-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
-
S A H e a r t Ea r l y Re p e r f u s i o n P i l o t P ro j e c
t
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
• Research demonstrates that the optimal time to treatment for
an acute myocardial infarction (AMI) is
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Cardiovascular disease
Still the biggest ‘killer’ in the world
Acute ST elevation Myocardial Infarction
(STEMI) represents c.40% of all MI
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Symptoms of a heart attack Most typical
discomfort/pain zones
Other possible discomfort/pain
zones
There may be a rapid, weak pulse
Sharp stabbing pain in the left
side of the chest is usually NOT
heart pain
This may feel like indigestion, spread to shoulders, arms,
neck or jaw and/or last for more than
15 minutes. It may stop or weaken and then return Sweating,
sickness,
faintness or shortness of
breath may be experienced
http://www.heartfoundation.co.za/how-your-heart-works/symptoms-heart-attack
(accessed on 7 Feb 2013
Heavy pressure, tightness, crushing
pain or unusual discomfort in the
centre of the chest
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Ischemic Symptoms - Explained
• Discomfort or Pain in the Center of the Chest that lasts
>20 minutes (MI), or that goes away and comes back (Crescendo
Angina/UAP).
• Feels like an Uncomfortable Pressure, Squeezing or Burning. It
often spreads to the neck/jaw, arms or the abdomen and is not
respiratory dependant. Chest pain may also include back pain.
• Sublingual (oral) Nitroglycerine has minimal or no effect.
• Common accompanying symptoms are Nausea, Dizziness, Vomiting,
Cold sweat, Anxiety and possibly Dyspnea.
Symptoms in women are often different than in men. Women are
more likely to experience nausea, dizziness, and anxiety.
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
STEMI: ECG Diagnosis
* lack of blood
supply leads to
permanent
myocardial
infarction
Q* vs.
Non-Q MI STEMI
vs. NSTE-ACSI
Clot within the main lumen of the coronary artery
Ruptured plaque with hemorrhage
Adapted from J Davies (pathological specimen)
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
STEMI ECG
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
• Need to open the blocked vessel as soon as possible either via
thrombolysis or PCI
• PPCI recommended over fibrinolysis if performed by an
experienced team within 120 minutes of first medical contact
• Longer PCI-delay (DB – DN time) are associated with higher
mortality rates and reduced PPCI survival advantage (Pinto D S et
al. Circulation 2006;114:2019-2025)
• Often not a 24 hour service!
Reperfusion Therapy Options
Stone, Circulation, 2008
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
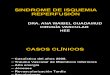
Relationship Between Mortality Reduction and Extent of
Salvage
Time to treatment is critical Opening the IRA (PCI >
lysis)
Mortality reduction (%)
Modifying factors
•Collaterals •Ischemic preconditioning •MVO2 •Stuttering
infarction
Extent of salvage (% of area at risk)
Gersh: JAMA, 2005
Hours
%
20
40
60
80
100
1 3 6 12 24
Impact of time delay - Time is critical!
0
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
-
TIME TO REPERFUSION IS
CRITICAL
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
• Saved myocardium
• Reduction in morbidity
• Improved quality of life
• Reduction in downstream healthcare costs
Benefits of Early Reperfusion
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
• Reperfuse now! • Immediate PCI (< 120 mins)
OR
• Thrombolysis (> 120 mins)
• Reperfuse how? • Ship immediately to closest cathlab (< 120
mins)
OR
• Drip and then ship to closest cathlab (> 120 mins)
• Reperfuse where? • Closest cathlab location
What Do I Do?
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
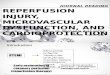
Reperfusion choice depends on time to treatment
Multivariable analysis estimating the treatment effect of
reperfusion
therapy with PCI or fibrinolysis based on increasing
PCI-related
delay.
Pinto D S et al. Circulation 2006;114:2019-2025
N= 192 509 pts from 645 National Registry of Myocardial
Infarction Hospitals
If < 120 min PPCI
If > 120 min Thrombolysis MUST BE
followed by PCI
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
• Reperfuse now! • Immediate PCI (< 120 mins)
OR
• Thrombolysis (> 120 mins)
• Reperfuse how? • Ship immediately to closest cathlab (< 120
mins)
OR
• Drip and then ship to closest cathlab (> 120 mins)
• Reperfuse where? • Closest cathlab location
What Do I Do?
1st
1st
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
What is PPCI?
