Embed Size (px)
Citation preview

RWANDA NATIONAL HIV AND AIDS MONITORING AND EVALUATION PLAN 2006-2009
PART A : SYSTEMS AND FRAMEWORK
NATIONAL AIDS CONTROL COMMISSION (CNLS)
JUNE 2006

i
Table of Contents
TABLE OF CONTENTS ...................................................................................................... I LIST OF TABLES AND DIAGRAMS .................................................................................. III
DIAGRAMS ....................................................................................................................III ACRONYMS AND ABBREVIATIONS................................................................................. IV ACKNOWLEDGEMENTS.................................................................................................. VI
1.0 NATIONAL HIV M&E CONCEPTUAL FRAMEWORK.............................. 1 1.1 OVERVIEW OF HIV/AIDS STATUS IN RWANDA ................................................ 1 1.2 NATIONAL STRATEGIC FRAMEWORK FOR HIV/AIDS ..................................... 1 1.3 PRINCIPLES OF DEVELOPING AN M&E PLAN .................................................... 3 1.4 METHODS/APPROACHES FOR THE DEVELOPMENT OF THE M&E PLAN.......... 4 1.5 LOGICAL FRAMEWORK IN M&E ....................................................................... 5
2.0 HIV NATIONAL MONITORING & EVALUATION ..................................... 7 IMPLEMENTATION STRATEGY ............................................................................... 7
2.1 PURPOSE OF NATIONAL HIV M&E SYSTEM .................................................... 7 2.2 RWANDA NATIONAL M&E INSTITUTIONAL FRAMEWORK ............................ 12
2.2.1 National Level ................................................................................................. 12 2.2.2 District Level............................................................................................. 13 2.2.3 Ministries/Public Sector Level .................................................................. 13 2.2.4 National Level NGOs, Faith Based Organization, Umbrella Organizations & the Private Sector Level…………………………………………………………………14
3.0 DATA COLLECTION STRATEGY FOR M&E............................................ 26 3.1 COORDINATION OF M&E................................................................................. 26 3.2 DATA SOURCES: ............................................................................................... 26 3.3 INFORMATION PRODUCTS AT NATIONAL LEVEL ............................................ 27 3.4 REPORTING LEVELS AND DATA FLOW ............................................................ 29
3.5.2 Reporting to the CDLS.............................................................................. 31 3.5.3 Reporting of Health related Indicators: e.g. HIS/SIS to CNLS, TRAC to CNLS ......................................................................................................................... 32 3.5.4 Reporting from Other Government ministries and institutions ..................... 33 3.5.5 Reporting from the Civil Society, Umbrella Organizations and the Private sector......................................................................................................................... 33
4.0 THE ROLE OF STAKEHOLDERS IN HIV/AIDS M&E & ........................ 31
COORDINATION MECHANISMS ............................................................................ 31 4.1 THE ROLE OF CNLS /M&E UNIT IN MONITORING NATIONAL RESPONSE .... 31 4.2 THE ROLES AND RESPONSIBILITIES OF DISTRICT M&E FOCAL PERSONS.... 33 4.3 THE ROLE OF GOVERNMENT MINISTRIES AND OTHER PUBLIC INSTITUTIONS/ORGANIZATIONS. .................................................................................. 33 4.4 THE ROLE OF OTHER STAKEHOLDERS. ................................................................ 34
5.0 DISSEMINATION AND USE OF DATA/INFORMATION ......................... 31 6.0 STRENGTHING OF THE NATIONAL HIV M&E SYSTEM: THE IMPLEMENTATION PLAN ........................................................................................ 31

ii
6.1 HARMONIZATION AND IMPLEMENTATION OF THE NATIONAL HIV/AIDS M&E PLAN ............................................................................................................................. 31 6.2 COMPONENTS/AREAS OF INTERVENTIONS ...................................................... 32
7.0 ANNEXES ................................................................................................................ 44

iii
List of Tables and Diagrams Tables Table 1: M&E Results Pyramid ................................................................... 6 Table 2: M&E Results Pathway................................................................... 6 Table 3: Summary for the National Indicators for HIV/AIDS M&E System……15 Table 4: Implementation Plan for Strengthening of M&E System ................ 35 Diagrams Diagram 1: National HIV/AIDS M&E System............................................ 11 Diagram 2: National HIV/AIDS Monitoring and Evaluation Data / Information
Flow ................................................................................... 30 Diagram 3: Data Flow from CDLS to CNLS .............................................. 32

iv
Acronyms and Abbreviations APELAS Association du Privé et du Para-étatique pour la lutte contre
le SIDA ARV Anti-Rétroviraux ART Antiretroviral Therapy CAMERWA Centrale d’Achat des Médicaments Essentiels au Rwanda CBF Common Basket Found BCC Behavioural Change Communication CBO Community Based Organization CDC Center for Disease Control CCC Country Coordination Mechanism CNLS Commission Nationale de Lutte contre le SIDA
CDLS Commission de District de Lutte contre le SIDA
CTS Centre de Transfusion sanguine
DHS Demographic and Health Survey
DQA Data Quality Assurance EABC Education, Abstinence, Fidélité et Usage de préservatifs
EDSR Enquête Démographique et de Santé au Rwanda
FOSA Formation Sanitaire
GIPA Greater Involvement of People Living with HIV/AIDS
GLIA Great Lakes Initiative on AIDS
GoR Government of Rwanda HIS Health Information System HIV Human Immunodeficiency Virus IEC Information, Education, Communication IO Infections Opportunistes IST Infections Sexuellement Transmissibles MAP Multi-sectorial AIDS Program MDG Millennium Development Goals
M&E Monitoring and Evaluation MINADEF Ministère de la Défense
MINALOC Ministère de l’Administration Locale, de la Bonne Gouvernance, du Développement Communautaire et des Affaires Sociales
MINECOFIN Ministère des Finances et de la Planification Economique
MINEDUC Ministère de l’éducation, des Sciences, de la Recherche et de la Technologie
MIGEPROFE Ministère du Genre et de la Promotion de la Famille
v
MIFOTRA Ministère de la Fonction Publique et du Travail
MIJESPOC Ministère de la Jeunesse, de la Culture et des Sports
MINISANTE Ministère de la Santé
MoH Ministry of Health
NRL National Referral Laboratory NGO Non-governmental Organization ONUSIDA Programme conjoint des Nations Unies contre le SIDA OPDAS Organisation des Premières Dames d’Afrique contre le SIDA OVC Orphelins et Autres Enfants Vulnérables PEP Prophylaxie Post Exposition PEPFAR President’s Emergency Plan For AIDS Relief PMTCT/PMTE Prevention of Mother To Child Transmission PNLS Programme National de Lutte contre le SIDA PNM Plan National Multisectoriel PRSP Poverty Reduction Strategic Paper
PVVIH Personnes Vivant avec le VIH/SIDA RCLS Réseau des Confessions Religieuses de Lutte contre le SIDA RGPH Recensement Général de la Population et de l’Habitat RRP+ Réseau des Personnes Vivant avec le VIH/SIDA SIDA Syndrome de l’Immunodéficience Acquise SIS Système d’Information Sanitaire TB Tuberculose TRAC Treatment and Research on AIDS Center UA Union Africaine UNGASS United Nations General Assembly Special Session on AIDS VCT Voluntary Counseling and Testing

vi
Acknowledgements The development of a national HIV and AIDS monitoring and evaluation plan is as an important a task as it is to track the progress in the implementation of strategies for national response to HIV and AIDS. This plan would have been incomplete and indeed lacking ownership without the consensus and a wider participation from different stakeholders and partners for whom the CNLS is particularly acknowledges their contribution to the finalization of this document. The CNLS boasts of the active and committed national HIV and AIDS monitoring and evaluation technical working group (M&E TWG). This committee has had insightful technical contribution in all the process of development of this plan. The conception of this document was made possible though technical team comprised of Monitoring and Evaluation experts from the CNLS, USAID/PEPFAR, MEASURE EVALUATION/Constella Futures Group, UNAIDS, Tulane University and from the World Bank/GAMET. We highly acknowledge the Rwanda USG/PEPFAR for providing financial support to facilitate the whole process of conception, drafting, validation and subsequently producing manuscripts of this important document. Our appreciation also goes to all the CNLS staff, key development partners and the umbrella organizations who participated in one way or the other in making the production of this report possible. The overall leadership and coordination role played by the Executive Secretary of the CNLS, and the Directorate of Planning, Coordination, Monitoring and Evaluation is highly appreciated. Rev. Pastor Nathan Gasatura President National AIDS Control Commission, CNLS.
vii
Foreword The GoR has demonstrated a high level commitment to fight HIV/AIDS, through a multi-sectoral response, involving a multidimensional and community based approach. The creation of the National AIDS Control Commission (CNLS) in 2001, and subsequent creation of the decentratilized coordination structures and the umbrella organizations has enabled a harmonized coordination of the implementation of HIV/AIDS interventions in the country. To facilitate effective coordination of monitoring and evaluation of national response to HIV/AIDS, the CNLS has developed a National HIV/AIDS Monitoring and Evaluation Implementation Plan Part I that is a basis of enhancing national HIV Monitoring and Evaluation (M&E) system. The following issues make the establishment of a functional HIV M&E system mandatory in Rwanda: The GoR’s commitment to scale up existing HIV/AIDS interventions and
effectively coordinate the same requires a comprehensive M&E system that would provide accurate and reliable data in a timely manner for decision making and targeting;
There are different players and stakeholders who invest resources into
HIV/AIDS programmes and are operating in different parts of the country. Tracking progress of their interventions and impact they are making requires a functional national HIV M&E system;
Currently, there are many sources of funding for HIV/AIDS programmes in
Rwanda, including bilateral agencies, the Global Fund to fight AIDS, Tuberculosis and Malaria, the World Bank’s Multi-country Programs (MAP) for Africa and the USA Presidential Emergency Plan for AIDS Relief (PEPFER). In this era of accountability and transparency, stakeholders and development partners within and outside the country demand effective performance and transparency in the use of funds. Besides, they demand to see what kind of outcomes and impacts are created by the invested resources. A functional HIV M&E system is essential in meeting these demands.
From this perspective, a functional national M&E system becomes a core business in national response to HIV/AIDS. A functional system must be put in place as: a source of information on the progress being made under various interventions in the country. ii. A management tool for the CNLS and various implementers at both national and district levels, across different public and private sectors. After many consultations with different stakeholders, the national M&E Conceptual framework for the Multi−sectoral response to HIV/AIDS in RWANDA is now finalized. The framework will be followed by the development of an M&E

viii
operational manual (users’ guides) targeting implementers of HIV/AIDS interventions in the country. The execution of this national HIV/AIDS M&E Plan requires human, financial and physical resources. There is need, therefore, to build consensus on investment strategy for enhancing national HIV M&E system. In this regard, all stakeholders are reminded to give due emphasis to the M&E system by allocating enough resources and enhancing the capacity of their own staff through training and sharing their experiences and best practices. Finally, I would like to take this opportunity to thank the development partners, organizations and individuals that supported the development and finalization of the National HIV/AIDS M&E Framework.
Dr Agnes BINAGWAHO Secretary Executive of the CNLS

ix
Organization of the Document The National HIV and AIDS Monitoring and Evaluation Plan Part I provides the conceptual framework and defines the Rwanda National HIV Monitoring and Evaluation (M&E) System. This conceptual document is divided into 6 Sections.
Section I presents an overview of HIV/AIDS status in Rwanda, the principles and process of the development of this document and the logical framework in the M&E system;
Section II describes the national HIV M&E system including the implementation strategy, institutional framework and national HIV indicators; Section III presents data collection strategy, data sources, information products and reporting levels/data flow; Section IV describes the role of different stakeholders: CNLS, CDLS, public sector, research institutions, and umbrella organizations, in HIV/AIDS M&E and coordination mechanisms; and
Section V describes dissemination and use of data/information for decision making and evidence-based planning of HIV/AIDS activities in the country.
Section VI describes the harmonization the national M&E plan and presents the framework for strengthening the CNLS M&E system,
including specific areas of intervention, the indicative budget and sources of funding.
Part II of this document (an operational manual / users’ guide) will be
developed and published at a later date. This will be a technical document describing each data source, its data flow and frequency. The document will also have a costed national ‘road-map’ – detailed operational (work) plan for M&E at decentralized levels. It will also have formats of required information products.

1
1.0 National HIV M&E Conceptual Framework 1.1 Overview of HIV/AIDS Status in Rwanda The third Demographic and Health Survey conducted in 2005 indicates that in Rwanda 3% of the people live with HIV. The data shows that women are particularly vulnerable to HIV infection. About 3,6 per cent of women are infected compared with 2,3 per percent of their male counterparts. Prevalence rates according to rural and urban settings show a higher infection in urban areas 7,3 percent compared to 2,2 percent in rural population. Kigali city showed a comparatively highest proportion of population infected with HIV with 5,6 percent, followed by the Western Province 3,2 percent, Southern Province 2,7 percent, Eastern Province 2,5 percent and Northern Province with 2,2 percent.
According to TRAC report, January 2005, the prevalence rates from the sentinel surveillance sites were between 2-4% in rural areas and 7-11% in urban areas. . A nationwide PLACE study in 2005 shows that age of sex debut is less than 20 years, with important urban-rural differences in the selected sites. For youth aged 15-19, 57 percent males and 60 percent females in urban areas started sexual relations, compared with 44 percent males and 47 percent females in rural areas. Likewise, use of condom is still low. The study indicates that many young people are still engaged in risky sexual behaviour, for example, it is indicated that during the last sexual intercourse, 75 percent males and 71 percent females in urban areas reported condom use, compared to 21 percent males and 13 percent females in rural sites. Quantitative information about other vulnerable groups such as refugees and prisoners are not readily available. This also applies to most at risk populations such as MSM, sex workers and IDUs. 1.2 National Strategic Framework for HIV/AIDS The National AIDS Control Commission (CNLS) has, in consultation with stakeholders in the country, developed documents to guide the national response to HIV/AIDS. These include the following: The National Strategic Framework for HIV/AIDS Control (2002-2006) and its
operational Multisectoral National Plan for HIV/AIDS response; National HIV/AIDS Monitoring and Evaluation Plan 2002-2006;
The revised National Strategic Framework for HIV/AIDS Control (2005-2009);
and
2
The National Policy on HIV/AIDS (2005-2009). In addition, several strategies and policies have been developed to respond to specific thematic areas in an endeavor to prevent the chain of transmission of the epidemic, treatment, care and support to infected and affected people as well as improving socio-economic status of PLWA and other vulnerable groups. Following the recommendations of the joint Mid-Term Review (MTR) of the implementation of the National Multi-sectoral Plan for HIV/AIDS response (2002-2006) concluded in January 2005, the is now a revised National Strategic Framework for the program cycle of 2005-2009. The new Strategy has five strategic components. These are as follows:
1. Reinforce measures of preventing HIV/AIDS transmission; with the
following intermediate results: I.1 Change (reduce) high risk sexual behavior (in the population); I.2 Change behavior of health personnel to reduce the transmission of HIV/AIDS, STI, OI and TB; I.3 Reduce transmission of HIV through medical prophylaxis; and I.4 Create a cultural environment more favorable to preventing HIV and STI
transmission. 2. Assure that the national response to HIV and AIDS is adapted to
Rwanda’s evolving socio-economic & health conditions by using of surveillance and research results, with the following intermediate results:
II.1 Increase the usefulness of surveillance results with respect to the national response to HIV and AIDS;
II.2 Increase the usefulness of research results, studies and evaluations; II.3 Facilitate the interpretation and use of surveillance and results for
and by all stakeholders. 3. Improving HIV/AIDS-related treatment for persons infected and
affected by AIDS; with the following intermediate results: III.1 Increase access to high quality care and treatment at health facilities; III.2 Increase access to high quality community-based care and treatment; III.3 Assure that HIV/AIDS related care and treatment is sustainable. 4. Mitigate the socio-economic impact of HIV and AIDS, with the
following intermediate results: IV.1 Improve the social and economic conditions in Rwanda (and ensure vulnerable groups benefit as much as others); IV.2: Defend and promote human rights; and IV.3 Strengthen decision making capacities of associations involved in
3
HIV/AIDS notably through the concept of GIPA. 5. Coordination of the Multi-sector response for increased cost-
Effectiveness, with the following intermediate results: V.1: Improve the capacities of national HIV/AIDS coordination structures; V.2: Assure that HIV/AIDS strategies within national sector plans are
Implemented; V.3 Increase HIV/AIDS related regional initiatives that are jointly executed; V.4. Assure that intervention agencies benefit from national planning and
monitoring as much as the coordination agencies; and V.5 Jointly evaluate the multi-sectoral response to HIV and AIDS. 1.3 Principles of Developing an M&E Plan Based on the nature of national response to HIV and AIDS and being committed to the “Three Ones” principles, various partners at both national and decentralized levels are committed to the development and operation of a national HIV Monitoring and Evaluation (M&E) system. The following principles guided the development of the national HIV M&E Plan: o Building strategic dialogue and partnership for M&E: The multi- sectoral approach to national response to HIV and AIDS builds on a continuous dialogue and partnership among various stakeholders. This principle also applies to the development of a functional national HIV M&E system. o Mainstreaming M&E into HIV/AIDS Programme: National HIV M&E system will be mainstreamed into the national HIV and AIDS programme. Enough financial resources will be mobilized and allocated for the establishment of a functional M&E system. o Standardized core national system: A comprehensive national system will have core national indicators and a standardized system / tools that would enhance data collection, analysis, and production of national information products for dissemination to various stakeholders at the international, national and districts levels. Simplicity: Simplicity will guide data collection, analysis and dissemination of information products to various stakeholders. This is to make data user friendly and simple to use for decision making and programming. o Data Quality Assessment (DQA): A good M&E requires both internal self-assessment and external verification of data/information. Thus,

