Embed Size (px)
Citation preview

FIELD ACTION REPORT
Service Uptake and Characteristics of InjectionDrug Users Utilizing North America's First MedicallySupervised Safer Injecting Facility
Evan Wood, PhD. Mark W, Tyndall, ScD, MD, Zhenguo Qui, PfiD, Ruth Zhang, MSc, Jutio S,G, Montaner, MD.and Thomas Kerr, PhD
In 2003, tfie city of Vancouver, British Columbia, opened NorthAmerica's first government sanctioned safer injecting facility,where injection drug users (IDUs) can inject preobtained illicitdrugs under the supervision of nurses. Use of the service byIDUs was followed by measurable reductions in public drug useand syringe sharing, IDUs who are frequently using the programtend to be high-intensity cocaine and heroin injectors and home-less individuals.
The facility has provided high-risk IDUs a hygienic space wheresyringe sharing can be eliminated and the risk of fatal overdosereduced. Ongoing evaluation will be required to assess its im-pact on overdose rates and HIV infection levels, as well as its abil-ity to improve IDU contact with medical care and addiction treat-ment {Am J Public Health. 2006:96:770-773. doi:10.2105/AJPH.2004.057828)
ILUCIT INJECTION DRUG USEhas led to serious public healthproblems, such as HIV infectionand overdoses, as well as majorcommunity concems, such aspublic injection drug use.'"** Toaddress these concems, a num-ber of European cities and Syd-ney, Australia, have opened saferinjection facilities (SIFs), whereinjection drug users (IDUs} caninject preobtained illicit drugs,'Unfortunately, there is a dearthof quantitative evaluations ofthese facilities in the publicbealth literature." In September2003, Vancouver, British Colum-bia, Canada, opened NorthAmerica's first government-sanc-tioned SIF in the city's Down-town Eastside (Figure 1), TheSIF, known as Insite, is lundedby Vancouver Coastal Health(the local health authority). We
report on service uptake andclient characteristics,
VANCOUVER SAFERINJECTING FACILITY
The Vancouver SIF began oper-ating on September 22, 2003,and !S open daily between 10:00AM and 4:00 ,\M, 'I"he eventsleading to the program's imple-mentation have recently been de-scribed,^ Within the SIF, IDUsare provided with sterile injectingequipment and emergency carein the event of overdose, as wellas primary medical care services.In addition, an addictions coun-selor is available on site to meetwith clients and to help facilitatereferral to treatinent programs.To date there have been nomajor adverse events or harmsamong members of the Insitestalf."*
The methodology for evaluat-ing the SIF-through the recruit-ment of a representative cohortof SIF users, known as the Scien-tific Evaluation of Supervised In-jecting (SEOSI) cohort-has re-cently been described in detail.We present cohort baseline char-acteristics and our examinationof factors associated with report-Ing daily SIE use at the time ofparticipant's baseline interview.Variables of interest are listed inTables 1 and 2. and variable def-initions were identical to those
used in previous studies of Van-couver IDUs,'"""'^ Variables po-tentially associated with daily SIFuse were examined in bivariateaiialyses.
DISCUSSION ANDEVALUATION
The average number of dailyvisits to the SIF in its first weekof operation was approximately200; an approximate average of500 visits per day has been con-sistently observed since the 2months after the facility's open-ing. Diiring the latest 6 monthsfor which data are available fromthe SIF database (March 1,2004, to August 31, 2004). theaverage breakdown of sub-stances injected per month in-cluded heroin (42%), cocaine(32%), and other substances(26'y()): there were an average of104 visits with the addictionscounselor per month, and therewere an average of 19 responsesto potential overdoses per month.
