Embed Size (px)
Citation preview
SACRED ENCOUNTERS
INSIDE
w WhyMagnet?byCNOKatieSkelton
w NewsfromTheCenterforCancerPreventionandTreatment
w UnpackingtheNew KnowledgeComponent
oftheMagnetJourney
w DesignforPerfectCareUpdate
w SacredEncounters/HealthiestCommunities
w PerfectCare/Growth
w TestYourNursingKnowledge
w QualityAwards
w BlessingoftheDocuments
w CalendarofEvents
EDITORIALBOARD:
PattiAubé
SoudiBogert
CarmenFerrell
StaceyFischer
SheilaHolliday
DanielleLinden
INSIDE THIS WINTER 2011 ISSUE
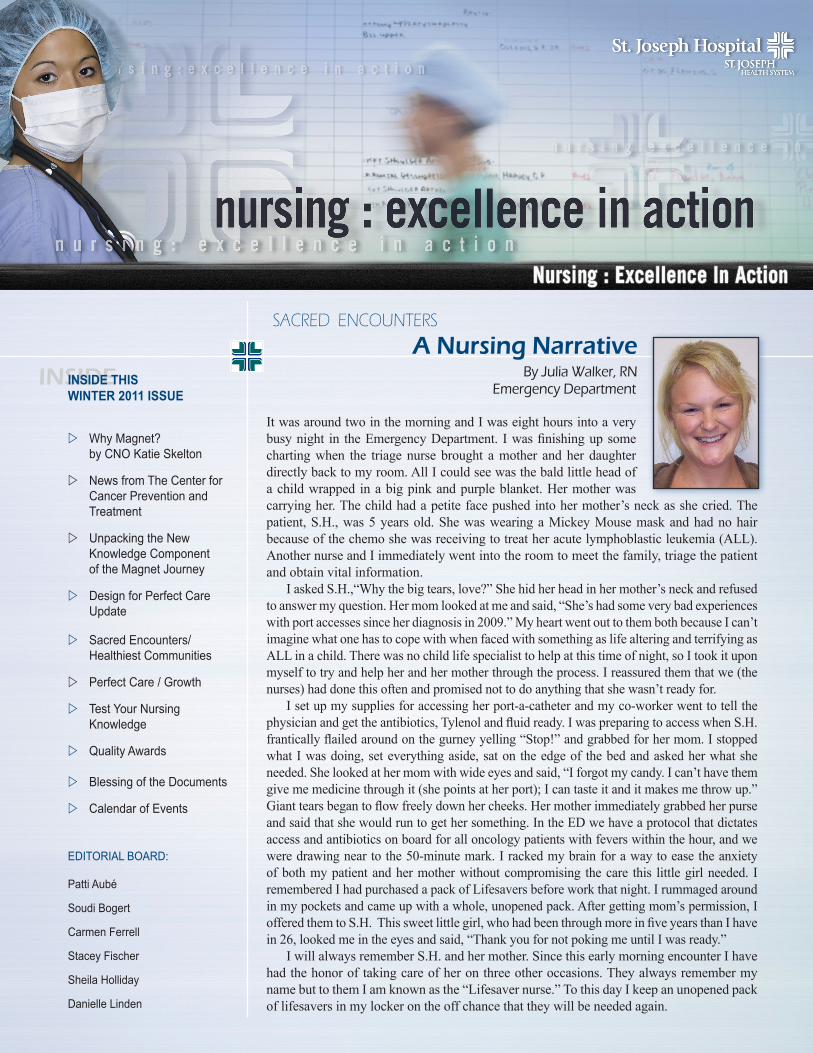
A Nursing NarrativeBy Julia Walker, RN
Emergency Department
It was around two in the morning and I was eight hours into a very busy night in the Emergency Department. I was finishing up some charting when the triage nurse brought a mother and her daughter directly back to my room. All I could see was the bald little head of a child wrapped in a big pink and purple blanket. Her mother was carrying her. The child had a petite face pushed into her mother’s neck as she cried. The patient, S.H., was 5 years old. She was wearing a Mickey Mouse mask and had no hair because of the chemo she was receiving to treat her acute lymphoblastic leukemia (ALL). Another nurse and I immediately went into the room to meet the family, triage the patient and obtain vital information. I asked S.H.,“Why the big tears, love?” She hid her head in her mother’s neck and refused to answer my question. Her mom looked at me and said, “She’s had some very bad experiences with port accesses since her diagnosis in 2009.” My heart went out to them both because I can’t imagine what one has to cope with when faced with something as life altering and terrifying as ALL in a child. There was no child life specialist to help at this time of night, so I took it upon myself to try and help her and her mother through the process. I reassured them that we (the nurses) had done this often and promised not to do anything that she wasn’t ready for. I set up my supplies for accessing her port-a-catheter and my co-worker went to tell the physician and get the antibiotics, Tylenol and fluid ready. I was preparing to access when S.H. frantically flailed around on the gurney yelling “Stop!” and grabbed for her mom. I stopped what I was doing, set everything aside, sat on the edge of the bed and asked her what she needed. She looked at her mom with wide eyes and said, “I forgot my candy. I can’t have them give me medicine through it (she points at her port); I can taste it and it makes me throw up.” Giant tears began to flow freely down her cheeks. Her mother immediately grabbed her purse and said that she would run to get her something. In the ED we have a protocol that dictates access and antibiotics on board for all oncology patients with fevers within the hour, and we were drawing near to the 50-minute mark. I racked my brain for a way to ease the anxiety of both my patient and her mother without compromising the care this little girl needed. I remembered I had purchased a pack of Lifesavers before work that night. I rummaged around in my pockets and came up with a whole, unopened pack. After getting mom’s permission, I offered them to S.H. This sweet little girl, who had been through more in five years than I have in 26, looked me in the eyes and said, “Thank you for not poking me until I was ready.” I will always remember S.H. and her mother. Since this early morning encounter I have had the honor of taking care of her on three other occasions. They always remember my name but to them I am known as the “Lifesaver nurse.” To this day I keep an unopened pack of lifesavers in my locker on the off chance that they will be needed again.