4
implementing partners will collect their own data but an external agency, in this case the CNLS, will put in place DQA protocols to verify the completeness and accuracy of the data collected. Consensus must be built on supervision visits for both internal assessment and external verification of primary data. o Action Orientation: Data colleted at the district or national levels will be used for decision making and programming of HIV/AIDS interventions. There will be a direct link among data collection, analysis, and decision making at all levels of programme implementation. o Timeliness and Reliability of Data: Data collected, disseminated and used through a good M&E system will be timely and reliable. All the implementing partners will be required to be transparent and accountable to the internal M&E system they have and the data they collect and provide to the CDLS and CNLS. These principles are to be put in mind all the time when any M&E activity is planned for, undertaken or reviewed. 1.4 Methods/Approaches for the Development of the M&E Plan Participatory and qualitative methods were used to develop this plan. This participatory process was coordinated by the CNLS M&E Unit and was spearheaded by the M&E Technical Working Group (TWG). An External Consultant provided technical Assistance to the process. Specifically the approaches used included the following: Review of both national and international documents on HIV/AIDS in general
and M&E in particular. The documents included the National HIV/AIDS Strategic Framework 2005-2009; Annual M&E Report, 2005; DHS Report, UNGASS Report, UNAIDS Monitoring and Evaluation Modules, 2000; 2003; National HIV/AIDS Monitoring and Evaluation Plans for Ethiopia, Ghana, Kenya, Malawi and Uganda.
Consultative meetings with the CNLS management and M&E focal persons to
assess the M&E needs and build consensus on the way forward for the plan and strengthening the M&E system.
Consultative meetings with members of the M&E Technical Working Group
and various stakeholders from the umbrella groups, civil society and the development partners. This was to establish the M&E gaps and needs and build consensus on the M&E plan and how to strengthen national HIV M&E System.
5
A one day consultative and technical workshop with members of the M&E
Technical Working Group was held to review draft plan and input into it. A one day national review meeting was also held, bringing together
stakeholders from both the public and private sectors, the civil society organizations and the development partners, where the Draft plan was presented, discussed and consensus built on its content.
1.5 Logical Framework in M&E
There is a simple distinction between monitoring and evaluation. Monitoring is the routine, regular assessment of ongoing activities and progress being made in a programme or project. On the other hand, evaluation is the episodic assessment of overall achievements and the extent to which they can be attributed to specific interventions. In short, monitoring looks at what is being done while evaluation examines the effectiveness of what is being done.
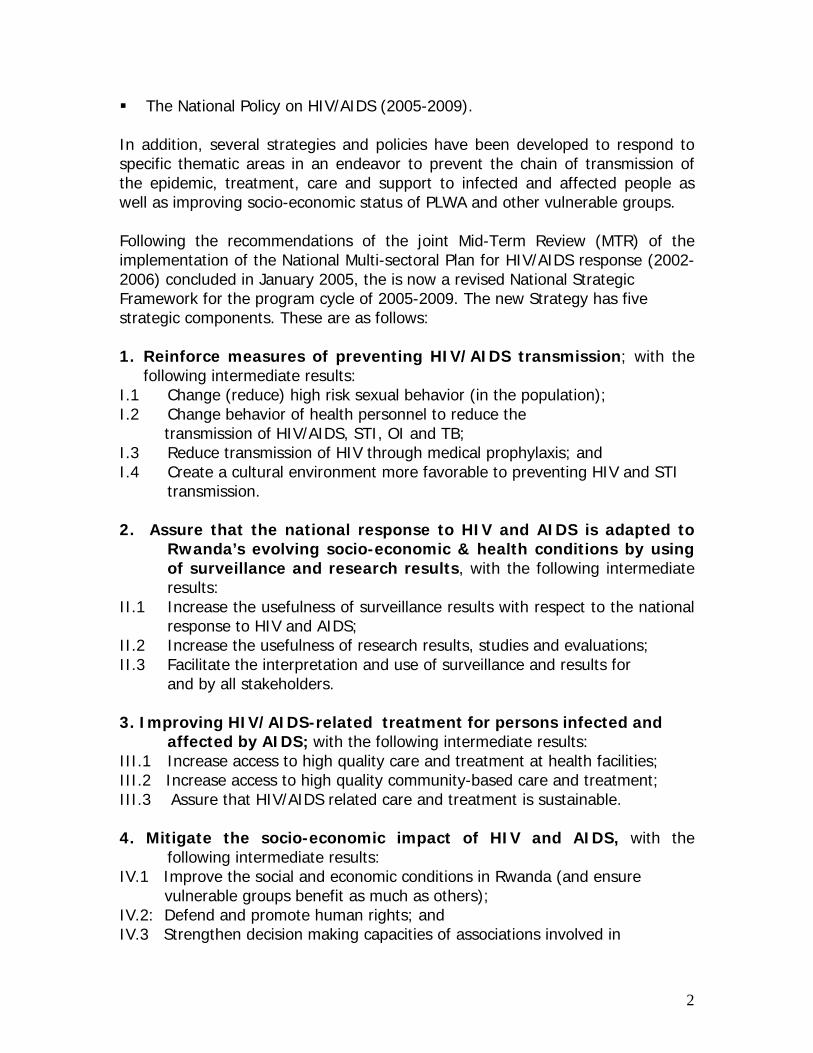
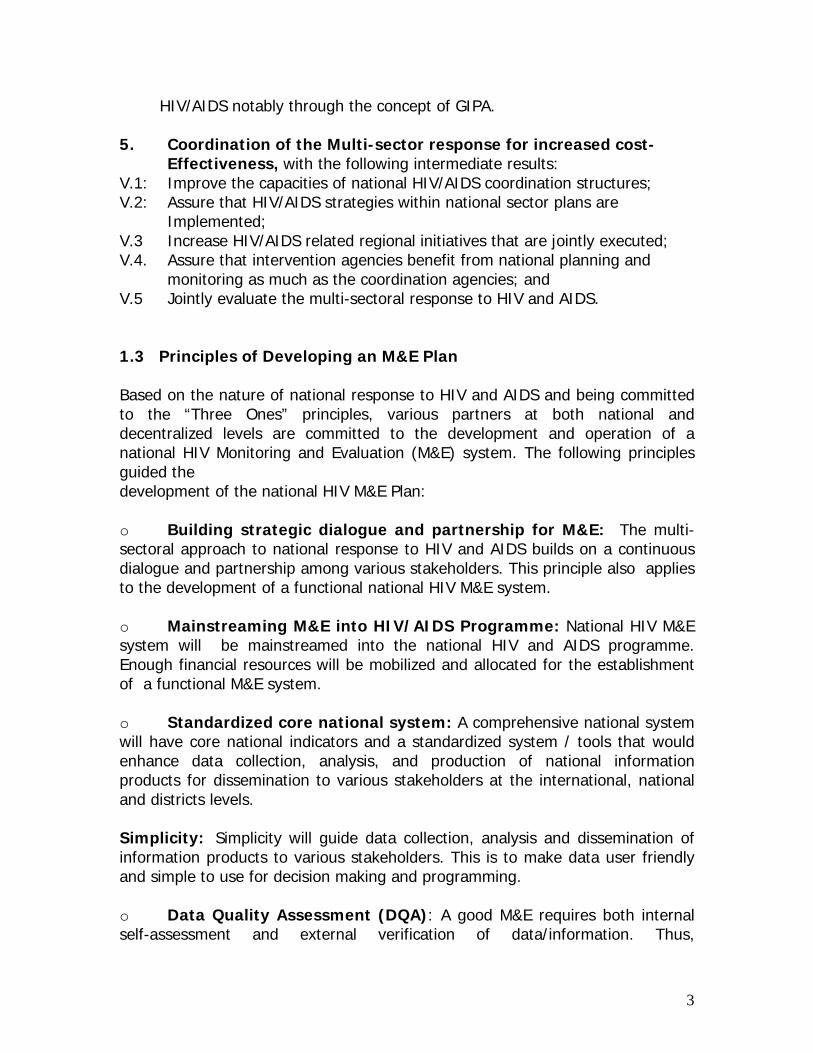
Evaluation draws from data generated by the monitoring system and links this to primary beneficiaries to determine the impact of programmes. Monitoring must be integrated within the programme management structure, whilst evaluation with its comparative characteristics may not need such integral component. An effective M&E system has a clear logical pathway of results which encompass the major levels that include inputs, outputs, outcomes and impacts. Tables 1 and 2 demonstrate these interconnections where:
i. Inputs are the people, training, equipment and resources that are put into a programme in order to achieve the delivery of services;
ii. Outputs are the activities or services delivered, including HIV/AIDS prevention, care and support services, in order to either improve the well being of beneficiaries or change their behaviors;
iii. Outcomes are changes in behavior or skills, especially safer HIV prevention practices and increased ability to cope with AIDS;
iv. Impact is, for example, measurable health changes that are associated with outcomes, particularly reduced STI/HIV transmission.
6
Table 1: M&E Results Pyramid
Table 2: M&E Results Pathway
Program-based Data Population-based Biological, Behavioral & Social Data
StaffFundsMaterialsFacilitiesSupplies
# Staff Trained# Condoms Distributed# Test Kits Distributed# Clients Served# Tests Conducted
Provider BehaviorRisk BehaviorService Use BehaviorClinical Outcomes
HIV Incid/PrevQuality of LifeSocial NormsSTI Incid/PrevAIDS Morb/Mor
Input (Resources)
Output (Service Delivery)
Outcomes(Intermediate
Effects)
Impact(Long-term
Effects)

7
2.0 HIV NATIONAL MONITORING & EVALUATION IMPLEMENTATION STRATEGY 2.1 Purpose of National HIV M&E System
The goal of a National Multisectoral HIV Monitoring and Evaluation System is to enable the CNLS and its partners to monitor the spread and impact of the HIV/AIDS epidemic in Rwanda, to monitor the efficiency of the national response to HIV, and to evaluate the effectiveness of the national response to HIV, providing relevant and accurate HIV data for use in planning effective interventions.
The specific objectives of the national M&E System are to:
• Develop clear M&E strategies that will enable systematic collection of data that can be used to detect changes in the epidemic and effects of interventions (efficiency and effectiveness) and then inform and guide the national HIV response;
• Define the roles of stakeholders – the CNLS, Ministries, Departments and Agencies, local government, networks and umbrella organizations and Civil Society organizations (CSOs) – in the systematic collection, collation, analysis and use of HIV data in order to avoid duplication of efforts;
• Improve information sharing and dissemination of information and the use of data in planning interventions;
• Promote creation of partnerships and linkages between various development stakeholders at the various levels of implementation;
• Promote coordination of HIV services, and ensure equity in the provision of, access to and utilization of HIV services; and
• Monitor the success of the national response as well as identifying lessons learnt and best practices for scaling up.

1
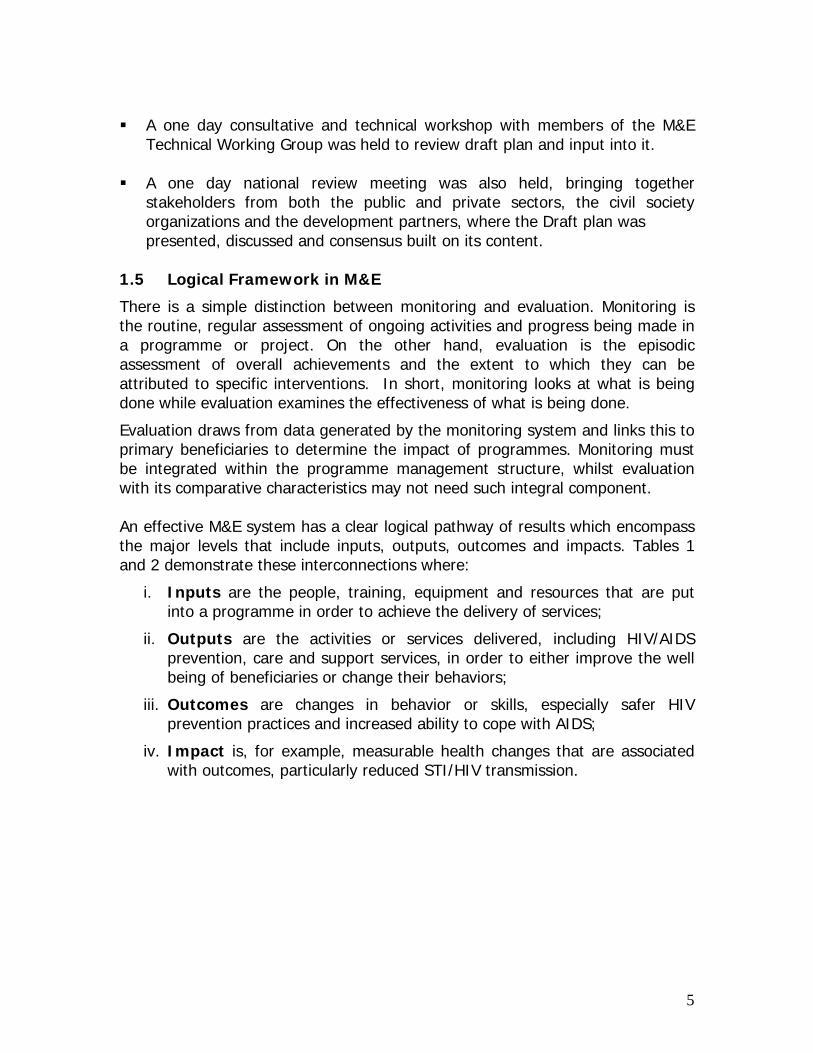
The UNAIDS has provided Checklist of Features of a good and functioning M&E system, which CNLS is committed to use in strengthening the national HIV M&E System. These are summarized in Panel 1: Panel 1: Checklist of Features of a Good and Functioning National M&E System ------------------------------------------------------------------------------------------- M&E Unit: An established and functional M&E Unit with qualified staff and adequate funding and equipment. Such a unit has to be formally linked to the research institutions and leading NGOs, development partners and NGOs. The unit should be able to process data and package and the dissemination of information to various stakeholders. ------------------------------------------------------------------------------------------------------------ Clear Goals There has to be a clear and well-defined national HIV/AIDS programme with clear goals, targets and implementation plan, where regular and participatory reviews and evaluations of progress are undertaken on a regular basis. There are guidelines and guidance to districts and linking M&E to other sectors. Besides, there is coordination of the national and donor M&E needs. ------------------------------------------------------------------------------------------------------------Indicators: A set of agreed upon routine and periodic indicators at different levels. Indicators must be comparable over time, and a number of key indicators that are comparable with other countries. ------------------------------------------------------------------------------------------------------------ Data Collection and Analysis: A national level data collection and analysis plan, including data quality assurance plan. There has also to be a plan to collect data and analyze indicators at different decentralized levels. There has to be second generation surveillance, where behavioral data are linked to HIV/STI surveillance data. ------------------------------------------------------------------------------------------------------------ Data Dissemination: There has to be a national level data/information dissemination plan. This can be in the form of a well-disseminated, informative annual report of the M&E unit, annual meeting to disseminate and discuss M&E and research findings with policy-makers and planners, a centralized data bank and library of all HIV/AIDS/STI-related data collection, including on-going research, and a coordination of national and development partners’ M&E needs. Source: Adapted from UNAIDS et al. (June 2000). National Aids Programme: A Guide to Monitoring and Evaluation. Geneva, Switzerland. The Rwanda National HIV/AIDS M&E System is depicted in Diagram 1 below.

11
Diagram 1: National HIV/AIDS M&E System
National HIV/AIDS Strategic Framework
National HIV/AIDS M&E System
A. National M&E Framework
M&E Operational Manual / Guides
B. Data Sources: BSS, program monitoring data, special studies, etc.
C. CNLS: M&E Unit > Develops
D. Information Products:Service coverage report. M&E Annual Report. Research report. UNGASS report
Priority Indicators:- To Assess Impact To Assess Outcome Monitoring Programme Outputs
F. HIV/AIDS Domain Interventions: Promotion of ABC. Surveillance & research BCC. . Care, Support & treatment VCT / PMTCT. . Legal & human rights Coordination. Support to PLWHA. Capacity Bld.
E. Stakeholders• At National and
District levels:
- Government - Development partners - Umbrella organizations - Civil Society Organizations - NGOs - CBOs
Basis for
M&E results used to enhance interventions
Provide funding
And/Or Implement
Disseminated to stakeholders
12
2.2 Rwanda National M&E Institutional Framework
As of 1st January 2006, the geo-political landscape in Rwanda changed when the Government of Rwanda implemented its decentralisation policy. The 106 districts and 12 provinces were amalgamated into 30 districts, and powers decentralised to these 30 districts. With decentralisation in mind, the CNLS has disbanded the CPLSs and created new CDLSs (District AIDS Coordinating Committees). For now, the Commission has agreed with government that there will be one officer at the district level to coordinate the HIV response. Besides, there is also one office in charge of M&E / data at this level. There are also several NGOs running program activities at both national and district levels. Besides, there are some initiatives within the private sector. In essence, the CNLS’s decentralisation implies: first, that all implementers of HIV/AIDS interventions are to submit work plans in a standard format to the districts, and report on the progress in the implementation of these work plans; and, second, that all HIV interventions will be planned, coordinated and monitored at the district level. Decentralization is to allow districts and communities to focus on their unique challenges and activities specific to their region as far as HIV/AIDS is concerned. From this decentralization policy and a multi-sectoral approach to addressing AIDS pandemic, the National M&E Institutional Framework / Structure is divided into four levels for efficiency and effectiveness of monitoring and evaluating the national response. These levels include the following: The National Level, District Level, Ministries/Public Sector Level and NGOs/Private Sector Level. Although described separately, these levels are linked and form an integral part of the national response package.
2.2.1 National Level The National AIDS Control Commission, CNLS, has the mandate of coordinating, monitoring and evaluating the national response to HIV/AIDS in the country. The Directorate of Planning, M&E, and Coordination, supported by the M&E Focal Person and Data analysts are responsible for M&E. The CNLS has also created a national HIV and AIDS M&E Technical Working Group (TWG), whose members are the M&E experts from the UN agencies, multilateral and bilateral agencies, CNLS umbrella organizations from the public and private sectors, academic and research experts. This team is charged with the responsibility of providing technical assistance in the course of implementation of the national monitoring and evaluation roadmap, and providing training to the coordinating structures, implementing agencies and stakeholders in M&E of programmes.
13
The CNLS is developing a SQL database to capture all indicator information at the district level. This database is functional, although it needs strengthening.
2.2.2 District Level The District AIDS Coordinating Committees (CDLSs) will be chaired and coordinated by one official in each of the 30 CDLS that have been created. There will also be an officer in charge of M&E at this level. CDLS will monitoring and evaluating HIV/AIDS program activities implemented by different players including the public sector, NGOs, CBOs and the private sector operating at the district level. They are also in-charge of submitting program activity data to the CNLS. Other roles include the following: - Organizing district M&E dialogues involving programme implementers and
communities; and - Participating in national M&E dialogues and reviews.
2.2.3 Ministries/Public Sector Level HIV/AIDS is expected to be mainstreamed in each ministry, department and any public sector in the country. Thus, there will be HIV/AIDS control units or sections in each ministry and all public institutions. The role of these units is to: - Develop and mainstream HIV/AIDS activities at ministerial /public institution / organization level; - Monitor implementation of activities and progress being made as per the
ministerial/public sector plan; - Submit HIV/AIDS activity data to the CNLS; - Participating in national M&E review dialogues; and - Contributing to annual M&E reports. The role of TRAC and other research institutions is as follows: ♦ Development of policy, standards and directives 9on research; ♦ Development and dissemination of guidelines and training modules; ♦ Training of trainers; ♦ Supervision of research at the district level; ♦ Coordination of research on STI, OI, VCT/PMTCT, TB and care by ARV,
Socio- behavioral aspects; ♦ Submitting data to MoH and the CNLS.

14
2.2.4 National Level NGOs, Faith Based Organization, Umbrella Organizations & the Private Sector Level The national NGOs and umbrella organizations will be in-charge of monitoring their own HIV/AIDS activities, lobbying and mobilizing resources for such activities. Those NGOs/CBOs at the district level will be in charge of monitoring programme activities and outputs, collecting and analysing activity data, and providing / submitting the same to the CDLS in an agreed format. Specifically there roles include the following:
- Coordinate and mainstream HIV/AIDS activities in their specific
organizations and umbrellas at different levels in the country; - Monitor and evaluate programme / projects outputs and progress being made as per the agreed objectives; - Submit HIV/AIDS programme activity data and information products to
the CDLS and CNLS; - Participating in the national M&E review dialogues; and - Contributing to annual M&E reports. 2.3 Indicators for Monitoring and Evaluation of national response to
HIV and AIDS Core national indicators were selected for inclusion in this framework in a participatory manner. This framework contains both the 62 national top priority indicators and the additional ones as per the Axes (Table 3). Annex 1 presents the indicators, the data sources and the operational definitions for the indicators. The National M&E system has primarily two types of indicators. They include the following: 1. Impact/outcome-level indicators (to measure the long-term and intermediary results in the results framework); and
2. Output/input-level indicators (to measure the activities that have been implemented under each domain). These two types of indicators are complementary. Further more, all the indicators are divided into two categories – medical-related indicators that focus on those efforts driven by the health sector (i.e. those activities that take place at health facilities and in the Ministry of Health and that is being collected by TRAC), and community-related indicators that measure all other efforts in HIV prevention, care, support and impact mitigation that takes place within communities (not at health facilities).

15
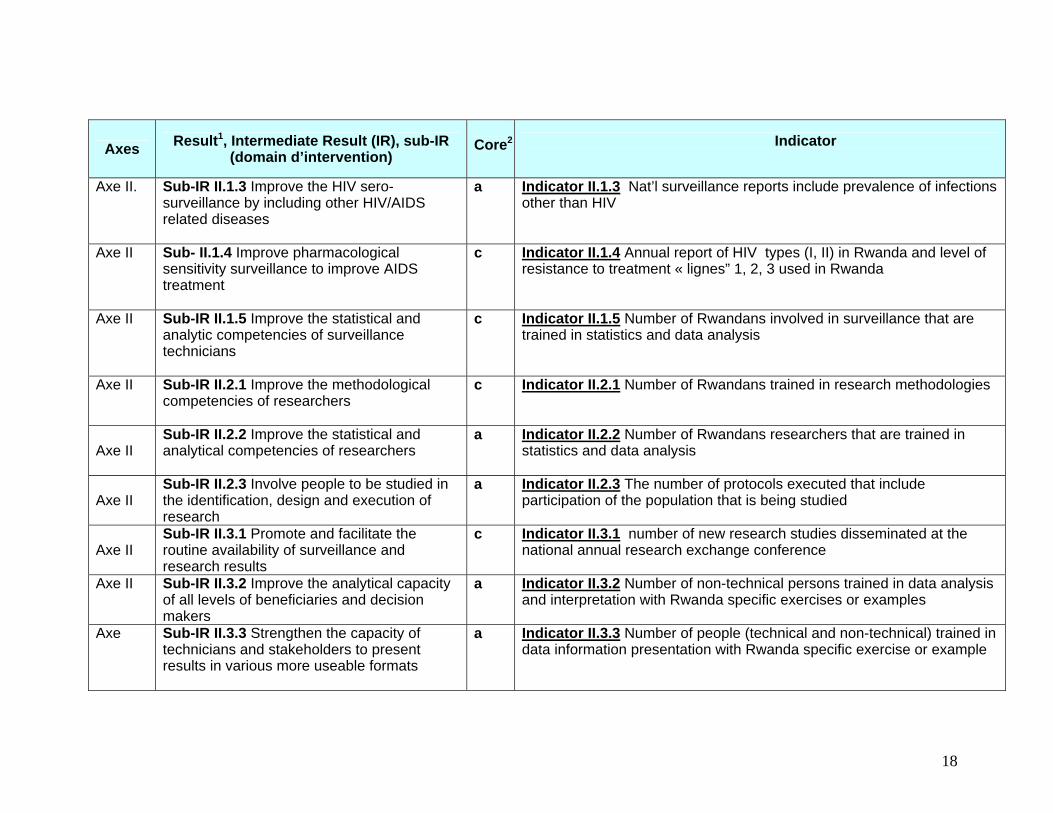
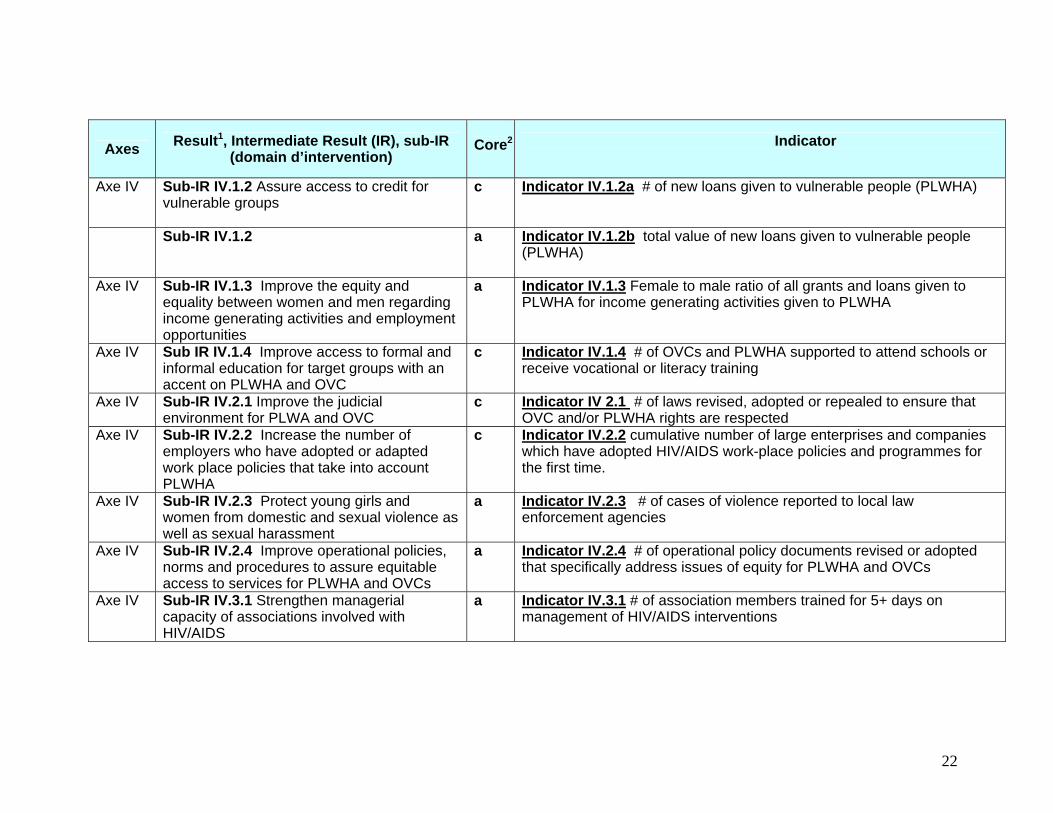
Table 3: Indicators for Monitoring and Evaluation of national response to HIV and AIDS
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Assessing Impact Axe
I
Result: Reinforce measures of preventing HIV/ AIDS transmission
Indicator 1: Change in prevalence of HIV/AIDS in people aged 15-24 years (this is best proxy for change in incidence of HIV/AID for people 15-49)
Assessing Outcomes Axe I IR I.1; Change high risk sexual behavior (in
the population) c Indicator I.1a Change in percentage 15-24 year-olds reporting condom
use last time they had sex with non-marital non-cohabitating partner (this is measure of protected sex)
Axe I IR I.1 a Indicator I.1b Change in percentage 15-24 year-olds reporting sex with non-marital, non-cohabitating partner last 12 months (this is measure of fidelity)
Axe I IR I.2 Change behavior of health personnel to reduce transmission of HIV/AIDS, STI,OI and TB
c Indicator I.2. percent of facilities where team is practicing safe injections
Axe I IR I.3 Reduce the transmission of HIV through medical prophylaxis
c Indicator I.3 Proportion of all HIV+ pregnant women given medical prophylaxis
Axe I IR I.4; Create a culture environment more favorable to preventing HIV & STI transmission
c Indicator I.4; Number of MSC stories that address change in cultural environment more favorable to preventing HIV & STI transmission
Monitoring Programme Outputs Axe I Sub-IR I.1.1 Promote EABC (through IEC for
behavior change) c Indicator I.1.1 Number of new messages that promote EABC
Axe I Sub-IR I.1.2 Increase access to and use of condoms
c Indicator I.1.2a Number of condoms sold or distributed to end users
1 Result is IMPACT level; Intermediate Result = outcome level and Sub-IR = output level 2 Core legend: c=indicator is included as top priority; a=additional indicator as per Axes

