure for several years. Given that the systolic
pressure was elevated currently, a change in medication may have beeen
indicated. Changes are often made to medication regiments when
hypertension still presents, as different patients react differently to different
medications. Trial and error is often used to determine the best treatment
(Black & Hawks, 2009).
Name Propranolol HCL 80mg/day oral
Class antianginals, antiarrhythmics (Class II), antihypertensives, vascular headache
suppressants
Action Blocks stimulation of beta1(myocardial) and beta2 (pulmonary, vascular, and
uterine)-adrenergic receptor sites.
Indication • Management of hypertension, angina, arrhythmias, hypertrophic
cardiomyopathy, thyrotoxicosis, essential tremors, pheochromocytoma.
• Also used in the prevention and management of MI, and the prevention of
vascular headaches.
Dose Range Antianginal — 80–320 mg/day in 2–4 divided doses or once daily as
extended/sustained-release capsules.
Antihypertensive — 40 mg twice daily initially; may be as needed (usual
range 120–240 mg/day; doses up to 1 g/day have been used); or 80 mg once
daily as extended/sustained-release capsules, as needed up to 120 mg.
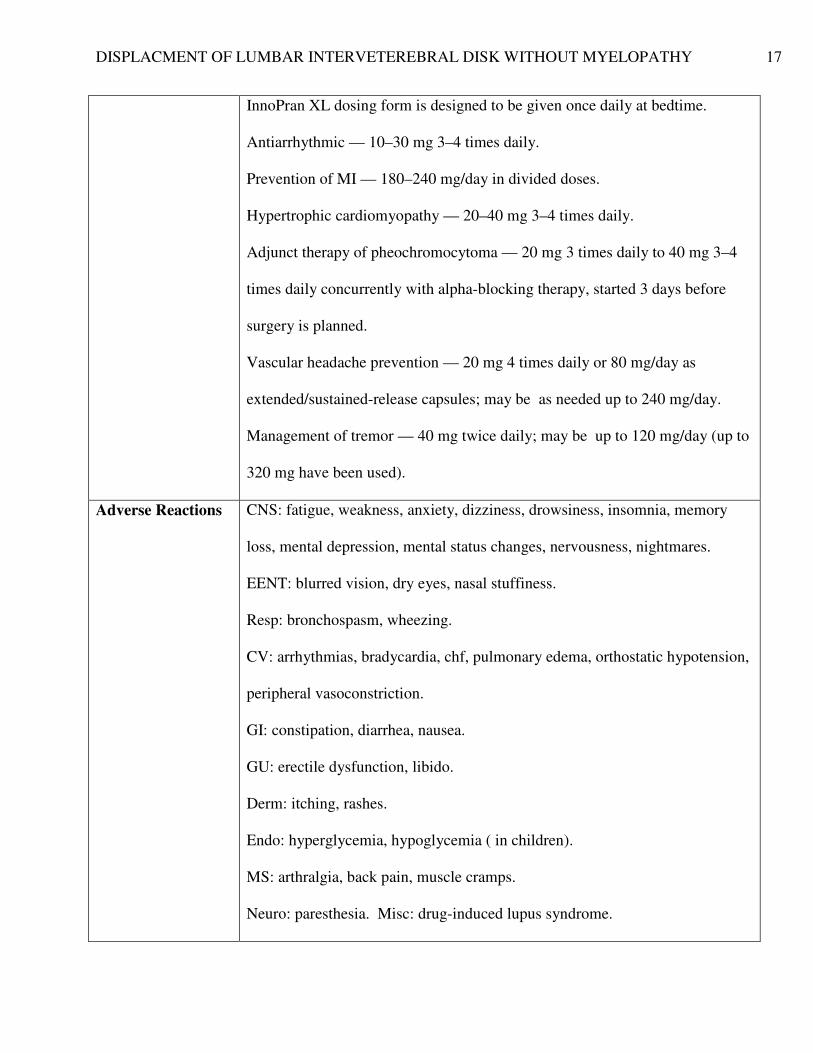
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 17
InnoPran XL dosing form is designed to be given once daily at bedtime.
Antiarrhythmic — 10–30 mg 3–4 times daily.
Prevention of MI — 180–240 mg/day in divided doses.
Hypertrophic cardiomyopathy — 20–40 mg 3–4 times daily.
Adjunct therapy of pheochromocytoma — 20 mg 3 times daily to 40 mg 3–4
times daily concurrently with alpha-blocking therapy, started 3 days before
surgery is planned.
Vascular headache prevention — 20 mg 4 times daily or 80 mg/day as
extended/sustained-release capsules; may be as needed up to 240 mg/day.
Management of tremor — 40 mg twice daily; may be up to 120 mg/day (up to
320 mg have been used).
Adverse Reactions CNS: fatigue, weakness, anxiety, dizziness, drowsiness, insomnia, memory
loss, mental depression, mental status changes, nervousness, nightmares.
EENT: blurred vision, dry eyes, nasal stuffiness.
Resp: bronchospasm, wheezing.
CV: arrhythmias, bradycardia, chf, pulmonary edema, orthostatic hypotension,
peripheral vasoconstriction.
GI: constipation, diarrhea, nausea.
GU: erectile dysfunction, libido.
Derm: itching, rashes.
Endo: hyperglycemia, hypoglycemia ( in children).
MS: arthralgia, back pain, muscle cramps.
Neuro: paresthesia. Misc: drug-induced lupus syndrome.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 18
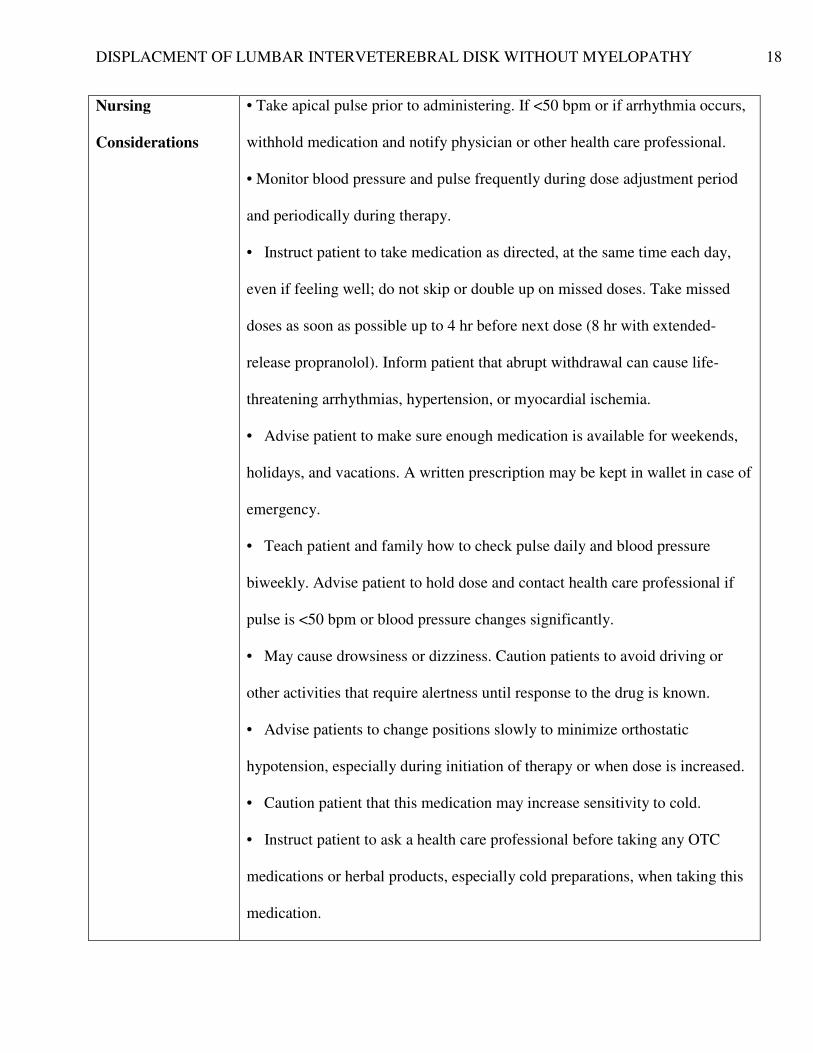
Nursing
Considerations
• Take apical pulse prior to administering. If <50 bpm or if arrhythmia occurs,
withhold medication and notify physician or other health care professional.
