Embed Size (px)
Citation preview

SAAD DIGEST
JOURNAL OF THESOCIETY FOR THE ADVANCEMENTOF ANAESTHESIA IN DENTISTRY
VOLUME 34 | 2018
Dementia | Intranasal Midazolam | Clinical Hypnotherapy
Patient Information Audit

TACRINE
SAAD DIGEST | VOL.34 | 2018
STORY BEHIND THE COVER
The D word, Dementia, is a diagnosis that none of us want tohear, but it’s on the rise and currently there are 850k peoplewith dementia in the UK. By 2025 there will be 1m, and therecould be more than 2m by 2050.1 It is the leading cause of deathin UK women: 13.7% of deaths ~ approximately 40K per year. Incontrast with invasive breast cancer there are 53K new cases ofcancer each year but, because there are effective treatmentsthere are 11.4K deaths (survival rate is 78% and 27% of casescould have been prevented).2 Two thirds of dementia patientslive in the community and currently, there are 670K carers. Sowhat can be done? How can we treat it and prevent it?
Given that there are different types of dementia (Alzheimer’s isthe most common type), there will be different causes. Sadly weknow very little about any of them and there are no effectivetreatments. On the assumption that Alzheimer’s sufferers have adeficiency of cortical acetyl choline, a potential treatment is acentrally acting anticholinesterase drug, and Tacrine was thefirst. Discovered by Adrien Albert in Sydney, and then patentedby William Koopmans Summers in Los Angeles in 1984, the drugoffered hope. The FDA approved its use in 1993 under the tradename of Cognex but by 2013 it was withdrawn because it washepatotoxic, and new drugs promised to have a better safetyprofile.
Today there are two types of drugs available for dementia. Noneof them cure the disease or slow the inevitable deterioration,but they may help by temporarily by reducing the symptoms.Three anticholinesterases are available (Donepezil, Rivastigmineand Galantamine) and a glutamate antagonist (Memantine).These may help with reduced anxiety and improvements inmotivation, memory, concentration and daily living but theunpleasant side effects are typical of cholinergic stimulationand include diarrhoea, nausea, vomiting, abdominal discomfort,dizziness, headache, anxiety, blurred vision, dry mouth and
insomnia. Memantine may help reduce agitation or aggressivebehaviour but can cause dizziness, headaches, tiredness,increased blood pressure and constipation. Other drugs thatelderly patients often take include anti-depressants and anti-pyschotics and both can cause a dry mouth which is a factor inthe build-up of dental plaque.3
Anaesthesia (or sedation) should be used with great care inpatients with dementia. Firstly, patients are likely to have pre-existing diseases (e.g. heart failure, hypertension, diabetes)which incur a burden of professional care and attention thatcalls for special healthcare staff and facilities. Secondly, there is apossibility that anaesthesia itself causes a loss of cerebralfunction.4 Whereas the evidence in humans does not supportthis view, it is possible that anaesthesia causes deterioration insome patients. Yet dental decay is likely to be common indementia patients5 and it would be a reasonable considerationin a confused irritable patient that they could have dental painwhich, if relieved, could calm them. For these people, a dentistcould make a big difference.6
Mike Sury
References(1) https://www.alzheimers.org.uk/site/scripts/documents_info.php?
documentID=341
(2) http://www.cancerresearchuk.org/health-professional/cancer-
statistics/statistics-by-cancer-type/breast-cancer
(3) https://www.alzheimers.org.uk/site/scripts/documents_info.php?
documentID=138
(4) https://www.scientificamerican.com/article/can-general-anesthesia-
trigger-dementia/
(5) https://www.bda.org/dentists/education/sgh/Documents/Dental%20
problems%20and%20their%20management%20in%20patients%20with
%20dementia.pdf
(6) http://www.oralhealthgroup.com/features/oral-health-and-dementia-
obstacles-assessments-and-management-of-patients-with-dementia/

CONTENTS
1SAAD DIGEST | VOL.34 | 2018
SAAD Trustees:
Officers
President: Francis Collier BDS MSc DipDSed (Lond)Hon. Secretary: Sadie Hughes BDS MFDS RCPS(Glas) MScAssistant Hon. Secretary: Manni Deol BDS MJDF PGCMedEd DipDSedHon. Treasurer & President-elect: Stephen Jones BDS MSc DDPHRCSDip SedAssistant Hon. Treasurer: Kellie Downie BDS MFDS RCPS (Glas)DipConSedCourse Director: David Craig BA BDS MMedSci FDS RCS(Ed)Assistant Course Director: Carole Boyle BDS FDS RCSEng MMedSciMSND RCSEd FDS RCSEd FDTFEd Communications Secretary: Paul Howlett BDS MFDS DipConSed Editor: Nigel Robb TD PhD BDS FDS RCS(Ed) FDS(Rest Dent) FDSRCPS FDTF FHEA
Members
Leah Adams BDS MSc ConSedChristopher Holden BDS LDSRCS (Eng) DGDP(UK)Yi Kwan Loo BDS MFDS RCS (Edin) DipConSed AFHEADavid Pearson BDS MFDS M Oral Surg PG Cert Leadership Shilpa Shah BDS MJDF RcS (Eng) MSc (Fixed & Remov Pros)Zahra Shehabi BDS MFDS MSc(Sed Spec Care) MSCD MSc(Management)
The SAAD Digest is published by the Society for the Advancementof Anaesthesia in Dentistry. The SAAD Newsletter is publishedelectronically by the Society in April and November.
Editorial Board:
Fareed Ahmad BDS LDSRCS (Eng)Jennifer Hare DHealthPsy CPsychol AFBPSDev Mahtani BSc MBChB FCARCSIChristopher Mercer BDS FDSRCS (Eng) PhD FHEANigel Robb (Editor) TD PhD BDS FDS RCS(Ed) FDS(Rest Dent) FDSRCPS FDTF FHEAFiona Trimingham BSc(Hons) MA MRSC CT(ABRSM)Rosemary Whatling BSc BDS FDSRCS(Eng)(Paed Dent) MPaed DentRCS (Eng) MClin Dent (Paed Dent) MFDSRCS (Eng)
Original articles and correspondence should be addressed to:
Fiona TriminghamSAAD Editorial Board21 Portland Place, London W1B 1PYTel: 01302 846149 Email: [email protected]
Membership: £40 (UK) and £43 (international) per annum andincludes the SAAD Digest and SAAD Newsletters, which arepublished on behalf of SAAD, 21 Portland Place, London W1B 1PY.
The opinions expressed in this and previous SAAD Digests andNewsletters are those of the authors and are not necessarily those ofthe Editorial Board nor of the SAAD Board of Trustees.
ISSN 0049-1160
2 Editorial
3 Refereed Papers
3 What’s new in... Dementia and Dentistry
8 The Use of Intranasal Midazolam in aSpecial Care Dentistry Department ina Hospital Setting
13 Can Clinical Hypnotherapy Be Used as an Adjunct or an Alternative toConscious Sedation in Dentistry?
19 Audit of Written Patient Information for Conscious Sedation across aCommunity Dental Service
24 Case Study
26 Opinion
29 Journal Scan
36 SAAD Essay Prizes
51 Symposium 2017
64 Profiles
69 Training
74 Forum
75 Electronic Record Keeping
78 SAAD Courses
81 Essay Prize Details
82 SAAD Supplies
83 SAAD Website
84 Product News
89 Guidelines for Authors
90 CPD
92 Diary Scan

2 SAAD DIGEST | VOL.34 | 2018
EDITORIALWelcome to the 2018 issue ofSAAD Digest. The last year hasbeen another busy butproductive one for SAAD. TheDiamond Jubilee was markedwith a really special opening toour Annual Symposium, with apiper playing the Presidentinto the Hall followed by thePresidential Diamond JubileeProclamation, the text of whichcan be found in the Autumn2017 Newsletter.
Ian Brett and Chris Holden dida double act providing aninteresting and informativepersonal view of the History ofour Society. Many of the issues
we have faced throughout our history are the same as thosewe face today, although as a result of the IACSD and AoMRCpublications, I feel that there is now a better understandingbetween anaesthetists and dentists on the way ahead forsedation. Whilst it is always good to learn the lessons of historyto avoid repeating previous mistakes, it is also important tolook forwards rather than back. There is still a huge need forsedation, as there is no sign of a reduction in the number ofpatients who are anxious or phobic of dental care. TheSociety’s motto of “Abolish Pain to Conquer Fear” appears toosimplistic, as despite advances in pain control, patients with noexperience of dental care are still presenting as “too anxious tohave treatment under local anaesthesia”.
In June 2017, a commissioning guide for sedation in primarydental care in England was published by NHS England. Thisdocument was so heavily based on the IACSD 2015 standardsthat it has now laid to rest any further debate about whetherthese standards should be implemented. It is written forcommissioners, not providers, and is available on the NHSEngland website.1 Once again members of SAAD wereinvolved in advising on the content. The group included twoSAAD Trustees (David Craig and Nigel Robb) and a member ofSAAD Course Faculty (Leah Adams).
The SAAD Courses for new starters in sedation for bothDentists and Dental Nurses have now run three times.Enrolment is increasing and those who have successfullycompleted training are now moving to provide sedation intheir practices. More details can be found on page 72.
This issue of Digest again covers a wide range of articles,which I trust will mean there is something of interest to allmembers. Our “What’s New in” series article is on dementia.This is particularly timely as, in the autumn of last year, theFaculty of General Dental Practitioners published “Dementia-friendly Dentistry: Good Practice Guidelines”.2 Themanagement of patients with dementia is going to become anincreasing part of our practising lives, with all the challengesthat it entails.
Our other refereed papers include two audits of sedationservices. Given the increasing emphasis on audit, I hope thatthese papers may give members ideas that they can use toaudit their own practices.
In a departure from our normal practice, the essay prizes lastyear had a set title rather than free choice. The title set was“Anxiety Management and Sedation in Dentistry; the next 60years?”. We are publishing the three winning entries in theDental Nurse’s, Dental Student’s and Drummond Jacksonprizes. The articles provide different views on the future. Whilstit is unusual to have three papers with the same title in ajournal, the differences in approach make an interesting read.
Our online CPD continues to attract members and non-members to participate and collect their CPD hours. The CPDwill be available again this year, and I would encourage readersto take advantage of the opportunity to use these towards therequired 12 hours in every 5-year cycle.
In last year’s Digest, we included an article by Joe Hulin whosePhD was funded by SAAD. Another paper based on his PhDwas published this year. It is “Development of a decision aid forchildren faced with the decision to undergo dental treatmentwith sedation or general anaesthesia”.3 A review of the paper isincluded within the Journal Scan. We had hoped to be able toreprint the entire article for members who do not subscribe tothe journal, but were unable to reach a suitable arrangementwith the publishers.
I would like to take this opportunity to thank all the membersof the Editorial Board for their hard work leading to theproduction of the Digest. The Digest would not appear but fordedicated individuals undertaking the reading, reviewing,proof-reading etc voluntarily and usually in their own time.One of the strengths of SAAD is that it operates as it is run by agroup of family and friends – long may it last.
I would also like to thank all who have submitted papers to theDigest for consideration for publication, as withoutsubmissions we would have nothing to publish. We welcomesubmissions from members and non-members alike covering awide range of subjects under the theme of pain and anxietycontrol in dentistry.
We have welcomed Dr Dev Mahtani to the Board this year. Devis a Consultant Anaesthetist at Guy's and St Thomas’, where hehas a regular involvement with anaesthesia and sedation fordental patients. We are very pleased to have his anaestheticinput, especially his contribution to the Journal Scan coveringjournals that members of the dental profession would notnormally read.
I hope you and enjoy this year’s Digest and that it enhancesyour knowledge.
Nigel Robb
1. https://www.england.nhs.uk/publication/commissioning-dental-services-service-standards-for-conscious-sedation-in-a-primary-care-setting/
2. https://www.fgdp.org.uk/publication/dementia-friendly-dentistry
3. Hulin J, Baker S R, Marshman Z et al Int J Paed Dent 2017;27: 344-355

3SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
AbstractCurrently it is thought that over 850,000 people in the UnitedKingdom (UK) are living with dementia, with numbers set to rise toover one million by 2025. It is known that dementia cancompromise an individual’s oral health, particularly as the diseaseprogresses. Dental practitioners can have an important role to playin reducing the impact of dementia on oral health. This articlelooks at the oral care problems dental teams might encounterwhen delivering care to patients with dementia, and whatevidence is available on how dental care professionals can providethe highest possible level of care for this patient group.
IntroductionDementia is a largely irreversible clinical syndrome in which thereis deterioration in memory, thinking, behaviour and the ability toperform everyday activities.1
The 2014 Dementia UK report2 revealed that 1.3% of thepopulation of the UK are living with the disease. The prevalence ofdementia is set to rise - it is estimated there will be 2 millionpeople living with dementia in the UK by the year 2051. The reportalso demonstrated that the impact of dementia is widespread -with there being physical, psychological, social, and economicalimpact on carers, families and society. At present the financialburden of dementia to the wider society in the UK is thought to be£26.3 billion - funded through the NHS, private and public socialcare, and the contribution of unpaid carers.
Within the UK, the Department of Health’s ‘Challenge on Dementia2020’3 guidance puts the delivery of high quality health and careas one of its core commitments to this patient group. With a shifttowards an aging population and a greater portion of patientsmaintaining their teeth for longer, an understanding in theprevention of oral disease, and the provision and timing of dentalcare for patients with dementia can be assumed to be essential forfuture dental practice. The Faculty of General Dental Practitioners’(FGDP) comprehensive guidance on Dementia-Friendly Dentistry4
demonstrates the commitment of our profession to this patient
group. It ensures that dental care professionals have theknowledge and skills they need to provide high quality dental carefor individuals with dementia. This article aims to provide a briefoverview on the subject of dementia and its impact on thedelivery of general dental care, and to review what recent evidenceis available regarding the safety and efficacy of providing sedationand general anaesthesia for people with dementia.
Signs and SymptomsEarly signs of dementia may not be particularly obvious, and mayinclude forgetfulness or losing track of time. As the diseaseprogresses symptoms may become clearer - and can includememory loss, mood or personality changes and problems withreasoning, communication and geographical orientation.1
Risk factorsThe leading risk factor for dementia is age. Above the age of 65years, a person's risk of developing Alzheimer's disease or vasculardementia doubles roughly every 5 years. It is estimated thatdementia affects one in 14 people over 65 years old and one in sixover 80 years old. Women are twice more likely to be affected thanmen.5 The National Institute of Health and Care Excellence (NICE)6
also include a number of non-age-related factors thought toincrease an individual’s risk. These include certain lifestyle factors-such as smoking, excessive alcohol consumption, obesity, diabetes,hypertension and raised cholesterol levels, and genetic factors -such as mutations and Down’s syndrome.
DiagnosisDementia can be classified as reversible, that is, dementia that issecondary to a potentially treatable condition, or irreversible. Thisarticle will primarily focus on irreversible dementias. The four mainsubtypes of which are Alzheimer’s disease; vascular dementias;frontotemporal dementias; and dementia with Lewybodies/Parkinson’s disease.7
What’s new in... Dementia and Dentistry
Claire Sims BDS MFDS RCS (Edin) DIP D SED (KCL)Specialist in Special Care DentistryBristol Dental Hospital, Lower Maudlin Street, Bristol
Jessica Mann BDS Specialty Registrar in Special Care DentistryBristol Dental Hospital, Lower Maudlin Street, Bristol
Mysa Al-Fozan BDS, MFDS RCS (Edin), MSc in Special Care Dentistry (UCL) Associate DentistBristol Dental Hospital, Lower Maudlin Street, Bristol
Tony Brooke BDS MFDSRCS(Eng) MSNDRCS(Ed) FDSRCS(Ed)Consultant in Special Care Dentistry Bristol Dental Hospital, Lower Maudlin Street, Bristol
Corresponding Author: [email protected]

4 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERIf a diagnosis of dementia is suspected, a physician will arrange fora cognitive assessment which should include an examination ofattention and concentration, orientation, short and long-termmemory, praxis, language and executive function. Examplesinclude the Mini Mental State Examination (MMSE) and the 6-ItemCognitive Impairment Test (6-CIT). Imaging may be used to excludeother cerebral pathologies.8
Dental care professionals are often in a position where they see anindividual regularly for ongoing care. It has, therefore, beenrecognised that general dental practitioners may have a role inrecognising early changes in an individual’s behaviour.9 If signs orsymptoms of dementia are seen, a referral to an appropriatemedical professional should be carried out, if it has not yet takenplace.
TreatmentTreatment is broadly split into pharmacological and non-pharmacological interventions. The main non-pharmacologicalintervention is cognitive stimulation therapy (CST) provided bytrained individuals. CST includes group activities such as recallingand discussing past events, or revisiting skills such as usingmoney.10
The main pharmacological interventions are theacetylcholinesterase inhibitors Donepezil, Galantamine andRivastigmine. These are used to treat the cognitive symptoms ofmemory and learning deficits in mild to moderate Alzheimer’sdisease and other dementias. The drug Memantine is used inmoderate to severe Alzheimer’s disease or in those individuals withan intolerance or contraindication to acetylcholinesterases.11
Newer techniques, such as deep brain stimulation, are currentlybeing trialled with promising results.12
Dementia and Oral HealthIt has long been recognised that oral health is an important part ofan individual’s general health. Poor oral health can impact ongeneral health and wellbeing, diet and nutrition, behaviour andcognitive function.13 There are no known oral manifestations ofdementia, however, several studies have shown a higherprevalence of oral disease, such as periodontal disease, caries andxerostomia, in this cohort of patients.14,15
Impact of dementia on dentistry
AccessPatients with dementia may have difficulty accessing dentalservices. Short-term memory loss can affect the individual’s ability to organise and arrange appointments. Considerationshould be given to liaising with family members and carers,especially as the disease progresses, as they may play a role infacilitating access to dental care.16 Patients may benefit fromreminders of appointments in the form of a phone call or a textmessage.
The timing of appointments can also be important. Discussionwith the patient and their supporting carers may reveal the timesof day a patient is more or less co-operative, or certain activities or
mealtimes where disrupting the routine should be avoided.Compliance may be better for short periods, so schedulingmultiple appointments may be preferred over a single long visit.
Some patients may be frail, have issues with mobility or use awheelchair. Services should be wheelchair accessible and considerproviding care in the wheelchair if the patient has difficultytransferring. Wheelchair recliners can improve the dental carepractitioner’s access for examinations and treatment. In caseswhere transfer is required, aids can be used, or a hoist, providingthe dental team is appropriately trained.
In patients who have been regular attenders to a dental serviceand are the early stages of dementia, maintaining continuity withtheir regular dental team may lessen confusion and enhance co-operation for dental care. However, these patients may requirelonger appointments and treatment may be more timeconsuming. At the present time there is no consideration given tothis issue within the NHS remuneration system for general dentalpractitioners17 hence many patients with dementia are being seenwithin the Community Dental Service, which is commissioned byNHS England in line with local oral health needs assessments, andprovides care for especially vulnerable groups.18
In 2015 the Department of Health released guidance for providingdementia friendly health and social care environments.19 Many ofthese principles can be applied to dental practices - such asavoiding busy and crowded environments, patterned walls andflooring, unnecessary clutter and noise from televisions and radios.In some cases, care may need to be considered on a domiciliarybasis - this may lessen confusion and enhance co-operation as it isprovided in familiar surroundings.
CommunicationA patient with dementia may have difficulty communicating thatthey have a dental problem or that they are in pain. For example,they may have trouble finding the right word, or will repeat wordsor phrases. They may also have other sensory impairments, such ashearing problems, which may hinder communication further. Theymay have slurred or muffled speech which may be challenging forthe clinician to understand. Patients may become frustrated if theycannot communicate their problem, and may exhibit unusualbehaviour as they are trying to communicate what they no longercan verbally.20 Perception of pain can also be altered in patientswith dementia - some studies have shown that patients withAlzheimer’s dementia have an unchanged pain threshold but ahigher pain tolerance.21 These aspects combined can mean it isdifficult to ascertain an accurate pain history. Changes in eatingand drinking patterns (such as avoidance of hot, cold or hard food),sleeping patterns or noticeable changes in behaviour (such asincreased agitation or self-injurious behaviour) can all beindications of dental pain, therefore potential dental pathologyshould be investigated and excluded if these signs are exhibited.
ConsentDementia can affect the functioning of an individual’s mind orbrain, and therefore may affect their capacity to consent to dentalexamination and a treatment plan. It should be assumed that apatient has capacity unless assessed otherwise. A dental careprofessional should be able to assess an individual’s capacity using

5SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERsection 3.1 of the Mental Capacity Act.22 This act clarifies that forsomeone to have the capacity to consent they must be able tounderstand the information including the risks and benefits of alloptions discussed, as well as the consequences of no intervention.They must be also able to retain the information, weigh up therisks and benefits of each option and communicate their decision.If an individual is assessed to lack capacity to consent for a specificdecision, a best interest decision should be made following theprinciples of this act. It is best practice to involve the patients caregivers and family members in the best interest discussion. If thepatient does not have any close relatives or unpaid carers then areferral should be made to appoint an Independent MentalCapacity Advocate (IMCA). Where the treatment proposed is radicalor irreversible, there should be documented agreement from twoindependent health professionals that the treatment is in the bestinterests of the patient.
EducationSome individuals with dementia may be able to provide their ownoral care with minimal support or intervention. Others need moresupport or are dependent on carers for their routine oral care. It isimportant that the level of support required is assessed, and thatindividuals and their carers receive targeted oral hygiene and dietadvice in an attempt to minimise the risk of intervention in thefuture. NICE guidance on ‘Improving Oral Health in Care Homes’specifically mentions the need for care staff to provide theirresidents with daily support to meet their mouth care needs.Studies have shown effective carer education improves the oralhealth and denture hygiene of individuals with dementia.23, 24, 25
Carers in these studies were taught feasible tooth brushingtechniques, handling of interdental brushes and mouth rinses. A randomised control trial25 looking at comparing the efficacy ofelectric compared to manual toothbrushes in a nursing homeshowed that both were effective in reducing plaque scores.Interestingly, it noted that electric toothbrushes may beparticularly effective for nursing-home residents with cognitiveimpairment, but required a period of habituation. Alternatively,the use of a ‘Superbrush’ or Collis Curve, with the facility to brushthree surfaces at one time, may expedite effective oral hygiene inindividuals who struggle to tolerate oral care.
Surgery It is beneficial for an individual to see a dentist soon after adiagnosis of dementia, so that appropriate prevention, advice, andtreatment planning can be provided. The British DentalAssociation’s evidence summary ‘The Management of DentalProblems in Patients with Dementia’26 stated that treatmentplanning should have the following aims:
• To prevent further oral disease• Restore and maintain health • Make oral health care a normal part of the patient’s life• Treatment plans should be flexible, anticipating a decline in
patient health over time• Be realistic given the patient’s disorder and physical status.
Some patients with dementia will allow the provision of routinedental care without complaint or issue. Some, particularly as thedisease advances, may find it difficult to comply with care. In thesecases, The BDA document states that consideration should begiven to the patient’s level of independence, co-operation,
cognitive state and physical impairment; the presence of dentalproblems and whether they are symptomatic or asymptomatic andthe individual’s ability to give informed consent. The British Societyfor Disability and Oral Health guidelines ‘Principles of Interventionfor People Unable to Comply with Routine Dental Care’27 providescomprehensive advice on a proactive approach to oral care andtreatment provision, including aspects of safe holding and plannedphysical intervention.
Conscious Sedation and Dental TreatmentSome patients with dementia find it difficult to tolerate dentaltreatment due to communication difficulties or a lack of co-operation which can be exacerbated by anxiety or stress broughton by the dental environment. Sedation can help facilitate dentaltreatment by inducing anxiolysis and improving co-operation withcare, however, there are several aspects to consider before takingthis approach.
In terms of pharmacokinetics, with increasing age there is a relativeincrease in body fat, a decrease in total body water, and areduction in plasma proteins available for binding, which results inan increase in drug elimination.28 The elimination half-life ofmidazolam in adults over 60 years of age may be prolonged up tofour times that of a healthy adult.29 There is also alteration in phase1 metabolism resulting in a reduction in the P450 cytochromesystem.30 Midazolam is metabolised by at least three differentcytochrome P450 enzymes31 therefore the metabolism of the drugwill be reduced. Additionally, an increased incidence inpolypharmacy is seen in older adults. Some medications canimpact on the sedative action of midazolam. For example, theantihypertensive calcium channel blockers have been shown toenhance or prolong the effects of midazolam, whereas certain anti-epileptic drugs, for example carbamazepine, have been shown toreduce the effect.32
The 2015 Intercollegiate Advisory Committee for Sedation inDentistry (IACSD) guidelines33 defines conscious sedation as ‘atechnique in which the use of a drug or drugs produces a state ofdepression of the central nervous system enabling treatment to becarried out, but during which verbal contact with the patient ismaintained throughout the period of sedation. The drugs andtechniques used to provide conscious sedation for dentaltreatment should carry a margin of safety wide enough to renderloss of consciousness unlikely.’ Particular challenges in relation tothis definition when considering a patient with dementia may ariseif the individual has difficulty in communicating and therefore maynot normally respond to verbal communication or understandverbal prompts. In these cases a clinician has to rely on both theclinical monitoring, as well as observing the patient’s behaviour toassess when an appropriate level of sedation has been reached.
A review of the main biomedical literature databases of the terms‘sedation’, ‘dementia’ and ‘dental treatment’ produces eight articlespublished within the last ten years. Five of these were on the use ofintravenously administered midazolam or propofol34,35,36,37,38 one onthe use of oral midazolam39, one on the use of nitrous oxide as asedative agent40, and one was an update article on the provision ofdental care for patients with Huntington’s Disease.41 Of the fivepapers on Intravenously administered midazolam only two wereaccessible in English.34,36

6 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERSedation with nitrous oxide is a useful and non-invasive technique.No cannula is required and recovery is rapid. However, for it to besuccessful requires a level of co-operation and understanding fromthe patient, which is not always possible in patients with dementia.The single paper40 within the literature review which looked at theuse of nitrous oxide as a sedative agent highlighted that it is a verysafe way of sedating a medically complex patient, butacknowledged a degree of safe holding is likely needed to allowthe placement of the hood. It also advocated the use of a 50:50 mixof nitrous oxide and oxygen delivered by a mask covering both themouth and nose, referring to this process as an ‘induction’. Oncethe patient was adequately sedated the mask was removed andtreatment carried out. This appears to pertain to a much deeperlevel of sedation than is defined as conscious sedation by theIACSD guidelines.33
Sedation with a benzodiazepine, such as midazolam is a usefulalternative. Thought must be given to the method ofadministration, as not all patients will be co-operative withcannulation for intravenous sedation. In these situations, trans-mucosal techniques, such as oral or intra-nasal sedation, may bebeneficial. The included paper on the administration of oralmidazolam39, reviewed the success of orally administeredmidazolam in 61 adults with dementia to allow dental treatment,using the accepted guidance of 0.2 mg/kg body weight for thoseunder 65 years of age and 0.1-0.15 mg/kg body weight for thoseover 65 years of age. It found on average it took twenty minutesuntil sufficient sedation was observed, and for those who nosedation was seen at this stage an additional oral dose was given.90% of patients allowed the planned treatment to be completed.The reasons attributed to the 10% of failed treatment includedpoor acceptance or no observed effect of the drug. It concludedthat acceptance was not found to be dependent on dose, the typeof dental treatment performed or interacting drugs and that pooror no acceptance of treatment at the first sedation does not ruleout good co-operation at subsequent appointments.
There were no papers found in the literature review whichincluded the use of intranasal midazolam. However, a broadersearch of the method showed it to have a quicker onset andquicker recovery time for the patient compared to oraladministration,42 but side effects such as coughing and sneezingand nasal drug delivery have been related to epistaxis.43,44
The risk with trans-mucosal techniques is that with theadministration of a bolus dose there is a risk of over sedation. TheIACSD guidelines provide a clear definition of the differencebetween oral sedation and pre-medication, and highlight the needthat clinicians using trans-mucosal techniques should be suitablytrained in intravenous sedation.
Only one of the papers on intravenous sedation34 retrospectivelyassessed the usability and precautions required when usingpropofol in patients with dementia. All patients included in thestudy allowed treatment under intravenous sedation where theyhad previously not allowed dental treatment. It noted dentaltreatment with water usage (mainly restorative treatment)required a longer sedation time and more propofol usage, and themain complication in these cases was coughing (41.5% of theparticipants). Bradycardia (13.8%), hypotension (12%) and snoring(16.9%) were noted as other complications seen during themanagement of these patients.
Finally, a case report36 on the use of a Bispectral index monitor (BIS)as a way of evaluating the sedation level in a patient withfrontotemporal dementia was included in the review. BIS monitorsmonitor the level of consciousness in patients undergoingsedation and anaesthesia. It analyses electroencephalogram waveforms and quantifies this information to produce a numerical valueof 0-100. The study noted a numerical value of 99 was seen in theindividual prior to the administration of a propofol infusion (speedof 1.5-3.5 mg/kg/hr) whereas a score in the low 80s was seen at thesedation end point. Dental treatment was provided uneventfully.BIS monitors, therefore, might be a useful adjunct in clinicalmonitoring in some patients with dementia patients undergoingsedation, where other clinical signs may be a less clear due tocognitive impairment.
General anaesthesiaIn some circumstances, general anaesthesia might be the onlyremaining viable option for the delivery of dental care. It should beconsidered the most restrictive option for the provision of dentaltreatment and only explored if all other, less restrictive optionshave been discussed or explored. The benefit of dental treatmentunder general anaesthetic is that all necessary treatment can beprovided in a single visit. There is a growing body of evidence thatthere is a risk of a disturbance in cognitive functioning followinggeneral anaesthesia within the elderly population. There are twomain clinical conditions described in the literature
i) Delirium. This is the acute onset of disturbed mental function.Symptoms can include visual hallucinations, delusionalthoughts, anxiety and distress. It may be attributed to anunderlying cause, such as an infection, but is also associatedwith various drugs such as those with anticholinergic actions.45
Delirium is a reversible condition which can affect medical orsurgical patients. The recently released guidance from theAmerican Geriatrics Society46 includes the presence of chroniccognitive decline or dementia as being risk factors for post-operative delirium. Delirium can have serious consequences,such as increased mortality and risk of falls as well as asignificant association with accelerated functional andcognitive decline.47,48
ii) Postoperative cognitive dysfunction (POCD). POCD can bedefined as a long term, possibly permanent, disablingdeterioration in cognitive function following surgery. A studyby Moller et al 49 including a cohort of more than 1200 patientsaged above 60 years old found an incidence of POCD of 25% atone week and 10% at three months postoperatively. Thesepatients were followed up two years after their surgery and itwas noted that approximately 1% still had unresolved POCD.This shows the potential long-term effect of this condition. Riskfactors are thought to be increasing age, with an incidenceclose to one in three in those individuals in the study over 80years old. Pre-existing cognitive impairment is a risk factor forPOCD.50
ConclusionProviding dental care for patients with dementia can bechallenging, especially as the disease progresses. Through theprovision of personalised prevention advice, collaboration with thepatient’s relatives and caregivers, and careful planning for the

7SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERindividual’s future, the impact of their dementia on their oralhealth can be reduced. Should intervention be required, all effortsshould be made to explore the least restrictive options first, withgeneral anaesthesia used only as a last resort. Research specificallysurrounding sedation and general anaesthesia within dentistry islimited, the dental profession would likely benefit if future researchwas carried out in this area.
References1. The World Health Organisation. Dementia Fact Sheet. Retrieved from
http://www.who.int/mediacentre/factsheets/fs362/en/ Accessed October 2017.
2. The Alzheimer’s Society. The Dementia UK report. Retrieved fromhttps://www.alzheimers.org.uk/info/20025/policy_and_influencing/251/dementia_uk accessed October 2017.
3. Department of Health. Prime Minister’s Challenge on Dementia 2020. 2016
4. Foundation of General Dental Practitioners Dementia Friendly Dentistry: GoodPractice Guidelines 2017
5. Age UK What is Dementia Retrieved from www.ageuk.org.uk/health-wellbeing/conditions-illnesses/dementia Accessed 2017
6. National Institute of Health and Care Excellence Dementia: supporting peoplewith dementia and their carers in health and social care 2006. Updated 2016. NICEclinical guidance.
7. Jacob HG, Caspar S, MacDonald S Clinical features and multidisciplinaryapproaches to dementia care. Journal Multidisciplinary Healthcare 2011; 4:125–147
8. National Institute of Health and Care Excellence Dementia: supporting peoplewith dementia and their carers in health and social care 2006. Updated 2016. NICEclinical guidance.
9. McNamara G, Millwood J, Rooney Y. Forget me not.- the role of the general dentalpractitioner in dementia awareness. Br Den J 2014; 217: 245 - 248
10. Spector A, Thorgrimsen L, Woods B, Royan L, Davies S, Butterworth M and Orrell M.Efficacy of an evidence-based cognitive stimulation therapy programme forpeople with dementia: Randomised Controlled Trial. British Journal of Psychiatry2003; 183: 248-254.
11. National Institute of Health and Care Excellence ‘Pharmacological interventionsfor the cognitive symptoms of Alzheimer's disease Dementia’. Supporting peoplewith dementia and their carers in health and social care guidelines 2006.
12. Hescham S, Wei Lim L, Jahanshahi A. Deep brain stimulation in dementia-relateddisorders. Neuroscience & Biobehavioral Reviews 2013, Volume 37, Issue 10, Part 2Pages 2666-2675.
13. Ship J, Puckett S. Longitudinal study on the oral health in subjects withAlzheimer’s disease. J Am Geriatr Soc 1994; 42: 57–63.
14. Fiske J, Griffiths J, Jamieson R, Manger D. Guidelines for oral health care for long-stay patients and residents. Gerodontology 2002a; 17: 55–64.
15. Warren JJ, Chalmers JM, Levy SM, et al. Oral health of persons with and withoutdementia attending a geriatric clinic. Spec Care Dentist 1997; 17: 47–53
16. National Working Group for Older People. Meeting the challenges of oral healthfor older people: a strategic review. Gerodontology 2005; 22 (Suppl. 1): 1–48.
17. British Society of Gerodontology. Guidelines for the Development Of LocalStandards of Oral Health Care for People with Dementia. Gerodontology 2006; 23 (Suppl. 1): 3–32
18. NHS England. The Review Body on Doctors’ & Dentists’ Remuneration Review for2017 General Medical Practitioners and General Dental Practitioner. Retrievedfrom https://www.england.nhs.uk/wp-content/uploads/2016/10/nhse-initial-written-evidnc-ddrb.pdf accessed October 2017.
19. Department of Health. Dementia Friendly Health and Social Care Environments.Retrieved from https://www.gov.uk/government/publications/dementia-friendly-health-and-social-care-environments-hbn-08-02. 2015. Accessed October 2017.
20. Alzheimer’s UK. Communication and Language. Retrieved fromhttps://www.alzheimers.org.uk/info/20064/symptoms/90/communicating_and_language. Accessed October 2017.
21. Rainero I, Vighetti S, Bergamasco B, Pinessi L, Benedetti F. Autonomic responsesand pain perception in Alzheimer’s disease. Eur J Pain 2000; 4: 267–274
22. Department of Health. The Mental Capacity Act 2005. Published 2005. Legislation 2007.
23. De Visschere L, de Baat C, Schols JM, Deschepper E, Vanobbergen J. Evaluation ofthe implementation of an ‘oral hygiene protocol’ in nursing homes: a 5-yearlongitudinal study. Community Dent Oral Epidemiol 2011; 39: 416–425.
24. Van der Putten GJ, Mulder J, de Baat C, De Visschere LM, Vanobbergen JN, ScholsJM. Effectiveness of supervised implementation of an oral health care guideline incare homes; a single-blinded cluster randomized controlled trial. Clin Oral Investig2013; 17: 1143–1153.
25. Zenthöfer A, Meyer-Kühling I, Hufeland AL. Carers’ education improves oral healthof older people suffering from dementia – results of an intervention study.Clinical Interventions in Aging. 2016. Dovepress.
26. The British Dental Association. Evidence summary for Dental Problems and theirManagement in Patients with Dementia. 2013.
27. Nunn J, Greening S, Wilson K. Principles of Intervention for People Unable toComply with Routine Dental Care. The British Society for Disability and OralHealth Guidelines. 2004.
28. L.C. Hutchison, C.E. O׳Brien. Changes in pharmacokinetics and pharmacodynamicsin the elderly patient. J Pharmacy Practice 2007; 20: 4-12
29. The New Zealand Medicines and Medical Devices Safety Authority. Midazolam forInjection 1mg/1ml. Retrieved fromhttp://www.medsafe.govt.nz/profs/Datasheet/m/MidazolaminjPfizer.pdf.Accessed 2017.
30. Schroeck J, Ford J, Conway E et al. Review of Safety and Efficacy of SleepMedicines in Older Adults. Clinical Therapeutics 2016; 38: 2340-2372
31. Wandel C, Bocker R, Bohrer H et al. Midazolam is metabolized by at least threedifferent cytochrome P450 enzymes. BJA: British Journal of Anaesthesia 1994; 73: 658–661
32. Hovstadius BHK, Anstrand B, Petersson G. Increasing Polypharmacy- an individualbased study of the Swedish population 2005-2008. BMC Clin Pharmacology 2010;10: 16
33. The Dental Faculties of the Royal Colleges of Surgeons and the Royal College ofAnaesthetists IACSD guidelines - Standards for Conscious Sedation in theProvision of Dental Care, 2015
34. Sugimura M; Kudo C; Hanamoto H; Oyamaguchi A et al. Considerations duringintravenous sedation in geriatric dental patients with dementia. Clinical Oralinvestigations 2015; 19: 1107-111
35. Huang Y.-H.; Huang T.-S.; Ko E.-S et al. Intravenous sedation assisted dentaltreatment on patients with dementia. Source Clinical Neurology 2016; 56
36. Iwamoto R.; Nitta Y.; Takuma S.; Shibuya M et al. Intravenous sedation using BISmonitor for a dental patient with frontotemporal dementia. Journal of JapaneseDental Society of Anesthesiology 2013; 41: 34-37
37. Murata K.; Kawai M.; Yamashita T et al. A study of dental treatment for patientswith dementia under intravenous sedation. Journal of Japanese Dental Society ofAnesthesiology 2010; 38: 39-40
38. Mochizuki K.; Tsujino K.; Ohtawa Y et al. Dental care for physically or mentallychallenged at public dental clinics. The Bulletin of Tokyo Dental College 2007; 48: 135-142
39. Rignell L; Mikati M; Wertsén M; Hägglin C. Sedation with orally administeredmidazolam in elderly dental patients with major neurocognitive disorder.Gerodontology 2017; 34: 299-305
40. Nicolas E; Lassauzay C. Interest of 50% nitrous oxide and oxygen premix sedationin gerodontology. Source Clinical interventions in aging 2009; 4: 67-72
41. Boyle CA, Frolander C, Manley G. Providing dental care for patients withHuntington's disease. Dental update 2008; 35: 333-336
42. Musani IE, Chandan NV. A comparison of the sedative effect of oral versus nasalmidazolam combined with nitrous oxide in uncooperative children. Eur ArchPaediatr Dent 2015; 16: 417–424.
43. Hartgraves PM, Primosch RE. An evaluation of oral and nasal midazolam forpediatric dental sedation. ASDC J Dent Child 1994; 61: 175–181.
44. Agarwal S, Kriel R, Brundage R. A pilot study assessing the bioavailability andpharmacokinetics of diazepam after intranasal and intravenous administration inhealthy volunteers. Epilepsy Research 2013; 105: 362-367
45. Fines D, Severn A. Anaesthesia and cognitive disturbance in the elderly.Continuing Education in Anaesthesia, Critical Care & Pain 2006; 6
46. American Geriatrics Society. Clinical Practice Guideline for post operative deliriumin older adults. 2015.
47. Sprung J, Roberts RO, Weingarten TN et al. Postoperative delirium in elderlypatients is associated with subsequent cognitive impairment. Br J Anaesth 2017;119: 316-323
48. Fines D, Severn A. Anaesthesia and cognitive disturbance in the elderly.Continuing Education in Anaesthesia, Critical Care & Pain 2006; 6
49. Moller JT, Cluitmans P, Rasmussen LS, et al. Long-term postoperative cognitivedysfunction in the elderly: ISPOCD1 study. Lancet 1998; 351: 857–61
50. Deine. S, Silverstein.J.H. Postoperative delirium and cognitive dysfunction. BritishJournal of Anaesthesia 2009; 103: i41–i46

8 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
AbstractIntranasally (IN) administered midazolam has allowed patientswho require conscious sedation but struggle to toleratecannulation to receive dental treatment under sedation. Studieshave demonstrated a mean bioavailability of 82.4% can beachieved with IN midazolam due to the high vascularity withinthe nose. These studies have also demonstrated that peak plasmaconcentrations can be reached within 10 minutes, which signifiesthe fast onset of action. The standard bolus dose of IN midazolamis 10-12mg, which can be reduced or increased depending on thepatient’s age and susceptibility to benzodiazepines. The bolus canalso be repeated if adequate sedation is not reached. Some 17patients received a standard dose of 10mg of midazolam. Therewere two cases of desaturation below 92%, which responded withoxygen and encouraging the patient to breathe. A protocol foradministering IN midazolam is outlined and two cases arediscussed.
IntroductionFor some people with disability, the continuing management oforal health including periodontal care, routine examinations andthe provision of restorative treatment is very difficult.1 The use ofconscious sedation in dentistry is one of the most widelydiscussed and regulated areas in the profession. In the last twentyyears, there have been many publications providing guidance and clinical standards for practice in this area.2 The use ofintravenous midazolam alone is defined as a standard technique.3
Intravenous (IV) sedation using midazolam has had a greatlypositive effect on the provision of dental care; it has improvedaccess to dental care and reduced reliance on generalanaesthesia. The patient must, however, be able to tolerateintravenous cannulation, and many patients with disabilitystruggle with this aspect of conscious sedation. To overcome thisproblem, patients with disability were often premedicated withoral midazolam, but following oral administration it may take upto 60 minutes to achieve peak plasma concentrations.4 The timetaken to achieve an adequate degree of sedation is frequentlyprotracted. Oral midazolam is broken down in the liver, and thefirst pass reduces its bioavailability to between 35-44%.5
Veldhorst-Janssen et al. have found the mean bioavailability ofintranasal midazolam is approximately 82.4%.6 The mainadvantages of intranasal midazolam are, firstly, the highbioavailability, as the nasal route in not subject to first passmetabolism,7 and secondly, peak plasma concentration ofmidazolam can be reached after 10 minutes.8
Intranasal sedation is not new, but has not been widely adoptedand any method or technique which could help achieve bettertreatment outcomes for people with disability should be madewidely available. The technique has been used in some areas ofclinical practice for many years, and in the Special CareDepartment of Dorset County Hospital for six months prior to thepreparation of this paper in 2015.
Clinical pharmacology of midazolamMidazolam is an imidazobenzodiazepine and is the standard drugused in the practice of intravenous conscious sedation.9 It hasanxiolytic, sedative, hypnotic, anticonvulsant muscle-relaxant, andanterograde amnesic effects.10 Midazolam enhances the effect ofGABA, which is an inhibitory neurotransmitter. It also reduces theexcitability of neurones in the brain by increasing the uptake ofchloride ions.11 Midazolam also impairs episodic memory.12
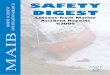
Rationale for the use of theintranasal routeThe nasal route is a very attractive method of delivery due to therich vascular plexus (Figure 1) that is present within the nasalcavity and the ease of accessibility to this vascular bed, allowingdelivery of medications directly to the blood steam.13 Othertechniques of transmucosal sedation, including sublingual, aredescribed in the literature, but often require a greater degree ofpatient cooperation.
The safest way to administer the agents in conscious sedation isby titrating them against the patient’s response, and this is therecommended technique for intravenous sedation withmidazolam. Intranasal administration of midazolam is, in effect, abolus dose technique.
The potential for over-sedation is greater with bolus dosetechniques. It is standard practice that, for all techniques wheremidazolam is used to produce conscious sedation, an intravenouscannula should be placed, as the patient may require reversal. Forthis reason, the technique should only be used by dentists andsedationists who are fully trained and competent in cannulationand should not be seen as a technique to provide sedation forpatients with difficult IV access. The same standards of monitoringapply as for intravenous midazolam sedation.
The use of intranasal midazolam in a special care dentistrydepartment in a hospital setting; technique and cases. David Drysdale, BDS, MSc, DIC, MFDF RCSEd, Dip Con Sedation Speciality Dentist in Paediatric DentistryKing’s College Hospital, Denmark Hill, London SE5 9RS
Nigel D Robb, TD PhD BDS FDSRCSEd FDS(Rest Dent) FDSRCPS FDTF FHEAReader and Honorary Consultant in Restorative Dentistry, Specialist in Special Care DentistryBristol Dental School, University of Bristol, Lower Maudlin Street, Bristol BS1 2LY
Corresponding Author: [email protected]

9SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
Intranasal Midazolam DosingIt is widely accepted that the standard dose for IN midazolam is0.25-0.3mg/kg body weight up to a maximum of 10-12mg givenas a single bolus dose. This bolus can be repeated if the patient isnot adequately sedated. The bolus can also be increased ordecreased. This bolus dose initially seems very high. Veldhorst-Janssen found a mean bioavailability of 82.4% for IN administeredmidazolam,6 this would equate to a dose of around 8.24mg ofmidazolam. This technique has a high record of safety, andManley14 conducted an audit of 222 episodes using this technique.Only one episode of significant desaturation was recorded, whichresponded with the administration of oxygen.
Some patients are tolerant to midazolam. In these patients, thestandard dose may not be sufficient to produce an adequatedegree of sedation to allow dental treatment to be completed. Insome cases, it may be possible to place an intravenous cannulaand titrate midazolam to the endpoint. In others, there may beinsufficient anxiolysis to allow the patient to accept cannulation. If the patient cannot accept either cannulation or treatment, it isoften recommended that they are allowed to recover andreappointed either to have an increased dose of sedative ortreatment under general anaesthesia.
To allow treatment to proceed as planned, an appropriatelyexperienced sedationist might consider giving a supplementalintranasal dose of midazolam. The decision as to whether to givethe additional dose and, if so, how much to give and when, mustbe judged by careful patient assessment, including their responseto the initial dose. The potential for over-sedation should not beunderestimated. This procedure should not be a matter of routine,but a considered judgement taken case-by-case. The second dosewould normally be no greater than 50% of the initial dose. Theauthors would only consider using this approach when the40mg/ml presentation of midazolam is used.
The technique involves the administration of two bolus doses ofmidazolam. The advantages of titration vs bolus doses havealready been discussed. The administration of a second bolus dose
will increase rather than decrease the unpredictability. Thistechnique, whilst practised in a number of centres has not beenthe subject of any clinical trials, and so must be viewed as thepersonal opinion of the authors. A third dose should not beadministered.
Protocol for Intranasal sedationThe patient must go through a pathway of selection, assessment,history, examination, contraindications and consent. Theseprocesses should follow the IACSD standards15 and are describedin the relevant texts16,17 Table 1, outlines a practical protocol whichcan be followed. IN 40mg/ml midazolam + 2mg/ml Lidocaine isprepared in boxes of five ampoules. Each ampoule has a volumeof 0.5ml, thus 10mg of Midazolam would equate to 0.25ml ofsolution. A Luer lock syringe must be used to attach the MAD
""
$ $ $ $
" " " " " " " " " " " " " " "" " " " " " " " " "
" " " " " " " " " " " " "" " " " " " " " " " " " " " " "
" " " " " " "
$ $ $ $ $ $ $ $
" " " " " " " " " " " " " " " " " " "" " " " " " " " " " " " " " " " "" " " " " " " " " " " " "
" " " " " " " " " " " " " " ""
# " " " " " " " " " " " " " " " "" " " " " " " " " " " "
" " " " " " " " " " " ""
# " " " " " " " " " " " " " " " "" " " " " " " " " " " " "
" " " " " " " " " " " " " " " " "" " " " " " " " " " " " " " " "
" " " " " " " " " " " " " " " " "" " " " " " " "
" " " " " " " " " " " " " " " " "" " " " " " " " " " ""Figure 1: Figure 1 illustrates the vascular anatomy of the nasalseptal blood supply. A large number of arteries supply the areaand converge to form Kiesselbach’s plexus.
Figure 2: IN Midazolam is given as a non-titratable bolus, andthe patient’s response cannot be predicted.
""
"
$ $ $ $$
# " " " " " " " " " " " "" " " " " " " " " " " "
" " " " " " " " " " " " " " " "" " " " " " " " " " " " " " " "
" " " " " " " " " " " " " " " " "" " " " " " " " " " " " " " " "" " " ""
# " " " " " " " " " " " " " " " " " " " "" " " " " " " " " " " " " " " " " "" " " " " " " " " " " " " " " " " "
" " " " " " " " " " " " " " " " E)", " " " " " " " " " " " " " " " " " "
" " " " " " "
" " " " " " " " ""
"
" ""
B " " " " " " """
Figure 3: An example of IN device being used.
3. If a sufficient level ofsedation is reached,
cannulate the patient. Ifthis level has not been
reached considerwhether a top up dose
should be given
1. Administer thedecided dose of
intranasal midazolaminto the patient’s
nostril.
2. Monitor patient for 10-12 minutes.

