Embed Size (px)
Citation preview
S T E P SDr MIKE SCOTTChief PharmacistUnited Hospitals TrustAntrim HospitalNorthern IrelandProcurement Distribution Interest Group (PDIG)
8 June 2006

safe
therapeutic
economic
pharmaceutical
selection
STEPS(Modified SOJA)


Medicines Management
“Encompassing the entire way that medicines are selected, procured, delivered, prescribed, administered and reviewed, to optimise the contributions that medicines make to producing informed and desired outcomes of patient care.”
Audit Commission 2001

Integrated Medicines Management
Decreased length of stayDecreased readmission rateReduced wastage of patients’ own drugsMore accurate drug historyImproved appropriateness of medicine use
Improved patient safetyImproved use of medical and nursing staff timeFaster discharge processImproved discharge prescription accuracyImproved medicine use – counsellingImproved communication across the interface
Tasks Undertaken
Communication with primary care on admissionAccurate medical historyManagement of patients’ own drugsInpatient management including counsellingPharmacist discharge and counsellingCommunication with primary care on discharge
More Accurate Drug History
Mean number of queries on the initial inpatient kardex was reduced by 4.2 per patient, reflecting improved medicines
management and impacting on length of stay.
Improved Medicine Use
There was a significant improvement in the medication appropriateness index.
AdmissionDischargeControl 13.16 9.97Intervention 17.48 5.69

Health Service Journal Award 2003

Lack of Integrated Product Use
This was identified as a significant deficient element in the current medicines management system.
- different choice of agents in a therapeutic class
- different generics and parallel imports being used in primary care
- confusion for patients, particularly the elderly

CostSECONDARY CARE PROCUREMENT
Contract based - 3 yearsAll trusts contributeTender by generic nameBids assessed by a pharmacist advisory panelRecommendations made to the Executive Panel for approvalExecutive Committee of Trust Chief Executives

SuccessThis contract process has worked well and achieved significant savings for the secondary sector.
In the 2004-2007 contract savings in excess of £2 million per annum were achieved representing a 7.6% reduction.
87.2% being subject to good procurement practice as defined by the Audit Commission.
Problems
Lack of primary care element
Loss leading to gain primary care business (80% of spend is in the community)
Product name constraint therefore there is no mechanism to consider therapeutically equivalent usage

Procurement Primary Care
Independent contractors both GP and pharmacist
GP prescribes ideally generically
Pharmacist supplies cheapest product by procurement
Prices set by CSA on tariff
Hello! Hello!

Northern Health and Social Services Board (NHSSB)
Population of 440,000
Three stage process -Stage one – branded genericsStage two – therapeutic classesStage three – generic generics

NORTHERN AREA PRESCRIBING FORUM
Professional Secretary - Dr M ScottConsultantsGeneral PractitionersCommunity PharmacistsHospital PharmacistsBoard Director of Pharmacy
(Chairman)Area Medical AdvisorPrescribing Advisors (Boards)Prescribing Advisors (PCGs)NursesMedicines Information Pharmacist

Local Medical Committee
Locality Groups for Community Pharmacists
Drug and Therapeutics Committee
IMPLEMENTATIONPhase OnePrimary Care
Prescribing advisors and prescribing support assistants actually promoted and implemented the changes with GPs
Secondary CareConsultants agreed to the product switches automatically carried out by pharmacistsUnited gave notice to companies tendering for Regional Contract that NHS price would be a determination in their adjudication – hence different products used
THREE YEAR PERIOD
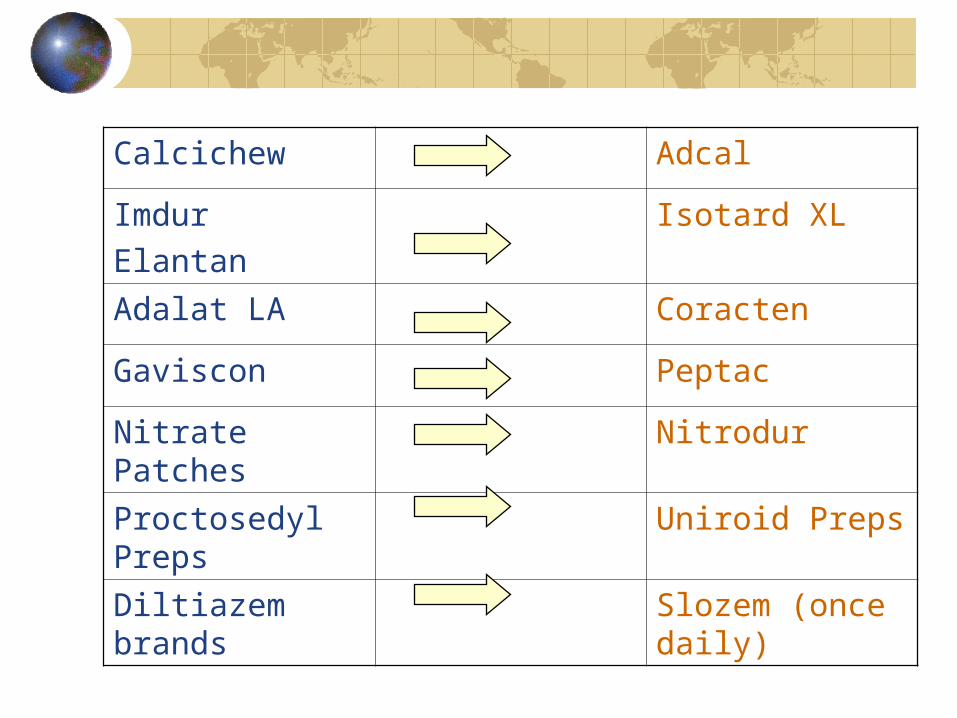
Calcichew Adcal
ImdurElantan
Isotard XL
Adalat LA Coracten
Gaviscon Peptac
Nitrate Patches Nitrodur
Proctosedyl Preps
Uniroid Preps
Diltiazem brands
Slozem (once daily)