Between December 1, 2003,fuid July 30, 2004, 904 SIFusers were randomly invited toenroll in the SEOSI study,among whom 735 (81,3%) at-tended the extemal research siteto leam about participation inthe SIF evaluation. Overall. 5were deemed by research staffunfit to provide informed con-sent and were not enrolled, and
770 I Field Action Report | Peer Reviewed | Wood et al. American Journal of Public Health | May 2006, Vol 96, No, 5
FIELD ACTION REPORT
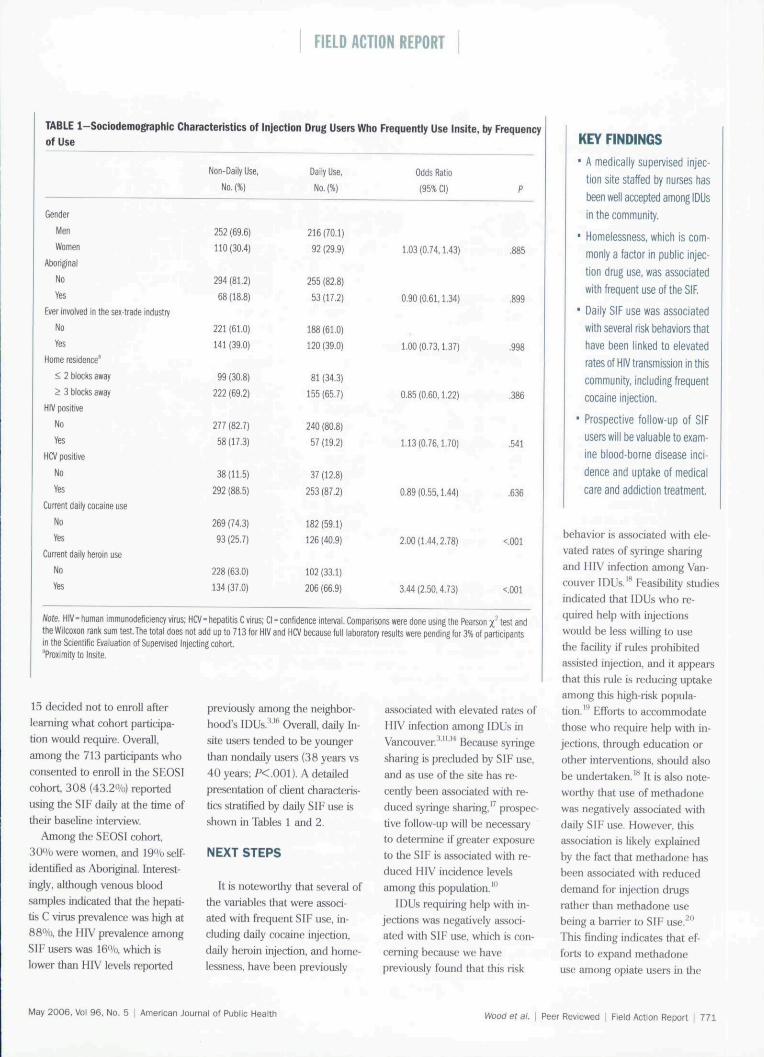
TABLE 1-Sociodemographic Characteristics of Injection Drug Users Who Frequently Use Insite, by Frequencyof Use
Gender
MenWomen
Aboriginal
NoVes
Ever involved in the sex-trade industry
NoYes
Home residence'
< 2 blocks away
> 3 bJocks away
HIV positive
NoYes
HCV positive
NoYes
Current daily cocaine use
NoYes
Current daily heroin use
NoVes
Non-Daily Use,
No, (%)
252 (69,6)
110 (30,4)
294 (81,2)
68 (18.8)
221 (61,0)
141 (39,0)
99 (30.8)
222 (69,2)
277 (82,7)
58(17,3)
38(11,5)
292 (88,5)
269 (74.3)
93 (25,7)
228 (63,0)
134 (37.0)
Daily Use,
No, (%)
216 (70,1)
92 (29.9)
255 (82,8)
53(17,2)
188 (61,0}
120 (39,0)
81 (34,3)
155 (65.7)
240 (80,8)
57 (19.2)
37 (12,8)
253 (87,2)
182 (59.1)
126 (40,9)
102 (33,1)
206 (66.9)
Odds Ratio
(95% Cl)
1,03(0,74,1,43)
0.90 (0,61,1,34)
1,00 (0.73,1,37)
0,85 (0,60,1.22)
1,13(0,76,1,70)
0.89 (0.55,1,44)
2,00(1,44,2,78)
3,44(2,50,4,73)
P
,885
,899
,998
,386
,541
,636
<,001
<,001
Note. HIV- human immunodeficiency virus; HCV- hepatitis C virus; Cl - confidence interval. Comparisons were done using the Pearson x^ test andthe Wilcoxon rank sim test,The total does not add up to 713 for HIV and HCV hecajse full laboratory results were pending tor 3% of participantsin the Scientffic Evaluation of Sipen/ised Injecting cohort,'Proximity tclnsite.
15 decided not to enroll afterlearning what cohort participa-tion would require. Overall,among the 713 participants whoconsented to enroU in the SHOSIcohort, 308 (43,2%) reportedusing the SIF daily at the time oftheir baseline interview.