10 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
device, as this prevents the mucosal atomisation device (MAD)from detaching during application.
The MAD is locked onto the syringe and then placed into the rightor left nostril and the bolus is given (Figure 3). It may helpful tostand behind the patient’s head and use safe holding to gentlybrace the head when working with patients who might not beable to stay still. If given successfully, the effects should occurwithin 10-12 minutes, at which point the patient should becannulated. If the sedation is not sufficiently effective after 12-15 minutes, a decision needs to be taken as to the next courseof action, as described above.
CasesPatient 1
An eighteen-year-old male attended with his parents. Hecomplained of pain in the lower left quadrant. He presented witha mobile tender LL4. He also had an UL1 with an incisal edgefracture. Medically, the patient had adult learning difficulties, waspartially deaf and was undergoing testing for Marfan’s syndrome.He communicated with sign language and picture cards on hisipad. All previous treatment had been conducted under generalanaesthetic.
The options for treatment were discussed, and a treatment planwas formulated which involved the extraction of the LL4 toothand the restoration of the UL1 tooth under conscious sedationusing IN Midazolam. The patient was consented with bestinterests.
A 10mg dose of IN midazolam was administered in the rightnostril, and after approximately 12 minutes the patient wassufficiently sedated to allow cannulation. We were able to extractthe LL4 and restore the UL1 without providing the patient withsupplemental intranasal midazolam or intravenous midazolam.Pulse, SpO2 and blood pressure remained normal throughout thetreatment.
Patient 2
A seventy-year-old woman attended the clinic in pain with herhusband, who is her carer. Medically, the patient suffers fromdementia and can only manage to sit down briefly for dentalexaminations before getting up and walking around the surgery.On examination, UR6 was symptomatic.
Options were discussed. The plan agreed involved extracting thetooth with IN Midazolam conscious sedation, and if that failed, toextract the tooth under general anaesthetic. The patient wasconsented with best interests.
A 10mg dose of IN midazolam was administered, and afterapproximately 12 minutes the patient was sufficiently sedated toallow cannulation. The patient was adequately sedated to allowthe extraction of the tooth without the need for additionalintravenous midazolam. Pulse, SpO2 and blood pressure remainednormal throughout the treatment.
Lessons from these cases histories
These two patients had very different needs. Intranasal midazolam(40mg/ml midazolam and 20mg/ml lidocaine) is an off-licence
Suggested Sequence Action
1. Carry out pre-sedation checks.
2. Check the ampoule of Midazolam paying attention to the name Midazolam HCl 40mg/ml +Lidocaine 20mg/ml, Batch number and expiry date.
3. Insert a 1ml Luer locking syringe into the ampule and draw up the decided volume + additionaldead space volume. Carefully label the syringe Midazolam 40mg/ml + Lidocaine 20mg/ml anddispose of the sharps.
4. Inspect the nostrils for blockages, attach a monitor to the patient to monitor SpO2 and Pulse.
5. Lock the MAD device onto the Luer lock syringe, place into the patient’s nostril and advise thepatient to sniff as the plunger is pushed.
6. Continue monitoring the patient’s vital signs for and look for changes in consciousness. 7. After 10-12 minutes assess the patient for acceptability of intravenous cannulation and dental
treatment.
8. Cannulate patient if sufficiently sedated. If compliant, carry out dental treatment.
9. If the patient tolerates intravenous cannulation, but cannot tolerate the dental treatment consideradding a titrated dose of intravenous midazolam.
10. If the patient is unable to tolerate intravenous cannulation or dental treatment, consider a seconddose of intranasal midazolam.
Table 1 - Suggested protocol for administering IN conscious sedation.

11SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERmedication, and that must be explained and documented as partof the consent process. The first patient with good supportmanaged to have dental treatment using intranasal sedation. Thiscase shows the benefits to both patient and carers. The fact thatthe patient was not required to starve made his parents’ livesmuch easier. His parents commented that, as treatment wasconducted in familiar surroundings, the episode was lessdistressing for their son.
The second patient, with the help and support of her husband,managed to have an extraction using intranasal sedation. Thepatient’s husband was keen to avoid general anaesthetic for hiswife when we realised that the treatment plan would involve theextraction of a tooth. The patient was not required to starve priorto treatment, and the total time in which the patient remained inthe clinic from admission to discharge was significantly shorterthan if she had undergone general anaesthesia. After treatment,the patient’s husband wrote a thank you card and admitted hehad been sceptical of the technique, but that it had made thingsso much easier for both him and his wife.
There are some patients who will never accept dental treatmentunder local anaesthesia without additional pharmacologicalintervention. Conscious sedation with intravenous midazolam hasbridged the gap between dental treatment with local anaesthesiaand general anaesthetic, but only if the patient can toleratecannulation. A significant number of patients with cognitiveimpairment find accepting any form of injection impossible totolerate. Both the patients would most likely have been offeredextractions under general anaesthetic as the only option fortreatment. The use of IN sedation in the special care dentistrydepartment allowed these patients to receive a full spectrum ofdental care. There are also a large number of needle-phobicindividuals for whom IN sedation offers the chance to accessdental care.
Adverse effects, risks andcontraindicationsThe risk from IN administered conscious sedation is the same asfor IV midazolam. Some patients have complained of a blocked orrunny nose for 24 hours, and teary eyes. The method iscontraindicated in patients who suffer from nasal polyps, inpatients with cold- and flu-like symptoms, and for patients whosuffer from regular nose bleeds. An absolute contraindication isthat this technique must not be carried out by practitioners whoare not experienced in cannulation, as there would be no way toreverse the patient if required. It is, however, sometimes difficult toadminister the solution to patients with challenging behaviour.Training in safe handling is required if considering using thistechnique in people with special needs and challengingbehaviour.
Initial ResultsThe Special Care Dentistry Department at Dorset County Hospitalhas seen great early success with this technique. 17 patientsreceived a standard dose of 10mg of Midazolam. This wasadministered either as a single dose, repeated or used with orwithout additional IV midazolam or IV propofol. All the patients
were men and women over the age of twelve and were ASA 1 orASA 2. There were two cases of desaturation below 92%, whichresponded to oxygen and encouraging the patient to breathe.Two patients experienced epistaxis: one patient with learningdifficulties placed his fingers in his nose which caused a resultantbleed, and the other had a spontaneous bleed a few minutes afterthe IN bolus was given.
Flumazenil useFlumazenil was administered to three patients who had moderateto severe behavioural difficulties. The patients all had normal vitalsigns. Flumazenil was administered to these patients to improvedisorientation rather than reverse any ill effects from oversedation. As discussed, this technique of conscious sedation isnew to the department and the cohort of patients is very small.
DiscussionThe technique involving the titration of intravenous midazolamhas allowed many patients to access dental care, including thosewith special needs and needle phobias who have previously beenunable to receive dental treatment with the IV technique. Theintranasal technique could be beneficial to these patients. INmidazolam application is a basic technique provided that thepractitioner can demonstrate competence in intravenoussedation.3 The technique of IN sedation is not as widely used as IVsedation, however, research has found it effective and safe; Manleyet al.14 found that in 222 episodes of sedation, 128 (57.65%)accepted treatment.
ConclusionThe purpose of this paper was to demystify the use of INmidazolam as a technique in conscious sedation. This paper alsooutlines a practical protocol which other clinicians could follow intheir own practices for administering IN midazolam. The SpecialCare Dentistry Unit at Dorset County Hospital is within a teachinghospital, and our sedation service is consultant anaesthetist led. Atthe time of writing in 2015, the technique had been in use withinthe department for a period of six months. The initial results havebeen very positive.
AcknowledgementsThe authors would like to thank Grace Drysdale, the amazing staffat the Special Care Dentistry Unit at Dorset County Hospital, andgive a special thank you to Dr David Craig for second chances.
Conflict of interestNo conflict.
Sources of FundingNo funding was received.

12 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERReferences 1. Manley MCG, Ransford NJ, Lewis DA, Thompson SA and Forbes M. Retrospective
audit of the efficacy and safety of combined intranasal/intravenous midazolamsedation technique for the dental treatment of adults with learning disability.British Dental Journal 2008; 206:E3
2. Robb N. The role of alternative (advanced) conscious sedation techniques indentistry for adult patients: a series of cases. British Dental Journal 2014; 216
3. Standards for conscious sedation in dentistry: Alternative Techniques. A Reportfrom the standing Committee on Sedation for Dentistry 2007.
4. Greenblatt DJ, Abnerethy DR, Locniskre A, Harmatz JS, Limjuco RA and ShadlerRi. Effect of age, gender and obesity on midazolam kinetics. Anesthesiol 1984; 61:27-35
5. Smith MT, Eadie MJ and Brophu TO, The pharmacokinestics of midazolam in man.Eur J Clin Pharmacology 1981; 19: 271-278.
6. Veldhorst-Janssen NM, Fiddelers AA, van der Kuy PH, Theunissen HM, de KromMC, Neef C, Marcus MA. Pharmacokinetics and tolerability of nasal versusintravenous midazolam in healthy Dutch volunteers: a single-dose, randomized-sequence, open-label, 2-period crossover pilot study.
Clin Ther 2011; 33: 2022-8. doi: 10.1016/j.clinthera.2011.10.012. Epub 2011 Nov10.
7. Schwagmeier R, Alincic S Stribel HW. Midazolam pharmacokinetics followingintravenous and buccal administration. Br J Clin Plarmacol 1998; 46: 203-206
8. Walberg EJ, Wills RJ, Eckhert J. Plasma concentration of midazolam in childrenfollowing intranasal administration. Anesthesiology 1991; 40: 233-235
9. D Drysdale. Transcutaneous carbon dioxide monitoring in conscious sedation: Aliterature review: OHDM 2014; 13
10. Ari Kupietzky, Milton Hopt. Midazolam a review in conscious sedation inchildren. Peadiatric dentistry 1993; 15
11. Fox C, Liu H, Kaye AD. Manchikanti L, Trescot AM, Christo PJ, et al, eds. ClinicalAspects of Pain Medicine and Interventional Pain Management: A ComprehensiveReview. Paducah, KY: ASIP Publishing 2011. Antianxiety agents; pp. 543–552
12. Buffett-Jerrott SE, Stewart SH. Cognitive and sedative effects of benzodiazepineuse. Curr Pharm Des. 2002; 8: 45–58.
13. Training Procedure for Intranasal Naloxone. Tim Wolfe. 2008.
14. Manley MC, Ransford NJ, Lewis DA, Thompson SA, Forbes M.
Retrospective audit of the efficacy and safety of the combined intranasal/intravenous midazolam sedation technique for the dental treatment of adultswith learning disability. Br Dent J. 2008; 205: 84-5. doi: 10.1038/sj.bdj.2008.521.Epub 2008 Jun 1
15. Conscious Sedation in the Provision of Dental Care. Report of The IntercollegiateAdvisory Committee for Conscious Sedation in Dentistry. The Dental Faculties ofThe Royal Colleges of Surgeons and The Royal College of Anaesthetists April2015. http://www.rcseng.ac.uk/fds/publications-clinical-guidelines/docs/standards-for-conscious-sedation-in-the-provision-of-dental-care-2015 (cited 7th July 2016)
16. Meechan JG, Robb ND & Seymour RA. Pain and Anxiety Control for the ConsciousDental Patient”. Oxford University Press May 1998. ISBN 0-19-262849-6
17. Craig DC, Skelly AM. Practical Conscious Sedation. 1st ed. London: Quintessence,2004. ISBN 1-85097-070-X
Online CPD fromthe SAAD Website
Log-on to the membership area and follow the link ‘Online CPD’
Answer the multiple-choice questions relating to the refereed papers section
of this issue of the SAAD Digest
CPD certificate provided as a download

13SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERCan Clinical Hypnotherapy be used as an adjunct or analternative to Conscious Sedation in Dentistry?Munir Ravalia BDS MFDS RCS Pg Cert Sed DCHyp General Dental PractitionerMedical Clinical HypnotherapistWimbledon, UK
Corresponding Author: [email protected]
AbstractSome patients are unable to tolerate dental procedures without aform of pharmacological intervention, whether it be via conscioussedation or general anaesthesia. However, it should not beforgotten that the first line of pharmacological intervention is theuse of local anaesthesia. Hypnotherapy understandably raiseseyebrows, as many imagine the scene where a stagehypnotherapist makes subjects carry out comical acts in front of arapturous audience, so in a clinical context, it is clear to see whymany perceive it with scepticism. Current options in terms ofbehavioural management include: ‘tell show do’, distraction,positive reinforcement, memory restructuring, modelling andsystematic desensitisation. These management techniques,although beneficial, are time consuming and carry their own risks.A rarely explored alternative is clinical hypnosis, which can beemployed with minimal risks or side effects. Clinical hypnosis aimsto investigate and manage the underlying aetiology of the needfor behavioural or pharmacological management, regardless of theidentified cause, rather than moving directly to pharmacologicallyled management, which often leads to dependency on the chosentechnique. The author's aim is to explore the correlation betweenthese differing treatment modalities and to assess whetherhypnosis as a stand alone technique can be employed successfullyor utilised in a combination technique, 'hypnosedation'.
Keywords: hypnotherapy, conscious sedation, systematicdesensitisation, hypnosedation
Aims and Objectives:The aim of this paper is to examine and analyse the use of hypnosisin relation to dental sedation. The object is to explore the following:1. Causes of dental phobia and anxiety2. What is conscious sedation, Cognitive Behavioural Therapy
(CBT) and clinical hypnotherapy?3. Indications for their use4. Hypnotherapy uses in phobia, desensitisation techniques.5. Hypnotherapy use as an adjunct to reduce sedative drug
regimen6. Reasons for its under-utilisation in clinical practice and stigmas
attached to it7. Recommendations
Methods:This paper was informed by, a literature search using Pubmed;direct interviews with clinical hypnotherapists and finally, theAuthor's personal reflections from working in this field.
Introduction:The Diagnostic and Statistical Manual of Mental Disorders1 defines“Specific Phobia” as being when "the individual experiencesexcessive and persistent fear of a specific object or situation,experiences feelings of anxiety, fear, or panic immediately uponencountering the feared object or situation, leading to significantdistress or interference in the person’s day-to-day life."Odontophobia is well recognised and encountered at differinglevels by all dental clinicians.
The General Dental Council's “First Five Years”2 encourages theawareness ‘of the existence and a range of complimentarytherapies’. Currently, many would define hypnotherapy likeacupuncture to be a complimentary therapy, however, clinicianstrained in these fields may argue otherwise!
The aetiology of dental phobia is multifactorial and may include:direct experiences (learning); modelling; helplessness andperceived lack of control. It can commonly arise from a processknown as conditioning, a process of behaviour modificationwhereby a subject comes to associate a behaviour with apreviously unrelated stimulus. The conditioning effect of a baddental experience has been shown to be one of the mostimportant; Ragnarsson,3 found that more phobic people thananxious ones attributed their fear to an adverse incident (90.5% vs.65.8%). In children, conditioning may be only one of a number offactors implicated in the development of dental anxiety, thoughreports of traumatic experiences were significantly more frequentin anxious than non-anxious children in one study.4 Which dentisthasn't experienced a child sitting in the surgery in pain, theirparents warning them on the way into the surgery that if theydon't co-operate, the 'nice' dentist will stick a long needle in theirmouth? Truly a recipe for disaster; the parent’s potentialmisconceptions or past experiences manifesting as potential fears,which whether well-founded or not, are passed like tracing paperstraight to their child. The Chief Medical Officer noted the highestadmittance to general anaesthesia in UK between 2014 and 2015was for dental caries. Whether this was because of the extent oftreatment required or the inability of the child/parents to cope in ageneral practice setting, is yet to be analysed.
Assessment of Sedation/Hypnotherapy need:The indicator of sedation need (IOSN), was developed to aiddentists in their clinical decision making, utilising informationabout a patient’s anxiety, medical and behavioural status andtreatment complexity. It includes the Modified Dental Anxiety

14 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERScale (MDAS),5 a short questionnaire that may be completed in afew minutes by the patient. It consists of five questions and gives atotal summed score between 5 and 25 that is then translated bythe dentist to a rank score of 1-4 which can be entered into theIOSN.6
Indicator of Sedation Need (IOSN)
MATRIX TO BE COMPLETED BY THE DENTIST
SEDATION NEED domain 1 + 2 + 3 scores
Total Rank Score Source Descriptor Sedation Need
3-4 Minimal need No
5-6 Moderate No
7-9 High need Yes
10-12 Very high need Yes
This same scoring system could quite easily be adapted to producean Indicator of Hypnosis Need. (IOHN). It could be adapted toinclude appropriate factors used to assess suitability for clinicalhypnosis, such as past experience of the technique, awareness andbias to the technique as well as failed hypnosis in the past.
As such, hypnosis could be very useful for patients who are ASA III,enabling them to be treated safely in General Dental Practice, andnot requiring to be referred to hospital.
What is Conscious Sedation?The Poswillo Report in 19997 criticised the then existing definitionsof sedation on the grounds that they failed to emphasise theessential basic element of hypnotic suggestion and reassurance,and emphasised central nervous system depression, rather thanmood alteration. Its principal recommendation was that simpledental sedation be defined as “a carefully controlled technique inwhich a single intravenous drug or a combination of oxygen andnitrous oxide, is used to reinforce hypnotic suggestion andreassurance in a way which allows dental treatment to beperformed with minimal physiological and psychological stress”. 7
However, even today the standard definitions of conscioussedation are unchanged and do not take this into account.
Conscious sedation is presently defined as 'a technique in whichthe use of a drug or drugs produces a state of depression of thecentral nervous system enabling treatment to be carried out, butduring which verbal contact with the patient is maintainedthroughout the period of sedation. The drugs and techniques usedto provide conscious sedation for dental treatment should carry amargin of safety wide enough to render loss of consciousnessunlikely.'8
Commonly used techniques for sedation include inhalation withNitrous Oxide/Oxygen, and oral, intranasal, and intravenoustechniques, with intravenous Midazolam being the single mostcommonly used sedative agent. Inhalation or relative analgesia, isunderutilised in general dental practice but is a very safe andpredictable technique.
What is Clinical Hypnosis?Clinical hypnosis can be defined as a technique of deep relaxation,within which the individual becomes highly suggestible.9 It is quiteoften described as the medicine of imagination. The term“hypnosis” has been around since the early 1840’s, there aredocumented records of hypnosis going back 3000 years in Egyptand China. Ibn Sina (Avicenna), a respected 11th century Persianphysician and psychologist, was the earliest to make a distinctionbetween hypnosis and sleep. In his book, 'The Book of Healing',published in 1027,10 Avicenna referred to hypnosis in his Arabictext, as the 'pleasant dreamy imagination', stating that one couldcreate conditions in another person so that they accept the realityof hypnosis.
There are two well defined and recognised types of hypnosis; stagehypnosis and clinical hypnosis. Stage Hypnosis is conducted for thepurposes of entertainment and subjects are often pre-selected tobe those of higher suggestibility, to ensure the desired outcome ofentertainment, and those found not to be co-operating are quicklyeased off stage. Clinical hypnosis is conducted with the full co-operation of the patient and such that the hypnotherapist makessuggestions designed to help the patient calculate specific internalprocesses (memories, feelings, images, etc.) that will lead tomutually agreed-upon outcomes.
How does clinical hypnotherapy work in a dental setting? Dentalphobia is very common and even though informal hypnotic(suggestions of relaxation etc.) techniques are used by dentists ona daily basis for patients undergoing routine dental treatment,formal hypnotherapy does not enter most clinician’s minds.Specific phobias have been treated using psychodynamicpsychotherapy,11 but the treatments of choice have beensystematic desensitisation with or without hypnosis.12, 13, 14
A study15 was carried out, in which interestingly, the authors talk ofthe term 'Hypno-sedation'. Their findings concluded that forhypno-sedation to be effective, it is necessary for the patient to bemotivated, co-operative, and attentive to the suggestions of thehypnotist. Unco-operative patients with short attention spans arepoor candidates for hypnotic techniques.
Hypnosis for sedation, especially for children, has been shown toreduce the amounts of propofol and lignocaine required, withaccompanying reductions in pain, nausea, fatigue, discomfort andemotional upset.14
Indications for Hypnotherapy andConscious Sedation:
Indication Hypnotherapy Conscious sedation
Dental anxiety and Yes Yesneedle phobia
Pronounced gag reflex Yes Yes
Complex surgical Yes Yesprocedure

15SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
Table Note:Glove analgesia = a Hypnotherapeutic technique taught topatients, which allows them to envisage that a hand has beenrendered essentially numb, and they can then transfer this lack ofsensation to other parts of the body.
It should be noted that the terms ‘Moderate Sedation’ and ‘DeepSedation’, are descriptions of sedation that do not conform to theUK guidelines for ‘Conscious Sedation’.
Cognitive Behavioural Therapy is a well-known technique and is apsycho-social intervention. CBT is a talking therapy that can help apatient manage their problems by changing the way they thinkand behave. It focuses on the development of personal copingstrategies that target solving current problems and changingunhelpful patterns in cognitions (e.g. thoughts, beliefs, andattitudes), behaviours, and emotional regulation.
Recent research on hypnotherapy is increasingly focused upon theintegration of hypnotherapy and CBT. In 199516 Kirsch’s researchteam pooled data from 18 separate controlled studies to include577 participants, and compared the efficacy of cognitive-behavioural hypnotherapy with CBT alone. They showed that forbetween 70-90% of clients, cognitive and behavioural therapieswere more effective when integrated with hypnosis, i.e., that forthe vast majority of clients cognitive-behavioural hypnotherapy issuperior to CBT alone. “We believe on the basis of our clinicalexperience that when behaviour therapy and hypnosis are usedtogether, a synergistic effect results.”17
The main hypnotherapeutic technique utilised is based on aprocess known as systematic desensitisation, a behaviouraltechnique commonly used to treat anxiety disorders, fear andphobias. Systematic desensitisation uses the principle of reciprocalinhibition. It is commonly referred to as graduated exposuretherapy and is a type of Pavlovian therapy developed by a SouthAfrican psychiatrist, Joseph Wolpe.18 The process of systematicdesensitisation occurs in three stages.
Stage 1 involves the identification of an anxiety-inducing stimulushierarchy, Subjective Units of Distress Scale (SUDS). This is a scaleof from 0 to 100 for measuring the subjective intensity ofdisturbance or distress currently experienced by an individual.Stage 2 is the learning of relaxation or coping techniques. Oncethe individual has been taught these skills, they must use them instage 3 to react towards and overcome situations in theestablished hierarchy of fears. The goal of this process is for theindividual to learn how to cope with, and overcome the fear ineach step of the hierarchy.
Hypnoanalysis can be used to discover the root cause of the fearallowing the issue to be addressed. Hypnosis is used to train theunconscious mind and re-evaluate thinking patterns andbehaviour.
In clinical hypnosis, the patient is guided by the hypnotist tosuggestions for changes in subjective experience, alterations inperception, sensation, emotion, thought or behaviour.
In a study conducted in Hungary which examined 45odontological patients, hypnosis proved to be a useful adjunctmethod to reduce anxiety for 84.4% of the patients.19
In a prospective comparative clinical study, researchers evaluatedthe effectiveness of hypnosis using 45 highly anxious and non-anxious patients who had to undertake maxillofacial surgery. They were assessed based on the following objective parameters:EEG, ECG, heart rate, blood pressure, blood oxygen saturation andrespiration rate. The results both during and subsequent to thesurgery showed that hypnosis helped patients significantly toreduce systolic blood pressure and respiration rate, and changes inthe EEG were also registered. Moreover, the subjective level ofrelaxation increased at the same time as the neurophysiologicanxiety reactions (vital parameters) decreased. The authorsconcluded that hypnosis influenced both the psychological andthe physiological reactions of dental anxiety during surgery andthe results had long-term effects in future treatments.20
Differences between Hypnotherapy and Conscious Sedation
Hypnotherapy Minimal Moderate Deep GeneralSedation Sedation Sedation Anaesthesia
Level of Light/medium/ Normal response to Purposeful response Purposeful response Unconsciousconsciousness Deep trance like state. verbal commands - to verbal commands- to repeated
Responses to anxiolysis light touch painful stimuliverbal commands.
Conscious sedation
Response Verbal Verbal Light touch Painful stimuli Nil
Airway Maintained Maintained Maintained Maintained/ lost Obstructed
Ventilation Maintained Maintained Maintained Maintained/ lost Inadequate
Anaesthesia Glove analgesia Still required Still required Still required Complete technique can be anaesthesiaused to render norequirement for LA

16 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERMore recently, a further study noted that surgery is associated withsignificant anxiety and stress in a majority of patients. Mostmedications used to achieve anxiolysis and sedation are limited bytheir side effects. ‘Non-pharmacological hypnosis’ is defined as asubjective state, during which alterations of perception andmemory can be elicited by suggestions.21 The results found weresignificantly relevant to those in clinical practice. Hypnosissuccessfully reduced anxiety from a range of 45 to 90 (median of60) to a range of 1 to 20 (median of 10). When calculated andanalysed as means, the mean decrease was 56 (95% CI: 51.81, 60.04)(p<0.001). Twelve of fifteen patients had their intravenous accessestablished under hypno-analgesia with no memory of that event.Thirteen patients had successful prevention of nausea and vomitingwithout anti-emetics. Hypnosis also decreased the dose ofinduction agent required in all patients having general anaesthesia.
A further study noted that the main objectives of premedication inchildren are to facilitate the separation from the parents, to reducepre-operative anxiety, to smooth the induction of anaesthesia andto lower the risk of post-operative behavioural disorders. Hypnosisenables a state of relaxation to be achieved but has never beenevaluated as a premedication technique. The aim of this study wasto evaluate the efficacy of hypnosis on anxiety and peri-operativebehavioural disorders versus midazolam. The authors concluded
that hypnosis seemed effective as premedication in childrenscheduled for surgery. It alleviated pre-operative anxiety, especiallyduring induction of anaesthesia and reduced behaviouraldisorders during the first post-operative week.22
When behavioural treatments have been compared to generalanaesthesia, both produced a reduction in dental anxiety but moreof the patients treated behaviourally were able to successfullycomplete dental treatment. 78% vs. 53% of the GA patients,23 whichmay be a difficulty, as behavioural management seemed toproduce more anxiety reduction when compared to intravenoussedation, and further, that more patients maintained high levels ofdental anxiety following IV sedation.24
Interestingly, another paper found that midazolam requirementswere significantly lower in the hypnosis group (P < .001) ascompared with the intravenous sedation group: respectively, 0.04+/- 0.002, 0.07 +/- 0.005, and 0.11 +/- 0.01 mg/kg/h. Greater patientsatisfaction with the anaesthetic procedure and greater surgicalcomfort were also reported in the hypnosis group. They went on toconclude that successful hypnosis, as an adjunct sedationprocedure to conscious IV sedation, provided better pain andanxiety relief than conventional IV sedation and allowed for asignificant reduction in midazolam and alfentanil requirements.25
Hypnotherapy- Conscious Sedation procedure
Stage Hypnotherapy Conscious sedation- single drug General Anaesthesia
Pre op No stimulants such as coffee, nicotine, +/-Oral premed/EMLA +/-Premed/EMLAmind altering drugs
Induction Techniques include Titrated Midazolam Induction agents1. Simple eye closure2. Rapid Eye defocusing3. Tactile Induction4. Eye fixation/Eye roll
Deepener Techniques include Increased Titrated Increased drug usage-1. limb catalepsy Dose to response e.g. opiates/propofol2. 10-1 countdown3. Hand rotation4. Limb heaviness
Maintenance Continued suggestions Titration- Midazolam IV/Inhalational
Recovery Awakening technique Sedative stopped Reversal agents
Side Effects Very rare Amnesia Nausea/vomiting
Table Note:Induction: An hypnotic induction is the process undertaken by ahypnotist to establish the state or conditions required for therapyto occur. Various techniques can be utilised, but essentially the aimis to render the patient into a relaxed state, with full eye closure.
Deepener: Once the patient has been induced into a hypnoticstate, a deepener is used to render the patient in a much deeper
state, to be able to listen to the positive suggestions of thetherapist. Again multiple techniques can be utilised (only a fewhave been given as examples).
Awakening: At the end of the session, patients must be wokenfully, so they are fully cognitively back in their normal state, similarto awakening someone who has been in a deep sleep, but in a veryprecise and controlled manner.

17SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERAuthor’s Reflections:Clinical hypnotherapy is not mentioned in the Royal College ofSurgeons' clinical guidelines for non-pharmacological behaviourmanagement, however, the author believes it is a crucial frontlinebehavioural management technique for patients.26
Sharon Waxkirsh, a specialist dental clinical hypnotherapistconducted self-hypnosis for her own wisdom tooth removal withcontrol of post op blood flow. Ms Waxkirsh says "I hypnotisedmyself and it is so effective. It didn’t ever become painful, and Ididn’t have any blood loss at all."27
Ms Waxkirsh kindly related to me her experience and thoughts onthis topic. Paediatric patients, she describes, often need parents tobe involved. She told me of a case where a child took three days forthe effects of general anaesthesia to wear off. This scared the fatherand he decided to seek Sharon's help, "You have to play the game,put the child in a place where they feel in control". She used theglove analgesia technique to create numbness in the child and hisfather by using a special word to trigger this numb feeling. Whendescribing the subconscious mind, Waxkirsh states, "Techniques areone thing but dealing with what emerges is another".
A highly respected and leading dentist in this field, Dr Mike Gowdescribes, “In one case, hypnosis was used instead of localanaesthetics in a sinus lift procedure and implant placement and,in another case, I demonstrated hypnosis being used instead oflocal anaesthetic for the extraction of two upper incisors withimmediate implant placement."28,29
The author's personal experience highlights the use of such atechnique successfully being able to treat several patients whohad a severe phobia to dentistry or uncontrolled gag reflex. In onecase a patient was told by a leading UK teaching hospital therewas nothing that could be done for her due to her pronouncedgag reflex. She was managed successfully with a combinationtechnique - hypnotherapy combined with conscious sedation andthen hypnotherapy alone.
Recommendations and Conclusion:Clinical Hypnosis has been used successfully in the medical anddental fields to effectively manage anxiety and fear. Patientsachieve lower scores on Dental Anxiety Scales post-operativelyfollowing hypnosis and also report decreased anxiety for follow upappointments. Hypnosis is monetarily inexpensive and has a verylow risk of side effects. Hypnosis may very well be a safe alternativeto conscious sedation and general anaesthesia.
There are well researched and evidence-based empirical studiessupporting the benefits of hypnosis as an adjunct technique indentistry. Anecdotal evidence by the authors who currently usethis technique is also present. On the basis of available evidence,further research in these areas is justified.30
Dentists should be encouraged to explore further the use of formalhypnotic techniques. This would not only assist patients to copebetter with treatment, but also reduce costly health care bills andthe need for hospitalisation.
It is the Author’s opinion that clinical hypnosis is a reasonablealternative and adjunct to conscious sedation and can be utilised,
as long as the patient is willing to accept it, as a conjunctivetherapy. In answer to the question thus posed by this paper, CanClinical Hypnotherapy be used as an Adjunct and or an Alternativeto Conscious Sedation in Dentistry? Yes it can, by correctly trainedclinicians and based, as with anything, on correct case selection.Hypnosis could be a powerful tool at the disposal of the dentalsurgeon, but is rarely exploited. However, this does not rule out theneed for conscious sedation and general anaesthesia in selectedcases.
Sadly there is a lack of training in this field. 'There is a lack ofappropriately trained dentists offering hypnosis, and this will affectboth the patient's awareness and access to clinical hypnosis.30,31
Courses are available but the minefield of organisations training inhypnotherapy becomes a little overwhelming. Those dentists whoare trained in this field find it difficult to utilise hypnotherapy forNHS patients, as there is no funding for it, hence it becomes amanagement option only for those who can self finance it. Aserious question to pose would be 'should it be taught at sedationcourses?’
Based on this review, there is an obvious need for furtherinvestigation and research, but it may well be time those dictatingdental policy and dental professionals alike, started lookingoutside the conventional. Maybe so-called 'alternative' techniquesmight not be as alternative as they currently are, but becomeintegrated into dental undergraduate training as a mainstay ofdental behavioural management. From the information provided itcan be said that hypnosis can be used as both an adjunct andmain intervention for dental fear.
References1. American Psychiatric Association: The Diagnostic and Statistical Manual of Mental
Disorders DSM-5, Washington: 2013; 300: 23
2. The first five years, London: General Dental Council: 2002 :101-105
3. Ragnarsson B, Arnlaugsson S, Karlsson KO. Dental anxiety in Iceland: anepidemiological postal survey. Acta Odontology Scandinavia 2003: 61:283-8.
4. Townend E, Dimigen G, Fung D. A clinical study of child dental anxiety. BehaviourResearch and Therapy 2000; 31-46
5. Chadwick, BL. Assessing the Anxious patient. Dental update 2002; 29: 448-454
6. Paul Coulthard. Indicator of Sedation Need. Dental Update 2013; 40: 466-471
7. General Anaesthesia, Sedation and Resuscitation in Dentistry. Poswillo Report.London,1990
8. Standards for Conscious Sedation in the Provision of Dental Care: The dentalfaculties of the Royal Colleges of surgeons and the Royal College of AnaesthetistsReport of the Intercollegiate Advisory Committee for Sedation in Dentistry.London 2015
9. Vickers A, Catherine Zollman, and David K Payne; Hypnosis and relaxationtherapies Western Journal of Medicine 2001; 175: 269–272.
10. Jan Bakos. Sina I. Kitab ash-Shifa (book of Healing). Prague: 1027, 1956
11. Seligman, M. The effectiveness of psychotherapy. American Psychologist. 199; 50:965–974.
12. Craske MG, Mohlman J, Yi J, Glover D, Valer: Treatment of claustrophobia’s andsnake/spider phobias Behavioural Research Therapy 1995; 33:197-203
13. Emmelkamp P, Theo K. Bouman & Agnes: Anxiety disorders. A practitioner’s guide.Chichester: John Wiley & Sons, 1989
14. Paediatric Sedation Outside of the operating room: Keira P Mason HarvardMedical School 2012
15. Dominic P. Lu, DDS, Gabriel P. Lu, and Elliot V. Hersh: Augmenting Sedation withHypnosis in Drug-Dependent Patients: University of Pennsylvania 1995; 42: 139-143.
16. Kirsch I, Montgomery G, Sapirstein. Hypnosis as an adjunct to cognitivebehavioural psychotherapy: A meta-analysis. Journal of Consulting and ClinicalPsychology 1995; 63: 214-220.
17. Kroger & Fezler, Hypnosis and Behaviour Modification 1976; 74.

18 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER18. Wolpe, J. The Practice of Behaviour Therapy: New York, Volume 1: Pergamon Press
1990
19. Fabian, T.K.Comparative evaluation of 45 cases of hypnosis. Hypnosis in dentistry1995; 88: 111-115.
20. Eitner S, Wichmann M, Paulsen A, Holst S: Changes in neurophysiologicparameters in a patient with dental anxiety by hypnosis during surgicaltreatment. Journal of Oral Rehabilitation 2006; 33: 496-500.
21. Harsha S, Vidya Jeurkar. The Use of hypnosis as a substitute premedication andadjunct to anaesthesia. Department of Anaesthesiology and Pain Medicine,Michael De Groote School of Medicine, McMaster University. 2013
22. Calipel S, Lucas-Polomeni MM, Wodey E, Ecoffey C. Premedication in children:hypnosis versus midazolam. Paediatric Anaesthesia 2015; 15: 275-81
23. Berggren U, Carlsson, S.G. Dental fear and avoidance: a comparison of two modesof treatment Journal of Dental Research 1984; 63: 1223-1227
24. Dailey YM, Humphris GM, Lennon MA. The use of dental anxiety questionnaires: asurvey of a group of UK dental practitioners. British Dental Journal 2001; 190:450–453
25. Faymonville M, Fissette J, Mambourg PH, Roediger L, Joris J, Lamy M. Hypnosis asadjunct therapy in conscious sedation for plastic surgery. Regional Anesthesia.1995; 20: 145-51
26. Royal College of Surgeons: Behaviour Management: Online information availablefrom https://www.rcseng.ac.uk/fds/publications-clinical-guidelines/clinical_guidelines/documents/non_ph_behaviour_mgmt.pdf
27. Innes. E. Moment. Woman has wisdom tooth extracted, using nothing buthypnosis to deal with the pain. Online information available fromhttp://www.dailymail.co.uk/health/article-2622560/Woman-wisdom-tooth-extracted-using-HYPNOSIS-deal-pain.html#ixzz3zJOn5BTZ, 2014
28. Gow M.A. Dental Extractions, Immediate placement and temporisation of dentalimplants in the aesthetic zone. Dentistry 2008; 53.
29. Gow M.A. Internal sinus lift and placement of an osseointegrated implant usinghypnosis as the sole method of pain control, a first in dental practice. ImplantDentistry Today 2008; 2: 31-37.
30. Lynn S J, Irving Kirsch. Essentials of clinical hypnosis. An evidence-basedapproach. Washington, D.C.: American Psychological Association 2006; 55: 167–88
31. Wolley et al. Hypnosis alternative, or complimentary to conscious sedation indentistry? A review. Journal of Disability and Oral Health 2006; 7: 161.
CONTACT DETAILS
Fiona Trimingham 01302 846 149 • [email protected] Secretary & Webmaster
Course enquiries, payments, cancellations and deferralsHygienist & Therapist course logbooksMembership and website enquiries
SAS and SASN schemes
Toni Richman 07583 039 309 • [email protected] Administrator
Course weekend logistics
Emma Lee • [email protected] Assessed Sedation Nurse scheme Co-ordinator
SAAD, 21 Portland Place, London W1B 1PY+44 (0)20 7631 8893 (NOT COURSE ENQUIRIES) • [email protected]

19SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
AbstractAim:Background: New sedation guidelines have included best practicerecommendations relating to written information provided forconscious sedation that is provided to dental patients. The auditpresented here compares the currently available patientinformation within one community dental service againststandards derived from the new guidance, along with theavailability and quality of the literature provided to patients.
Method: All patient information sheets, relating to dentistprovided forms of conscious sedation from 10 sites of a communitydental service, were collected. The collected sheets were thencompared against pre-defined criteria, derived from nationalguidelines.
Results: There was insufficient available patient information inrelation to patient options, age-appropriate information, materialfor the learning disabled, and separate information sheets forescorts currently available at any site. The quality of availableinformation was variable, with areas for improvement including:out of hours contact details, subjective feelings of sedation, anddescriptions of the dental procedures. Practical preparation of thepatients, as well as risks and benefits, were well documented.
Conclusion: This audit highlights that the new guidance placesnew best practice standards on the written information that weprovided to patients, and indicates areas of potential change thatmay need to be addressed.
IntroductionIt is widely recognised that written patient information is avaluable adjunct to the consent and patient preparation processfor elective procedures. This has been recognised in the consensusguidelines relating to conscious sedation in a dental setting by theIntercollegiate Advisory Committee for Sedation in Dentistry(IACSD)1 recommending that;
“… the healthcare team makes available both verbal and writteninformation of high quality in a form that is easily assimilated bypatients, their parents or carers.”
It is also a recommendation of the new commissioning guidelinesthat content must be age and capacity appropriate2 also formingpart of the SAAD sedation checklist.3 Furthermore, the IASCDdocumentation recognises the need for high quality care toinvolve audit and reflection, which is also echoed by the recentlySDCEP guidance on the same topic.4
The Harrogate and District Foundation Trust incorporates a largegeographical area, and includes 10 sites in which sedation iscarried out. Dentist led sedation is limited to basic techniquesacross all sites, with additional advanced techniques beinganaesthetist led in the service, and as such excluded from thisaudit. Whilst it is recognised that the needs of services vary, theaudit presented here may form a useful template for local auditson this topic.
Aims• The availability of information for different patient groups
seen within our service• The quality of available the information that is provided
compared against the standards laid out in the IACSDguidelines1
Materials and MethodsThe following patient user groups of our conscious sedationservices were identified as: Adults, Younger children (6-12), Olderchildren (12-16), Parents, Carers, Escorts and Learning-disabledadults – with intravenous sedation not being routinely offered tothose under 16. Once identified this was further broken down intowhat patient information should be available to each group, withagreement from the sedation leads for the service, shown in Table 1.
The following patient groups for inhalation sedation should havewritten information available: Adults, Parents of children youngerthan 16, Older Children, Younger children, Escorts/Carers and EasyRead. This should include separate age appropriate information,and separate sheets for instructions for escorts. Furthermore,information relating to intravenous sedation should be availablefor: Adults, Carers and Escorts. This should include easy readinformation for the learning disabled, and separate instructions for escorts.
Audit of written patient information for ConsciousSedation across a Community Dental ServiceThomas D Evans Dental Core Trainee 2 Harrogate and District Foundation Trust
Alice Harding Specialist in Special Care Dentistry Senior Salaried Dental Practitioner Harrogate and District Foundation Trust
Louise Diver Senior Dental Officer Harrogate and District Foundation Trust
Caroline Graham Consultant in Special Care Dentistry Harrogate and District Foundation Trust
Corresponding Author: [email protected]

20 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
Information was collected with a request to every clinic within theservice providing sedation via e-mail to provide all informationcurrently provided to any patient, or available to be provided inthe clinics. This was then followed up by phone for non-responding clinics. The availability of patient literature at eachclinic was recorded. Each information leaflet provided was thenassessed for quality by a single auditor. All data were recorded andanalysed in Microsoft Excel. They were assessed for quality againstthe recommendations for written patient information adaptedfrom the IACSD guidance.1 These can be seen in Table 2, pleasenote that not all standards are required for all types of writtenpatient information.
ResultsResponse rate
All 10 sites carrying out inhalation sedation responded, with the 3sites that were carrying out dentist led intravenous sedation alsoproviding IVS related patient information.
Availability of information
All sites had appropriate written patient information relating toinhalation and intravenous sedation, if carried out on that site.Written information relating to options was sometimes present, butnever as a separate information sheet. No site had separate ageappropriate information to provide to children (older or younger)relating to conscious sedation, but was, in part, included in the
Service User Group
Conscious sedation Parent Adult Learning Escort Age specificinformation type / Carer Disabled (if required) information
Older Child Young Child
Inhalation Sedation Yes Yes Yes No Yes Yessedation information
Care Yes Yes Yes Yes No NoInstructions
Intravenous Sedation Yes Yes Yes No N/A N/Asedation information
Care Yes Yes Yes Yes N/A N/AInstructions
Table 1 – Table showing user groups identified and the patient information required for each user group
Standard Required for: Standard
All Information Sheets Description of the sedation procedure that has been suggested and recommended as the most appropriate
Benefits
Risks
Alternatives
Subjective feelings during sedation
Subjective feelings after the sedation
Contact details of the care provider
Out-of-hours contact details for emergency advice and services
Adults and Young People Instructions regarding the practical arrangements to be followed pre- and post-operatively
Separate information sheet describing the responsibilities of the escort for the patient togive the escort (I.V. only)
Children Separate age appropriate information regarding the sedation procedure
Sheets provided to those with Information about the preparation of the child/patient prior to the appointmentParental/Caring responsibilities
Post-operative instructions for the sedation provided
Description of the dental treatment performed
Table 2 – Showing quality standards used in the audit

21SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERTable 3 – Summary of availability of recommended patient information
User group Written information type Percentage availability across clinics that offer this sedation (Number of clinics available/Number of clinics offering)
Parent/Carer Patient options (separate) 0% (0/10)
Inhalation Sedation 100% (10/10)
Intravenous sedation 100% (3/3)
Adult Patient options (separate) 0% (0/10)
Inhalation sedation 100% (10/10)
Intravenous sedation 100% (3/3)
Learning Disabled Easy Read Inhalation sedation 0% (0/10)
Easy Read Intravenous sedation 0% (0/3)
Separate Escort information Inhalation sedation (included in N/A(if required) parent/carer/adult information)
Intravenous sedation 67% (2/3)
Younger Child Inhalation sedation age specific information 0% (0/10)
Older Child 0% (0/10)
Table 4 – Summary of quality of written patient information sheets that were available.
Standard Percentage of sheets Commentsmeeting standards
Description of the sedation procedure that has beensuggested and recommended as the most appropriate
89.29%
Benefits 100.00%
Risks 85.71%
Alternatives17.86%
Where discussed generalanaesthetic only
Subjective feelings during sedation 57.14%
Subjective feelings after the sedation 46.43%
Contact details of the care provider 78.57% 5 Information sheets were stillusing outdated phone numbers
Out-of-hours contact details for emergency advice and services
3.57%
Instructions regarding the practical arrangements to be followed pre- and post-operatively
100.00%
Separate information sheet describing the Available in intravenous sedation, responsibilities of the escort for the patient 11.11% but not for inhalation sedation – to give the escort not necessarily a requirement.
Separate age appropriate information regarding the sedation procedure
0.00%
Information about the preparation of the child/patient prior to the appointment
81.25%
Post-operative instructions for the sedation provided 71.43%
Description of the dental treatment performed 28.57% Only related to LA administration
For allInformationsheets
Adults andYoung People
Children
Those withParentalResponsibility:

22 SAAD DIGEST | VOL.34 | 2018
REFEREED PAPERinformation provided to parents available at all sites. Noinformation was available in an easy read format for the learningdisabled. Information for escorts was available at all sites, but onlyavailable as a separate information sheet at 2 out of 3 sites whereintravenous sedation was carried out. These findings aresummarised in Table 3.
Quality of information available
A summary of the quality of the information that was available canbe seen in Table 4. Red amber Green (RAG) rating, where Redwhere <50 percent, Amber between 50 percent to 99% compliantand Green where 100 percent compliant.
DiscussionAvailability of Patient information
This audit highlighted a large variability in the availability ofpatient information, despite trust wide protocols. This has likelyrisen through good intentions; all versions were provided in paperformat derived from the originals; the different versions in usecould have potentially arisen through use of a master paper copyopposed to using the updated digital copy. Consistency wouldprovide clarity for patients as well as staff.
Supplemental information sheets for both children and escortswere not available, except for at some intravenous sedation clinics.Whilst information is often given chairside, it remains a timepressured environment, which is not ideal for patients or carers todigest information, and often escorts are not present at theassessments. This should therefore be a priority to rectify.
Furthermore, it is incumbent on clinicians to provide writteninformation that is capacity appropriate – this includes maximisingthe ability for someone to consent as per the mental capacity act.Written information in an appropriate format can be a valuableadjunct to communication to both the carer and the patient.
Quality of patient information
It is acknowledged that many of the omissions found in theinformation sheets will already form part of the clinicalconsultation, however, written information is recommended.Descriptions of the sedation experience are given as part of thewritten information provided, and whilst one individual’sexperience of any form of sedation varies from another, a patient’sexpectations should be managed in a reasonable manner.Providing written information is one way of carrying this out inboth a measured, consistent and recorded way.
It is perhaps not surprising that when information sheets arewritten the benefits are emphasised over the risks – but in severalcases, there were no mention of risks at all (such as sedationfailure). Considering the Montgomery test level of consent,5 it isvital that all material risks that a reasonable patient would expectto know are included. It should be noted that risks and benefitswere well presented on the current patient information in use.
The alternative forms of sedation (or other methods of anxietycontrol) are again probably being discussed as part of the clinicalassessment, and are been offered by either availability or patientfactors. There were 2 sites that had information sheets that brieflymentioned general anaesthetic as an alternative. However, withpatient choice and informed consent being paramount, a written
summary of all alternatives would be useful for the patient, carer or guardian.
The subjective feelings, both during and after sedation, arerecommended to be included by the IACSD guidelines. This can beimproved, and may reinforce some of the sedations effects bysuggestion, as well as preparing the patient for their sedationjourney.
Contact details for the clinic attended were presented in mostcases, though the contact details on 5 information sheets wereusing out of date phone numbers. The details for which service tocontact if there were any out of hours’ concerns were very poor;although signposting occurs on some answer phone messages, it isconsidered best practice that emergency contact numbers aredetailed on the information we provide to patients, as this is likelytheir first port of call should a problem occur out of hours.
Pre-and post-sedation instructions for all available informationsheets were excellent, and presented in a clear format and will behopefully carried through to any new information leafletsdeveloped.
Information provision to parents/carers regarding pre-and post opinstructions is well presented across all information sheets. Theguidelines recommend that a description of the dental treatmentis provided, this would typically be individualised, and included onthe written consent. Therefore, it could be reasonably be arguedthat treatment details should only be included in broad terms oninformation sheets.
Actions taken• Revision of patient information relating to dentist
conscious sedation service wide• Creation of new “easy read” formats for sedation types used
in the service, samples of which can be seen in Figure 1developed in conjunction with learning disability team
• Creation of new age appropriate patient information –adapted from royal college guidelines
• Added to audit schedule for annual re-audit
Figure 1 – Samples of new “Easy Read” versions of writtenpatient information
""
"
"
& & & & & & & & & & & & &&
7 (" " " " " " " " " " " " " " " "
" " " " " " " " " " " " " " " "" " " " " " " " " " " " "" " " " " " " " " " " " " "
" " " " " " " " " " " "" " " " " " " " " " " "
" " " " " " " " " " " " "" " " " " " " "
"" ;.',6'16("A%1"0%,(72%9(";-6'.2%,"2,".$-">1%+2(2%,"%A")-,.'/"0'1-"kP,.-1,-.lC"P " " " " " " " " " " " "
" "
"
"" @AA27-"%A"0$2-A")-,.'/"@AA27-1"*,5/',6C"0%&&2((2%,2,5")-,.'/";-1+27-(M";-1+27-"( " " " " " " " " " " " "
" " " " " " "
"
""
"
"
& & & & & & & & & & & & &&
7 (" " " " " " " " " " " " " " " "
" " " " " " " " " " " " " " " "" " " " " " " " " " " " "" " " " " " " " " " " " " "
" " " " " " " " " " " "" " " " " " " " " " " "
" " " " " " " " " " " " "" " " " " " " "
"" ;.',6'16("A%1"0%,(72%9(";-6'.2%,"2,".$-">1%+2(2%,"%A")-,.'/"0'1-"kP,.-1,-.lC"P " " " " " " " " " " " "
" "
"
"" @AA27-"%A"0$2-A")-,.'/"@AA27-1"*,5/',6C"0%&&2((2%,2,5")-,.'/";-1+27-(M";-1+27-"( " " " " " " " " " " " "
" " " " " " "
"

23SAAD DIGEST | VOL.34 | 2018
REFEREED PAPER
ConclusionsAt the time of writing 2 years have passed since the publication ofthe IACSD guidance, which has been accepted as the standard UKwide with SDCEP publishing its report in early 2017. Bothacknowledge the advantages of written patient information aspart of the consent process. Patient literature is only a tool for
obtaining consent, and should always be used in conjunction witha full assessment and discussions with patients. Comprehension ofthe information provided should always be checked with thepertinent person. This audit brings into focus and areas wherewritten patient information may require changing to adhere tobest practice standards.
References1. Standards for Conscious Sedation in the Provision of Dental Care [Internet].
Intercolligate Advisory Committee for Sedation in Dentistry; 2015 [cited 2017 Jan9]. Available from: www.rcseng.ac.uk%2F-%2Fmedia%2Ffiles%2Frcs%2Ffds%2Fpublications%2Fdental-sedation-report-2015-web-v2.pdf%3Fla%3Den&usg=AFQjCNE1-RzABns-QObyD2EwYZr0wLSUDw
2. Office of Chief Dental Officer England. Commissioning Dental Services: Servicestandards for Conscious Sedation in a primary care setting [Internet]. NHSEngland; 2017 [cited 2017 Mar 9]. Available from:https://www.england.nhs.uk/wp-content/uploads/2017/06/dental-commissioning-guide-service-standards-conscious-sedation-2.pdf
3. The Safe Sedation Practice Scheme [Internet]. The Society for the Advancement ofAnaesthesia in Dentistry; 2015 [cited 2017 Mar 9]. Available from:https://www.saad.org.uk/images/Linked-Safe-Practice-Scheme-Website-L.pdf
4. Concious Sedation in Dentistry - Dental Clinical Guidance - 3rd Edition [Internet].Scottish Dental Clinical Effectiveness Programme; 2017 [cited 2107 Mar 9].Available from: http://www.sdcep.org.uk/wp-content/uploads/2017/07/SDCEP-Conscious-Sedation-Guidance.pdf
5. Consent – an update. Bright E, D’Cruz L, Milne E. BDJ. 2017 May 12; 222: 655–7
PRACTICE EVALUATIONS
Have your Practice evaluated in accordance with
the SAAD Safe Sedation Practice Scheme:
A Quality Assurance Programme for
Implementing National Standards in
Conscious Sedation for Dentistry in the UK.
The Evaluation document may be downloaded
from the Documents section of the SAAD website
www.saad.org.uk
For further details or to arrange an evaluation
Please contact [email protected]
""
"
"
& & & & & & & & & & & & &&
7 (" " " " " " " " " " " " " " " "
" " " " " " " " " " " " " " " "" " " " " " " " " " " " "" " " " " " " " " " " " " "
" " " " " " " " " " " "" " " " " " " " " " " "
" " " " " " " " " " " " "" " " " " " " "
"" ;.',6'16("A%1"0%,(72%9(";-6'.2%,"2,".$-">1%+2(2%,"%A")-,.'/"0'1-"kP,.-1,-.lC"P " " " " " " " " " " " "
" "
"
"" @AA27-"%A"0$2-A")-,.'/"@AA27-1"*,5/',6C"0%&&2((2%,2,5")-,.'/";-1+27-(M";-1+27-"( " " " " " " " " " " " "
" " " " " " "
"
""
"
"
& & & & & & & & & & & & &&
7 (" " " " " " " " " " " " " " " "
" " " " " " " " " " " " " " " "" " " " " " " " " " " " "" " " " " " " " " " " " " "
" " " " " " " " " " " "" " " " " " " " " " " "
" " " " " " " " " " " " "" " " " " " " "
"" ;.',6'16("A%1"0%,(72%9(";-6'.2%,"2,".$-">1%+2(2%,"%A")-,.'/"0'1-"kP,.-1,-.lC"P " " " " " " " " " " " "
" "
"
"" @AA27-"%A"0$2-A")-,.'/"@AA27-1"*,5/',6C"0%&&2((2%,2,5")-,.'/";-1+27-(M";-1+27-"( " " " " " " " " " " " "
" " " " " " "
"

24 SAAD DIGEST | VOL.34 | 2018
CASE STUDY
AbstractMidazolam is a short-acting benzodiazepine which is anxiolytic,causes anterograde amnesia and has sedative properties and istherefore commonly used in conscious sedation to undertakedental procedures. Midazolam has a high safety margin with fewsevere adverse effects with appropriate usage. This paper is thefirst to describe two cases of injection-site reactions followingintravenous delivery of Midazolam and aims to increase awarenessamongst clinicians and nurses undertaking sedation.
BackgroundCommon side-effects of Midazolam include drowsiness, confusion,euphoria as well as paradoxical reactions.1 Manufacturers have alsostated the potential for anaphylactic and anaphylactoid reactions,a case of which has been reported in the medical literature.2
However, an additional resultant skin reaction has also been listedas an adverse effect of Midazolam in the British NationalFormulary, which has been termed an injection-site reaction.1
Injection-site reactions are rare and are defined as localised skinreactions which occur following intravenous delivery of a drug.Symptoms may include erythema, itchiness or tenderness. Thefollowing paper details two cases of injection-site reactionassociated with intravenous Midazolam.
Case 1A 27 year old fit and well female was referred to the Oral SurgeryDepartment by her General Dental Practitioner for extraction ofthe lower left third molar, which was partially erupted and hadbeen causing recurrent pain. On examination, the lower left thirdmolar was partially erupted and horizontally impacted and she waslisted for extraction under local anaesthesia with intravenoussedation.
Ten minutes after delivery of the Midazolam, she developed a rashinitially at the cannula site which then spread superiorly to justabove the antecubital fossa. The skin was not itchy and thepatient’s observations were stable and there was no suggestion ofan anaphylactic type reaction. There was no tenderness topalpation in the antecubital fossa or in the surrounding tissues andthere was no evidence of extravasation. No further sedation wasadministered and within 15 minutes of intravenous administrationof the Midazolam, the skin had fully recovered. The extraction wasperformed uneventfully. The patient and escort were informedand reassured. Having checked the British National Formulary, itwas noted that this was an injection-site reaction secondary toMidazolam administration.
Follow-upThe patient was reviewed 2 weeks later and she confirmed nofurther skin reaction had arisen and she had remainedasymptomatic.
Case 2A 33 year old medically fit and well female was referred to the OralSurgery Department for extraction of her lower left third molardue to recurrent pericoronitis. On examination, the lower left thirdmolar was partially erupted and there was tenderness to palpationof the overlying operculum. The vertically impacted lower leftthird molar was scheduled to be extracted under local anaesthesiawith intravenous sedation.
Five minutes after intravenous administration of the Midazolam,the same type of reaction as in Case 1 also occurred. Raised wealsand erythema of the overlying skin above the antecubital fossadeveloped. There was no associated pruritis and again,observations were stable and there was no tenderness topalpation around the cannula site. As this was the second case inwhich this type of reaction had occurred, clinical photographswere taken. The reaction was transient following withholding offurther titration with Midazolam. Following further carefuladministration of Midazolam, the skin reaction occurred againwithin 5 minutes and disappeared within 10 minutes (Figures 1aand 1b). Treatment was performed uneventfully and the patientand her escort were informed and reassured.
Figure 1 a) Transient skin reaction b) Resolution of skin reaction
Figure 1a)
A Cautionary Tale of the Use of MidazolamTina Halai BDS MJDF RCS (Eng) Academic Clinical Fellow in Oral SurgeryDepartment of Oral Surgery, Eastman Dental Hospital, 256 Gray’s Inn Road, London WC1X 8LD
Josiah Eyeson LDS (Eng) FDSRCS (Eng) FDS (OS) PHD FHEAConsultant in Oral Surgery and Clinical LeadDepartment of Oral Surgery, Eastman Dental Hospital, 256 Gray’s Inn Road, London WC1X 8LD
Corresponding Author: [email protected]
Although these reactions are
r

25SAAD DIGEST | VOL.34 | 2018
CASE STUDYFigure 1b)
Follow-upThe patient was reviewed 1 week later and she confirmed therehad been no further rashes on her arms. Written consent wasobtained to use the photographs for publication. At this stage, thetourniquet was also placed above the antecubital fossa and was
left on for a time period equivalent to that required forvenepuncture. The patient was monitored for 15 minutesthereafter. There was no skin reaction which confirmed thetourniquet could not be implicated as the cause. Therefore thechanges in skin had occurred due to an injection-site reactionassociated with Midazolam.
ConclusionCases of injection-site reactions related to Midazolam have notbeen reported in the literature or by the National Patient SafetyAgency. Although these reactions are rare and are not concerning,any team undertaking sedation should always be vigilant whenassessing whether a reaction is occurring due to a hypersensitivityreaction, potentially due to anaphylaxis or if it is the rarer injection-site reaction.
References1. Joint Formulary Committee. British National Formulary September 2016 – March
2017. London: BMJ Group and Pharmaceutical Press, Chapter 4 Nervous System,pg. 310.
2. George C, Williams A. Anaphylaxis with midazolam: our experience. Indian JAnaesth. 2011; 55: 630–631.
Symposium & AGM 2018
Saturday 22 September 2018
Royal Society of Medicine, London
Details will be posted atwww.saad.org.uk

26 SAAD DIGEST | VOL.34 | 2018
OPINION
AbstractThe appropriate choice of local anaesthetic has a significantimpact on patient management. The implementation of articainein dental practice more than two decades ago vastly improvedclinical care, particularly when involving more complex dentalprocedures such as oral or periodontal surgery. Clinicians wouldlike to be supported by clear evidence regarding the indicationsand safety of local anaesthetics in dental patients. Somecontroversies associated with the use of articaine for inferioralveolar nerve block still exist1, despite the robust data confirmingthe safety of its use, speculating a sub-inflammatory local effectwithin soft tissues. Inflammatory responses play important role inthe development of peri-operative failure, post-operative pain andcomplications associated with LA’s action.2 The crucial questionarises whether some LA agents are superior to others, especiallyconsidering their biological interaction with the various cellscomposing the soft tissues, which are affected during regionallocal anaesthesia? What would be the optimal local anaesthetic touse in certain medical conditions, and when considering variousclinical aspects of dental care? Robust future meta-analyses, basedon both in vitro and in vivo studies, would produce unbiased andreliable data which could guide dental practitioners and help themto select the optimal LA for every individual case.
Our research team’s recent study3 evaluated, in vitro, the effect ofcommon local anaesthetics: lidocaine, articaine and mepivacaineon human fibroblasts which were exposed to differentconcentrations of each LA, ranging from 1.17 µg/ml to 150 µg/ml: a‘golden standard’ in dentistry 2% lidocaine with epinephrine1:80,000, 4% articaine with epinephrine 1:100,000 (forte), 4%articaine with epinephrine 1:200,000 and 3% plain mepivacainewithout vasoconstrictor agent. All investigated LAs did not inducesignificant cell death via the apoptosis/necrosis pathway, asrevealed by using a flow cytometry technique (annexin V–FITC andpropidium iodide). Mepivacaine at a concentration of 112.5 µg/mlslightly decreased cell viability. Within the limitations of our study(selected LAs concentrations) a concentration-dependent cytotoxiceffect was not observed for any of the LAs evaluated, however, thisresult could be explained by the relatively low LA doses used inthe experiments. The rather unexpected results showed thatapparently articaine with adrenaline 1:100,000 diminished thepercentage of apoptotic cells, revealing a slightly ‘protective’ actionwith potential 'enhancement' of cell viability. No significantdifferences were noticed between LAs in terms of reactive oxygenspecies (ROS) production, apart from articaine ‘forte’, which mildlystimulated an intracellular level of ROS production at the highestconcentration. These results of our study are partially consistentwith the findings demonstrated by Azuma and Ohura4 who statedthat epinephrine may stimulate the production of superoxideanion and inhibit the production of hydrogen peroxide. The sameresults were obtained by them for lidocaine with epinephrine.Mikawa et al. observed an inhibitory effect of lidocaine andmepivacaine for the production of ROS by neutrophils.5
Interestingly, up-regulation of pro-inflammatory cytokinesinterleukine 6 and interleukine 8 was observed only formepivacaine in our experiments. On the contrary, for both articaineand lidocaine an attenuation of both gene expressions waselucidated. These results are similar to those obtained by Gallos etal6 who confirmed that lidocaine may reduce inflammatorymarkers, including cytokines and chemokines. Of interest, otherstudies have indicated that lidocaine may selectively up-regulatepro-inflammatory proteins and down-regulate anti-inflammatorymolecules.7 Taking into consideration in vivo studies, anintravenous infusion of lidocaine significantly relieves post-operative pain and decreases immune alterations associated withsurgery by reduction of production of IL-1ra and IL-6 cytokines.8
Generally, local anaesthetics are able to inhibit local inflammatoryresponses without major impact on host immunity9, as shown byCassuto et al. who investigated in vitro that lidocaine decreasedTNF-α-induced surface expression of CD11b/CD18 onneutrophils.10
A pioneer in vitro neurotoxicity study carried out by Kasaba at al.using cultured neurons exposed to the different LAs: procaine,mepivacaine, ropivacaine, bupivacaine, lidocaine, tetracaine, anddibucaine elucidated that lidocaine was more toxic than the othertested LAs, and that mepivacaine had the least-cytotoxic effects oncone growth of neuron cells compared to the other localanaesthetics.11 Radwan et al. observed the morphological changesin growing neurons induced by lidocaine and mepivacaine, forwhich the neurotoxic effect was significantly higher in comparisonto the control values.12 On the other hand, the accumulated datarelated to the life science field may also indicate that localanaesthetics possess a range of potentially anti-inflammatoryactions through their impact on the immune system.10 Additionally,in vitro experiments demonstrated that lidocaine has a dose-dependent anti-proliferative effect on hepatocarcinoma cells.13 Ithas been proved that local anaesthetics may interfere with somelevels of the ‘inflammatory cascade’ producing a ‘protective effect’and this is a possible explanation of their action. The cellularmechanisms of action can be associated with the impact on thecell membrane proteins/lipids, altering cell metabolism andmigration.14
In this context, within the limitations of in vitro study, weelucidated that local anaesthetic agents are not cytotoxic tohuman fibroblasts. None of the LAs was found to be more toxicthan others. Our results are in agreement with other reportsstating that articaine does not have mutagenic potential up to themaximum tolerated dose level and that the local tolerance ofarticaine is very high.15 Interestingly, according to the newest study,among dental anaesthetics, articaine is the least neurotoxic, whilstmepivacaine, prilocaine and lidocaine were identified as LAs withmedium neurotoxicity.16 With regards to apoptotic induction andpotency caused by different local anaesthetics, the cytotoxicity ofarticaine is lower compared to lidocaine and mepivacaine.17
Cytotoxicity of Local AnaestheticsArkadiusz Dziedzic DDS PhDDepartment of Conservative Dentistry with EndodonticsMedical University of Silesia
Corresponding Author: [email protected]

27SAAD DIGEST | VOL.34 | 2018
OPINIONWardenhausen et al. observed a concentration-dependentcytotoxicity to non-neuronal T-lymphoma cells, including cellnecrosis and apoptosis, for various investigated LAs, based on LC50value (lethal concentration required to kill 50% of the exposedcells). These authors noticed the variability in the level of localanaesthetics’ toxicity, in the following decreasing order: tetracaine> bupivacaine > ropivacaine > prilocaine > procaine > lidocaine >articaine > mepivacaine. Interestingly, they also concluded thatstructural factors such as ester or amide linkage did not have anyimpact on the level of cytotoxicity.18
Results of the other non-clinical studies using mesenchymal stemcells, which play an essential role in healing following surgery,clearly revealed that lidocaine has the most noticeableconcentration-related detrimental effects on stem cell viability.19
Similar results were obtained by the research team of Rahnama etal. who found that lidocaine could significantly decreasemesenchymal stem cell viability.20 Another team led by Dregalla etal. found that exposure of human mesenchymal stem cells to LAshas an impact on their viability and adhesion and that amide-typelidocaine may stimulate cell apoptosis in a time- and dose-dependent manner.21
The main clinical significance in dental practice, is the effect oflocal anaesthesia on post-operative healing in the case of surgicalinterventions, whilst their influence on systemic reactions dependsupon the direct interaction of the LA with vital cellularcomponents. Our preliminary research, which has been providingevidence of the non-cytotoxic activity of the common LAs towardsfibroblasts, also has important clinical implications, confirming aminimal risk of post-operative local complications such as pain,neurological problems and trismus, confirming the safety of LAs.Our findings also support oral and maxillofacial surgeons bydemonstrating a safe interaction between an LA agent andconnective tissue cells – fibroblasts, with no major impacts on thewound healing process. Pre-clinical data indicate that articaine canbe considered a safe local anaesthetic, and this finding hassignificant clinical relevance and practical implications, whenselecting a local anaesthesia for dentistry. However, these cellculture experiments and non-clinical studies must be re-validatedin the clinical/physiological environment due to the major fact thatan LA’s pharmacokinetics in in vivo conditions may not be fullyreplicated clinically. Advances in drug biotechnology appears topromise exciting results for new LA formulations in future.Cytotoxicity assays confirmed that the encapsulation of articaine(nanocapsules, nanovesicles) reduced its ‘standard’ toxicity whenlinked to the free LA molecules.22 It means that nano-carriersystems can be potentially used in practical applications in eg.medically compromised patients who have an increased risk ofsystemic LA-associated complications.
The conclusions from clinical studies show that articaine LA withadrenaline 1:200,000 is generally more strongly recommended foruse with dental patients as it is considered safer than lidocainewith adrenaline 1:80,000 and articaine with higher concentrationof adrenaline 1:100,000.23 The main advantage is that currentlyavailable cartridges containing articaine have a lowerconcentration of adrenaline compared to lidocaine, the onset ofanaesthesia is more rapid due to better absorption/diffusion, and itis a safer option for patients with liver disfunction due to plasmametabolism. Kambalimath et al. concluded that lidocaine withadrenaline 1:80,000 causes more alterations in the cardiovascularsystem of elderly patients with medical conditions.24 Due to the
fact that the articaine molecule contains an ester group andtherefore is efficiently hydrolysed by plasma esterases25, its half-lifeelimination is 4-times shorter in comparison to lidocaine (approx20 min vs. appox 90 min. This means additional articaine agent re-injection is much safer, because the first LA dose will bemetabolised in the patient’s blood almost completely after 30min.26 Additionally, a specific intra-ligamentary anaesthesiaprocedure (PDL) using articaine seems to have distinct advantagesand is more effective in certain circumstances. The assessment ofthe interaction of lidocaine, articaine and mepivacaine with thecentral nervous system stimulant pentyl-enetetrazole using ananimal model showed that LAs did not induce seizures, and thatarticaine is likely to be the safest ‘LA of choice’ for patients withepilepsy.27
In regards to hypothetical prolonged anaesthesia following IANBadministration of articaine, conclusions drawn by authors in themost recent article from 201728 have confirmed that articaine doesnot have a higher (neuro)toxicity when compared with otheramide anaesthetics. According to them, the local anaesthesiaefficiency of articaine is not significantly different to other short-acting LAs like lidocaineand prilocaine and there is no conclusiveevidence demonstrating above-average neurotoxicity. Tosummarise, no sound scientific evidence can be provided tosupport the statement that articaine is linked to an increased riskof local neurological complications (paraesthesia). Undoubtedly, itis essential to indicate a clear causative factor or range of factorsresponsible for LA-related complications, focusing on well-designed, controlled studies and analysing currently available datafrom both in vitro and in vivo studies.
References:1. van Eeden S P, Patel M F. Prolonged paraesthesia following inferior alveolar nerve
block using articaine. Br J Oral Maxillofac Surg. 2002; 40: 519-20.
2. Hollmann MW, Durieux ME. Local anesthetics and the inflammatory response: anew therapeutic indication? Anesthesiology. 2000; 93 :858-75.
3. Dziedzic A. The comparative effects of common local anaesthetics on humanfibroblasts. Annual Meeting, Society for the Advancement of Anaesthesia inDentistry (poster presentation), 2016, London.
4. Azuma Y, Ohura K. Immunological modulation by lidocaine-epinephrine andprilocaine-felypressin on the functions related to natural immunity in neutrophilsand macrophages. Curr Drug Targets Immune Endocr Metabol Disord. 2004; 4: 29-36.
5. Mikawa K, Akamatsu H, Nishina K, Shiga M, Maekawa N, Obara H, Niwa Y. Inhibitoryeffect of local anaesthetics on reactive oxygen species production by humanneutrophils. Acta Anaesthesiol Scand. 1997; 41: 524-8.
6. Gallos G, Jones DR, Nasr SH, Emala CW, Lee HT. Local anesthetics reduce mortalityand protect against renal and hepatic dysfunction in murine septic peritonitis.Anesthesiology. 2004, 101: 902–911.
7. Chiang N, Schwab JM, Fredman G, Kasuga K, Gelman S, Serhan CN. AnestheticsImpact the Resolution of Inflammation. 2008; PLoS ONE 3: e1879.
8. Yardeni IZ, Beilin B, Mayburd E, Levinson Y, Bessler H. The effect of perioperativeintravenous lidocaine on postoperative pain and immune function. Anesth Analg.2009; 109: 1464-9.
9. Cruz FF, Rocco PRM, Pelosi P. Anti-inflammatory properties of anesthetic agents.Critical Care. 2017; 21:67. doi:10.1186/s13054-017-1645-x.
10. Cassuto J, Sinclair R, Bonderovic M. Anti-inflammatory properties of localanesthetics and their present and potential clinical implications. ActaAnaesthesiol Scand. 2006; 50; 265-82.
11. Kasaba T, Onizuka S, Takasaki M. Procaine and mepivacaine have less toxicity invitro than other clinically used local anesthetics. Anesth Analg. 2003; 97: 85-90.
12. Radwan IA, Saito S, Goto F. The neurotoxicity of local anesthetics on growingneurons: a comparative study of lidocaine, bupivacaine, mepivacaine, andropivacaine. Anesth Analg. 2002; 94 : 319-24.
13. Jurj A, Tomuleasa C, Tat TT, Berindan-Neagoe I, Vesa SV, Ionescu DC.

28 SAAD DIGEST | VOL.34 | 2018
OPINIONAntiproliferative and Apoptotic Effects of Lidocaine on Human HepatocarcinomaCells. A preliminary study. J Gastrointestin Liver Dis. 2017; 26: 45-50.
14. Nellgard P, Jonsson A, Bojo L, Tarnow P, Cassuto J: Small-bowel obstruction andthe effects of lidocaine, atropine and hexamethonium on inflammation and fluidlosses. Acta Anaesthesiol Scand 1996; 40: 287.
15. Leuschner J, Leblanc D. Studies on the toxicological profile of the localanaesthetic articaine. Arzneimittelforschung. 1999; 49: 126-32.
16. Malet A, Faure MO, Deletage N, Pereira B, Haas J, Lambert G. The comparativecytotoxic effects of different local anesthetics on a human neuroblastoma cellline. Anesth Analg. 2015;120: 589-96.
17. Werdehausen R, Fazeli S, Braun S, Hermanns H, Essmann F, Hollmann MW, Bauer I,and Stevens MF. Apoptosis induction by different local anesthetics in aneuroblastoma cell line. Br J Anaesth 2009; 103: 711-8.
18. Werdehausen R, Braun S, Fazeli S, Hermanns H, Hollmann MW, Bauer I, Stevens MF.Lipophilicity but not stereospecificity is a major determinant of local anaesthetic-induced cytotoxicity in human T-lymphoma cells. Eur J Anaesthesiol. 2012; 29: 35-41.
19. Wu T, Smith J, Nie H, Wang Z, Erwin PJ, van Wijnen AJ, Qu W. Cytotoxicity of LocalAnesthetics in Mesenchymal Stem Cells. Am J Phys Med Rehabil. 2018; 97: 50-55.
20. Rahnama R1, Wang M, Dang AC, Kim HT, Kuo AC. Cytotoxicity of local anestheticson human mesenchymal stem cells. J Bone Joint Surg Am. 2013; 95: 132-7.
21. Dregalla RC, Lyons NF, Reischling PD, Centeno CJ. Amide-Type Local Anestheticsand Human Mesenchymal Stem Cells: Clinical Implications for Stem Cell Therapy.Stem Cells Translational Medicine. 2014; 3: 365-374.
22. Silva de Melo NF, Campos EV, Gonçalves CM, de Paula E, Pasquoto T, de Lima R,Rosa AH, Fraceto LF. Development of hydrophilic nanocarriers for the chargedform of the local anesthetic articaine. Colloids Surf B: Biointerfaces. 2014; 121: 66-73.
23. Abu-Mostafa, N., Al-Showaikhat, F., Al-Shubbar, F, Al-Zawad K, Al-Zawad F.Hemodynamic changes following injection of local anesthetics with differentconcentrations of epinephrine during simple tooth extraction: A prospectiverandomized clinical trial. J Clin Exp Dent, 2105; 7: e471-e476.
24. Kambalimath, DH, Dolas, RS, Kambalimath, HV, Agrawal, SM. Efficacy of 4 %Articaine and 2 % Lidocaine: A clinical study. J Max Oral Surg 2013; 12: 3-10.
25. Oertel R, Rahn R, Kirch W. Clinical pharmacokinetics of articaine. ClinPharmacokinet 1997; 33: 417-425.
26. Isen DA. Articaine: Pharmacology and clinical use of a recently approved localanesthetic. Dent Today 2000; 19: 72-77.
27. Zółkowska D, Pikuła A, Borzecki A, Sieklucka-Dziuba M. Interaction between localanesthetics and centrally acting antihypertensive drugs. Ann Univ Mariae CurieSklodowska Med. 2002; 57: 569-73.
28. Hopman AJG, Baart JA, Brand HS. Articaine and neurotoxicity – a review. Br Dent J2017; 223: 501–506.
The SAAD Editorial Boardwould welcome receivingcase reports of interest
and original papersfor publication
in the SAAD Digest
Submission deadline 31st July 2018
Please refer to the guidelines for authors on page 89
Contact - [email protected]

29SAAD DIGEST | VOL.34 | 2018
JOURNAL SCAN
The Odyssey of Dental Anxiety: From Prehistory tothe Present. A Narrative Review
Facco E1, 2 and Zanette G2, 3
1 Studium Patavinum, University of Padua, Padua, Italy2 Franco Granone Institute – Italian Centre of Clinical & ExperimentalHypnosis (CIICS), Turin, Italy3 Chair of Dental Anaesthesia, Department of Neurosciences,University of Padua, Padua, Italy
Front. Psychol 2017; 8:1155. doi: 10.3389/fpsyg.2017.01155
AbstractDental anxiety (DA) can be considered as a universal phenomenonwith a high prevalence worldwide; DA and pain are also the maincauses for emergencies in the dental setting, so their prevention isan essential part of patient safety and overall quality of care. DAand its consequences are closely related to the fight-or-flightreaction and it seems reasonable to argue that the odyssey of DAbegan way back in the distant past, and has since probably evolvedin parallel with the development of fight-or-flight reactions, implicitmemory and knowledge, and ultimately consciousness. Basicemotions are related to survival functions in an inseparablepsychosomatic unity that enable an immediate response to criticalsituations rather than generating knowledge, which is why manyanxious patients are unaware of the cause of their anxiety.
The wealth of data now available makes it definitively clear thatthe origin of DA is multidimensional and includes bothendogenous and exogenous causes. Several psychological ailmentssuch as low self-esteem, general fearfulness, conduct disorder,agoraphobia, simple phobia, alcohol dependence, or multiplemental disorders are more frequent in patients with high DA.
The exogenous factors include conditioned fear (yielded byprevious bad experiences or information), fear of somaticintraoperative reactions and distrust of dental professionals; thelatter, in turn, is usually caused by dentists’ and/or physicians’inappropriate behaviour and traumatic dental treatments, leadingto patient’s helplessness, threat of autonomy loss and violation. Thefear these situations may induce throws us back to ancient times,
when our ancestors had to face and react to dangers andpredators on a daily basis.
Reviewer’s commentsThis is a fascinating article examining the history of fear in all itsaspects and relating it to the psychology, pathophysiology,assessment and management of dentophobia in the modern age.The authors mention that dental care was introduced as long agoas the Neolithic period (archaeology has revealed that a 6500 year-old tooth had been restored with a beeswax ‘filling’) and arguethat it is reasonable to assume that the odyssey of DA must alsohave originated at that time because of the ‘indissoluble marriage’of dentistry with pain. They also outline the development ofpharmacological techniques to manage the symptoms includingthe use of psychotropic plants ‘which were capable of takinghumans to realms of ethereal wonder’. They also describe the Alepposponge used by Arab physicians to induce ‘sedation and a sort ofinhalational anaesthesia.’
Delving even further back into the birth of anxiety, the authorsexamine the controversial ‘Sapient Paradox’ where there was anapparent great change in human consciousness, and arguably, inhuman emotions and anxieties, about 100,000 years ago. Theparadox stems from the observation that our DNA was much thesame across the age since that period, while the explosion ofhuman culture only dates back from about 20,000 years ago. It ishard to explain this time lag on genetic grounds only.
From various sources of information, they state ‘Judging from theabove-mentioned data, it seems reasonable to argue that forms ofhuman anxiety—including DA—can be seen as a sort of odysseybegun in prehistory, when our ancestors were faced many times aday with danger, pain, stress, and the related fight-or-flightresponses, as well as with diseases, toothache and some sort ofdental treatments. Animals clearly know fear too, but humanbeings are often reluctant to admit that they belong to the animalkingdom. On the other hand, human anxiety also entails a muchgreater use of memory and imagination with respect to animals,enabling one to move backwards and forwards in time, a mindfaculty related to the human’s well-developed default modenetwork.
A Synopsis of articles of interest from the last twelve monthsto inspire further reading
Fareed Ahmad Rosie WhatlingJennifer HareDev Mahtani

30 SAAD DIGEST | VOL.34 | 2018
JOURNAL SCANFurther, they state a home truth in that the ‘data shows the crucialrole played by health professionals in the pathophysiology of DA,by leading to patients feeling unbearably helpless, beingthreatened with the loss of their autonomy, and violated, yieldingavoidable suffering, pain, and opening the doors to medicalemergencies. Thus, dentists and physicians look like the two -facedJanus, the Ancient Roman god of time in the past and future, inwar and peace (the month of January is named after him): theymay be gentle and protective experts providing safe and painlesscare, or turn into torturers capable of causing great suffering. Theirinappropriate behaviour can exacerbate existing anxiety disordersor trigger a new form of anguish (anxiety, phobia, and PTSD) thatmay persist for life if not properly managed.’
The focus of the article remains on appreciating the stressfulscenario of dentistry which demands an appropriate managementof anxiety, pain and the related physical reactions. In this regard,the patient centred approach is the ethical gold standard inmodern dentistry in which pharmacological anxiolysis can alsoplay a key role.
FA
Can we safely avoid fasting before abortions withlow-dose procedural sedation? A retrospectivecohort chart review of anaesthesia-relatedcomplications in 47,748 abortions
Wiebe E Ra, Byczko Ba, Kaczorowski Jb, McLane A Lc
aDepartment of Family Medicine, University of British Columbia,Vancouver, BC, Canada V5Z1H9b Département de médicine familial et d'urgence, Université deMontréal, Montréal, CanadacThompson Rivers University, Kamloops, BC, Canada Contraception 2013; 87: 51-54
Abstract
Background: Some licensing authorities require fasting beforeabortions under intravenous sedation to avoid aspiration of gastriccontents. This study was conducted to estimate the incidence ofanaesthesia-related complications in women undergoingabortions without pre-procedure fasting.
Study Design: This was a retrospective cohort chart review ofpatients having abortions with both fentanyl and midazolam attwo urban freestanding abortion clinics with routine policy ofadvising women to eat a light meal before the procedure.
Results: There were no reports of anaesthesia-relatedcomplications in the 47,748 charts reviewed from 1998 to 2010.Applying Hanley's formula for rare events that have not occurred,the upper 95% confidence interval for the true incidence ofanaesthesia-related complications for women having abortionunder low-dose procedural sedation without fasting, wasestimated to be 0.00006%.
Conclusions: This large retrospective cohort chart reviewidentified no complications related to low-dose proceduralsedation in over 47,000 consecutive non-fasting patients havingabortions through 18 weeks' gestation. Eliminating the
requirement to fast would decrease unnecessary stress andunpleasant symptoms without increase in the anaesthesia-relatedcomplications for women having abortions.
Reviewer’s Comments:The need for fasting prior to dental treatment under conscioussedation is the subject of constant discussion and debate becausealthough airway reflexes are assumed to be maintained, this doesnot consider the potential for inadvertent over-sedation and theloss of protective airway reflexes.
This review showed the benefits of minimising fasting includeimproved postoperative well-being and some clinical outcomes,such as reduced post-operative hospital stay, reduced dehydrationand improved muscle strength and mass. In a study of dentalsurgery patients, 79% reported unpleasant symptoms from pre-procedure fasting. In a study of pregnant patients in labour, 27% ofwomen considered restriction of food in labour “moderately” to“most” stressful; 57% found restriction of fluids to be “moderately”to “most” stressful.
Although the evidence from this study seems to be overwhelmingthat fasting need not be imposed on patients undergoingprocedures under conscious sedation, it has to be taken intoaccount that the cases were treated in a hospital setting wherebackup facilities would be readily available to support thesedationist in an unlikely aspiration event. In any case, working inthe oral environment is completely different from abdominalsurgery, it can be tricky if access is limited, or if the patient suffersfrom a gag reflex - and evoking a retching response is always arisk - even under sedation.
The reviewers highlight the stress caused to patients by imposinga fasting rule, especially the restriction of fluids and state that‘minimal’ fasting i.e. having a light meal before the procedure isbeneficial. Reducing the stress element is very relevant to themanagement of the dentophobic patient and therefore the dentalpractitioner may consider adjusting the fasting instructions on acase to case basis. The simple example may be permitting a patientto have a sip or more of water on a hot summer’s day or ensuringthat a diet-controlled diabetic patient does have a light meal acouple of hours before the appointment.
Nevertheless, it is essential to keep in mind NICE guidelines whichspecify that ‘Clinicians who choose to sedate patients withoutfasting should be prepared to justify this choice.’
FA
Perception of simulation training in emergenciesfor dental sedation practitioners
Hadfield A, Thompson S, Hall J and Diaz-Navarro C.Cardiff and Vale University Health Board, Cardiff University, UKThe Clinical Teacher 2017; 13: 1-5
Abstract
Background: Simulation education is an important part of healthcare education and training. There is growing evidence to supportthe usefulness of simulation, especially in training for infrequently

31SAAD DIGEST | VOL.34 | 2018
JOURNAL SCANoccurring situations, such as medical emergencies seen by dentalpractitioners. There are, however, few data on the longer-termeffects of simulation, including usefulness, relevance, emotionaleffect and ability to affect changes to daily practice.
Methods: Dentists and dental nurses who had undergonesimulation training in medical emergencies for dental sedationpractitioners undertook a semi-structured interview about theirperception of the simulation experience. They exploredrecollection of the experience and its emotional weight,perception of usefulness and relevance, specific learning outcomesand changes to practice prompted by the simulation session.
Results: Participants reported finding the simulation sessionsworthwhile, realistic, challenging and almost universallyemotionally positive. In situ simulation training was particularlywell received, both in terms of realism, as well as identifying systemflaws in emergency drugs and equipment. Participants reportedgaining both increased clinical knowledge and human factorsskills, which were reflected in subsequent changes to theirpractice.
Discussion: The results support the usefulness and applicability ofsimulation education to training in medical emergencies for dentalsedation practitioners. In particular, specific benefits reported fromin situ sessions and in human factors concepts, prompts a furtherreview of the structure of teaching to maximise the benefit toparticipants.
Reviewer’s commentsThe authors state that although there is no specific dataquantifying incidents under dental sedation, up to 70% of UKdentists have encountered a medical emergency. However, lessthan 30% of newly qualified dentists feel ‘well’ or ‘fairly well’prepared for an emergency situation. Training for emergencies ismandatory for all dental clinical staff and although these exercisesdo improve confidence immediately afterwards, there is littlepublished research on how participants perceive the sessions at alater date. This, therefore, is an interesting study, albeit limited bythe small number of participants, of the emotional and other longterm effects of both simulation and in situ training in terms ofperception, relevance and learning.
Nine out of 13 candidates perceived that their main learningoutcome was increased clinical knowledge, yet the majority ofchanges to practice they described seemed to have resulted froman improvement in non-technical skills. Therefore, the studysuggests that it may be more efficient to focus these sessions onhuman factor aspects in terms of boosting confidence and self-esteem and thereby facilitating better retention of the subjectmatter. Feedback was particularly positive for the in situ sessions,which seemed to be observed as more realistic than training in thesimulation centre. This reinforces the requirement for regular in-house practice sessions where familiarity with one’s usual place ofwork assists team dynamics and identifies any weaknesses in thelocal emergency set-up and protocol.
In conclusion, this study suggests that simulation education inmedical emergencies for dental sedation practitioners isworthwhile, relevant, and provides improvements in clinicalknowledge and non-technical skills. It also identifies potentialadvantages of in situ simulation, which include realism, team
training and systems testing. The authors acknowledge that furtherstudies would be useful to fully assess the retention of knowledgefrom the sessions, and the impact of simulation learningexperiences on everyday practice.
FA
Pulmonary aspiration during procedural sedation:a comprehensive systematic review
Green S M, Mason K P, Krauss B S,Br J Anaesth 2017; 118: 344-54
Background: Pulmonary aspiration is a rare but potentially life-threatening complication of sedation and general anaesthesia. Ithas been extensively studied in general anaesthesia but much lessis known about aspiration during procedural sedation.
Aim/Objectives: This is the first systematic review of all publishedinstances of aspiration during procedural sedation, detailing thecircumstances and outcomes of these events.
Methods: A comprehensive, systematic review of PubMed, Web ofScience, and the Cochrane Library from January 1985 to May 2016.
Results: 35 articles found describing one or more occurrences ofpulmonary aspiration during procedural sedation.- Gastrointestinal endoscopy procedures: 292 occurrences, with
eight deaths.- Non-endoscopy procedures: 34 occurrences, with a single
death in a moribund patient, full recovery in 31, and unknownrecovery status in two.
- Propofol was the most common sedative agent used in reportsof aspiration.
- No occurrences of aspiration in non-fasted patients receivingsedation for non-endoscopy procedures.
Conclusions: The data suggests that aspiration during proceduralsedation is rare, idiosyncratic, and typically benign. Very fewoccurrences of aspiration were identified in non-endoscopicprocedural sedation, with most making a full recovery.
Reviewer’s commentsThis is a comprehensive review of the literature that has identifiedvery few occurrences of pulmonary aspiration during proceduralsedation. Whilst the review format is not designed to quantify riskfactors or prevalence of aspiration, the authors make severallogical points of interest:(i) The nature of gastrointestinal endoscopy procedures has an
inherently greater risk of aspiration.(ii) The finding that propofol was the most common sedative
agent used in cases of aspiration reflects a target of ‘deep’sedation, supporting the general assumption that this state hasa higher aspiration risk than ‘moderate’ or ‘mild’ sedation.
(iii) There is no clear association between fasting (or lack of it) andthe incidence of aspiration, particularly in non-endoscopyprocedures.
(iv) Underlying co-morbidities were present in the majority ofaspiration occurrences and are known to increase risk.However, many patients with similar conditions do not aspirate