As we finalize our Magnet documents for submission to the ANCC, I can’t help but think back to the beginning of our Magnet journey here at SJO. It began way back in 2001. That year our RN turnover rate was at a high of 18% and we couldn’t hire an experienced nurse. They went elsewhere. That year we hired 100 new RNs (new graduates) and lost 105 experienced RNs, only to be further in trouble, losing years of accumulated RN expertise and spending millions of dollars (literally) in orientation hours and RN registry costs. It didn’t take a genius to realize we needed to do things differently if we were going to live up to the values of Dignity, Service, Excellence and Justice for our patients and our staff. How could we deliver great outcomes for our patients if we didn’t have a stable, empowered, competent workforce of nurses whose voices and expertise could lead patient safety and quality work? What did we do? We looked to the literature, finding everything we could on great workplaces for nurses and clinicians. It was the Magnet literature that outlined exactly what we needed to create: An empowered, highly engaged workforce. A practice environment that supported personal, professional and leadership development. The guarantee that the colleague standing next to you would be caring, competent and well trained. A collaborative, respectful environment that honored teamwork, collaboration and excellence. A core group of us from SJO, Mission and St. Jude began developing the road map for creating a Nursing Center of Excellence. This roadmap came directly from the Magnet model. It included developing a clinical ladder that rewarded expert nurses for staying at the bedside. It involved developing a robust shared governance council structure that highlights the voice of the bedside nurse in organizational decision making. It outlined the leadership development necessary for sustained achievement of strategic goals. It called for staffing models that matched the needs of the patient population served. So, how have we done? What has the Magnet journey done for us at SJO? Our RN turnover has plummeted from a high of
18% to a low of 7%, and this occurred well before the economic downturn. It has been sustained over many years. Cost savings to the organization on this indicator alone factors into the millions. The retention of RN expertise and knowledge is priceless. Our physician satisfaction scores with nursing care place us in the 97.7% of the PRC national database. The Institute for Healthcare Improvement has recognized SJO’s outcomes and requested our help in helping others, hence the Mentor status from IHI. SJO has received one of the two SJHS Quality Awards for the past five years. Our workplace injuries have decreased. Our nurse satisfaction scores rank in the top quartile nationally. Critical Care and Respiratory have together achieved zero ventilator acquired pneumonia for more than 47 months for their patients. And, when not busy taking care of patients, our nurses are back in school earning their BSN or MSN. Now, more than 50% of our RNs have their BSN, up from 30% when this journey began. Our Magnet journey has fueled a spirit of inquiry within our nursing ranks. SJO nurses are actively contributing to the growing body of research in nursing. This past year, nine articles were accepted for publication in nursing journals, and SJO nurses presented 27 podium or poster talks nationally. This work helps other hospitals learn and improve care to the entire community at large. The question of “Why Magnet?” should really be, “How could we not pursue Magnet?” The framework has proven itself to be highly effective in improving outcomes for patients. Is it a lot of work? YES. Does it take a financial investment? YES. Is there a Return on Investment? ABSOLUTELY! Empowered and accountable staff who “own” their outcomes and every year improve those outcomes, whether it be decreasing falls, pressure ulcers or infections, make this Magnet journey well worth the effort!
Katie Skelton, RN, NEA-BC, Chief Nursing Officer
2www.sjo.org/nursing
Why Magnet?
“Bless us as we dedicate these documents to Your glory,” Chaplain David Hodgson prayed. At left, he and Executive Nursing Director and Magnet Program Director Patti Aube, RN-BC, MSN, hold the flash drive containing the St. Joseph Hospital (SJO) Magnet Re-designation Documentation. It was submitted to the American Nurses Credentialing Center (ANCC) on January 31 following the “Blessing of the Documents” by Chaplain Hodgson in the Healing Garden. The event capped 10 months of intensive work gathering data for the submission. Many thanks to all of the Nursing team members and supporting staff who worked so diligently to tell our story, and whose exceptional patient care on a daily basis has made our Magnet designation and re-designation submission possible. We expect to hear our re-designation status in the spring and to welcome the Magnet surveyors to our campus sometime this summer. For more coverage of the event please see page 9.
Unpacking the New Knowledge, Innovations & Improvements Component
of the Magnet Journey
3www.sjo.org/nursing
How is new knowledge translated into nursing practice at St. Joseph Hospital (SJO)? How does St. Joseph Hospital support and foster its ongoing and plentiful innovations? For improvements grand and small to come to fruition, these structures are key:
• The SJO Institutional Review Board (IRB) is a multidisciplinary administrative body responsible for protecting the rights and welfare of human subjects choosing to participate in research studies conducted under the auspices of SJO. Along with physicians, legal counsel, a pharmacist, a non-scientific member and community members, the nurses serving on the IRB are Vivian Norman, RN, MSN, CCRN, and Tina Tillman, RN, BSN, OCN.
• The Office of Nursing Research (ONR) provides leadership and is the hub through which all Nursing research and related activities transpire. The office is currently comprised of two individuals, Nursing Research Facilitator Dana Rutledge, RN, PhD, and Assistant Research Facilitator Victoria Morrison, RN, MSN, FNP-BC.
• Nursing Councils, Special Interest Groups and Unit-Based Councils provide an excellent channel to introduce, implement and track the incorporation of new knowledge into nursing practice. For example:
» The Nursing Research Council’s (NRC’s) primary role is to facilitate, support and promote Nursing research, working closely with the Nursing Research facilitator. The current co-chairs are Beth Winokur, RN, MSN, PhD, and Dana Rutledge, RN, PhD.
» The Nursing Informatics Special Interest Group (NISIG) meets monthly and supports nursing needs specific to care delivery technology and database administration. Through the Design for Perfect Care initiative now well underway, the goal is to integrate the patient’s health information with current technology, thereby connecting our clinicians and patients with the right information when they need it to make decisions. Doris Fischer, RN, BSN, and Shannon Mori, RN, chair this SIG.
» Burlew Medical Library (www.burlewmedicallibrary.org) has one of the largest nursing journal collections in the hospital library community - approximately 100 print nursing journals and more than 150 electronic nursing journals. In addition, its blog at http://
evidencebasednursing. blogspot.com communicates Nursing research activities.
• Through Nursing Grand Rounds, SJO is able to share clinical expertise, the outcomes of Nursing research and other sources of evidence.