• PPCI is a mechanical technique used to open up blocked
coronary blood vessels that may or may not use stent(s) or other
devices
• Procedure is performed under x-ray guidance and requires
specialised skills and team-members
• More effective in reopening occluded arteries than
thrombolysis
• For both AHA and ESC Primary PCI is a class 1A indication for
Acute STEMI if it can be performed within 120min of first medical
contact (90 minutes if presenting early with a large infarct and
low risk of bleeding complications)
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Benefits of PPCI vs Thrombolysis
• Lower in-hospital mortality
• Less complications
• Fewer ambulance journeys
• Reduced unscheduled revascularisation
• Shorter length of stay
• More cost-effective for the healthcare economy
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Immediate PCI ( < 120 mins) Anti-Platelet Agents and
Fibrinolytic Therapy
• How and what do I administer (primary care)?
• Starting dose Aspirin 150-500 mg orally or 250mg IV
• Clopidogrel
• GP IIb/IIIa inhibitors such as Aggrastat (tirofiban) or
Integrilin (eptifibatide) should not be used
• Ship the patient to the nearest cathlab
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
A Patient With The Following Criteria Is Suitable For Direct
Transfer To A PPCI Cathlab
History of symptoms compatible with MI (
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Two Different STEMI Subgroups Undergoing Ppci After Pre-hospital
Resuscitation
Initial neurological presentation in 135 consecutive patients
with resuscitated cardiac arrest and STEMI
(2000-2004)
Conscious on admission
49 (36%)
Mortality 0%
Comatose on admission
86 (64%)
Mortality 43%
Gorjup et al. Resuscitation 2007;72:379-85.
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Where Is My Nearest Cathlab In Pretoria & Centurion?
Dr George Mukhari
Montana
Eugene Marais
Steve Biko Academic
Pretoria Heart
Zuid Afrikaans 1 Military Wilgers
Unitas
Nelspruit Mediclinic
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
• Reperfuse now! • Immediate PCI (< 120 mins)
OR
• Thrombolysis (> 120 mins)
• Reperfuse how? • Ship immediately to closest cathlab (< 120
mins)
OR
• Drip and then ship to closest cathlab (> 120 mins)
• Reperfuse where? • Closest cathlab location
What Do I Do?
2nd
2nd
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Does Early Thrombolytic Therapy Affect Rate Of Survival?
1.2
8.7
0
5
10
15
20
%
Mortality
Time to treatment
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
But What About The Risks Associated With Thrombolysis?
Thrombolysis is highly effective but there is 1% chance of
intracranial bleeding
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Thrombolysis Absolute Contraindications • Previous intracranial
haemorrhage or stroke of unknown origin at any time
• Ischaemic stroke in the preceding 6 months
• Central nervous system damage or neoplasms or atrioventricular
malformation
• Recent major trauma/surgery/head injury (within the preceding
3 weeks)
• Gastrointestinal bleeding within the past month
• Known bleeding disorder (excluding menses)
• Aortic dissection
• Non-compressible punctures in the past 24 h (e.g. liver
biopsy, lumbar puncture)
ESC Guidelines for the management of AMI in patients presenting
with ST segment elevation, European Heart Journal (2012), 33: 2569
- 2619
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Tenectaplase Has A Lower Rate Of Non Cerebral Bleeding And Easy
Administration
Tenectaplase
Tenectaplase
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
How Does Success Of Thrombolysis Affect Survival Rates?
Blocked vessel has been opened
Blocked vessel has only been partially opened
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
So Do I Wait To Check On The Success Of Thrombolysis?
Routine transfer and PCI within 6 hours
after lysis
OR
Transfer after 24 hours and elective
cath within 2 weeks or urgent transfer
for failed lysis (rescue PCI)
(Cantor et al., STREAM study, NEJM 2009)
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
STREAM Study Conclusions
• Fibrinolysis with bolus tenecteplase and contemporary
antithrombotic therapy given before transport to a PCI-capable
hospital: • Circumvents the need for urgent PCI in about two thirds
of
fibrinolytic treated STEMI patients
• Is associated with small increased risk of intracranial
bleeding
• Is as effective as PPCI in STEMI patients within 3 hours
symptom onset who cannot undergo PCI within 1 hour of first medical
contact
(Cantor et al., STREAM study, NEJM 2009)
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
• Reperfuse now! • Immediate PCI (< 120 mins)
OR
• Thrombolysis (> 120 mins)
• Reperfuse how? • Ship immediately to closest cathlab (< 120
mins)
OR
• Drip and then ship to closest cathlab (> 120 mins)
• Reperfuse where? • Closest cathlab location
What Do I Do?