32 SAAD DIGEST | VOL.34 | 2018
JOURNAL SCANduring sedation, thus making underlying illness anunpredictable risk factor.
(v) The prevalence of aspiration in the literature for proceduralsedation is lower than that reported with general anaesthesia;estimated to be one-third to one-half that of generalanaesthesia
A review of this nature is clearly limited by publication bias andone must be mindful that the lack of published reports does notequate to lack of occurrence. Nevertheless, considering thatprocedural sedation is administered millions of times annuallyworldwide, judging from the published literature, the incidence ofaspiration during procedural sedation is extremely rare.
Finally, it is noteworthy that none of the 326 published incidencesof aspiration occurred during dental procedures, in keeping withthe widely held view that procedural sedation is a very safetechnique when used correctly in appropriately selected patientsby appropriately trained personnel.
DM
Dental procedures, antibiotic prophylaxis, andendocarditis among people with prosthetic heartvalves: nationwide population based cohort and acase crossover study
Tubiana S, Blotiere P, Hoen B, Lesclous P, Millot S, Rudant J, Weill A,Coste J, Alla F, Duval XBr Med J 2017; 358: j3776.
Background: Infective endocarditis is a rare but severe diseasewith high morbidity and mortality (40% at five years). The efficacyof antibiotic prophylaxis in patients with predisposing cardiacconditions undergoing invasive dental procedures is not clear;current data suggest that everyday life bacteraemia (e.g. fromtooth brushing, chewing) is more likely to be responsible forinfective endocarditis than that caused by invasive dentalprocedures.
Aim/Objectives: To assess the relation between invasive dentalprocedures and infective endocarditis associated with oralstreptococci in people with prosthetic heart valves.
Methods: This was a nationwide population study based on theFrench national health insurance administrative data and nationalhospital discharge database; included all adults who underwentinsertion of prosthetic heart valves between July 2008 and July2014.
Cohort Study: Assessed and compared the incidence of oralstreptococcal infective endocarditis – with or without dentalprocedures; invasive or non-invasive procedures; with or withoutantibiotic prophylaxis.
Case crossover study: Looked at all cases of oral streptococcalinfective endocarditis in patients with a prosthetic heart valve.Cases acted as their own controls when comparing exposure toinvasive dental procedures during the three-month period
preceding oral streptococcal infective endocarditis (case period)with three earlier control periods.
Results: Cohort of 138,876 people with prosthetic heart valves:- 267 cases of oral streptococcal infective endocarditis during a
median follow-up of 1.7 years (incidence rate 93.7 per 100,000person years, 95% confidence interval 82.4 to 104.9).
- The overall rate of oral streptococcal infective endocarditis was1.4 cases per 10,000 invasive dental procedures.
- In comparison to patients with no exposure to dentaltreatment, there was no statistically significant difference in therate of infective endocarditis during the three months after aninvasive dental procedure (relative rate 1.25, 95% confidenceinterval 0.82 to 1.82; P=0.26); nor after an invasive dentalprocedure without antibiotic prophylaxis (1.57, 0.90 to 2.53;P=0.08).
- The difference between invasive and non-invasive dentalprocedures was also not statistically significant.
The case crossover study included 648 cases of oral streptococcalinfective endocarditis:- Exposure to invasive dental procedures was more frequent
during case periods than during matched control periods(5.1% v 3.2%; odds ratio 1.66, 95% confidence interval 1.05 to2.63; P=0.03).
- There were no statistically significant differences in odds ratioswhether or not patients received antibiotic prophylaxis (forboth invasive and non-invasive dental procedures).
Conclusions: Only the case crossover study showed statisticalsignificance associating invasive dental procedures and oralstreptococcal infective endocarditis. However, both suggest thatinvasive dental procedures may contribute to the development ofinfective endocarditis in adults with prosthetic heart valves.
Reviewer’s commentsPatients with prosthetic heart valves are at higher risk fordeveloping infective endocarditis and have historically receivedantibiotic prophylaxis during invasive dental procedures. However,there is a paucity of scientific evidence for both the associationbetween dental procedures and oral streptococcal infectiveendocarditis, as well as the efficacy of antibiotic prophylaxis. Thishas led to the development of different guidelines over the pastdecade: (1) NICE recommends prophylaxis is not ‘routinely’required; (2) the European Society of Cardiology (ESC) andAmerican Heart Association (AHA) continue to recommendantibiotic prophylaxis in patients at high risk of infectiveendocarditis (includes prosthetic heart valves) undergoing invasivedental procedures. In addition, there seems to be a growing trendtowards an increased incidence of infective endocarditis followingthe guideline changes. It is no wonder that healthcare practitionersare now confused about the role of antibiotic prophylaxis, apossible reason why even within this study, only about half thepatients having invasive dental procedures actually receivedantibiotic prophylaxis!
This is a well-conducted database study with a very large cohort ofpatients, essential when considering the low incidence of infectiveendocarditis.- Neither the cohort nor case crossover studies demonstrated a
statistically significant reduction in the rate of infectiveendocarditis with the use of antibiotic prophylaxis. However,

JOURNAL SCAN
33SAAD DIGEST | VOL.34 | 2018
the authors do admit that the study was probablyunderpowered for this subgroup analysis.
- Only one of the two studies (the case crossover) showedstatistical significance for an association between invasivedental procedures and oral streptococcal infectiveendocarditis. However, even then, the rate of invasive dentalprocedures during the three months preceding oralstreptococcal infective endocarditis was low at only 5.1%.Whilst this shows an association between the two, themagnitude of this association remains uncertain.
- The incidence of oral streptococcal infective endocarditis inrelation to everyday life bacteraemia (e.g. tooth brushing,chewing) was 94.6 per 100,000 person years (95% confidenceinterval 82.5 to 106.6) adding to the evidence that most casesof oral streptococcal infective endocarditis in patients withprosthetic heart valves are most likely related to this.
Although this study doesn’t definitively associate invasive dentalprocedures with infective endocarditis, or demonstrate a benefitwith antibiotic prophylaxis, it does add to the body of literatureshowing a trend in this direction. Until further evidence isavailable, I would personally recommend the use of antibioticprophylaxis as per the ESC/AHA guidelines … at least until Brexit iscomplete!
DM
A novel way to secure the laryngeal mask airwayduring oral surgery procedures.
Mireles R, Devgun R, Tucker B, Votta T, Chahal P, Ramsdell R, Heard CAnesthesia & Analgesia 2017, 124: 1836-8.
Background: The flexible/reinforced Laryngeal Mask Airway (LMA)is widely used to manage the airway during general anaesthesiafor oral surgery. This is commonly secured in place by externaltapes/ties or mouth gag, both of which can interfere with surgicalaccess. Alternatively, the LMA is left unsecured so it can be movedby the surgeon, with the attendant risks of dislodgement.
Aim/Objectives: Design and pilot of a novel device – the LMA-PROP – a modified mouth prop that also allows the flexible LMA tobe snapped in and secured, alleviating positioning concerns.
Methods: The LMA-PROP was custom-manufactured using siliconeelastomer to fit LMA sizes 3 and 4. The device was piloted in aseries of healthy patients (14 years and over) undergoing electivethird molar extractions under general anaesthesia. The LMA-PROPis placed between the upper and lower molars, providing surgicalexposure, and the flexible LMA is then snapped into a groovemoulded on the lingual side of the LMA-PROP. If use of the LMA orLMA-PROP was unsatisfactory, it was removed and the patient wasintubated.
Results: The LMA-PROP was evaluated in ten patients between theages of 16 and 34 years. Several changes were made to the LMA-PROP during the course of the pilot to improve functionality. TheLMA-PROP was unsuccessful in only 1 of the 10 patients who had asmall oral cavity and required nasal intubation to facilitate surgical
access. There were no serious airway complications and nocomplaints recorded during patient follow-up. Assessment of thedevice by both surgeon and anaesthetist was satisfactory.
Conclusions & Reviewer’s commentsThis is a modification of the standard mouth prop that is routinelyused in oral surgery procedures. It has the added advantage ofbeing able to secure the LMA in place thus avoiding the notinfrequent problem of the LMA moving mid-procedure due tosurgical manipulation, which often then causes a failed or partiallyobstructed airway.
Each LMA-PROP cost US$170.00 to manufacture but could bereused up to 30 times following sterilisation. This equates to justunder $6.00 per case – a nominal amount in isolation but wouldprobably add up quite significantly, based on the number of oralsurgery cases each centre does in a year.
DM
Virtual Reality Exposure Therapy for the Treatmentof Dental Phobia: A Controlled Feasibility Study
Gujjar, KR., van Wijk, A., Sharma, R. & de Jongh, A. Behavioural and Cognitive Psychotherapy 2017, Sep 14: 1-7Published online: 14th September 2017
Abstract:
Background: Virtual reality exposure therapy (VRET) has been
used to treat a variety of fears and phobias.
Aim: To determine the feasibility (i.e. safety and efficacy) of usingVRET to treat dental phobia.
Method: Safety was evaluated by determining any adverse eventsor symptom exacerbation. Efficacy of VRET was evaluated bycomparing the reduction in dental anxiety scores (measured 16times within a 14-week study period, and at 6-month follow-up),and its behavioural effects with that of an informational pamphlet(IP) on ten randomised patients with dental phobia using acontrolled multiple baseline design. Participants' heart rateresponse during VRET, and their experience post-VRET, wereindexed.
Results: No personal adverse events or symptom exacerbationoccurred. Visual analysis and post-hoc intention-to-treat analysisshowed a significantly greater decrease in dental anxiety scores[higher PND (percentage of non-overlap data) scores of 100% andlower POD (percentage of overlap data) of 0%, Modified DentalAnxiety Scale, F (1,8) = 8.61, p = 0.019, and Dental Fear Scale, F (1,8)= 10.53, p = 0.012], and behavioural avoidance in the VRETcompared with the IP group [d = 4.2 and -1.4, respectively). Therewas no increase in average heart rate during VRET. Of the ninetreatment completers, six (four from the VRET group and two fromthe IP group) no longer had dental phobia at 6-month follow-up.Four of the five VRET participants, but none of the IP participants,scheduled a dental treatment appointment following theintervention.

34 SAAD DIGEST | VOL.34 | 2018
JOURNAL SCANConclusion: VRET is a feasible alternative for patients with dentalphobia.
In view of this reviewer’s current interest and research into the useof Virtual Reality (VR) in the treatment of dental phobia, thisresearch article could not escape inclusion within the Digest’sJournal Scan.
For those less familiar with Cognitive Behavioural Therapy (CBT), itis important to highlight the vital role of graded exposure withinthe behavioural elements of CBT treatment for dental phobia. Thisarticle focusses on applying the theory of graded exposure withina virtual environment – hence the term – Virtual Reality ExposureTherapy, or VRET. VRET has gained increasing attention in thetreatment of anxiety disorders, including specific phobias –particularly for phobic objects or situations that may be difficult toexpose oneself to in vivo (i.e. heights, flying, spiders etc.). It involvesimmersing an individual within a virtual (or simulated) world withthe use of head mounted display (HMD) devices; and as Dr BryanKerr demonstrated in September’s SAAD Symposium, these VRtechnologies are light-years ahead from their initial launch in the 90s.
In this article, Kumar and the team demonstrate the encouraginguse of VRET for dental phobia in a controlled feasibility studyconducted in Malaysia, to explore safety and efficacy of theintervention. Participants with dental phobia (rated by a ModifiedDental Anxiety Scale score >15) were randomly assigned to eitherreceive a VRET intervention (using computer-simulatedenvironments and computer generated avatars) or a control groupwho received an information pamphlet about dental anxiety only.The VRET videos included common dental scenarios from sittingpassively in the dental chair, to oral examination and introductionto dental injections and drills – which were played to participantsseated in a dental chair. Consistent with the principles of gradedexposure, participants could not view the subsequent dentalscenario until their state anxiety level had fallen to a manageablelevel (rated as 2/10: on the 1-10 Subjective Units of Distress scale[SUDs]).
While the results are preliminary and this was a small-scale studyof 10 individuals, the authors observed encouraging results, whichthey suggest shows VRET to be both safe and acceptable toindividuals. Additionally, it seems the use of VRET significantlyreduced both state and trait dental anxiety, as well as reducingbehavioural avoidance and increasing the likelihood of futurearrangement of dental appointments. While participants ratedmoderate presence and realism (measures of quality of VRexperience) from the VRET intervention, all but one reportedexperiencing nausea (or cyber sickness). No other adversereactions were observed during VRET. This study therefore showspromise for the use of VRET as a mechanism to reduce dentalanxiety, with further research to establish its efficacy, both in theshort and long-term.
These are exciting times in the psychological treatment of dentalphobia and we await the publication of the authors’ fullrandomised controlled trial (RCT) – as well as the current researchunderway in the UK by the current reviewer (outlined in theabstracts of the symposium – see page 55).
JH
Non-pharmacological interventions for managingdental anxiety in children. (Protocol for CochraneReview)
Anthonappa RP, Ashley PF, Bonetti DL, Lombardo G, Riley PCochrane Database of Systematic Reviews 2017, Issue 6Published online: 5th June 2017
Abstract: This is a protocol for a Cochrane Review (Intervention). Theobjectives are as follows:
This review aims to assess the effectiveness of non-pharmacological interventions for reducing dental anxiety inchildren.
As the authors of this Cochrane protocol note, there have beenvery few published reviews evaluating the efficacy or effectivenessof non-pharmacological interventions for managing children’sdental anxiety – so this proposal offers an exciting opportunity toconsider the current evidence-base.
The protocol outlines the background of the problem, definingphobia and dental fear and anxiety among children, as well asdistinguishing dental behaviour management problems (DBMP),which may or may or not be associated with anxiety. The authorslist an array of non-pharmacological interventions which havebeen used with children for anxiety management, from tell-show-do to Cognitive Behavioural Therapy (CBT). These techniques aregrouped into four theoretical clusters, as suggested by an authorof a prior review for anxiety management techniques in adults,which include: 1) communication skills, 2) behaviour-modificationtechniques, 3) CBT, and 4) physical restraints.
The review aims to assess the effectiveness of the interventionsbased on: 1) post-treatment anxiety differences betweenintervention and control groups; 2) with secondary outcomesexploring differences in behaviour, whether planned treatmentwas completed or not, and observations of adverse events. Thereview is planned to only include randomised control trials (RCTs)with parallel design, focusing on all children/adolescents up to 16-years-old. Varying levels of anxiety will be included, with or withoutthe use of sedation methods; inclusion will also cover childrenreceiving any dental treatment (from simple restorations, dentaltraumas and orthodontic treatment). Research involving childrenwith medical conditions or syndrome will be excluded from thereview.
While most clinicians develop their own practice-based sense ofeffective interventions that help reduce or manage dental anxietyin the children they treat, this Cochrane review offers the chance toadd clarity to the types of interventions with a stronger evidence-base. It will also likely highlight intervention areas that warrantfurther exploration, as we continue to hone the techniques used,so to provide a full spectrum of anxiety-managementinterventions across the lifespan.
JH

35SAAD DIGEST | VOL.34 | 2018
JOURNAL SCANThe care and cure of dental phobia: the use ofcognitive behavioural therapy to complementconscious sedation
Newton, T., & Gallagher, J.Faculty of Dental Surgery. 8 (4): 160–163 Published online : 29 September 2017
How can CBT help rehabilitate patients who suffer from severeanxiety about dental treatment?
In a very recent opinion piece published, Professors Tim Newtonand Jennifer Gallagher outline the case to include CognitiveBehavioural Therapy (CBT) “within a framework of a comprehensiveservice” for conscious sedation. The article nicely distinguishes thevital role of each form of intervention – in which the care providedfrom conscious sedation, can be followed by a cure of theunderlying anxiety. Here lies the distinction – anxiety managementfollowed by anxiety rehabilitation.
In the spirit of full transparency, it may already be known by somethat I work with Professor Newton, within a service that are able toprovide both aspects of intervention in the care pathway, foradults with dental phobia. That is, individuals referred to us areable to access both conscious sedation and CBT, for the long-termmanagement of their phobia.
The opinion piece offers more information about CBT and theevidence-base of the approach; suggesting what a combinedservice might look like and what resources would be necessary toimplement this.
JH
Development of a decision aid for children facedwith the decision to undergo dental treatment withsedation or general anaesthesia
Hulin J, Baker S R, Marshman Z, et al.Int J Paed Dent 2017; 27: 344-355
Reviewer’s evaluation, opinion and points of interest This article is, perhaps, the first study to develop a decision aidwhich actively involved children in any decision-making processrelating to dental health care. The authors from Sheffield andLiverpool Schools of Dentistry set out to raise awareness of suchlittle-known resources.
Whilst being a small study with only 58 participants made up ofcontrols, children and parents, initial findings suggest that thedecision aid could be helpful to patients and their parents facedwith the decision to undergo dental treatment either withinhalation sedation, IV sedation or GA in terms of providing a morein-depth knowledge of the treatment options on offer. We nowwork in an era where clinicians inform what treatment modalitiesare available rather than dictate, but it is ultimately the patient orparents' choice which they select, therefore, all developments tohelp guide them as to what may be the most suitable choice arewelcomed.
Sadly, no statistically significant differences between the controland intervention groups were found in relation to reducing anxietyor decisional conflict. The authors propose that future studiesshould be focused on the introduction of the decision aid inprimary care settings, using a controlled before/after design tohelp aid understanding of how the decision aid may impact uponmeasures of anxiety and decisional conflict and how thesemeasures may alter over time.
RW
Comparison of single tooth anaesthesia bycomputer-controlled local anaesthetic deliverysystem (C-CLADS) with a supraperiosyealtraditional syringe injection in paediatric dentistry
Perugia C, Bartolino M, Docimo REur J Paed Dent 2017; 18: 221-225
Reviewer’s evaluation, opinion and points of interest:This study from researchers in Rome looked at comparing theefficacy of a computerised system for intraligamentaryadministration of local anaesthetic (C-CLADS) against traditionallocal infiltration delivery using a conventional syringe on primarymolar teeth in patients aged between 5 and 13. Previous studies todate have mainly focused on comparisons between the 2techniques in adults, the histological effects of high pressureintraligamental injections on the periodontal ligament, or onwhether there is any effect on the underlying permanent toothgerms.
This study focused on the onset time and anaesthetic effect overtime using a pulp tester, and the relative comfort perceived by thechild whilst the injection was given. As well as the distress somechildren exhibit from 'feeling numb', trauma to the soft tissues isparticularly common in children post injection. Hence it wasparticularly encouraging to see that no undesired collateralnumbness to the lip occurred in the C-CLADS group, whereas inthe conventional anaesthesia group 80% of the children reporteddiscomfort due to the numbness. The patients expressed a markedpreference for intraligamentary injection using C-CLADS,compared to buccal infiltrations or inferior dental nerve injection.In 88% of the children in the study disruptive behaviour wasobserved when using a traditional syringe compared to 0% withthe C-CLADS.
This study gives further encouragement that pain free anaesthesiacan be given with such techniques. As the authors are keen topoint out, the significant reduction of pain-induced disruptivebehaviour in children brings about lifelong benefits to them asadults when accepting dental treatment. I look forward to furtherlarger studies with increased sample sizes.
RW

36 SAAD DIGEST | VOL.34 | 2018
DJ ESSAY PRIZE WINNER
AbstractAnxiety and pain management has evolved tremendously sincethe inception of SAAD. As this organisation celebrates its diamondjubilee now is a good time to reflect on what the next 60 yearsmay hold?
This essay attempts to gaze into the future and discuss some ofthe factors which may influence how we practice over the next sixdecades. At a population level, we review how the change indemographics might influence our practise. At an organisationallevel we examine the changing culture of the NHS and the movetowards specialisation and multi-disciplinary teams. Also, touchingon some aspects of research and development in areas such aspharmacology, neurosciences, and psychology, and their impact onhow we might care for our patients in the future.
IntroductionHistorically, dentists have played a key role in the development ofanaesthesia and its implementation. In the 1980s the use ofgeneral anaesthesia in dentistry was under the spotlight followinga number of tragic deaths. In response to this, the Poswillo Report(1990)1 was commissioned; the use of general anaesthesia andworking practices were re-evaluated. The Conscious Decision (2000)2
document led to a cultural shift toward developing andintegrating best practice in the delivery of sedation, and ultimatelyto the cessation of general anaesthetic provision in primary care.Over subsequent years there has been an increasing focus onimproving patient safety, experience, and involvement in thedelivery of anxiety management and sedation strategies; patient-centred care continues to be at the core of the dental journey, andthis ethos looks set to continue well into the future.
Since the publication of the Conscious Decision (2000) report,sedation in dentistry has been used increasingly in preference togeneral anaesthesia. With the assistance of anxiety managementand sedation techniques, dentists are able to provide a range ofdental treatment including complex surgical procedures in primaryand secondary care dental settings. Procedures such as implants,bone augmentation and sinus lifts would previously havenecessitated a general anaesthetic but can now be undertakenroutinely with the adjunctive use of sedation. This averts the needfor admission to a ward, the provision of pre- and post-operative
care, and thus streamlines the treatment process. Patientsexperience fewer adverse events associated with conscioussedation as opposed to general anaesthesia; they recover morerapidly and are discharged swiftly, allowing for increases intreatment provision and reduced waiting times for receipt oftreatment.
The use of midazolam has a well-documented safety record and isthe mainstay of dental sedation.3 Advanced sedation techniquesincluding the use of fentanyl and propofol are being used by thedental team with increasing confidence and their formalintegration into the sedation dentist’s armamentarium of tools formanaging the anxious patient is being encouraged. At present,there is growing acceptance and research in support ofpsychological management techniques and complementarytherapies that can reduce the need for pharmacologicalintervention.4 This paper will discuss the future of these techniquesand attempt to crystal ball gaze into the next 60 years to describethe ways in which demographic changes such as the ageing andincreasingly overweight population, NHS culture shifts focusing onpatient safety, evidence-based practice and multi-disciplinaryworking, and rapidly advancing technological developments arelikely to impact upon the provision of anxiety management andsedation.
Sedation practices over the next60 yearsDemographic shifts and implications for the provision of care
The population of the United Kingdom is rapidly changing. Overallwe are increasing in size and age. Over the next 60 yearsconsideration must be given to the ways in which these factors willimpact upon the delivery of safe sedation. The Office for Nationalstatistics (2015)5 predicts that the population of those people overthe age of 75 is likely to increase to 9.9 million by 2039 and forthose over the age of 85 that figure is estimated to reach 3.6million. In the year 2077, the elderly will make up a greaterproportion of the population than at present. This population havegrown up with a state funded healthcare system, have high dentalaspirations and are likely to be on multiple medications for a rangeof chronic health conditions that previously would have beenconsidered life-limiting. As this group come to constitute a greaterproportion of the population, provision of sedation for the older
Anxiety management and sedation in dentistry;the next 60 years Janine Doughty BDS, MDPH, DDPH RCS (Eng) Eastman Dental Institute, 256 Grays Inn Road, WC1X 8LD, University College London / Department of Dental Public Health 1-19 Torrington Place, WC1E 7HB.
Amar Kaul BDS MFGDP (UK) MFDS (RCS Eng) DSCD (RCS Eng)Eastman Dental Institute, 256 Grays Inn Road, WC1X 8LD, University College London / Department of Dental Public Health 1-19 Torrington Place, WC1E 7HB.
Corresponding Author: [email protected]

37SAAD DIGEST | VOL.34 | 2018
DJ ESSAY PRIZE WINNERperson is also likely to become more common. The knock-on effectof this demographic shift may mean that by 2077 more sedationtreatments will be provided in secondary care environments or inprimary care environments with the assistance of anaesthetists.Evidence-based midazolam administration protocols may bedeveloped for the older patient to reduce the risk of over-sedationas far as reasonably practicable. Additionally, the dentist of thefuture will be responsible for the holistic assessment of the patientprior to undertaking sedation, this may include developing careplans that take into consideration the medical, functional,psychological and social needs of the patient and may involve,geriatricians, specialist nurses, community therapists, familymembers and general practitioners.6 Objective measures of frailtysuch as the Rockwood clinical frailty scale will become routinelyused and important for those older people who may have verylittle wrong with them medically, but are put at risk by their frailty.7
In addition to the aging population, obesity is a public healthconcern that almost certainly will impact on the practice ofconscious sedation in dentistry in the next 60 years. Estimates havepredicted that obesity is likely to affect 60% of men and 50% ofwomen by 2050.8 For these patients a multidisciplinary medicaland dental team may be necessary to facilitate dental treatmentunder sedation. Not only are obese patients more at risk ofhypertension, cardiovascular disease, diabetes mellitus, sleepapnoea, and gastro-oesophageal reflux, all of which have potentialimplications for the provision of sedation, but also additionalchallenges may arise with airway management and cannulation.9
As the number of obese people attending dental practicesincreases, there may be an increase in the provision of inhalationsedation and non-pharmacological anxiety managementstrategies in an attempt to mitigate the risks of respiratorydepression associated with midazolam.
National Health Service culture shiftand implications for care Patient safety
Patient safety is paramount in the NHS, this includes theavoidance of adverse events and the consistent recording of anyuntoward outcomes associated with treatment. Measures toimprove safety that may arise or become more commonly usedover the next 60 years include the routine incorporation ofsurgical safety checklists, such as those developed by the WorldHealth Organisation, prior to undertaking any episode of sedationin primary or secondary care. Where possible, for medicallycomplex or obese patients who are at an increased risk of adverseevents during sedation, behavioural management techniques willbe employed in the first instance and where sedation isunavoidable, there may be collaborative working withanaesthetists.
As the demographic shifts described above are realised,undergraduate and postgraduate students will be encouraged tobecome more familiar with the management of complicationsoccurring in the dental surgery and during dental sedation. Theuse of simulation in teaching has become ever more sophisticatedand is now frequently used in medicine. Simulation has beenshown to increase performance in high-stakes situations and has
shown promise in the simulation of routine dental techniques suchas delivery of local anaesthesia.10,11
We are likely to see simulation incorporated into sedationteaching, students will be able to simulate the administration of avariety of sedative agents in varying concentrations or quantitiesin order to improve understanding of the physiological effects thatsedative drugs have on the body to understand and learn how tomanage adverse events, especially those which become criticalover a short space of time such as over-sedation.
As a result of the Francis Report’s12 recommendations for duty ofcandour, a culture of transparency and accountability has becomeessential in the practice of medicine and dentistry, and is now arecommendation of the General Dental Council (2016).13 We arelikely to see more candid and accurate reporting of adverse eventsand an increasing openness in the sharing of lessons learned as aresult. Overall, the outcome of these changes over the next 60years will be improved patient safety and experience.
Evidence-based clinical decisionmaking Over the coming 60 years there is likely to be a greater need tojustify treatment decisions with high quality evidence, to provideclinicians with specific care pathways to determine which patientsare likely to benefit from sedation or psychological therapies andfor treatment indices that facilitate decision-making to becomemore commonplace. Cost effectiveness and sedation indices thatprovide a framework for objective assessment of treatment needhave the potential to aid in decision making for dentists workingwithin a public funded healthcare system. By 2077, validatedmeasures of sedation-need are likely to be integrated into servicesand completed electronically prior to the patient’s firstappointment. This will help to more accurately determine thepatient pathway, thereby reducing time of the appointment,prevent wasted treatment sessions for those patients unlikely tobenefit from psychological or relative analgesia methods, thuscreating a more streamlined and replicable care pathway. Suchindices may also be of benefit when commissioning dentalservices to give an overview of the sedation needs assessment of a population. Existing indices have suggested thatapproximately 5.1% of the population have a high need ofconscious sedation14.
Multidisciplinary and team working The management of patients with increasingly complex medicalhistories and the need to safely provide them with comprehensivedentistry is likely to lead to more integration between dentists andmedical teams. For obese patients, airway management isconsiderably more challenging and may require the assistance ofan appropriately trained anaesthetist during some sedationprocedures. Additionally, for those high risk patients we are likelyto see more multi-disciplinary team meetings with anaesthetists,dentists and psychologists taking place. Psychologists have beenintegrated into the dental team in some secondary care unitswhere their role is to help in the management of chronic facial

38 SAAD DIGEST | VOL.34 | 2018
DJ ESSAY PRIZE WINNERpain, as sedation becomes more risky for specific cohorts, we arelikely to see increasing reliance upon evidence-based behaviouralmanagement techniques and much more close working withpsychiatrists, psychologists and general practitioners..15
Dental phobia can be severely debilitating, leading people toneglect their oral health, to experience unnecessary and avoidablepain and can affect self-esteem. Unlike other mental healthproblems, such as agoraphobia or post-traumatic stress disorderfor example, the impact of dental phobia on quality-of-life isseldom considered. In the future, we can anticipate that the widerimplications of dental phobia will be recognised by our medicalcolleagues and appropriate, tailored management plans will bedeveloped to facilitate the routine provision of simple dentaltreatment for these patients.
With increasing specialisation comes the risk of increasingfragmentation of knowledge. The role of the specialist willincreasingly rely on being able to access and synthesiseknowledge, adapting it to the needs of their speciality. As AtulGwande16 eloquently states, “the extreme complexity of medicinehas become more than one individual can handle, but not morethan teams of clinicians can handle”.
Team working is a key component to successful dental sedationpractice. In recent years there has been an impetus to up-skill allmembers of the dental team, dental nurses are now able toundertake additional training to provide impressions, radiographs,fluoride varnish application and can develop advanced dentalnursing skills for sedation. One of the outcomes of a systematicreview exploring behaviour management strategies in dentistry,suggested that cognitive behavioural therapy (CBT) could beeffectively provided by dental staff at various training levels,furthermore, this concept is supported by Porrit, Jones andMarshman17 who describe a dental nurse-led integrated carepathway that has been successful in reducing dental anxiety byproviding low-level psychological interventions. Full utilisation ofthe dental team in the care pathway for the dentally anxiouspatient provides a cost effective way to assist patients in themanagement of their dental anxiety and is likely to be an area ofgrowth over the next 60 years.
Improving patient experienceIn the future the drive toward patient centred care will continue,putting the patient at the heart of the dental treatment plan, withpatient choice and experience being the cornerstone of decision-making for elective anxiety management and sedation procedures.Positive experiences and associations are a key part of the dentaljourney for the management of anxiety. Evidence is emerging thatthe dental environment can be modified to reduce feelings ofanxiety. Emergent evidence from randomised controlled trialssuggests that small changes to the dental environment, such asthe scent of lavender, can lead to statistically significant reductionsin levels of anxiety as measured by the Modified dental AnxietyScale (MDAS) and systematic reviews have suggested the benefitsof music therapy for anxious adults.18,19 In 2077 we may see theseevidence-based pre-emptive therapies employed to create asoothing environment for the anxious dental patient.
Technological advances and theirimplications for careThe integration of advancing technology in anxiety managementand sedation is unavoidable; the potential for improved patientcare and experience will no doubt be facilitated by a variety oftechnological advances. The technological boom will almostcertainly impact on the way in which treatments are delivered, forexample in the delivery of carefully titrated advanced sedationtechniques, superior systems for monitoring patients and tools toimprove the patient experience and environment.
Whilst technological advances infiltrate into the provision ofsedation, the backdrop to the practice of dentistry will bechanging simultaneously. As such, over the next sixty years we arelikely to see a shift in the nature of dental treatment beingprovided under sedation or general anaesthesia. Sedation may bereserved for dental extractions and surgical procedures whilstneedle-free local anaesthesia delivery systems and toothrestoration without conventional drills have the potential toreduce the distress associated with these procedures. Dentalmaterials are likely to have improved handling, reduced moisturesensitivity and, as such, will be placed with greater ease in thedental phobic or patient with challenging behaviour. There hasbeen a remarkable drop in the caries prevalence in England inrecent years; primary coronal caries has fallen from 38 per cent in1998 to 23 per cent in 2009.20 Multiple contributory factorsincluding the normalisation of oral hygiene, the common use offluoride containing dentifrices and the public health agenda toreduce sugar consumption look set to lead to a continuedreduction in caries incidence.21 Additionally, genetically modifiedreduced cariogenicity Streptococcus Mutans may have a role to playin the future for the reduction of caries experience.
During the sedation procedure, more sensitive technology maybecome routine practice in the management of medically complexASA III/IV patients. For example, capnography which graphicallydisplays “the concentration of exhaled and inhaled carbon dioxideplotted against time” has been shown to be a method for the earlydetection of respiratory depression.22 Capnography is routinelyused during general anaesthesia and in intubated patients. As thenumber of patients who are elderly or have multiple comorbiditiesincreases, we may find that over the next 60 years the use ofcapnography becomes routine practice for dental sedation.Additionally, modalities such as pre-oxygenation of patients,especially those who are overweight can help to reduce the risk ofrespiratory depression during intravenous sedation and maybecome a mainstay of treatment for the at-risk patient.
As previously mentioned, closer working within multidisciplinaryteams including dentists, anaesthetists, outreach teams andpsychologists is anticipated in the future for patients with multiplecomplexities. These teams may be virtual. Telemedicine is alreadybeing used to monitor and treat patients in some branches ofmedicine which do not require the expert to be physically present,and a variant of this may be used in the management of dentalpatients where centrally located teams of specialists could provideexpert opinions, treatment plans and clinical supervisionremotely.23

39SAAD DIGEST | VOL.34 | 2018
DJ ESSAY PRIZE WINNERTechnology is not only beneficial in the monitoring of patientsundergoing sedation, it can also be useful in non-pharmacologicalbehavioural management. Sound-excluding earphones can beused in the dental surgery to block out distressing noises; thesecan be linked to microphones that enable the dentist tocommunicate with the patient. Over the next 60 years we may seevirtual reality programmes developed that allow the patient tobecome immersed in a three-dimensional dental experience wherethey can safely become desensitised to the experience ofattending the dentist; virtually inspecting instruments, operatingdental hand-pieces and integrating this further through the use ofavatars similar in appearance to themselves. Hypnotic principlesare currently being pioneered through virtual reality head-sets,which focus the patient’s attention away from the procedure andonto alternatives experiences, creating states of focused attention,relaxation, and immersion into another reality.
Developments in anxietymanagement strategiesFollowing on from the current trends in the provision of dentalcare in the UK, the future of anxiety management and sedation islikely to continue to move toward a holistic, patient-centred andmultidisciplinary approach. Anxiety management and sedationtechniques will likely be guided by high quality evidencegenerated from rigorously controlled trials and synthesisedevidence to support the efficacy and safety of these techniques inthe hands of the dental team. Anxiety management strategies arelikely to become multimodal, utilising methods which show everincreasing evidence in support of their effectiveness such asmindfulness meditation, cognitive behavioural therapy andhypnotherapy. In 2016, the National Institute of Health and CareExcellence made formal recommendations for the use ofmindfulness based cognitive behavioural therapy in themanagement of depression, revealing the increasing acceptance ofalternative therapeutic techniques within the medical sphere andwith continued evidence in support of this, is likely to be an areathat continues to increase over the next 60 years. A systematicreview by Gordan et al , found that cognitive behavioural therapy(CBT) was successful in the reduction of dental anxiety, this successalso extended to CBT undertaken in group sessions and showedsome improvements after just one session. These techniquesprovide the patient with a way to develop their internal locus ofcontrol, thereby empowering them and providing them withcoping strategies that can enable them to conquer their dentalanxieties.
As behavioural management therapies become integrated intomainstream practice and gain further high quality evidence insupport of their benefits and effectiveness, the under- and post-graduate curriculum will gradually morph to reflect theseadvances. Over the next 60 years we may see the development ofstructured behavioural management modules in theundergraduate curriculum educating young dentists to providesimple cognitive behavioural therapies, prescribe mindfulnessregimes for patients to practice at home, and to deliver simplehypnotherapy-based relaxation techniques. The impact of sucheducation may be a reduction in the number of dental phobiacases referred into community dental services or secondary care
settings and an increased confidence in the use of non-pharmacological methods of anxiety reduction. Ultimately,developing behavioural management techniques in theundergraduate curriculum will reduce the reliance on sedation andencourage patients to overcome their dental anxieties.
We have described the increases expected in the medicallycomplex older population, but at the other end of the age range,children with equally complex medical, and genetic conditions arethriving into adulthood thanks to advances in medicine andsurgery. These patient groups require dental care consistent withthat provided for the general population but due to their medicalcomplexities may struggle to access, tolerate and comply withdental procedures. These challenges may mean that generalanaesthesia is contra-indicated and therefore anxiety managementmay be crucial in facilitating access to care.
These changes in population demographic and our knowledge ofanxiety management techniques creates an ethical imperative forthe conscientious dental practitioner to provide a holisticapproach to patient care and to move away from the perceptionsof the mind body dichotomy. Psychological techniques will need tobe integrated as adjuncts to pharmacological approaches.Pioneering researchers have explored the use of a combination ofregional or local anaesthesia with sedation and hypnosis, utilisinginnovative management strategies drawn from multipledisciplines. Their research has shown promise for the cognitivemodulation of dental pain and the combined benefits of conscioussedation in conjunction with hypnotic states to facilitate painrelief.26
Current concepts in neuroplasticity are already exploring thepotential for ‘rewiring’ the brain by changing neuroncommunications and networks. This in turn may have promise forthe complete elimination of the patient’s stress and anxietypathways. In the future, sedation may no longer be required asneurologists and psychiatrists begin to successfully remodel thebrain of the dental phobia patient. Neuro-psycho-pharmacologymay very well be the future for anxiety management.
By 2077, we are likely to see a move away from the medical modelof treatment provision and a push toward empowering patients totake responsibility for their coping strategies and to develop theirpersonal resilience alongside care provided by supportivepractitioners.
Advances in sedation techniques For many years midazolam sedation has been shown to be aneffective agent in the management of the anxious or challengingpatient. The route of administration has primarily beenintravenous, but in recent years the use of intranasal midazolamadministered using a Mucosal Atomisation Device has becomeincreasingly popular for both children and adults. 28 The use of suchdevices is likely to develop in the future with ever moresophisticated versions emerging. Patient-controlled sedation hasbeen shown to have high levels of patient satisfaction, minimalcardiorespiratory complications and a good safety record.29,30 Theaim of sedation is to maintain an optimum state where the patientis still able to respond to verbal commands and does not require

40 SAAD DIGEST | VOL.34 | 2018
DJ ESSAY PRIZE WINNERassistance to maintain their airway. Increasingly sensitive andresponsive administration systems will help to improve the safetyof both midazolam and multidrug advanced sedation techniques.Sedation methods are likely to be tailored to the specific needsand preferences of the patient, with advanced sedation becominga more frequently used method in secondary care.
Advanced sedation techniques using continuous propofol infusionand combinations of midazolam and fentanyl have becomeincreasingly popular for the management of those patients forwhom midazolam may have been ineffective. Pioneering advancedsedation courses are being developed to up-skill dentists to safelyprovide these alternative techniques and over the next 60 yearsthere are likely to be a greater number of dentists undertakingsuch courses.31
With an increasing move towards the use of anaesthetic andsedation-based procedures the nature of the operating theatre willchange to accommodate the semi-conscious patient who may ormay not experience post-operative amnesia, this may involvecreating an environment conducive to both surgeon and patient.The lighting, the sounds, the nature of team operations andinteractions need to create a harmonious atmosphere to supportthe patient.
ConclusionsOver the next 60 years we are likely to see anxiety management andsedation change dramatically. Gazing into the crystal ball reveals thebenefits that technology can have to improve patient experienceand also the safety of sedation through more rapidly responsivemonitoring of at-risk (ASA III/IV) patients and more sensitivemethods of sedation administration. There will be closer liaisonbetween the dental team and medical specialities. Dentists will workclosely with psychologists to deliver behaviour managementtechniques as an evidence-based way to mitigate the risk ofsedation or general anaesthetic for medically complex patients andto reduce reliance upon pharmacological sedative interventions. Asmidazolam sedation continues to prove itself as a safe method forreducing dental anxiety and the acceptance of advanced sedationtechniques delivered by the dental team increases, appropriatelyselected patients unsuitable for behavioural managementintervention will be provided with optimum, evidence-based carepathways for the delivery of the most efficacious sedation strategy,ensuring that we’re “getting it right first time”.
References1. General Anaesthesia, Sedation and Resuscitation in Dentistry. Report of an expert
working party prepared for the Standing Dental Advisory Committee March.London: Standing Dental Advisory Committee, 1990.
2. Department of Health. A conscious decision. London: Department of Health, 2000.
3. Henthorn K M, Dickenson C. The use of flumazenil after midazolam-inducedconscious sedation. Br Dent J 2010; 11: 209.
4. Oyekunle O M, Fulton J, Hayes C. What is the most effective treatment for themanagement of dental anxiety amongst adults? A systematic review ofinterventions. J Comm Pub Health Nurs 2016; 2:4.
5. Office for National Statistics. National population predictions: 2014-basedstatistical bulletin. London: ONS, 2015. Online information available athttps://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationprojections/bulletins/nationalpopulationprojections/2015-10-29
6. British Geriatric Society. Fit for frailty. Consensus best practice guidance for thecare of older people living with frailty in community and outpatient settings.London: British Geriatrics Society, 2014.
7. Dalhousie University. Clinical Frailty Scale. Geriatric Medicine Research. Onlineinformation available athttp://geriatricresearch.medicine.dal.ca/pdf/Clinical%20Faily%20Scale.pdf(Accessed online 30th March 2017)
8. Foresight. Reducing obesity: future choices. London: Department of Health, 2007.
9. Reilly D, Boyle C A, Craig D C. Obesity and dentistry: a growing problem. Br Dent J2009; 207: 171-175.
10. Bruppacher H R, Alam S K, LeBlanc V R. Simulation based training improvesphysicians’ performance in patient care in high-stakes clinical setting of cardiacsurgery. Anesthesiology 2010; 112:775–6.
11. Lee J S, Graham R, Bassiur J P, Lichtenthal R M. Evaluation of a Local AnesthesiaSimulation Model with Dental Students as Novice Clinicians. J Dent Educ 2015;79:1411-7.
12. Francis R. Report of the Mid-Staffordshire NHS Foundation Trust Public Inquiry.Executive Summary. London: The Stationary Office, 2016.
13. General Dental Council. Being open and honest with patients when somethinggoes wrong. London: General Dental Council, 2016.
14. Coulthard P. The indicator of sedation need (IOSN). Dent Update. 2013; 40: 466-471.
15. Zakrzewska J M. Differential diagnosis of facial pain and guidelines formanagement. Br J Anaes 2013; 111: 95-104.
16. Gwande A. The Checklist Manifesto. New York: Henry Holt and Company, 2010.
17. Porritt J, Jones K, Marshman Z. Service evaluation of a nurse-led dental anxietymanagement service for adult patients. Br Dent J 2016; 220: 515 – 520.
18. Venkataramana M, Pratap K V N R, Padma M, Kalyan S, Reddy A A, Sandhya P..Effect of aromatherapy on dental patient anxiety: A randomized controlled trial.Pub Health Dent 2016; 14: 131-134.
19. Moola S, Pearson A, Hagger C. Effectiveness of music interventions on dentalanxiety in paediatric and adult patients: a systematic review. JBI Libr Syst Rev2011; 9: 588-630.
20. White D, Pitts N, Steele J, Sadler K, Chadwick B. Disease and related disorders. Areport from the adult dental health survey 2009. London: The Health and SocialCare Information Centre, 2011.
21. Public Health England. Sugar reduction: achieving the 20%. London: Public HealthEngland. 2017.
22. Brady P, Gallagher C, McCarthy C, O’Halloran K, McCreary C, Ioham G.Capnography monitoring during the dental conscious sedation. Oral Surgery.2016. Online information available athttp://onlinelibrary.wiley.com/doi/10.1111/ors.12239/full#ors12239-bibl-0001(Accessed 23rd March 2017)
23. Mihailovic B, Vujicic B, Miladinovic M. Telemedicine in Dentistry (Teledentistry).2011. Online information available at cdn.intechopen.com (Accessed 23rd March2017)
24. National Institute for Health and Care Excellence. Depression in adults:recognition and management. NICE: London. 2016 [Accessed 23rd March 2017]https://www.nice.org.uk/guidance/cg90/chapter/1-Guidance
25. Gordan D, Heimberg R G, Tellez M, Ismail A I. A critical review of the approaches tothe treatment of dental anxiety in adults. Journal of Anxiety Disorders, 2013; 27:365-378.
26. Wolf T G, Wolf D, Callaway A, Below D, d'Hoedt B, Willershausen B, Daubländer M.Hypnosis and Local Anesthesia for Dental Pain Relief-Alternative or AdjunctTherapy?-A Randomized, Clinical-Experimental Crossover Study. Int J Clin ExpHypn 2016; 64: 391-403.
27. McEwen et al. Stress and anxiety: Structural plasticity and epigenetic regulationas a consequence of stress. Neuropharmacology 2012; 62: 3–12
28. Harbuz D K, and O’Halloran M. Techniques to administer oral, inhalational, and IVsedation in dentistry. Australas Med J 2016; 9: 25–32.
29. Leitch J A, Anderson K, Gambhir S. et al. A partially blinded randomised controlledtrial of patient-maintained propofol sedation and operator controlled midazolamsedation in third molar extractions. Anaesthesia 2004; 59: 853–60.
30. Höhener D, Blumental S, Borgeat A. Sedation and regional anaesthesia in theadult patient. Br J Anaesth 2008; 100: 8–16.
31. Nizarali N, Edwards J, Kerr B. Advanced conscious sedation training--the pilotcourse, training and impact on a hospital service. SAAD Dig 2014; 30: 41-3.

41SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNER
AbstractDental fear and anxiety (DFA), often recognised as one of thebarriers to oral health, could impact a patient’s dental health andsocial life. Current approaches for severe DFA often require the useof conscious sedation, general anesthesia and psychologicaltherapies. New technological advances and scientific discoveries inthe near future have the potential to open up a diverse range ofpossible treatment options for DFA.
Recent advances in pharmacogenomics, robotic deliverytechnologies and nanotechnology hold promises for improvingthe safety and effectiveness of the current approaches. Newapproaches, such as decoded fMRI neurofeedback, computerisedcognitive behavioural therapy and use of post-retrieval amnesicagents, are likely to bring new insights into treatments of DFA. Theaetiology of DFA will be more effectively understood using moreadvanced neuro-imaging and molecular genetics technologies,allowing dentists to tailor a more “personalised” therapy for thepatient. Overall, technological developments look set to yieldpositive developments in field of DFA and these researchopportunities should be capitalised upon.
Dental anxiety, often recognised as one of the barriers to oralhealth care in scientific literature,1 has not only been known toresult in poorer dental health due to the patient’s avoidancebehaviour,2 but also to impact their social life by interfering withwork and personal relationships.3 Dental fear and dental anxiety(DFA) are often referred as the state of apprehension which occursprior to dental treatment and visits due to a perceived inability topredict and control upcoming situations.4 Dental phobia, thoughoften reported separately, is actually a severe form of DFA and ischaracterised by active avoidance of dental care and out-of-proportion fear towards the actual danger posed by the dentalsituation.4 Statistics5 show that prevalence is high, with nearly halfof the population reporting to have moderate to extreme levels of DFA.
Currently, the typical approach for patients with mild to moderateDFA is to create a calm and welcoming environment.6 Those withsevere DFA or dental phobia may often require more intensiveinterventions, such as pharmacological strategies using conscioussedation and general anaesthesia(GA), and psychologicaltherapies.6 Scientific and technological breakthroughs in the next 60 years could potentially improve the effectiveness andsafety of current approaches, and yield new approaches in treating DFA.
Robotic delivery of anaesthesia andartificial intelligenceRobotic surgery is already a familiar concept in medical field in the21st century; it is frequently reported to offer advantages such aslower post-operative pain7 and complication rates amongpatients.8 Despite the apparent benefits of robotic surgery,developments in robotic delivery have only just started in the fieldof anaesthesiology. The development of Artificial intelligence (AI), abranch of engineering that utilises computers to simulateintelligent behaviour with minimal human intervention, often goeshand in hand with that of robots.9
AI, installed with machine learning algorithms and knowledgemanagement programmes, could be used to design computeriseddecision support systems for conscious sedation and GA and boostnew discoveries in molecular medicine by identifying commonpatterns. 9 These systems could enable health professionals toidentify subjects with higher risk of developing certain symptoms,via integration of the patient’s medical history, genetic informationand data from scientific research using computer algorithms,9
subsequently suggesting a range of pre-operative investigationsand optimal treatment modalities “personalised” for the patient.10
These systems could also be used in post-operative care byproviding reminders for administrating prophylaxis for post-operative nausea and vomiting to high risk patients to improvepatient comfort.9
Progress has also been made in robotic delivery of generalanaesthesia and conscious sedation. For instance, McSleepy is thefirst pharmacological drug delivery system designed to monitor allthree components of GA (hypnosis, analgesia and musclerelaxation) via automated closed-loop delivery systems, allowingautomatic control of anaesthesia induction, maintenance andemergence.11,12 The system also includes in-built safety features anda touch screen with a user-friendly interface to permit bidirectionalcommunication with the anesthesiologist.11 Although clinicaltrials13,14 have been performed to demonstrate the feasibility of thedevice, research investigating the safety of the system is stilllacking for clinical translation. SEDASYS, another semi-automateddrug delivery system that administrates profopol calculated usingpatient’s physiological parameters,15 was shown to provide higherpatient satisfaction and a more rapid recovery time whenproviding conscious sedation in gastrointestinal endoscopy andcolonoscopy procedures.16,17 Having said that, the use of the devicehas never been investigated in a dental setting and severallimitations concerning the safety of the device are still present,such as delayed oxygen delivery in situations of hypoventilation,18
Anxiety Management and Sedation in Dentistry;the next 60 years? Yui Yin Ko
Dental Student Leeds Dental Institute, The Worsley Building, Clarendon Way, Leeds LS2 9LU
Corresponding Author: [email protected]

42 SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNERand inability to carry out ventilation with a face mask in an overlysedated patient,19 thus the device can only be currently used in thepresence of an anaesthesiologist or a nurse anaesthetist.20
Fig. 121: Illustration showing the use of McSleepyTM duringsurgeryhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC3728848/
Advancements in robotic technology in the future may potentiallyallow the development of a safer automated device that is capableof both recognising anaesthesia emergencies based on thepatient’s clinical parameters and pre-operative risk assessmentscarried out using AI, and carrying out appropriate managementtowards these emergencies, therefore increasing the availability ofconscious sedation and GA in primary dental settings. Roboticdelivery has a potential role in increasing patient safety viareducing mistakes due to human error, as well as side effects bydelivering an optimal dosage of sedative drugs.
PharmacogenomicsAdvancements in molecular technologies have led to an explosionof research in pharmacogenomics, a branch of science thatinvestigates the effect of genetic variability on an individual’sresponse to drug therapy.22 This has allowed the identification ofpolymorphism in genes encoding drug metabolising enzymes,transporters and receptors as a predictive factor in an individual’smetabolic capacity towards the drug.22
Pharmacogenomics could be used to select the right sedationdrug for patients and several genotypes related have already beenidentified with the current technology available. For instance, astudy by Khan et al.23 discovered genetic polymorphism in genescould have an impact in metabolism and clearance of propofol,resulting in variability in induction dose and time of loss ofconsciousness among patients. Another study by Nagele et al.24
found that patients who are homozygous for the genetic variantMTHFR 677C>T or 1298A>C are at a higher risk of developinghyper-homocysteinemia after the use of nitrous oxide as a sedativeagent. Case reports25,26 suggest these patients could suffer fromcatastrophic neurologic outcomes, such as diffuse myelopathy oreven death, if treatment wasn’t provided promptly. Genetics havealso been shown to influence other commonly used sedatives,such as midazolam27 and diazepam.28 Pharmacogenomics can alsobe applied in local anaesthetic used in a clinical dental setting.Lidocaine, one of the most commonly used agents,29 was found tobe less effective towards redheads due to mutations of themelanocortin 1 receptor.30
Future developments in pharmacogenetics could allow testing tobe conducted at chairside to provide patient-tailored drugselection and dosage individualisation, which could reduce anyadverse side effects, increase effectiveness of the drug, or evenprevent mortalities.31
NanotechnologyWith the increasing incorporation of nanotechnology, a branch ofengineering that manipulates matter by one atom or molecule tocreate structures with unique properties,32 into medicine, a newbranch - nanodentistry is slowly emerging.
Development of nanorobots could reduce or even eliminate theneed for dental drills and needles in treatment, which are the twomost reported fears among patients.33 To induce anaesthesiawithout the use of needles, dentists could place a colloidalsuspension containing millions of active analgesic dentalnanorobots on the patient’s gingivae, which are all controlled bythe dentist using a nanocomputer. Upon contact with the surfaceof the crown or mucosa, nanorobots could migrate into the pulpvia gingival sulcus, lamina propria and dentinal tubules to shutdown any sensitivity in the tooth and induce numbness. Likewise,restoration of sensation could also be achieved by orderingnanorobots to egress from the tooth.34 Nanorobotic dentrifices,delivered in the form of toothpaste or mouthwash, could beinstructed using a nanocomputer to destroy any cariogenicpathogens and decayed tissue by metabolising trapped organicmatter into harmless and odourless vapours, hence eliminating theuse of drills when treating tooth decay.35
(( ( ( ( ( ( ( ( ( (
(((
( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( ( (((!!

43SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNERNanotechnology could also be applied to improve the drugdelivery systems in sedation. Improved emulsion delivery systemsin nano-lipospheres allow drugs to pass through the blood-brainbarrier and directly transport sedative molecules to the targetreceptor, thus increasing bioavailability of drugs and reducingeffects of toxicity to other healthy tissues.36,37 Preclinical trials withsedative agents with nanoparticles have so far been positive. Forinstance, a preclinical trial38 showed that intranasal delivery ofnanoparticles loaded with midazolam improved drug entrapment,which may reduce the need for repeated administration andincrease patient compliance with fewer side effects. Anotherpreclinical trial39 discovered that intravenous delivery of profopolusing hydroponically alginate nanoparticles may be able toovercome some of the drawbacks in the currently delivered lipid-based formulation, such as pain during injection and emulsioninstability.
With the technologies available now, most current studies are stillin the preliminary stage. Although nanodentistry has a lot ofpotential in modifying anxiety management by eliminating the useof drills and needles, issues such as biocompatibility, technicalissues of assembling molecular-scale parts and achieving publicacceptance will need to be addressed before implementation intoclinical practice.32
Understanding dental anxiety Advanced developments of functional neuroimaging techniques,such as functional magnetic resonance imaging (fMRI), allows themapping of brain physiology by detecting changes in blood flow,metabolism and receptor-ligand binding.40 Application of thesetechniques has allowed us to understand the underlyingpsychopathological mechanism of mental illnesses, such asdepression, OCD and even phobias.40
Recently, sex differences in neuroanatomy of dental phobicpatients is demonstrated with the use of fMRI.41 While femalepatients show a greater activation of caudate nucleus, malesexhibit enhanced dorsolateral prefrontal cortex (DLPFC)involvement. This indicates that females are more likely to avoiddental care when facing phobia and may benefit more with theuse of distraction and hypnosis, whereas males are more likely tobenefit from exposure therapy. Enhanced basal ganglia internalconnectivity and reduced frontostriatal coupling were alsoidentified in brains of phobic patients, which could be used asneuromarkers for diagnosis and monitoring of dental phobiaduring therapies.42
Genetics has always been believed to be not strongly related todental phobia development,43 however, a recent study44 hasdemonstrated that dental fear may share heritability with fear ofpain via a family-based cohort study. Despite advances inmolecular genetic testing, the role genetics play in thedevelopment and maintenance of DFA is still unclear.
Future developments in neuro-imaging, such as ultrahigh fieldstrength MRI systems, new fMRI contrasts and diffusion tensorimaging,45 could give rise to the production of brain activationmaps with higher spatial resolution and validity for interpretation,46
allowing us to understand the cognitive processing of the brainand the neuropsychology behind dental phobia in more detail.
Genomewide association studies, combined with new informationobtained from neuroimaging and molecular genetic studies, canallow us to identify the biological processes involved with specificgenes involved with dental phobia, e.g. heightened pain sensitivity,over-activation of anxiety pathway.44 With increased availability ofthese techniques and the emergence of personalised medicine,interpretations of a patient’s MRI scan and genetic “fingerprint”,alongside with psychometric assessments, could be incorporatedto tailor therapy for dental anxiety.
Prevention of dental phobia andpaediatric sedationWith half of the population reporting onset of dental phobia inchildhood,47 it’s crucial to take a shift towards its prevention.Current behaviour management techniques used for children withdental anxiety, such as relaxation and distraction, are mainlytargeted to modify the child’s behaviour to make it easier toperform dental procedures.48 Meta-analysis48 also suggested thereare a lack of studies investigating the effectiveness of differentapproaches towards preventing dental anxiety in children. Whilepromoting a warm and welcoming child-friendly environment andavoidance of negative experiences may be useful in preventingdental phobia, there’s little evidence supporting these approachesand longitudinal studies exploring the predictors of phobiadevelopment would be crucial in designing effectiveinterventions.6,48
Children with behavioural management problems, severe dentalanxiety and in need of complicated treatments are often indicatedas needing conscious sedation.49 In recent years, medications usedin sedation and anaesthesia have been suggested to causedamage to the developing brain.50,51 However, bias from otherconfounding factors are often present in these studies52 andadverse neurological outcomes could be difficult to recognise.53
With advances in neuroscience and improved study designs, long-term effects and safety of paediatric anaesthesia could then beconfirmed. A Cochrane review54 published recently also highlightedthe lack of quality research in the efficacy of sedative agents usedin paediatric dentistry, with weak evidence supporting the currentuse of oral midazolam and nitrous oxide. In addition, only one newsedative, dexmedotomidine, was introduced in the past decade,showing that researches in new methods of delivery and newsedative drugs are certainly lacking.55 New drugs, such asremimidazolam56 and derivatives of etomidate57, are currentlyundergoing clinical investigations and could potentially offerbenefits in the future. With improvements in safety of deliveryequipment, paediatric sedation could become slowly moreavailable in dental practice rather than hospital settings alone.55
Virtual Reality technologyAdvances in virtual reality (VR) technology in the last decade haveopened many research opportunities into the treatment of mentalhealth, of which virtual reality exposure therapy (VRET) isdeveloped in treating specific phobias. The therapy allows patientsto confront their fears by immersing them in a virtual environmentthat integrates real-life computer graphics, body tracking devices,visual displays and sensory input devices.58 Despite success of thetherapy being reported in treatment of phobias of flying and

44 SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNERbrain activity patterns are identified using rtfMRI and thesepatterns will be compared to the ideal pattern. These patterns willthen be repeatedly induced without explicit presentation of thestimulus during neural reinforcement sessions, while the patientswill receive feedback on how close their current brain activitypatterns are to the desired healthy pattern, thus slowly inducing achange in behaviour as the patient learns to induce the idealneural pattern.63 Success of this technique has been reported invarious treatments, such as chronic pain control64, depression65 andsmoking addiction66, thus prompting a recent study by Koizumi etal.67 in exploring the possibility of applying this technique intreatments of phobia. Using the concept of counter-conditioning,when neural activation patterns that represent a conditioned fear-specific stimulus shows up on the patients’ rtf MRI scans, thepatients will be rewarded while remaining unaware of theintention of the procedure, thus slowly dampening patient’s feartowards the stimulus. Without an explicit presentation of thestimulus, dental phobic patients may find it easier to accept thisintervention than exposure therapy.
Future developments of this technique will coincide of that ofneuroimaging techniques, with clearer physiological signals tofacilitate better neurofeedback performance.68 Fundamental issues,such as the long-term effectiveness of the intervention andidentification of suitable candidates, will need to be addressedbefore clinical translation.
Computerised CBTCognitive behaviour therapy (CBT), a brief psychological therapycombining behaviour modification techniques and cognitiverestructuring procedures,6 is proven to be successful in treatingDFA.69 However, CBT services are often only available fortreatments of depression and general anxiety issues.6 A study byTellez et al.70 demonstrated the successful use of computerisedCBT in reducing patients’ DFA. The intervention, based on apsychoeducation module, educates the patients on the nature ofDFA and the advantages of overcoming their phobia. Theintervention also includes exposure exercises and motivationenhancements to encourage attendance in future dentalappointments.
Although further trials addressing the effectiveness of theintervention are needed, computerised CBT, without needing one-to-one interventions with a clinician trained in psychotherapy, willhave a potential role in increasing accessibility of CBT to dentalphobic patients.
Use of a post-retrieval amnesic agentA study by Soeter and Kindt71 recently addressed the feasibility ofusing post-retrieval amnesic agent in one session therapy intreating phobias. In the study, participants with spider phobia weregiven a single oral dose of propranolol, a medication that disruptsreconsolidation of fear memories, after exposing the participantsto a tarantula for 2 minutes. Results have been promising andchange in fear behaviour was still observed even after a year.
At present, studies72 investigating the effectiveness of thisintervention on dental phobia are ongoing. Future research carried
spiders,58 it is not well explored as an approach to treat dentalphobia. To treat dental phobia in VRET, patients will experiencevirtual reality scenarios, such as receiving a basic oral examinationand injection set in a simulated dental clinic in first person view.59
VR technology is also applicable in treating patients with mild tomoderate dental anxiety, for instance, the use of virtual realitydistraction system showing relaxing nature worlds was found tohelp patients in reducing anxiety and pain during dentalprocedures.60
Fig. 261: A dentally anxious patient using VR distractionhttp://journals.plos.org/plosone/article?id=10.1371/journal.pone.0091276
Future developments in VR technology could allow thecontribution of multimodal stimuli (visual, auditory, tactile andolfactory) in VRET, giving patients a sense of actual presence in thevirtual world.62 With an increase in portability and a decrease inequipment cost in the future, VRET could be made available inhome-use as well as private practice, allowing patients who are tooanxious to undergo real-life exposure therapy to face their fears.VRET also gives the possibility of generating gradual assignmentswith increasing intensity, allowing patients to face their fears attheir own pace.62 Other than VRET, VR can also be augmented toprovide other psychological interventions, such as hypnosis andbiofeedback, thus increasing availability of these interventions in aclinical setting.62 Investigations about the neurobiologicalmechanisms underlying the analgesic effects of VR are currentlyongoing, which will be critical in developing age anddevelopmentally appropriate clinical interventions for painmanagement as an alternative to pharmacologic analgesia.62
Decoded fMRI neurofeedback(DefNef) DefNef is a recently developed technique that combines the use ofreal life functional (rtf MRI) and online feedback system. As thesubject is being evoked by the presentation of a stimulus, certain
! ! !( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
((
(( ( ( ( ( ( ( ( (
(((
( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( (
( ( ( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( ( (

45SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNERout could aim to outline the optimal conditions to trigger memoryreconsolidation in clinical settings. Because it requires only onetherapy and doesn’t demand extensive psychotherapy training forprofessionals, this intervention has several cost-effectivenessadvantages.71
ConclusionManagement of dentally anxious patients could be challengingand potentially problematic for the dental team. Yet, withaccelerating technological advances and explosion of scientificdiscoveries, a more diverse range of cost-effective options could bemade available in the future to dentally anxious patients toovercome their fears.
Application of pharmacogenomics and robotic delivery look likelyto increase the safety and availability of conscious sedation andGA. Aetiology of DFA will be more effectively understood with thedevelopment of neuroimaging and molecular geneticstechnologies, allowing dentists to yield a far more diverse and“personalised” therapy for the patient. Overall, technologicaldevelopments look set to yield positive developments in the fieldof DFA. These opportunities should be capitalised upon, withresearch focusing on the relative benefits of each technique.
References 1. Freeman R. The psychology of dental patient care: Barriers to accessing dental
care: patient factor. Br Dent J 1999; 187: 141-144.
2. Eitner S, Wichmann M, Paulsen A, Holst S. Dental anxiety – an epidemiologicalstudy on its clinical correlation and effects on oral health. J Oral Rehabil 2006; 33:588-593.
3. Cohen S, Fiske J, Newton J. Behavioral dentistry: The impact of dental anxiety ondaily living. Br Dent J 2000; 189: 385-390.
4. Morgan A G, Porritt J. Background and Prevalence of Dental Fear and Anxiety. InCampbell C (ed) Dental Fear and Anxiety in Pediatric Patients: Practical Strategiesto Help Children Cope. pp 3-20. Switzerland: Springer International Publishing,2017.
5. Access and barriers to care- a report from the Adult Dental Health Survey 2009.London: The Health and Social Care Information Centre, 2011.
6. Newton T, Asimakopoulou K, Daly B, Scambler S, Scott S. The management ofdental anxiety: time for a sense of proportion?. Br Dent J 2012; 213: 271-274.
7. Gerhardus D. Robot-assisted surgery: the future is here. J Healthc Manag 2003; 48:242-251.
8. Hussain A, Malik A, Halim M U, Ali A M. The use of robotics in surgery: a review. IntJ Clin Pract 2014; 68: 1376-1382.
9. Hamet P, Tremblay J. Artificial intelligence in medicine. Metabolism 2017; 69S: S36-S40.
10. Hemmerling T M, Cirillo F, Cyr S. Decision Support Systems in Medicine:Anesthesia, Critical Care and Intensive Care Medicine. InTech 2012.
11. Wehbe M, Arbeid E, Cyr S, Mathieu P, Taddei R, Morse J et al. A technicaldescription of a novel pharmacological anesthesia robot. J Clin Monit Comput2013; 28: 27-34.
12. Hemmerling T, Arbeid E, Wehbe M, Cyr S, Taddei R, Zaouter C. Evaluation of a novelclosed-loop total intravenous anaesthesia drug delivery system: a randomizedcontrolled trial. Br J Anaesth 2013; 110: 1031-1039.
13. Hemmerling T, Charabti S. McSleepy™ – A Completely Automatic AnesthesiaDelivery System. Anesthesiology 2009: A460.
14. Zaouter C, Hemmerling T, Lanchon R et al. The Feasibility of a CompletelyAutomated Total IV Anesthesia Drug Delivery System for Cardiac Surgery. AnesthAnalg 2016; 123: 885-893.
15. Banerjee S, Desilets D, Diehl D L et al. Computer-assisted personalized sedation.Gastrointest Endosc 2011; 73: 423-427.
16. Pambianco D, Vargo J, Pruitt R, Hardi R, Martin J. Computer-assisted personalizedsedation for upper endoscopy and colonoscopy: a comparative, multicenterrandomized study. Gastrointest Endosco 2011; 73: 765-772.
17. Pambianco D, Whitten C, Moerman A, Struys M, Martin J. An assessment of com-puter-assisted personalized sedation: a sedation delivery system to administerpropofol for gastrointestinal endoscopy. Gastrointest Endosco 2008; 68: 542-547.
18. Urman R D, Maurer W G. Computer-Assisted Personalized Sedation: Friend or Foe?.Anesth Analg 2014; 119: 207-211
19. Atchabahian A, M Hemmerling T. Robotic Anesthesia: How is it Going to ChangeOur Practice?. Anesth Pain Med 2014; 3: e16468.
20. Summary of Safety and Effectiveness Data (SSED): Computer-AssistedPersonalized Sedation System. Silver Spring: U S Food and Drug Administration,2013.
21. Hemmerling T M, Taddei R, Wehbe M et al. Robotic Anesthesia – A Vision for theFuture of Anesthesia. Transl Med UniSa 2011; 1: 1-20.
22. Oscarson M. Pharmacogenetics of Drug Metabolising Enzymes: Importance forPersonalised Medicine. Clin Chem Lab Med 2003; 41: 573-580.
23. Khan M, Zetterlund E, Gréen H et al. Pharmacogenetics, Plasma Concentrations,Clinical Signs and EEG During Propofol Treatment. Basic Clin Pharmacol Toxicol2014; 115: 565-570.
24. Nagele P, Zeugswetter B, Wiener C et al. Influence of MethylenetetrahydrofolateReductase Gene Polymorphisms on Homocysteine Concentrations after NitrousOxide Anesthesia. Anesthesiology 2008; 109: 36-43.
25. Lacassie H. Reversible nitrous oxide myelopathy and a polymorphism in the geneencoding 5,10-methylenetetrahydrofolate reductase. Br J Anaesth 2006; 962: 222-225.
26. Selzer R, Rosenblatt D, Laxova R, Hogan K. Adverse Effect of Nitrous Oxide in aChild with 5,10-Methylenetetrahydrofolate Reductase Deficiency. N Engl J Med2003; 349: 45-50.
27. Floyd M D, Gervasini G, Masica A L et al. Genotype–phenotype associations forcommon CYP3A4 and CYP3A5 variants in the basal and induced metabolism ofmidazolam in European- and African-American men and women.Pharmacogenetics 2003; 13: 595-606
28. Qin X P, Xie H G, Wang W et al. Effect of the gene dosage of CYP2C19 on diazepammetabolism in Chinese subjects. Clin Pharmacol Ther 1999; 66: 642-646
29. Golzari S, Soleimanpour H, Mahmoodpoor A, Safari S, Ala A. Lidocaine and PainManagement in the Emergency Department: A Review Article. Anesth Pain Med2014; 4: e15444.
30. Liem E, Joiner T, Tsueda K, Sessler D. Increased Sensitivity to Thermal Pain andReduced Subcutaneous Lidocaine Efficacy in Redheads. Anesthesiology 2005;102: 509-514.
31. Haga S. Using Pharmacogenetics to Improve Drug Safety and Efficacy. JAMA 2004;291: 2869-2871.
32. Garg N, Garg A. Textbook of Operative Dentistry. 3rd ed. New Delhi: JaypeeBrothers Medical Publishers, 2015.
33. Executive Summary: Adult Dental Health Survey 2009. London: The Health andSocial Care Information Centre, 2011.
34. Freitas R. NANODENTISTRY. J Am Dent Assoc 2000; 131: 1559-1565.
35. Shetty N J, Swati P, David K. Nanorobots: Future in dentistry. Saudi Dent J 2013; 25:49-52.
36. Elgart A, Cherniakov I, Aldouby Y, Domb A, Hoffman A. Lipospheres and pro-nanolipospheres for delivery of poorly water soluble compounds. Chem Phys Lipids2012; 165: 438-453.
37. De Rosa G, Salzano G, Caraglia M, Abbruzzese A. Nanotechnologies: A Strategy toOvercome Blood-Brain Barrier. Curr Drug Metab 2012; 13: 61-69.
38. Sharma D, Sharma R K, Bhatnagar A et al. Nose to Brain delivery of MidazolamLoaded PLGA Nanoparticles: In Vitro and In Vivo Investigations. Curr Drug Deliv2016; 13: 557-564.
39. Hassani Najafabadi A, Azodi-Deilami S, Abdouss M, Payravand H, Farzaneh S.Synthesis and evaluation of hydroponically alginate nanoparticles as novel carrierfor intravenous delivery of propofol. J Mater Sci Mater Med 2015; 26: 145.
40. McGuire P K, Matsumoto K. Functional neuroimaging in mental disorders. WorldPsychiatry 2004; 3: 6-11.
41. Schienle A, Scharmüller W, Leutgeb V, Schäfer A, Stark R. Sex differences in thefunctional and structural neuroanatomy of dental phobia. Brain Struct Funct2013; 218: 779-787.
42. Scharmüller W, Leutgeb V, Schöngaßner F, Hermann A, Stark R, Schienle A. Alteredfunctional connectivity of basal ganglia circuitry in dental phobia. Soc CognAffect Neurosci 2013; 9: 1584-1588.
43. Carter A E, Carter G, Boschen M, AlShwaimi E, George R. Pathways of fear andanxiety in dentistry: A review. World J Clin Cases 2014; 2: 642-653.
44. Randall C, Shaffer J, McNeil D, Crout R, Weyant R, Marazita M. Toward a geneticunderstanding of dental fear: evidence of heritability. Community Dent OralEpidemiol 2016; 45: 66-73.
45. Fritz J. Neuroimaging Trends and Future Outlook. Neurol Clin 2014; 32: 1-29.
46. Bandettini P. What's New in Neuroimaging Methods?. Ann N Y Acad Sci 2009;1156: 260-293.
47. Locker D, Liddell A, Dempster L, Shapiro D. Age of Onset of Dental Anxiety. J DentRes 1999; 78: 790-796.
48. Öst L, Skaret E. Future research and applications. In Öst L, Skaret E (ed) CognitiveBehavioral Therapy for Dental Phobia and Anxiety. pp 221-229. Chichester: Wiley-Blackwell, 2013.

46 SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNER49. Hallonsten A, Jensen B, Raadal M et al. EAPD Guidelines on sedation in paediatric
dentistry. Eur Arch Paediatr Dent 2003: 8-9.
50. Sun L. Early childhood general anaesthesia exposure and neurocognitivedevelopment. Br J Anaesth 2010; 105: i61-i68.
51. Stratmann F. Review article: Neurotoxicity of anesthetic drugs in the developingbrain. Anesth Analg 2011; 113: 1170-1179.
52. Vutskits L. Anesthetic-Related Neurotoxicity and the Developing Brain. PediatrDrugs 2012; 14: 13-21.
53. Nelson T, Xu Z. Pediatric dental sedation: challenges and opportunities. ClinCosmet Investig Dent 2015; 7: 97.
54. Lourenço-Matharu L, Ashley P F, Furness S. Sedation of children undergoingdental treatment. Cochrane Database Syst Rev 2012; 3: Cd003877.
55. Mason K. Challenges in paediatric procedural sedation: political, economic, andclinical aspects. Br J Anaesth 2014; 113: ii48-ii62.
56. Antonik L, Goldwater D, Kilpatrick G, Tilbrook G, Borkett K. A Placebo- andMidazolam-Controlled Phase I Single Ascending-Dose Study Evaluating theSafety, Pharmacokinetics, and Pharmacodynamics of Remimazolam (CNS 7056):Part I. Safety, efficacy, and basic pharmacokinetics. Anesth Analg 2012; 115: 274-283.
57. Cotton J F, Husain S S, Forman S A. Methoxycarbonyl-etomidate: a novel rapidlymetabolized and ultra–short-acting etomidate analogue that does not produceprolonged adrenocortical suppression. Anaesthesiology 2009; 111: 240-249.
58. Powers M, Emmelkamp P. Virtual reality exposure therapy for anxiety disorders: A meta-analysis. J Anxiety Disord 2008; 22: 561-569.
59. Raghav K, Van Wijk A, Abdullah F, Islam M, Bernatchez M, De Jongh A. Efficacy ofvirtual reality exposure therapy for treatment of dental phobia: a randomizedcontrol trial. BMC Oral Health 2016; 16: 25.
60. Wiederhold M, Gao K, Wiederhold B. Clinical Use of Virtual Reality DistractionSystem to Reduce Anxiety and Pain in Dental Procedures. Cyberpsychol BehavSoc Netw 2014; 17: 359-365.
61. Tanja-Dijkstra K, Pahl S, White M P et al. Improving Dental Experiences by UsingVirtual Reality Distraction: A Simulation Study. PLoS One 2014; 9: e91276.
62. Li A, Montaño Z, Chen V, Gold J. Virtual reality and pain management: currenttrends and future directions. Pain Manag 2011; 1: 147-157.
63. Shibata K, Watanabe T, Sasaki Y, Kawato M. Perceptual Learning Incepted byDecoded fMRI Neurofeedback Without Stimulus Presentation. Science 2011; 334:1413-1415.
64. deCharms R, Maeda F, Glover G et al. Control over brain activation and painlearned by using real-time functional MRI. Proc Natl Acad Sci U S A 2005; 102:18626-18631.
65. Linden D, Habes I, Johnston S et al. Real-Time Self-Regulation of EmotionNetworks in Patients with Depression. PLoS ONE 2012; 7: e38115.
66. Li X, Hartwell K, Borckardt J et al. Volitional reduction of anterior cingulate cortexactivity produces decreased cue craving in smoking cessation: a preliminary real-time fMRI study. Addict Biol 2012; 18: 739-748.
67. Koizumi A, Amano K, Cortese A et al. Fear reduction without fear throughreinforcement of neural activity that bypasses conscious exposure. Nat HumBehav 2016; 1 : 0006.
68. Sulzer J, Haller S, Scharnowski F et al. Real-time fMRI neurofeedback: progress andchallenges. Neuroimage 2013; 76: 386-399.
69. Kani E, Asimakopoulou K, Daly B et al. Characteristics of patients attending forcognitive behavioural therapy at one UK specialist unit for dental phobia andoutcomes of treatment. Br Dent J 2015; 219: 501-506.
70. Tellez M, Potter C, Kinner D et al. Computerized Tool to Manage Dental Anxiety. J Dent Res 2015; 94: 174S-180S.
71. Soeter M, Kindt M. An Abrupt Transformation of Phobic Behavior After a Post-Retrieval Amnesic Agent. Biol Psychiatry 2015; 78: 880-886.
72. Steenen S, van Wijk A, van Westrhenen R, de Lange J, de Jongh A. Effects ofpropranolol on fear of dental extraction: study protocol for a randomizedcontrolled trial. Trials 2015; 16: 536.
SAADESSAY PRIZES
Three essay prizes are available annually
Drummond-Jackson Essay Prize of £500
Dental Student Essay Prize of £300
DCP Essay Prize of £300
Details on page 81

47SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNER
AbstractThe aim of managing dental anxiety is to work towards eradicatingthe fear of the dentist, enabling the provision and maintenance oforal health. In order to understand the extent of the impact of oralhealth on overall health, a greater infiltration in the medicalprofession is needed in the future. Current practice in dentistry hasfavoured the use of a single-drug method of midazolamadministration, however, despite its excellent properties comparedwith previously used agents, it is not always the ideal drug forintravenous sedation. The increase in the size of the elderlypopulation and prevalence of bariatric patients has seen changesin clinical practice. The next 60 years of dentistry will surely see thedevelopment of increasingly effective sedation agents, such asremimazolam. It will be interesting to see if this new member ofthe benzodiazepine family will find a place in dentistry. Goodquality evidenced-based research will need to be conducted toestablish any potential in dentistry, in comparison with the safetyand efficiency of midazolam, of any new drug with anxious dentalpatients. Other future changes in clinical practice will be reliant onsustainability plans, with the possible increase in provision ofcommunity hubs.
IntroductionAnxiety management is an important aspect to consider whenproviding dental treatment. Looking back at the development ofdental management methods for anxiety, fear and phobia gives anappreciation of the many techniques currently available to thedental team.
These techniques can be broadly split into two categories;pharmacological and non-pharmacological. Using pharmacologicalmodalities can provide more comfortable treatment and reducethe likelihood of patient avoidance and encourage regularattendance.1,2 The use of local anaesthesia proved to be animmense development in dentistry and has changed patients’perspectives of dental procedures to a great extent.3
Conscious sedation is another pharmacological adjunct which is animportant fundamental aspect of the modern practice of dentistryand is considered by many to be an integral element in controllingpain and anxiety when delivering dental care.1,4 It should beremembered that although sedation is a proven technique fordealing with dental phobia, it should not be used an alternative toeffective local anaesthesia or good behavioural management.5
PharmacologicalPrior to the development of local anaesthesia, patients had toendure any pain without complaint and accept the inevitable;often prior self-medication with alcohol was the only way ofcoping with operative dental care.1 More treatment options arenow available to patients due to developments in moderndentistry and the development of safe and reliable localanaesthesia, successful administration of which remains the mostimportant skill for the practitioner.3 Effective anaesthesia and paincontrol can be all that is needed to manage anxiety depending onthe severity.6 It is widely recognised that the fear of dentalinjections remain a clinical problem and is a common trigger ofdental anxiety. For this reason alternatives to conventionalmethods of administering local anaesthetics are actively sought.7,8
Topical anaesthetic agents and the development of computer-controlled anaesthetic delivery systems, such as the Wand, havehelped minimise pain and discomfort whilst delivering localanaesthesia.3,9 Innovative techniques are being developed, withone study examining a nasal spray to induce anaesthesia ofanterior maxillary teeth and measuring its efficacy, safety andtolerability in patients.10 Newer improved devices include thesyringe micro vibrator (SMV) designed to provide a practical wayto relieve injection pain.11 These are promising advancements inpain and anxiety management, and devices like these couldpotentially be the future of everyday clinical practice.
Despite these advances, routine dental treatment is not alwaystolerated using local anaesthetics alone and some surgicalinterventions render local anaesthesia insufficient. Conscioussedation can provide an adjunct to local anaesthesia and soappropriate patients need not fear surgical procedures in thefuture.12,13 Both conscious sedation and general anaesthesia aretwo pharmacological intervention techniques available.8,14
Conscious SedationPharmacological methods to manage anxiety have beendeveloped over the years with dentists often at the forefront ofanaesthesia research, many of the world's first anaesthetics weregiven in a dental setting.15,16 It is this ongoing research anddevelopment that has seen a historical shift from using onesedative agent to another, with each showing advantages over itspredecessor. Further developments in the drugs and techniquesused for dental conscious sedation have formulated the practiceseen today. Nowadays sedation techniques are classified as eitherbasic or advanced.4 The basic techniques of conscious sedationhave been found to be safe and effective for the management of
Anxiety Management and Sedation in Dentistry; the next60 years?Kimberley Illing BSc (Hons)
Specialist Dental NurseKing’s College Hospital Dental Institute, Denmark Hill, London, SE5 9RS
Corresponding Author: [email protected]

48 SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNERcomplications are much lower if identified and treated pre-operatively with continuous positive airway pressure (CPAP).31 Thishas prompted the development of new devices one of which is theOptiflow which provides pre-oxygenation via a nasal cannula toextend the apnoea time of patients with difficult airways, and iscurrently being trialled in general anaesthesia.32 This practice couldbe transferable to dental conscious sedation, but research isrequired to validate this.
Obese individuals have an increased risk of cardiovascular disease,diabetes and pulmonary disease.28,29 These physiological changesare likely to result in altered drug pharmacokinetics.30 This has leadthe focus of modern research in anaesthesia on soft drugdevelopment (self-metabolising, organ-independent drugs).22,25,27
Current developments in anaesthesia are primarily focused on thetargeted modification of structures of existing compounds in orderto improve their pharmacodynamic and pharmacokineticproperties, specifically against the two most commonly usedagents, midazolam and propofol. It is against these two agents thatany newly developed ones will be assessed.22 An innovativemember of the benzodiazepine group of drugs, remimazolam (CNS7056), is currently being investigated in clinical trials.25 Thestructure of remimazolam was modified to produce a drug that isindependently metabolised and not dependant on organmetabolism.33 It combines the properties of two unique drugs,midazolam and remifentanil. Remimazolam acts on GABAreceptors like midazolam and its metabolism occurs in the blood,thus it is organ-independent like remifentanil, a desirable trait forthe increasing number of medically compromised patients.26
Similar to currently used midazolam, remimazolam has the abilityto be reversed with the antagonist flumazenil. This makes it highlydesirable when given by non-anaesthetists not highly trained inairway management which adds to its safety were an overdose tolead to significant respiratory depression.22
After the introduction of midazolam, attempts were made toidentify short-acting benzodiazepines, but these showed nosignificant advantages over midazolam. So why is remimazolamdifferent?34
Based on the existing data, remimazolam does appear to havepotential advantages over midazolam. The time to recover fromsedation is shorter and more consistent with remimazolamcompared to midazolam.33 It shows great promise as a sedativeagent for outpatient sedation where fast and predictable onset ofaction26 and rapid recovery is highly desirable.22 However, thestandard titration techniques of intravenous midazolam sedationare approved and have excellent safety records5,19 when it isadministered according to guidelines12 and its use is notcontraindicated. Short-acting drugs require an infusion methoddue to increased potency.34 Acceptance within the dentalprofession is largely determined by convenience of administration;sedation by bolus injections is preferred over infusion pumpmethods.34 In addition, the definition of conscious sedation mustbe kept in mind, which refers to ‘a margin of safety wide enough torender loss of consciousness unlikely’.5
Another point worth considering is the management of failedsedation appointments. Robb20 demonstrated how the logical useof advanced sedation techniques allowed patients, who wereunmanageable with the basic sedation techniques, to receive
anxiety in adult dental patients requiring sedation to allow them toundergo dental treatment.5 These include inhalation sedation withnitrous oxide, oral or transmucosal benzodiazepine sedation andintravenous sedation with a titrated dose of midazolam. Followingits first use in 1983, midazolam still remains recognised as the drugof choice for intravenous sedation in anxious patients.1, 2
Advanced conscious sedation techniques are far less widely used,and more complex to administer than the basic techniques, but forpatients with high levels of anxiety the standard techniques ofsedation are not always appropriate or successful.17,18 Midazolamcan be used along with other agents, such as an opioid, propofoland/or ketamine, to obtain better sedative effects.19,20 Propofol is asedative-hypnotic agent that was introduced in 1977. It hasminimal side effects and rapid recovery, but unlike midazolam ithas no antagonist.1,2,21 In general, midazolam is used to producesedation, and propofol to induce general anaesthesia, but propofolcan be used as an intravenous sedative agent in adults. However,when used at appropriate doses, both agents may achieve eitherclinical endpoint thus requiring specific training in theiradministration.1,2,17,22 The pain caused by propofol on injection cancontraindicate the very reason, to remediate pain, that its use ishoping to achieve.2 Studies have been conducted using patient-controlled sedation with good results.23,24 A lack of control duringdental treatment can provoke a patient's fear and returning thecontrol to the patient can help to decrease anxiety.14 It was foundthat propofol had favourable properties for patient-controlledsedation, and provided a safe and acceptable intra-operativeanxiolysis for phobic dental patients.23
Every drug has its drawbacks in clinical practice despite havingbeen established in anaesthesia due to its properties of deliveringrelatively safe and effective outcomes.25 Currently, there is noclinically available hypnotic agent that possesses all of the desiredproperties required in such a drug. Both midazolam and propofolpossess significant advantages for sedation over hypnosis,however, their limitations present the incentive to continue tosearch for new innovative anaesthetic agents.22 Many areunconvinced that a single drug will ever be found that could meetall the pharmacological and safety requirements.26 Driving thedevelopment of new sedative and anaesthetic drugs has been thechange in demands of clinical practice over the last decade. Boththe practice of anaesthesia and the dental profession have seen anincreasingly older population with a greater number ofcomorbidities.22 The elderly show increased sensitivity toanaesthetic medications and often have exaggerated effects dueto their decreased rates of metabolism and excretion, which canprolong the effects of the agent and postpone recovery.27 Thedramatic prevalence of obesity has also demanded a change inclinical services, with a global surge in the prevalence of bariatricpatients.28-30 The Society for Obesity and Bariatric Anaesthesia’s(SOBA) guidelines state that obese patients are not suitable forsingle operator-sedation procedures, as with sleep-disorderedbreathing, they are likely to have airway obstruction with evenminimal sedation.31 This could have implications for the largerpatient having conscious sedation for dental treatment in thefuture, thus requiring a second practitioner. A reason for this issleep-disordered breathing, which describes the spectrum ofconditions ranging from obstructive sleep apnoea (OSA) throughto obesity hypoventilation syndrome (OHS). The risks of

49SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNERdental treatment under sedation rather than having to resort togeneral anaesthesia. It is highly likely the future will continue tosee an increase in these advanced techniques to avoid the risks ofgeneral anaesthesia and ultimately maintain cost-effectiveness.35
Another advanced technique is the use of sevoflurane, studied asan alternative to nitrous oxide, particularly due to its minimalimpact on the environment.1
With the potential increase in use of advanced techniques,additional respiratory monitoring of bariatric patients may berequired during sedation, for their safety. Current guidelines areunable to recommend the routine use of capnography because ofthe lack of evidence based dental-specific research.4 This void hasprompted researchers to look at the use and validity ofimplementing capnography monitoring alongside pulseoximetry.36 Nevertheless, if advanced sedation techniques becomemore widely employed and practised, as polypharmacy sedation ismore risky, it is essential the patient's respiratory function bemonitored closely.2,23 Will the future of sedation see sampledexhaled gas or transcutaneous capnography as the gold standardof intra-operative monitoring?4,36 If warranted by new research,future changes in practice will undoubtedly result in changes toexisting guidelines. It is essential for the whole dental team to keepup to date with the latest guidelines, to ensure patient safety.
Non-pharmacologicalGiven the complexity of treating bariatric patients and anincreasingly elderly population, it is highly likely there will be anincrease in use of alternative non-pharmacological modalities.These anxiety management techniques are simple to perform,12
ranging from good communication and establishing rapport, tothe use of systematic desensitisation and hypnosis.37 Assessment ofthe patient is paramount to identify the causes of anxiety, and toestablish the patient’s expectations of treatment. Deciding whattechniques are required depends on the level of the anxiety and isultimately adapted to the patient’s individual needs.12,38 The art ofhypnosis has great therapeutic benefits in dentistry, ranging fromsimple relaxation of the anxious patient, to complete analgesia forsurgery, with no after effects and no drugs required.12,39 A powerfultool yet poorly understood, hypnosis can provide effective‘sedation’, whilst leaving the patient in full control.39
Thom et al.40 compared psychological behavioural and cognitivebehavioural approaches to managing dental phobia, seeinggreater changes with the long-term management of anxiety, asopposed to a one session administration of pharmacologicalagents. Annual follow-ups of these patients revealed reducedlevels of dental anxiety and a greater frequency of visiting adentist.41 This may be due to the amnesic effects of somepharmacological agents.2 It is necessary to escalate the justificationand the increasing relevance of psychology and behaviouralsciences to dental training and clinical practice.42 Hill et al.43 foundboth undergraduates and postgraduates would be interested infurther training if financial support was available, the key is toincrease confidence with additional behavioural managementskills.39
Alternative methods for anxiety management may include the useof the olfactory system and the effects of aromatherapy,particularly lavender and orange scents, and to investigate their
impact on anxiety, mood, alertness and calmness in dentalpatients.44,45 It has been shown that odours are capable of alteringemotional states and have proved helpful in reducing anxiety indental patients.45 Another alternative method is acupuncturewhich is a generally safe and non-toxic supplement toconventional treatment46 and produces negligible adversereactions.47 Clinical trials have shown that ear acupuncture is aseffective as intranasal midazolam in reducing dental anxiety andthe gag reflex.47
An additional, widely acknowledged cause of anxiety is the fear ofthe dental drill.6 Modern developments such as air abrasion andlasers may increasingly be used in conjunction with, or replace,traditional methods.48-50 These developments, although notcurrently implemented in everyday practice, are important givingthe hope to eradicate the use of the dental drill and to changeperceptions of dentistry by removing this major contributingfactor to anxiety.
SustainabilityIt is important, when looking at the future, to be aware ofproposals concerning the sustainability of the National HealthService. These will undoubtedly impact the delivery of dental care,despite practitioner preference for advanced techniques forpaediatric patients to be delivered in a secondary care setting.51
There is a growing need for sustainability and transformationplanning of special care dentistry.52 As hospitals are becomingoverwhelmed, there needs to be greater primary care access andprovision for anxious patients. It will be necessary to increaseaccessibility of alternative treatments in practice and communitycentres.52 As part of an integrated care pathway (ICP), low-levelpsychological intervention delivered by dental nurses showedsignificant reduction in dental anxiety.53 Care pathways are alsodiscussed in the Intercollegiate Advisory Committee for Sedationin Dentistry (IACSD) standards.4
ConclusionAs well as remimazolam, other compounds have been synthesiseddue to changes in clinical practice. This has given rise toanaesthesia research in the pursuit of more suited agents.22
Unpinning evidence-based practice of new agents is needed andshould be dental specific, to ensure patient safety is paramount.
Klass et al.28 highlights the importance of managing oral health inrelation to other conditions. It is important the dental teamencourage regular attendance; if oral health impacts on chronicdiseases, providing effective anxiety management techniques forthe attendance of the dental phobic patient to be possible.
References:1. Craig D C, Skelly A M. Practical Conscious Sedation. 1st ed. London: Quintessence,
2004.
2. Ireland R S. Advanced dental nursing. 2nd ed. London: Wiley-Blackwell, 2010.
3. Saxena P, Gupta S K, Newaskar V, Chandra A. Advances in dental local anesthesiatechniques and devices: an update. Natl J Maxillofac Surg 2013; 4: 19-24.
4. Intercollegiate Advisory Committee for Sedation in Dentistry. Standards forConscious Sedation in the Provision of Dental Care. Royal College of Surgeons ofEngland, 2015.