• The Clinical Institute is a physician-driven team, and physicians collaborate with nurses to provide evidence-based care. A few examples of this collaboration include the creation of the Patient Family Conference Progress Note, the Sepsis Order Sets and Algorithm, the Hospice GIP order set, the PCA order sets and all the Cath Lab order sets.
• Multidisciplinary Clinical Excellence Teams (CETs) were created as a means to bring nurses together with physicians to answer the question, “How can we improve patient care?” Each team has RN/MD co-chairs. They are: Acute Myocardial Infarction (AMI), Heart Failure (HF), Venous Thrombus Embolism (VTE), the Surgical Care Improvement Project (SCIP), Infection Prevention (IC), and the Cardiovascular Surgery (CV), Critical Illness and Acute
Stroke. Read more about their good work on page 4.
• St. Joseph Way Rapid Improvement Event (RIE) teams provide opportunities for SJO nurses to be intimately involved with problem-solving.
Numerous other structures and tools at SJO contribute to the implementation of new nursing knowledge, such as New Hire Orientation, Show Me the Evidence posters seen on the units, the Clinical Education Update newsletter and annual Skills Days. Renee notes, “Nursing leadership has worked hard to create a climate that promotes scholarly inquiry and evidence-based practice (EBP), and to ensure that every SJO nurse understands EBP, which is essential for effective and efficient patient care.”
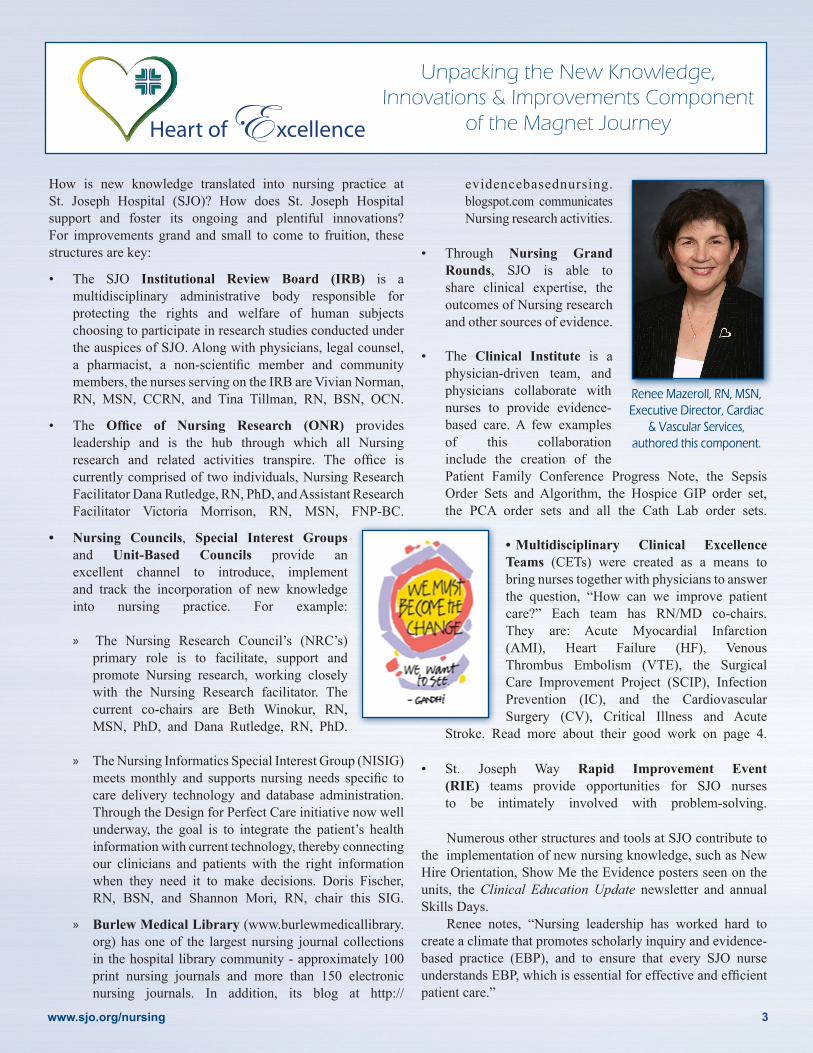
Renee Mazeroll, RN, MSN,Executive Director, Cardiac
& Vascular Services, authored this component.

Meditech 5.64 implementation this past December was just the beginning of the information technology advances we’ll be seeing in 2011 and beyond. Next up: the launch of the Emergency Department Management (EDM) system. Mentor training is set for March 21 - 25, with ED staff training to take place March 29 - April 22, and go-live on April 26. The EDM includes the Tracker and online ED Nursing Documentation which will enhance patient safety and satisfaction by improving patient flow and coordination of treatment. The EDM Tracker is interactive and allows the ED staff and physicians to document patient care functions and manage patient flow from a central point of entry. Inpatient units will also be able to view the Tracker and chief health complaint to help determine staffing and bed reservations for the unit. ED Nursing documentation will be reflected in MEDITECH, allowing staff on inpatient units to view ED documentation once a patient is admitted. This will improve patient care and enhance communication between the ED and the units. In June, inpatient units - initially the Orthopedic and Mother Baby Units - will start implementing an electronic medical
record with online clinical documentation, electronic Medication Administration (eMAR) and bedside medication verification (BMV), utilizing barcode technology. The BMV provides lots of checks and balances to ensure administration with the right patient, dose, time, method and medication. This fall, a new physician documentation system called PDoc will roll out. PDoc will enable online documentation of daily progress notes and pave the way for the next steps of electronic medical record (EMR) implementation. This will include a computerized physician order entry (CPOE), which physicians will be able to access from their home or office. “The Design for Perfect Care initiative is a major investment for our ministry,” states Design for Perfect Care Facilitator Tammy Alvarez, RN, MSN, CCRN. “Moving toward fully integrating an electronic medical record is not only a central piece of healthcare reform and the American Recovery and Reinvestment Act; it is the right thing to do for our patients.”
www.sjo.org/nursing
DPC: What’s Next?