Among the SEOSI cohort,30% were women, and 19% self-identified as Aboriginal, Interest-ingly, although venous bloodsamples intlicated that the hepati-tis C virus prevalence was high at88%, the HIV prevalence amongSIF users was 16%, which islower than HIV levels reported
previously among the neighbor-hoods IDUs.'"• Overall, daily In-site users tended to be youngerthan nondaily users (38 years vs40 years; P< ,001), A detailedpresentation of client characteris-tics stratified hy daily SIF use isshown in Tables 1 and 2,
NEXT STEPS
It is noteworthy that several ofthe variables that were associ-ated with frequent SIF use, in-cluding daily cocaine injection,daily heroin injection, and honie-lessness, have been previotisly
associated with elevated rates ofHIV infection among IDUs inVancouver.'"'"' Because syringesharing is precluded by SIF use,and as use of the site bas re-cently been associated with re-duced syringe sharing,'' prospec-tive foUow-up will be necessaryto determine if greater exposureto the SIF is associated with re-duced HIV incidence levelsamong this population."'
IDUs requiring help with in-jections was negatively associ-ated with SIF use, which is con-cerning because we havepreviousiy found that tiiis risk
KEY FINDINGS• A medically supervised injec-
tion site staffed by nurses hasbeen well accepted among IDUsin the community,
• Homelessness, which is com-monly a factor in public injec-tion drug use, was associatedwith frequent use ofthe SIF,
• Daily SIF use was associatedwitfi several risk betiaviors thathave been linked to elevatedrates of HIV transmission in thiscommunity. Including frequentcocaine injection.
• Prospective follow-up of SIFusers will be valuable to exam-ine blood-borne disease inci-dence and uptake of medicalcare and addiction treatment.
behavior is associated with ele-vated rates of syringe sharingand HIV infection among Van-couver IDUs.'" Feasibility studiesindicated that IDUs who re-quired help with injectionswould be less willing to usethe facility if rules prohibitedassisted injection, and it appearsthat this rule is reducing uptakeamong this high-risk popula-tion, ' ElTorts to accommodatethose who require help with in-jections, through education orother inteiventions, should alsobe undertaken."^ It is also note-worthy that use of methadonewas negatively associated withdaily SIF use. However, thisassociation is likely explainedby the fact that methadone hasbeen associated witb reduceddemand for injection drugsrather than methadone usebeing a barrier to SIF use,^"This finding indicates that ef-foits to expand methadoneuse among opiate users in the
May 2006, Vol 96, No, 5 ! American Journal of Public Health Wood et al. \ Peer Reviewed | Field Action Report | 771

FIELD ACTION REPORT
communi^ should be increased,and futiire studies must examinethe impact of tbe SIF on refer-rals to addiction treatmentprograms.''
Conversely, it is encouragingtliat daily use of the SIF was as-sociated with several high-riskbehaviors including cocaine in-jection and bomelessness. Thefact that the daily SIF use wasassociated with homelessness isperhaps not suipnsing given thatprevious studies have indicatedthat SIF use may be associatedwith not having a safe place toinject.' Given that homeless per-sons may be more likely to injectin public, (he association be-tween homelessness and fre-quent SIF use may partially ex-plain why the opening of the SIFwas linked to substantial reduc-tions in public drug use."'
Our study was limited by itscross-sectional study design andthe evaluation is limited by itsobservational nature. Unfortu-nately, this cohort will have tobe followed longitudinally forseveral years before an examina-tion of blood-borne infection in-cidence will be possible, and it islikely that ethical concems willprevent interventional studiesthat randomize participants to
TABLE 2-Prevalence of Frequent Insite Use Stratified by Behavioral and Drug Use Variables
Currently using methadone
NoYes
Currently homeless
NoYes
Ever use a "shootiig gallery"^
NoYes
Currently having difficulty accessing syringes
NoYes
Ever borrowing syringes in the past 6 moriths
NoVes
Ever borrow equipment in the past 6 months'"
NoYes
Ever use injection drugs in piibiic
NoYes
Ever require help injecting drugs
NoYes
Binge drug use in the past 6 months
NoVes
Non-Daily Use,
No.(%)
265 (73,2}
97 (26.8)
321 (88,7)
41(11,3}
41 (11,3)
321 (88,7)
317 (87,6)
45 (12.4)
328 (90,6)
34 (9,4)
269 (74,3)
93 (25,7)
322 (89.0)
40(11,0)
78(21,5)
284(78,5}
129 (35,6)
233 (64,4)
Daily tise,
No.(%)
263 (85,4)
45 (14.6)
236 (76,6)
72 (23,4)
32 (10.4)
276 (89.6)
280 (90,9)
28 (9.1)
265 (86.0)
43 (14,0)
238 (77,3)
70 (22.7)
266 (86,4)
42 (13,6)
96(31,2)
212 (68,8)
126 (40,9)
182 (59,1)
Odds Ratio
(95% Cl}
0,47(0.32.0,69)
2.39(1.57,3,63)
1,10(0,68,1,80}
0.70 (0,43,1.16)
1,57(0,97,2,53)
0,85(0,60,1,21}
1.27 (0,80,2,02)
0.61(0.43,0,86)
0,80(0,59,1,09)
P
<,001
<.O01
,698
,168
,066
.373
,309
,005
.161
Note, Cl - confidence interval. Comparisons were done with the Pearson -^ test and the Wilcoxon rank sum test,A nonsanctioned space where drug users congregate to inject drugs,
^Spoons, cookers, filters, cotton, or plungers.