16
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe 1 a Indicator I.1.2b Number of social marketing distribution points for condoms.
Axe I Sub-IR I.1.3 Educate youth on sexual responsibility
c Indicator I.1.3; number schools that receive sex education and/or life-skills curriculum AND teachers are trained in its use
Axe I Sub-IR I.1.4 Increase the number of people in the population that know their HIV/ serological status (Voluntary Counseling & Testing)
c Indicator I.1.4 # of persons tested who come back to VCT centers for results
Axe I Sub-IR I.1.5 Increase the proportion of the population that knows the causes, symptoms and consequences of STI, OIs and TB
c Indicator I.1.5 Number of new messages targeting an increase in knowledge of symptoms of STI, OIs and TB.
Axe I Sub-IR I.2.1 Adopt universal precautions in health care-related establishments
c Indicator I.2.1 number of health care personnel who are trained in Universal Precautions (UP)
Axe I Sub-IR I.2.2 Adopt provider-initiated diagnosis of STIs, OIs and TB
c Indicator I.2.2 # of persons who receive treatment for STI
Axe 1 Sub-IR I.2.3 Adopt blood safety measures a Indicator I.2.3 % transfused blood units which were screened in last 12 months
Axe 1 Sub-IR I.3.1 Motivate more pregnant women and their partners to use PMTCT services
a Indicator I.3.1 # of pregnant women who use PMTCT services
Axe I Sub-IR 1.3.2 Increase access to high quality PMTCT services
a Indicator I.3.2 Number of PMTCT sites using national protocol
Axe I Sub-IR I.3.3 Assure Post Exposure Prophylaxis (PEP) for health care personnel
a Indicator I.3.3 Number of public health facilities (FOSA) which have PEP kits available
Axe I Sub-IR I.3.4 Assure PEP for rape victims a Indicator I.3.4 Percentage of providers trained in identification, care and treatment of rape victims

17
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe I Sub-IR I.4.1 Promote (the retention of) Rwandan cultural practices that contribute to preventing HIV and STI transmission
c Indicator I.4.1 Number of new messages targeting retention of Rwanda cultural practice that contribute to preventing HIV, STI transmission
I.4.2a Sub-IR I.4.2 Promote abandoning Rwandan cultural practices that contribute to the transmission of HIV and other STIs
a Indicator I.4.2 Number of new messages targeting abandoning cultural practices that contribute to the transmission of HIV and other STIs
Assessing Impact
Axe II
Result II: National response to HIV/AIDS adapted to Rwanda’s conditions and surveillance/research results
Indicator II; Number of strategic planning/policy documents that have references or citations of Rwanda-specific surveillance or research documents.
Assessing Outcomes Axe II IR II.1 Increase the usefulness of
surveillance results with respect to the national response to HIV/AIDS
c Indicator II.1 Number of articles submitted with a Rwandan among 1st 3 authors to peer-review journals using HIV/AIDS related surveillance and/or research data results.
Axe II IR II.2 Increase the usefulness of research results, studies and evaluations
c Indicator II.2 Number of documents which reference Rwanda-specific research or surveillance.
Axe II IR II.3 Improve ability of stakeholders to interpret and use surveillances and research results
c Indicator II.3; Number of MSC stories that address stakeholder ability to interpret and use surveillance and research results
Monitoring Programme Outputs Axe II Sub-IR II.1.1 Improve national systems for
case notification of morbidity and mortality related to AIDS
a Indicator II.1.1a Percentage of all AIDS-related deaths that are reported through national health information system
Axe II Sub-IR II.1.1 a Indicator II.1.1b Number of medical and non-medical people trained to accurately determine causes of deaths
Axe II Sub-IR II.1.2 Establish a sustainable behavioral surveillance system
c Indicator II.1.2 annual report on behavioral change using National BSS and other behavioral studies is regularly disseminated
18
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe II. Sub-IR II.1.3 Improve the HIV sero-surveillance by including other HIV/AIDS related diseases
a Indicator II.1.3 Nat’l surveillance reports include prevalence of infections other than HIV
Axe II Sub- II.1.4 Improve pharmacological sensitivity surveillance to improve AIDS treatment
c Indicator II.1.4 Annual report of HIV types (I, II) in Rwanda and level of resistance to treatment « lignes” 1, 2, 3 used in Rwanda
Axe II Sub-IR II.1.5 Improve the statistical and analytic competencies of surveillance technicians
c Indicator II.1.5 Number of Rwandans involved in surveillance that are trained in statistics and data analysis
Axe II Sub-IR II.2.1 Improve the methodological competencies of researchers
c Indicator II.2.1 Number of Rwandans trained in research methodologies
Axe II
Sub-IR II.2.2 Improve the statistical and analytical competencies of researchers
a Indicator II.2.2 Number of Rwandans researchers that are trained in statistics and data analysis
Axe II
Sub-IR II.2.3 Involve people to be studied in the identification, design and execution of research
a Indicator II.2.3 The number of protocols executed that include participation of the population that is being studied
Axe II
Sub-IR II.3.1 Promote and facilitate the routine availability of surveillance and research results
c Indicator II.3.1 number of new research studies disseminated at the national annual research exchange conference
Axe II Sub-IR II.3.2 Improve the analytical capacity of all levels of beneficiaries and decision makers
a Indicator II.3.2 Number of non-technical persons trained in data analysis and interpretation with Rwanda specific exercises or examples
Axe
Sub-IR II.3.3 Strengthen the capacity of technicians and stakeholders to present results in various more useable formats
a Indicator II.3.3 Number of people (technical and non-technical) trained in data information presentation with Rwanda specific exercise or example

19
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Assessing Impact
Axe III
Result III: Improve HIV/AIDS treatment, care and support for persons infected and affected by HIV and AIDS
Indicator III Percentage of persons on ART that are alive 12 months after starting treatment
Assessing Outcomes Axe III IR III.1 Increase access to high quality care
and treatment at health facilities c Indicator III.1 Percent of male and females with advanced HIV/AIDS
infection receiving ARV combination therapy
Axe III IR III.2 Increase access to high quality the community- based care and treatment
c Indicator III.2 Percent of eligible households that receive Rwanda’s minimum package (or more) of community-based services in their home
Axe III IR III.3 Assure that HIV/AIDS related care and treatment is sustainable
c Indicator III.3 Number of objectives in the national sustainability plan that are reached
Monitoring Programme Outputs Axe III Sub-IR III.1.1 Assure equitable coverage of
ART services with accent on pediatric care c Indicator III.1.1 % of health care and other facilities that are treating
HIV+ infants and adults according to national norms and procedures
Axe III Sub-IR III.1.2 Improve treatment of OIs according to national norms and procedures
c Indicator III.1.2 % of all service providers trained in diagnosis and treatment of OI according to national guidelines
Axe III
Sub IR III.1.3 Reduce the real cost of accessing HIV/AIDS related care and treatment
c Indicator III.1.3 % of people that are TB+ who receive TB therapy
Axe III
Sub IR III.1.4 Promote the approach “Provider Initiated Diagnosis” (PID)
a Indicator III.1.4 % of all service providers trained in diagnosis and treatment of PID according to national guidelines
Axe III
Sub IR III.1.5 Improve the collaboration and the service referrals between health care providers and community agents
a Indicator III.1.5 Number of joint sessions/meetings between medical corps and community health care providers

20
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe III
Sub-IR III.1.6 Improve therapeutic nutritional support for people on ART
c Indicator III.1.6 # of FOSA with capacity (trained personnel and equipment) to provide nutrition therapy as part of in-patient support to HIV/AIDS patients
Axe III Sub-IR III.1.7 Integrate care and treatment of OIs among other illnesses supported through health mutuals
a Indicator III.1.7 % of health insurance providers (mutuelles de sante) that have included OI in the list of illness covered
Axe III Sub-IR III.1.8 Strengthen health care providers’ capacity to deliver the highest quality care.
a Indicator III.1.8 % of all employees working at FOSA trained in quality assurance
Axe III Sub-IR III.2.1 Assure equitable coverage of community- based care and treatment services
a Indicator III.2.1 percent of administrative sectors in which home-based care is provided
Axe III
Sub-IR III.2.2 Improve the community-based care and treatment of people living with HIV/AIDS (medical, psychosocial and spiritual)
c Indicator III.2.2 # of HIV+ people assisted in their homes for ART adherence
Axe III Sub-IR III.2.3 Strengthen the technical capacity of people and organizations providing community-based care and support
c Indicator III.2.3 # of people trained in techniques for HIV/AIDS home based care.
Axe III Sub-IR III 2.4 Integrate home-based care and treatment for PLWHA within community-based health services
c Indicator III.2.4 # homes visited regularly by trained MOH Program d’Animateur de Sante (PAS) agents for HIV/AIDS-related care .
Axe III Sub-IR III.2.5 Develop and standardize out-patient and mobile treatment services
a Indicator III.2.5 # of rural administrative sectors visited by mobile treatment units that adhere to national standards and protocols
Axe III Sub-III.2.6 Improve the nutritional status of people infected and affected by HIV/AIDS
c Indicator III.2.6 # of homes of PLWHA that are provided with nutritional and/or food security support
Axe III Sub-IR III 3.1 Improve decentralized HIV/AIDS related procurement, management and distribution systems (equipment, regents, consumable, medicine etc,)
a
Indicator III.3.1 # of FOSA that report no stock-outs for ARV or AZT or IO

21
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe III Sub-IR III.3.2 Increase Rwandan human resources needed for HIV/AIDS-related care and treatment
a Indicator III.3.2 # of health care providers at FOSA qualified to provide AIDS, OI or STI treatment
Axe III Sub-IR III.3.3 Establish system to supply communities with required materials
a Indicator III.3.3 # of administrative sectors reporting no stock-outs of home-based care kits.
Axe III Sub-IR III.3.4 Execute a national plan to assure that the expanded quality global care and treatment is sustainable.
a Indicator III.3.4 % of activities in the annual operation plan of the national sustainability plan that are completed.
Assessing Impact
Axe IV
Result IV: Mitigate the socio-economic impact of HIV and AIDS
Indicator: Change in GDP
Assessing Outcomes Axe IV IR IV.1 Improve the socio-economic
conditions in Rwanda (and assure vulnerable groups benefit as much as others)
c
Indicator IV.1a Per capita income
Axe IV IR IV.2 Defend and promote human rights c Indicator IV.2 number of cases that come to court claiming violation of human rights with respect to HIV/AIDS have been used.
Axe IV IR IV.3 Strengthen decision making capacities of associations involved in HIV/AIDS notably through the concept of GIPA (Greater Involvement of People living with HIV/AIDS)
c . Indicator IV.3 Number of organizations including PLWHA in their policy/planning development and program assessment.
Monitoring Programme Outputs Axe IV Sub-IR IV.1.1 Create employment
opportunities in particular for vulnerable groups
c
Indicator IV.1.1 % of vulnerable people (members of associations of PLWHA ) who are unemployed
22
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe IV Sub-IR IV.1.2 Assure access to credit for vulnerable groups
c Indicator IV.1.2a # of new loans given to vulnerable people (PLWHA)
Sub-IR IV.1.2 a Indicator IV.1.2b total value of new loans given to vulnerable people (PLWHA)
Axe IV Sub-IR IV.1.3 Improve the equity and equality between women and men regarding income generating activities and employment opportunities
a Indicator IV.1.3 Female to male ratio of all grants and loans given to PLWHA for income generating activities given to PLWHA
Axe IV Sub IR IV.1.4 Improve access to formal and informal education for target groups with an accent on PLWHA and OVC
c Indicator IV.1.4 # of OVCs and PLWHA supported to attend schools or receive vocational or literacy training
Axe IV Sub-IR IV.2.1 Improve the judicial environment for PLWA and OVC
c Indicator IV 2.1 # of laws revised, adopted or repealed to ensure that OVC and/or PLWHA rights are respected
Axe IV Sub-IR IV.2.2 Increase the number of employers who have adopted or adapted work place policies that take into account PLWHA
c Indicator IV.2.2 cumulative number of large enterprises and companies which have adopted HIV/AIDS work-place policies and programmes for the first time.
Axe IV Sub-IR IV.2.3 Protect young girls and women from domestic and sexual violence as well as sexual harassment
a Indicator IV.2.3 # of cases of violence reported to local law enforcement agencies
Axe IV Sub-IR IV.2.4 Improve operational policies, norms and procedures to assure equitable access to services for PLWHA and OVCs
a Indicator IV.2.4 # of operational policy documents revised or adopted that specifically address issues of equity for PLWHA and OVCs
Axe IV Sub-IR IV.3.1 Strengthen managerial capacity of associations involved with HIV/AIDS
a Indicator IV.3.1 # of association members trained for 5+ days on management of HIV/AIDS interventions

23
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe IV Sub-IR IV.3.2 Balance of the composition of HIV/AIDS related associations (increase proportion of male, middle class & HIV – members).
c Indicator IV.3.2a. # of association members trained for 5+ days on management of HIV/AIDS interventions
Sub-IR IV.3.2 a Indicator IV.3.2b. % of members of associations of PLWHA not HIV+ Axe IV Sub-IR IV.3.3 Increase involvement of
PLWHA in the planning, execution and review of programmes
a Indicator IV.3.3 # of associations of PLWHA involved in the planning, implementation, and review of programmes /projects
Assessing Impact
Axe V
Result V: Coordinate the multi-sectoral response for increased cost effectiveness
Indicator V The ratio of the value of government expenditures on HIV/AIDS to value of external assistance for HIV/AIDS
Axe V IR V.1 Improve the capacities of national HIV/AIDS coordination structures
c Indicator V.1; Number of MSC stories that address capacity of national HIV/AIDS coordination structures
Axe V IR V.2 Assure that HIV/AIDS strategies within national sector plans are implemented
c Indicator V.2 Number of HIV/AIDS-related objectives in national sector plans that have been achieved..
Axe V IR V.3 Increase HIV/AIDS related regional initiatives that are jointly executed
c Indicator V.3 Number of regional interventions that are jointly executed
Axe V IR V.4 Assure that intervention agencies benefit from national planning and monitoring as much as the coordination agencies
c Indicator V.4; Number of MSC stories that address intervention agencies perception of usefulness/benefits of contributing to national planning, M&E
Axe V IR V.5 Jointly evaluate the multi-sector response to HIV and AIDS
c Indicator V.5 mid-term review of HIV/AIDS national response (2007) and end-of period evaluation (2009/10) are jointly executed with representation from all stakeholders.
24
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
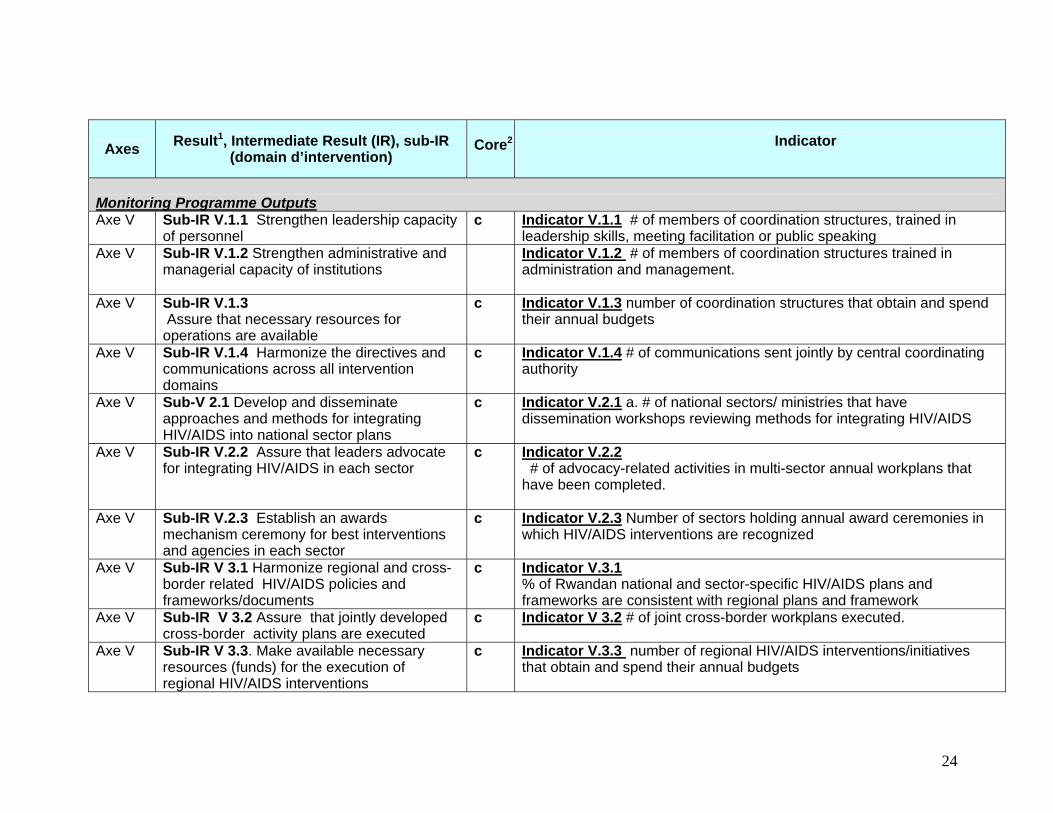
Monitoring Programme Outputs Axe V Sub-IR V.1.1 Strengthen leadership capacity
of personnel c Indicator V.1.1 # of members of coordination structures, trained in
leadership skills, meeting facilitation or public speaking Axe V Sub-IR V.1.2 Strengthen administrative and
managerial capacity of institutions Indicator V.1.2 # of members of coordination structures trained in
administration and management.
Axe V Sub-IR V.1.3 Assure that necessary resources for operations are available
c Indicator V.1.3 number of coordination structures that obtain and spend their annual budgets
Axe V Sub-IR V.1.4 Harmonize the directives and communications across all intervention domains
c Indicator V.1.4 # of communications sent jointly by central coordinating authority
Axe V Sub-V 2.1 Develop and disseminate approaches and methods for integrating HIV/AIDS into national sector plans
c Indicator V.2.1 a. # of national sectors/ ministries that have dissemination workshops reviewing methods for integrating HIV/AIDS
Axe V Sub-IR V.2.2 Assure that leaders advocate for integrating HIV/AIDS in each sector
c Indicator V.2.2 # of advocacy-related activities in multi-sector annual workplans that have been completed.
Axe V Sub-IR V.2.3 Establish an awards mechanism ceremony for best interventions and agencies in each sector
c Indicator V.2.3 Number of sectors holding annual award ceremonies in which HIV/AIDS interventions are recognized
Axe V Sub-IR V 3.1 Harmonize regional and cross-border related HIV/AIDS policies and frameworks/documents
c Indicator V.3.1 % of Rwandan national and sector-specific HIV/AIDS plans and frameworks are consistent with regional plans and framework
Axe V Sub-IR V 3.2 Assure that jointly developed cross-border activity plans are executed
c Indicator V 3.2 # of joint cross-border workplans executed.
Axe V Sub-IR V 3.3. Make available necessary resources (funds) for the execution of regional HIV/AIDS interventions
c Indicator V.3.3 number of regional HIV/AIDS interventions/initiatives that obtain and spend their annual budgets