PRIMARY CARE PERCENTAGES FOR NITRATES
Elantan LA 25 -10.4%
Elantan LA 50 -17.6%
Imdur SR -27.2%
Modisal MR -23.5%
Monomax SR -31.9%
Ismo Retard -58.3
Isotard XL +223.9%

STAGE IITherapeutic Tendering
Competitive tendering for pharmacologically similar products
Current processes use generic name for bidding purposes
By default excludes similar chemical entities with the same pharmacological actions and range of potential therapeutic issues
Tendering therapeutically will create competition and therefore ensure product standardisation at best value

Eeeny MeenyMiny Mo

safe
STEPS
therapeutic
economic
pharmaceutical
selection

STEPSQuality first, then safety, then cost- effectivenessFull product integration between primary and secondary care Full ownership by both general practitioners and hospital consultants Standardisation of generics (plus branded)Therapeutic tendering

STEPSSelection - agreed criteria (weighted)1st Step - Clinical Evaluation2nd Step – Safety Evaluation3rd Step – Budgetary Impact AssessmentSelected medicines for 70% prescribingNo restrictionsTransparent and Defensible

STEPS
Improve quality of prescribing information across primary / secondary careFramework updated regularly with emerging evidenceThree year formulary (for 70% prescribing will be class specific)No discount into the secondary care sector International Links
STEPS ____________________
MATRIX CONSTRUCTION AND
CLINICAL EVALUATION

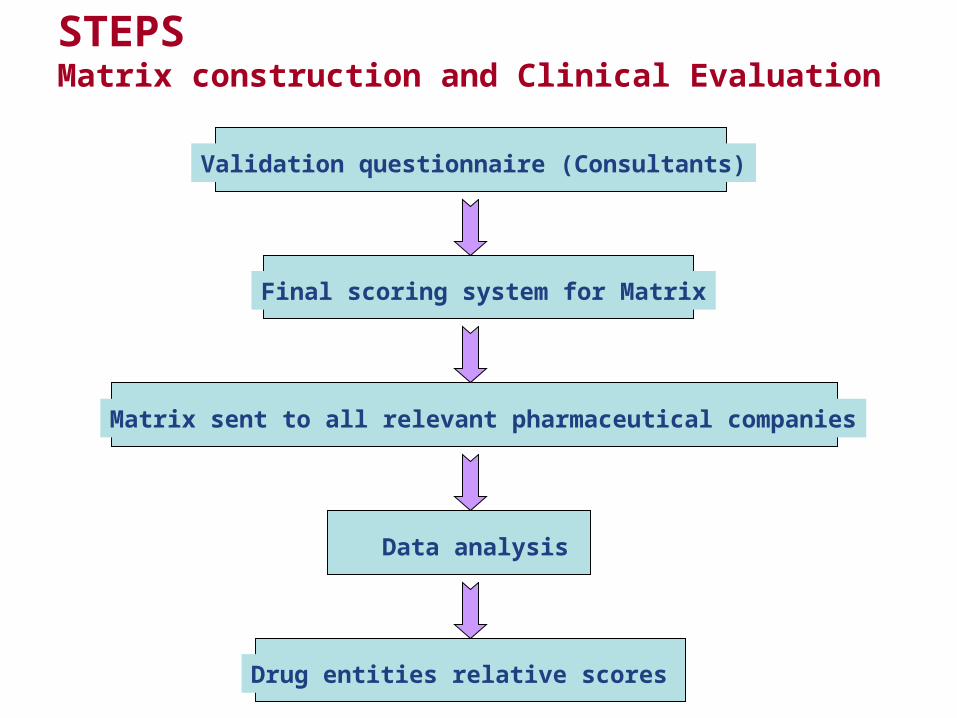
STEPSMatrix construction and Clinical Evaluation
Extensive literature review
Selection criteria identification
Expert panel – Consultants, GPs, Pharmacists
Relative weight assignments
Draft indicative scoring system
STEPSMatrix construction and Clinical Evaluation
Final scoring system for Matrix
Matrix sent to all relevant pharmaceutical companies
Validation questionnaire (Consultants)
Data analysis
Drug entities relative scores