FIGURE 1-Vancoifver's supervised Injecting facility.
SIF use VS nonuse.^^ Anotherlimitation is that the evaluationlargely relies on seif-repoil;therefore, it is likely that wehave underestimated sociallyundesirable behaviors, such assyringe sharing.^'' Finally, fre-quent use of the SIF was onthe basis of self-report and wasmeasured cross-sectionally atthe time of recruitment into thestiidy. Future studies examiningexposure to the SIF will requireprospective examination of SIFuse through the use of the SIFdatabase.
This report is the first presen-tation of the sociodemographicand risk characteristics of a rep-resentative sample of SIF usersin the public health literature.Our study indicates that the SIFwas well accepted by high-riskIDUs in the community and thatfrequent use is characterized byhomelessness and high-intensitydrug use, induding cocaine injec-tion. The site's opening was re-cently associated with improvedpublic order and reduced syringesharing,''^' and it is noteworthythat frequent use was associated
772 I Field Action Report | Peer Reviewed | Wood et al. American Journal of Public Health | May 2006, Vol 94, No, 5

FIELD ACTION REPORT
with homelessness in the presentstudy because homeless drugusers may be particularly proneto public drug use,"^ Althoughthese preliminary findings are en-couraging, prospective evaluationof SIF users wili be required toexamine the impact of SIF useon a number of outcomes, suchas rates of blood-borne infections.In addition, program rules thatmay create barriers to uptakemust be further examined. •
About the AuthorsAt the lime ofthe study, all authors werewith the British Columbia Centre for Excel-lence m HIV/AIDS St Pauls Hospital.Vancouver. British Columbia. Evan Wood.Mark W Tyndall. Julio S. G. Montaner.and Thomas Kerr are also with the De-partment ofMediiine at the University ofBritish Columbia. Vancouaer.
Requests for reprints should be sent toEvan Wood. PhD. Division of Epidemiol-ogy and Population Health. British Colum-bia Centre for Excellence in HIV. AIDS.60S-1081 BurrardSt. Vancouver. BCV6Z I Y6. Canada (e-maii [email protected]).
This Tvport uus accepted Aprd 15.2005.
ContributorsH, Wood designed the study and pre-paj-ed the first draft of Ihe article.E, Wood, R, Zhang, atid Z, Qui con-ducted the dala analyses. Ml authorscontrihuted to tlie design of Ihe study,as well as to the draffinjr and revision ofthe article.
AcknowledgmentsThe safer injoctiiig facility' evaluation wasmade possible hy a financial coiitrihiitioiifrom Health Canada. Ottawa, Ontario,
The authors wish to thaiilf the stafTofthe Insite .safer InjectiTig facility and Van-couver Coastal lleallh (Chris Buchncrand I leather Hay), We also thank Deb )-rah Crahani, Bonnie Devlin, AaronEddie, Suzy Coulter, Megan Oleson,Peter Vann, Dave Isham. Daniel Kane,Steve Ciaspar. Carl Bognaj. and EvelynKing for their research and adrrmiistra-dve assistance.
Note, The views expressed herein donot represent the official policies ofHealth Canada,
Human Participant ProtectionniLs study was appnwed hy the Univer-
.sily of British Columbia's research ethicsboard al St Paul's Hospilai,
Referencest, Strathdee SA, Calai N. Safaiean M,et al. Sex differences in risk factors forHIV seroconversion among injectiondrug users: a 10-year perspective. ArchIntemMed. 2001;16t:1281-1288,
2. Des JarlaLs DC. Hagan H, Fried-man SR. et ai. Maintaining low HIVseropre vale nee in pojiulations of injeet-ing drug users. y/iAf/1. 1995,274:1226-1231
3. Tyndall MW, Currie S, Spittal P, elal. Intensive injection cocaine use as theprimajy risk factor in the VancouverH[V-1 epidemic,/4/DS 20(B;]7:887-893,
4. Garfield J, Drucker E, Fataloverdttse trends in major US cities:1990- t997 Addictions Research andTheoiy. 2001,9:425-436.