Thank you to the following nurses who helped train staff as well as provide 24/7 support to the units during go-live of Meditech 5.64. The front-line mentors were able to answer questions, help staff adapt to the system and escalate any necessary issues. Design for Perfect Care Educator Karen Brooks, who coordinated mentoring for the launch, credited the mentors for much of the successful December 8 roll-out.RN MentorsMercedes AlojamientoJennifer AdrianKaryn AndesAlma AraqueJohanna ArmerdingErlinda ArnedoBrooke BaitchLeila BaleteCelerina BelesarioDenise BoydShelley BurkeJennifer CamposJenny CaoTheresa CimmarrustiSandra ColeMandy CosioMelinda CostelloKhanh DaoGail DenhamWendy EscobedoThorsten EvertErin FeilmeierSabrina FeltenbergerDoris FischerMercedes FloresTeodora FrigillanaRachel GassTanya GillespieCatherine GodoyTanya Greer
Debra HanamotoStephanie HarfordAmy HayesAmy HeerschapKacie HolmesDebra KahlerCamille KatigbakNeda KheirkhahLindsay KurthConnie LandayanLisa LanhamSong LeeApril LiwagChristine LongGilia LopezKathleen MajeskiPriscilla Malagon BonDiane MartinezSela MoaJennifer MockDennis MontejoShannon MoriPaz MunozAnitha MuraleedharanMary MurrayDawn NagelKristina NagelDiana NguyenQuynh NguyenDarleen NguyenJune Nguyen-Huynh
Angela PagnanelliNora ParboNita PatelJillian PayneCarrina PerezDarlene Mary PlandoRia Ann QuizonRichard RodriguezCherri SaleskyMarvi SanchezJennifer SariganCameron SchleppRobert SelwayJune SikesJill SneedHeather SternErric SwallowsRhona TristanArsenia TupasiRichard UrgelCelerine VillamorInez WhiteHong Tai Yu Clinical Coordinator MentorsLilia Acevedo-CosioGrace AlonzoRay ApterNorina AquinoStacy BoginJennifer Bonifacio
Linda Boose-ShutesYvette BoylePatricia BrandenburgerJaimie BrowneJennifer CaldeiraDanielle ChopraKort ColpeanEsmeralda De Los ReyesAlicia Dela CruzSusan DuncanLorna EstiandanNathan EvansNancy ForsueloRoxanne HaineySusan Hampton-AshBarbara HolmesAudrey JunorElizabeth KovacsKim LawrenceJeannine LoucksElizabeth MartinezKristen MerkhMelinda NguyenSandra OrellanaFilomena PahamotangCynthia PaulsenMaria RansilPatricia RudolphBrenda TalleyJacoba WalshTraci Warren
4

SACRED ENCOUNTERS / HEALTHIEST COMMUNITIES Kathy Keener, RN, BSN, OCN
5www.sjo.org/nursing
MB, an 82-year-old woman, presented to the Emergency Depart-ment with altered mental status and hypotension, with a barely palpable pulse. She had evidence of a urinary tract infection and septic shock and was treated with IV fluids, antibiotics and ste-roids. Slowly her condition stabilized and MB was admitted to 3 North Pulmonary for recovery. Recovery was complicated for MB because she also suffered from Alzheimer’s. Once MB began to wake up and became more alert, she was frightened by her unfamiliar surroundings. She was inconsolable, except when her family was present. Her fam-ily was her lifeline to the past and the only thing she knew. In the past, the one thing MB loved to do more than anything was to dance. Most of her 52 years of marriage with her husband were spent socializing with friends around the art of dancing. She especially loved square dancing and ballroom dancing. At her 50 year wedding anniversary, everyone was in awe watching them glide across the dance floor so effortlessly. After the death of her husband 10 years ago, MB’s mind was slowly robbed by the horrible effects of Alzheimer’s. Her vivacious personality slipped away and MB became just a shell of her for-mer self. On rare and random occasions MB would be given a glimpse into her past and be able to recall a pleasurable moment. Today was one of those special days. MB had gotten up to the chair for lunch but needed assistance to get back to bed. The NA and the daughter requested the assistance of the Lift Team. When Ray Singer walked into the room MB immediately perked up. Ray introduced himself, placed the safety belt around her waist and proceeded to stand her up. He then gave step-by-step instructions as to how he wanted her to move from the chair to the bed. He saw instantly that she was confused and the instruc-tions were too difficult for her to follow. He said to MB, “Do you know how to dance?” MB exclaimed with excitement,“Why yes, I love to dance!” Ray sang a happy melody and we watched in amazement as he led her in the direction in which he wanted her to go. MB gently laid her head on his shoulder and they swayed back and forth until he had her placed into bed as if she were a rare and precious gift. MB was so happy and she thanked him for the dance. For that brief moment, MB saw through the cobwebs of her memories and recalled the joy of dancing. Ray walked out of the room never knowing the impact of that Sacred Encounter. MB died three months later having never danced again. I wanted to take this opportunity to share this Sacred Encounter that I witnessed between Ray and my very precious gift, my Mother.
- Kathy Nielsen Keener
At the age of 4, Kathy Keener knew she wanted to be a nurse. When she began her nursing career 30 years ago, she prayed before her interview at St. Joseph Hospital that God would put her where He needed her. She wound up on the Oncology floor, which was not her first choice. She recalls, “It was physically and
emotionally draining, especially when I would connect with a patient and he or she died. After a year I dropped to my knees and prayed, ‘I can’t do this by myself. I need You to give me strength.’ I felt I was told, ‘Be as loving and compassionate as you can, and leave the rest to me.’ I learned that my job as an oncology nurse is to be there for that person at that moment in time. It was freeing for me to love them. Now, I can’t imagine doing anything else.” Kathy claims she has “discovered her purpose” in nursing and as a volunteer while serving on medical mission teams from Saddleback Church to places such as Haiti, Albania, Mexico and Africa. Three of Kathy’s mission trips have been to Kenya (pictured here). On her most recent visit in 2010, her 18-year-old daughter, who is thinking of becoming a nurse, also joined the team and “fell in love” with the people coming to their Oasis of Hope clinic. Kathy recounts that her team erected a minor treatment tent under an Acacia tree, and how some of the patients would walk all day to receive medical attention. “The affects of poverty, HIV/AIDS, malaria and parasitic infections are rampant,” she remarks. “Many of the children are orphans, and the women in the rural areas won’t even give their babies names until they are a year old because so many die.” At the end of their time in the clinic, the women came and sang for them and offered them a goat to thank them for their help. She shares, “It was an awakening to realize that God shaped me to do this type of work, and I feel I’ve gotten more out of it than I’ve given. It’s so satisfying, and you realize how fortunate we are to live in the United States. I am in awe that a lot of time, people who have so little are happier than we are, in the purest sense. It makes you a more caring person.”