25
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe V Sub-IR V 4.1 Simplify and harmonize planning and monitoring tools
c Indicator V.4.1 # variables collected by national coordination structures and large bi/multi-lateral projects
Axe V Sub-IR V 4.2 The level of detail needed for national planning and workplan monitoring is appropriate for national level reporting (in decentralized context)
c Indicator V.4.2 number of activities identified in workplans submitted to CNLS
Axe V Sub-IR V 4.3 Strengthen capacity to facilitate planning and monitoring workshops and meetings
c Indicators V.4.3 # coordination structure personnel trained in facilitating planning workshops/meetings, and in reporting
Axe V Sub-IR V.4.4 Assure that the national HIV/AIDS strategic framework and M&E plan are used by all agencies for activity planning & monitoring
c
Indicators V.4.4 % of activities identified in work plans submitted to CNLS that correctly identify the Axe, IR and sub-IR as well as the indicator(s) to which they contribute
Axe V Sub-IR V.5.1 Harmonize and operationalize national indicators and M&E and planning tools
c Indicator Sub-IR V.5.1.a Indicator values submitted by intervention agencies are comparable.
Sub-IR V.5.1 c Indicator Sub-IR V.5.1.b Same M&E and planning formats are used at district level by interveners
Axe V Sub-IR V.5.2 Strengthen capacity at all levels to evaluate the national response
a Indicator V.5.2 # of people trained in data use/interpretation using Rwanda indicators & data
Axe V Sub-IR V.5.3 Jointly develop and validate information products from national evaluation
a Indicator V.5.2 # of organizations regularly participating in TWG to develop/modify/validate national M&E products
Axe V Sub-IR V. 5.4 Assure that national M&E products are available and useable (to/by information providers and users).
c Indicator V.5.4 # of M&E products that stakeholders have obtained/accessed and find useable

26
Axes Result1, Intermediate Result (IR), sub-IR (domain d’intervention)
Core2
Indicator
Axe V Sub-IR V.5.5. Coordinate research and training.
c Indicator V.5.5a. existence and use of national long-term or annual HIV/AIDS-related research plans
Axe V Sub-IR V.5.5. a Indicator V.5.5b existence and use of a national training database
26
3.0 DATA COLLECTION STRATEGY FOR M&E 3.1 Coordination of M&E The CNLS will work closely with various stakeholders at both national and district levels, in both public and private sectors, to coordinate collection of data that will be used to generate information products. The CNLS will facilitate and coordinate the standardization of instruments and methodologies for data collection. Besides, it will establish data quality assessment protocols in a participatory and consultative manner with all the stakeholders. The 62 national and 23 district indicators that have already been agreed upon (for a list of indicators and their definitions refer to Annex 1) will form the basis for data collection for assessing program outputs, outcomes and impact of HIV/AIDS interventions. HIV/AIDS programme/project interventions, as described in the National Strategic Framework for HIV/AIDS Control / Results Framework 2005-2009, will provide programme monitoring data at the district and community levels. The data collection strategy for the routine data at this level will entail CBOs and NGOs compiling data from their interventions in various communities and preparing monthly and quarterly progress reports. These information products will then be submitted to the CDLS, and copied to their national umbrella organizations. The modalities and the actual process of doing so will be agreed upon and a district M&E operational plan developed in a participatory and inclusive manner. The CNLS will supervise this exercise and make sure that district-level operational manual/guideline is developed and disseminated widely to all stakeholders. To ensure accurate, comprehensive and timely reporting, the CNLS will coordinate sustained capacity building and training programme in M&E at all levels, especially in the areas of data collection, analysis, interpretation, production of information products and use of the data for decision making and programming. Strengthening M&E activities at the CDLS will be a key priority. 3.2 Data Sources: In order for the national M&E system to function, core data sources of each of the indicators have been identified and agreed upon (for details refer to Annex 1). There two categories of data sources: those for output (routine) indicators; and those for outcome/impact indicators. Some of the data sources include the following:

27
i. Data source for routine (output) indicators: - These are routine reports from project / program implementers at various levels in both public and private sectors. They include the following:
- Program activity (routine) data from CBOs and NGOs at district levels, umbrella organizations and the private sector: e.g. District IEC/BCC report, VCT/PMTCT/ARV reports, and
- District and national health facility coverage report - Service coverage reports - DHT supervision reports - Data from Sector monitoring system, e.g. HIS/SIS - Data from national blood transfusion center - Social agency marketing reports - CNLS HIV/AIDS financial management report - TRAC research reports - MoH reports - CNLS Database - SIS database/reports - Desk review reports
ii. Data sources for Impact/Outcome assessment from the following:
- Sentinel surveillance report - Second generation surveillance - Routine population based national surveys like DHS, population
census - Special studies, e.g. Clinical studies, HIV/AIDS operational
research, impact assessment in key sectors and capacity assessment).
- Health Facility Surveys (HFS) - VCT site reports - PMTC site report - ART site reports
3.3 Information Products at National Level For effective monitoring and evaluation of national response to HIV/AIDS, the CLNS will develop information products, from the data sources mentioned above, that will be disseminated to stakeholders at both national and district levels Besides, some of the information products, for example UNGASS Report, are for meeting the international requirements. The information products that will be retrieved by the CNLS include the following: Quarterly Service Coverage Report: This report provides information
on coverage statistics per HIV programme area, and is essentially based on the main interventions as envisaged in the Multi-sectoral National Plan. It therefore

28
depends largely on the information that the implementing agencies submit quarterly to the district AIDS Control Commission (CDLS), and subsequent analysis report that the monitoring and evaluation coordinator at the district submits to the CNLS. The report from the implementing agencies to the district and from the district level to the CNLS ought to conform to the terms of minimum reporting standards, as well as CNLS reporting format. CNLS Bi-annual Report: This report provides the semiannual activities
on the national response to HIV/AIDS, and is based on the quarterly reports which have been submitted by the CDLS and national umbrella organizations (through PMU). The content of the report include issues to do with coordination, implementation (results being achieved), M&E, emerging issues including challenges and any special study report which has been submitted. National HIV/AIDS M&E Annual report: This report provides a
comprehensive overview of the national response to HIV in a year period. The report is done by reporting on selected list of national level indicators as contained in the national HIV/AIDS M&E Plan. It also provides key observations and guidance for future implementation. The content of this report includes a summary of quarterly reports on the community non-medical programmes indicators which the district submits to the CNLS. The report on the medical programme indicators is provided by TRAC, the National Laboratory, and the Health Information system (HIS/SIS). All the relevant indicators from survey and research findings conducted in the course of the year are also reported. The National HIV/AIDS M&E annual report is finalised in February and its national dissemination is done in March in an organised workshop, which brings together a wide range of stakeholders and partners in the fight against HIV/AIDS. Annual PRSP progress report on HIV/AIDS. The CNLS will ensure
that every year that the data collection and analysis for the HIV/AIDS annual report on review of poverty reduction strategies are reported to the Ministry of Finance and Economic Planning (MINECOFIN) for eventual incorporation in the overall national annual PRSP report. CNLS HIV/AIDS Database: - The National HIV/AIDS Database will be
updated from time to time and equipped with necessary equipment and programmes for efficiency and effectiveness. The database will be linked to other HMIS and micro M&E sub-systems in other government ministries and institutions. From this database, the CNLS will produce the necessary periodic updates on topical issues on HIV/AIDS in Rwanda. Ad hoc reports: In addition to the specific information products listed
above, some stakeholders/partners might have specific information needs at some stage. Although the CNLS encourages the use of existing information

29
products, it opts to assist if there are any specific and ad hoc information needs that are not covered in one of the above information products. Such a request is made in writing to the CNLS. If possible, the request will be accommodated within the budget limitations of the Planning, Coordination, M&E Unit. If it is not possible, the person/institution will be informed of the cost implications. Annual UNGASS report: Rwanda is a signatory to the 2001 Declaration
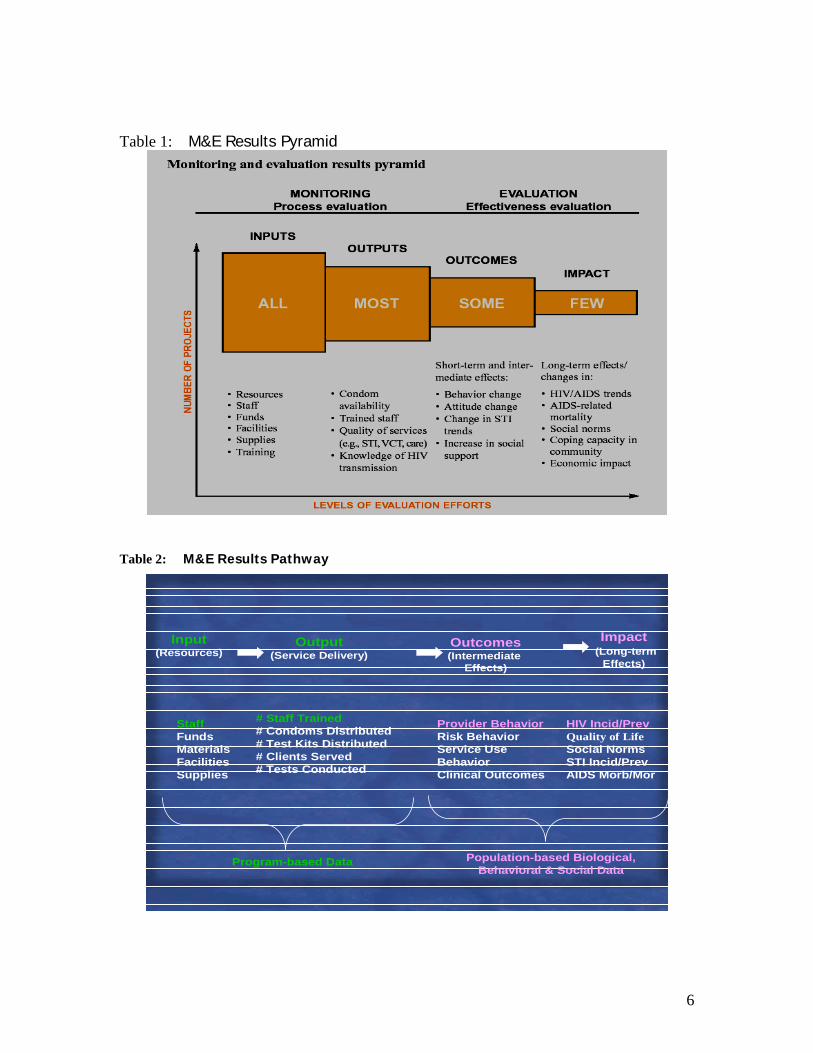
of Commitment on HIV/AIDS at the United Nations Special Session on HIV/AIDS (UNGASS). Part of this Declaration of Commitment includes a set of indicators that the Government of Rwanda has agreed to report on to UNAIDS on a periodic basis. The CNLS collaborates with the UNAIDS to produce this report before February of every year. 3.4 Reporting Levels and Data flow This section presents the reporting linkages and data flow in general - from programme implementers at the district level to CDLS, CDLS to CNLS; and from health facilities through TRAC to CNLS (Diagrams 2 and 3). Specific data flow for each data source will be described in detail in the M&E Implementation Plan Part II. 3.4.1 Reporting to CNLS An effective national M&E system requires that data flow structures and reporting mechanisms are clearly defined to avoid the problem of double counting. Diagram 2 is a pictorial presentation of data flow and the information linkages from the district level (CDLS & health facilities) to CNLS.

30
Diagram 2: Comprehensive HIV Monitoring and Evaluation Data / Information Flow
Key: Flow 1 = Red arrows: District based NGOs, CBOs, private sector, and Government district level structures.
CNLS M&E Unit: DataBase Ressource Centre.
Government / Public Sector
Civil Society The Private Sector
GoR Ministries MOH
District Gov. Depts.
Health Facilities
Research Work
TRAC
RIs & Universities
CDLS: District M&E Coordinator
Districts NGOS
Districts CBOs
OtherAssociations
National NGOs
National Umbrella Organization
Other National Associations
Structures at National Level ,e.g. APELAS
Structures at District Level
Proj.Man. Unit.
Dissemination to StakeholdersDisseminate to Stakeholders
1
2
3
4
5
6
National Level
District Level

31
Reporting directly to CDLS
Flow 2: = Double black arrows: CDLS reports to CNLS and the later feeds back
to the former. Flow 3: = Green arrows: Health facilities to TRAC and MoH. Flow 4: = Green arrows – national level: Public sector: Government Ministries
and public institutions reporting to CNLS Flow 5: = Sky blue arrows: National organizations/umbrellas reporting both
financial and national coordination activities to PMU/development partners (sources of funding), who aggregate the data and report to CNLS M&E unit.
Flow 6: = Dotted arrows: Implementers at district level report to national umbrella organizations just for information. Organizations at national level not required to report this data to PMU/CNLS.
3.5.2 Reporting to the CDLS Data collection and reporting system at the district level is depicted in Diagram 3 below:
• All the HIV/AIDS program implementers will provide regular quarterly reports to the CDLS using the CNLS data collection format.
• The CBOs and NGOs will compile monthly and quarterly progress reports and submit them to CDLS.
• Clinical data from health facilities will be sent to TRAC.
• To avoid double counting there will be one way reporting from implementing agencies to District and from District to CNLS.

32
Diagram 3: Data Flow from CDLS to CNLS
The implementers will, as usual, be reporting to their funding agencies for accountability. The funding agencies will not be required to report on this data to the CNLS:
• Data collection forms will be submitted to the CDLS M&E Agents, who will quality control these forms and aggregate before sending them to the CNLS for data capture.
• The CNLS M&E unit will ensure that the data from each district are
captured onto a central M&E database To ensure effective, timely and non-duplication of data/information reported, all the organisations and agencies implementing the HIV/AIDS community non-medical interventions will report their activities on a quarterly basis to the District AIDS Control Commission, CDLS.
3.5.3 Reporting of Health related Indicators: e.g. HIS/SIS to CNLS, TRAC to CNLS The TRAC is in charge of coordinating and collecting and analyzing most of health (clinical) related data. The clinical data will be collected at the health
NationalCommunity District
CDLS
HF
CNLS
FBO / Work Place
NGOs
CBOs
Donors : UN Agencies
Umbrella Org.
CNLS M & E Unit
TRACNET+ HC Ref.Hosp & Lab

33
facilities in the country at all levels, using standardized and agreed upon tools. Such data will be submitted to TRAC. The TRAC will analyze and aggregate the data and produce information product and submit them to the Ministry of Health (MoH), with a copy to the CNLS. The National Referral Laboratory and the National Blood Transfusion Centre Health will collect and analyze data and submit the same MoH - Information system (HIS/SIS). This also applies to any research institution/organization undertaking clinical research in the country.
3.5.4 Reporting from Other Government ministries and institutions The Government Ministries at national level and other public institutions will monitor HIV/AIDS activities in their specific structures, produce information products and submit the same to the CNLS in agreed format. The Ministries headquarters will not submit information on activities implemented by government departments at the district levels. To avoid the problem of double counting, the government department at district levels will submit HIV/AIDS related data/information directly to the CDLS, with a copy to their headquarters at the national level. The CDLS will then submit such activities to the CNLS.
3.5.5 Reporting from the Civil Society, Umbrella Organizations and the Private sector
The National civil society and umbrella organizations operating in the country will submit both financial and national programme activities, like coordination, capacity building, advocacy and mobilization, to HIV/AIDS Programme Management Unit (PMU) and relevant donors using an agreed format. To avoid the problem of double counting, the NGOs, CBOs and other associations implementing the HIV/AIDS activities at the district level will send monitoring activity data directly to the CDLS, with a copy going to their parent organizations. The CDLS will send such data to the CNLS. Umbrella organizations and other associations at national level are not required to submit data on the district based interventions by the organizations or associations they fund.
31
4.0 THE ROLE OF STAKEHOLDERS IN HIV/AIDS M&E & COORDINATION MECHANISMS 4.1 The Role of CNLS /M&E Unit in Monitoring national response As mentioned earlier, the National AIDS Control Commission, CNLS – one national authority-, has the mandate of coordinating monitoring and evaluation of the national response to HIV/AIDS in Rwanda. In a nut-shell, the role of the CNLS in M&E includes the following:
• Coordination, supervision and provision of technical assistance and guidance to monitoring and evaluating national response and tracking progress made in the program activities at all levels;
• Coordination and provision of a national coherent plan for monitoring
progress and evaluating outcomes of a comprehensive HIV/AIDS programme. CNLS is responsible for defining strategic objectives and targets; guiding and supervising systematic data collection, processing and analysis of data at various levels; and providing the platform for partnership, networking and collaboration between the national level and local level stakeholders in monitoring and evaluating;
• Creation of a multi-sectoral functional HIV M&E system, with a database,
that links with other HIS systems, research organizations and other micro/M&E units in other government ministries, civil society organizations and the private sector. The CNLS has developed a simplified, but complete reporting format for use by all the stakeholders/partners;
• Supervision and data auditing: The responsibility of supervision as a
component of coordination remains the key role of the CNLS secretariat. The commission will coordinate the standardization of M&E methodologies and tools across multiple actors at various programme levels so that meaningful comparisons could be made over time. The supervision mainly focuses to the reporting agencies to ensure that the data provided is audited for verification and credibility purposes, but also providing technical assistance in data collection, analysis and reporting. The commission also facilitates the standardization of M&E methodologies and tools across multiple actors at various programme levels so that meaningful comparisons could be made over time;
• Development of standardized tools and methodology for collecting non-
clinical data and information production and reporting is an important activity in this exercise. Besides, the CNLS has to establish, in a
32
participatory manner, data quality assessment (DQA) protocol(s) that will coordinate and guide data collection, analysis and processing for quality assurance purposes;
• Generation of national information products, as agreed and demanded by
both the national and international stakeholders, and disseminating these products in a user friendly and in a timely manner. Some of these products include National HIV/AIDS Annual Report, Rwanda Annual UNGASS Report. The CNLS will ensure and facilitate the annual national disseminations and review activities; and
• Coordinate and support all capacity building and training in M&E at both national and district levels. This is to ensure that the M&E systems, at the district level in particular, are functioning and have necessary resources. The CNLS will organize periodic supervision visits and reviews of district based M&E systems and organize for capacity building activities accordingly.
Although the CNLS Executive Secretary is the overall overseer of these roles, the Directorate of Planning, M&E, and Coordination and M&E Focal Person and his/her term are directly responsible in coordinating these M&E activities and making sure that they are implemented efficiently and effectively, within an agreed timeframe.

33
4.2 The Roles and Responsibilities of District M&E Focal Persons Given the decentralisation of the HIV/AIDS response in Rwanda, data collection on the HIV/AIDS activities will be done by the districts. The CDLS will mainly monitor programmme activity outputs level indicators, and will be in charge of making sure that data is submitted to CNLS in an agreed format and in a timely manner. Specifically, CDLS are expected to: - Register and submit names of NGOs and CBOs involved in the HIV/AIDS
activities in the District to the CNLS;
- Coordination and supervision of M&E at the district level;
- Facilitate and demand for the filled standardized forms for data collection from the NGOS/CBOs;
- Submit the data forms to the CNLS in an agreed format in a timely manner;
- Sensitize and advocate for the use of information products for programming activities; and
- Disseminate and sensitize partners at the District/community levels on the pandemic using information from the CNLS.
Therefore, a district-level coordination and programme monitoring system will be developed. This will be the mechanism through which the CDLSs obtain standard work plan data and standard data on the implementation of activities in those work plans on an annual basis. Such a district-level coordination and programme monitoring system is thus part of the government’s national HIV/AIDS M&E plan.
4.3 The Role of Government ministries and other public
institutions/organizations. Specifically, such institutions are expected to: - Mainstream the HIV/AIDS interventions in their core business; - Mobilize resources and coordinate HIV/AIDS activities within their
institutions; - Advocacy and sensitization on HIV/AIDS at workplace; - Facilitate training on the M&E for the staff; - Report on specific indicators for the institution to the CNLS using
standardized reporting format and in a timely manner; and - Participate in annual HIV/AIDS annual reviews.
34
4.4 The Role of other stakeholders. Many stakeholders are involved in fighting the pandemic in one way or the other. Chief among them is: the research organizations e.g. TRAC, Civil society organizations, and Umbrella organizations including PLWA, Faith Based Organizations, the private sector, and the development partners. Their role will include the following: o Civil Society, Umbrella Organizations and The private sector:
- Participate in the M&E Technical Working Group (TWG);
- Ensure that their members are familiar with the National HIV/AIDS Framework/Plan;
- Participate in strengthening their M&E units using the National M&E Framework/plan provided by the CNLS;
- Submit national activities to the PMU and donors;
- Those operating at district level to conduct program activity output monitoring;
- Submit required data to CDLS using a standardized format based on an agreed timelines;
- Sensitization and advocacy for M&E and use of data; and
- Participation in the national M&E dialogue and reviews. o Research Organizations and Universities:
- Participate in the development of the CNLS Research Strategy;
- Conduct high quality research, in a timely manner;
- Disseminate research findings to: the Ministry of Health – Research Unit, the CNLS: the M&E Unit and Research Unit, Program/Project Implementers;
- Use research findings to inform policy and programs; and
- Participation in the national M&E dialogue and reviews. o Development Partners: The development partners play an important part in supporting the national response to HIV/AIDS. They provide financial and TA support to the CNLS and

35
various implementers at the national and district levels. In terms of M&E, they are expected to: - Be part of the HIV/AIDS M&E Technical Working Group;
- Support the strengthening of the national HV/AIDS M&E system;
- Build the culture of M&E among their implementers and make it a mandatory requirement in their MoUs;
- Build consensus on harmonizing information requirements and reporting framework to avoid using different frameworks or reporting system;
- Participation in the national M&E dialogue and reviews.
31
5.0 DISSEMINATION AND USE OF DATA /INFORMATION The reports produced by the CNLS are disseminated twice a year to stakeholders and partners. This M&E cycle is synchronized with the annual planning and programming cycle, thus maximizing the opportunity for the M&E results to be used for decision making. From this perspective, therefore, data and information from the DCLS, umbrella organizations, other public sectors and institutions must also reach the CNLS in time in order for the same to be included in the dissemination process. The dissemination plans will be developed and agreed upon by all stakeholders in the country.
Using the data and information products from various sources and levels, the CNLS will produce the Annual HIV/AIDS M&E Reports, using top priority indicators to show the national response to the pandemic. It will also prepare the annual PRSP progress report on HIV/AIDS and submit it to the Ministry of Finance. The national level M&E results/findings will also be disseminated through annual HIV surveillance reports, HIV/AIDS summary reports, electronic and print media, and through special occasion gatherings like when celebrating the HIV/AIDS day. These reports will also be submitted to the Minister of State for national and regional dissemination. The CNLS will also participate in preparing the Annual UNGASS report.
The CDLS will undertake dissemination of M&E results in their districts to implementers and communities through organized meetings, religious institutions and local leaders meetings.
The dissemination of the M&E results is expected to serve the following purposes:
Provide feedback to various implementers on the efforts being made, progress and the difference being made;
Sharing and using the data and information for better targeting and planning of the HIV/AIDS interventions at the district and community levels in the country;
Increase awareness and public commitment to the national response to HIV/AIDS;
Provide feedback on efforts and resource utilization in the national response to HIV/AIDS and articulate lessons learned, gaps and challenges faced at the district and national levels; and
Enhance networking, harmonization and resource mobilization for national
response to HIV/AIDS.