• Monitor blood pressure and pulse frequently during dose adjustment period
and periodically during therapy.
• Instruct patient to take medication as directed, at the same time each day,
even if feeling well; do not skip or double up on missed doses. Take missed
doses as soon as possible up to 4 hr before next dose (8 hr with extended-
release propranolol). Inform patient that abrupt withdrawal can cause life-
threatening arrhythmias, hypertension, or myocardial ischemia.
• Advise patient to make sure enough medication is available for weekends,
holidays, and vacations. A written prescription may be kept in wallet in case of
emergency.
• Teach patient and family how to check pulse daily and blood pressure
biweekly. Advise patient to hold dose and contact health care professional if
pulse is <50 bpm or blood pressure changes significantly.
• May cause drowsiness or dizziness. Caution patients to avoid driving or
other activities that require alertness until response to the drug is known.
• Advise patients to change positions slowly to minimize orthostatic
hypotension, especially during initiation of therapy or when dose is increased.
• Caution patient that this medication may increase sensitivity to cold.
• Instruct patient to ask a health care professional before taking any OTC
medications or herbal products, especially cold preparations, when taking this
medication.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 19
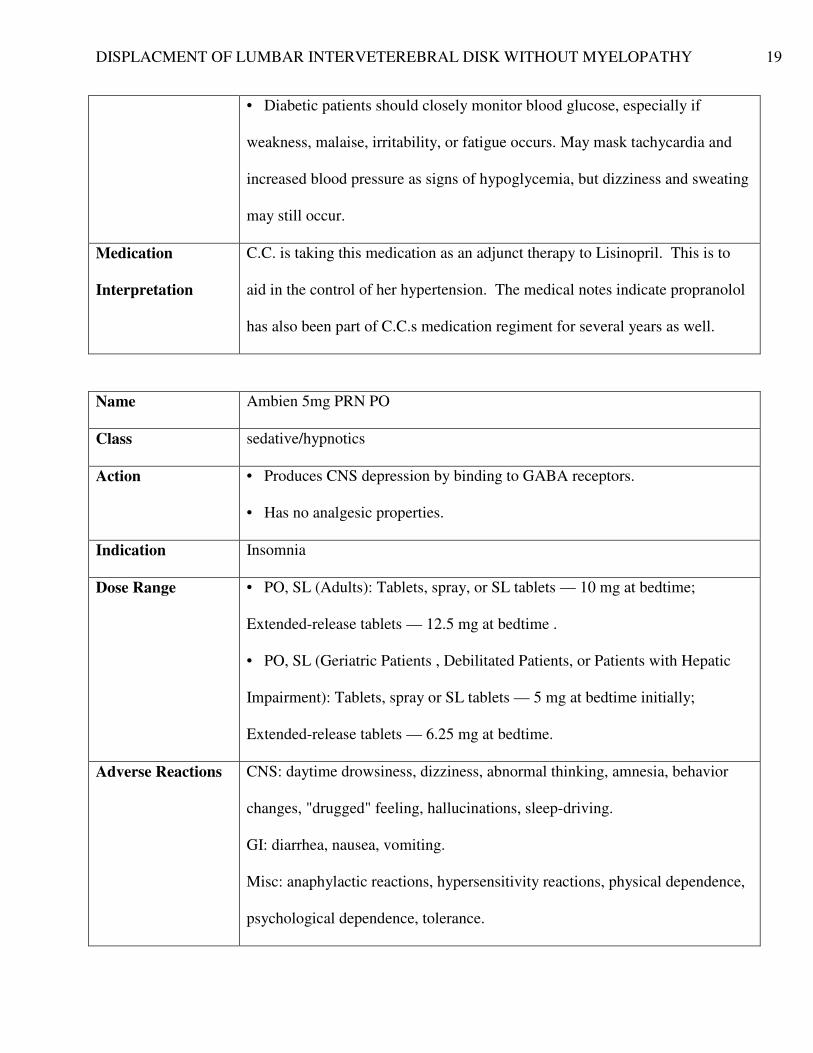
• Diabetic patients should closely monitor blood glucose, especially if
weakness, malaise, irritability, or fatigue occurs. May mask tachycardia and
increased blood pressure as signs of hypoglycemia, but dizziness and sweating
may still occur.
Medication
Interpretation
C.C. is taking this medication as an adjunct therapy to Lisinopril. This is to
aid in the control of her hypertension. The medical notes indicate propranolol
has also been part of C.C.s medication regiment for several years as well.
Name Ambien 5mg PRN PO
Class sedative/hypnotics
Action • Produces CNS depression by binding to GABA receptors.
• Has no analgesic properties.
Indication Insomnia
Dose Range • PO, SL (Adults): Tablets, spray, or SL tablets — 10 mg at bedtime;
Extended-release tablets — 12.5 mg at bedtime .
• PO, SL (Geriatric Patients , Debilitated Patients, or Patients with Hepatic
Impairment): Tablets, spray or SL tablets — 5 mg at bedtime initially;
Extended-release tablets — 6.25 mg at bedtime.
Adverse Reactions CNS: daytime drowsiness, dizziness, abnormal thinking, amnesia, behavior
changes, "drugged" feeling, hallucinations, sleep-driving.
GI: diarrhea, nausea, vomiting.