PERFECT CARE / GROWTH
www.sjo.org/nursing
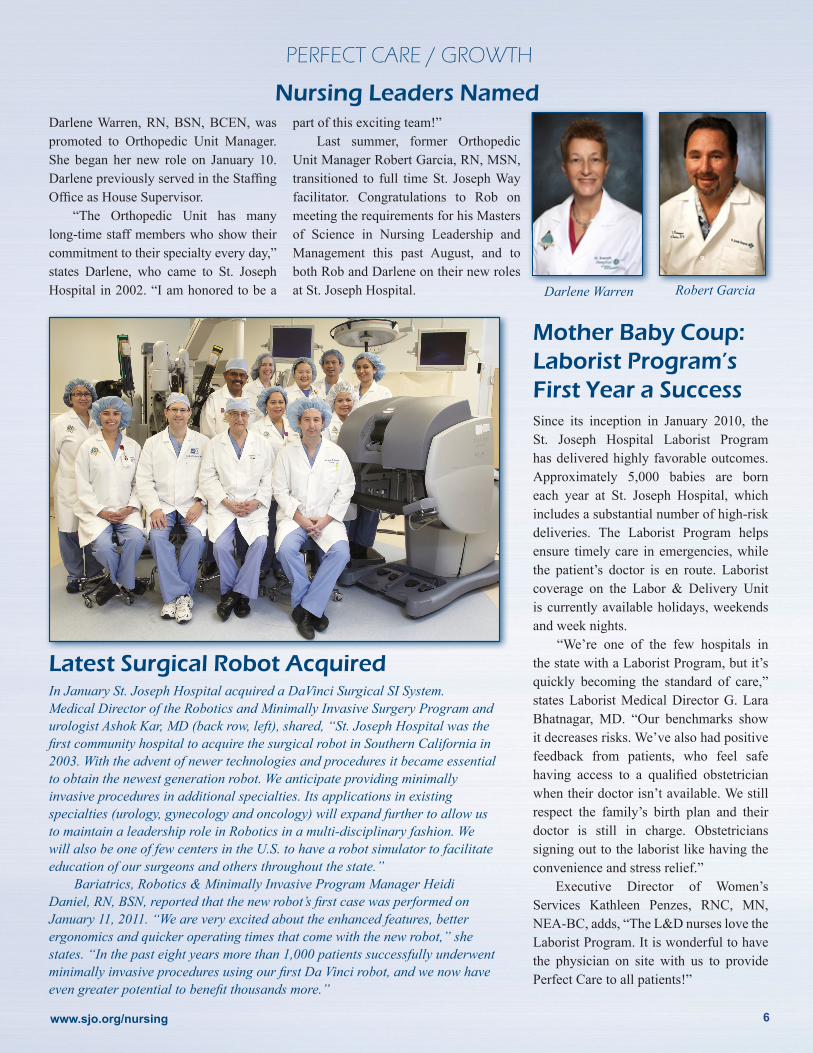
Latest Surgical Robot AcquiredIn January St. Joseph Hospital acquired a DaVinci Surgical SI System. Medical Director of the Robotics and Minimally Invasive Surgery Program and urologist Ashok Kar, MD (back row, left), shared, “St. Joseph Hospital was the first community hospital to acquire the surgical robot in Southern California in 2003. With the advent of newer technologies and procedures it became essential to obtain the newest generation robot. We anticipate providing minimally invasive procedures in additional specialties. Its applications in existing specialties (urology, gynecology and oncology) will expand further to allow us to maintain a leadership role in Robotics in a multi-disciplinary fashion. We will also be one of few centers in the U.S. to have a robot simulator to facilitate education of our surgeons and others throughout the state.” Bariatrics, Robotics & Minimally Invasive Program Manager Heidi Daniel, RN, BSN, reported that the new robot’s first case was performed on January 11, 2011. “We are very excited about the enhanced features, better ergonomics and quicker operating times that come with the new robot,” she states. “In the past eight years more than 1,000 patients successfully underwent minimally invasive procedures using our first Da Vinci robot, and we now have even greater potential to benefit thousands more.”
Mother Baby Coup: Laborist Program’s First Year a SuccessSince its inception in January 2010, the St. Joseph Hospital Laborist Program has delivered highly favorable outcomes. Approximately 5,000 babies are born each year at St. Joseph Hospital, which includes a substantial number of high-risk deliveries. The Laborist Program helps ensure timely care in emergencies, while the patient’s doctor is en route. Laborist coverage on the Labor & Delivery Unit is currently available holidays, weekends and week nights. “We’re one of the few hospitals in the state with a Laborist Program, but it’s quickly becoming the standard of care,” states Laborist Medical Director G. Lara Bhatnagar, MD. “Our benchmarks show it decreases risks. We’ve also had positive feedback from patients, who feel safe having access to a qualified obstetrician when their doctor isn’t available. We still respect the family’s birth plan and their doctor is still in charge. Obstetricians signing out to the laborist like having the convenience and stress relief.” Executive Director of Women’s Services Kathleen Penzes, RNC, MN, NEA-BC, adds, “The L&D nurses love the Laborist Program. It is wonderful to have the physician on site with us to provide Perfect Care to all patients!”