ACE INHIBITORS MATRIXNumber of licensed indicationsNumber of formulationsTrough / peak ratio BP lowering
effectVariability in biovailabilityInteractionsClinical efficacySide-effectsDosage frequency
TOTAL 1000 pts

DRUG ENTITIES SELECTION
RISK ASSESSMENT
A - CRITICAL INFORMATION STEP
1. Labelling2. Packaging3. Storage conditions4. Blisters5. Patient information
leaflets
Accept

B - ADDED VALUES STEP (EXTRA POINTS)
1. Calendar packs2. EAN barcode3. Pack size4. Tab/cap colouring and
marking5. Label instructions space
BUDGET IMPACT ANALYSIS
DDD profilingDDD fractions refiningCost calculation both primary and secondary care pricesAffordability (selection / budget)

FINAL SELECTION OF PRODUCT LINES

Therapeutic Classes Completed
Statins July 06Proton Pump Inhibitors July 06ACE Is (now being regionalised) Oct 06
In progress –ARBs Oct 06SSRIs Oct 06

Key Requirements
COMMUNICATION80 meetings with key stakeholdersInteractive sessions
OWNERSHIP – LOCALConsultantsGPs

Key Messages
1) Patient care is enhanced
2) Efficiencya) Reduced cost to achieve the same
quality of patient careb) Reimbursement of the efficiency to –
i. Pay for new expensive treatment modalitiesii. Pay for primary care infrastructure, eg CPN

DEVELOPMENT

Development
1) Regional Steering Group

Regional Steering GroupChair - Consultant Clinical
PharmacologistConsultantsGPsHospital PharmacistsCommunity PharmacistsPrescribing AdvisorsABPI representation
Decide and oversee the work programme

Development
1) Regional Steering Group2) Regional Pharmaceutical
Procurement Unit

Regional Pharmaceutical Procurement Unit
Regional Procurement Pharmacist
2.5 wte Pharmacists
1 wte Clerical Officer
Requiring a Pharmacoeconomic Pharmacist
Linked to SGCE and PCEG
Contracting by RSS

Development
1) Regional Steering Group2) Regional Pharmaceutical Procurement
Unit3) Reorganisation of hospital contracts

Reorganisation of the Hospital Contracts
Coverage of all main therapeutic classes
Rolling 3-year contacts rather than one massive contract
Regional generic generics contract

Development
1) Regional Steering Group2) Regional Pharmaceutical Procurement Unit3) Reorganisation of hospital contracts4) Primary Care aspects

Primary Care Aspects
Linkage to quality and outcomes framework for new GMS contractLinkage to regional prescribing incentive schemeLinkage to new community pharmacy contract based on qualityLinkage to community pharmacy “Managing Your Medicines scheme” (IMM)

Development
1) Regional Steering Group2) Regional Pharmaceutical Procurement
Unit3) Reorganisation of hospital contracts4) Primary Care aspects5) Guidance

GuidanceAssessment relative to indication, egACEIs in hypertension
in heart failurein diabetic patients
Regional guidanceNICE? SMC

OTHER APPLICATIONS

DRESSINGS
Surgical dressings
Wound management products Aug 06
FOR BOTH PRIMARY AND SECONDARY CARE

BENEFITSOptimised patient careFully integrated product use in both sectorsSelection of product on safety and therapeutic efficiency as the prime determinantQuality at best value for the serviceRobust, transparent, defensible system of selectionWeb-based formulary – evidence basedDynamic with regular updatesCompliance with EU legislation

Matrices created for the different categories
HydrocolloidsSilver dressings
Logistics assessment

Pharmaceutical Clinical Technology
1) Medical and surgical disposables• Significant involvement of pharmacy
in their management• Improved management and cost
control
2) Point of Care Testing• Managed and controlled by pharmacy
via the regional contracting process

Pharmaceutical Clinical Technology
a) Medical and surgical disposableseg sutures Oct 06
endosurgery Jan 07endoscopy Jan 07
b) Point of Care Testing- urine testing Oct 06- blood glucose Dec 06- misc, eg troponin, BNP,
drugs of abuse screen Mar 07

Pharmaceutical Services Improvement Programme (PSIP)
Repeat dispensing
Minor ailments
28-day dispensing
Generic substitution
Medicines governance
Integrated medicines management
Therapeutic tendering
Pharmaceutical Clinical Technology





