Misc: anaphylactic reactions, hypersensitivity reactions, physical dependence,
psychological dependence, tolerance.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 20
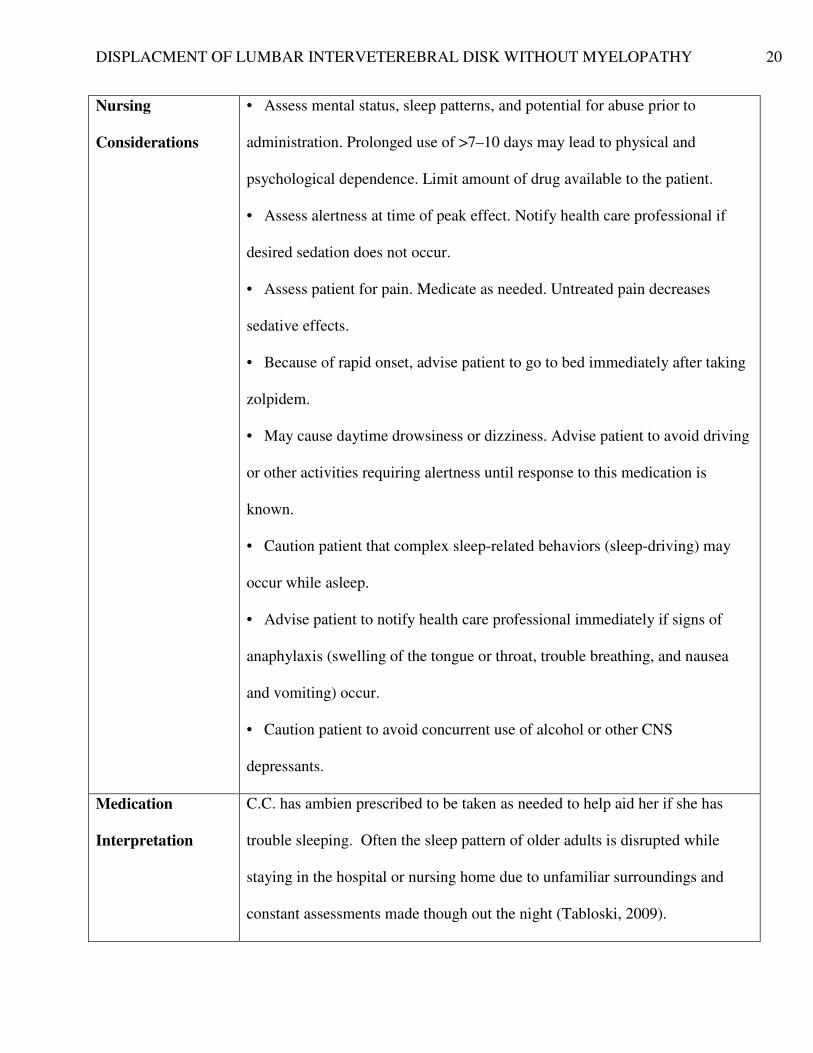
Nursing
Considerations
• Assess mental status, sleep patterns, and potential for abuse prior to
administration. Prolonged use of >7–10 days may lead to physical and
psychological dependence. Limit amount of drug available to the patient.
• Assess alertness at time of peak effect. Notify health care professional if
desired sedation does not occur.
• Assess patient for pain. Medicate as needed. Untreated pain decreases
sedative effects.
• Because of rapid onset, advise patient to go to bed immediately after taking
zolpidem.
• May cause daytime drowsiness or dizziness. Advise patient to avoid driving
or other activities requiring alertness until response to this medication is
known.
• Caution patient that complex sleep-related behaviors (sleep-driving) may
occur while asleep.
• Advise patient to notify health care professional immediately if signs of
anaphylaxis (swelling of the tongue or throat, trouble breathing, and nausea
and vomiting) occur.
• Caution patient to avoid concurrent use of alcohol or other CNS
depressants.
Medication
Interpretation
C.C. has ambien prescribed to be taken as needed to help aid her if she has
trouble sleeping. Often the sleep pattern of older adults is disrupted while
staying in the hospital or nursing home due to unfamiliar surroundings and
constant assessments made though out the night (Tabloski, 2009).
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 21
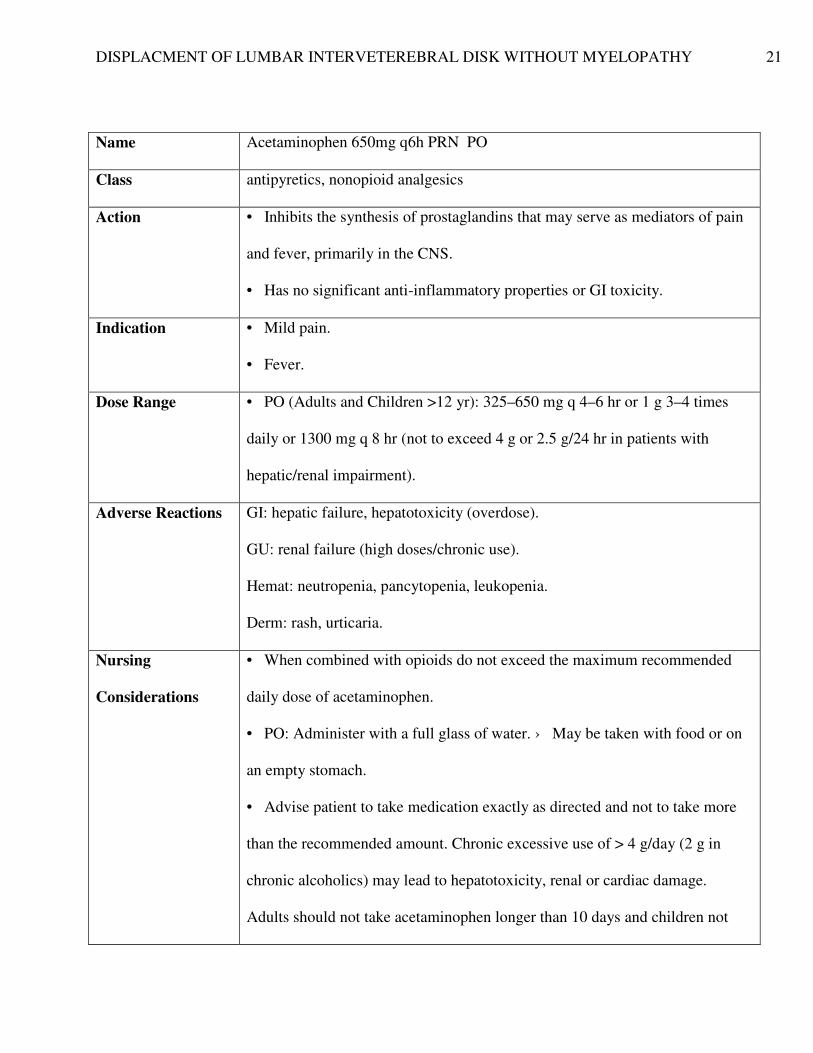
Name Acetaminophen 650mg q6h PRN PO
Class antipyretics, nonopioid analgesics
Action • Inhibits the synthesis of prostaglandins that may serve as mediators of pain
and fever, primarily in the CNS.
• Has no significant anti-inflammatory properties or GI toxicity.
Indication • Mild pain.
• Fever.
Dose Range • PO (Adults and Children >12 yr): 325–650 mg q 4–6 hr or 1 g 3–4 times
daily or 1300 mg q 8 hr (not to exceed 4 g or 2.5 g/24 hr in patients with
hepatic/renal impairment).