50 SAAD DIGEST | VOL.34 | 2018
SAAD ESSAY PRIZE WINNER5. Craig D C, Wildsmith J A. Conscious sedation for dentistry: an update. Br Dent J
2007; 203: 629-631.
6. Mellor A. Management of the anxious patient: what treatments are available?Dent Update 2007; 34: 108-114.
7. Armfield J M, Milgrom P. A clinician guide to patients afraid of dental injectionsand numbness. Saad Dig 2011; 27: 33-39.
8. Rafique S, Banerjee A, Fiske J. Management of the petrified dental patient. DentUpdate 2008; 35: 196-207.
9. Versloot J, Veerkamp J S J, Hoogstraten J. Pain behaviour and distress in childrenduring two sequential dental visits: comparing a computerised anaesthesiadelivery system and a traditional syringe. Br Dent J 2008; E2: 205.
10. Ciancio S G, Hutcheson M C, Ayoub F et al. Safety and efficacy of a novel nasalspray for maxillary dental anesthesia. J Dent Res 2013; 92: 43S-8S.
11. Hashem A, Bonjar S. Syringe micro vibrator (SMV) a new device being introducedin dentistry to alleviate pain and anxiety of intraoral injections, and a comparativestudy with a similar device. Ann Surg Innov Res 2011; 5: 1.
12. Odell E W. Clinical problem solving in dentistry. 3rd ed. London: Churchill-Livingstone, 2010.
13. Juodzbalys G, Giedraitis R, Mačhiulskienė V, Luc W. J, Huys L W J. Kubilius R. Newmethod of sedation in oral surgery. J Oral Implant 2005; 31: 304-308.
14. Appukuttan D P. Strategies to manage patients with dental anxiety and dentalphobia: literature review. Clin Cosmet Investig Dent 2016; 8: 35-50.
15. Beirne O R. Current and future research in dental sedation and anesthesia. AnesthProg 1986; 33: 193-196.
16. Finder R. The art and science of office-based anesthesia in dentistry: a 150-yearhistory. Inter Anesth Cli 2003; 41: 1-12.
17. Craig D. Safe and effective sedation. Br Dent J 2011; 211: 343.
18. Girdler N M, Rynn D, Lyne J P, Wilson K E. A prospective randomised controlledstudy of patient-controlled propofol sedation in phobic dental patients. Anaesth2000; 55; 327-333.
19. Chen Q, Wang L, Ge L, Gao Y, Wang H. The Anxiolytic Effect of Midazolam in ThirdMolar Extraction: A Systematic Review. PLoS One 2015; 10: e0121410.
20. Robb N. The role of alternative (advanced) conscious sedation techniques indentistry for adult patients: a series of cases. Br Dent J 2014; 216: 223-227.
21. Cillo J E. Propofol anesthesia for outpatient oral and maxillofacial surgery. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1999; 87; 530-8.
22. Chitilian H V, Eckenhoff R G, Raines D E. Anesthetic drug development: Noveldrugs and new approaches. Surg Neurol Int 2013; 4: S2-S10.
23. Rodrigo C, Irwin M G, Yan B S, Wong M H. Patient-controlled sedation withpropofol in minor oral surgery. J Oral Maxillofac Surg 2004; 62: 52-56.
24. Rodrigo M R C, Tong C K A. A comparison of patient and anaesthetist controlledmidazolam sedation in the dental surgery. Anaesth 1994; 49: 241-244.
25. Wesolowski A M, Zaccagnino M P, Malapero R J, Kaye A D, Urman R D.Remimazolam: Pharmacologic considerations and clinical role in anesthesiology.Pharmacotherapy 2016; 36: 1021-1027.
26. Goudra B G, Singh P M. Remimazolam: The future of its sedative potential. Saudi JAnaesth 2014; 8: 388-391.
27. Pawloski J. Soft drug strategies in anesthesiology. Inter Anesth Cli 2015; 53: 55-62.
28. Klass C, Wanonyi S, White A, Walmsley D, Hunt N, Gallagher J E. A recipe for futureresearch. Br Dent J 2017; 222: 321.
29. Reilly D, Boyle C A, Craig D C. Obesity and dentistry: a growing problem. Br Dent J2009; 207: 171-175.
30. Morrish G A, Pai M P, Green B. The effects of obesity on drug pharmacokinetics inhumans. Exp opi drug meta tox 2011; 7: 697-706.
31. Association of Anaesthetists of Great Britain and Ireland. Peri-operativemanagement of the obese surgical patient 2015. Anaesth 2015; 70: 859-876.
32. Ang K S, Green A, Ramaswamy K K, Frerk C. Preoxygenation using the Optiflowsystem. Br J Anaesth 2017; 118: 463-464.
33. Rogers W K, McDowell T S. Remimazolam, a short-acting GABA (A) receptoragonist for intravenous sedation and/or anesthesia in day surgical and non -surgical procedures. IDrugs 2010; 13: 929-37.
34. Sneyd J, Robert M D. Remimazolam: new beginnings or just a me-too? AnaesAnalgesia 2012; 115: 217-219.
35. Jameson K, Averley P A, Shackley P, Steele J. A comparison of the ‘cost per childtreated’ at a primary care-based sedation referral service, compared to a generalanaesthetic in hospital. Br Dent J 2007; 203: E13.
36. Brady P J, Wilson K E, Meeke R, Girdler N M, McCreary C. Capnometry monitoringduring intravenous sedation with midazolam for oral surgery. Oral Surg 2016; 9:94-101.
37. Armfield J M, Heaton L J. Management of fear and anxiety in the dental clinic: areview. Aus Dent J 2013; 58: 390-407.
38. Newton T, Asimakopoulou K, Daly B, Scambler S, Scott S. The management ofdental anxiety: time for a sense of proportion? Br Dent J 2012; 213: 271-274.
39. Allison N. Hypnosis in modern dentistry: challenging misconceptions. Facul Dent J2015; 6: 172-175.
40. Thom A, Sartory G, Jöhren P. Comparison between one-session psychologicaltreatment and benzodiazepine in dental phobia. J Con Clin Psych 2000; 68: 378-387.
41. Getka E J, Glass C R. Behavioural and cognitive-behavioural approaches to thereduction of dental anxiety. Behav Therap 1992; 23: 433-448.
42. Facco E, Zanett G, Casigilia E. The role of hypnotherapy in dentistry. Saad Dig2014; 30: 3-6.
43. Hill K B, Hainsworth J M, Burke F J T, Fairbrother K J. Evaluation of dentistsperceived needs regarding treatment of the anxious patient. Br Dent J 2008; 204:E13.
44. Kritsidima M, Newton T, Asimakopoulou K. The effects of lavender scent on dentalpatient anxiety levels: a cluster randomized-controlled trial. Community Dent OralEpidemiol 2010; 38: 83–87.
45. Lehrner J, Marwinski G, Lehr S, Johren P, Deecke L. Ambient odors of orange andlavender reduce anxiety and improve mood in a dental office. Physiol behav2005; 86: 92-95.
46. Rosted P. Acupunture: Introduction to acupuncture in dentistry. Br Dent J 2000;189: 136-140.
47. Naik P N, Kiran R A, Yalamanchal S, Kumar V A, Goli S, Vashist N. Acupuncture: Analternative therapy in dentistry and its possible applications. Med Acupunct 2014;26: 308-314.
48. Walsh L J. The current status of laser applications in dentistry. Aus Dent J 2003; 48:146-155.
49. Santos-Pinto L, Peruchi C, Marker V A, Cordeiro R. Evaluation of cutting patternsproduced with air abrasion systems using different tip designs. Op Dent 2001; 26:308-312.
50. Hedge V S, Khatavkar R A. A new dimension to conservative dentistry: Airabrasion. J of Conser Dent 2010; 13: 4-8.
51. Coulthard P, Craig D, Holden C et al. Current UK dental sedation practice and the‘National Institute for Health and Care Excellence’ (NICE) guideline 112: sedationin children and young people. Br Dent J 2015; 218: E14.
52. NHS England. Sustainability and transformation plan footprints. 2016. Onlineinformation available at https://www.england.nhs.uk/wp-content/uploads/2016/02/stp-footprints-march-2016.pdf (accessed March 2017).
53. Porritt J, Jones K, Marshman Z. Service evaluation of a nurse-led dental anxietymanagement service for adult patients. Br Dent J 2016; 220: 515-520.
SAAD Essays of MeritEssays submitted for the SAAD Essay Prizes that do not win the prize but that theSAAD Essay Judging Panel note as worthy of merit will be published on the SAAD
website in a new section…’SAAD Essays of Merit’ – always worth a read!www.saad.org.uk/prizes-and-grants/essays

51SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017
SAAD celebrated its 60th anniversary, or Diamond Jubilee in 2017and to mark the occasion, this year’s symposium was the bestattended yet! Francis Collier, SAAD’s current President made hisentrance in a truly celebratory fashion by being played in by aScottish piper, and then gave a wonderful welcome address to alldelegates.
The first presentation of the day was a joint address by currentSAAD trustee (and former President) Chris Holden and HonoraryLife member of SAAD, Ian Brett. They delivered a very detailedaccount of how SAAD was instrumental throughout the last 60years in promoting and improving anaesthesia and later sedationin dentistry in the U.K. Their presentation was also given a veryhuman face by the addition of a collage of pictures over the yearsof the people that made and shaped the society, some of whomare sadly no longer with us.
The next speaker was Prof. Vince Bissell who chaired thecommittee from the Scottish Dental Clinical EffectivenessProgramme (SDCEP) reviewing the current guidelines on sedationin the U.K. He explained how the SDCEP functions and how theycome to formulate guidance for any specific area in dentistry. Ascan be expected the guidelines are comprehensive but broadlyconsistent with those published by the Intercollegiate AdvisoryCommittee for Sedation in Dentistry (IACSD) in 2015. He welcomedany feedback on the new guidance via the SDCEP website.
Next followed a very entertaining and informative presentation byBrid Hendron, a qualified dentist and communication coach. Herexpertise lies in working with and treating anxious and dentalphobic patients through understanding the psychologicalprocesses that underpin these patients’ behaviour and thoughtprocesses. By listening to her explain these processes step by step,she helped attendees better understand some of their nervouspatients, as well as how to deal with them more effectively.
Following on from this topic we heard of a very practical approachto treating dental phobic patients through the use of CognitiveBehaviour Therapy aided by the use of Virtual Reality. This was ajoint presentation by Jennifer Hare, a registered HealthPsychologist and her colleague at Guy’s and St Thomas’ NHS Trust,Bryan Kerr, a Consultant in Special Care Dentistry. They explainedhow they were making use of Virtual Reality scenarios in a dentalsetting to improve the outcomes for nervous patients receivingCognitive Behaviour Therapy. They also kindly offered todemonstrate the Virtual Reality during the lunch break to thosewho were interested.
This rounded up the morning session, but before breaking forlunch, as well as the SAAD Annual General Meeting, the followingPrizes were awarded by SAAD’s President Francis Collier:
Dental Care Professional Essay Prize: Kimberley Illing
Dental Student Essay Prize: Yui Yin Ko
Drummond Jackson Essay Prize: Janine Doughty and Amar Kaul
The President’s Award for the best poster presentation wasawarded to Ruixiang Yee from Singapore for “Intramuscularketamine sedation in managing paediatric oro-dental trauma”.
Francis also presented a gift from SAAD to Will Botha who wasstepping down as a SAAD Trustee.
After a lovely lunch, the afternoon session kicked off with a jointpresentation of some interesting case studies by Dan Bateman, WillBotha and Nicole Sturzenbaum. These three speakers each gave anaccount of cases they have dealt with, ranging from Daniel’s lookback over the last ten years and how he has changed and evolvedhis own operator-sedationist practices,; to Will’s case of a five yearold boy who developed severe post-sedation agitation and how toidentify risk factors and manage this phenomenon; finally toNicole’s chronical of a deeply traumatised patient with complexdental needs over many years and chosing the best way of treatingher using different forms of sedation and behavioural management.
The next speaker was Dr. Michael Zybutz who gave a very personalaccount of a “surgeon’s” or operator’s perspective of conscioussedation for dental and oral surgical procedures. Michael went onto share some practical tips he has gained through his extensiveexperience working with many different sedationists over manyyears in practice.
The last speaker of the day was Mick Allen who gave a veryinteresting talk about what the future might hold for sedation anddentistry, judging by how much it has changed over the last fewdecades. He suggested that changes might come in many differentforms ranging from new drugs to different ways of working andmixing clinical skills, to technological advances such as making useof Nanobots to treat disease! However, even though these changesmight one day become reality, as human beings, we will alwaysneed a human touch!
At the end of a thoroughly enjoyable and interesting day, FrancisCollier thanked everyone for attending our Diamond JubileeSymposium and invited everyone back for next year’s symposiumon 22nd September 2018 to be held again at the Royal Society ofMedicine in London.
Will Botha, September 2017
SAAD Diamond Jubilee Symposium 2017A Strong Foundation for a Bright FutureSaturday 23 September 2017
The Royal Society of Medicine, London, UK

52 SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017
looking. We have worked with our medical colleagues, theeducational authorities, the medical and dental indemnityorganisations and the medical and dental regulators withincreasing knowledge and acceptance all furthering ourmembers needs.
Knowing our past, leads to an understanding of the role SAADhas taken in developing standards of patient care whilst beingopen to change and promoting education beyond the basictraining available in the first decades. We have taken leadershipinternationally with considerable impact. It is the talent of ourmembership that has been SAAD’s success so far. A diversegroup of individuals whose stories are sometimes strange andnot infrequently viewed as quizzical but who have co-operatedtogether in the pursuit of abolishing pain to conquer fear.
This presentation describes our past and illustrates that SAAD’ssuccess has been born of challenging the status quo, led byindividual members and the will of the Board. SAAD has muchto celebrate and we look forward to the coming decades ofclinical changes steered by a proactive membership whoseindividuality and drive must reflect the talents of those whohave shaped our past.
Not only has SAAD been a national leader in education in painand anxiety control but the development of the Societychanged the face of UK dentistry. From the embryonic stages ofa study club, through design of the first dental chairs for supinedentistry and team working, SAAD has been instrumental inthe modernisation of dentistry. It has not been an easy pathwith periods of professional clashes with anaestheticcolleagues; high court litigation; and a maturing into a leadingeducational society.
In the 21st Century, SAAD has flourished co-operating with thedental faculties and medical Royal Colleges to agree trainingpathways for sedation. SAAD has provided representation orindividuals with expertise on every major guidance documentin the training and provision of dental pain and anxiety controlin the last generation.
The society has developed with increasing confidence,capability and co-operation providing guidance together withprofessional practical training that has the respect of dentistsboth in the UK and worldwide.
Our past can teach us lessons about how to thrive in anincreasingly evidence-focused provision of dental services. Ourfuture is dependent on challenging the status quo, beinginnovative in patient care, and pushing for change in a medicaland dental world where doing nothing for change is the easyoption but not the option that delivers improvement for ourpatients.
SAAD: A History of the last sixty years
Christopher Holden & Ian [email protected]
Ian is an Honorary Life member of SAAD, now retired frompractice.
Christopher is a GDP with a background postgraduate servicetraining post in general anaesthesia and oral surgery. Hispractice is devoted to care of the anxious and frightenedpatient. As a continuing elected member of SAAD Council andBoard (including a term as president) since 1984 he has seenthe development and achievements of modern SAAD. He is thelongest ever serving Board member of SAAD. UK andworldwide postgraduate teaching, and experience as an expertat the GDC, GMC, tribunals and courts in a number ofjurisdictions has enabled Christopher to bring the needs andchallenges of sedation practice to help SAAD guide ourmembers as contemporaneous standards develop. As amember of the Intercollegiate Advisory Committee forSedation in Dentistry (IACSD) Christopher is actively involved infurthering future standard setting and training in dentalsedation. He is a past president of IFDAS (InternationalFederation of Dental Anesthesiology Societies) and he iscurrently the elected European Representative on theexecutive.
SAAD has evolved over the last sixty years from a small studygroup to a mature, sophisticated specialist society. Ananecdotal look at a picture album of our development may listour achievements and time line but would miss the trueessence of SAAD. Our membership is, and always has been, aneclectic mix of dental and medical practitioners, theeducationally gifted, the politically powerful and curiouslyinteresting individuals.
Driven by a shared desire to improve the patient journey, SAADhas filled a niche both educationally and politically. Knowingthat change for the better requires leadership entwined withdemocracy, discussions in Council and the Board haveoccasionally been robust but always respectful and forward
SAAD Annual Symposium Abstracts

53SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017MILESTONES IN THE HISTORY OF SAAD:
1955 Study Club founded by Stanley Drummond Jackson(D-J)
1957 Society founded. Trust deed drawn up by LordChancellor
1957 First Course, Meetings and News sheet
1957 Intermittent Brietal (Methohexitone) techniquetaught
1957 Interest in mortality and morbidity began
1960 Jorgensen Loma Linda technique promulgated
1961-1965 Development of the first supine electrically drivendental chair (Syncromat)
1966 First Jumbo Course. Mass demonstration of clinicalsedation.
1967 10% of all UK dentists had attended a SAAD course
1968 Intravenous Valium taught
1969 Libel Case: High Court
1970 Expansion of ultralight techniques
1975 Death of D-J. Re-organisation of the society
1979 SAAD 79 -2nd International Congress on ModernPain Control London
1980 Inhalational sedation as RA expanded teaching
1980’s Proliferation of benzodiazepine and opiodtechniques
1981 Inter Faculty Working Party on Training in DentalAnaesthesia
1984 Evaluation Scheme for GA /sedation starts
1984 Start of Update and Lifesaver Courses
1986 First guidance document: Monitoring
1987 National Course in Conscious Sedation for Dentistry
1990 General Anaesthesia, Sedation and Resuscitation inDentistry (Poswillo)
1993 1st Annual Symposium of the modern era
1996 Lifesaver II presented in Australia
2000 Standards in Conscious Sedation for Dentistry-SAAD
2003 SAAD hosts IFDAS 2003 Edinburgh
2003 A Conscious Decision
2003 Conscious Sedation in The Provision of Dental Care
2006 Conscious Sedation in Dentistry: Dental ClinicalGuidance
2007 Standards for Conscious Sedation in Dentistry:Alternative Techniques
2009 Evaluation Scheme for Sedation implementsnational standards
2013 Framework for Commissioning Sedation Guidance
2013 Academy of Medical Royal Colleges: Standards andGuidance
2015 Standards for Sedation in the Provision of DentalCare (IACSD)
2016 SAAD Assessed Sedationist and SAAD AssessedSedation Nurse Schemes
2017 Conscious Sedation in Dentistry (SDCEP)
SDCEP Conscious Sedation in Dentistry:Updating the Guidance
V Bissell PhD MRDRCS (Edin) FDSRCS (Edin) BChD (Leeds) Dean, University of Liverpool School of DentistryPembroke Place, Liverpool, L3 5PS, [email protected]
Vince Bissell graduated from the University of Leeds in 1985. Hecompleted his specialist training in Restorative Dentistry inEdinburgh and, following a brief stint in the Middle East, he wasappointed Senior Lecturer and Honorary Consultant inRestorative Dentistry at the University of Glasgow. In 2011 hewas appointed to a Chair in Restorative Dentistry and DentalEducation at Glasgow. He is currently Chair of the GeneralDental Council’s Overseas Registration Examination AdvisoryGroup and recently chaired the SDCEP Guidance DevelopmentGroup revising the Conscious Sedation guidance.
The role of the Scottish Dental Clinical EffectivenessProgramme (SDCEP) is to produce clinical guidance on prioritytopics to promote high quality clinical care. SDCEP firstpublished guidance on conscious sedation in 2006 and a fullreview and revision of the guidance was due in 2016/17. In2015 the Intercollegiate Advisory Committee for Sedation inDentistry (IACSD) published “Standards for conscious sedationin the provision of dental care”. This document, whilst clearlyfocussed on patient safety and high-quality sedation practice,raised significant concerns for some sectors of the profession. Itwas considered that there was some confusion surrounding anumber of the recommendations. Consequently, in 2016 theChief Dental Officers of the four UK nations asked SDCEP tobring forward its review of conscious sedation guidance and, indoing so, to address the concerns raised by the IACSD report.
SDCEP uses a robust methodology, now accredited by NICE, toproduce guidance. The process begins with establishing thescope for the guidance, through structured interviews withpractitioners and patients. Using feedback from theseinterviews, the scope is defined through the development of anumber of clinical questions that the Guidance DevelopmentGroup (GDG) will consider. The SDCEP team then gatherevidence to inform the discussion by conducting acomprehensive and systematic search of online databases. The

54 SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017GDG was made up of members drawn from a variety of dentalprofessional roles, and also included patients. The GDGconsidered the evidence in relation to each clinical question,along with expert opinion, the balance of risks and benefits,patient and practitioner perspectives etc., prior to makingrecommendations and producing a draft document. The draftguidance was then subject to a four-week consultation. Therewere 65 consultation responses, some from individuals, andsome from organisations. All responses were considered andthe guidance amended accordingly.
The updated guidance was published in 2017 and containsrecommendations that are broadly consistent with those in theIACSD report. It is presented as key recommendations followedby further explanation and advice; a number of tools to aidimplementation are also included. The report attempts toclarify requirements in relation to a number of issues, forexample, the timing of assessment for sedation and its relationto consent, the need for fasting, and the inclusion of specialistexpertise to insure effective treatment planning. There are alsoclear recommendations on training and an endorsement of thetraining curricula specified by IACSD.
SDCEP welcomes feedback on the new guidance, which can beprovided via its website, http://www.sdcep.org.uk/published-guidance/
“Be not afraid...”; Understandingnervous patients.
Brid Hendron BA BDent Sc Dip Consc Sed Dip CHyp NLP TrainerSFFMLM [email protected]
Brid Hendron is a qualified dentist and communication coach.Her clinical interests have always been shaped by an interest inworking with nervous patients to eliminate dental relatedanxiety and reintegrate them into mainstream care. Brid is aqualified NLP trainer and is qualified in hypnosis. She alsoprovides customised training for healthcare professionals andtheir teams to optimise performance and eliminate stress. Shepresents extensively on these subjects at seminars across the
UK. Brid also enjoys roles as Postgraduate Dental Dean and asRegional lead for Community & Hospital dental services andDental Public Health in Northern Ireland.
Dental professionals frequently encounter patients with dentalanxiety in their day to day delivery of care. The anxietyexperienced can vary greatly both in magnitude and in itsability to impact on access to care and subsequent oral healthchoices. Clinicians understandably find it challenging tounderstand how a patient can retain a negative perceptiondespite the high standard of compassionate care they makesure they provide. This is one of the great challenges ofworking with nervous patients.
The effect of perception and the subjective experience ofreality can be outlined using the Neuro LinguisticProgramming (NLP) communication model. This presents aworking explanation of what we observe in clinical practice. Itcan be used to highlight that how we think affects how we feelwhich in turn impacts on our behaviour including ourinteractions and communication with others. Thereforenegative thoughts (such as those predominant in a nervouspatient’s mind during treatment) are not only visible in theoutward physical presentation but are frequently revealedthrough compromised behaviour and poor communicationboth in speaking and listening. This explains why nervouspatients tend to “forget” or more accurately fail to pick up andretain information provided. It also accounts for theobservation that nervous patients can find it difficult toarticulate their thoughts and deliver a comprehensive history.The model also explains how a previous negative experiencecan completely short circuit a patient’s ability to engage withthe present and this can result in negative behaviour even in acurrently positive and supportive environment. This helps usunderstand why some nervous patients can seem difficult andconfrontational at the outset of care, and yet as their anxietydissipates they become much more amenable and flexible. Anunderstanding of the mindset of a nervous patient using thissimple model can greatly empower us as clinicians to remainpatient and supportive . Simple tools such as repeatingimportant information voluntarily, offering choices andretaining an agreeable disposition can go a long way toimproving the dental care experience for nervous patients.
Cognitive Behaviour Therapy (CBT) andVirtual Reality for Dental Phobia: ThePast, The Present and The Future
Jennifer Hare DHealthPsy, CPsychol AFBPS , Health Psychologist Bryan Kerr BDS, MSc, MSpec Care Dent, Consultant in Special CareDentistryDental Health Psychology Service and Sedation & Special CareDentistry,Guy’s and St Thomas’ NHS Foundation Trust, London, SE1 9RT, [email protected] [email protected]

55SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017
Jen is a registered Health Psychologist based within the DentalHealth Psychology Service at Guy’s and St Thomas’ NHS Trust, inthe department of Sedation & Special Care Dentistry. Jen’sprimary role is to lead and develop the NHS-based service;providing psychological interventions (including CognitiveBehaviour Therapy) to patients with dental anxiety. She hasworked across a range of physical health psychology serviceswithin the NHS and has held roles in both community andhospital-based dental services. Jen became a member of theSAAD teaching faculty in June 2014, providing a psychologicalperspective in the National Course in Conscious Sedation forDentistry and now maintains a role on the Editorial Board forSAAD Digest. Jen also provides teaching to postgraduatedentists and dental professionals in her role with KCL.
Bryan was inspired by his undergraduate teaching in Sedationat Glasgow Dental Hospital and won the SAAD student essayprize. He then went on to pursue a career focused on thedelivery and teaching of conscious sedation techniques. Hecompleted an MSc in Sedation and Special Care Dentistry atKing's College London (KCL) and is now a Consultant at Guy'sHospital, London. He provides training in conscious sedation toundergraduate and postgraduate dentists at KCL. Bryan is thecurrent Honorary Secretary for DSTG and is a member of theSAAD teaching faculty. In view of both their interests, Jen andBryan have teamed-up to explore the utility of Virtual Reality(VR) within the treatment of dental phobia using CognitiveBehavioural Therapy (CBT). Their talk at the Symposium aimedto support the day’s programme (“A strong foundation for abright future”), by providing an outline of CBT’s past, presentand future in the management of dental phobia.
The presentation began by providing an overview of thecurrent role and use of CBT in managing dental phobia,followed by a brief exploration of where we are now inimplementing CBT – highlighting the challenges faced –leading to the role of VR in providing a possible solution tothese challenges. They presented the very recent findings fromKumar Gujjar1 and his team in Malaysia, which have shown howVRET provides evidence for the application of VR in thetreatment of dental phobia (for further details, please refer tothe journal scan on page 33 of this issue). The presentationended with a summary of their own research proposal,designed to explore the use and efficacy of VR exposuretherapy (or VRET) within the treatment of dental phobia.
This will be the first research project conducted by the Guy’sbased team into the role and utility of VRET for dental phobia,for which a modest pump-priming research grant was providedby SAAD to support the study. A second research proposalfollowing the feasibility study (further outlined below) willemploy a blinded and randomised control trial (RCT),comparing traditionally delivered CBT (with standard exposureresources, i.e. photos, 2D videos) with VR-enhanced CBT (withincorporated VRET), to identify the efficacy of VR to enhanceCBT, for the treatment of specific dental phobia.
Their presentation concluded before lunch, during which timeBryan and Jen provided an opportunity for the Symposiumattendees to trial the VR equipment and videos – immersingthemselves into the virtual world of dental treatment.Interestingly nearly all attendees chose to view the localanaesthetic video, and provided some helpful feedback andcomments.
The research abstract of their proposed study is outlinedbelow:
A feasibility study to explore the use of immersive 360-degreevideo in graded exposure within a Cognitive Behaviour Therapy(CBT) approach for dental phobia
Dental phobia is estimated to affect 11% of the UK population.The recommended treatment for specific dental phobia isCognitive Behaviour Therapy (CBT), advocated by the NationalInstitute for Health & Clinical Excellence2. Exposure-basedtherapy in CBT can utilise many approaches and resources,including imaginal exposure (i.e. imagining theobject/situation), as well as photographs, sounds, videos andthe objects/situations in real life. Recent innovations intechnology have witnessed the provision of exposure therapyutilising a virtual environment for anxiety and specific phobias;known as ‘virtual reality exposure therapy’ (VRET), individualscan become fully immersed within simulated environments,created by 360-degree videos, viewed through speciallydesigned head mounted display devices (HMD). The lastdecade has seen encouraging research findings in the use ofVRET for a number of phobias and anxieties, however, there hasbeen no research into the use of virtual environment exposurefor dental phobia, until a very recent study protocol to trial itsuse among dental phobics in Malaysia was published1. Thispaper was unknown to the researchers as they were designingtheir own video-software to create a virtual exposureprogramme for UK dental patients, and the results of thisrandomised control trial (RCT) study have yet to be published.While preliminary findings are encouraging, this research wasconducted using computer-simulated virtual dentalenvironments, as opposed to in-real-life videos using 360-degree video software. Therefore, the primary aim of thecurrent proposal is to pilot a feasibility study among dentalpatients in the UK. Employing a questionnaire design,individuals successfully treated with traditional CBT will beasked to view 360-degree videos created of the dental settingand provide feedback, to ascertain: acceptability, immersion,

56 SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017ease of use, level of nausea and whether the use of VRET fordental phobia would be considered of benefit withintraditional CBT treatment.
References1. NICE (2011). Generalised anxiety disorder and panic
disorder in adults: management. Clinical guidelines CG113.National Institute for Health & Clinical Excellence, January2011. Available from:https://www.nice.org.uk/guidance/cg113
2. Gujjar K R, Wijk A V, Sharma R & de Jongh A D (2017). Virtualreality exposure therapy for the treatment of dental phobia:a controlled feasibility study. Behavioural and CognitivePsychotherapy, in press.
Sedation Case Studies
The Operator-Sedationist
Daniel Bateman BDS (Lon), DPDS (Bris), D Imp Dent RCSEd, DwSiGallions Reach Dental Clinic, Bentham Road, London SE28 [email protected].
Daniel qualified from The London Hospital Medical College in1997. Since 2001 he has worked in a large referral basedpractice where he has treated approximately 25,000 patientsunder IV conscious sedation. The majority of these cases havebeen in conjunction with a sedationist, however, in the last 5years he has been an operator/sedationist. Daniel was part of atrio of speakers who each discussed cases.
Daniel’s presentation was a light-hearted look back at threecases from the past 15 years. Just as technology has changed,we as dentists have changed in our techniques. The first twocases highlighted how his technique has evolved fromincreased dosages of midazolam to lower levels with morepatient management and distraction techniques. Both caseshad the same end result successfully providing treatment andinvolving sedation, but with significantly reduced dosages.
The third case was a more recent case involving sedation andpoor patient co-operation, moving towards a successful
conclusion of a complicated and stressful case which wasultimately completed without sedation, just adequate localanaesthesia.
Advanced SedationA case study demonstrating Post-sedation Agitation in a child.
Will Botha MBChB, PDD(Sedation)Sedation Solutions LLP [email protected]
Will Botha is a medical practitioner and has been working as afull time sedationist since 2005, treating both adult andpaediatric patients in private dental practices as well assedation for other medical and surgical procedures. Hecompleted a post-graduate diploma in sedation and paincontrol at the University of the Western Cape under Prof JamesRoelofse.
With a special interest in paediatric sedation, Dr Botha joinedthe sedation team at the Toothbeary Dental Practice inRichmond at the start of 2011, treating children from age 2yrsand older, using advanced, multidrug sedation techniques forpatients requiring complex treatment or with complex needs.
This case study showed the development of post-sedationagitation in a 3 year-old boy undergoing sedation for dentaltreatment. The patient presented on the day of treatment withan active upper airways infection (URTI), but at the same timesuffering with significant pain from dental decay in two areas.
It was decided to proceed with intra-venous sedation in orderto treat the problem areas only, due to the current URTI, andthen to arrange a follow-up visit to complete the othertreatment still required.
The patient was sedated with a combination of Midazolam,Ketamine and Propofol over 40min and the proposedtreatment was completed successfully. During his treatment hewas fairly active and conditions were challenging.
During recovery, the patient developed post-sedation agitationwhich seem to last longer than usual. Two weeks later the

57SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017patient’s mother reported that he was very unsettled afterleaving the clinic following his sedation session and that hewas also suffering with nightmares at night, which she felt wasrelated to his sedation, even though he had no memory of thetreatment itself.
The parents were counseled regarding the likelihood of himdeveloping post-sedation agitation if he had sedation again,but they decided the need for his dental treatment outweighedthe risk.
During the subsequent treatment under sedation, conditionswere much better and the patient recovered without anyproblem.
A discussion followed identifying risk factors for developmentof post-sedation agitation:1. Younger age2. Pre-operative anxiety3. History of behavioural problems 4. URTI5. Post-operative pain6. Deep sedation7. Physical restraint during treatment8. Certain drugs used in anaesthesia
Recommendations in approaching this problem weresuggested including identifying potential patients prone tothis, as well as counselling these patients and parents about theproblem. Other measures include ensuring adequate pain reliefto patients post-operatively and avoiding over-sedation.
Regional Anaesthesia with Nitrous Oxide
Different sedation techniques and their limitations: Acase study of a needle phobic patient over a period of8 years
Dr med dent Nicole Sturzenbaum, Clinical director Toothbeary358A Richmond Road, East Twickenham, TW1 [email protected]
Nicole holds a Dentistry degree (Wuerzburg, Germany), aPostgraduate Certificate in Paediatric Dentistry and adoctorate (Dr med dent) in Paediatric Dentistry (University ofJena, Germany). Nicole worked in paediatric dental practicesfor 7 years before relocating to London to establish, in 2008,Toothbeary an innovative award-winning children’s onlydental practice. Nicole is on the Reader Panel of the BDJ Team,has published in several national and international journalsand regularly features as an expert regarding children’s dentalhealth matters in television, radio and newspapers.
Nicole presented a case study of a severely traumatised andneedle phobic girl named Victoria, who she treated over an 8year period with different sedation and behaviourmanagement techniques. Victoria was traumatised by anegative experience in hospital at the age of 5 and over thenext 10 years she was unable to cope with dental treatment ather local dentist despite an urgent need for fillings on her 6year molars. Victoria was 16 when she first visited Toothbeary.Following her initial consultation and an OPG it becameapparent that additional treatment was needed due to adisplaced UR3. Different treatment approaches and optionswere discussed and agreed, namely to start with IV sedationfor the filling therapy and then to prepare Victoria for herorthodontic treatment and surgical exposure of UR3. However,Victoria couldn’t cope with IV sedation, even with a pre-treatment with Midazolam. It was therefore decided thatbehaviour management therapy was required to help Victoriaovercome her needle phobia before any further treatmentattempts could be made. Victoria was referred to Tim Newton’steam at Guy’s and over a 6 month time-frame she learned howto apply breathing and relaxation techniques to deal withchallenging treatment situations. Following this, Nicole wasable to treat Victoria with Nitrous Oxide for fillings, she alsoaccepted treatment with IV Sedation for the surgical exposureof her UR3 and received treatment with incognito to align theUR3. Over the following eight years Nicole applied diversesedation and behaviour management techniques to build upVictoria’s confidence and overcome her fear, which ultimatelyled her to have treatment with local anaesthesia alone.However, when subsequently transferred to a generalpractitioner, Victoria initially was only able to accept treatmentwith Nitrous Oxide when Nicole applied the local anaesthesia,and it took one year before she tolerated treatment with localanaesthesia alone.
Nicole discussed the approach of high frequencyappointments and reflected on the challenges of high-enddentistry within this patient group, but concluded that thelong-term benefit, in particular the improved self-esteem andenhanced quality of life for the patient, more thancompensated for the overall effort.

58 SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017One Periodontist’s View on ConsciousSedation
Micahel Zybutz BDS Rand; MS UWashington77 Harley St London W1G [email protected]
Michael Zybutz is a specialist Periodontist and Diplomate ofthe American Board of Periodontology. Dr. Zybutz obtained hisMasters Degree at the University of Washington and his BDS atthe University of the Witwatersrand. He is a fully accreditedmember of the American Academy of Cosmetic Dentistry, apast president of the Alpha Omega Dental Fraternity in the UKand a member of the American Academy of Periodontologyand the Academy of Osseointegration. He is currently thePresident of The American Dental Society of London. Hisinterest is in immediate dental implant therapy. His teamutilise sedation routinely for procedures such as the ‘All onFour’ technique and zygomatic implant placement. Havingworked with many different sedationists he is in an excellentposition to evaluate the effectiveness of various approachesand techniques.
As with any treatment, sedation has a number of advantagesand disadvantages. Minimising the barriers to treatment whilemaximising the advantages make conscious sedation a worth-while procedure for the dental surgeon. Observed barriers toTreatment and observed ways to minimise these follow.
Additional Coordination Issues and Increased Set-Up Time
The sedationist should arrive in good time with sufficientmargin to fully set up equipment and discuss the case(s) priorto the scheduled surgery start time. Sedationist and surgeonshould discuss the case(s) prior to the start.
Adverse Intra-operative Experience (Induction;Maintenance; Recovery/post op)
Effective local anaesthesia is vital during conscious sedation.The sedation should facilitate local anaesthesia by providingpain control during the initial local anaesthesia injections.Utilisation of low dose Ketamine and/or a low dose of Opiateis extremely helpful.
During maintenance, effective intra-operative experienceappears to be consistently smoothest in patients treated withMidazolam as well as a Propofol utilising a Propofol pump andlow dose Ketamine infusion. Very often a lightly sedatedpatient utilising these drugs is more co-operative than aheavily sedated patient.
Post-op nausea should be avoided at all costs. For this reasonavoidance of, or at least utilisation of low dose Opiates issomething to consider.
Analgesia is greatly facilitated by use of IV Paracetamol(Perfalgin) administered in the last 30 minutes of theprocedure.
‘Tomorrow and tomorrow andtomorrow…’ A Personal view of thefuture of Conscious Sedation.
Mick Allen BDS (Lond) MScD (Cardiff ) MFDS RCPS (Glasg).Aneurin Bevan University Health Board Community DentalServices, 26 Clytha Park Road, NEWPORT NP20 [email protected]
Mick’s interest in Conscious Sedation started as a Year 4student at UCH. Since then he has developed services inConscious Sedation in South Wales, establishing the only NHSGDS Conscious Sedation referral practice in Wales in 2007. Hehas taught Sedation and Special Care Dentistry to 20 year’s ofUndergraduate and Postgraduate students. With a careerchange to become a Consultant in Special Care Dentistry forAneurin Bevan University Health Board CDS he worked withhis practice team to establish the U.K.’s first NHS GDSEmployee-Owned Enterprise with all staff becomingshareholders. In his spare time he enjoys fly-fishing on hisbeloved River Usk, Beekeeping and cycling. He is the livingembodiment of the MAMIL!
The aim of the presentation was to reflect upon howconscious sedation has changed since the mid-1980s up to the

59SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017present day, and to consider short, medium and long termpotential developments.
In the career span of the presenter, conscious sedation hadmoved forward from a completely unregulated situationwhere patient experiences and sedation education were notwhat we would expect today. For example, techniquesemployed included the administration of intermittentmethohexitone from a glass syringe which was sterilised andre-used; having used diazemuls to sedate patients duringliquid helium cryotherapy to treat trigeminal neuralgia theywere then recovered as a group in a room on hospital trolleys,and in some dental schools the ‘see one, do one, teach one’approach to sedation education was the common approach.The development of undergraduate education; training byorganisations such as SAAD and the publication of IACSDStandards have moved things forward considerably sincethose days.
Short term developments in drugs, such as remimazolam, andpro-drugs such as fospropofol were described and thepossibility of their use in the near future considered. Thetechnological advances in intra-oral scanning and thepotential use of 3-D printing will allow for less invasive
techniques for some patients, and could reduce the need forsedation, for instance in those patients with pronounced gagreflexes.
In the medium term, the potential to increase the use of skill-mix was suggested. The use of therapists and hygienists inproviding inhalation sedation is a step forward, butanaesthetic practice in some parts of the world is seeing feweranaesthetists involved in routine cases. The potential is thereto consider training therapists in the use of IV sedation.In the longer term, the development of nano technology andits potential for use in dentistry was explored. Nanobots are indevelopment for drug delivery, and could be used to providemore targeted local analgesia, and delivery of a sedative agentto the CNS. The nanobots could be activated or de-activatedremotely to raise or lower the level of sedation, and whencompleted, be completely de-activated and excreted.Dentifrobots might be used to clean and repair teeth,negating the need for invasive and destructive dentaltreatment.
Above all, humans are social creatures and despite the rise oftechnology we will always need people to ‘hold our hands’even in the high-tech future!
Letters to the Editorial Board
of the SAAD Digest
We welcome letters concerning any subject related to Conscious Sedation, Anxiety Control, General Anaesthesia or Analgesia in dentistry.
Subject to editorial control, these will be published on the SAAD website at
www.saad.org.uk/digest-newsletters/lettersalong with any replies.

60 SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017
This first Poster presentation was awarded the SAAD
President’s Prize for the best Poster Presentation.
Intramuscular ketamine sedation usedin managing paediatric oro-dentaltrauma in an Emergency Department
R Yee BDS, MSc, Grad Cert in Advanced Clinical Dental Practice,MPaedDent RCS (England)
P L Chay BDS, DClinDent
L P Tham MBBS, MMed
Dental Service, KK Women’s and Childrens’ Hospital 100 BukitTimah Road, 229899, Singapore
Corresponding Author: [email protected]
Introduction: Ketamine sedation is useful for management ofpaediatric emergencies. However, there is limited evidencedocumenting its safety specifically in management of oro-dental trauma. This study is the first of its kind in an Asianpopulation.
Methodology: Ethics approval was obtained. The existingdatabase of all paediatric procedural sedations performed atthe KK Womens’ and Childrens’ Hospital EmergencyDepartment from January 2014 to December 2016 wasscreened. Cases where intramuscular ketamine sedation wasadministered for dentists’ treatment of oro-dental traumawere identified. The clinical notes were reviewed to determine:(a) type/number of sedation-related adverse events(b) patient demographics(c) dental diagnoses and type of dental procedures
performed
Results: Over three years, 167 intramuscular ketaminesedations were administered for treatment of oro-dentaltrauma. Patient median age was 3.6 years (range=1.1-12).There were 19 adverse events reported (11.4%) (n=19); themost common being emesis (9.0%, n=15) followed bytransient desaturation (1.8%, n=3) and hypersalivation (0.6%,n=1). One case had two types of adverse events. The mostcommon dental diagnosis was primary tooth luxation injuries(49.1%, n=82). The most common dental treatment wasprimary teeth extractions (70.7%, n=118).
Conclusion: Intramuscular ketamine sedation administeredby trained Emergency Department personnel is safe andeffective in managing paediatric oro-dental trauma.
Patient Related Outcomes andExperience Measures (PROMS/PREMS)relating to Oral Surgical proceduresunder IV sedation: A summary of alocal project and a suggested movetowards a standardised questionnaire.
Alexander Adams BDS (Hons) MJDF RCS(Eng) PgCert(TLHP) FHEA
Sobie Akram BDS BDS (Hons) MFDS RCS(Edin)
Richard Kerr BDS FDS RCS(Eng) PgDip DSed(Ncl)
Aurimas Kudzinskas 3rd year Medical Student
Royal Devon and Exeter Hospital
Corresponding Author: [email protected]
Abstract: Conscious IV sedation (IVS) is a useful adjunct formany patients undergoing oral surgical or dental procedures.The clinical team should strive to improve the quality, safetyand satisfaction of the service provided for patients. Evidenceof this is becoming increasingly important in thecommissioning of NHS services.
We studied the Patient Reported Experience and Outcomes(PREMS/ PROMS) of the Oral Surgery outpatient IVS service atthe Royal Devon and Exeter Hospital (RD&E). Thequestionnaire included criteria from two nationalcommissioning documents. 100 questionnaires were sent bypost with pre-paid return envelopes. All patients underwentdental extraction(s) and were over 18 years of age. 43questionnaires were returned and results analysed.
Patient satisfaction was generally very high, on a Likert scalefrom 5 (excellent) to 1 (very poor), 90% answered excellentwhile 98% answered 4 or higher. 95% of patients woulddefinitely, and 5% would possibly, recommend the service to afriend or family member. 7% of patients needed to seekadvice or assistance post-procedure and 5% requiredadditional surgery. The widespread use of standardisedPROMS/ PREMS criteria would help evaluate and compare IVSservices consistently across providers. SAAD or otherorganisation(s) could consider developing such aquestionnaire.
Poster Presentation Abstracts

61SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017The pre-operative conscious sedationassessment is imperative for the safetreatment of dentally anxious patients,ensuring the most effective treatmentmodality is chosen.
Sumeet Champaneri BDS (Hons) MFDS RCPS (Glasgow)Dental Core Trainee in Restorative Dentistry, Royal LondonHospital (Barts Health NHS) Corresponding Author: [email protected]
Aim: To evaluate parameters of the pre-operative consultationand their effect on treatment outcomes for patients at BartsHealth Trust.
Method: Pre-operative baseline measurements, peri-operativeobservations and post-operative outcomes were assessedretrospectively.
Results: 200 patients; male (36%) and female (64%) with amean BMI of 28.86kg/m2 were included. Mean midazolamdosages were higher in patients with a higher BMI (p=0.053).There was no noted difference in first attempt cannulationsuccess, with varying BMI groups; no association between BMIand Ellis Grade and no significant occurrence in desaturationbelow 90%. Hypertensive readings (>140/90mmHg) in 26.8%and referral to GMP in 1.5% of patients (BP>179/110mmHg).Highly anxious patients (MDAS 19+) were more likely to havetreatment under IVS than IHS (p=0.02) although this had noeffect on Ellis Scores.
Conclusion: Pre-operative assessments are useful in decidingsuitability for sedation and modality. Individual readings such aBMI should be considered with further assessments prior tosedation provision and should not be a deterrent for outpatientIVS when high.
Ehlers Danlos Syndrome andHypermobility Spectrum Disorders –Can we control the pain?
Hana Cho BDS MJDF RCS Eng
Fatimah Alsayer BDS MFDS RCS (Ed) MSc MSCD RCS (Ed)
Special Care Dentistry Department, Eastman Dental Hospital,University College London Hospitals NHS Foundation Trust,London UK
Corresponding Author: [email protected]
Introduction: Ehlers Danlos Syndrome (EDS) is a group ofhereditary connective tissue disorders, characterised by jointhypermobility, skin hyperflexibility and tissue fragility.Hypermobility Spectrum Disorders (HSD) have similarpresenting features as hypermobile type EDS (hEDS). The
efficacy of local anaesthesia (LA) may be reduced in bothconditions. Alternative techniques to enable pain and anxietycontrol for dental treatment may be required for this group ofpatients. The management of patients with EDS or HSD withresistance to LA will be presented.
Case reports: This report will focus on a total of seven patientswith EDS or HSD who had their dental treatment completedeither under conscious sedation or general anaesthesia (GA) atUniversity College London Hospitals. Three patients underwentconscious sedation (intravenous) and the other four had GA. Allof them reported previous resistance to LA.
All patients had other co-morbidities and those undergoing GArequired a multidisciplinary team approach and special arrange-ments. The dental treatments were completed successfully.
Conclusion: Adequate pain and anxiety control can beachieved with conscious sedation or GA in patients with EDS orHSD who present with resistance to LA. A multidisciplinaryteam approach may be required to enable safe delivery oftreatment.
A Retrospective Evaluation of ConsciousSedation Methods used within aCommunity Dental Service
Emma Lawrence BSc (Hons) BDS (Lond) Dental Core Trainee inSpecial Care Dentistry
Chloe Bass Dental Core Trainee in Special Care Dentistry
Zahra Shehabi Consultant in Special Care Dentistry
Royal London Dental Institute, Barts Health NHS Trust
Corresponding Author: [email protected]
Aims: To evaluate the conscious sedation methods used withina community dental setting in patients with learningdisabilities (LD).
Introduction: Patients with LD still face many inequalitieswhen accessing health care. Challenging behaviour, co-morbidities and the ability to give consent can make treatingthese patients challenging. Unfortunately, a high proportion ofthese patients therefore undergo treatment under generalanaesthetic (GA).
Method: Data was collected from day lists and records inpatients with learning disabilities seen by the CommunityDental Service in Hackney between the periods of June 2012 toJuly 2013.
Results: 134 patients with LD required treatment undersedation. 76 patients received intravenous sedation (IVS) withmidazolam, 30 received intranasal (IN) midazolam and IVS, 9received oral sedation (OS) with midazolam and IVS, 6 patients

62 SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017received INS, OS and IVS at the same appointment, 12 patientsreceived inhalation sedation (IHS) and 1 patient received oralmidazolam only. 16 patients had previously undergone dentaltreatment under general anaesthetic.
Conclusion: Historically, patients with LD at Barts Health under-went dental treatment under GA. However, the development ofa sedation service which offers novel techniques hassuccessfully enabled patients to receive comprehensive dentaltreatment and as a result, reduced the need for a GA.
The benefits of sedation for thediagnosis of head and neckabnormalities
Zahra Nimaa Dental Core Trainee
Zahra Shehabi Consultant Special Care Dentistry
Stacey Clough Consultant Special Care Dentistry
Department of Special Care Dentistry, The Royal London DentalHospital, Turner Street, London, E1 1BB
Corresponding Author: [email protected]
Introduction: Intravenous sedation in dentistry is an invaluabletool in the care of patients with special care needs, who areotherwise unable to co-operate for a thorough examination.This poster presents four cases where examination, onlypossible under IVS, highlighted important head and neckfindings that led to patients being referred and managedappropriately for the conditions discovered.
Case Description: Case 1: a 51 year old patient with Down’s Syndrome was foundto have bilateral mandibular fractures.
Case 2: discovery of a healed ramus fracture on a 36 year oldpatient with severe learning disability.
Case 3: medicine related osteonecrosis of the jaw in a 70 yearold lady with severe dementia.
Case 4: 40 year old patient with Sturge-Weber syndrome andsevere learning disability requiring investigation of oralinvolvement prior to tooth extraction.
Discussion: The benefits of IV sedation are such that a quickassessment and diagnosis of incidental findings can be made inpatients who are unable to co-operate with an assessment ofthe head and neck region. These case studies highlight thepotential misdiagnosis of vulnerable patients with head andneck abnormalities had intravenous sedation not beenprovided.
Action research in the development ofundergraduate education in LocalAnaesthesia
Tarik Shembesh, Jesal Patel, Adam Lorincz , Jonathan Sad Diegoand Nadine Khawaja Tarik Shembesh, Oral Surgery Clinical Teacher, King’s CollegeLondon Dental InstituteCorresponding Author: [email protected]
Objectives: E-learning platforms that utilise effectivepedagogy have the capacity to enhance student learning andoutcome. King’s College London Dental Institute (KCLDI) hasdeveloped an innovative training programme to introduceundergraduate dental students to Local Anaesthesia (LA) byblending online and clinical education using a virtual learningenvironment (VLE) platform.
The aim of the study is to demonstrate the use of actionresearch methodology to develop an introduction symposiumon LA and to demonstrate the ability of the VLE as a tool togather and analyse feedback data to aid development.
Methods: 160 2nd year undergraduate dentistry students atKCLDI were instructed to view an online narrated presentationas well as given links to an online repository of multimedialearning resources. Students were then invited to attend smallgroup workshops facilitated by academic and clinical staff onanatomy, anaesthetic techniques, equipment andcomplications and dosing. At the end of the course studentswere instructed to complete an online feedback questionnaire.Quantitative and qualitative data were collected and analysedvia KEATS (King’s E-Learning and Teaching Service) platformwhich is a Moodle operated VLE.
Results: The narrated presentation had 346 views. 77 (48%)feedback forms were submitted. (90%) feel familiar with theequipment and the procedures for LA. (88%) feel skulls andmodels were useful to simulate LA. (88%) feel moreknowledgeable about the subject. (30%) feel confident andready to start practicing local anaesthesia.
Conclusion: VLEs can be used to support clinical courses bybuilding on prior learning, accommodating different learningstyles & allowing students to re-enforce learning as needed.Feedback provided a useful insight into the students’perceptions as well as opportunities for improvements. Actionresearch is a valid methodology for systematically andempirically attempting to develop undergraduate education inLocal anaesthesia.