Darlene Warren, RN, BSN, BCEN, was promoted to Orthopedic Unit Manager. She began her new role on January 10. Darlene previously served in the Staffing Office as House Supervisor. “The Orthopedic Unit has many long-time staff members who show their commitment to their specialty every day,” states Darlene, who came to St. Joseph Hospital in 2002. “I am honored to be a
part of this exciting team!” Last summer, former Orthopedic Unit Manager Robert Garcia, RN, MSN, transitioned to full time St. Joseph Way facilitator. Congratulations to Rob on meeting the requirements for his Masters of Science in Nursing Leadership and Management this past August, and to both Rob and Darlene on their new roles at St. Joseph Hospital. Darlene Warren Robert Garcia
Nursing Leaders Named
6
Magnet Survey PreParation
Nurses: Test Your Knowledge1. St. Joseph Hospital nurses use a Professional Practice Model to visually describe:
___ A. How we practice
___ B. How we collaborate
___ C. How we communicate
___ D. How we develop professionally
___ E. All of the above
2. The target of our nursing practice, shown at the center of the model is:
___ A. Collaboration and Clinical Development
___ B. Patient, Care Team, Family and Community
___ C. Applying the four Core Values of our Ministry
3. “Why we do what we do” stems from our four core values, which are:
_______________________________________
_______________________________________
4. The three encircling Domains of Nursing Practice describe “how we do what we do.” They are:
_______________________________________
_______________________________________
5. The four supporting structures for Nursing surrounding the Professional Practice Model energize us. They are:
_______________________________________
_______________________________________
6. The Nursing Theory providing the framework for our nursing practice is called:
_______________________________________
______________________________________
Thank you for testing your knowledge of St. Joseph Hospital nursing practice. You will find the answers on page 9.
HEALTHIEST COMMUNITIES / GROWTHBiospecimen Repository Opens
The Center for Cancer Prevention and Treatment at St. Joseph Hospital has opened a Biospecimen Repository. After nearly three years of plan-ning and with generous contributions from the St. Joseph Hospital com-munity, the repository became operational in January 2011. “We are very excited to provide an evidence-based biobanking resource for researchers that will spur development of new therapies to treat and cure cancer,” stated Pathology Liaison Aaron Sassoon, MD, who leads the seven-member Biospecimen Repository team. “Not only are we one of the only community cancer centers in the nation with a biospecimen repository; we serve a population with greater diversity than is found in most academic centers, enabling us to procure diverse specimens.” To ensure specimen quality, the Repository is located in close proximity to the hospital’s outpatient surgery center, adjacent to the surgical pathology suite. Operational guidelines and infrastructure came from National Cancer Institute (NCI) best practices and NCI’s technologically advanced cancer Biomedical Informatics Grid (caBIG®) tools. St. Joseph Hospital was one of just 14 sites in the country and the only hospital on the West Coast to participate in the NCI Community Cancer Centers Program (NCCCP), a community-based cancer center network fostering cancer research, access and quality of care. “We hope to share this remarkable resource of biomedical information and tissue specimens with cancer research investigators locally, regionally and nationwide for insights into the risk, prevention and treatment of cancer,” said Lawrence D. Wagman, MD, Executive Medical Director of The Center for Cancer Prevention and Treatment.
PERFECT CARE
Cancer Center Accolades The Center for Cancer Prevention and Treatment at St. Joseph Hospital recently received a prestigious, three-year Accreditation with Commendation from the Commission on Cancer (CoC) of the American College of Surgeons. This is the highest level of accreditation from the CoC, awarded to programs that comply with all CoC standards and receive a commendation for one or more of the eligibility categories of standards. Accreditation by the CoC is given only to those facilities that have voluntarily committed to providing the highest level of cancer care and that undergo a rigorous evaluation and review of their performance and processes. This is SJO’s second consecutive Accreditation with Commendation. The Breast Program was named a “Center of Excellence” in accelerated partial breast irradiation (APBI) for its use of the SAVI™ applicator. The designation, by SAVI developer Cianna Medical, Inc., signals that SJO has one of the first cancer centers in the U.S. proficient in using this advanced treatment for women with early stage breast cancer. SAVI breast brachytherapy is performed as part of breast conservation therapy, which includes lumpectomy followed by radiation rather than mastectomy. It typically involves two treatments per day for five days - a shorter time frame than traditional, external beam radiation delivered over six or seven weeks. The SAVI device also allows for precise radiation delivery and minimizes radiation exposure of healthy tissue. Along with Intraoperative Radiation Therapy (IORT), it gives patients options in their fight with breast cancer, thereby providing them with a greater sense of control in their treatment and cancer journey.
7www.sjo.org/nursing
Clinical Excellence Teams received awards at the January St. Joseph Hospital’s (SJO’s) Board of Trustees meeting for outstanding performance in FY10 Perfect Care outcomes. With multidisciplinary members from across the hospital, these teams focused on select clinical conditions that contribute to our Perfect Care goals.AMI: (Heart Attack Care): Achieved Perfect Care for eight out of 12 months and ended the year with a failure rate of 3.3% (97% Perfect Care).
Critical Illness Clinical Excellence Team: Focused on early identification and treatment of sepsis and reducing overall mortality. We were identified as “Best Practice” nationally and by the St. Joseph Health System for achieving a mortality ratio of 0.67 (33% less than expected). This equates to 130 lives saved through evidence-based strategies for sepsis, end-of-life care and other conditions.
Heart Failure Clinical Excellence Team: Achieved six months of zero failures and an overall failure rate of 7.52%. In addition, they achieved zero readmissions for five of 12 months and an overall readmission rate of 4.98% (well below the national average for heart failure patients).
Our only Clinical Excellence Team that covers the continuum of care, Heart Failure CET members represent primary care physicians, Home Health, Hospice and the Patient Family Advisory Council.
Surgical Care Improvement Project (SCIP): While their work focuses on multiple surgical procedures, this award recognized them for their National Top Decile Performance for Total Hip and Knee Joint Replacement Surgery.
Critical Care Team: Doctors, nurses and respiratory therapists implemented and sus-tained an evidence-based, multidisciplinary approach to prevent Ventilator Associated Pneumonia (VAP) in our ICU patients. Their streak of 42 consecutive months of zero Ventilator Associated Pneumonia through FY10 is a best practice. They are currently at 45 months with zero VAPs. Infection Prevention Clinical Excel-lence Team: Everyone at SJO contributes to the prevention of hospital acquired in-fections and these exceptional outcomes:• Decreased incidence of hospital
acquired C.Difficile by 50% in one year-exceptional performance.
• Decreased incidence of hospital acquired Multi-Drug Resistant Organisms
(MRSA and VRE) by 45% in two years.
Central Line Infection Prevention sub-committee: Focused on developing standard protocols to care for these patients and trained all staff to adhere to the protocols. In FY10 our caregivers achieved a 42% reduction in Central Line Associated Blood Stream Infections (CLABSI) and in two years we reduced these infections by 62% by utilizing evidence-based medicine strategies, such as checklists and bundles. These outcomes also represent exceptional breakthrough performance.