Adverse Reactions GI: hepatic failure, hepatotoxicity (overdose).
GU: renal failure (high doses/chronic use).
Hemat: neutropenia, pancytopenia, leukopenia.
Derm: rash, urticaria.
Nursing
Considerations
• When combined with opioids do not exceed the maximum recommended
daily dose of acetaminophen.
• PO: Administer with a full glass of water. › May be taken with food or on
an empty stomach.
• Advise patient to take medication exactly as directed and not to take more
than the recommended amount. Chronic excessive use of > 4 g/day (2 g in
chronic alcoholics) may lead to hepatotoxicity, renal or cardiac damage.
Adults should not take acetaminophen longer than 10 days and children not
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 22
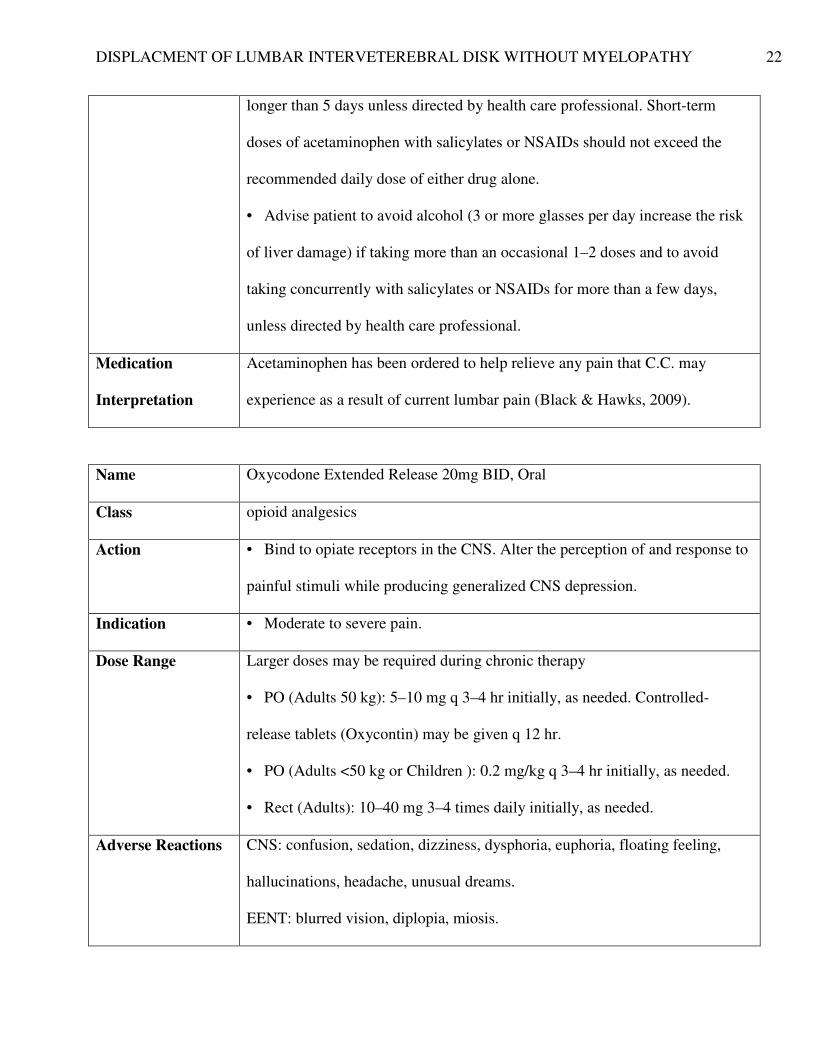
longer than 5 days unless directed by health care professional. Short-term
doses of acetaminophen with salicylates or NSAIDs should not exceed the
recommended daily dose of either drug alone.
• Advise patient to avoid alcohol (3 or more glasses per day increase the risk
of liver damage) if taking more than an occasional 1–2 doses and to avoid
taking concurrently with salicylates or NSAIDs for more than a few days,
unless directed by health care professional.
Medication
Interpretation
Acetaminophen has been ordered to help relieve any pain that C.C. may
experience as a result of current lumbar pain (Black & Hawks, 2009).
Name Oxycodone Extended Release 20mg BID, Oral
Class opioid analgesics
Action • Bind to opiate receptors in the CNS. Alter the perception of and response to
painful stimuli while producing generalized CNS depression.
Indication • Moderate to severe pain.
Dose Range Larger doses may be required during chronic therapy
• PO (Adults 50 kg): 5–10 mg q 3–4 hr initially, as needed. Controlled-
release tablets (Oxycontin) may be given q 12 hr.
• PO (Adults <50 kg or Children ): 0.2 mg/kg q 3–4 hr initially, as needed.
• Rect (Adults): 10–40 mg 3–4 times daily initially, as needed.
Adverse Reactions CNS: confusion, sedation, dizziness, dysphoria, euphoria, floating feeling,
hallucinations, headache, unusual dreams.
EENT: blurred vision, diplopia, miosis.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 23
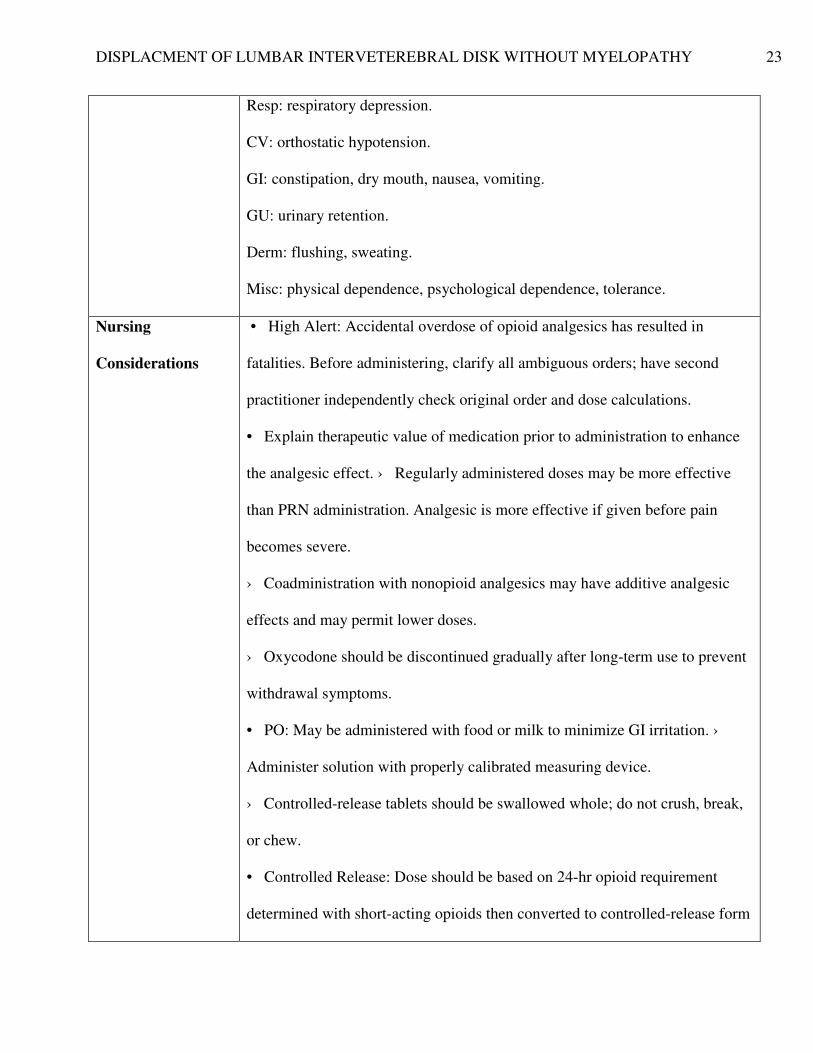
Resp: respiratory depression.