63SAAD DIGEST | VOL.34 | 2018
SYMPOSIUM 2017An audit on the IV Sedation Pre-Assessment Forms within thePaediatric Department of the EastmanDental Hospital
Andrea Smith, Senior Dental Nurse, Eastman Dental HospitalCorresponding Author: [email protected]
Background and Aim: Standards for Conscious Sedation inthe Provision of Dental Care (2015)1 state that the patientassessments for conscious sedation must be based on a fullhealthcare check and psychological assessment and takeaccount of management needs. The aim of this audit was toinvestigate accuracy in completion of pre-assessment formsagainst expected standards (90%).
Methodology: 49 clinical records of patients who underwentIV sedation from January 2017 to June 2017 were obtained. Pre-assessments are completed by a range of clinicians with finalapproval by the consultant (for trainees) within the PaediatricDepartment at the Eastman Dental Hospital. 29 aspects in thepre-assessment form were evaluated.
Results: 35% of pre-assessment forms were fully completed;22/29 questions (76%) had a percentage of completion abovethe standard.
Conclusions Compliance with the pre-assessment formcompletion was below the expected standards (90%). Poorcompliance was due to different reasons, such as bloodpressure machine unavailability, lack of clinician signature andpresence of outdated forms.
Recommendations ensure equipment availability; correct formsavailability; regular staff training; 2nd cycle after 1 year.
Reference: 1. Standards for Conscious Sedation in the Provision of Dental
Care: Report of the Intercollegiate Advisory Committee forSedation in Dentistry (IACSD) 2015; Royal College ofSurgeons of England.
A pilot study of dental foundationtrainees. Are we meeting curriculumrequirements in dental sedationtraining?
Alison Walshe and Louise Ormondroyd Department of Oral Surgery, Guy’s HospitalCorresponding Author: [email protected]
The 2016 UK Dental Core Training Curriculum includesspeciality specific competencies relating to dental sedation. TheOral Surgery competencies include: understanding anxietymanagement; being able to carry out sedation and being able
to insert an intravenous cannula. Those competencies areadded to under the specialty of Sedation and Special Care withthe addition of an awareness of the current sedation guidelinesand protocols.
It was noted in the Oral Surgery department at Guy’s Hospitalthat dental foundation trainees reported and demonstrateddiffering levels of skill and awareness of the above-mentionedcompetencies at the end of their DF2 year.
Method: A pilot study was conducted using a retrospectivequestionnaire at the start and end of the year. Trainees ratedtheir personal perceived competency in a variety of skills,including those mentioned in the curriculum. Results showed that following their DF2 year, despite anincrease in confidence, none of the trainees rated theirconfidence at 100% for the skills we would like them to havegained as part of training in dental sedation.
A Two-cycle Clinical Audit of Complianceof Conscious Sedation Practice inNorfolk & Norwich University HospitalOMFS unit with New NationalGuidelines
Xin Hui Yeo BDS MFDSDCT, Norfolk and Norwich University Hospital Corresponding Author: [email protected]
Aims and Objectives: To determine whether Norfolk andNorwich University Hospital OMFS unit is meeting standards ofbest practice for conscious sedation in oral surgical procedureswith intravenous Midazolam.
Methods: Patients who had oral surgery procedures underconscious sedation with IV Midazolam in the outpatientdepartment between January and March 2017 were prospectivelyrecruited after a new sedation monitoring form wasimplemented in December 2016 following the first audit. Datawas collected from patient records by independent auditors.
Results: Recommendations from the first cycle audit have ledto improvement in standards in all 3 domains (pre-, peri- andpost-operative care). Out of the 21 identified criteria from thenational guidelines, 12 had met 100% compliance.
Discussion & Conclusion: There is still room for improvementto meet the gold standard, especially in peri-operative care andmonitoring, which calls for further training and review of thesedation monitoring form. It would be good to follow up with are-audit of a bigger sample size.
These results and trainee comments will be used improve andstandardise trainee experience and learning. Thesecompetencies should be assessed and observed throughoutthe year to ensure trainees are progressing as expected.

64 SAAD DIGEST | VOL.34 | 2018
PROFILE
After some work experience at a local MaxFax dept, (and despitefainting whilst watching a fraenetomy), I decided a career indentistry was for me. So, after venturing across the border from myhometown in South Wales, I took up a place at Birmingham DentalSchool, qualifying in 1997.
During my VT year I was fortunate to have a great trainer who wasa real enthusiast for using Inhalation Sedation for nervous patientsand who was keen for me to develop this skill. Full of enthusiasm, I attended my first SAAD course in 1997 and haven’t looked backsince.
Treating nervous and anxious adults and children is somethingthat I have always enjoyed and found extremely rewarding, and Ifelt early on that I’d found my niche in dentistry.
After VT, I continued working in Birmingham, both in practice andin hospital before moving to Cheltenham with my husband in2000. Moving to an area with very few NHS practices I didn’t quitefeel ready to move into the private sector, so started workingwithin the Community Dental Service where I stayed for sevenyears. I particularly enjoyed doing the paediatric and special needsGA sessions and treating anxious patients using Sedation. Duringthis time, I also found an enthusiasm for teaching, and becameinvolved in teaching on the local NEBDN course.
Wanting to further my skills in conscious sedation, I enrolled on aPain and Anxiety management course at Bristol University, andfollowing this decided a new challenge was needed. So in 2007 Iwas very lucky to start working in a fantastic private sedationpractice, where I continue to practise, and where we provideInhalation Sedation and Intravenous Sedation to our own anxiouspatients as well as to referral patients from around the county andregion. As sedation lead in the practice, I am responsible, amongother things, for all our sedation policies and protocols, sedationupdate training and for mentoring staff during their supervisedclinical practice.
In 2013 I completed an MSc in Conscious Sedation at CardiffUniversity, and during my time there I was invited to become aClinical Lecturer and taught on the MSc and Diploma course forseveral years.
I have always enjoyed teaching sedation and am passionate aboutpassing on this valuable and essential skill to others. It was a realprivilege to be asked to join the SAAD teaching Faculty in 2016,which has been great fun to be a member of, and which I amthoroughly enjoying.
In the first part of 2017, I was invited to be part of the steeringgroup for the document, ‘Commissioning Dental Services:Standards for Conscious Sedation in Primary Care’, a potentiallysignificant milestone in the provision of sedation within primarycare.
Towards the end of 2017 I will be embarking on a new challengeas Paediatric Lead back within the CDS, aiming to help furtherdevelop their paediatric as well as adult sedation services, but willalso continue working part-time in the practice.
Since attending my first SAAD course 20 years ago, I have gainedsignificant experience in providing sedation, primarily within aprimary care setting, and as a Trustee, I look forward to being ableto use my experience and enthusiasm to help further and developSAAD’s essential role within primary care.
Outside of work, we are kept busy with two very active children,Jacob (15) and Milly (12) but when I have time, I love cooking andentertaining, trying to keep fit, playing the occasional game ofnetball, drinking prosecco at book club and doing the oddtriathlon (well, one so far!). I also love nothing more than filling thecar with all the surf boards, heading to the coast, and catchingsome waves (although not particularly well as my children willattest!!).
Leah AdamsBDS MSc ConSed New SAAD Trustee

65SAAD DIGEST | VOL.34 | 2018
PROFILE
Manni DeolBDS, MJDF, PGCMedEd, PGDipConSed.
New SAAD Trustee and Assistant Honorary Secretary
From the age of 12 I wanted to be a dentist. I was born and broughtup in West London and was fortunate enough to attend UMDS(Guy’s Hospital) for my BDS (1997). From the start, the area ofDentistry that inspired me the most was the management ofanxious dental patients. A certain sedation demonstrator at Guy’shad told me to “just get on with it……” and the rest was history.
I did my vocational training in Deptford, London, in a practice thatused to provide GAs. My trainer encouraged me to treat anxiouspatients under IV Sedation. When I moved north, to Coventry I againfound myself in a practice that used to provide GAs and had areputation for dealing with anxious patients. I was fortunateenough to continue providing treatment under sedation.
Over the next 10 or so years with the help of my husband we set upNHS and private practices and I developed my sedation practice.Postgraduate learning and development has always beenimportant to me and as such I embarked and completed the MJDFfrom the RCS England. Having attended the SAAD course a fewtimes and being a SAAD member I felt I wanted to expand myknowledge base further in the field. In 2014 I went back to Guy’sand embarked on the Diploma in Sedation. Having achieved thequalification I continued to be part of the team at Guy’s workingone day a week in the Department of Sedation and Special CareDentistry, teaching undergraduates and treating patients. As ageneral dental practitioner this was and still is a unique opportunityto learn more about Special Care and Sedation.
Alongside this I have been fortunate to have been a VocationalTrainer for over 10 years in the West Midlands Deanery. During thistime I achieved the Postgraduate Certificate in Education for HealthProfessionals from University of Birmingham. Being a VT-trainer hasalways been a privilege and in parallel to that I have been a Mentorfor the West Midlands Post-Graduate Deanery Coaching andMentoring scheme. More recently, I have been lecturing on sedationand providing practical training sessions to Diploma students,sedation practitioners and Foundation Dentists.
Being an NHS practitioner as well, I have been an electedcommittee member for Coventry Local Dental Committee since2006, which has been an honour and a rewarding way to representmy colleagues. This has kept me continuously involved with NHSdepartment managers for many the years, most recently interactingwith the NHS Area Team and contributing to the MCN of Sedationand Special Care.
Aside my passion for Dentistry, I am busy bringing up three childrenand fit in hobbies of spin-cycling, gym, cooking, gardening andtravelling. This summer I have just returned from a rural region ofNepal, where I did two weeks of volunteering in a Dental Hospital.This was an amazing experience and one I hope to revisit.

66 SAAD DIGEST | VOL.34 | 2018
PROFILE
I am a GDP and hospital Specialty Dentist who graduated from theUniversity of Birmingham in 2010. In 2012 I worked as a foundationtrainee in the Community setting gaining experience in SpecialCare, Oral Surgery and Paediatric dentistry with a strong emphasison practical conscious sedation training. I completed my SAADcertificate in conscious sedation the following year and have beena member of SAAD ever since. I gained my MJDF membership in2012. I continued to gain experience of practising conscioussedation in various OMFS and restorative training posts across theNorth West. In 2013 I was appointed to the role of of a SpecialityDentist at Manchester Dental Hospital, leading a service for themanagement of anxious patients within the RestorativeDepartment. Working full-time and independently in this posthelped me to gain significant experience and develop my skillsover a relatively short period of time. I have also recently beenawarded an MSc in Fixed and Removable Prosthodontics with theUniversity of Manchester.
I am dedicated to improving pain and anxiety control withinDentistry. Above all I am committed to help expand and develop
conscious sedation services both within the NHS and the privatesector. I currently work in several established private practices inthe North West as a GDP and sedationist. I am also part-time atManchester Dental Hospital working in both the Oral Surgery andRestorative departments treating anxious adults under conscioussedation and supervising other practitioners to achievecompetency in intravenous sedation.
In 2015 I started a service delivering sedation services to privatepractices within the North West with the aim to improve access. Weare steadily expanding and now regularly provide sedationservices to over 15 dental practices in and around the Manchesterarea. I have been invited to lecture for several surgical implantcourses, advocating the use of conscious sedation as an adjunct tocomplex surgical treatment. I was honoured to be invited to speakat the last SAAD symposium in 2016 - 'Sedation is alive and well inGeneral Dental Practice', sharing my journey of setting up my ownsedation service.
Shilpa ShahBDS MJDF RCS (Edin) MSc (Fixed & Remov Pros)
New SAAD Trustee

67SAAD DIGEST | VOL.34 | 2018
PROFILE
I grew up in Hampshire on the south coast. Being the product ofscience teacher parents, a career in something requiring science A-levels beckoned and dentistry soon caught my eye.
Dental School at King’s followed, where I was fortunate to trainunder a wealth of talented pre-clinical as well as clinical teachers.My biochemistry tutor, Professor Nunn was a particular inspirationwho focused my scientific mind on how neurotoxins work. I thenspent a glorious year completing an intercalated BSc with the awe-inspiring dental anatomist Barry Berkovitz, doing electromicroscopyhunting for elusive nerve endings in periodontal ligaments, in abasement in Kensington.
Clinical studies called me back to Denmark Hill where I was taughtby dedicated professionals such as the anaesthetist Jose Ponte andthe restorative dentist Steve Dunne. Junior house officer positionsfollowed, and I was somewhat relieved to discover I really enjoyeddentistry. I honed my IV sedation skills whilst taking out wisdomteeth in Oral Surgery that first year. I recall one of my first sedationpatients asking me afterwards if my nurse and I really had beentopless for the procedure! But it was the department of Paediatricdentistry where I found I was most at home. Under the excellentdiscipleship of Petra Smith, Kate Barnard and Registrar MeeraAhluwalia, my love of inhalation sedation and all things paeds wasborn.
Following VT in Bermondsey, a stint with the masterful RobMcGeogh in Tower Hamlets CDS developed my sedation skillsfurther. I fell on my feet when senior house jobs, a Masters inClinical Dentistry and registrar positions in Paediatric Dentistry atthe Royal London Hospital soon followed. I was so fortunate to be
trained by Professor Wong, whose constant zest for new techniquesand materials kept me ahead of the game, and Janice Fearne whonever ceases to be an inspiration and developed my researchinterests in enamel defects and molar incisor hypomineralisation.
I was appointed a Consultant in Paediatric Dentistry at the RoyalLondon Hospital in 2007 where I have been Clinical Lead since2013. It is a very busy unit receiving over 5000 referrals a year, and Ihead the Children’s Sedation and Comprehensive dental care andsurgical GA services. We are currently training 6 registrars, 2 DCTsand 3 clinical Fellows.
Since 2011 I have been an examiner for the Royal College ofSurgeons’ Membership in Paediatric Dentistry exams and currentlysit on the exam board. I am also an Honorary Senior Lecturer atQueen Mary, University of London, teaching on the Masters inClinical Dentistry postgraduate programme and am the internalexaminer for the Hygiene Therapy School. Since 2015 I have beenthe external examiner for the University of Dundee Therapy School.
Recently, I was somewhat bemused to discover my 4 times great-grandfather Dr PH Van der Weyde was one of the first advocates forthe use of nitrous oxide in dentistry back in1864. He is quotedsaying in the New York Times, ‘’When we look at the hundreds ofcases directly killed by ether or chloroform on the operating chairor table, the comparative value of nitrous oxide must be apparent.’’
I am married with 3 children who keep me busy. In rare moments ofspare time I play percussion and am trying (and failing) to learn toplay the drum kit!
Rosie WhatlingBSc, AKC, BDS, MFDS, MClin Dent, M Paed Dent, FDS (Paed Dent) RCS Eng
New SAAD Editorial Board Member

68 SAAD DIGEST | VOL.34 | 2018
PROFILE
I graduated from the University of Leeds medical school in 1998.Following a thoroughly gruelling yet enjoyable year of pre-registration house officer posts in Leeds and York, I made my waydown to London to begin postgraduate training in anaesthesia. Icompleted specialist registrar anaesthetic training on the NorthCentral Thames – University College London & Royal Free Hospitalsrotation. This included subspecialty training at several prestigiousLondon hospitals including: The Royal Marsden Hospital, The RoyalBrompton Hospital and The Evelina Childrens’ Hospital. Uponcompletion, I was delighted to be appointed to a Consultantanaesthetist post in paediatric and cardiac anaesthesia at Guy’s &St Thomas’ hospitals, where I have been ever since 2007.
My clinical interests have since evolved to include anaesthesia andsedation for dental surgery in both children and adults, with aparticular interest in adults who have special needs. I have thepleasure of working with one of SAAD’s past Presidents (Dr CaroleBoyle) and our weekly special care dental GA list is not infrequentlythe most enjoyable and at times the most challenging part of mywork!
Aside from clinical work, my other main interest is training andeducation. I am Clinical Adviser to undergraduate medicalstudents at King’s College London School of Medicine, as well asCollege Tutor and Training Lead for over 50 postgraduateanaesthesia trainees at Guy’s & St Thomas’ hospitals. I was lucky tohave been taught by some amazing and truly inspiringConsultants during my training and it’s a major passion of mine totry and do the same for future generations.
I am honoured to have been invited to join the Editorial Board ofSAAD. Anaesthesia and Dentistry have a strong historicalassociation and I feel very privileged to represent my specialty onthe Board and continue to maintain the strong links between ourspecialties.
Outside of the world of anaesthesia, there was a time when I had apassion for travel to far and exotic lands. Having become a fatherlast year, I am now very much a family man revelling in the joy andprecious moments of life with my now 8-month-old son.
Dev MahtaniBSc MBChB FCARCSI
New SAAD Editorial Board Member

69SAAD DIGEST | VOL.34 | 2018
TRAININGCognitive Behavioural Therapy (CBT) for dental phobia:services and training options for dental professionalsTim Newton BA PhD CPsychol AFBPS CSci Professor of Psychology as Applied to Dentistry
Jennifer Hare DHealthPsy, CPsychol AFBPS Health Psychologist
King’s College London Dental Institute and Guy’s & St Thomas’ NHS Foundation Trust: Dental Health Psychology Service, Sedation and Special Care Dentistry, Floor 26 Tower Wing, Guy’s Dental Hospital, London, SE1 9RT
Corresponding Author: [email protected]
AbstractThis article will explore the use of psychological approaches(specifically Cognitive Behavioural Therapy, CBT), for themanagement of people with dental phobia. While dental anxiety iscommon, it should be considered as a continuum, becoming aphobia when it meets the criteria outlined by the Diagnostic andStatistical Manual of Mental Disorders (DSM-5).1 Specifically thismeans the phobia has a significant impact on an individual’swellbeing in areas of physiological, psychological or socialfunctioning; with marked avoidance and experience of significantdistress associated with encounters related to the dental setting.Recognised as one of the most common specific phobias,2 dentalphobia is estimated to affect 11% of the UK population.3
Consequently, increasing interest and attention on the applicationof CBT for dental phobia and the use of psychological approachesinformed by the principles of CBT (i.e. Cognitive Behavioural-techniques) for dental anxiety management, has led to an increasein the demand for both services and trained professionals withinthe dental care setting. To this end, it is important to note thedistinction between CBT and CB-techniques; for individuals withmild-to-moderate dental anxiety, a range of psychologicalapproaches may be employed, some of which draw on theprinciples of CBT (i.e. CB-techniques) but do not necessarilyconstitute formalised CBT for the treatment of phobia. This articleaims to briefly outline the role of CBT within dental phobia carepathways, outline existing services which provide CBT approacheswithin the UK and identify the possible training options availableto dental care professionals interested in the approach. Theauthors wish to note that the UK services and training optionsoutlined in this article, were those known to them at the time ofwriting – there may be others we are not aware of.
IntroductionThe use of Cognitive Behavioural Therapy (CBT) for the long-termmanagement of dental phobia has been well documented4 andhas a strong evidence-base for both its efficacy (i.e. how well CBTinterventions treat dental phobia)5,6 and its effectiveness (i.e. howwell these CBT interventions work in “real-world” clinical settings).7,8
In a very recent publication in the Royal College of Surgeons(England) Faculty Dental Journal, the complementary use of CBTwithin a conscious sedation care pathway has been endorsed,9 inwhich conscious sedation is deemed to provide an excellentapproach to deliver dental care to the anxious individual, with CBT
providing the long-term cure of the anxiety itself. Suchrehabilitative benefits of CBT within the sedation care pathwaywere demonstrated in a case report published in the Digest lastyear,10 and further the rationale for services to develop sustainablecare pathways to both care for and cure dental phobia.
What is CBT?For those unfamiliar with the approach, CBT is a psychologicaltalking therapy which combines two traditional theoreticalapproaches of behaviour therapy and cognitive therapy, that helpan individual learn new strategies to solve problems related totheir thoughts and behaviour. CBT is used to treat a broad range ofpsychological problems including depression and anxietydisorders, including dental phobia, with both general and disorder-specific treatment methods.
To draw a distinction from other psychological therapies, the focusof CBT is on the here and now, rather than the original cause orpast experiences and is a brief time-limited approach. The aim oftherapy is to help an individual make sense of their problems bybreaking them down into manageable steps, and to identify theconnections between thoughts, behaviours, emotions and physicalsensations – so to demonstrate the impact of our thinking on howwe feel (both emotionally and physically). However, CBT movesbeyond insight of the problem and seeks to change unhelpfulstrategies with action-based methods, towards specific andconcrete goals; this occurs both in-session and within agreedhomework tasks, where the learning is applied in natural situationsand is a crucial determinant of the success of therapy.11
CBT for specific dental phobia primarily centres on exposure-basedbehavioural intervention alongside cognitive strategies; wherebyan individual is exposed to their feared object/situation. Typicallythis occurs in a graded fashion (i.e. “graded exposure”12), in order toacclimatise to each anxiety-provoking situation and learn that theircatastrophic predictions are unlikely to occur.
CBT requires close collaboration between the individual and thepractitioner, so that the therapeutic relationship fostersindependence for the patient to help themselves and apply theirlearnt strategies in the future management of the problem –therefore offering a form of long-term management or “cure” if you will.

70 SAAD DIGEST | VOL.34 | 2018
TRAININGWhat CBT services for dental phobiaare currently available? In 2008, the Improving Access to Psychological Therapies (IAPT)programme was launched across the UK to provide evidence-based treatments for adults with anxiety and depression, of whichspecific phobias are included.13 Currently over 900,000 peopleaccess their local IAPT services each year, with plans for furtherservice expansion in the next 5-years. Across the country,individuals can be referred by the general practitioner forassessment and treatment; with some localities offering self-referral and referral by health-care professionals (HCP). CBT is theprimary therapy provided and if deemed suitable for treatment,sessions with a CBT therapist or psychologist would typicallyinvolve working in a non-dental setting. Collaboration between thepatient and their local general dental practitioner (GDP) or dentalservice would be beneficial in this instance, to allow the necessarybehavioural aspects of intervention. IAPT services would provide alocal option for CBT intervention where specialised dental phobiaservices do not exist: details of local IAPT services are available onNHS Choices.
The established and specialised dental phobia services providingCBT within the UK typically adopt one of two models; psychologist-led services and dental nurse-led services (usually withpsychologist or CBT Therapist input and supervision). That is, theseservices are embedded within special care dental services, whichtypically offer the full care pathway from conscious sedation toCBT, and additionally enable the graded exposure elements oftherapy to be easily delivered.
Currently there is the Dental Health Psychology Service (developedand delivered by the authors) at Guy’s & St Thomas’ NHSFoundation Trust (GSTT) and King’s College London DentalInstitute (KCLDI) in London, which has been established since 2008.In Sheffield, a team of dental-nurses have been trained andsupervised to provide low-level psychological interventions towork with anxious patients, as part of the nurse-led dental anxietymanagement service (NDAMS) within the Sheffield SalariedPrimary Care Dental service. Both services have published serviceevaluations demonstrating the effectiveness of CBT-basedinterventions within this setting.7,8 However other CBT-basedintervention pathways have been recently established within otherUK special care dental services, in the following localities:Birmingham, Isle of Man, Port Talbot, Wolverhampton, Stoke onTrent, Lancaster and Edinburgh. This demonstrates the growingdemand for access to CBT-based interventions for the long-termmanagement of dental phobia.
What options are there to provideCBT for dental phobia and whattraining is available? Based on our experience, for the management of individuals withdental phobia, CBT could be provided in one of two ways:
1) By employing fully trained CBT Therapists (or equivalent)within dental services, who can apply their skills and approachto the dental situation
2) By devising a highly structured CBT protocol specifically for
dental phobia, and training non-CBT Therapists in how todeliver the therapeutic interventions
Individuals who are employed in the second group would only betrained to use CBT for dental phobia and would not therefore beeligible to be called CBT Therapists. However they would bedelivering an intensive course of management for dental phobiafollowing CBT principles.
With either approach, the provision of CBT or CB-techniques fordental phobia requires new roles or personnel training; along withthe facilities to provide the approach and planned care pathwaysfor the management of psychological comorbidity or complexcases. Given the similarity in service outcomes7,8, such servicescould be either psychologist/CBT-therapist-delivered or dentalnurse-delivered, provided there was access to psychologists/CBT-therapists for supervision and complex case management. Dentalhygienists/therapists and dentists may also be well suited orinterested in training, though the cost of service provision may bea consideration in planning suitable personnel.
To become a fully accredited CBT therapist in the UK requiresundertaking an accredited level 2 course (or a level 1 course withadditional hours of supervised therapy) in order to meet theminimum training standards outlined by the British Association ofBehavioural and Cognitive Psychotherapies (BABCP). Within IAPT,there are specific opportunities to train as psychological wellbeingpractitioners (PWPs) or high intensity therapists – these wouldrequire full-time employment and training within the IAPT trainingprogrammes.
Introductory courses in CBT are available, though there are veryfew specialising in specific phobia alone; those advertised by theBABCP or BPS (British Psychological Society) would be a usefulplace to start but caution should be exercised before seekingtraining from an unrecognised teaching body.
Local training from existing services may also be an option, whereCB-techniques can be applied in the dental setting. Indeed,following the development of a training manual for CBT in dentalphobia14, created by psychologists and dental clinicians at KCLDIand GSTT, online and face-to-face training courses are available:see “Cognitive Behavioural Techniques for the Management ofAdults with Dental Fear” provided by KCL (https://alumni.kcl.ac.uk/dental-e-learning-course). The online learning course runs twiceyearly, providing an introduction to the principles of CBT for thetreatment of dental phobia. As part of the course, participantsreceive a copy of the training manual,14 along with course materialsand interactive forums for learning. Course teaching is provided byboth academic staff and clinicians currently delivering the CBTservice at GSTT.
The authors are also aware that other teaching courses in dentalanxiety management within the UK may also provide sometraining on Cognitive Behavioural principles, that can be appliedfor mild-moderate dental anxiety; including the “Post GraduateCertificate in Clinical Conscious Sedation and AnxietyManagement” provided by the University of Bristol. SAAD itself alsoprovide the “National Course in Conscious Sedation for Dentistry”,which now includes a 40-minute lecture on psychologicalapproaches. However, these courses are designed to supporttraining in sedation rather than a stand-alone CBT-based approach.

71SAAD DIGEST | VOL.34 | 2018
TRAININGConclusionsThere is no question that CBT provides an effective approach torehabilitating patients with dental phobia. However currentavailability of services providing CBT for dental phobia within theUK are limited. There are two broad options for increasing access toCBT for patients: 1) liaison with local psychological services (i.e.IAPT) or 2) development of specialised services within the dentalsetting. The latter has an existing evidence-base of successfulservices currently in operation, and there are two options forstaffing to achieve this. Currently KCL provide training and supportfor the development of CBT services through a variety of trainingresources and courses, with other more generalised courses on theCBT principles for mild-moderate anxiety management.
References1. American Psychiatric Association. (2013). Diagnostic and statistical manual of
mental disorders (5th ed.). Washington, DC. American Psychiatric Publishing.
2. Oosterink, F.M., de Jongh, A., & Hoogstraten, J. (2009). Prevalence of dental fearand phobia relative to other fear and phobia subtypes. Eurpean Joural of OralScience, 117, 135-143.
3. Humphris, G., Crawford, J., Hill, K., Gilbert, A., & Freeman, R. (2013). UK populationnorms for the modified dental anxiety scale: Adult Dental Health Survey 2009results. BMC Oral Health, 13: 29.
4. Öst L, Skaret E. Cognitive Behaviour Therapy for Dental Phobia and Anxiety.London: Wiley. 2013.
5. Kvale G, Berggren U, Milgrom P. Dental fear in adults: a meta-analysis ofbehavioural interventions. Community Dent Oral Epidemiol 2004; 32: 250-264.
6. Wide Boman U, Carlsson V, Westin M, Hakeberg M. Psychological treatment ofdental anxiety among adults: a systematic review. Eur J Oral Sci 2013; 121: 225-234.
7. Kani E, Asimakopoulou K, Daly B, Hare J, Lewis J, Scambler S, Scott S, Newton J T.Characteristics of patients attending for Cognitive Behavioural Therapy at onespecialist unit for dental phobia in the UK and outcomes of treatment. Br Dent J2015; 219: 501-506.
8. Porritt J, Jones K, Marshman Z. Service evaluation of a nurse-led dental anxietymanagement service for adult patients. British dental journal. 2016 May 27;220(10): 515-20.
9. Newton T, Gallagher J, Wong F. The care and cure of dental phobia: the use ofcognitive behavioural therapy to complement conscious sedation. Faculty DentalJ 2017; 8 (4): 160-163.
10. Hare J. Combining sedation and cognitive behavioural therapy (CBT) to overcomedental phobia: a case report. SAAD Digest 2017; 33: 29-33.
11. Kazantzis N, Whittington C, Dattilio F. Metaanalysis of homework effects incognitive and behavioral therapy: a replication and extension. ClinicalPsychology: Science and Practice. 2010 Jun 1;17(2):144-56.
12. Marks I M. Fears, phobias and rituals. New York: Oxford University Press, 1987.
13. NHS England: Adult Improving Access to Psychological Therapies programme.Retrieved from: https://www.england.nhs.uk/mental-health/adults/iapt/ on 20thOctober 2017.
14. Newton T, Asimakopoulou K, Boyle C, Scambler S, Scott S. Cognitive BehaviourTherapy for Adults with Dental Anxiety: A Toolkit. Stephen Hancocks Limited:London. 2011.
** NHS Choices link: https://www.nhs.uk/Service-Search/Psychological%20therapies%20%28IAPT%29/LocationSearch/10008
RA LOAN
Inhalational Sedation and Scavenging System
Available for a six-month loan to SAAD members
who have recently attended a SAAD course
Opportunity to purchase the system
after the loan period
Details of the scheme at
www.saad.org.uk
or email [email protected]

72 SAAD DIGEST | VOL.34 | 2018
TRAININGSAAD Shows the way for ‘New Starters’ in Dental Sedation“Education is not the learning of facts, but the training of the mind to think” Albert Einstein
Since the publication of the IACSD Standards for ConsciousSedation in the Provision of Dental Care (2015) the expectationsaround training courses in dental sedation have increaseddramatically and this is significant for both course providers andpotential delegates. As a profession we have a duty of care toprovide appropriate pain and anxiety control for our patients and itis imperative that those practising conscious sedation are able todeliver this in a safe and predictable way. Sedation practitioners arerequired to have a good understanding of the techniques used andto be able to apply their knowledge for each patient and in allclinical situations thereby ensuring a successful outcome.
The newly formed Sedation Training Accreditation Committee (STAC)is responsible for accrediting all independent courses intending totrain ‘New Starters’ in dental sedation, including sedationists anddental nurses. Courses need to demonstrate they fulfil therequirements described in the IACSD education syllabuses and thatstudents will obtain the necessary knowledge, skills and experienceto prepare them for independent sedation practice. These changeshave necessitated course providers to reflect on their own coursesand develop and improve them to meet the new standard.
As a premier education provider in dental sedation, the Society forthe Advancement of Anaesthesia in Dentistry (SAAD) hasresponded to this challenge and new demands, by developing andgaining accreditation for two new courses; the SAAD AssessedSedationist scheme (SAS) and the SAAD Assessed Sedation Nursescheme (SASN). These two courses are in addition to the existingaccredited course in inhalation sedation for Dental Hygienists andDental Therapists, the SAAD Assessed Sedation Therapists (SAST)scheme. The SAS, SAST and SASN scheme are structured to deliver adetailed two-day programme of didactic training followed bysupervised clinical experience, thereby fulfilling the requirementsdetailed in the IACSD Standards’ Syllabus 1: Basic conscioussedation techniques for children, young people and adults, andSyllabus 5: Dental nurses: Assisting during conscious sedation,respectively.
These courses build upon the success and popularity of the existingSAAD National Course for Dental and Medical Practitioners and theDental Nurse Course, but offer a great opportunity to combinethese with a well-structured and thorough clinical experiencemodule for ‘New Starters’. Course participants identify a suitableclinical supervisor in advance of the course who will be approvedby the SAAD Training Board after providing details of their sedationexperience, qualifications and current practice. This providesdelegates with the flexibility to work with a clinical supervisoreither within their own practice environment or locally, thusfacilitating easier access to the clinical experience. This proximity tothe clinical supervisor promotes not only a positive andconstructive working relationship during the formal process ofsupervision and assessment, but also an increased likelihood ofcontinued mentorship, support and peer review.
SAAD Assessed Sedationist (SAS) scheme‘New Starters’ interested in joining the SAS scheme need to registerat the time of booking onto the National Course. A clinical
supervisor should then be identified by the applicant and approvedby SAAD in advance of attending the course. On the second day ofthe National Course, delegates will undergo a written assessmentusing the Single Best Answer format. The clinical experiencemodule consists of a series of Direct Observation of ProceduralSkills (DOPS) totalling 20 Intravenous sedation (IV) and/or 10Inhalation sedation (IHS) cases. In addition practitioners arerequired to complete a logbook of experience and undertake apractice evaluation checklist using the SAAD Safe Practice Schemedocument. All documentation must be submitted for approval bySAAD within 12 months of the date of the National Course.
SAAD Assessed Sedation Therapist(SAST) schemeDental Hygienists and Therapists registered for the SAST schemesubmit the details of their clinical supervisor for approval by SAADat the time of registration. They then attend the two-day SAADNational Course, for the knowledge and skills training. On thesecond day of the course there is a written (Single Best Answerformat) and a practical assessment. The clinical experience moduleis completed in the same manner as the SAS scheme for 10 IHScases, with the documents being submitted within 12 months ofattending the SAAD National Course.
SAAD Assessed Sedation Nurse(SASN) schemeDental Nurses wishing to join the SASN scheme need to registertheir interest either before attending the Dental Nurse Course orwithin the first four weeks after the course. A suitable clinicalsupervisor needs to be identified and approved by SAAD as withthe SAS scheme. The clinical experience module is completed inexactly the same manner as the SAS scheme with the requisitenumber of DOPS and a clinical experience logbook. Dental Nursesare required to compile a practice profile detailing a description ofthe clinical setting. As with the SAS scheme, course participantshave 12 months to complete the required documentation and oncethis is received and approved, individuals will be invited to attendfor their final assessment including written and practical elements.These assessments are scheduled on the Saturday morning of eachSAAD National Course course held in London.
November 2016 saw the first cohorts enter the SAS and SASN schemes and two further cohorts have begun their journeys in March and June of this year. Thus far a total of eight sedationists and two dental nurses have successfully completed the schemes, thereby fulfilling the requirements to be able to practise independently. The SAAD Training Board is very enthusiastic and positive about the impact of these new schemes and feels confident that the robust, well rounded and thorough training pathway will equip new sedationists and dental nurses with the required knowledge, skills and experience to be able to practise dental sedation safely, effectively and so provide a positive outcome for their patients.
If you have any questions or would like some more information about the SAS or SASN schemes please visit www.saad.org.uk or email Fiona at [email protected]
Paul HowlettSAAD Training Board

73SAAD DIGEST | VOL.34 | 2018
TRAININGSAS SCHEME
REGISTER (BEFORE ATTENDING THE SAADNATIONAL COURSE)The deadline for registering for the SAS scheme is theFriday before the weekend of the SAAD NationalCourse.
eg for the SAAD National course taking place on the16th & 17th June 2018, the SAS scheme registrationdeadline is 8th June 2018
INFORMATION REQUIREDWhen registering you will need to be able to providethe following information…• Date you will attend the SAAD National Course• Intended sedation technique(s)• Age group of patients (adults, children or both)• Name of proposed clinical supervisor(s)• GDC / GMC No. of proposed clinical supervisor(s)• Qualifications of proposed clinical supervisor(s)• Sedation experience of proposed clinical
supervisor(s)• Sedation services offered by proposed clinical
supervisor(s) including approx. no. of sedation casesper month.
• Address of the practice(s) where the clinicalsupervision will take place
• A brief description of sedation facilities
APPROVALThe information about the nominated clinicalsupervisor (s) and the sedation facility where thesupervised clinical practice will take place issubmitted for approval to the SAAD Training Board.
SAAD NATIONAL COURSEAttend the SAAD National Course for the knowledgeand skills training.
WRITTEN ASSESSMENTThis is a Single Best Answer paper on the Sunday ofthe National Course weekend.
ASSESSSMENT RESULTSThe week after the National Course the results of theassessment are emailed along with the link to the SASscheme webpage.
SAS SCHEME WEBPAGEFrom this page is will be possible to download all ofthe documents required to complete the supervisedclinical practice.
DOPS formLogbookPractice Self-Evaluation Checklist
Also available is guidance on setting up the SAADDocument Repository (SDR)
SUPERVISED CLINICAL PRACTICE20 IVS and/or 10 IHS cases should be documentedand signed by the approved clinical supervisor.
ACCESS THE SAAD DOCUMENT REPOSITORY (SDR)This enables SAS scheme documents to be uploaded,via a secure section of the SAAD website, andsubmitted for approval. All documents must besubmitted within twelve months of attending theSAAD National Course.
eg if attending the SAAD National Course on 16th &17th June 2018 all documents must be submitted by17th June 2019.
APPROVAL AND CERTIFICATIONSuccessful practitioners will receive a SAAD certificateconfirming ‘SAAD Assessed Sedationist’ status whichwill enable you to practise independently.
SASN SCHEMEREGISTER (BEFORE OR AFTER THE SAAD NATIONALCOURSE)The deadline for registering for the SASN scheme isfour weeks after the weekend of the SAAD NationalCourse.
eg for the SAAD National course taking place on the16th & 17th June 2018, the SASN scheme registrationdeadline is 14th July 2018.
INFORMATION REQUIREDWhen registering you will need to be able to providethe following information…• Date you attended the SAAD National Course • Intended sedation technique(s)• Age group of patients (adults, children or both)• Name of proposed clinical supervisor(s)• GDC / GMC No. of proposed clinical supervisor(s)• Qualifications of proposed clinical supervisor(s)• Sedation experience of proposed clinical
supervisor(s)• Sedation services offered by proposed clinical
supervisor(s) including approx. no. of sedation casesper month
• Address of the practice(s) where the clinicalsupervision will take place
• A brief description of sedation facilities
APPROVALThe information about the nominated clinicalsupervisor (s) and the sedation facility where thesupervised clinical practice will take place issubmitted for approval to the SAAD Training Board.
SAAD NATIONAL COURSEAttend the SAAD National Course for the knowledgeand skills training
SASN SCHEME WEBPAGEFrom this page is will be possible to download all ofthe documents required to complete the supervisedclinical practice.
DOPS formsPractice profile
Also available is guidance on setting up the SAADDocument Repository (SDR)
SUPERVISED CLINICAL PRACTICE20 IVS and/or 10 IHS cases should be documentedand signed by the approved clinical supervisor.
ACCESS THE SAAD DOCUMENT REPOSITORY (SDR)This enables SASN scheme documents to beuploaded, via a secure section of the SAAD website,and submitted for approval.
SUBMIT DOCUMENTS FOR APROVALAll documents should be submitted to be approvedwithin twelve months of attending the SAAD NationalCourse.eg. If attending the SAAD National Course on 16th &17th June 2018 the final opportunity to submitdocuments is 4th May 2019.
WRITTEN AND PRACTICAL ASSESSMENTAfter the submitted documents have been approved,return to the SAAD National Course venue to sit thesingle best answer paper and the practicalassessment on one of the SAAD weekends withintwelve months of attending the SAAD NationalCourse.eg. If attending the SAAD National Course on 16th &17th June 2018 the final opportunity to attend forassessment is 15th June 2019
ASSESSSMENT RESULTSCandidates will receive their results approximately aweek after the assessment.
APPROVAL AND CERTIFICATIONSuccessful practitioners will receive a SAAD certificateconfirming ‘SAAD Assessed Sedation Nurse’ statuswhich will enable you to assist with the provision ofdental sedation as the second suitable trained person.
SAST SCHEMEREGISTER (BEFORE ATTENDING THE SAADNATIONAL COURSE)The deadline for registering for the SAST scheme is amonth before the course dates.
eg the deadline for the course commencing on 3rd & 4th Novemer 2018 is Friday 5th October 2018
INFORMATION REQUIREDWhen registering you will need to be able to providethe following information…• Age group of patients (adults, children or both)• Name of proposed clinical supervisor(s)• GDC / GMC No. of proposed clinical supervisor(s)• Qualifications of proposed clinical supervisor(s)• Sedation experience of proposed clinical
supervisor(s)• Sedation services offered by proposed clinical
supervisor(s) including approx. no. of sedation casesper month.
• Address of the practice(s) where the clinicalsupervision will take place
• A brief description of sedation facilities
APPROVALThe information about the nominated clinicalsupervisor (s) and the sedation facility where thesupervised clinical practice will take place issubmitted for approval to the SAAD Training Board.
SAAD NATIONAL COURSEAttend the SAAD National Course for the knowledgeand skills training.
WRITTEN ASSESSMENTThis is a Single Best Answer paper on the Sunday ofthe National Course weekend.
ASSESSSMENT RESULTSThe week after the National Course the results of theassessment are emailed along with the link to theSAST scheme webpage.
SAST SCHEME WEBPAGEFrom this page is will be possible to download all ofthe documents required to complete the supervisedclinical practice.
DOPS formLogbookPractice Self-Evaluation Checklist
Also available is guidance on setting up the SAADDocument Repository (SDR)
SUPERVISED CLINICAL PRACTICE10 IHS cases should be documented and signed bythe approved clinical supervisor. For at least five ofthese cases you should have provided both thesedation and the treatment.
ACCESS THE SAAD DOCUMENT REPOSITORY (SDR)This enables SAST scheme documents to beuploaded, via a secure section of the SAAD website,and submitted for approval. All documents must besubmitted within twelve months of attending theSAAD National Course. eg if attending the SAAD National Course on 3rd &4th November 2018 all documents must be submittedby 5th Novmeber 2019.
APPROVAL AND CERTIFICATIONSuccessful practitioners will receive a SAAD certificateconfirming ‘SAAD Assessed Sedation Therapist’ statuswhich will enable you to practice independently.