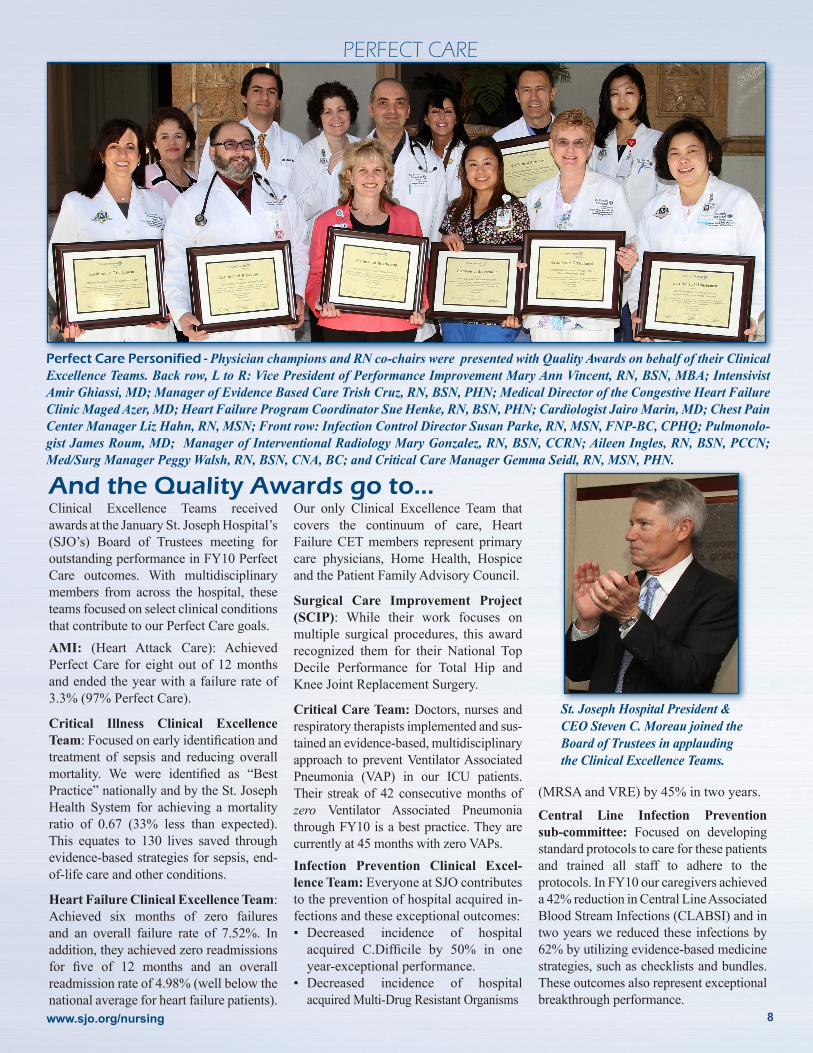
Perfect Care Personified - Physician champions and RN co-chairs were presented with Quality Awards on behalf of their Clinical Excellence Teams. Back row, L to R: Vice President of Performance Improvement Mary Ann Vincent, RN, BSN, MBA; Intensivist Amir Ghiassi, MD; Manager of Evidence Based Care Trish Cruz, RN, BSN, PHN; Medical Director of the Congestive Heart Failure Clinic Maged Azer, MD; Heart Failure Program Coordinator Sue Henke, RN, BSN, PHN; Cardiologist Jairo Marin, MD; Chest Pain Center Manager Liz Hahn, RN, MSN; Front row: Infection Control Director Susan Parke, RN, MSN, FNP-BC, CPHQ; Pulmonolo-gist James Roum, MD; Manager of Interventional Radiology Mary Gonzalez, RN, BSN, CCRN; Aileen Ingles, RN, BSN, PCCN; Med/Surg Manager Peggy Walsh, RN, BSN, CNA, BC; and Critical Care Manager Gemma Seidl, RN, MSN, PHN.
PERFECT CARE
And the Quality Awards go to...
St. Joseph Hospital President & CEO Steven C. Moreau joined the Board of Trustees in applauding the Clinical Excellence Teams.
www.sjo.org/nursing 8

The January 31 Blessing of the Documents by Chaplain David Hodgson (above, right) and send-off of St. Joseph Hospital’s web-based Magnet Re-designation submission was a major Magnet moment for our ministry. Data gathered from throughout the organization over the last 10 months tells a remarkable story of Nursing excellence at St. Joseph Hospital. The thumb-size flash drive (shown at left with Maggie) contains the documentation, which was even more detailed than the 15-inch printed version produced for the original submission in 2008. SJO’s Magnet website incorporates a whopping 987 links and 888 PDF documents for surveyors to review.
Clinical Ed Program Coordinator Caroline Rae, RN, BSN, and ER’s Amy Waunch, MSN, FNP, CEN, joined the ceremony and celebration. Below: Case Manager & Critical Care Nurse Cara Buenaventura, RN, Magnet Coordinator Soudi Bogert, RN, BSN, and other Magnet Ambassadors brought M&Ms to the Nursing Units to mark the milestone.
Director of Communications Cathy Semar edited the massive document and built the website; Executive Director Pat Brydges, RN, BSN, MHA, ACM, wrote much of the Structural Empowerment component.Below: Orthopedic Unit Manager Darlene Warren, RN, BSN, BCEN, and Medical Pulmonary Manager Cathy Leong, RN, also attended the Blessing.
Magnet Milestone
To illustrate our four core values and connect them to the Magnet components covered in the Magnet Re-designation documents, the artwork of Sister Madeleva Williams, CSJ, was used for the website title pages. The quotes appearing on the artwork follow:
Organizational
Overview
For Joseph it wasn’t a question of success, it was being faithful
to the mix we call life.
Transformational Leadership
“A candle loses nothing by lighting another candle.”
Erin Majors
Structural Empowerment
“Alone we can do so littletogether we can do so much.”
Helen Keller
Exemplary Professional Practice
“My life is my message.”Gandhi
New Knowledge, Innovations & Improvements
“We must become the change we want to see.”