CV: orthostatic hypotension.
GI: constipation, dry mouth, nausea, vomiting.
GU: urinary retention.
Derm: flushing, sweating.
Misc: physical dependence, psychological dependence, tolerance.
Nursing
Considerations
• High Alert: Accidental overdose of opioid analgesics has resulted in
fatalities. Before administering, clarify all ambiguous orders; have second
practitioner independently check original order and dose calculations.
• Explain therapeutic value of medication prior to administration to enhance
the analgesic effect. › Regularly administered doses may be more effective
than PRN administration. Analgesic is more effective if given before pain
becomes severe.
› Coadministration with nonopioid analgesics may have additive analgesic
effects and may permit lower doses.
› Oxycodone should be discontinued gradually after long-term use to prevent
withdrawal symptoms.
• PO: May be administered with food or milk to minimize GI irritation. ›
Administer solution with properly calibrated measuring device.
› Controlled-release tablets should be swallowed whole; do not crush, break,
or chew.
• Controlled Release: Dose should be based on 24-hr opioid requirement
determined with short-acting opioids then converted to controlled-release form
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 24
Medication
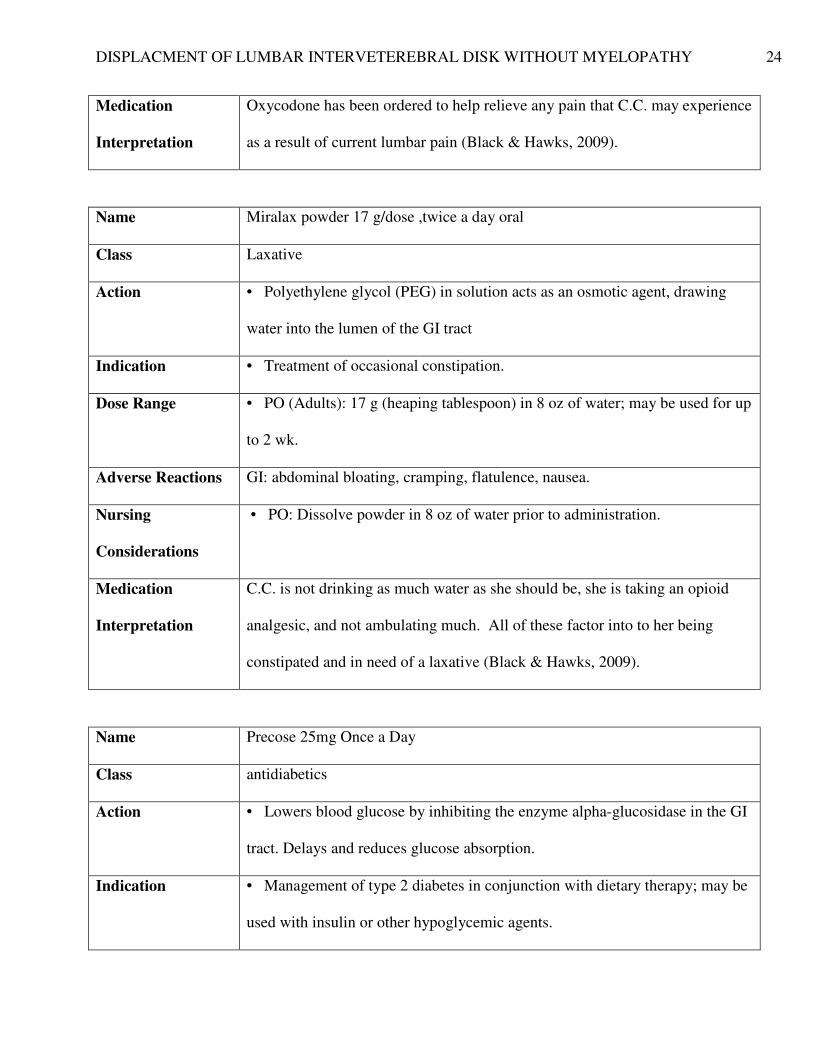
Interpretation
Oxycodone has been ordered to help relieve any pain that C.C. may experience
as a result of current lumbar pain (Black & Hawks, 2009).
Name Miralax powder 17 g/dose ,twice a day oral
Class Laxative
Action • Polyethylene glycol (PEG) in solution acts as an osmotic agent, drawing
water into the lumen of the GI tract
Indication • Treatment of occasional constipation.
Dose Range • PO (Adults): 17 g (heaping tablespoon) in 8 oz of water; may be used for up
to 2 wk.
Adverse Reactions GI: abdominal bloating, cramping, flatulence, nausea.
Nursing
Considerations
• PO: Dissolve powder in 8 oz of water prior to administration.
Medication
Interpretation
C.C. is not drinking as much water as she should be, she is taking an opioid
analgesic, and not ambulating much. All of these factor into to her being
constipated and in need of a laxative (Black & Hawks, 2009).
Name Precose 25mg Once a Day
Class antidiabetics
Action • Lowers blood glucose by inhibiting the enzyme alpha-glucosidase in the GI
tract. Delays and reduces glucose absorption.