31
6.0 STRENGTHING OF THE NATIONAL HIV M&E SYSTEM: THE IMPLEMENTATION PLAN 6.1 Harmonization and Implementation of the National HIV M&E System Plan In line with the CNLS mandate to coordinate the national response to HIV/AIDS and having one national M&E System, the execution of the national plan for the M&E system requires commitment and partnership guided by the principles articulated in Section 1.3 of this document. The following will be necessary for the successful execution of the M&E system: Developing and building consensus on a national work plan (operation plan)
for data collection and reporting at the national and district levels;
Coordinating and harmonizing the M&E technical and financial support going to implementers at the district levels. The CNLS should receive and coordinate the distribution of the M&E support coming from different development partners and international NGOS;
Building and strengthening a functional national M&E System, with a
database linked to the HIS and other sub-systems; Establishing and strengthening the M&E units at the CDLS and the umbrella
organizations;
Mounting capacity building / training activities on M&E at the district levels and also targeting umbrella organizations. An M&E Training manual will have to be developed and a training work plan agreed upon by the stakeholders.
The execution of this national plan will require human, financial and physical resources. There is need, therefore, to build consensus on the investment strategy for M&E. From this perspective, any resources from the different development partners and government, for the M&E activities need to be channeled and coordinated by the CNLS. The coordination of the various activities in this plan by the CNLS and the support from the various stakeholders including the development partners will be critical.

32
6.2 Components/Areas of Interventions Based on needs assessment of the existing HIV/AIDS needs assessment at the CNLS and DCLS, the following areas of interventions are key priorities and need strengthening within the strategic plan period. These include the following:
Capacity Development for M&E at the CNLS, CDLS and Umbrella organizations
This area of intervention targets enhancing the knowledge and skills of M&E focal persons at the CNLS, CDLS, the public sector and umbrella organizations. This is to enhance their capacity to effectively coordinate, conduct data collection and analysis, prepare information products and submit them to appropriate levels in a timely manner. Besides, it is to help them make use of data for decision making and programming of the HIV/AIDS activities. The specific activities include the following:
o Sensitization, advocacy and sharing of the national HIV/AIDS M&E documents including the national M&E Plan;
o Facilitation and development of the M&E training program/manual for CBOs, NGOs, the public sector and umbrella organizations;
o Training the M&E focal persons/points at different levels in the new national M&E Implementation Plan (for example in data collection, development and use of information products, and reporting mechanisms;
o Training of the M&E focal points in relevant M&E and data soft-ware and relevant management principles;
o Organizing for dissemination and networking seminars and workshops for the exchange of new ideas in M&E.
Institutional Strengthening
The intervention targets making the M&E systems at the CNLS and CDLS functional and effective. Specific activities include:
o Creation of a functional database at the CNLS and micro databases at the CDLS;
o Providing the CDLS with the necessary M&E ICT equipments/facilities, e.g. computers, soft-ware, lap-tops, telephone and internet facilities;

33
o Linking the CDLS micro databases with the CNLS database;
o Linking the HIV/AIDS M&E with other HIS/SIS systems, TRAC an other public sectors e.g. MINECOFIN, MINEDUC;
o Carrying out supervision and data audit at all levels;
o Establishing a functioning resource center including virtual library;
o Organizing workshops / seminars to establish and enhance the culture of M&E, e.g. targeting advocacy and sensitization.
Strengthening Data Collection, Analysis and Reporting
This component targets making data collection, analysis, and reporting more efficient and timely. Besides, it is to enhance the quality of data and make it available for decision making and programming for the HIV/AIDS activities at all levels. The specific areas of interventions include:
o Develop national HIV M&E operational guide (User’s guide) o Develop the DCLS level M&E annual data collection plan – with
clear activities and timeframe;
o Establishing a baseline for core National HIV/AIDS indicators, where there are not available;
o Developing and building consensus on a standardized, user friendly data collection instrument (s) and reporting formats;
o Launch a data collection exercise at the DCLS, the public sector and the Umbrellas;
o Establish Data Quality Assessment Protocols and coordinating Supervision;
o Creation of functioning data bases at the CDLS and CNLS.
Strengthening coordination of HIV/AIDS Research and Surveys This component aims at enhancing the coordination of the HIV/AIDS research, thus avoiding duplication and making research findings useful and available for decision making and programming. Specific activities include the following:
o Development of national the HIV/AIDS research protocol / norms;
o Finalizing the development of national HIV/AIDS research strategy;
o Enhancing the national steering committee of research by providing them with necessary facilities;

34
o Identifying and coordinating the carrying out of strategic non- medical research in identified sectors;
o Enhancing reporting and dissemination of research results to the CNLS, national and regional forums including publications in international journals.
Coordinating National Consultative Meetings and Reviews of the
National M&E Plan. This component of intervention targets dissemination of information products by the CDLS, the public sector, umbrella organizations and CNLS to appropriate stakeholders and implementers. The dissemination of information products has to be coordinated to reach various stakeholders in time and in an effective manner. Specific activities in this component include the following:
o Organize the annual national stakeholders meeting on the HIV/AIDS response;
o Organize workshops for the dissemination and discussion of results with HIV implementers in sentinel site Districts;
o Organize dissemination workshops in all the districts for sharing good practice and lessons learned in the HIV/AIDS programme activity monitoring and district responses;
o Organizing and supporting AIDS week/day celebrations at the national and district levels.
In the framework in Table 4 below, the interventions, budget and sources of funding are just indicative and they are targeting strengthening the CNLS monitoring and evaluation system only. The development partners interested and willing to fund any of the interventions articulated in the table need to inform the CNLS. It should be noted that the specific operational budget for M&E annual work-plans at decentralized levels will have to be developed and agreed upon.
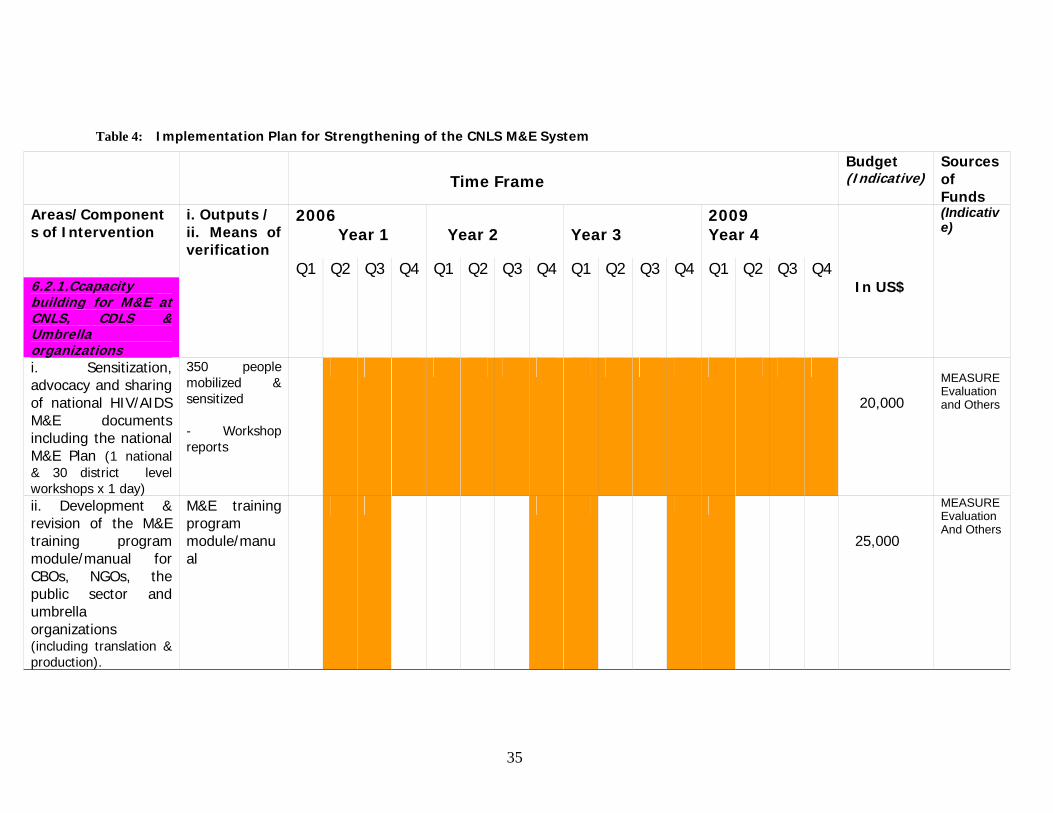
35 35
Table 4: Implementation Plan for Strengthening of the CNLS M&E System
Time Frame
Budget (Indicative)
Sources of Funds
Areas/Components of Intervention
i. Outputs / ii. Means of verification
2006 Year 1
Year 2
Year 3
2009 Year 4
(Indicative)
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 6.2.1.Ccapacity building for M&E at CNLS, CDLS & Umbrella organizations
In US$
i. Sensitization, advocacy and sharing of national HIV/AIDS M&E documents including the national M&E Plan (1 national & 30 district level workshops x 1 day)
350 people mobilized & sensitized - Workshop reports
20,000
MEASURE Evaluation and Others
ii. Development & revision of the M&E training program module/manual for CBOs, NGOs, the public sector and umbrella organizations (including translation & production).
M&E training program module/manual
25,000
MEASURE Evaluation And Others

36 36
iii. Training M&E focal persons/officers in the districts: CDLS, CBOs & NGOs based on the new national M&E Implementation Plan (for example in data collection, development and use of information products, and reporting mechanisms (5 days/district).
70 M&E/data people trained - Workshop reports
100,000
CNLS, MEASURE Evaluation and identified partners
iv. Training of M&E focal persons/officers in relevant M&E and data soft-ware and relevant management principles (5 days incl. trainers)
35 M&E persons trained. - Workshop reports
15,000
CNLS and identified partners
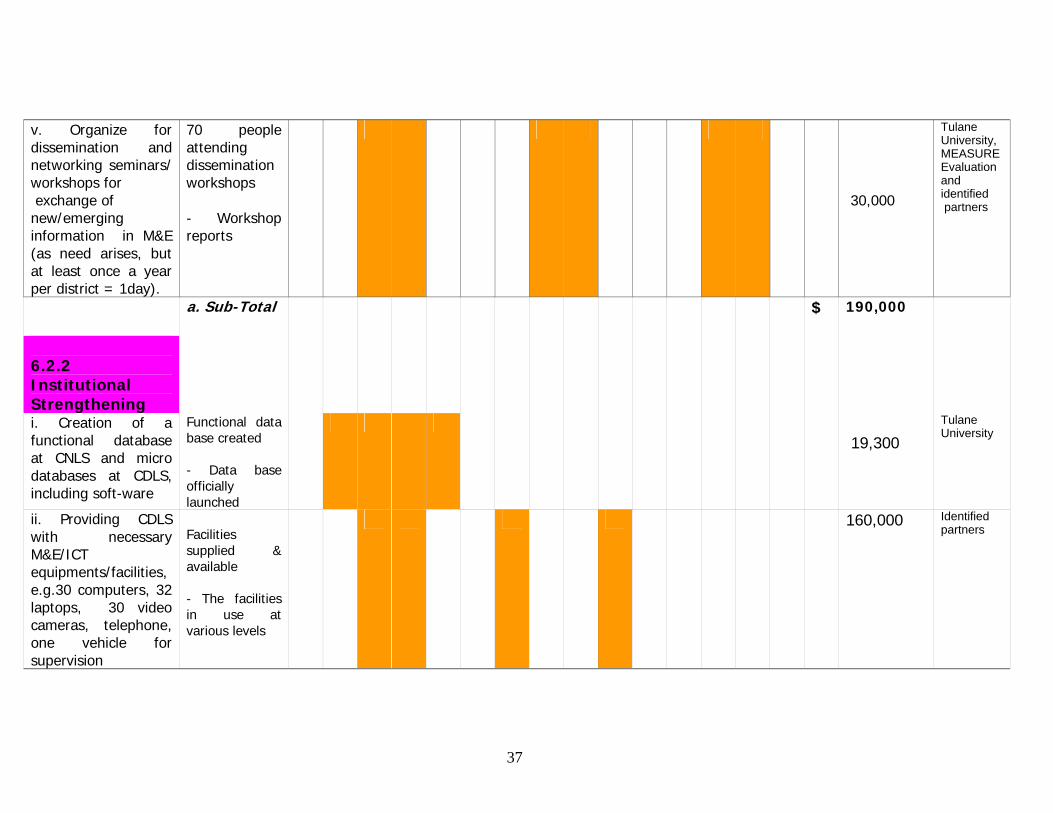
37 37
v. Organize for dissemination and networking seminars/ workshops for exchange of new/emerging information in M&E (as need arises, but at least once a year per district = 1day).
70 people attending dissemination workshops - Workshop reports
30,000
Tulane University, MEASURE Evaluation and identified partners
a. Sub-Total $ 190,000
6.2.2 Institutional Strengthening
i. Creation of a functional database at CNLS and micro databases at CDLS, including soft-ware
Functional data base created - Data base officially launched
19,300
Tulane University
ii. Providing CDLS with necessary M&E/ICT equipments/facilities, e.g.30 computers, 32 laptops, 30 video cameras, telephone, one vehicle for supervision
Facilities supplied & available - The facilities in use at various levels
160,000 Identified partners

38 38
iii. M&E needs assessment at district and linking CDLS micro databases with CNLS database incl. Internet connectivity
CDLS data bases linked to CNLS data base. - M&E Needs assessment report
40,000 Tulane University and identified partners
iv. Linking HIV/AIDS M&E with other HIS/SIS systems, TRAC and other public sectors e.g. MINECOFIN, MINEDUC
Data base at CNLS linked with other HIS/TRAC/Ministries & functional
10,000 MoH/TRAC/ MINICOFIN/ CNLS
v. Carrying out supervision and data audit at district levels (at least one supervision per year)
No. of supervision carried out -Supervision report available
35,000 CNLS/UNDP/ BAD
vi. Establishing & updating a functioning resource center, including e-library, acquisition of books, journals etc
Resource centre available at CNLS & accessible - Reports from Library officer
15,000
CNLS
b. Sub-Total
$ 299,300

39 39
6.2.3 Strengthening Data Collection, analysis Reporting
i. Develop national M&E operational manual (users’ guide) & DCLS level M&E annual data collection Plan (incl translation & reproduction).
Operation manual / plan developed - Manual available at CNLS/CDLS is used for training
100,000
MEASURE Evaluation
ii. Establishing baseline for core National HIV/AIDS indicators, where there are not available (Outsourced consultant & M&E Team).
Baseline figures available for identified indicators -Consultant report on indicators study
15,000
CNLS
iii. Developing and building consensus on a standardized, user friendly data collection instrument (s) & the reporting formats (1 day meeting and reproduction)
Standardized tools and format available - Consensus building report
3,000
CNLS
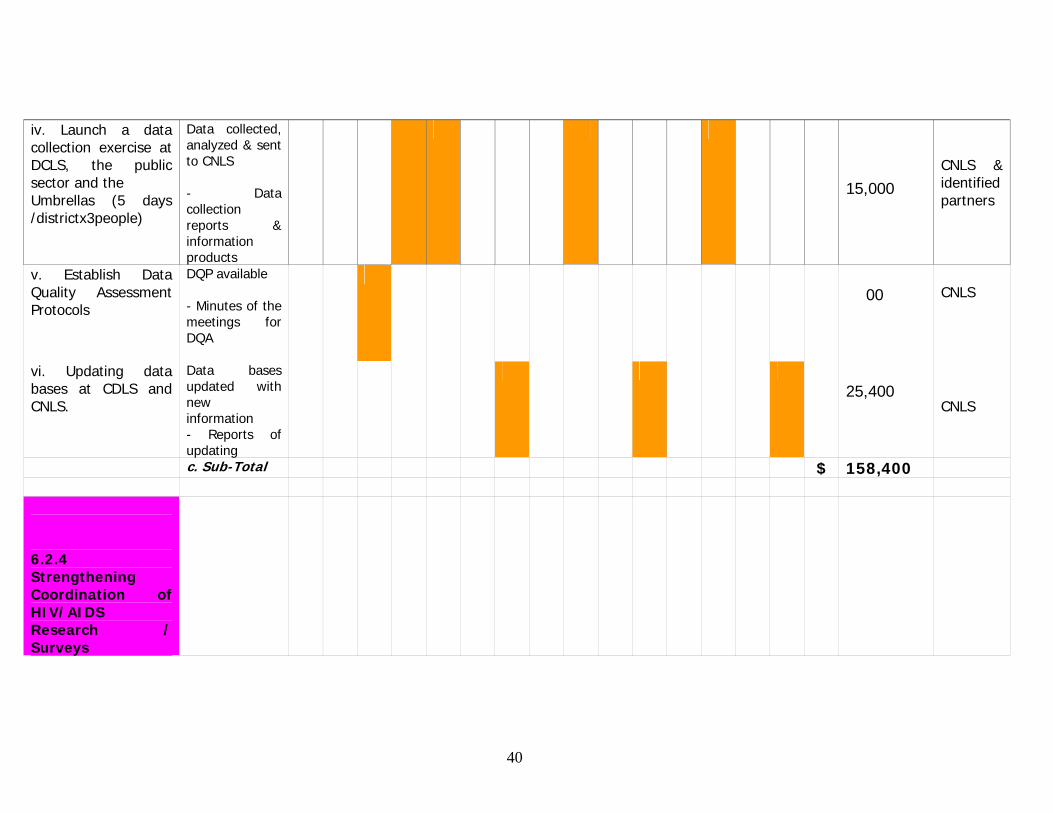
40 40
iv. Launch a data collection exercise at DCLS, the public sector and the Umbrellas (5 days /districtx3people)
Data collected, analyzed & sent to CNLS - Data collection reports & information products
15,000
CNLS & identified partners
v. Establish Data Quality Assessment Protocols
DQP available - Minutes of the meetings for DQA
00
CNLS
vi. Updating data bases at CDLS and CNLS.
Data bases updated with new information - Reports of updating
25,400
CNLS
c. Sub-Total $ 158,400 6.2.4 Strengthening Coordination of HIV/AIDS Research / Surveys
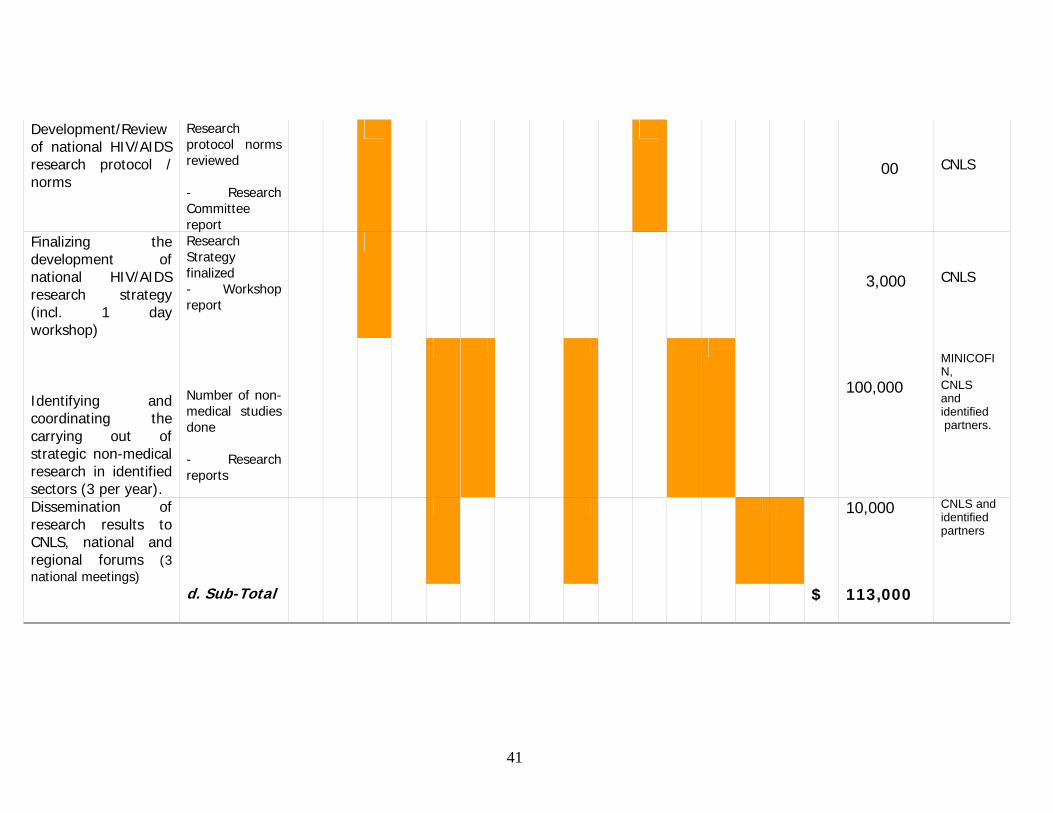
41 41
Development/Review of national HIV/AIDS research protocol / norms
Research protocol norms reviewed - Research Committee report
00
CNLS
Finalizing the development of national HIV/AIDS research strategy (incl. 1 day workshop)
Research Strategy finalized - Workshop report
3,000
CNLS
Identifying and coordinating the carrying out of strategic non-medical research in identified sectors (3 per year).
Number of non-medical studies done - Research reports
100,000
MINICOFIN, CNLS and identified partners.
Dissemination of research results to CNLS, national and regional forums (3 national meetings)
10,000 CNLS and identified partners
d. Sub-Total $ 113,000