Gandhi9
www.sjo.org/nursing
1100W.StewartDriveOrange,CA92868www.sjo.org
10
February 2011Magnet re-designation survey education and preparation
Tuesday, February 22Burlew Medical Library Event Experts from UpToDate, OVID, and EBSCOHost will be on campus for hands-on training in the latest evidence-based research tools available to all St. Joseph Hospital staff. Stop by Burlew Medical Library from 11 a.m.-1 p.m. for lunch and a demon-stration. For details contact us at 714-771-8291 or [email protected].
Saturday, February 26Many Hearts, One Passion community event from 9 a.m. - 2 p.m.This community event will be held in the St. Joseph Hospital Outpatient Pavilion and feature physician lectures, free health screenings, vendor exhibits and opportunity drawings.
Monday, March 11Golf Tournament sponsored by AramarkFor volunteer and play information visit www.sjo.org/waystogive
Wednesday, March 30March Madness! This full day event will includ Magnet re-designation journey updates, a review of the evidence submitted, Council updates, Component updates, Special program highlights and research and EBP highlights
Wednesday, March 30National Doctors’ DayExpress appreciation to our dedicated physicians!
April 10 - 16 National Volunteer WeekPlease join in recognizing our treasured volunteers!
April 30 Donate Life Run/Walk A St. Joseph Hospital team is forming for this 5K/1K run/walk to educate and inspire the community about organ and tissue donation and benefit Donate Life California Organ and Tissue Donor Registry. Starts at Memorial Grove at Cal State Fullerton. Visit www.donatelifeoc.org or call the Kidney Transplant Center, 714-771-8033.
May 6 - 12National Nurses Week The Blessing of the Hands will be May 9, 10 a.m. in the Bldg. 2 Healing Garden. The Nurse Week Awards Ceremony will be Tuesday, May 10, 5 p.m. in the Sister Frances Dunn Bldg (CR I, II, III). A Nurse Week Reception follows from 6 - 9 p.m.
Saturday, May 14Melanoma Symposium from 7:30 a.m. to 2 p.m.Category 1 CME credit toward credit for contact hours. Call 1-866-714-1777.
June 26, 201115th Annual Circles of Life Fashion Show & Luncheon10 a.m. - 2:15 p.m. at the Hilton Anaheim, benefitting the Neuro-Oncology Program at The Center for Cancer Prevention and Treatment. For details call the St. Joseph Hospital Foundation, 714-347-7900.
Summer 2011Magnet surveyor site visit; a celebration of our success!
Calendar of Events
Magnet Survey Readiness: Testing Nursing Knowledge(Answers to questions on page 7)
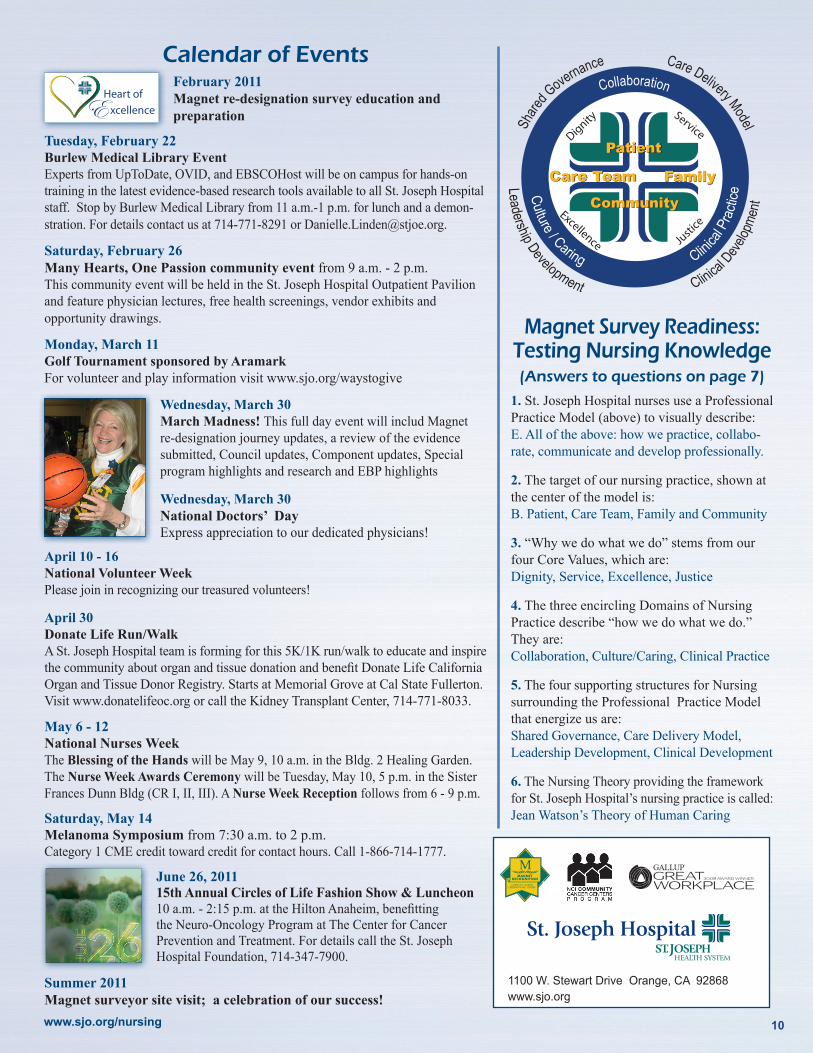
1. St. Joseph Hospital nurses use a Professional Practice Model (above) to visually describe:E. All of the above: how we practice, collabo-rate, communicate and develop professionally.
2. The target of our nursing practice, shown at the center of the model is:B. Patient, Care Team, Family and Community
3. “Why we do what we do” stems from our four Core Values, which are:Dignity, Service, Excellence, Justice
4. The three encircling Domains of Nursing Practice describe “how we do what we do.” They are: Collaboration, Culture/Caring, Clinical Practice
5. The four supporting structures for Nursing surrounding the Professional Practice Model that energize us are:Shared Governance, Care Delivery Model, Leadership Development, Clinical Development
6. The Nursing Theory providing the framework for St. Joseph Hospital’s nursing practice is called:Jean Watson’s Theory of Human Caring
Dignity
Justice
Excellence
ServicePatient
CommunityCommunity
Care TeamCare Team FamilyFamily
Culture / Caring C
linica
l Pra
ctice
Share
d Governance Care Delivery Model
Nursing Center of Excellence
www.sjo.org/nursing