Indication • Management of type 2 diabetes in conjunction with dietary therapy; may be
used with insulin or other hypoglycemic agents.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 25
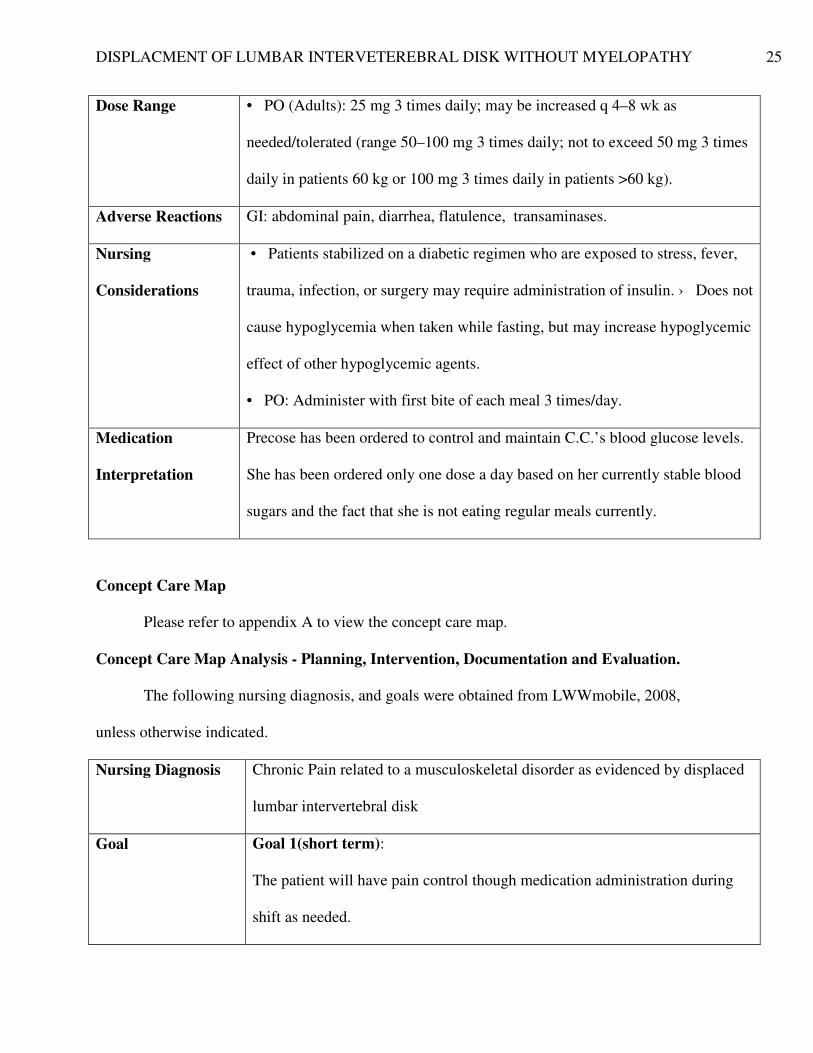
Dose Range • PO (Adults): 25 mg 3 times daily; may be increased q 4–8 wk as
needed/tolerated (range 50–100 mg 3 times daily; not to exceed 50 mg 3 times
daily in patients 60 kg or 100 mg 3 times daily in patients >60 kg).
Adverse Reactions GI: abdominal pain, diarrhea, flatulence, transaminases.
Nursing
Considerations
• Patients stabilized on a diabetic regimen who are exposed to stress, fever,
trauma, infection, or surgery may require administration of insulin. › Does not
cause hypoglycemia when taken while fasting, but may increase hypoglycemic
effect of other hypoglycemic agents.
• PO: Administer with first bite of each meal 3 times/day.
Medication
Interpretation
Precose has been ordered to control and maintain C.C.’s blood glucose levels.
She has been ordered only one dose a day based on her currently stable blood
sugars and the fact that she is not eating regular meals currently.
Concept Care Map
Please refer to appendix A to view the concept care map.
Concept Care Map Analysis - Planning, Intervention, Documentation and Evaluation.
The following nursing diagnosis, and goals were obtained from LWWmobile, 2008,
unless otherwise indicated.
Nursing Diagnosis Chronic Pain related to a musculoskeletal disorder as evidenced by displaced
lumbar intervertebral disk
Goal Goal 1(short term):
The patient will have pain control though medication administration during
shift as needed.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 26
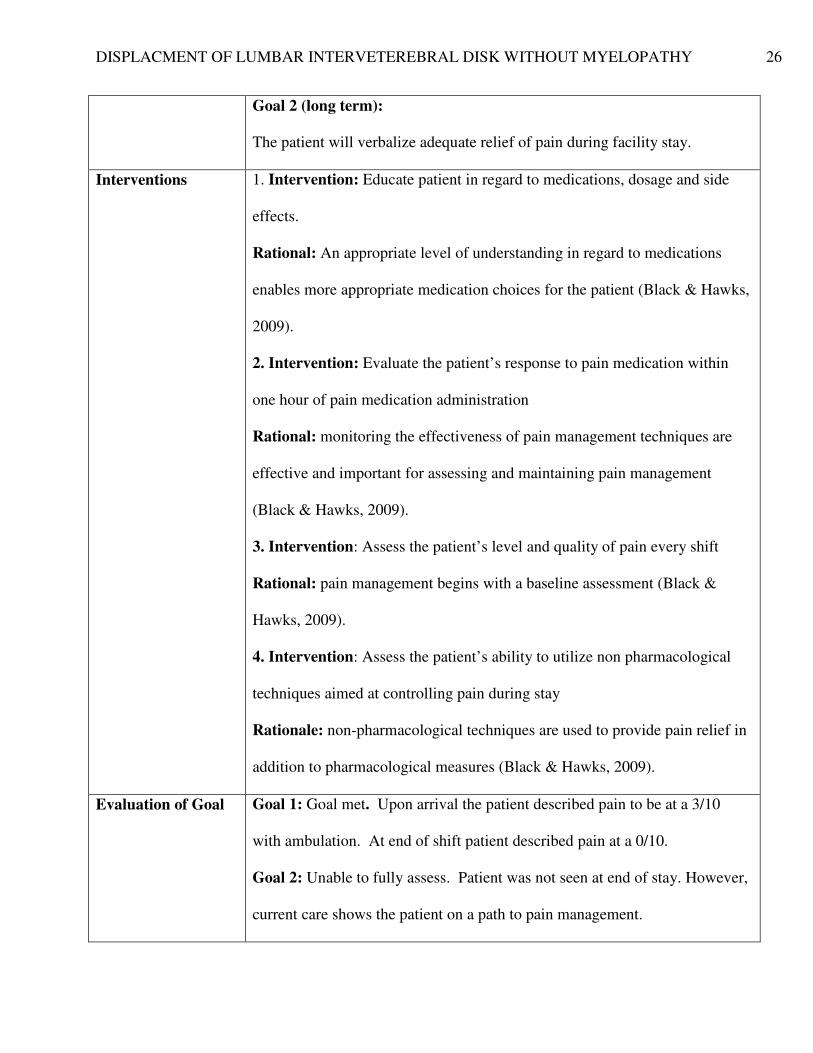
Goal 2 (long term):
The patient will verbalize adequate relief of pain during facility stay.
Interventions 1. Intervention: Educate patient in regard to medications, dosage and side
effects.
Rational: An appropriate level of understanding in regard to medications
enables more appropriate medication choices for the patient (Black & Hawks,
2009).
2. Intervention: Evaluate the patient’s response to pain medication within
one hour of pain medication administration
Rational: monitoring the effectiveness of pain management techniques are
effective and important for assessing and maintaining pain management
(Black & Hawks, 2009).
3. Intervention: Assess the patient’s level and quality of pain every shift
Rational: pain management begins with a baseline assessment (Black &
Hawks, 2009).
4. Intervention: Assess the patient’s ability to utilize non pharmacological
techniques aimed at controlling pain during stay
Rationale: non-pharmacological techniques are used to provide pain relief in
addition to pharmacological measures (Black & Hawks, 2009).