5. Wood F. Tyndall MW, Spittal PM,et al. Unsafe injection practiees in a eo-hort of injection drug users in Vancou-ver: could safer injecting ix>onis help?CMAJ. 200t;lt)Fi,4()5-410,
a. Coffin PO. Galea S, Ahem J, LeonAC. Vlahov D. "IardifT K, Ojiiates, co-caine and alcohol combinations in acci-dental drug overdose deatlis in NewYork City, 1990-9B. Addiction. 2003;98:739-747,
7. Dolan K. Kimber J, Fr> C, Eitzger-ald J, McDonald D, I mutmann V. Dnigconsumption facilities in Europe and theestablishment of supervised injectingcentres in Australia, Drug Alcohol Rev.2000;19:337-346.
8. Kimber J, Dotan K. van Heck I,Hedrich D, Zurhold H, Dmg consump-tion facilities: an update since 2000,[hug Alcohol Rev. 2{}0y.22.227-2-^3.
9. Wood E, Kerr T, Montaner JS, elal. Rationale for evaluating Nortii Amei -ica's first medically supervised safer-injecting facility. Lancet Infect Dis 2004;4:301-306,
10. Wood E. Kerr T. Lloyd-Sniith E. etal. Mediodologj' for evaluating Insite:Canada's fii"st medically supervised saferinjection facility for injection drug users,HarmReductJ 2004:1:9,
11. Spittal PM, Craib KJ, Wood E, etal. Risk factors for elevated HIV inci-dence rates among female injectiondrug users in Vancouver. CMAf 2002;166:894-899,
12. Miller CL, Spittal PM, LaLiberte N,et al. Females experiencing sexual anddrug vulnerabilities are at elevated riskfor HIV infection among youth who useinjection drugs, / Acquir Immune DejicS fcdr, 2002:30:335-341,
13. Wood E, Tyndall MW, Spittal PM.et al, Tactors associated with persistenthigh-risk syringe sharing in the presence
of an established needle exchange \>m-gi-amme, AIDS 2002;16:941-943,
14. Comcil TA, Ktiyper I.M, Shovelloi'j , et al, tJnstahlo housing, associated riskbehaviour, and increased risk Ibr HIVinfection among injeelion drug asers.Health Place. 2006; 12:79-85,
15. Tyndall MW, Craib KJ. Currie S, LiK. O'Shaughnessy MV, Sehechter MT,Impact of HIV infection on mortality ina cohort of injection drug users, / AcquirImmune Defw Si/ndr. 2001;28:351-357
16. Strathdee SA, Patrick DM, CurrieSL, et al. Needle exchange is notenough: lessons from Ihe Vancouverinjecting drug use study, AIDS. 1997;11:F59-F65.
17 Kerr T, Tyndall M, I.i K, MontanerJS, Wood E, Safer injection facility useand syringe sharing in injection drugusers. Lancet. 2005;40:115J-llft7
18, Wood F. Spittal HM, Kerr T, et ai.Requiring help injcfaiiig as a risk factorlor HIV infection in tlie Vancouver epi-dtinic: implications for HIV prevention,CanJ Public Health. 2003;94:355-359,
19, Kerr T, Wood F.. Small D, f^lepuA, Tyndall MW Potential use of saferinjecting facilities among injection drugusers in Vancouver's Downtown East-side. CMAf 20()3;169:759-763,
20, Gibson DR, Elynn NM. McCarthyJJ. ElTectiveness of methadone treatmentin reducing IllV risk behavior and HIVserocon version among injecting drugusers. AIDS. 1999;13:1807-1818,
21, Wood E, Kerr T. Small W. et al.Changes in public order after the open-ing of a medically supervised safer in-jecting facility for illicit injection drugusers, CMAJ 2004,171:731-734.
22, Christie T, Wood F, Sehechter MT,O'Shaughnessy MV, A comparison ofthe new Pederal Guidelines regulatingsupervised injection site research inCanada and the Tri-Coundl PolicyStatement on Ethical Conduct lor Re-search Involving Human Subjects, IntJDrug Policy. 2003; 15:66-73.
23, DesJ^lais DC, Paone D, MillikenJ, et al. Audio-computer interviewing lomeasure risk behaviour for HIV amonginjecting drug usei-s: a quasi-randomisedtiial. Lancet. 1999:353:1657-1661.
24, Broadhead RS. Kerr Tl 1, GmndJPC, Altite FL, Safer injection facilitiesin North America: their piace in publicpolicy and health initiatives, J DrugIssue.f. 2OO2;32:329-355,
May 2006, Vo) 96, No. 5 | American Journal of Public Health Wood era/. | Peer Reviewed | Field Action Report | 773