2nd
2nd
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Thrombolysis – Common Agents (Delayed PCI >120mins)
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Thrombolysis (Delayed PCI >120mins)
• What do I administer? – European Society of Cardiology
recommends:
• Tenecteplase (fibrinolytic therapy) within 12h of symptom
onset if PCI cannot be performed within 120 mins of first medical
contact
PLUS
• Oral/IV aspirin must be administered
• Clopidogrel
• Ship the patient to nearest cathlab ESC Guidelines for the
management of AMI in patients presenting with ST
segment elevation, European Heart Journal (2012), 33: 2569 -
2619
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Where Is My Nearest Cathlab In Pretoria & Centurion?
Dr George Mukhari
Montana
Eugene Marais
Steve Biko Academic
Pretoria Heart
Zuid Afrikaans 1 Military Wilgers
Unitas
Nelspruit Mediclinic
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Impact of PCI with Fibrinolytic Therapy
TIMI Flow Rates Associated With Thrombolysis Following PCI
(confirms the value of thrombolysis)
(Cantor et al., STREAM study, NEJM 2009)
Blocked vessel has been opened
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Impact of PCI with Fibrinolytic Therapy
White, H.D. Circulation (2008): 118: 219-222
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Treatment Choice Conclusions • During first 2-3 hours after
symptom-onset, time to
treatment is critical
• After 3 hours, PPCI is preferred if it can be done within 2
hours of first medical contact.
• If not, then a pharmacoinvasive strategy with thrombolysis
followed by immediate transfer for PCI within next 3-24 hours may
improve myocardial salvage and survival.
• Immediate or ‘rescue’ PCI for failed thrombolysis
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Summary of Common Challenges • Not obtaining a history of
cardiac chest pain • Not performing immediate ECG on all patients
triaged as
possible cardiac chest pain • Not performing serial ECG when
appropriate • Repeated ECGs when diagnosis is clear • Lack of
knowledge regarding closest cathlab • Administering drugs before
activating EMS • Rotating and temporary staff unaware of protocol •
Thrombolytics not being carried on board ambulance • Lack of beds
available at hospital with a cathlab (call to
check!) • Possible medical aid authorisation delays
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
What Can You Do To Help? • Know where all your local cathlabs
are • Find out who the cardiologists are and their contact
numbers • If you think the patient might have had an MI,
perform
an ECG • Take a picture of the ECG with your mobile phone
and
send it ahead to the cardiologist • Carry and administer
thrombolysis according to the
guidelines • Ask questions if you are unsure • Do not delay
getting your patient to a cathlab
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Your Nearest Cardiologist…
Hospital Name Contact Number
1 Military Dr Mpe 012 341 1894
Dr George Mukhari Dr Mutati 012 317 6924
Eugene Marais Dr Dannheimer 012 335 4070
Dr Benson 012 335 9703
Montana Dr Bushidi 012 523 3114
Dr Zeelie 012 548 4528
Nelspruit Mediclinic Dr Fourie 013 745 8167
Dr Maree 013 745 7781
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Your Nearest Cardiologist…
Hospital Name Contact Number
Pretoria Heart
Dr Adeyemo 012 440 0354
Dr Bushidi 012 341 2713
Dr Makotoko 012 341 1894
Dr Mpe 012 341 1894
Dr Milela 012 341 5983
Dr Motaung 012 440 0286
Dr van der Spuy 012 341 4741
Steve Biko Academic Prof Sarkin 012 354 2277
Unitas
Dr Badenhorst 012 664 5784
Dr Blomerus 012 664 5784
Dr Jacobs 012 664 7715
Dr Vorster 012 664 4682
Dr Ebrahim 012 664 6118
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Your Nearest Cardiologist…
Hospital Name Contact Number
Wilgers
Dr Bennett 012 807 1287
Dr Guerra 012 807 1287
Dr Mwangi 012 807 2452
Dr Snyders 012 807 6186
Dr Swanepoel 012 807 1287
Zuid Afrikaans
Dr da Silva 012 344 4854
Dr Benson 012 343 8246
Dr Lester 012 343 6038
Dr Osrin 012 343 8525
Dr van Niekerk 012 343 0970
Dr van Wyk 012 343 2500
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Where Is My Nearest Cathlab In Pretoria & Centurion?
Dr George Mukhari
Montana
Eugene Marais
Steve Biko Academic
Pretoria Heart
Zuid Afrikaans 1 Military Wilgers
Unitas
Nelspruit Mediclinic
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
Questions?
Thank you!
-
S A H E A R T E A R L Y R E P E R F U S I O N P I L O T P R O J
E C T
This project was made possible by an educational grant by the
following companies