Evaluation of Goal Goal 1: Goal met. Upon arrival the patient described pain to be at a 3/10
with ambulation. At end of shift patient described pain at a 0/10.
Goal 2: Unable to fully assess. Patient was not seen at end of stay. However,
current care shows the patient on a path to pain management.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 27
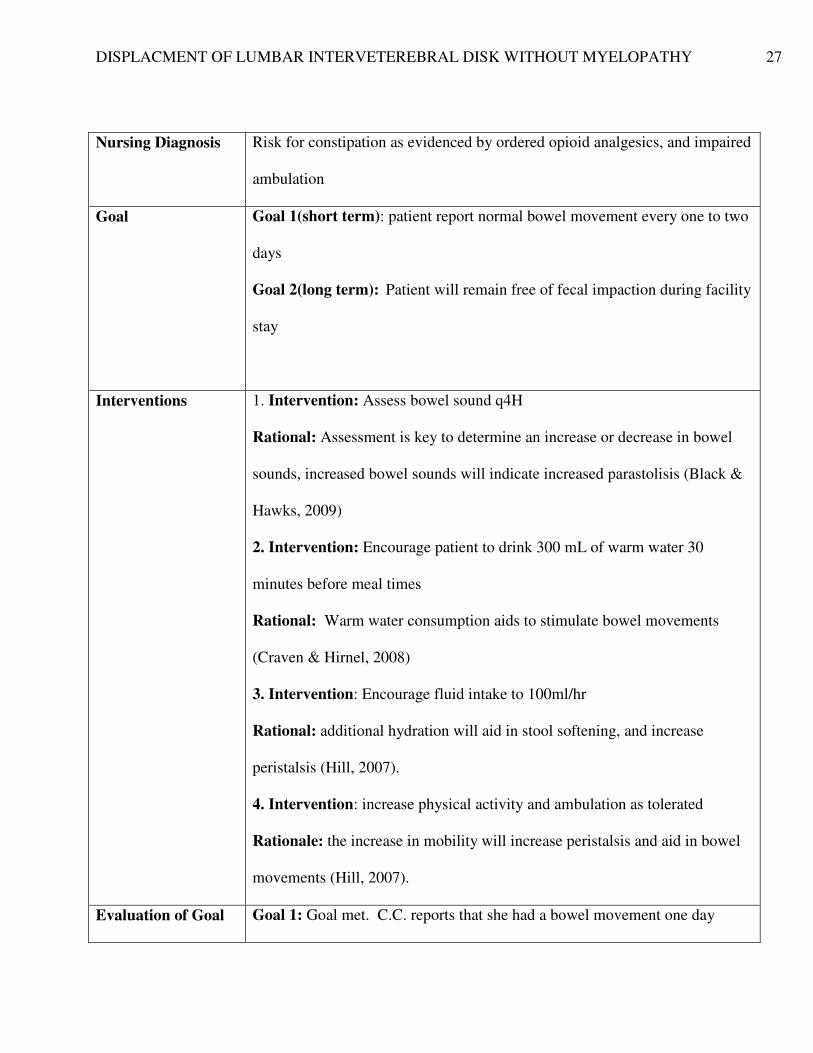
Nursing Diagnosis Risk for constipation as evidenced by ordered opioid analgesics, and impaired
ambulation
Goal Goal 1(short term): patient report normal bowel movement every one to two
days
Goal 2(long term): Patient will remain free of fecal impaction during facility
stay
Interventions 1. Intervention: Assess bowel sound q4H
Rational: Assessment is key to determine an increase or decrease in bowel
sounds, increased bowel sounds will indicate increased parastolisis (Black &
Hawks, 2009)
2. Intervention: Encourage patient to drink 300 mL of warm water 30
minutes before meal times
Rational: Warm water consumption aids to stimulate bowel movements
(Craven & Hirnel, 2008)
3. Intervention: Encourage fluid intake to 100ml/hr
Rational: additional hydration will aid in stool softening, and increase
peristalsis (Hill, 2007).
4. Intervention: increase physical activity and ambulation as tolerated
Rationale: the increase in mobility will increase peristalsis and aid in bowel
movements (Hill, 2007).
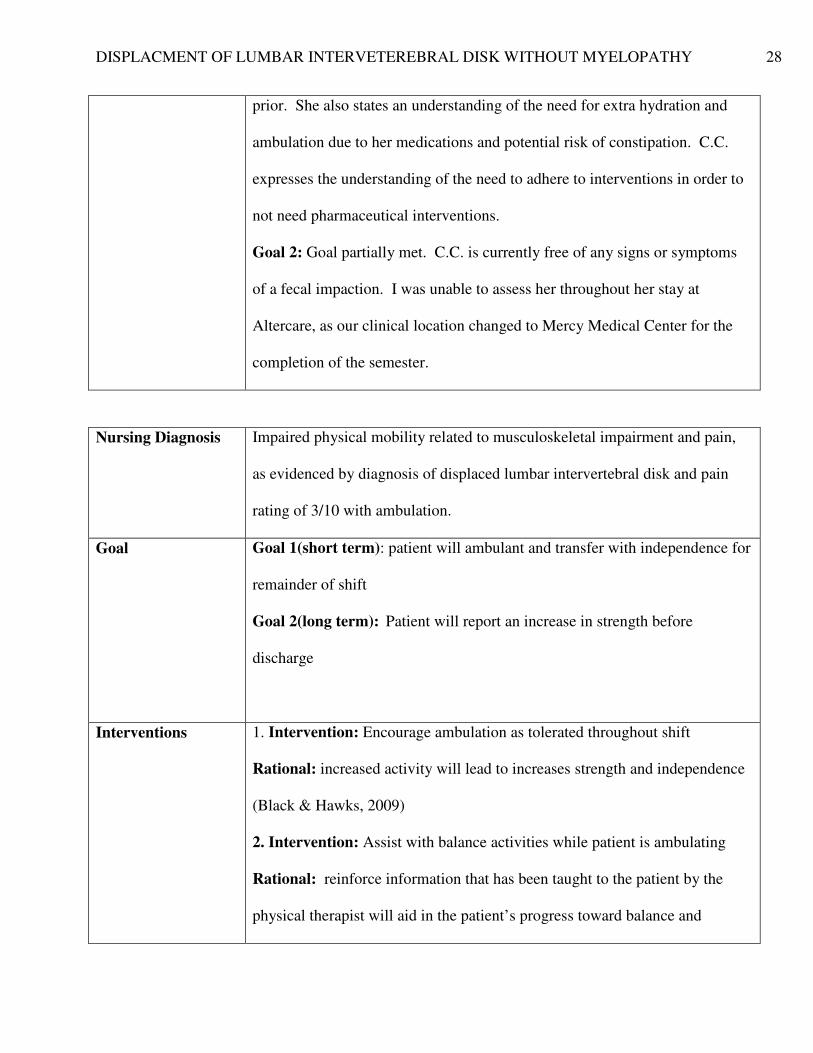
Evaluation of Goal Goal 1: Goal met. C.C. reports that she had a bowel movement one day
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 28
prior. She also states an understanding of the need for extra hydration and
ambulation due to her medications and potential risk of constipation. C.C.
expresses the understanding of the need to adhere to interventions in order to
not need pharmaceutical interventions.