42 42
6.2.5 Coordinating National Consultative Meetings and Reviews of M&E Plans
i. Organize Annual national stakeholders meeting on HIV/AIDS response (Dissemination of annual M&E report).
One annual national meeting organized per year - Report of the meeting
40,000
CNLS and identified partners
iii. Organize a workshop for dissemination and discussion of results with HIV implementers in sentinel site Districts
No. of dissemination workshops organized. -Workshop reports
20,000
MoH/Tulane University
iv. Organize dissemination workshop in all the districts for sharing good practice and lessons learned.
No. of dissemination workshops organized. -Workshop reports
5,000
CNLS and identified partners
e. Sub-Total $ 65,000

43 43
i. Total Financial Resources Required (a+b+c+d+e)
835,700
Budget Summary by Areas of Interventions: 6.2.1. Capacity building for M&E at CNLS, CDLS & Umbrella organizations …… 190,000 6.2.2 Institutional Strengthening ……………………………………………………….. 299,300 6.2.3 Strengthening data collection, analysis and reporting ……………………. 158,400 6.2.4 Strengthening Coordination of HIV/AIDS Research / Surveys ………….. 113,000 6.2.5 Coordinating National Consultative Meetings and Reviews of M&E Plans …. 65,000 ------------------------------------------------ Total US$ ……. 835,700

44 44
7.0 Annexes Annex 1: Indicators for Monitoring and Evaluation of national response to HIV and AIDS
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Assessing Impact
Axe I
Result: Reinforce measures of preventing HIV/AIDS transmission
Indicator 1: Change in prevalence of HIV/AIDS in people aged 15-24 years (this is best proxy for change in incidence of HIV/AID for people 15-49)
Percent of blood samples voluntarily given by pregnant women ages 15-24 at ANC clinics which test positive for HIV.
ANC Sentinel surveillance (TRAC) (One method of verification is retrospectively through DHS).
Assessing Outcomes Axe I IR I.1; Change high risk
sexual behavior (in the population)
Indicator I.1a Change in percentage 15-24 year-olds reporting sex with non-marital, non-cohabitating partner last 12 months (this is measure of fidelity)
Percentage of persons ages 15-24 years reporting sex with a non-regular [non-marital, non-cohabiting] partner in the last 12 months
Nat’l Behavioral Surveillance System (TRAC)
Axe I IR I.1 Indicator I.1b Change in percentage 15-24 year-olds reporting condom use last time they had sex with non-marital non-cohabitating partner (this is measure of protected sex)
Percentage of persons ages 15-24 years reporting condom use last time they had sex with non-regular [non-marital, non-cohabiting] partner in the last 12 months.
Nat’l Behavioral Surveillance System (TRAC)
Axe I IR I.2 Change behavior of health personnel to reduce transmission of HIV/AIDS, STI,OI and TB
Indicator I.2. percent facilities where team is practicing safe injections
Percent of health facilities in which all team members are using safe injection techniques as per National norms and procedures (during calendar year).
Summary of site supervisions (DHT) (if budgeted and programmed, can use facility-based surveys)
Axe I IR I.3 Reduce the transmission of HIV through medical prophylaxis
Indicator I.3 Proportion of all HIV+ pregnant women given medical prophylaxis
Percentage of HIV+ pregnant women attending PMTT sites that are given complete antiretroviral prophylaxis according to current protocol in last 12 months
PMTCT site reports (TRAC)
3 Result is IMPACT level; Intermediate Result = outcome level and Sub-IR = output level

45 45
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe I IR I.4; Create a culture
environment more favorable to preventing HIV & STI transmission
Indicator I.4; Number of MSC stories that address change in cultural environment more favorable to preventing HIV & STI transmission
Most Significant Change stories that are submitted to CNLS and meet review board criteria
Various intervention agencies (CNLS’ MSC unit)
Monitoring Programme Outputs Axe I Sub-IR I.1.1 Promote
EABC (through IEC for behavior change)
Indicator I.1.1 Number of new messages that promote EABC
New or significantly different messages that promote ABC which are disseminated in the year (i.e. brochures, Radio and TV sports, leaflets).
Various intervention agencies (does not exist; outsource)
Axe I Sub-IR I.1.2 Increase access to and use of condoms
Indicator I.1.2a Number of condoms sold or distributed to end users
Number of condoms distributed annually to end-users by government facilities and projects.
Social marketing agency reports (Camerwa, CNLS)
Axe 1 Indicator I.1.2b Number of social marketing distribution points for condoms.
Number of social marketing distribution points for condoms.
Social marketing agency reports. (Camerwa, CNLS)
Axe I Sub-IR I.1.3 Educate youth on sexual responsibility
Indicator I.1.3; number schools that receive sex education and/or llfe-skills curriculum AND are trained in its use
Number of schools receiving copy of nationally adopted sex education or life skills curriculum including educational support materials (e.g. audio-visual, exercise, stories, etc) and at least one teacher trained in 12 month period.
annual or ad-hoc reports (MINIDUC)
Axe I Sub-IR I.1.4 Increase the number of people in the population that know their HIV/ serological status (Voluntary Counseling & Testing)
Indicator I.1.4 # of persons tested who come back to VCT centers for results
Number of persons tested in VCT centers which report to TRAC who return to get their results.
VCT site monthly summary reports (TRAC)
Axe I Sub-IR I.1.5 Increase the proportion of the population that knows the causes, symptoms and consequences of STI, OIs and TB
Indicator I.1.5 Number of new messages targeting an increase in knowledge of symptoms of STI, OIs and TB.
New or significantly different messages that promote increase in knowledge of symptoms of STI, OIs and TB which are disseminated in the year (i.e. brochures, Radio and TV sports, leaflets).
Intervention agency reports. (does not exist; outsource)
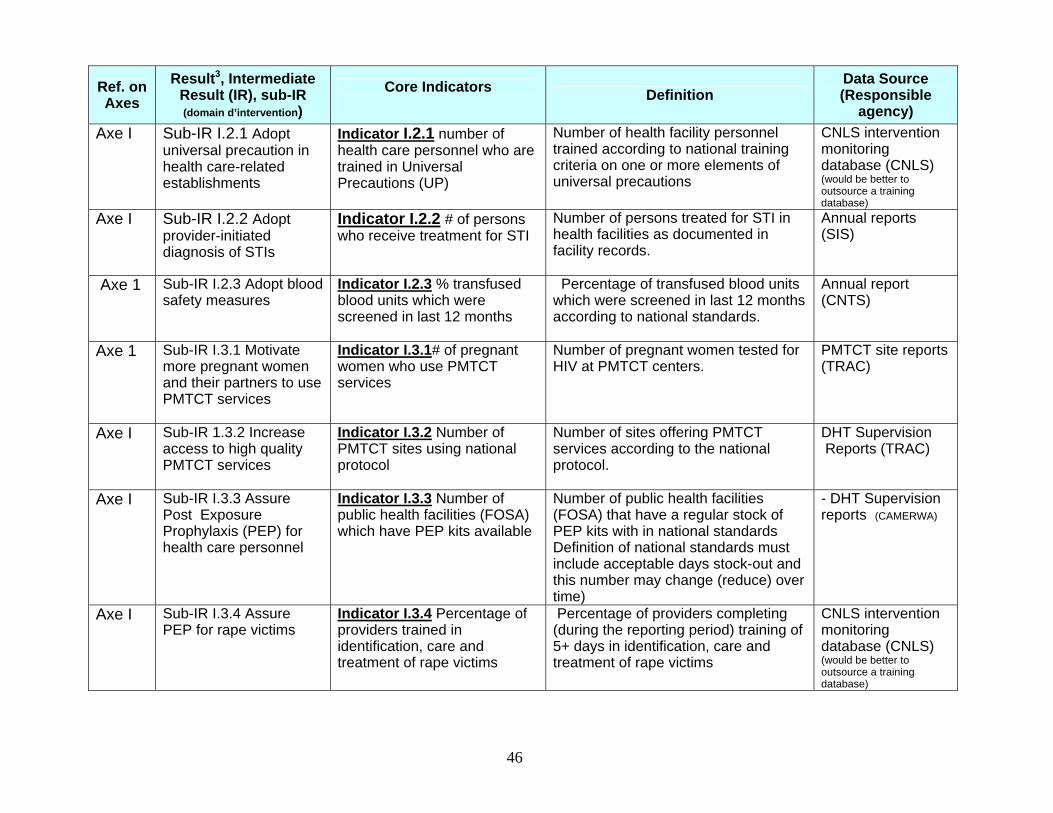
46 46
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe I Sub-IR I.2.1 Adopt
universal precaution in health care-related establishments
Indicator I.2.1 number of health care personnel who are trained in Universal Precautions (UP)
Number of health facility personnel trained according to national training criteria on one or more elements of universal precautions
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe I Sub-IR I.2.2 Adopt provider-initiated diagnosis of STIs
Indicator I.2.2 # of persons who receive treatment for STI
Number of persons treated for STI in health facilities as documented in facility records.
Annual reports (SIS)
Axe 1 Sub-IR I.2.3 Adopt blood safety measures
Indicator I.2.3 % transfused blood units which were screened in last 12 months
Percentage of transfused blood units which were screened in last 12 months according to national standards.
Annual report (CNTS)
Axe 1 Sub-IR I.3.1 Motivate more pregnant women and their partners to use PMTCT services
Indicator I.3.1# of pregnant women who use PMTCT services
Number of pregnant women tested for HIV at PMTCT centers.
PMTCT site reports (TRAC)
Axe I Sub-IR 1.3.2 Increase access to high quality PMTCT services
Indicator I.3.2 Number of PMTCT sites using national protocol
Number of sites offering PMTCT services according to the national protocol.
DHT Supervision Reports (TRAC)
Axe I Sub-IR I.3.3 Assure Post Exposure Prophylaxis (PEP) for health care personnel
Indicator I.3.3 Number of public health facilities (FOSA) which have PEP kits available
Number of public health facilities (FOSA) that have a regular stock of PEP kits with in national standards Definition of national standards must include acceptable days stock-out and this number may change (reduce) over time)
- DHT Supervision reports (CAMERWA)
Axe I Sub-IR I.3.4 Assure PEP for rape victims
Indicator I.3.4 Percentage of providers trained in identification, care and treatment of rape victims
Percentage of providers completing (during the reporting period) training of 5+ days in identification, care and treatment of rape victims
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)

47 47
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) I.4.2a Sub-IR I.4.1 Promote
(the retention of) Rwandan cultural practices that contribute to preventing HIV, STI transmission
Indicator I.4.2 Number of new messages targeting retention of Rwanda cultural practice that contribute to preventing HIV, STI transmission
New or significantly different messages that promote retention of Rwanda cultural practices that contribute to the prevention of HIV and other STIs which are disseminated in the year (i.e. brochures, Radio and TV sports, leaflets).
Intervention agency reports. (does not exist; outsource)
Sub-IR I.4.2 Promote abandoning Rwandan cultural practices that contribute to the transmission of HIV and other STIs
Indicator I.4.1 Number of new messages targeting abandoning cultural practices that contribute to the transmission of HIV and other STIs
New or significantly different messages that promote abandoning Rwanda cultural practices that contribute to the transmission of HIV and other STIs which are disseminated in the year (i.e. brochures, Radio and TV sports, leaflets).
Intervention agency reports. (does not exist; outsource)
Assessing Impact

48 48
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency)
Axe II
Result II: National response to HIV/AIDS adapted to Rwanda’s conditions and surveillance/research results
Indicator II; Number of strategic planning/policy documents that have references or citations of Rwanda-specific surveillance or research documents.
Number of strategic planning/policy documents that have references or citations of Rwanda-specific surveillance or research documents in 12 month period. planning/policy documents include strategic plans from Rwandan institutions. Nat’l or operational policy documents, guidelines, national sector plans, District development plans
Desk review: (Outsourced)
Assessing Outcomes Axe II IR II.1 Increase the
usefulness of surveillance results with respect to the national response to HIV/AIDS
Indicator II.1 Number of articles submitted with a Rwandan among 1st 3 authors to peer-review journals using HIV/AIDS related surveillance and/or research data results.
Number of articles with a Rwanda among first 3 authors submitted to peer-review journals with data from Rwanda’s HIV/AIDS surveillance system. Note: articles do not have to be published. We will add submitted articles to nat’l HIV/AIDS digital library
CNLS Desk review: (Outsourced)
Axe II IR II.2 Increase the usefulness of research results, studies and evaluations
Indicator II.2 Number of documents which reference Rwanda-specific research or surveillance.
Number of documents of any type which (1) are included in the “verified collection” of the national HIV/AIDS digital library, (2) reference specific Rwandan research or surveillance data or results Note; study documents that reference other studies may be included
Desk review (outsource)
Axe II IR II.3 Improve ability of stakeholders to interpret and use surveillances and research results
Indicator I.4; Number of MSC stories that address stakeholder ability to interpret and use surveillance and research results
Most Significant Change stories that are submitted to CNLS and meeting review board criteria
CNLS’ MSC unit (CNLS)
Monitoring Programme Outputs

49 49
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe II Sub-IR II.1.1 Improve
national systems for case notification of morbidity and mortality related to AIDS
Indicator II.1.1 Percentage of all AIDS-related deaths that are reported through national health information system
Percentage of all AIDS-related deaths that are reported through national health information system
SIS (and ?? to estimate total number AIDS-related deaths)
Axe II Sub-IR II.1.1 Indicator II.1.1b Number of medical and non-medical people trained to accurately determine causes of deaths
Number of medical and non-medical people completing training of 5+ days to accurately determine causes of deaths in 12 month period
CNLS intervention monitoring database (would be better to outsource a training database)
Axe II Sub-IR II.1.2 Establish a sustainable behavioral surveillance system
Indicator II.1.2 annual report on behavioral change using National BSS and other behavioral studies is disseminated
National annual report on behavioral change using National BSS and other behavioral studies is disseminated (proxy for sustainable system
Nat’l Behavioral Surveillance System and other behavioral studies (TRAC)
Axe II. Sub-IR II.1.3 Improve the HIV sero-surveillance by including other HIV/AIDS related diseases
Indicator II.1.3 Nat’l surveillance reports include prevalence of infections other than HIV
TRAC uses blood samples obtained during sentinel surveillance to test for pathogens other than HIV as evidence in TRAC surveillance annual reports
Annual surveillance reports (NRL & TRAC)
Axe II Sub- II.1.4 Improve pharmacological sensitivity surveillance to improve AIDS treatment
Indicator II.1.4 Annual report of HIV types (I, II) in Rwanda and level of resistance to treatment « lignes” 1, 2, 3 used in Rwanda
For each HIV serotype in Rwanda, the most recent pharmacy-sensitivity surveillance report identifies the level of resistance to treatment “lines 1, 2, 3” used in Rwanda.
NRL annual report (NRL)
Axe II Sub-IR II.1.5 Improve the statistical and analytic competencies of surveillance technicians
Indicator II.1.5 Number of Rwandans involved in surveillance that are trained in statistics and data analysis
Number of staff members of TRAC and others involved in surveillance analysis and reporting who completed training of 5+ days statistics and data analysis Note; this is subset of II.2.2
CNLS intervention monitoring database (would be better to outsource a training database)

50 50
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe II Sub-IR II.2.1 Improve
the methodological competencies of researchers
Indicator II.2.1 Number of Rwandans trained in research methodologies
Number of Rwandans completing (during the reporting period) training for 5+ days in research methods (with exercises that use HIV/AIDS-related examples and/or data
CNLS intervention monitoring database (would be better to outsource a training database)
Axe II
Sub-IR II.2.2 Improve the statistical and analytical competencies of researchers
Indicator II.2.2 Number of Rwandans researchers that are trained in statistics and data analysis
Number of Rwandan researchers who completed training of 5+ days statistics and data analysis
CNLS intervention monitoring database (would be better to outsource a training database)
Axe II
Sub-IR II.2.3 Involve people to be studied in the identification, design and execution of research
Indicator II.2.3 The number of protocols executed that include participation of the population that is being studied
Number of study protocols approved by the CNLS Research Committee that document the involvement of the population being studied in the design and/or execution and/or analysis of the study
National HIV/AIDS Research Committee annual report (CNLS)
Axe II
Sub-IR II.3.1 Promote and facilitate the routine availability and surveillance and research results
Indicator II.3.1 number of new research studies disseminated at the national annual research exchange conference
Number of new (not previously presented) research study abstracts that are reviewed and approved for dissemination by National HIV/AIDS Research Committee at the national annual research exchange conference
National HIV/AIDS annual conference report (CNLS)
Axe II Sub-IR II.3.2 Improve the analytical capacity of all levels of beneficiaries and decision makers
Indicator II.3.2 Number of non-technical persons trained in data analysis and interpretation with Rwanda specific exercises or examples
Number of non-technical and non-research/surveillance persons completing training for 5 or more days in data analysis and interpretation, with Rwanda-specific exercises or examples in past 12 months
CNLS intervention monitoring database (would be better to outsource a training database)
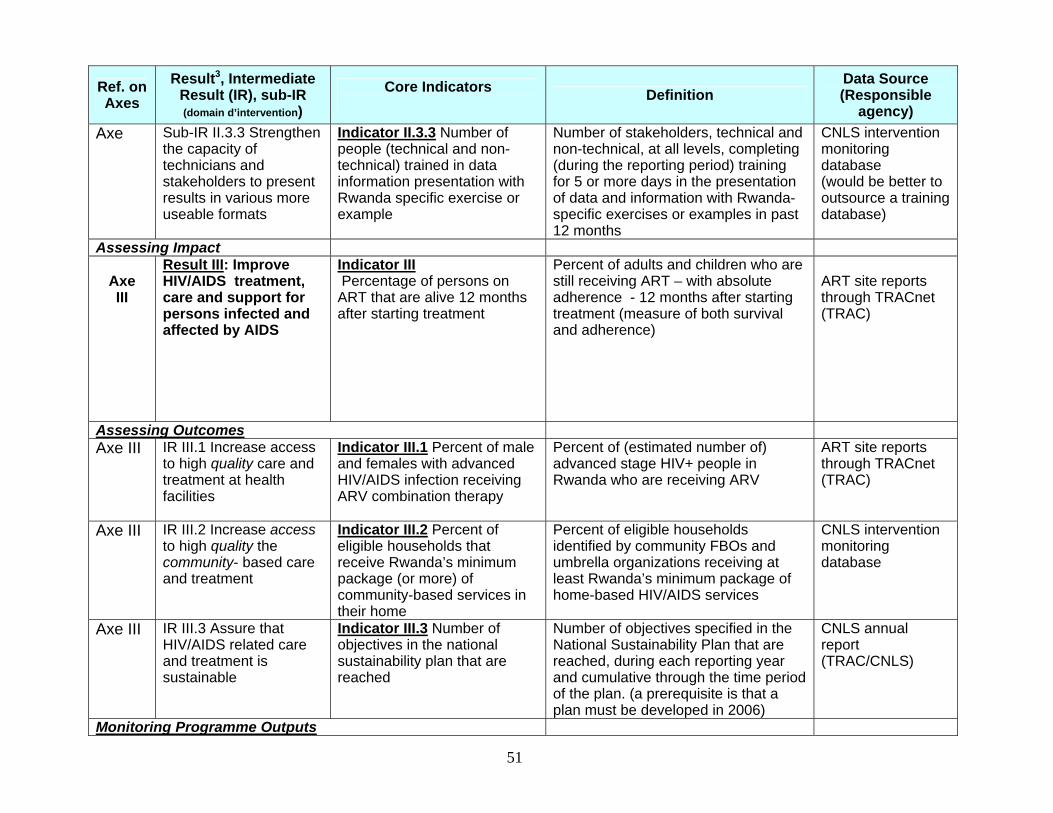
51 51
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe
Sub-IR II.3.3 Strengthen the capacity of technicians and stakeholders to present results in various more useable formats
Indicator II.3.3 Number of people (technical and non-technical) trained in data information presentation with Rwanda specific exercise or example
Number of stakeholders, technical and non-technical, at all levels, completing (during the reporting period) training for 5 or more days in the presentation of data and information with Rwanda-specific exercises or examples in past 12 months
CNLS intervention monitoring database (would be better to outsource a training database)
Assessing Impact
Axe III
Result III: Improve HIV/AIDS treatment, care and support for persons infected and affected by AIDS
Indicator III Percentage of persons on ART that are alive 12 months after starting treatment
Percent of adults and children who are still receiving ART – with absolute adherence - 12 months after starting treatment (measure of both survival and adherence)
ART site reports through TRACnet (TRAC)
Assessing Outcomes Axe III IR III.1 Increase access
to high quality care and treatment at health facilities
Indicator III.1 Percent of male and females with advanced HIV/AIDS infection receiving ARV combination therapy
Percent of (estimated number of) advanced stage HIV+ people in Rwanda who are receiving ARV
ART site reports through TRACnet (TRAC)
Axe III IR III.2 Increase access to high quality the community- based care and treatment
Indicator III.2 Percent of eligible households that receive Rwanda’s minimum package (or more) of community-based services in their home
Percent of eligible households identified by community FBOs and umbrella organizations receiving at least Rwanda’s minimum package of home-based HIV/AIDS services
CNLS intervention monitoring database
Axe III IR III.3 Assure that HIV/AIDS related care and treatment is sustainable
Indicator III.3 Number of objectives in the national sustainability plan that are reached
Number of objectives specified in the National Sustainability Plan that are reached, during each reporting year and cumulative through the time period of the plan. (a prerequisite is that a plan must be developed in 2006)
CNLS annual report (TRAC/CNLS)
Monitoring Programme Outputs