74 SAAD DIGEST | VOL.34 | 2018
FORUM
Q. I am the practice manager of a dental practice and waspreviously a sedation trained dental nurse, although I amno longer on the General Dental Council (GDC) register. CanI still occasionally act as a sedation nurse?
A. Unless you are on a recognised supervised trainingprogramme, to carry out any clinical procedure or assist in asurgery environment, you are required to be registered with anappropriate professional body. Registration with the GDC isrequired before you can become indemnified.
The GDC states that “To assist with any dental procedure youhave to be appropriately indemnified. To be indemnified you needto be registered with the GDC so unfortunately if you are no longeron the GDC register, you will not be able to assist clinically in anycapacity. To be registered with the GDC you have to work withinthe Scope of Practice guidance, which outlines the duties that eachmember of the dental team is able to carry out on registrationhttps://www.gdc-uk.org/professionals/standards/st-scope-ofpractice. Section 38 of the Dentists’ Act, states that it is a criminaloffence for a person who is not a registered dentist or a registereddental care professional to practise dentistry”.
Q: As a Dental Therapist can I provide inhalational sedation toa patient without a dentist being on the premises?
A: Yes, Dental Therapists or Dental Hygienists can provide dentalsedation without a dentist being on the premises as long asthey are supported by an appropriately sedation trained andexperienced individual (second appropriate person) such as asedation trained dental nurse.
This question forms part of the Standards for ConsciousSedation FAQs developed following the publication of theIACSD standards and can be found by following the link below. https://www.rcseng.ac.uk/dental-faculties/fds/publications-guidelines/standards-for-conscious-sedation-in-the-provision-of-dental-care-and-accreditation/faq/
Q: How do I provide an in-house sedation training course inmy own sedation practice for new staff?
A: For those staff completely new to sedation, the IACSDstandards training pathway should be followed. To trainindividuals in a conscious sedation technique that allows themto practise independently, you need to apply for courseapproval via an external verification process. This is provided bythe Sedation Training Accreditation Committee (STAC) andapplication forms are available from the Royal College ofSurgeons website. In line with the training pathways outlinedin the IACSD standards, courses must also include supervisedclinical practice. https://www.rcseng.ac.uk/-/media/files/rcs/fds/publications/
standards-for-conscious-sedation-and-accreditation/stac-course-accreditation-form-june-2017.doc?la=en
Continuing professional development in sedation or sedationupdate courses offering only knowledge and skills training, donot need STAC approval. University, dental school orpostgraduate deanery courses are also exempt from the STACapproval process.
Q: Do I have to cannulate a patient having oral sedation orpremedication to manage their dental anxiety?
A: Firstly, a distinction should be made between oralpremedication and oral sedation. Oral premedication for dentalprocedures is usually a low dose Benzodiazepine, taken by thepatient before attending the surgery or the night before theappointment. No additional monitoring is needed for oralpremedication and there is no requirement for additionalsedation skills such as cannulation.
Oral sedation, usually a higher dose Benzodiazepine, is given tothe patient when they arrive at the dental surgery by anappropriately sedation trained dental team member. In orderto administer oral sedation for dental procedures, sedationtraining in the form of knowledge, skills training andsupervised practice are mandatory. Appropriate monitoringequipment is required and the patient should be cannulated assoon as practicable following the oral sedation.
Q: How do I dispose of Midazolam safely?
A: Midazolam should be rendered irretrievable before disposal.This means that the remaining Midazolam in the syringe /ampoule should be squirted onto cotton wool / gauze (orsimilar) before being placed into the sharps bin, or acommercial controlled drugs kit used. The kits contain granuleswhich denature and congeal drugs rendering them harmlessand unfit for inappropriate use. You may find this documenthelpful: https://www.sps.nhs.uk/wp-content/uploads/2016/06/NW-QA178.4-Controlled-drugs-for-dentists-.pdf
Q: Do I need to open a new ampoule of Midazolam for everypatient?
A: The Association of Anaesthetists of Great Britain and Ireland(AAGBI) published a safety guideline in October 2008, ‘InfectionControl in Anaesthesia’. Under the heading of ‘PreventingContamination of Drugs’ it states that ‘A syringe must not beused for multiple patients even if the needle is changed. Beforeuse, prepared syringes and needles should be stored in a cleancontainer and syringes capped to avoid contamination………..Single use ampoules should be discarded after the requiredamount of drug is drawn up and not re-used for subsequentpatients.’ (AAGBI 2008: 6)
Secretary’s CorrespondenceSadie Hughes BDS MFDSRCPS(Glas) MScSAAD Honorary [email protected]
The following is a selection of the more commonly asked questions I have received as secretary over the last year:

75SAAD DIGEST | VOL.34 | 2018
ELECTRONIC RECORD KEEPINGElectronic Record Keeping in SedationKellie Downie BDS MFDS RCPS (Glas) DipConSed SAAD Trustee & Assistant Honorary [email protected]
Contemporaneous and accurate record keeping is becoming morechallenging and demanding of dentists’ clinical time. Failure tokeep good records not only depreciates patient care but also putsthe clinician at risk of regulatory or civil proceedings which maybe difficult to defend.
It is often the case that in a busy clinical environment, cliniciansmay wish to be able to make records as quickly and convenientlyas possible, however, it is of vital importance that the accuracy,completeness and integrity of the records are maintained. It is vitalthat a robust assessment record is followed by a a clear operativeand peri-operative record followed by a proper discharge record.
There is now more regulation of record keeping in dentistry bothfrom the GDC and CQC.
The GDC clearly defines a professional obligation to accuratelyrecord the dental treatment that is provided to patients. This isoutlined by the GDC in Standards for the Dental Team; Standard4.1.1
‘You must make and keep contemporaneous, complete andaccurate patient records’
The CQC has its own regulation relating to record keeping which isrelevant to the dental field -
Regulation 20 of the Health and Social Care Act 2008 (RegulatedActivities) Regulations 2014 (No 2936)2 states that:
1 The registered person must ensure that service users areprotected against the risks of unsafe or inappropriate care andtreatment arising from a lack of proper information aboutthem by means of the maintenance of:
1 an accurate record in respect of each service user whichshall include appropriate information and documentsin relation to the care and treatment provided to eachservice user; and
2 such other records as are appropriate in relation to
2 The registered person must ensure that the records referred toin paragraph (1) (which may be in paper or electronic form)are:1 kept securely and can be located promptly when required;2 retained for an appropriate period of time; and3 securely destroyed when it is appropriate to do so.
Many specialist dental software systems allow for templateproformas to be developed in order to act as an aide-memoireensuring basic information is recorded to which free hand notescan be added. Its now well recognised that template style recordsshould be used with caution. Pre populated fields create a risk ofinaccurate and meaningless records and should be avoided.Equally, cut and paste preformed text templates carry the risk ofbeing used as a process rather than a genuinely reflective note.
Each individual field should be considered and completed toaccurately reflect the appointment and treatment provided. It isthen generally well accepted that templates can be compiled andcompleted as a basic record which then can be developed andadded to in order to fully reflect the appointment that took place.
To provide a basic template for clinicians to utilise as a guide forrecording sedation services, a focus group of members of theSAAD Board of Trustees met and deliberated information thatshould be considered and recorded for appointments relevant tosedation services in dentistry and based on the current nationalstandards for sedation assessment, inhalation sedation andintravenous sedation. It was determined what essentialinformation should be recorded at each appointment and how thiscould be presented. This was developed on three softwaresystems R4, Software of Excellence and Systems for Dentists.
Screen shots prepared for each system are available now on theSAAD website, through the members section, to allow clinicians todevelop their own templates relevant to their practice and toinspire ideas to improve ease of record keeping. Templates forSoftware of Excellence are available to be directly integrated. Theother software can be devoped individually with software systemsto allow clinicians to edit, develop and utilise in their ownpractices.
1. General Dental Council. Standards for the Dental Team. Standard 4.1. Informationat https://standards.gdc-uk.org/pages/principle4/principle4.aspx (accessedDecember 2017).
2. Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 (No2936) Information athttp://www.legislation.gov.uk/uksi/2010/781/regulation/20/made (accessedDecember 2017).
& & & & &&3($&.$.4$#'5&.$%61&
&&&&
&&&
&&
!&
(3& & & & &
&& & &
&&&&
&&&
&&
&
5.4& & & & &
&& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
.$$(3& & & & &
&& & &
&&&&
&&&
&&
&
16%.$5'#$.4.$& & & & &
&& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
& & & & &&
& & &
&&&&
&&&
&&
&
Advert Board
Media / Logo
Member Documents
My Details
Subscription
Course History
Shop Orders
My Information
Update my details
Historic Certificates
FAQs
Electronic Records⁄

76 SAAD DIGEST | VOL.34 | 2018
ELECTRONIC RECORD KEEPING
Electronic RecordsSAAD recognises that sedation records can be adequately kept in narrative form either in manually written records or text input on computer software. Keepingrobust notes of the sedation assessment, clinical procedure and discharge of the patient can be assisted by the use of properly prepared custom screensrecording relevant data.The following are exemplars that have been developed by an expert working group that can be used in some commercially available dental software. Thesemay be developed further to meet your facilities individual needs. The content of these is considered to be guidance towards good practice.If the exemplars are modified then care should be taken to avoid pre filled data fields or those that default to a specific answer. There should be a tendencytowards the need for a positive action to complete a drop down box choice or radio button choice so that data can be considered valid and individual specific.Instructions for use of the SAAD electronic records below are a guide. SAAD does not offer technical support for downloads.
Software of Excellence: ExactDownload the files below to your computer. (Right click on the file name and select ‘download linked file’)
Each custom screen (file) is imported individually.
In Exact enter the Configure tab in the taskbar.
Choose Custom Screens.
Click Import on the lower right of the screen.
Find the file click Open.
Sedation Assessment: Sedation Assessment SOE-1.CSV
IV Sedation Treatment: IV Sedation Treatment SOE-1.CSV
Inhalation Sedation: Inhalation Sedation SOE-1.CSV
Recovery and Discharge: Sedation Recovery and Discharge SOE-1.CSV
Systems for DentistsDownload the files below to your computer. (Right click on the file name and select ‘download linked file’)
Please contact your software provider for software support to upload these files to your system.
Sedation Assessment: Sedation Assessment SFD-1.xml
IV Sedation Treatment: Intravenous Sedation Treatment SFD-1.xml
Inhalation Sedation: Inhalation Sedation Treatment SFD-1.xml
Recovery and Discharge: Sedation Recovery and Discharge SFD-1.xml
Kodak R4Download the templates below to adapt for your own systems.
Sedation Assessment: Sedation Assessment R4 Word Template
IV Sedation Treatment: IV Sedation Treatment R4 Word Template
Inhalation Sedation: IS Sedation Treatment R4 Word Template

Symposiumand AGM
Saturday 22 September 2018
The Royal Society of Medicine,1 Wimpole Street, London W1G 0AE
Details will be posted atwww.saad.org.uk
| s | w

10 SAAD DIGEST | VOL.32 | JANUARY 2016
FORTHCOMING COURSES:3/4 March 2018 2/3 March 201916/17 June 2018 15/16 June 20193/4 Nov 2018 2/3 Nov 2019
DETAILS AND ONLINE REGISTRATION www.saad.org.uk
NATIONAL COURSEIN CONSCIOUS SEDATIONFOR DENTISTS AND DENTAL NURSESDENTAL HYGIENISTS AND THERAPISTS
Patients appreciate being offered sedation for their dental treatment, whetherthey are fearful, phobic or simply have a long and tedious procedure in prospect.The SAAD course provides underpinning knowledge and training in the clinicalskills required to provide the Standard sedation techniques. Advanced sedationtechniques are introduced and discussed.It is designed both as an introduction and as an update for more experiencedsedationists. Guidance is given regarding further training and the acquisition ofclinical experience.‘New starters’ in conscious sedation are advised to refer to theSAAD Assessed Sedationist Scheme for information on how to obtain thenecessary clinical experience.Dentists are encouraged to enrol their dental nurses on the parallel course assuccessful sedation depends on effective team work.SAAD’s teaching is provided by a faculty that includes some of the best-knownnames in conscious sedation in the UK. The courses are ‘busy’ but fun with manyopportunities for hands-on sessions.Quotes from recent evaluation forms:‘A lively weekend with friendly and approachable lectures.’‘I am now confident that I can provide a better service to my patients.’The course is held atMile End Road Campus, Queen Mary, University of London.EnQUIRIES:Fiona Trimingham (Executive Secretary)Course enquiries, payments, cancellations and deferrals, hygienist & therapistcourse logbooks01302 846 149 [email protected] Richman (Course Administrator) Course weekend logistics07583 039 309 (text) [email protected] for the SAAD Assessed Sedationist and SAAD Assessed Sedation nurse scheme are on pages 79 & 80

SAAD Assessed Sedationist(SAS) scheme
Under current IACSD guidance, any practitioner who was not practising sedation independently prior to April 2015, is designated a ‘New Starter’ and will need to undergo a period of supervised clinical practice before being able
to practice sedation independently.
Following on from the SAAD National course, the new, IACSDaccredited, SAAD Assessed Sedationist scheme (SAS scheme)
facilitates acquisition of the required supervised clinical experience (see IACSD Standards, Table 1)
The new SAS scheme includes approval of a proposed supervisor(s),
verification of a Clinical Logbook, Direct Observation of Practice (DOP) forms
and the Practice Evaluation checklist.
Successful practitioners will receive a SAAD certificate confirming ‘SAAD Assessed Sedationist’ status
which will enable them to practise independently.
Enrolment in the SAS scheme is only available for ‘New Starters’registered for the SAAD National course.
The total fee for enrolment on the SAS scheme is £1000.(includes the National Course fee of £700)
Further details are available athttps://www.saad.org.uk/index.php/sas-scheme
Enquiries to [email protected]
NB: Practitioners who have already attended SAAD(or other sedation courses) are not eligible.

SAAD Assessed Sedation Nurse(SASN) scheme
Under the IACSD standards anyone who was not practising sedationbefore April 2015 must attend a university, deanery or IACSD accredited
sedation course that includes the provision of knowledge, skills andsupervised clinical practice.
The SAAD Assessed Sedation Nurse (SASN) scheme is IACSD accreditedand provides the skills, knowledge and supervised clinical practice
required to assist in the provision of sedation before a final assessmentof competence.
What is involvedThe first stage of the SASN scheme is the two day SAAD Dental Nurse
Course in Conscious Sedation for Dentistry, (SAAD National Course) thisis when you will acquire the underpinning knowledge and skills. Thiscourse is a stand alone course that can be also attended as a refresher.
How to enrolIf you would like to enrol for the SASN scheme please complete theonline registration for the first stage, SAAD Dental Nurse Course inConscious Sedation for Dentistry, the fee for the first stage is £400.
Then enrol for the second stage, SAAD Assessed Sedation Nurse scheme,via the SAAD website (www.saad.org.uk) the fee for this stage is £470.
The SASN scheme will run from the date you attend theSAAD National course
The total fee to become a SAAD Assessed Sedation Nurse is £870.
Any questions?Further details are available at
https://www.saad.org.uk/index.php/sasn-scheme
If you have any questions please contact [email protected] the first instance.

ESSAY PRIZESDRUMMOND-JACKSON ESSAY PRIZEDRUMMOND-JACKSON ESSAY PRIZE
££550000DCPsDCPs££330000
DENTAL STUDENTSDENTAL STUDENTS££330000
For essays on any subject related toConscious Sedation, Anxiety Control,
General Anaesthesia or Analgesia in dentistry.
The winners of the SAAD Essay Prize receive a complimentaryregistration for the SAAD Symposium in order to be presented withtheir award certificate and cheque. In addition to this the prize-winning essays are considered for publication in the SAAD Digest.
• Write an essay in ENGLISH in A4 format with double spacing, as a MicrosoftWord document. Drummond-Jackson not exceeding 5,000 words, DCPs notexceeding 2,500 words, Dental Students not exceeding 3,000 words.
• Entries must be received and acknowledged by 31st March.
• Essays must be written in accordance to SAAD’s Guidelines for Authorsavailable from the SAAD website and on page 89 of this Digest.
• The decision of the panel of assessors appointed by SAAD will be final.
• Entries, accompanied by name, address and telephone number, should beemailed to [email protected]
SAAD DIGEST | VOL.24 | JANUARY 2008 59
Saturday 26 September 2009
The Royal Society of Medicine1 Wimpole Street, London W1G 0AE
Enquiries:SAAD, 21 Portland Place, London W1B 1PY
020 7631 8893 | [email protected] | www.saad.org.uk
Annual Conference and AGM
SAAD Digest Vol 24_56-63.indd 59 21/12/2007 14:54:13

SAAD SuppliesNon Postage &
Membersmembers Packaging
CBT Toolkit £22.50 £30.00 £3.00
A History of SAAD by Peter Sykes £5.00 £5.00 £3.00
Order online at http://www.saad.org.uk/index.php/eshop
The SAAD record cards and leaflets are no longer available. These have become largely outdatedwith the more widespread use of electronic records.
Examples of electronic patient record templates are available to SAAD members from the SAADwebsite. Please see page 75 for details.
For patient information leaflets, we would encourage clinicians and service providers to refer toAppendix 3 in the IACSD 2015 document Standards for Conscious Sedation in the Provision ofDental Care for examples of patient leaflets/information.
Enquiries to [email protected] or 01302 846 149
SAAD Subscriptions
Please renew online by logging onto the
SAAD website using your email address
as your username or by contacting
[email protected] to pay by direct debit.
We would ask you to renew by direct debit
since this will enable us to keep administration costs
to a minimum for the Society.
82 SAAD DIGEST | VOL.34 | 2018

83SAAD DIGEST | VOL.34 | 2018
WEBSITEwwwwww..ssaaaadd..oorrgg..uukk
• Online CPDLog-on the membership area and follow the link ‘Online CPD’
Answer multiple choice questions related to the refereed papers in this issue of the Digest.
Download your CPD certificate
• Latest news relating to conscious sedation
• SAAD coursesdetails, dates and online registration
• Sedation related documents for downloading
• Membership details and subscribe online facility
• Download back issues of the Digest and Newsletter
• Details of RA machine loan scheme, research grants and essay prizes
• Online registration for the symposium
• SAAD contact numbers and email addresses
IN THE MEMBERSHIP AREA • Media page – members of SAAD may use the SAAD logo
on their literature. The logo is available in PDF or JPEG format to download from the website.
• Documents – course handbook
• Pay subscriptions online
• Forum for adverts(equipment, positions vacant, positions sought etc)
• Complimentary access to the online CPD
• Electronic template samples (see page 75 for details)

84 SAAD DIGEST | VOL.34 | 2018
PRODUCT NEWS!"#$%&'(")%$*+#',--")*%$"'.*/"'(011+2$'3+024"'''''''''''''''''''''''''52+-'6"4047&04'82%*#*#9'!
!!!!!!!!!!!!!!!!!!!!!!!!!!!"#$%!&'(!)*+,!-.*/$0+!*%%.1()!234!5&.1%(!6&1!0#(!5&'%5$&.%!!!!!
%()*0$&'!)('0*/!0(*7!$'5/.)(%8!!!!9! !"#$%&'(%)%*+(+),'")-./0")*'123","4+'1#+33/#+'4+),".%,"2)5')%3216%#&)*+%.5'
2#216%#&)*+%.'%"#$%&'%)0'7),+#3/#*"-%.'"8*+.9':1"-,/#+0;'!9! <+-2*)","2)'%)0'(%)%*+(+),'2='24+#'3+0%,"2)5'%)%16&.%>"35'-6+3,'1%")5'
%3,6(%5'3+"?/#+5'6&12*.&-%+("%'%)0'-62@")*''9! A(+#*+)-&'0+),%.'0#/*3B'$6+)5'62$5'
$6&''''''
9! CDE'%)0'0+="F#"..%,"2)'=2#'%0/.,'%)0'-6".0'
'9! G%#0"%-'%##+3,'3-+)%#"23''
'9! H+%('#2.+3'%)0'#+312)3"F".","+3''
!!!://!5&.1%(%!*1(!)(/$;(1()!*')!*%%(%%()!<+!=(%.%5$0*0$&'!2&.'5$/!>?@A!
5/$'$5*/!$'%01.50&1%!*')!)('0*/!7()$5*/!(7(1B('5+!%C(5$*/$%0%D'!E.55(%%6./!5*')$)*0(%!1(5($;(!F!-.*/$0+!*%%.1()!*')!;(1$6$*</(!(234!C&$'0%!*%!C(1!G42!HIJK!
B.$)(/$'(%D!2&.1%(!5&7C/$(%!L$0#!M:2E4!5&'%5$&.%!%()*0$&'!%0*')*1)%!HIJND!
Dental Sedation Immediate Life Support CourseFrom ResusPlus Training
Whichever pharmacological methods of conscious sedation you provide to your patients, recognition of inadvertent over-sedation with appropriate reversal techniques and urgent management and rescue of a compromised airway or reducedrespiratory drive is paramount for patient safety.
The 2015 Report of the Intercollegiate Advisory Committee for Sedation in Dentistry (IACSD) ‘’Standards for ConsciousSedation in the Provision of Dental Care’’ states that:
‘’The term ‘rescue’ derives from anaesthetic practice and means the ability to respond appropriately to . . . inadvertent over-sedation . . .practitioners must be able to perform Immediate Life Support/Paediatric Immediate Life Support, depending on the patient’s age,and that they must be able to recognise and manage sedation-related complications (including over-sedation, respiratorydepression/apnoea, unconscious patient, airway obstruction, vomiting, idiosyncratic responses, delayed recovery, failure of conscioussedation). ‘Deployable’ airway competencies (including basic airway manoeuvres, the use of airway adjuncts and the ability toadminister positive pressure ventilation) are mandatory. Alternative courses with equivalent content which are adapted to the needsof dental practice are acceptable: these might also include the management of common sedation, medical and dental emergencies.”
ResusPlus Training are based in the South Midlands and are medical emergency training specialists for health professionals.ResusPlus Training provide a dental focused 7-hour adult immediate life support and paediatric immediate life support course(ILS and PILS) in one day which meet the above IACSD conditions and more and with plenty of hands-on practice. Courses take place on a regular basis and can also take place at your own venue. For in-house courses please contactResusPlus Training with your individual practice requirements.
Dental Sedation Immediate Life Support Course: The course day starts with the adult component for a minimum of 5hours, then explores the changes required to assess, rescue and perform BLS on a child. This paediatric component takes 1.5 to2 hours and can provide invaluable theoretical and practical information for both adult and paediatric teams.
The course includes specific CPD learning outcomes regarding:
· Airway management including positive pressure ventilation with bag valve mask and pocket mask and use ofnasopharyngeal and oropharyngeal airway. It will also include i-gel insertion both during respiratory depression and incardiac arrest.
· ABCDE approach to the management of common sedation and dental medical emergencies such as CNS depression,anaphylaxis, chest pain, asthma, seizure, hypoglycaemia and choking.
· Emergency dental drugs with hands-on practice for the above conditions.
· BLS and defibrillation refresher practice for all.
· Cardiac arrest scenarios – a team approach.
· Team roles and responsibilities – leadership, communication, planning.
Who is the course for? The course is principally for conscious sedation-trained dentists, nurses, hygienists and therapists butcan also be attended by any dental professionals looking to take their life support skills to a higher level.
Delivered by: To ensure you receive the most beneficial training experience and ongoing quality assurance, courses aretaught using a high ratio of instructors to students and only by Resuscitation Council (UK) clinical instructors and dentalmedical emergency specialists.
Assessment: Is subject to quality assurance. Assessment is continuous and includes the ABCDE approach, i-gel and otherpractical airway management skills for both inadvertent over-sedation and cardiac arrest scenarios.
Certificates: For successful candidates, certificates provide 7 verifiable and quality assured, eCPD points and as per GDC 2018guidelines.
For contact information please refer to the advertisement on page 85

!"#$%&'(")%$*+#',--")*%$"'.*/"'(011+2$'3+024"'''''''''''''''''''''''''52+-'6"4047&04'82%*#*#9'!
!!!!!!!!!!!!!!!!!!!!!!!!!!!"#$%!&'(!)*+,!-.*/$0+!*%%.1()!234!5&.1%(!6&1!0#(!5&'%5$&.%!!!!!
%()*0$&'!)('0*/!0(*7!$'5/.)(%8!!!!9! !"#$%&'(%)%*+(+),'")-./0")*'123","4+'1#+33/#+'4+),".%,"2)5')%3216%#&)*+%.5'
2#216%#&)*+%.'%"#$%&'%)0'7),+#3/#*"-%.'"8*+.9':1"-,/#+0;'!9! <+-2*)","2)'%)0'(%)%*+(+),'2='24+#'3+0%,"2)5'%)%16&.%>"35'-6+3,'1%")5'
%3,6(%5'3+"?/#+5'6&12*.&-%+("%'%)0'-62@")*''9! A(+#*+)-&'0+),%.'0#/*3B'$6+)5'62$5'
$6&''''''
9! CDE'%)0'0+="F#"..%,"2)'=2#'%0/.,'%)0'-6".0'
'9! G%#0"%-'%##+3,'3-+)%#"23''
'9! H+%('#2.+3'%)0'#+312)3"F".","+3''
!!!://!5&.1%(%!*1(!)(/$;(1()!*')!*%%(%%()!<+!=(%.%5$0*0$&'!2&.'5$/!>?@A!
5/$'$5*/!$'%01.50&1%!*')!)('0*/!7()$5*/!(7(1B('5+!%C(5$*/$%0%D'!E.55(%%6./!5*')$)*0(%!1(5($;(!F!-.*/$0+!*%%.1()!*')!;(1$6$*</(!(234!C&$'0%!*%!C(1!G42!HIJK!
B.$)(/$'(%D!2&.1%(!5&7C/$(%!L$0#!M:2E4!5&'%5$&.%!%()*0$&'!%0*')*1)%!HIJND!
"&!<&&O!&1!6&1!7&1(!$'6&17*0$&'!C/(*%(!5&'0*50!=(%.%3/.%!"1*$'$'B!!!!!LLLD1(%.%C/.%01*$'$'BD5&7!!$'6&P1(%.%C/.%01*$'$'BD5&7!!!!! ! ! !!IJHKI!FIQIJQ!R!IFFI!HNI!SSTF'
!

RA Medical Services LtdInhalation Sedation Specialists
TO PLACE YOUR ORDER SIMPLY CALL...
HOLMES HOUSESKIPTON ROAD
STEETONWEST YORKSHIRE
BD20 6SD
T: +44 (0)1535 652444F: +44 (0)1535 653333
A specialist company for the supply, installation, repair and maintenance of Inhalation Sedation and associated equipment.
advice to help you setup
units to piped systems.
This is a well tried and trusted, safe and non-invasive technique
GDP’s anxious patients.
Other options are a Miniscav™unit.
MINISCAV ACTIVE SCAVENGER RA2046 £930.00
MDM SEDATION PACKAGE 9450 0150/P £3,600.00
We have a selection of R A
+44 (0)1535 652444
maintenance of Inhalation Sedation and associated equipment.
maintenance of Inhalation maintenance of Inhalation supply, installation, rsupply, installation, rA specialist company for the supply, installation, rmaintenance of Inhalation maintenance of Inhalation
equipment.
maintenance of Inhalation supply, installation, r
equipment.equipment.equipment.equipment.
supply, installation, rmaintenance of Inhalation
equipment.
A specialist company for the
equipment.equipment.Sedation and associated Sedation and associated Sedation and associated Sedation and associated Sedation and associated Sedation and associated maintenance of Inhalation maintenance of Inhalation maintenance of Inhalation maintenance of Inhalation maintenance of Inhalation supply, installation, rsupply, installation, rsupply, installation, rsupply, installation, rsupply, installation, rsupply, installation, rsupply, installation, rsupply, installation, rsupply, installation, rA specialist company for the A specialist company for the A specialist company for the A specialist company for the A specialist company for the A specialist company for the A specialist company for the A specialist company for the A specialist company for the A specialist company for the
Sedation and associated
A specialist company for the supply, installation, rsupply, installation, rmaintenance of Inhalation supply, installation, rmaintenance of Inhalation supply, installation, rA specialist company for the
epair and supply, installation, r
Sedation and associated Sedation and associated
A specialist company for the
Sedation and associated
epair and maintenance of Inhalation maintenance of Inhalation maintenance of Inhalation maintenance of Inhalation maintenance of Inhalation
epair and supply, installation, repair and supply, installation, rsupply, installation, rA specialist company for the supply, installation, rA specialist company for the A specialist company for the A specialist company for the A specialist company for the
e have a selection of R A W
e have a selection of R A e have a selection of R A
e have a selection of R A
units to piped systems.
advice to help you setup advice to help you setup
units to piped systems.units to piped systems.units to piped systems.
advice to help you setup advice to help you setup advice to help you setup advice to help you setup advice to help you setup advice to help you setup advice to help you setup
ACKAGETION P 9450 0150/P
£3,600.009450 0150/P
£930.00RA2046
MedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaMedicaRA

al Dent
kinL
iate Life Immed
e Ono thed tekke Consors fs forrddanSta
al Dent
pporSuiate Life
rseou CDaye isiorovPeh tn iiontSedas iouc Cons
tppor
rse510 2rel Caatne Dff onisio
kinL
o thed tekke Consors fs forrddanSta
isiorovPeh tn iiontSedas iouc Cons
510 2rel Caatne Dff D onisio
is Thwho
t ad eimais esurcois esusoicnscoevidopr
Nurl anteDd reeRegistirethinthwin odatie
ists nteDnd asesNurvers:codice anpract
vers:
who
esusoicnscoevidopr
Reforg ninlanP
n FactorsaHum
sessingAs
irethinthwin odatie
a(adultsnioitatscsuRe
ncyergemEcting effa
tieaPl lwen Unasessing
vers:codice anpract
n)erchildnda
mentgenaaMncy
nttie
vers:
Adults an
Airwa
phylaaAn
dAdults an SBLldiCh
tmenegnay MaAirwa
Fand aingxis, Fittphyla
inting
ow k nooBCGh Ewit
ow CG
w.eww
s@riequine 899 4234508
kg.co.uininragtcw.e.ukg.coininragtces@
3 899 @ _MKGCE

McKesson has been established for 80 years
in Great Britain, providing essential
equipment for dental sedation.
We continue to manufacture inhalation
sedation machines like the current McKesson
MC1 pictured here, at our factory, situated in
Chesterfield, Derbyshire.
We welcome all enquiries for inhalation
sedation equipment, including items for
scavenging, monitoring and resuscitation.
Contact us on Tel: 01246 [email protected]
Cestradent McKesson110 Park Road, ChesterfieldDerbyshire S40 2JX
!
!
!!! ! ! ! !!!!
!
!!! !!!
( ( ( ( ( ( ( ( ( ((( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( ( (
( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( (
( ( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
(
(((
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
! !
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
(
(((
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
(
(((
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
(
( (
!
!
!!! !! !!!
!
!!! !!!
( ( ( ( ( ( ( ( ((( (( ( ( ( (
( ( ( ( ( ( ( (( ( ( ( ( ( ( ( (
( ( (
( ( ( ( ( ( ( ((
( ( ( ( ((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((((
(
(
( (( (
((( (( (( (
(
(
( (
Celebrating 80 Yearsof McKesson
1938 - 2018

Guidelines for AuthorsSAAD Digest: Guidelines for Authors
SAAD Digest is the Journal of the Society for the Advancement of Anaesthesia inDentistry and has been published regularly in London UK, since 1970. It has beenproduced in its current format since 2006. One edition is published each year inJanuary. Copies of all editions produced since then are available online athttp://www.saad.org.uk/saad-digest/
The Digest has become a unique and invaluable international forum for all interestedin advancement of knowledge in pain and anxiety control for dentistry. The EditorialBoard invites contributions from all active in the field. Since only one edition isproduced each year, potential Authors should be aware of the following details andschedule to avoid excessive publication delay and disappointment.
Contribution formatsThe Board welcomes Research articles, Reports of Randomised controlled trials,articles derived from Diploma Dissertations, Practice-related articles, Education,Professional Opinion, Case Reports and General articles. If in any doubt about theformat or content of a proposed article please contact the Secretary beforesubmission. It should be noted that articles are now only accepted in digital formatand via email. It is a condition of acceptance of manuscripts that they are the worksolely of the author or authors stated and that they have not been previouslypublished elsewhere (either in print or electronic format) nor are they underconsideration by any other periodical. Manuscripts should meet the following criteria:they should be original, clearly written, relevant to dentistry, reader-orientated (inother words written to appeal to the readership of any interested in pain and anxietycontrol in Dentistry) and designed to inform, add to discussion or debate, or entertain.Research papers should also have appropriate study methods, valid data andconclusions that are supported by the data.
Publication ScheduleThe following annual publication schedule is provided for guidance only and assumesa Digest publication date of January Year 01.August Year -1 > July 31st Year 00: Articles may be submitted for Jan 01 EditionAugust 1st 00: Submission for Jan 01 edition closed. (Articles submitted after 31st Julywill be considered for Year 02 Edition)
Submission and reviewManuscripts may only be submitted by email to the Secretary at [email protected] will generally be processed as they are received and it is expected thatsubmission will be acknowledged by the Secretary soon after they are received, witha reference number allotted for future correspondence.
Authors should note that submitted papers not fully conforming to these ‘AuthorsGuidelines’, especially in terms of length and manuscript format, will be returnedfor correction without consideration or peer review, and in such cases publicationmight well be delayed or subsequently declined.
Peer review is carried out by at least two anonymous referees, and the Chairman of theEditorial Board. Additional statistical advice may be sought if required.
Authors will be advised as soon as possible, that either their Paper….1. is suitable for publication without amendment,2. is suitable for publication with some amendments,3. may be suitable but requires major rewriting,4. is rejected.
In any case, Authors will receive the anonymous structured feedback of the reviewersfrom the Secretary advising them of the decision level as above, and the action (if any)to be taken before resubmission. Delays in action on such advice may causepublication delay or even rejection if the publication deadlines are missed.
Once a manuscript is accepted for publication, authors will be advised whether theirpaper is to be published in the next issue or is, at the discretion of the Board, to be heldfor the following issue in order to obtain the appropriate balance for each edition. Forsimilar reasons, in some cases the final decision on acceptance may be delayed. Alldecisions to publish are at the discretion of the Board alone whose decision is final.
The principal author of a manuscript accepted for publication will later be e-mailed apdf version of their article for proofing. Any errors identified and requiring correctionmust be notified by email without delay, and at the latest within 1 week. No revisionof the wording or other change, other than correction of proofing errors, will beallowed at this stage.
Manuscript FormatManuscripts should be word-processed in Microsoft Word format and double-spacedwith a margin of at least 4 cm on the left-hand side. The pages should be numberedconsecutively with the numbers centred at the bottom of each page. The first page ofthe manuscript should give only the title of the article, and the author’s/authors’name(s), qualifications and address(es) including email address(es).
Length of contributionsContributions should be of no more than 3,000 words, to include tables and figures.Each table and figure will count as 100 words. Case reports are welcomed, but shouldbe of no more than 750 words in length.
Titles must be descriptive of the contents of the article, but yet concise. Papers shouldbe introduced with a short abstract which should be able to stand alone. The abstractshould not contain references or abbreviations, and should be no longer than 200words. The abstract will not contribute to the 3000 word limit.
Data or tables may be submitted in Microsoft Excel format or embedded in the text ofthe Word document.
Figures or images should be submitted as separately attached and clearly labelledfiles in JPEG format at a high resolution of 300 dpi. Colour illustrations are preferredwhere possible. If the illustration is of a subject’s face, written consent for itspublication must be obtained from the subject and attached with the article.Illustrations obtained from other sources such as books, or from colleagues, mustagain be accompanied by appropriate documentation indicating approval for theirpublication as part of the article from the copyright holder, or individual concerned.
Units used in the manuscript must conform to the Système Internationaled’Unités (SI).
References must be in the Vancouver style. They should be numbered in the order inwhich they appear in the text. The numbers should be inserted as superscripts eachtime the author is cited (Robb3-5 reported similar findings). Other references to thepaper should be given in the same way after punctuation (Other studies have shownthis to be true.4,5 Drummond-Jackson et al.6 demonstrated...) At the end of the articlethe full list of references should give the names and initials of all authors unless thereare more than six, in which case only the first three should be given followed by et al.The authors' names must be followed by the title of the article; the title of the journalabbreviated according to Index Medicus and Index to Dental Literature style; year ofpublication; volume number; and the first and last page numbers in full. Titles ofbooks should be followed by the place of publication, publisher, and the year. If thisreference citation style is not followed exactly, especially in relation to punctuationand spacing, the manuscript will be returned without review.
Examples of reference stylesReference to an article1. Molar L R, Fang-Jones Q, Jaw U. Are Teeth biting back?. Br Dent J 2006; 200: 144-146.Reference to a book2. Craig D C, Skelly A M. Practical Conscious Sedation. 1st ed. London: Quintessence,2004.Reference to a book chapter3. Robb N D. Conscious sedation in Dentistry. In Heasman PA (ed) Master Dentistry. Vol.2; Restorative Dentistry, Paediatric Dentistry and Orthodontics. pp 149-168.Edinburgh: Churchill Livingstone, 2003.Reference to a report4. Re-accreditation and re-certification for the dental profession. London: GeneralDental Council, 1997.Reference to a webpage3. General Dental Council. Scope of practice. 2009. Online information available atwww.gdc-uk.org/Newsandpublications/Publications/Publications/ScopeofpracticeApril2009[1].pdf (accessed April 2012).
The author/principal author is responsible for the accuracy of the reference list.
Acknowledgements should be grouped in a paragraph at the end of the text beforethe references. Permission and approval of the wording must be obtained from theperson(s) thanked. Where any research project was supported by industry, this shouldbe acknowledged in a covering letter to the Editor on submission of the manuscript.
Declaration of interests: Author(s) must ensure that they declare any possible conflictsof interest in their paper. This includes matters such as: direct funding from anorganisation or company for the research; funding received (or payment in kind) forany related work carried out from an organisation or company that could be linked tothe research; consultation or advisory positions held in an organisation or companyinvolved in the research or an organisation involved in similar research; any othersituation that could be construed as a conflict of interest.
EthicsArticles reporting clinical research must include a statement indicating thatappropriate Ethical Committee approval has been granted.
CopyrightUpon acceptance for publication in SAAD Digest, it is assumed that the author(s)assign(s) copyright of the article to the Society for the Advancement of Anaesthesia inDentistry. Single copies of the published article for personal study may be made freeof charge but multiple copies will require permission of the Editor prior to production.
89SAAD DIGEST | VOL.34 | 2018

90 SAAD DIGEST | VOL.34 | 2018
CPD 2017 ANSWERSSAAD Digest 2017Online CPDAnswers to the Questions
What's new in…capnography
1. In the UK, the term conscious sedation includes:a. Minimal sedationb. Deep sedationc. Moderate sedationd. General anaesthesia
Answers: a and c
2. For ASA 1 & 2 dental patients requiring conscious sedation,capnography monitoring is required in:a. Canadab. United States of Americac. United Kingdomd. Australia
Answers: a, b and d
3. In previous studies where patients were breathing room airduring their sedations and not routinely receivingsupplemental oxygen, the addition of capnography:a. Decreased the requirement for supplemental oxygenb. Did not decrease the rate of oxygen desaturationc. Increased the rate of oxygen desaturationd. Decreased the heart rate
Answer: b
4. Capnography measures:a. End tidal carbon dioxideb. Peripheral oxygen saturationc. Litres / minute of oxygend. AVPU score
Answer: a
Bispectral Index Guided Target Controlled Midazolam Sedation: a new advanced technique for dental procedures
1. With regards to BIS monitors, which of the followingstatements is FALSE:Bis monitors:a. monitor depression of the cerebral cortexb. monitor electrical activity c. use electroencephalography d. rank activity on a scale from 0 to 1000
Answer: d
2. In the described TCI-BIS sedation technique, the targetconcentration in the brain:a. is measured by means of chemical analysisb. is set at 80-90 ng/mlc. is calculated with the BIS machined. is initially set to 2 mg
Answer: b
3. In the described TCI-BIS sedation technique, the initial targetconcentration in the brain is set to:a. 0.75 mg/mlb. 2 mgc. 75 ng/Ld. 30 ng/ml
Answer: d
4. The described TCI-BIS sedation technique:a. enabled minimal sedation for prolonged treatment without
having to change the target concentrationb. prevented the cardiovascular response to midazolamc. enabled minimal sedation by a single operator/sedationist
within safe physiological limits for long treatments up to 3hours
d. prevents oversedation during induction of minimalsedation
Answer: c
A review of the use of flumazenil for the reversal of midazolam conscious sedation in dentistry.
1. In an emergency situation, where the reversal of midazolam isrequired, what is the standard dose of flumazenil that shouldinitially be administered intravenously as a slow bolus?a. 0.2 mgb. 0.5 mgc. 1 mgd. 2 mg
Answer: b
2. What is the approximate elimination half-life of flumazenil?a. 20 minutesb. 30 minutesc. 60 minutesd. 120 minutes
Answer: c
3. Following the Rapid Response Report (2008), whichconcentration of midazolam should be used in all clinical areas(except general anaesthesia or intensive care)?a. 0.5 mg / 1 mlb. 1 mg / 1 mlc. 2 mg / 1 mld. 5 mg / 1 ml
Answer: b

91SAAD DIGEST | VOL.34 | 2018
CPD 2017 ANSWERS4. Which of the following is NOT an indication for reversal of
midazolam induced conscious sedation in dentistry?a. Over sedationb. Patient with mobility issuesc. Patient with learning difficultiesd. Allergy to benzodiazepines
Answer: d
5. In which of the following groups of patients should caution beused if reversal with flumazenil is required?a. Patients with asthma requiring fluticasone inhaler useb. Patients with type 1 diabetes on subcutaneous insulinc. Patients with epilepsy taking clonazepamd. Patients with pernicious anaemia receiving 3 monthly
vitamin B12 injections
Answer: c
The decisional needs of young patients faced with the decision to undergo dental treatment with sedation or GA
1. The most frequently cited model of shared decision-making inhealthcare suggests the second stage of the process relates to:a. Deciding on which treatment to implementb. Information exchange c. Deliberation d. Evaluating the patient’s decision
Answer: c
2. A recent systematic review suggested that benefits of decisionaids for healthcare decisions include:a. Reduced decisional conflictb. Improved knowledgec. Reduced length of consultations d. Improved adherence to healthcare decisions
Answers: a and b
3. Themes that were identified as influencing the decision toundergo dental treatment with sedation or GA included:a. Timeb. Method of administrationc. Costd. Treatment type
Answers: a, b and d
4 According to Lagana and colleagues, what percentage of pre-anaesthesia consultations with paediatric patients failed toinclude discussion of the related risks of the procedure?a. 5%b. 20%c. 30%d. 50%
Answer: c
Sedation for Patients who LackCapacity
1. When assessing capacity, which of the following statements aretrue? a. a person can be deemed to lack mental capacity based on
their age, appearance or behaviourb. dental anxiety and phobia is irrelevantc. the clinician should have reasonable belief that the person
lacks capacity at the time the decision needs to be maded. a clinician should determine if a person’s understanding
will be better at a different time in the daye. appropriate communication measures should be taken for
patients with literacy and dyslexia difficulties
Answers: c, d and e
2. A Lasting Power of Attorney (LPA) is :a. the next of kin who can make decisions on behalf of thepersonb. a legal document made by the patient appointing one ormore persons to undertake decision making when the personlacks mental capacity c. a person appointed by the court of protection to safeguardthe patient’s best interestd. sought when the person lacking capacity has no otherrepresentatives other than paid carers e. all of the above
Answer: b
3. When undertaking a Best Interest assessment, the clinicianshould:a. consider if there are any valid and applicable advance
decisions to refuse treatmentb. seek advice from others relevant to the decision makingc. take into consideration the patient’s personal values,
beliefs, past and present wishes and feelingsd. seek advocacy if there are disagreements between carers
and health professionals.e. all of the above
Answer: e
4. The decision-maker should :a. clearly record the outcome on a Consent Form 2.b. discuss any form of clinical holding required at the best
interest assessment stagec. act to provide treatment in the least restrictive mannerd. should only suggest treatment option according to the
clinicians preferred choice of technique and not of thepatient’s needs
e. not need to review previous best interest decisions
Answers: b and c

DIARY SCAN Compiled by Dr C E Mercer
2018 DATE ORGANISATION THEME/TITLE VENUE CONTACT
MARCH
3 SAAD National Course in Conscious London www.saad.org.uk/index.php/Sedation for Dentistry coursesbyrole/view-all-courses
19 SEAUK Annual Scientific Meeting Cardiff www.seauk.org/asm2018/
APRIL
19-21 ADSA Annual Session Boston www.adsahome.org/annual-session
26-27 BSDH BSDH Spring Conference Poole www.bdsh.org
28 University of Portsmouth Conscious Sedation Update Portsmouth www.port.ac.uk/dental-academy/continuing-professional-development-cpd/conscious-sedation-update.html
MAY
1-2 British Pain Society Annual Scientific Meeting Brighton www.britishpainsociety.org/2018-asm-brighton/
9-12 World Institute of Pain 9th Congress Dublin wip2018.kenes.com/
15 DSTG Annual Symposium Newcastle www.DSTGsymposium.co.uk
JUNE
2-4 ESA Euroanaesthesia 2018 Copenhagen euroanaesthesia2018.esahq.org/
16-17 SAAD National Course in Conscious London www.saad.org.uk/index.php/Sedation for Dentistry coursesbyrole/view-all-courses
JULY
4-6 GAT Annual Scientific Meeting Glasgow www.gatasm.org
SEPTEMBER
6-8 ESPA/IAPA Congress Brussels www.euroespa.com/news/the-wfsa-has-endorsed-the-espa-iapa-congress-2018/
12-15 ESRA 37th Annual Congress Dublin www.esra-congress.com/2018/Pages/default.aspx#.WoXG2OfLjlU
22 SAAD Annual Symposium & AGM London www.saad.org.uk
26-28 AAGBI Annual Congress Dublin www.annualcongress.org
OCTOBER
5-7 IFDAS 15th International Dental Nara, Japan www.ifdas.orgCongress
NOVEMBER
3-4 SAAD National Course in Conscious London www.saad.org.uk/index.php/Sedation for Dentistry coursesbyrole/view-all-courses
DECEMBER
7 BSDH BSDH Winter Conference London www.bsdh.org
92 SAAD DIGEST | VOL.34 | 2018