Goal 2: Goal partially met. C.C. is currently free of any signs or symptoms
of a fecal impaction. I was unable to assess her throughout her stay at
Altercare, as our clinical location changed to Mercy Medical Center for the
completion of the semester.
Nursing Diagnosis Impaired physical mobility related to musculoskeletal impairment and pain,
as evidenced by diagnosis of displaced lumbar intervertebral disk and pain
rating of 3/10 with ambulation.
Goal Goal 1(short term): patient will ambulant and transfer with independence for
remainder of shift
Goal 2(long term): Patient will report an increase in strength before
discharge
Interventions 1. Intervention: Encourage ambulation as tolerated throughout shift
Rational: increased activity will lead to increases strength and independence
(Black & Hawks, 2009)
2. Intervention: Assist with balance activities while patient is ambulating
Rational: reinforce information that has been taught to the patient by the
physical therapist will aid in the patient’s progress toward balance and
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 29
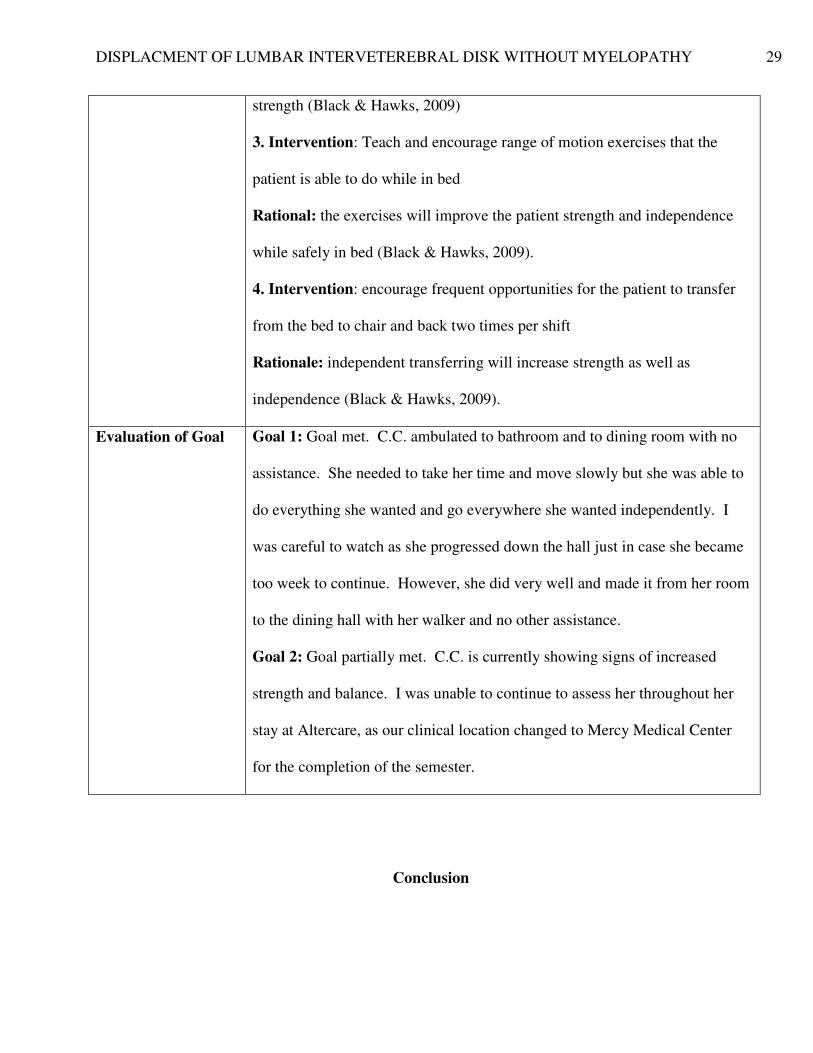
strength (Black & Hawks, 2009)
3. Intervention: Teach and encourage range of motion exercises that the
patient is able to do while in bed
Rational: the exercises will improve the patient strength and independence
while safely in bed (Black & Hawks, 2009).
4. Intervention: encourage frequent opportunities for the patient to transfer
from the bed to chair and back two times per shift
Rationale: independent transferring will increase strength as well as
independence (Black & Hawks, 2009).
Evaluation of Goal Goal 1: Goal met. C.C. ambulated to bathroom and to dining room with no
assistance. She needed to take her time and move slowly but she was able to
do everything she wanted and go everywhere she wanted independently. I
was careful to watch as she progressed down the hall just in case she became
too week to continue. However, she did very well and made it from her room
to the dining hall with her walker and no other assistance.
Goal 2: Goal partially met. C.C. is currently showing signs of increased
strength and balance. I was unable to continue to assess her throughout her
stay at Altercare, as our clinical location changed to Mercy Medical Center
for the completion of the semester.
Conclusion
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 30
At the conclusion of the shift it was my observation that C.C. had done quite well
throughout the day which I cared for her. Her physical status did not change much during the
course of my shift, except that as the night progressed she ambulated more frequently. As for
her spirits and general mood, she seemed to be feeling more comfortable and have a better
acceptance of her current condition. I was able to spend a great deal of time with her as a result
of her being one of only two patients for the day. As the day progressed she became more
comfortable with me and opened up about her ups and downs she has experienced both
physically and mentally throughout her life and current diagnosis.
DISPLACMENT OF LUMBAR INTERVETEREBRAL DISK WITHOUT MYELOPATHY 31
References
Black, J.M., Hawks, J.H. (2009). Medical-surgical nursing: Clinical management for positive
outcomes. (8th ed). St. Louis, MO: Saunders, an imprint of Elsevier Inc. Craven, R.F.,&
Hirnel, C.J. (Ed.). (2008). Fundamentals of nursing(6th ed.). Philadelphia, PA: Wolters
Kluwer
Craven, R.F. & Hirnle, C.J. (2009). Fundamentals of nursing: Human health and function. (6th
ed). Philadelphia: Lippincott Company.
Deglin, J., H., & Vallerand, A., H. (2009). Davis’s drug guide for nurses (11th
ed). Philadelphia:
F. A. Davis Company.
Hill, R. (2007). Conquering constipation. LPN, 3(4), 48-53. Retrieved from
http://www.nursingcenter.com/pdf.asp?AID=730744
Tabloski, P.A. (2009). Gerontological nursing (2nd
ed.). Upper Saddle River, NJ: Pearson
Prentice Hall.


![Effect of Seat and Seat Belt characteristics on the Lumbar Spine … · IRC-20-58 IRCOBI conference 2020 470. new head, neck, and rib cage models [16]. The lumbar spine was also modified,](https://img.pdfslide.net/doc/110x75/607c143349220e1d4c055427/effect-of-seat-and-seat-belt-characteristics-on-the-lumbar-spine-irc-20-58-ircobi.jpg)


