52 52
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe III Sub-IR III.1.1 Assure
equitable coverage of ART services with accent on pediatric care
Indicator III.1.1 % of health care and other facilities that are treating HIV+ infants and adults according to national norms and procedures
Percent of all public and para-public health facilities (FOSA) which treat HIV+ infants and adults according to national standards and procedures Note: this is also a proxy for proportion of all HIV+ infants who are on ARV.
TRAC annual reports (TRAC)
Axe III Sub-IR III.1.2 Improve treatment of OIs according to national norms and procedures
Indicator III.1.2 % of all service providers trained in diagnosis and treatment of OI according to national guidelines
Percent of all (appropriate) service providers that have been trained 5+ days in diagnosis and treatment of OIs according to the national protocol.
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe III
Sub IR III.1.3 Reduce the real cost of accessing HIV/AIDS related care and treatment
Indicator III.1.3 % of people that are TB+ who receive TB therapy Note: this is a proxy for reducing real-cost because, the greatest obstacle to people getting the free TB treatment, is the cost of their visiting a doctor to be diagnosed and eligible for the free treatment
Percent of (estimated number of ) TB+ people who received TB therapy during the 12 month reporting period
TRAC+ annual Report (TRAC+)
Axe III
Sub IR III.1.4 Promote the approach “Provider Initiated Diagnosis” (PID)
Indicator III.1.4 % of all service providers trained in diagnosis and treatment of PID according to national guidelines
Percent of all (appropriate) service providers that have been trained 5+ days in PID according to the national protocol.
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe III
Sub IR III.1.5 Improve the collaboration and the services referrals between health care providers and community agents
Indicator III.1.5 Number of joint sessions/meetings between medical corps and community health care providers
Number of joint sessions/meetings between medical corps (employees of FOSA) and community health care providers (non medical corps)
CDLS and DHT Report (CDLS)

53 53
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe III
Sub-IR III.1.6 Improve therapeutic nutritional support for people on ART
Indicator III.1.6 # of FOSA with capacity (trained personnel and equipment) to provide nutrition therapy as part of in-patient support to HIV/AIDS patients
Number of health facilities (FOSA) with both the necessary equipment, supplies, budget and trained personnel to provide therapeutic nutrition according to established norms Note; this is a composite indicator
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database) + Districts/MOH for info on budgets, plans, equipment
Axe III Sub-IR III.1.7 Integrate care and treatment of OIs among other illnesses supported through health mutuals
Indicator III.1.7 % of health insurance providers (mutuelles de sante) that have included OI in the list of illness covered
Percent of all Number of mutual health insurance societies that have included OIs (Specify eligible OIs) among the list of insured illnesses .
MoH ad-hoc reports (MOH)
Axe III Sub-IR III.1.8 Strengthen health care providers’ capacity to deliver the highest quality care.
Indicator III.1.8 % of all employees working at FOSA trained in quality assurance
Percent of all employees at FOSA (FOSA team) that have been trained 5+ days in (one or more components of) quality assurance)
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe III Sub-IR III.2.1 Assure equitable coverage of community-based care and treatment services
Indicator III.2.1 percent of administrative sectors in which home-based care is provided
Percent of all administrative "secteurs" in which home-based care is provided as reported by implementers to CDLS.
CDLS reports (CDLS)
Axe III
Sub-IR III.2 Improve the community-based care and treatment of people living with HIV/AIDS (medical, psychosocial and spiritual)
Indicator III.2.2 # of HIV+ people assisted in their homes for ART adherence Note: if ART adherence (DOT) is part of minimum HBC package, then this is redundant with indicator III.2
Number of HIV+ people on ARVs who are assisted with adherence (DOT) in their homes.
CDLS reports (CDLS)
Axe III Sub-IR III.2.3 Strengthen the technical capacity of people and organizations providing community-based care and support
Indicator III.2.3 # of people trained in techniques for HIV/AIDS home based care.
Number of non-medical people completing 5+ day training in techniques for HIV/AIDS home care during 12 month reporting period.
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
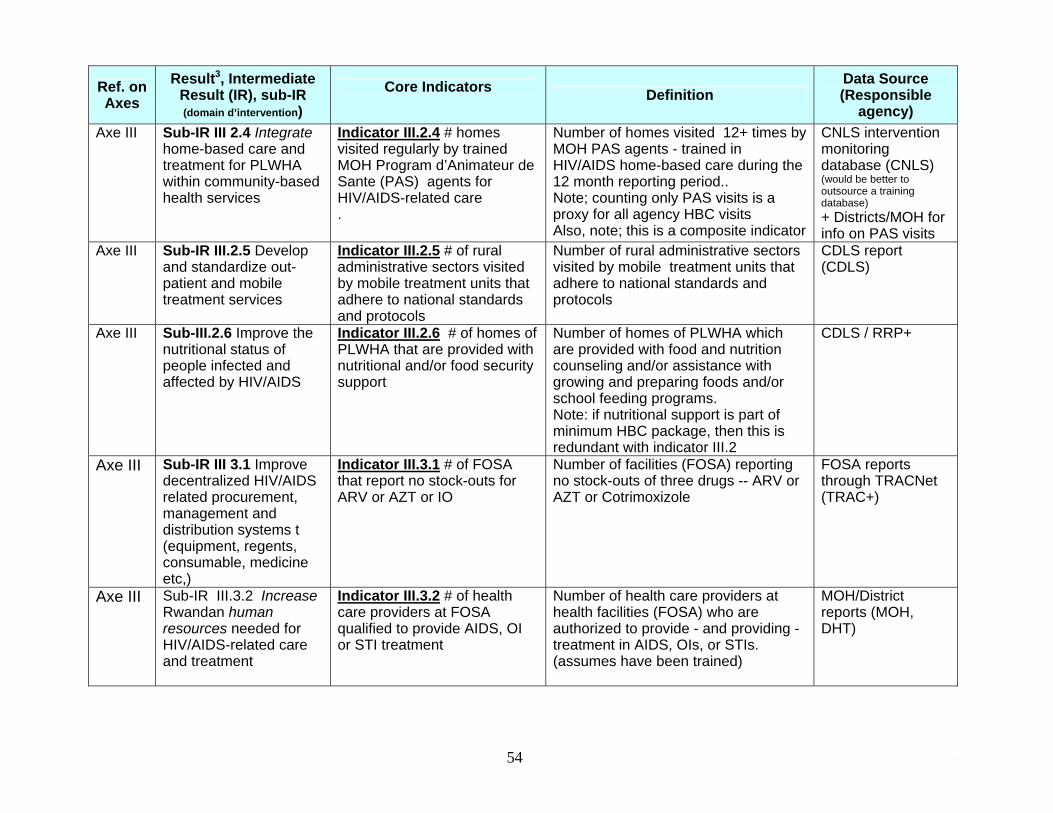
54 54
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe III Sub-IR III 2.4 Integrate
home-based care and treatment for PLWHA within community-based health services
Indicator III.2.4 # homes visited regularly by trained MOH Program d’Animateur de Sante (PAS) agents for HIV/AIDS-related care .
Number of homes visited 12+ times by MOH PAS agents - trained in HIV/AIDS home-based care during the 12 month reporting period.. Note; counting only PAS visits is a proxy for all agency HBC visits Also, note; this is a composite indicator
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database) + Districts/MOH for info on PAS visits
Axe III Sub-IR III.2.5 Develop and standardize out-patient and mobile treatment services
Indicator III.2.5 # of rural administrative sectors visited by mobile treatment units that adhere to national standards and protocols
Number of rural administrative sectors visited by mobile treatment units that adhere to national standards and protocols
CDLS report (CDLS)
Axe III Sub-III.2.6 Improve the nutritional status of people infected and affected by HIV/AIDS
Indicator III.2.6 # of homes of PLWHA that are provided with nutritional and/or food security support
Number of homes of PLWHA which are provided with food and nutrition counseling and/or assistance with growing and preparing foods and/or school feeding programs. Note: if nutritional support is part of minimum HBC package, then this is redundant with indicator III.2
CDLS / RRP+
Axe III Sub-IR III 3.1 Improve decentralized HIV/AIDS related procurement, management and distribution systems t (equipment, regents, consumable, medicine etc,)
Indicator III.3.1 # of FOSA that report no stock-outs for ARV or AZT or IO
Number of facilities (FOSA) reporting no stock-outs of three drugs -- ARV or AZT or Cotrimoxizole
FOSA reports through TRACNet (TRAC+)
Axe III Sub-IR III.3.2 Increase Rwandan human resources needed for HIV/AIDS-related care and treatment
Indicator III.3.2 # of health care providers at FOSA qualified to provide AIDS, OI or STI treatment
Number of health care providers at health facilities (FOSA) who are authorized to provide - and providing - treatment in AIDS, OIs, or STIs. (assumes have been trained)
MOH/District reports (MOH, DHT)

55 55
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe III Sub-IR III.3.3 Establish
system to supply communities with required materials
Indicator III.3.3 # of administrative sectors reporting no stock-outs of home-based care kits.
Number of administrative «sectors» which report no stockouts of home-based care kits Must define HBC “kit” and Need to define acceptable stock out standard
CDLS annual report (CDLS)???
Axe III Sub-IR III.3.4 Execute a national plan to assure that the expanded global care and treatment is sustainable.
Indicator III.3.4 % of activities in the annual operation plan of the national sustainability plan that are completed.
Percent of all planned activities in the annual operation plan of the national sustainability plan which were completed during the 12 month reporting period
CNLS Report
Assessing Impact Axe IV
Result IV: Mitigate the socio-economic of HIV and AIDS
Indicator: increase in GDP
market value of all final goods and services produced in Rwanda during the 12 month reporting period
MINECOFIN
Assessing Outcomes Axe IV IR IV.1 Improve the
socio-economic conditions in Rwanda (and assure vulnerable groups benefit as much as others)
Indicator IV.1a Per capita income)
Total income divided by the total population…
Ministry of Planning; MINECOFIN Reports
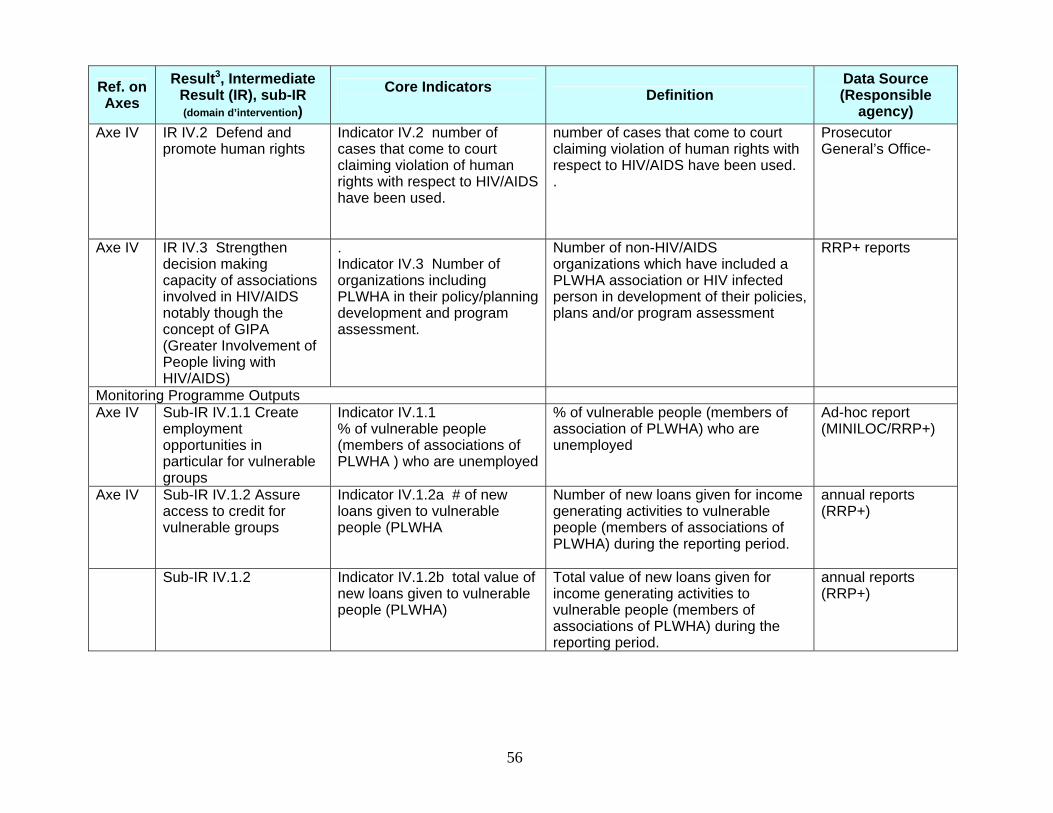
56 56
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe IV IR IV.2 Defend and
promote human rights Indicator IV.2 number of cases that come to court claiming violation of human rights with respect to HIV/AIDS have been used.
number of cases that come to court claiming violation of human rights with respect to HIV/AIDS have been used. .
Prosecutor General’s Office-
Axe IV IR IV.3 Strengthen decision making capacity of associations involved in HIV/AIDS notably though the concept of GIPA (Greater Involvement of People living with HIV/AIDS)
. Indicator IV.3 Number of organizations including PLWHA in their policy/planning development and program assessment.
Number of non-HIV/AIDS organizations which have included a PLWHA association or HIV infected person in development of their policies, plans and/or program assessment
RRP+ reports
Monitoring Programme Outputs Axe IV Sub-IR IV.1.1 Create
employment opportunities in particular for vulnerable groups
Indicator IV.1.1 % of vulnerable people (members of associations of PLWHA ) who are unemployed
% of vulnerable people (members of association of PLWHA) who are unemployed
Ad-hoc report (MINILOC/RRP+)
Axe IV Sub-IR IV.1.2 Assure access to credit for vulnerable groups
Indicator IV.1.2a # of new loans given to vulnerable people (PLWHA
Number of new loans given for income generating activities to vulnerable people (members of associations of PLWHA) during the reporting period.
annual reports (RRP+)
Sub-IR IV.1.2 Indicator IV.1.2b total value of new loans given to vulnerable people (PLWHA)
Total value of new loans given for income generating activities to vulnerable people (members of associations of PLWHA) during the reporting period.
annual reports (RRP+)

57 57
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe IV Sub-IR IV.1.3 Improve
the equity and equality between women and men regarding income generating activities and employment opportunities
Indicator IV.1.3 Female to male ratio of all grants and loans given to PLWHA for income generating activities given to PLWHA
total value (FRw) of grants and loans given to female PLWHA : total value (FRw) given to male PLWHA for income generating activities. during the reporting period
CDLS reports
Axe IV Sub IR IV.1.4 Improve access to formal and informal education for target groups with an accent on PLWHA and OVC
Indicator IV.1.4 # of OVCs and PLWHA supported to attend schools or receive vocational or literacy training
Number of OVC and PLWHA given material or financial support to attend secondary school, vocational training, or literacy programmes.
CDLS reports
Axe IV Sub-IR IV.2.1 Improve the judicial environment for PLWA and OVC
Indicator IV 2.1 # of laws revised, adopted or repealed to ensure that OVC and/or PLWHA rights are respected
# of laws revised, adopted or repealed to ensure that OVC and/or PLWHA rights are respected
Government Gazette (Primature)
Axe IV Sub-IR IV.2.2 Increase the number of employers who have adopted or adapted workplace policies that take into account PLWHA
Indicator IV.2.2 cumulative number of large enterprises and companies which have adopted HIV/AIDS work-place policies and programmes for the first time.
cumulative number of large enterprises and companies which have adopted HIV/AIDS work-place policies and programmes for the first time. a workplan policy/program should include (1) promotion of VCT (2) provide or pay (direct or indirect through insurance) for ARV (3) prevention (4) non discrimination (5) workplace plan of action
APPELAS, umbrella of public sector.
Axe IV Sub-IR IV.2.3 Protect young girls and women from domestic and sexual violence as well as sexual harassment
Indicator IV.2.3 # of cases of violence reported to local law enforcement agencies
# of cases of violence reported to local law enforcement agencies Violence included is “rape”, sexual harassment, assault and battery.
Ad-hoc report (ministry of internal affairs)

58 58
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe IV Sub-IR IV.2.4 Improve
operational policies, norms and procedures to assure equitable access to services for PLWHA and OVCs
Indicator IV.2.4 # of operational policy documents revised or adopted that specifically address issues of equity for PLWHA and OVCs
Number of operational government policy documents revised or adopted to specifically address issues of equity for PLWHA and OVCs, in the past year.
MoH/Umbrella organizations/NGOs > Public Sector report
Axe IV Sub-IR IV.3.1 Strengthen managerial capacity of associations involved with HIV/AIDS
Indicator IV.3.1 # of association members trained for 5+ days on management of HIV/AIDS interventions
Number of members of associations involved with HIV/AIDS who completed training in management for 5+ days during the reporting period. Note; training must include orientation to use of the RRP+ Administration & Finance Manual
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe IV Sub-IR IV.3.2 Balance of the composition of HIV/AIDS related associations (increase proportion of male, middle class & HIV – members).
Indicator IV.3.2a. % of members of associations of PLWA with secondary school education or higher
Percent of new members who had secondary school education or more at the time of joining, during the reporting period.
RRP+ membership records
Sub-IR IV.3.2 Indicator IV.3.2b. % of members of associations of PLWHA not HIV+
Percent new registered members of PLWA associations during the reporting period
RRP+ membership records
Axe IV Sub-IR IV.3.3 Increase involvement of PLWHA in the planning, execution and review of programmes
Indicator IV.3.3 # of associations of PLWHA involved in the planning, implementation, and review of programmes /projects
Number of associations of PLWHA association members who were involved in the planning, implementation, and/or review of programmes or projects, during the reporting period.
RRP+ reports
Assessing Impact

59 59
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe V
Result V: Coordinate the multi-sector response for increased cost-effectiveness
The ratio of the value of government expenditures on HIV/AIDS to value of external assistance for HIV/AIDS
The ratio of the adjusted value of government expenditures on HIV/AIDS to value of external assistance for HIV/AIDS The adjust value of government expenditures is determined by applying average external assistance values for human resources to government human resources.
outsource
Assessing Outcomes Axe V IR V.1 Improve the
capacities of national HIV/AIDS coordination structures
Indicator V.1; Number of MSC stories that address capacity of national HIV/AIDS coordination structures
Most Significant Change stories that are submitted to CNLS and meet review board criteria
Various intervention agencies (CNLS’ MSC unit)
Axe V IR V.2 Assure that HIV/AIDS strategies within national sector plans are implemented
Indicator V.2 Number of HIV/AIDS-related objectives in national sector plans that have been achieved..
Number of HIV/AIDS related objectives across all (sum total) of the sector plans, which have been achieved
Desk review of sector plans for MTR (CNLS)
Axe V IR V.3 Increase HIV/AIDS related regional activities that are jointly executed
Indicator V.3 Number of regional interventions that are jointly executed
Number of cross-border activities executed by Rwandans for which there are similar, coordinated activities executed by the country sharing that border and for which there are meetings to plan and/or exchange experiences/ideas Note; the cross-border activities are a proxy for all regional interventions even those that are not cross-border
CNLS reports on regional joint interventions.

60 60
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe V IR V.4 Assure that
intervention agencies benefit from national planning and monitoring as much as the coordination agencies
Indicator V.1; Number of MSC stories that address intervention agencies perception of usefulness/benefits of contributing to national planning, M&E
Most Significant Change stories that are submitted to CNLS and meet review board criteria
Various intervention agencies (CNLS’ MSC unit)
Axe V IR V.5 Jointly evaluate the multi-sector response to HIV/AIDS
Indicator V.5 mid-term review of HIV/AIDS national response (2007) and end-of period evaluation (2009/10) are jointly executed with representation from all stakeholders.
Joint Multisectoral reviews which have ensured the participation of a wider segment of stakeholders in annual of mid-term review. Stakeholders include beneficiaries, implementers, donors, and coordination structures (CNLS, TRAC, CDLS, umbrellas).
Ad-hoc report (CCM or similar structure or outsourced)
Monitoring Programme Outputs Axe V Sub-IR V.1.1 Strengthen
leadership capacity of personnel
Indicator v.1.1 # of members of coordination structures, trained in leadership skills, meeting facilitation or public speaking
Increase in Number of members of coordination structures completing training of 5+ days in leadership skills: meeting or workshop facilitation or public speaking during the 12 month reporting period.
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe V Sub-IR V.1.2 Strengthen administrative and managerial capacity of institutions
Indicator V.1.2 # of members of coordination structures trained in administration and management.
Increase in Number of members of coordination structures training for 5+ days in administration and management during the 12 month reporting period
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
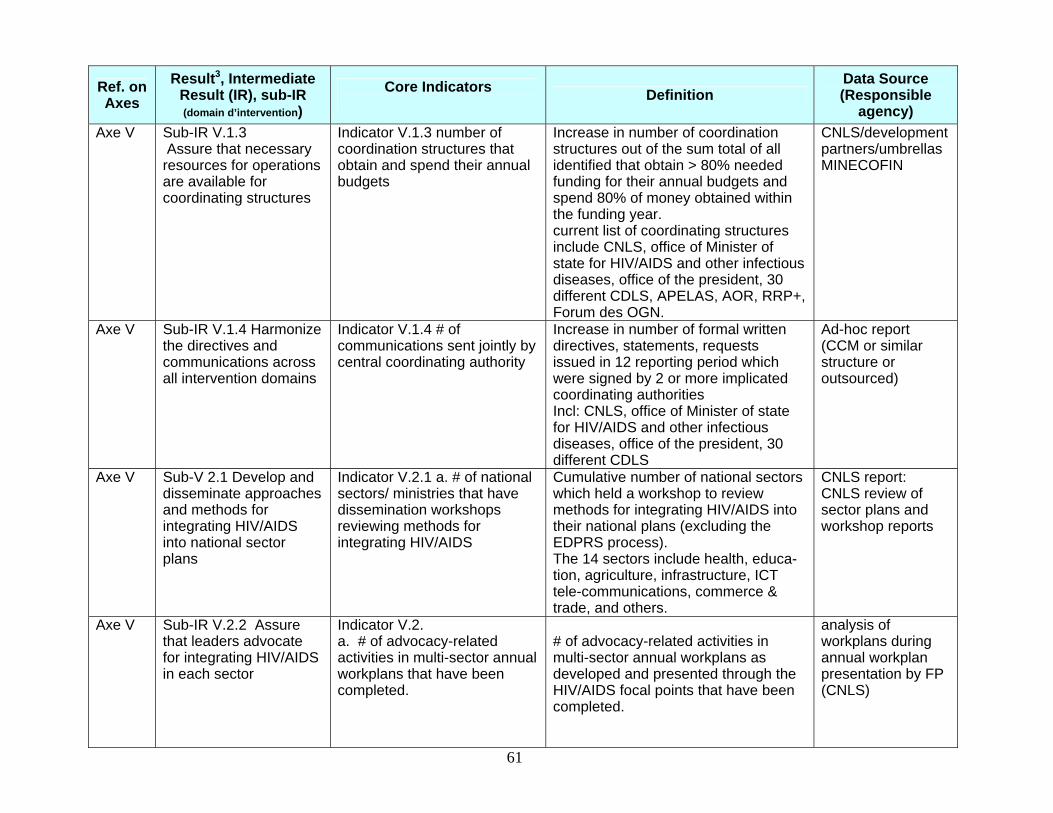
61 61
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe V Sub-IR V.1.3
Assure that necessary resources for operations are available for coordinating structures
Indicator V.1.3 number of coordination structures that obtain and spend their annual budgets
Increase in number of coordination structures out of the sum total of all identified that obtain > 80% needed funding for their annual budgets and spend 80% of money obtained within the funding year. current list of coordinating structures include CNLS, office of Minister of state for HIV/AIDS and other infectious diseases, office of the president, 30 different CDLS, APELAS, AOR, RRP+, Forum des OGN.
CNLS/development partners/umbrellas MINECOFIN
Axe V Sub-IR V.1.4 Harmonize the directives and communications across all intervention domains
Indicator V.1.4 # of communications sent jointly by central coordinating authority
Increase in number of formal written directives, statements, requests issued in 12 reporting period which were signed by 2 or more implicated coordinating authorities Incl: CNLS, office of Minister of state for HIV/AIDS and other infectious diseases, office of the president, 30 different CDLS
Ad-hoc report (CCM or similar structure or outsourced)
Axe V Sub-V 2.1 Develop and disseminate approaches and methods for integrating HIV/AIDS into national sector plans
Indicator V.2.1 a. # of national sectors/ ministries that have dissemination workshops reviewing methods for integrating HIV/AIDS
Cumulative number of national sectors which held a workshop to review methods for integrating HIV/AIDS into their national plans (excluding the EDPRS process). The 14 sectors include health, educa-tion, agriculture, infrastructure, ICT tele-communications, commerce & trade, and others.
CNLS report: CNLS review of sector plans and workshop reports
Axe V Sub-IR V.2.2 Assure that leaders advocate for integrating HIV/AIDS in each sector
Indicator V.2. a. # of advocacy-related activities in multi-sector annual workplans that have been completed.
# of advocacy-related activities in multi-sector annual workplans as developed and presented through the HIV/AIDS focal points that have been completed.
analysis of workplans during annual workplan presentation by FP (CNLS)

62 62
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe V Sub-IR V.2.3 Establish
an awards mechanism ceremony for best interventions and agencies in each sector
Indicator V.2.3 Number of sectors holding annual award ceremonies in which HIV/AIDS interventions are recognized
The number of sectors holding annual award ceremonies in which HIV/AIDS interventions are recognized, in the 12 month reporting period
review of Sector Annual Reports (CNLS)
Axe V Sub-IR V 3.1 Harmonize the [regional] HIV/AIDS policies and frameworks/documents
Indicator V.3.1 % of Rwandan national and sector-specific HIV/AIDS plans and frameworks are consistent with regional plans and framework
% national and sector-specific HIV/AIDS plans and frameworks are consistent with regional plans and framework Note; will identify and list the plans and frameworks to be compared
GLIA report. (GLIA secretariat or outsourced)
Axe V Sub-IR V 3.2 Assure that jointly developed cross-border HIV/AIDS activity plans are executed
Indicator V 3.2 # of joint cross border workplans executed.
# of joint cross border workplans executed
GLIA report. (GLIA secretariat )
Axe V Sub-IR V 3.3. Make available necessary resources (funds) for the execution of regional HIV/AIDS interventions
Indicator V.1.4 number of regional HIV/AIDS interventions/initiatives that obtain and spend their annual budgets
Increase in number of regional HIV/AIDS interventions/initiative out of the sum total of all identified that obtain > 80% needed funding for their annual budgets and spend 80% of money obtained within the funding year.
Regional secretariat e.g. GLIA > CNLS report
Axe V Sub-IR V 4.1 Simplify and harmonize planning and monitoring tools
Indicator V.4.1 # variables collected by national coordination structures and large bi/multi-lateral projects
# variables collected by national coordination structures and large bi/multi-lateral projects (CNLS, MAP, GF, PEPFAR) Note: this is a proxy for time it takes to report.
Ad-hoc review: planning and monitoring tools (CNLS)
Axe V Sub-IR V 4.2 The level of detail needed for national planning and workplan monitoring is appropriate for national level reporting (in decentralized context)
Indicator V.4.2 number of activities identified in workplans submitted to CNLS
Reduction in the sum total of all interventions (activities, tasks, milestones, etc) identified across all work plans submitted to CNLS during 12 month reporting period.
Ad hoc report (CNLS or outsourced)
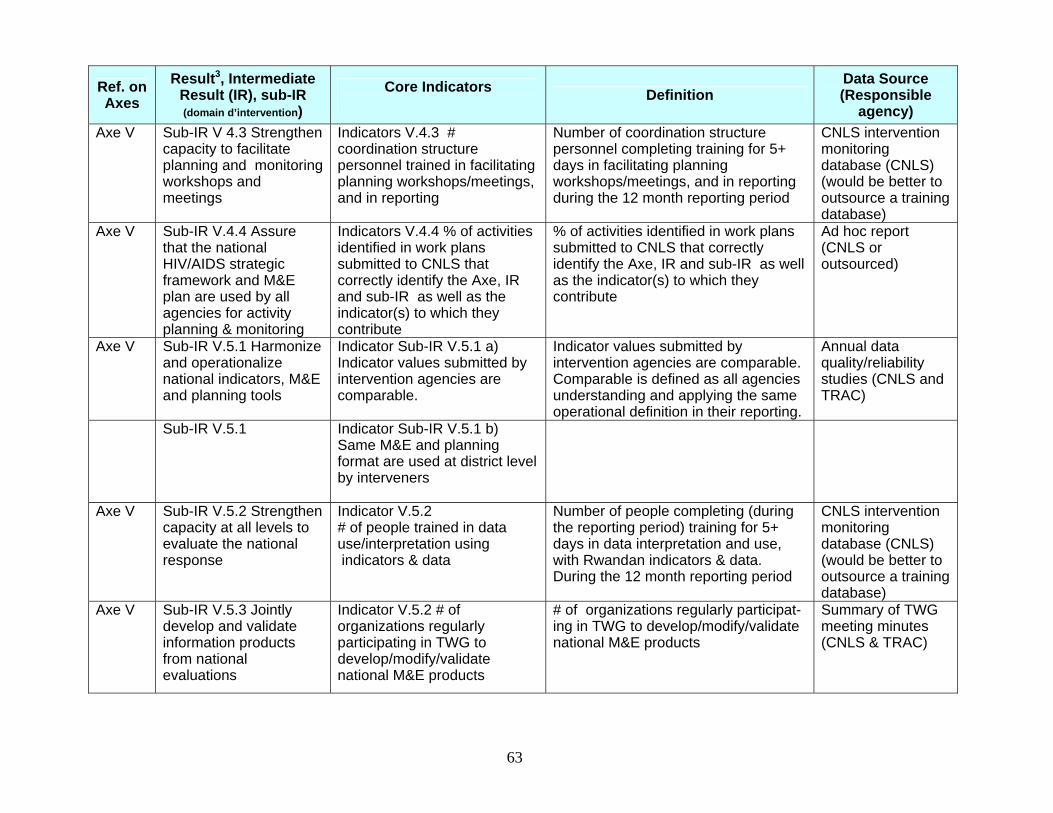
63 63
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe V Sub-IR V 4.3 Strengthen
capacity to facilitate planning and monitoring workshops and meetings
Indicators V.4.3 # coordination structure personnel trained in facilitating planning workshops/meetings, and in reporting
Number of coordination structure personnel completing training for 5+ days in facilitating planning workshops/meetings, and in reporting during the 12 month reporting period
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe V Sub-IR V.4.4 Assure that the national HIV/AIDS strategic framework and M&E plan are used by all agencies for activity planning & monitoring
Indicators V.4.4 % of activities identified in work plans submitted to CNLS that correctly identify the Axe, IR and sub-IR as well as the indicator(s) to which they contribute
% of activities identified in work plans submitted to CNLS that correctly identify the Axe, IR and sub-IR as well as the indicator(s) to which they contribute
Ad hoc report (CNLS or outsourced)
Axe V Sub-IR V.5.1 Harmonize and operationalize national indicators, M&E and planning tools
Indicator Sub-IR V.5.1 a) Indicator values submitted by intervention agencies are comparable.
Indicator values submitted by intervention agencies are comparable. Comparable is defined as all agencies understanding and applying the same operational definition in their reporting.
Annual data quality/reliability studies (CNLS and TRAC)
Sub-IR V.5.1 Indicator Sub-IR V.5.1 b) Same M&E and planning format are used at district level by interveners
Axe V Sub-IR V.5.2 Strengthen capacity at all levels to evaluate the national response
Indicator V.5.2 # of people trained in data use/interpretation using indicators & data
Number of people completing (during the reporting period) training for 5+ days in data interpretation and use, with Rwandan indicators & data. During the 12 month reporting period
CNLS intervention monitoring database (CNLS) (would be better to outsource a training database)
Axe V Sub-IR V.5.3 Jointly develop and validate information products from national evaluations
Indicator V.5.2 # of organizations regularly participating in TWG to develop/modify/validate national M&E products
# of organizations regularly participat-ing in TWG to develop/modify/validate national M&E products
Summary of TWG meeting minutes (CNLS & TRAC)

64 64
Ref. on Axes
Result3, Intermediate Result (IR), sub-IR (domain d’intervention)
Core Indicators Definition
Data Source (Responsible
agency) Axe V Sub-IR V. 5.4 Assure
that national M&E products are available and useable (to/by information providers and users).
Indicator V.5.4 # of M&E products that stakeholders have obtained/accessed.
# of M&E products that stakeholders have obtained/accessed and, if they have tried to use them, they find them useable M&E products are: all CNLS M&E reports, Nat’l virtual library, UNGASS report, outputs from intervention database, etc (to be identified in separate indicator target table (part II)
Email /phone survey (CNLS or outsourced)
Axe V Sub-IR V.5.5. Coordinate research and training.
Indicator V.5.4a. existence and use of national long-term or annual HIV/AIDS-related research plans
If annual and/or long-term plan for HIV/AIDS research exists, then evidence from meeting minutes and other sources demonstrate that it was used to coordinate research.
Desk review (CNLS or outsource)
Sub-IR V.5.5 Indicator V.5.4b existence and use of a national training database
If a national training database exists and evidence from meeting minutes and other sources demonstrate that it was used to coordinate training.
Desk review (CNLS or outsource)
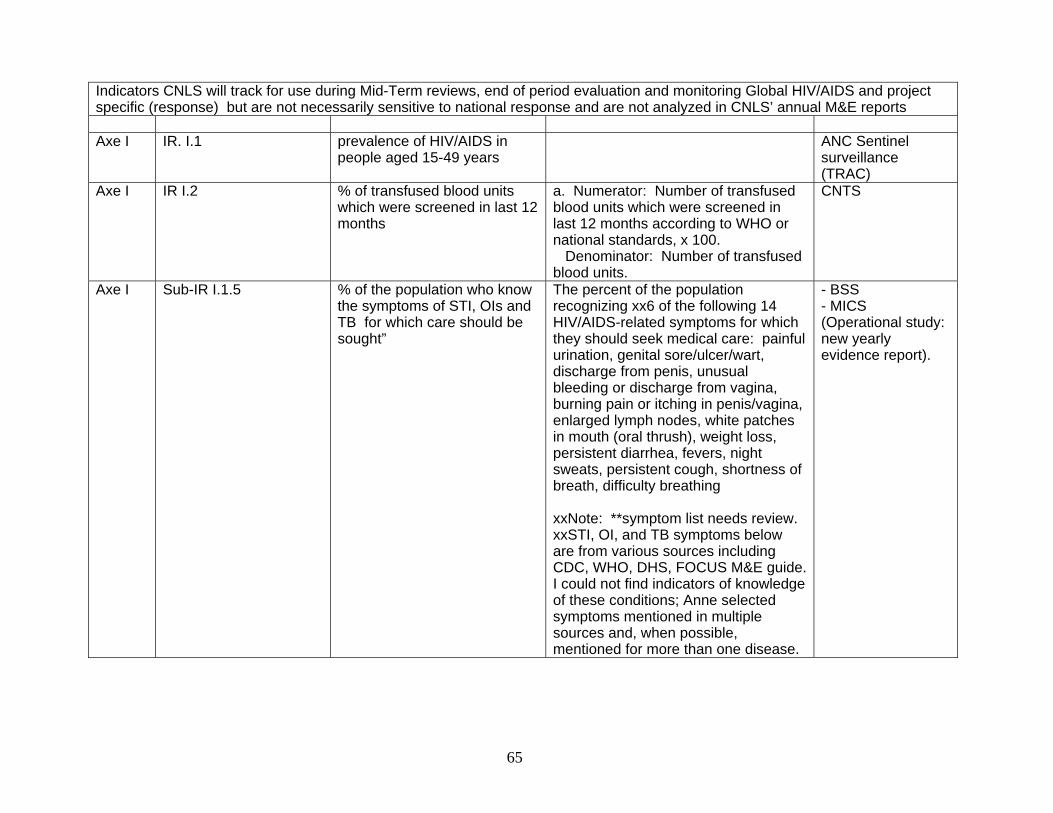
65 65
Indicators CNLS will track for use during Mid-Term reviews, end of period evaluation and monitoring Global HIV/AIDS and project specific (response) but are not necessarily sensitive to national response and are not analyzed in CNLS’ annual M&E reports Axe I IR. I.1 prevalence of HIV/AIDS in
people aged 15-49 years ANC Sentinel
surveillance (TRAC)
Axe I IR I.2 % of transfused blood units which were screened in last 12 months
a. Numerator: Number of transfused blood units which were screened in last 12 months according to WHO or national standards, x 100. Denominator: Number of transfused blood units.
CNTS
Axe I Sub-IR I.1.5 % of the population who know the symptoms of STI, OIs and TB for which care should be sought”
The percent of the population recognizing xx6 of the following 14 HIV/AIDS-related symptoms for which they should seek medical care: painful urination, genital sore/ulcer/wart, discharge from penis, unusual bleeding or discharge from vagina, burning pain or itching in penis/vagina, enlarged lymph nodes, white patches in mouth (oral thrush), weight loss, persistent diarrhea, fevers, night sweats, persistent cough, shortness of breath, difficulty breathing xxNote: **symptom list needs review. xxSTI, OI, and TB symptoms below are from various sources including CDC, WHO, DHS, FOCUS M&E guide. I could not find indicators of knowledge of these conditions; Anne selected symptoms mentioned in multiple sources and, when possible, mentioned for more than one disease.
- BSS - MICS (Operational study: new yearly evidence report).

66 66
Sub-IR I.1.5 % of persons with STI symptoms in last 12 months who sought care from a service provider
% of persons with one or more STI symptoms in last 12 months (painful urination, genital sore/ulcer/wart, discharge from penis, unusual bleeding or discharge from vagina, burning pain or itching in penis/vagina) who sought care from a service provider
- BSS - MICS (Operational study: new yearly evidence report).
IR III.2 Proportion of eligible households that receive 2 or more of 4 types of community-based services in their home
Numerator: Number of eligible households identified by FBOs and umbrella organizations receiving 2 or more types of community-based services in their homes, x 100. Denominator: Number of eligible households identified by FBOs/umbrella organizations. Eligible = adult age 18-59 chronically ill for 3 or more months or ill for 3 or more months before death (PEPFAR) Types of services are: medical, emotional/psychological, material, and other. Note: PEPFAR needs data on % receiving all 4 types.
Ad-hoc report (CDLS-> CNLS)
IV.2 Ratio of orphaned to non-orphaned children aged 10-14 currently attending school.
Number of non-orphaned 10-14 yr olds : number of orphaned 10=-14 yr olds An orphan is a child having lost both parents (should review definition to assure is same as current int’l norm)
MINEDUC Annual Report. -Census- NBS -Special study
IV.1 Ratio women/men of per capita income
GDP/population for women : GDP/population for men
Ministry of Planning; MINECOFIN Reports
I, II, III, IV, V AIDS Program Effort Index (API) score
Score on AIDS Program Effort Index
CNLS/UNAIDS report

67 67
BIBLIOGRAPHY 1. CNLS/RWANDA, Cadre Stratégique Multisectoriel de lutte contre le SIDA au RWANDA 2005-
2009, Kigali, 19 décembre, 2005. 2. CNLS/RWANDA, Plan National de Suivi et Evaluation pour les programmes du VIH/SIDA, 2002-
2006, Kigali, Janvier, 2003.
3. WHO, UNAIDS, GLOBAL FUND, USAID, MEASURE Evaluation, Family Health International (FHI), National AIDS Programmes. A guide to indicators for monitoring and evaluation national antiretroviral programmes, Geneva, 2005.
4. WHO, UNAIDS, Office of the United States Global AIDS Coordination, USAID, Patient monitoring
guidelines for HIV Care and antiretroviral Therapy (ART), Geneva, 2005.
5. Malawi National AIDS Commission, National HIV/AIDS, Monitoring and Evaluation Plan.Part B/Operations plan, Lilongwe 3, Malawi, July 2003.
6. Department of Health, Monitoring and Evaluation South Africa, Monitoring and Evaluation
framework for the comprehensive HIV/AIDS Care, Management and Treatment for South Africa. Technical notes: indicators, Numerators and denominators for the comprehensive HIV and AIDS Care, Management and treatment Plan South Africa/2004. South Africa, 2004
7. WHO, Monitoring the Declarational of commitment on construction of core indicators Geneva,
Switzerland August 2003.
8. Prevention and Control Office (HAPCO). National Monitoring and evaluation Framework for Multisectoral Response to HIV/AIDS in Ethiopia National HIV/AIDS, Ethiopia December 2003
9. GHANA AIDS Commission, USAID, The National Monitoring and Evaluation Plan for HIV/AIDS
in Ghana 2001-2005, Ghana, 2001
10. NACC/KENYA, National HIV/AIDS Monitoring and evaluation Framework). Nairobi July 2005.
11. NAC/MALAWI, National HIV/AIDS Monitoring and Evaluation Plan (Part A: Conceptual Framework), Lilongwe July 2003.
12. LaFond A, Frankel Nina, Staff Handbook on Capacity Building in Monitoring and Evaluation,
Measure Evaluation Project, Carolina Population Centre, University of North Carolina at Chapel Hill, April 2005.
13. CNLS/Rwanda : Community HIV and AIDS Programs Monitoring Operational Guide, Draft document,
2006
14. CNLS/RWANDA : Reports of National HIV and AIDS Planning, Monitoring and Evaluation Technical Working Group, 2005-2006

68 68
15.
: